El Paso’s Integrated Injury Clinic: One-Stop Care for Faster Recovery and Strong Legal Support
If you got hurt in a car crash or at work in El Paso, Texas, you know how frustrating it can be. You go to one place for an exam, another for therapy, and still another for special treatments. Papers get lost. Your story gets told many times. Healing slows down. An integrated, multidisciplinary injury clinic solves this problem. Everything happens under one roof. A team of experts works together on your care. They handle medical checks, hands-on therapy, and advanced healing methods. At the same time, they build clear, complete records that help your legal or workers’ compensation case.
This kind of care is different from going to separate offices. You get faster answers, smoother progress, and stronger support for your claim.
Why an Integrated Health System Works Better
Ordinary clinics often focus on one thing. You might get only adjustments or only medications. An integrated clinic brings many experts together in the same place. They share one plan for you. This stops gaps in care and mixed messages.
Here are the main advantages:
One team, one story: Every provider sees your full history and current progress. No one works in the dark.
Faster decisions: If you need a new test or different therapy, the group talks it over quickly.
Better healing: Treatments work in tandem. Chiropractic care improves movement while medical oversight watches your overall health.
Clear records from day one: Everything gets written down in one system. This matters a lot for insurance and legal needs.
Patients who use this model often feel less stressed. They spend less time driving between offices and more time actually getting better.
How the Team Works Together for You
In a true multidisciplinary setup, each expert brings their skills. Nurse practitioners handle full health evaluations. They can order tests, manage medications as needed, and monitor for other health issues that might slow healing.
Physical therapists, massage therapists, and chiropractors team up on your body’s movement. They improve flexibility, strength, and posture. Chiropractic adjustments help the spine and joints work better. Physical therapy builds safe exercises. Massage eases tight muscles. Together, they create a plan that fits your exact injuries.
This is not random care. It is coordinated. Everyone knows what the others are doing. That teamwork often leads to quicker pain relief and better long-term results.
Special Treatments That Help Serious or Lasting Injuries
Some injuries need more than basic care. Car accidents and work injuries can damage deep tissues, nerves, or joints. An integrated clinic offers modern options that directly target the problem.
Here are treatments often used together:
Spinal decompression: A special table gently stretches your spine. This takes pressure off pinched nerves and bulging discs. Many people feel relief from sciatica or radiating leg pain.
MLS laser and shockwave therapy: These use light or sound waves to wake up your body’s healing cells. They lower swelling and help soft tissues repair without drugs or surgery.
Epidural injections: When nerves are very irritated, guided injections can calm the area so you can move and heal.
Regenerative therapies: Treatments such as PRP (platelet-rich plasma), PRF (platelet-rich fibrin), and MFAT (micro-fragmented adipose tissue) use components of your blood or fat. They are placed exactly where tissue is damaged to support natural repair.
These options go beyond what a basic clinic usually offers. They aim at the root of the injury rather than merely masking pain.
Strong Medical-Legal Documentation That Protects Your Case
When your injury comes from a car accident or a job, good records are just as important as good treatment. Insurance companies and lawyers need proof. They want to see what happened, how bad it is, and that the care you received was necessary.
An integrated team creates one complete file. It includes:
Your accident story and first exam findings
Objective tests like range of motion, strength checks, and imaging
Daily notes on how you feel and what treatments you receive
Progress reports that show improvement or ongoing limits
A final summary that explains the lasting effects on your life and work
This kind of documentation helps personal injury lawyers build a stronger case. It shows a clear link between the crash or incident and your injuries. It also proves you followed a real treatment plan.
Many clinics work directly with attorneys. They send updates quickly and often handle cases on a lien basis. This means you can focus on healing while the legal side stays organized.
Expert Care Led by Dr. Alex Jimenez and Dr. Maria Guadalupe Cardenas in El Paso
At Injury Medical Clinic PA in El Paso, this integrated model is led by experienced professionals who understand both health and legal needs.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, CCST, CFMP, IFMCP, ATN, is dual-licensed as a chiropractor and board-certified family nurse practitioner. He has spent decades helping people with car accident injuries, work injuries, whiplash, sciatica, and soft tissue damage. His clinical observations focus on treating the whole person. He looks at root causes, not just symptoms. He stresses careful documentation with clear findings and progress measures, especially when a case involves an auto or work injury claim. His practice combines chiropractic care, functional medicine, rehabilitation, and regenerative options under one roof.
Working alongside him is Dr. Maria Guadalupe Cardenas, MD. She is board-certified in internal medicine with over 40 years of experience. Her NPI is 1164426749, and her Texas MD license is J2933. She serves as Medical Director and Collaborative Physician. In this multidisciplinary setting, she provides medical oversight, reviews overall health, guides advanced procedures, and helps ensure compliance with Texas rules.
Together, they create a powerful team. Chiropractic care from Dr. Jimenez addresses alignment, nerves, and movement. Medical direction from Dr. Cardenas provides safety, diagnostic, and medication management as needed. Functional medicine, personal injury documentation, and rehabilitation services all connect in the same location. This is the kind of collaborative model common in high-quality integrative injury clinics.
Your Simple Path to Recovery in El Paso
Here is what the journey usually looks like:
You call or come in for an evaluation. A nurse practitioner or medical director, along with the chiropractic team, sees you together.
They create one clear plan that may include adjustments, therapy, advanced treatments, or regenerative options.
You receive care in one place. Notes stay organized from the first visit to the last.
Progress is tracked and shared with your lawyer or insurance when needed.
You heal with less stress and stronger support for your claim.
Many patients notice they move better sooner and have less confusion about next steps.
Choose Coordinated Care for Your Injury
If you want care that treats your injury and protects your legal position, an integrated multidisciplinary clinic in El Paso is worth considering. You get medical diagnostics, physical therapy, advanced healing therapies, and solid documentation all in one coordinated system. Dr. Alex Jimenez and Dr. Maria Guadalupe Cardenas lead a team that puts your recovery and your case first.
You do not have to piece your care together alone. One roof, one team, one clear plan can make a real difference in how fast you feel better and how well your case is supported.
IV Infusion Therapy Benefits for Athletes: Faster Recovery After Tough Workouts and Events
After a long race, intense game, or heavy training week, your body can feel completely drained. You might feel exhausted, sore, thirsty, and slow to bounce back. Drinking water and eating nourishing food help a lot, but sometimes your stomach feels upset, or you need faster help to restore fluids and nutrients to your system. That is where IV infusion therapy can step in as a helpful tool.
IV infusion therapy puts fluids, electrolytes, vitamins, and other nutrients straight into your bloodstream through a small needle in your arm. This method provides your body with nearly 100 percent absorption because it bypasses the digestive system entirely. In sports, it serves as a targeted way to fix real problems like low fluid levels or nutrient shortages after intense effort. It is not a magic shortcut for healthy athletes who can eat and drink normally. Instead, it acts as a clinical support when your body is depleted and needs quick replenishment to recover and prepare for the next challenge.
Many athletes use this approach to feel better faster so they can return to training or competition with more energy and less downtime.
What IV Therapy Actually Does for Athletes
IV therapy delivers a mixture of saline or similar fluids, along with vitamins and minerals, directly into your bloodstream. This helps replace what you lose from heavy sweating, hard breathing, and muscle work. The process usually takes 30 to 60 minutes while you rest comfortably.
The main goals include restoring fluid balance, easing muscle fatigue, supporting energy production inside your cells, and calming inflammation that builds up during tough sessions. When done properly under medical guidance, it can shorten the time you feel wiped out after big efforts.
Rapid Rehydration When Oral Fluids Are Not Enough
During long endurance events or intense training camps, you can lose a large amount of water and important salts, such as sodium and potassium, through sweat. This drops your blood volume and can leave you feeling weak or dizzy. If you also have stomach upset or nausea, drinking large amounts of fluid becomes hard or even impossible.
IV therapy solves this by sending fluids and electrolytes straight into your circulation. Your body absorbs them right away instead of waiting for your gut to process them. This method works especially well when high-intensity exercise has already pulled blood away from your stomach to your working muscles, slowing normal digestion. Athletes often notice they feel rehydrated and more stable much quicker than with sports drinks alone.
Bypassing Digestion for Better Nutrient Delivery
Your digestive system sometimes struggles after very hard workouts. Blood flow shifts to your muscles, and gut movement can slow down. Oral supplements or drinks may not absorb well in these moments.
IV infusions avoid that problem completely. The nutrients go directly into your blood and reach your cells fast. This means depleted muscles and organs get what they need without delay. The result is faster support for repair and energy restoration than waiting for your stomach to do the work.
Reducing Inflammation and Muscle Soreness
Hard exercise causes minor damage to muscle fibers and produces additional free radicals that induce oxidative stress. This leads to delayed-onset muscle soreness (DOMS), which can make the next day or two feel stiff and painful.
Certain ingredients in athletic IV drips help fight this. Amino acids such as glutamine and arginine support muscle repair and calm inflammation. Antioxidants like vitamin C and glutathione help clear waste products and protect cells from extra stress. Many athletes report less lingering soreness and faster return to comfortable movement when these supports are added at the right time.
Supporting Cellular Energy and Recovery
Inside your cells are tiny structures called mitochondria that turn nutrients into usable energy. After intense training, these powerhouses can become stressed or less efficient. IV formulas often include magnesium, B-complex vitamins, vitamin B12, and NAD+ to give them direct support.
Magnesium helps muscles relax and prevents cramps while keeping your heart rhythm steady. B vitamins assist in turning food into energy at the cellular level. NAD+ aids in repairing small cell damage and keeping energy production running smoothly. Together, these nutrients help your body handle the repair work from training sessions more effectively.
Common Nutrients in Athletic IV Fluids and Their Roles
Here are some of the key ingredients often used and why they matter for active people:
Magnesium: Helps tight muscles relax, reduces cramp risk, and supports steady heart rhythm during and after exercise.
B-Complex Vitamins and B12: Aid everyday cell metabolism and energy creation so you feel less drained.
Amino Acids (such as Glutamine): Encourage protein building in muscles and help repair the small tears that come from hard training.
Vitamin C and Zinc: Act as antioxidants to fight free radicals created during workouts and support your immune system when training stress is high.
NAD+: Supports cell repair, DNA maintenance, and efficient energy production inside the mitochondria.
These are chosen based on what your body typically loses or uses up during demanding activity.
Important Anti-Doping Rules Every Competitive Athlete Must Know
If you compete at a level where drug testing happens, you need to understand the rules set by the World Anti-Doping Agency (WADA) and the U.S. Anti-Doping Agency (USADA). IV infusions or injections that total more than 100 milliliters in any 12-hour period are prohibited both in and out of competition. This limit applies even if the fluid contains only permitted substances, such as vitamins or saline.
Exceptions exist mainly for true medical needs:
Treatment inside a hospital or during emergency transport to a hospital.
Care given as part of surgery or certain diagnostic tests.
Urgent medical situations handled in a hospital-linked urgent care setting.
Three main reasons explain the restriction:
Large fluid volumes can temporarily increase blood plasma levels, which may improve heart and circulation performance for a short time.
IVs can sometimes interfere with how labs detect other banned substances in urine samples.
Quick changes in blood volume and values can affect the Athlete Biological Passport system that tracks an athlete’s blood markers over time.
Most everyday recovery IVs given in wellness clinics, hotel rooms, or non-hospital settings fall under the prohibited category if they exceed the volume limit. Always check with your sport’s governing body or a knowledgeable medical professional before considering any IV treatment if you are a tested athlete. In true emergencies, get medical care first and handle paperwork afterward.
IV Therapy Works Best as Part of a Bigger Recovery Plan
IV infusion therapy gives fast support when your body is low on fluids or nutrients. However, it works best alongside the basics: consistent quality sleep, proper daily fueling with whole foods, steady oral hydration, and smart training loads. Experts note that in most situations, drinking fluids and eating balanced meals remain the preferred and sufficient methods. IV therapy shines as an extra option during extreme events, multi-day competitions, or when stomach issues block normal intake.
Integrative Care That Supports Athletes in El Paso, Texas
Athletes looking for well-rounded support often benefit from clinics that combine different types of care under one roof. In El Paso, Texas, Injury Medical Clinic PA offers this kind of integrated approach. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, brings extensive experience in chiropractic and functional medicine, helping people recover from injuries and improve performance. He works closely with Dr. Maria Guadalupe Cardenas, MD, a board-certified internal medicine physician with more than 40 years of experience. She serves as Medical Director and Collaborative Physician, providing medical oversight for the team.
This setup allows chiropractic care for spine alignment, nervous system health, and mobility to work together with medical direction for therapies that may include IV infusions when appropriate. The clinic also emphasizes functional medicine to address root causes of fatigue or slow recovery, personal injury care, and structured rehabilitation programs. Clinical observations from Dr. Jimenez highlight that athletes recover better when care addresses the whole person—alignment, inflammation levels, nutrient delivery, and nervous system balance—rather than isolated symptoms. When IV therapy fits into a personalized plan, having an experienced internal medicine physician’s oversight helps ensure safety and proper use in accordance with the rules.
Many patients appreciate this team model because it combines hands-on therapies with advanced supportive options in a single coordinated setting.
Final Thoughts on Using IV Therapy Wisely
IV infusion therapy can help athletes rehydrate quickly, deliver key nutrients fast, ease inflammation, and support cellular energy after demanding efforts. IV therapy serves as a useful clinical tool when your body is truly depleted and oral methods fall short. At the same time, it is not a replacement for daily healthy habits or a way around anti-doping regulations.
If you train hard and sometimes struggle with recovery, speak with a qualified healthcare provider who understands the demands of sports and local regulations. They can help decide whether this option makes sense for your specific situation and guide you safely. When used thoughtfully as part of a complete plan, IV therapy can help you get back to feeling and performing at your best.
IV Infusion Therapy: How It Delivers Vitamins and Nutrients Straight to Your Body
IV infusion therapy puts vitamins, minerals, and fluids directly into your bloodstream. This bypasses the digestive tract, so your body can use more of the nutrients more quickly and fully. Clinics often use it to support immune function, fix dehydration, ease chronic fatigue, and correct nutritional shortfalls that oral supplements sometimes cannot fix well.
Many people feel run down, foggy, or slow to recover because their gut does not absorb everything from food or pills. IV therapy changes that by sending the mixture straight into circulation through a small tube placed in the arm. The result is higher amounts of nutrients reaching your cells faster than you can usually get from eating or swallowing capsules.
How Intravenous Therapy Works
Intravenous (IV) therapy uses a sterile mix of vitamins, minerals, and amino acids. A trained professional inserts a thin catheter into a vein, usually in the arm or hand. The liquid then drips in over 30 to 60 minutes while you rest in a comfortable chair.
Because it bypasses the stomach and intestines, the body absorbs nearly 100 percent of the nutrients. Oral supplements often lose a large portion during digestion. IV delivery avoids that loss and gives a rapid boost when someone needs quick rehydration or higher nutrient levels.
Why People Choose IV Infusion Therapy
Clinics report several common reasons patients try this therapy. Here are the main ones explained simply:
Fast hydration and electrolyte balance — After illness, intense workouts, travel, or long days, fluids and minerals go straight in to restore balance quickly.
More steady energy — B vitamins, magnesium, and other nutrients help cells produce energy. Many people notice less afternoon drag and better focus.
Immune support — High amounts of vitamin C, zinc, and antioxidants can give the body’s defense system extra help during cold and flu season or times of stress.
Recovery from physical stress — Athletes, active workers, and people healing from injuries often use it to supply building blocks for tissue repair and to reduce downtime.
Filling nutrition gaps — When digestion is off due to stress, medications, or long-term conditions, IV can deliver what the gut is missing.
These effects happen because the nutrients reach cells directly. Still, results vary from person to person. What works well for one individual may feel different for another.
IV Therapy Inside an Integrative Care Team
When an integrative chiropractic and functional medicine clinic offers IV therapy, patients gain extra layers of support. The approach focuses on three important ideas: personalized and data-driven treatment, a comprehensive care team, and a root-cause focus.
The team reviews lab work, health history, symptoms, and lifestyle before recommending a formula. They do not use a one-size-fits-all drip. Instead, they match the mix to what the person actually needs. This data-driven step helps avoid unnecessary or poorly matched nutrients.
A full care team means different experts work together. Chiropractic care addresses spinal alignment and nerve function. Functional medicine explores gut health, inflammation, and lifestyle factors. Medical oversight adds safety checks and the ability to handle more complex health pictures. Rehabilitation and personal injury support fit in when someone is recovering from accidents or ongoing pain.
It is crucial to consult a qualified healthcare professional to ensure the treatment aligns with your unique health profile and objectives, as individual needs and responses to IV therapies can vary.
How One El Paso Clinic Combines These Services
At Injury Medical Clinic PA in El Paso, Texas, this team model is in action every day. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, brings decades of experience in chiropractic care and advanced functional and integrative approaches. He works closely with Dr. Maria Guadalupe Cardenas, MD, a board-certified internist (NPI #1164426749, Texas MD License #J2933) with more than 40 years of experience.
Dr. Cardenas serves as Medical Director and Collaborative Physician. Her role provides medical direction and oversight for procedures such as IV infusions. This partnership is common in integrative or injury-focused clinics: the chiropractor handles structural and nervous system care, while the medical doctor ensures the safe, appropriate use of advanced therapies.
Patients receive coordinated care. Someone coming in after a car accident might receive chiropractic adjustments for whiplash, rehabilitation exercises, and, when appropriate, IV nutrients to support healing and energy. The medical oversight helps the team monitor interactions, select safe doses, and track lab results when needed. Dr. Jimenez has observed in his clinical work that patients with lingering fatigue, slow recovery, or chronic discomfort after injuries often respond better when nutrition and hydration are optimized alongside hands-on treatments.
This multidisciplinary setup allows the clinic to address the whole person rather than isolated symptoms. Chiropractic improves movement and nerve signaling. Functional medicine targets underlying drivers like inflammation or gut issues. IV therapy provides rapid nutritional support when oral intake is insufficient. Personal injury and rehabilitation services tie everything together, helping patients return to daily life with less pain and greater function.
What a Typical Session Looks Like
Most visits follow a clear, comfortable flow:
You meet with a provider to review your health history, current symptoms, and any recent labs.
The team selects or customizes a nutrient formula based on your goals.
A small catheter is placed in your arm (most people feel only a quick pinch).
You relax for 30–60 minutes while the solution drips in. Many people read, listen to music, or nap.
The catheter is removed, and you receive simple aftercare instructions, such as drinking extra water and resting as needed.
The whole process is designed to be low-stress. Clinics with proper medical oversight keep emergency supplies and trained staff on hand.
Safety and Smart Choices
IV therapy is generally well tolerated when performed by licensed professionals in a clinical setting. Mild side effects can include temporary bruising or soreness at the insertion site. More serious risks, such as infection or nutrient overload, are rare but possible, which is why medical supervision matters.
Experts note that while many people report feeling better, high-quality studies on broad wellness benefits for otherwise healthy individuals are still limited. IV therapy works best as one tool inside a larger plan that includes good nutrition, movement, sleep, and treatment of any underlying conditions. It is not a replacement for a healthy lifestyle or prescribed medical care.
People with certain conditions (kidney disease, heart issues, or specific medication regimens) should always check with their doctor first. In a clinic like the one described, the collaborative MD-NP team helps screen for these factors before any drip begins.
Putting It All Together
IV infusion therapy gives your body a direct route for vitamins, minerals, and fluids when you need fast, high-level support. By skipping digestion, it delivers higher usable amounts in less time. In an integrative setting that includes chiropractic care, functional medicine, rehabilitation, and strong medical oversight, it becomes part of a broader strategy aimed at addressing root causes and achieving lasting improvement.
Whether you are dealing with everyday fatigue, recovering from physical stress, or simply want to optimize how you feel, the key is to work with qualified professionals who personalize their approach. Clinics that combine these services under proper medical direction, such as the team model in El Paso, demonstrate how different therapies can support one another for better overall results.
Talk with your healthcare provider to see if IV infusion therapy fits your health picture. When used thoughtfully, it can be a helpful step on the path to feeling stronger, recovering faster, and supporting your body’s natural ability to heal and perform.
Regenerative Therapies Combined with Chiropractic Care Offer New Hope for Sports and Auto Accident Injuries in El Paso
Many people in El Paso deal with ongoing pain and limited movement after sports injuries or car accidents. Simple rest or basic physical therapy often helps at first, but sometimes healing stalls. Tissues stay inflamed, joints feel stiff, and daily life or sports become difficult again. When that happens, more people look for advanced options that work with the body instead of just covering up symptoms.
Regenerative therapies and integrative chiropractic care team up to tackle these tough problems. They focus on real repair at the tissue level while also fixing how the body moves. This combined approach helps many patients get back to feeling better and moving easier without jumping straight to surgery.
Why Standard Treatments Sometimes Fall Short
Injuries from sports collisions or car crashes often damage more than one area. Muscles tear, ligaments stretch, tendons become inflamed, and spinal discs or joints become irritated. Swelling and scar tissue can block normal blood flow and healing signals.
Physical therapy and rest build strength and reduce pain for many people. Yet when progress plateaus, underlying tissue damage or poor joint alignment may still be holding back recovery. That is when patients often seek care that actively supports the body’s repair systems instead of only managing symptoms.
What Regenerative Therapies Actually Do
Regenerative medicine uses materials from your body to kick-start healing. These treatments deliver growth factors and helpful cells directly to the damaged area. The goal is to lower inflammation, encourage new tissue growth, and improve long-term function.
Three main options stand out for musculoskeletal and spinal injuries:
PRP (platelet-rich plasma) comes from a small sample of your blood. The blood is spun in a machine to concentrate platelets, which carry natural growth factors. Doctors inject this concentrated solution into tendons, ligaments, joints, or around nerves. The growth factors signal cells to repair and rebuild.
PFP (platelet-fibrin products) uses protein concentrates from your blood. These capture growth factors and create a stronger, longer-lasting healing signal for tissues that have not responded well to simpler treatments.
MFAT (microfragmented adipose tissue) takes a small amount of your own fat tissue, processes it into tiny fragments, and injects it. The fat contains supportive cells and signaling factors that cushion joints and help repair cartilage, tendons, and soft tissues.
These are called orthobiologics because they come from your biology. They carry a low risk of allergic reactions or rejection since they use your materials.
Epidural injections sometimes join the plan for spine-related pain and nerve irritation. Under careful medical guidance, they reduce inflammation around spinal nerves while the regenerative injections work to repair deeper tissue.
How Chiropractic Care Completes the Picture
Injections alone help tissues heal, but they do not fix how the bones, joints, and muscles line up or move. That is where chiropractic adjustments come in. Gentle, precise realignments improve joint mobility, ease muscle tension, and restore better posture and movement patterns.
When regenerative injections and chiropractic care happen together, the results often last longer. The injections create a better healing environment inside the tissues. The adjustments keep the joints moving correctly so that new tissue forms properly and does not get stressed again. This partnership addresses both the biology of repair and the mechanics of the body.
The Strength of a True Multidisciplinary Team
Patients get the best results when they receive care from a well-established integrative and functional medicine clinic that brings different experts together under one roof. At Injury Medical Clinic PA in El Paso, Texas, the team combines advanced regenerative procedures with chiropractic expertise, functional medicine, rehabilitation, and personal injury support.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, leads the clinical approach. With decades of experience as a chiropractor and additional training as a board-certified family nurse practitioner, he focuses on whole-person recovery. His clinical observations show that patients with sports trauma or old auto accident injuries often improve when care targets both tissue repair and nervous system function. He uses detailed exams, imaging, and personalized plans that include regenerative injections, adjustments, rehabilitation, and lifestyle support.
Dr. Maria Guadalupe Cardenas, MD, a board-certified internal medicine physician with over 40 years of experience (NPI #1164426749, Texas MD License #J2933), serves as Medical Director and Collaborative Physician. She provides medical oversight for procedures, ensures safety and compliance, manages complex health factors, and brings an internal medicine perspective to every case. This collaboration means patients receive both expert spinal and musculoskeletal care from Dr. Jimenez and broad medical direction from Dr. Cardenas.
This setup is common in high-quality integrative injury clinics. The MD handles medical aspects and procedure oversight while the chiropractor and nurse practitioner team deliver hands-on treatment and functional strategies. Everyone works from the same records and goals, so care stays coordinated and thorough.
Clear Benefits Patients Notice
People who choose this combined path often report several practical improvements:
Noticeable drops in pain and swelling without relying only on medications
Better tissue repair that supports longer-lasting results
Improved joint movement and daily function
Faster return to work, sports, or normal activities when healing had stalled
Lower chance of needing more invasive procedures later
Thorough documentation that helps with insurance and legal needs after personal injury cases
Because the treatments use your own biological materials, side effects stay minimal for most people. Soreness at the injection site usually fades within a few days.
The functional medicine side of care looks at nutrition, inflammation levels, sleep, and stress. These factors influence how well tissues heal. Addressing them alongside the injections and adjustments gives the body every advantage.
What a Typical Care Journey Looks Like
Most patients start with a full evaluation that includes history, physical exam, and any needed imaging. The team identifies exactly which tissues need help and whether alignment issues are slowing progress.
Next comes a customized plan. This may include one or more regenerative injections (PRP, PFP, or MFAT), chiropractic adjustments over several weeks, guided rehabilitation exercises, and supportive therapies such as shockwave treatment when appropriate. Follow-up visits track progress and adjust the plan as tissues respond.
Many people begin to feel meaningful relief within weeks, with continued improvement over the next few months as repair progresses. The team stays involved through the entire process.
Who Benefits Most from This Approach
This type of care often helps adults dealing with:
Lingering pain after sports collisions or overuse injuries
Whiplash, back strain, or nerve irritation from car accidents
Old injuries that never fully settled
Joint or tendon problems that limit activity
It works especially well when conventional treatments have already been tried, and progress has slowed. The focus stays on restoring real function rather than temporary relief.
Moving Forward with Confidence
Healing from serious injuries takes time and the right tools. Regenerative therapies give tissues the biological signals they need. Integrative chiropractic care helps the body use those new repairs by improving movement and alignment. When both occur within a coordinated team that includes medical direction, functional medicine, and personal injury expertise, patients often regain greater comfort and capability than they expected.
If you or someone you know in the El Paso area continues to struggle after sports trauma or an auto accident, consider learning more about these combined options. A thorough evaluation at a clinic experienced in both regenerative procedures and chiropractic care can show whether this path fits your situation. Many people find it opens the door to meaningful, lasting improvement.
Regenerative Spine Care and Sciatica Relief in El Paso: How Epidural Injections, PRP, mFAT, and Shockwave Therapy Work Together
Sciatica and chronic back pain can affect almost every part of daily life. Sitting can hurt. Walking can feel limited. Sleep may be broken. Work, exercise, driving, and family time can become harder than they should be.
At El Paso Back Clinic, the goal is to look deeper than the pain signal. Pain is important, but it is often only the warning light. The real problem may involve an irritated nerve, a damaged disc, a strained ligament, a weak core, poor spinal motion, scar tissue, inflammation, or a past injury that never healed correctly.
This is why a modern spine care plan may combine chiropractic care, rehabilitation, medical oversight, functional medicine, epidural spinal injections, regenerative therapies, and shockwave therapy. Each part has a different job. Together, they may help calm nerve irritation, support tissue repair, improve movement, and help the body return to better function.
What Is Sciatica?
Sciatica is pain that travels along the sciatic nerve. This nerve starts in the lower back and travels through the buttock, hip, leg, and foot. When a spinal nerve root becomes irritated or compressed, pain can travel down the leg.
Common sciatica symptoms may include:
Low back pain
Buttock or hip pain
Burning pain down the leg
Numbness or tingling
Weakness in the leg or foot
Pain that worsens with sitting
Pain that improves when lying down or changing position
Sciatica is not always caused by the same problem. It may come from a herniated disc, disc degeneration, spinal stenosis, facet arthritis, muscle tension, pelvic imbalance, scar tissue, or inflammation. This is why a complete exam matters.
Why Chronic Back Pain Needs More Than Temporary Relief
Chronic back pain is pain that lasts longer than expected. It often continues for more than 12 weeks. By that time, the body may start to change how it moves. Muscles tighten. Joints stiffen. Nerves become more sensitive. The patient may avoid activity, which can lead to weakness and more pain.
Traditional care often focuses on short-term pain relief. That can help during a flare-up, but it may not be enough when the deeper problem is structural or inflammatory.
A more complete plan may look at:
Spinal alignment and joint motion
Disc health
Nerve irritation
Ligament and tendon stress
Muscle weakness
Core control
Inflammation
Nutrition
Sleep
Blood sugar and metabolic health
Prior auto, work, or sports injuries
This whole-person view is important because healing is not only about one painful spot. The spine is part of a larger system.
How Epidural Spinal Injections May Help Sciatica
An epidural spinal injection places medication or biologic material near an irritated spinal nerve. The goal is to reduce inflammation around the nerve root and help calm leg pain.
For a patient with strong nerve pain, this can be helpful. When pain is severe, the patient may not be able to move, stretch, exercise, or sleep well. If an epidural injection reduces the pain enough, the patient may be able to begin rehabilitation and chiropractic care more safely.
Epidural steroid injections are commonly used for spinal stenosis and nerve-related back and leg pain. However, long-term outcomes may vary. In one PCORI-supported report on lumbar spinal stenosis, epidural injections with corticosteroid plus lidocaine did not show long-term benefits over lidocaine alone for pain, function, opioid use, or surgery rates in the studied group (Friedly et al., 2019).
This does not mean epidural injections are useless. It means they should be used carefully and as part of a larger care plan.
Why Some Patients Look Beyond Repeated Steroid Injections
Steroids can reduce inflammation. That is why they are often used during painful flare-ups. But repeated steroid use may carry risks. Cortisone injections can have side effects, including cartilage damage, tendon weakening, blood sugar changes, infection risk, and bone thinning, especially when used too often or in high amounts (Mayo Clinic, 2026).
For some patients, this raises an important question:
Can we reduce pain while also supporting tissue repair?
This is where regenerative therapies may enter the conversation. Regenerative care does not simply try to hide symptoms. It aims to support the body’s natural healing response.
What Are Regenerative Spine Therapies?
Regenerative spine therapies use biologic materials, often from the patient’s own body, to support healing. These treatments may be considered for chronic spine pain, disc-related pain, ligament injury, facet joint pain, and nerve irritation when the patient is a proper candidate.
Common regenerative options include:
PRP: platelet-rich plasma
PFP: platelet-fibrin plasma or platelet-fibrin products
Platelet lysate: a platelet-derived fluid rich in growth factors
mFAT: microfragmented adipose tissue
These therapies are often called orthobiologics. “Ortho” refers to bones, joints, muscles, ligaments, and spine structures. “Biologics” refers to healing materials that come from living tissue.
The University of Iowa Health Care describes regenerative medicine as care that may use a person’s own cells, tissues, or biologic materials to support healing and repair (University of Iowa Health Care, n.d.).
PRP: Platelet-Rich Plasma for Spine and Nerve-Related Pain
PRP is made from a small sample of the patient’s blood. The blood is processed to concentrate platelets. Platelets are best known for helping blood clot, but they also carry growth factors and healing signals.
In spine care, PRP may be used to support damaged or irritated tissues, such as:
Disc-related pain areas
Facet joints
Ligaments
Tendons
Soft tissues around the spine
Research on PRP for low back pain is still growing. A narrative review on regenerative medicine for chronic low back pain described PRP and other biologic therapies as promising options, while also noting that more high-quality research is needed (Wang et al., 2023). A systematic review of PRP for low back pain found PRP was generally effective and safe for degenerative low back pain but also called for stronger studies and better treatment standards (Machado et al., 2023).
In simple terms, PRP is not a magic cure. But for selected patients, it may help support a better healing environment.
Platelet Lysate and Epidural Biologic Injections
Platelet lysate is made from platelets, but it is processed differently than PRP. The platelets are broken open, releasing growth factors into a thinner fluid. Because it is less thick than PRP, platelet lysate may be considered for nerve-related areas, including epidural use in some regenerative medicine settings.
A study of lumbar epidural platelet lysate for radicular pain reported improvements in pain and function through 24 months, with mild adverse events reported in a small percentage of patients (Centeno et al., 2017). More research is still needed, but this area is important because it examines biological support for nerve-related back and leg pain.
A 2025 meta-analysis also compared epidural PRP with steroid injections for lumbar disc disease with radiculopathy. The authors reviewed randomized controlled trials and examined pain and function outcomes over several time points (Muthu et al., 2025). This growing research shows why biologic epidural options are becoming a major topic in modern spine care.
PFP: A Natural Scaffold for Healing
PFP, or platelet-fibrin plasma, is similar to PRP but includes more fibrin activity. Fibrin is a natural protein involved in clotting and wound repair.
You can think of fibrin as a healing web. It may help hold platelets and growth factors in one area longer. This may be useful when the care plan is focused on damaged ligaments, tendons, or joint tissues.
PFP may support:
Local repair signaling
Tissue stability
Collagen remodeling
Longer contact time for healing factors
A more organized repair response
Like other regenerative options, PFP should be used after a detailed exam and proper diagnosis.
mFAT: Microfragmented Adipose Tissue
mFAT stands for microfragmented adipose tissue. Adipose tissue is fat tissue. In this treatment, a small amount of a patient’s own fat is collected, processed, and prepared for injection into a target area.
Fat tissue contains signaling cells and support structures that may help with tissue repair. mFAT is often discussed in regenerative medicine for joint, soft tissue, and orthopedic problems. It does not “regrow” a spine overnight. Instead, it may help support the local repair environment in selected cases.
For chronic spine problems, mFAT may be considered when there is deeper tissue degeneration, joint wear, or long-standing injury patterns. The key is proper patient selection, medical screening, imaging review, and follow-up care.
Shockwave Therapy: The Biological Catalyst
Shockwave therapy, also called extracorporeal shockwave therapy (ESWT), uses sound waves to stimulate tissue. It is non-surgical and does not involve medication.
Shockwave therapy may help painful tissues by creating a controlled healing signal. This process is called mechanotransduction. That means the body turns mechanical energy into a biological response.
ESWT may support healing by helping:
Increase local blood flow
Stimulate new small blood vessel formation
Improve cell activity
Reduce pain signaling
Break down scar-like tissue
Improve collagen remodeling
Support tissue repair pathways
A systematic review and meta-analysis found that ESWT improved pain and lumbar function in patients with chronic low back pain, with no serious adverse effects reported in the included studies (Liu et al., 2023). Another review described shockwave as a tool that may support tissue repair through blood vessel growth, anti-inflammatory effects, and cell signaling (Cheng & Wang, 2015).
Why Shockwave and Regenerative Injections May Work Well Together
Regenerative injections bring healing signals to damaged tissue. Shockwave therapy may help prepare the tissue to respond better.
This is why ESWT can be described as a biological catalyst. A catalyst helps a process move forward. Shockwave does not replace PRP, PFP, platelet lysate, or mFAT. It may help create a better local environment for healing.
A simple way to picture it is this:
PRP, PFP, platelet lysate, and mFAT bring healing signals.
Shockwave therapy helps wake up slow-healing tissue.
Chiropractic care improves joint motion and biomechanics.
Rehabilitation rebuilds strength, balance, and control.
Functional medicine looks for healing barriers inside the body.
When combined correctly, these tools may help the body repair itself more effectively than a single treatment alone.
The Role of Chiropractic Care at El Paso Back Clinic
Chiropractic care is often central to sciatica and back pain recovery because movement matters. If spinal joints, hips, pelvis, and soft tissues are not moving well, stress can build up around the nerves and discs.
At El Paso Back Clinic, chiropractic care may support:
Better spinal motion
Less joint stiffness
Improved posture
Better pelvic and hip mechanics
Reduced muscle guarding
Safer return to activity
Better rehab progress
Dr. Alexander Jimenez, DC, APRN, FNP-BC, CCST, CFMP, IFMCP, ATN, uses a dual-scope clinical view that connects chiropractic evaluation, injury care, functional medicine, and rehabilitation. His clinical observations often focus on how spinal structure, inflammation, metabolic health, and movement patterns work together.
This matters because many patients do not only have “a bad disc.” They may have a body system that is under stress.
Medical Oversight With Dr. Maria Guadalupe Cardenas, MD
At Injury Medical Clinic PA and within the larger integrative care model connected with El Paso Back Clinic, Dr. Maria Guadalupe Cardenas, MD, serves as Medical Director and Collaborative Physician. She is Board Certified in Internal Medicine, has over 40 years of experience as an internist, and is listed with NPI #1164426749 and Texas MD License #J2933.
This medical oversight is valuable because many spine patients have other health issues that can affect treatment safety and healing.
These may include:
Diabetes or blood sugar problems
High blood pressure
Autoimmune conditions
Medication use
Blood thinner use
Hormone changes
Infection risk
Poor sleep
Chronic inflammation
Older injuries or surgeries
A multidisciplinary clinic can help connect the dots between medical history, spine pain, nerve symptoms, and recovery goals.
Functional Medicine: Looking for Healing Barriers
Functional medicine asks a deeper question:
Why is this patient not healing well?
For chronic back pain and sciatica, the answer may lie beyond the spine. The body heals best when it has the right nutrients, blood flow, hormones, oxygen, sleep, and control of inflammation.
Functional medicine support may look at:
Vitamin D status
Blood sugar and insulin
Inflammation markers
Thyroid function
Hormone balance
Gut health
Nutrition
Weight management
Sleep quality
Stress load
This does not replace spine care. It supports spine care. A patient with poor blood sugar control, low protein intake, poor sleep, and high inflammation may heal more slowly. Improving these areas may help the patient respond better to chiropractic care, rehab, injections, and shockwave therapy.
Why Personal Injury Patients May Benefit
After a car crash, work injury, or sports injury, pain may not show up right away. Some symptoms appear hours or days later. Neck pain, back pain, headaches, sciatica, numbness, and stiffness can develop after the body’s stress response calms down.
Personal injury care needs careful documentation and a clear clinical plan. At El Paso Back Clinic, the care model may include:
Injury history
Orthopedic testing
Neurological testing
Range-of-motion findings
Imaging review when needed
Functional limits
Treatment response
Rehab progress
Referrals when needed
This matters because injury recovery is not only about pain relief. It is also about restoring function and documenting how the injury changed it.
A Step-by-Step Spine Recovery Plan
A patient-centered spine plan may include several phases.
Phase 1: Calm the Nerve
When sciatica is active, the first goal is to reduce irritation. This may include careful activity changes, decompression, gentle chiropractic care, targeted injection options, and pain-control strategies.
Phase 2: Improve the Healing Environment
Once pain is more controlled, regenerative therapies and shockwave therapy may be considered. The goal is to support tissue repair, improve circulation, and help chronic tissue move out of a stalled healing state.
Phase 3: Restore Motion
Chiropractic care, soft-tissue therapy, mobility work, and decompression may help the spine and pelvis move more freely.
Phase 4: Rebuild Strength
Rehabilitation helps the patient rebuild core strength, hip control, balance, posture, and endurance. This step helps protect the spine from future flare-ups.
Phase 5: Maintain Long-Term Function
The final goal is not just to feel better for a few days. The goal is to help the patient return to life with improved movement, strength, and awareness of how to prevent future problems.
Who May Be a Candidate?
A patient may be a candidate for this type of care if they have:
Sciatica
Chronic low back pain
Disc herniation
Disc degeneration
Annular tear
Facet arthritis
Ligament injury
Post-accident back pain
Pain that returns after basic care
Difficulty walking, sitting, or sleeping due to nerve pain
Not every patient is a candidate for every treatment. Severe weakness, loss of bowel or bladder control, fever, infection signs, cancer history, major trauma, or rapidly worsening nerve symptoms need urgent medical attention.
Final Thoughts
Sciatica and chronic back pain can be frustrating, but patients now have more options than short-term pain masking. Epidural spinal injections may help calm acute nerve irritation. Regenerative therapies such as PRP, PFP, platelet lysate, and mFAT may support repair in damaged or irritated tissues. Shockwave therapy may act as a biological catalyst by improving blood flow, stimulating cell activity, and helping chronic tissue respond.
At El Paso Back Clinic, this kind of care fits into a larger model that includes chiropractic care, medical oversight, functional medicine, personal injury care, and rehabilitation. With Dr. Alex Jimenez, DC, APRN, FNP-BC, working alongside Dr. Maria Guadalupe Cardenas, MD, Medical Director and Collaborative Physician, patients receive a team-based approach focused on structure, function, safety, and long-term healing.
The goal is simple: reduce pain, restore movement, support healing, and help patients return to the life they want.
Dashboard Knee Injury in Motor Vehicle Accidents: PCL Tears, Symptoms, and Integrative Care Options in El Paso
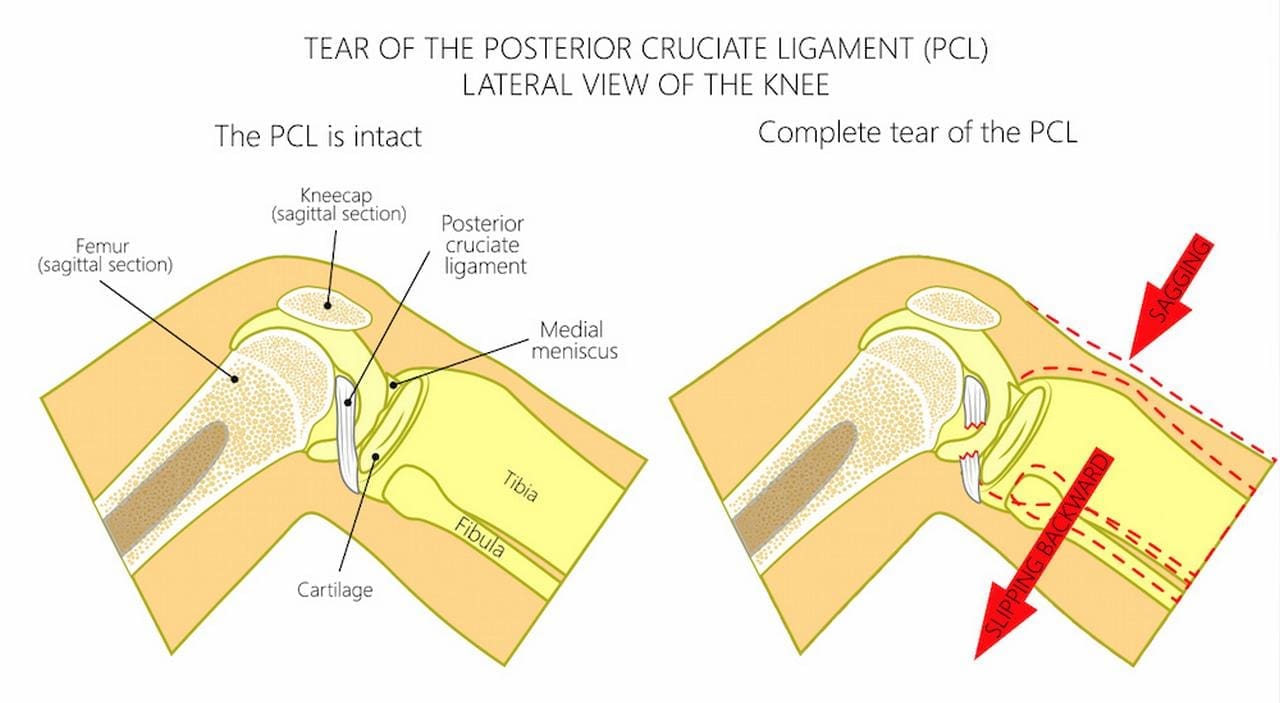
Car accidents often cause injuries that do not show up right away. One common but sometimes overlooked problem is called a dashboard knee injury. This happens when a bent knee slams into the car’s dashboard during a crash. The force violently pushes the shinbone backward. The result can include a torn posterior cruciate ligament (PCL), damage to the kneecap, and problems with the cartilage that cushions the joint.
People in El Paso and nearby areas like Horizon City who have been in motor vehicle accidents sometimes deal with ongoing knee pain, instability, or trouble walking. Understanding what happens and getting the right kind of care can make a big difference in recovery. Integrative clinics that combine medical oversight with chiropractic care and regenerative therapies offer a full approach to healing.
What Happens During a Dashboard Knee Injury
In a front-end collision, your body keeps moving forward even after the car stops. If your knee is bent, it hits the dashboard hard. This drives the top of the shinbone (tibia) backward relative to the thigh bone (femur).
The PCL is a strong band of tissue inside the knee that normally stops the shin from sliding too far back. When the dashboard impact happens, this ligament can stretch, partially tear, or completely rupture. At the same time, the direct blow can fracture the kneecap (patella) or damage the smooth cartilage on the ends of the bones. These injuries often occur together.
The damage does not always feel severe at first. Swelling and pain may appear hours or even days later. That is why some people do not realize the full extent of the injury until they try to return to normal activities.
Common Problems That Come with Dashboard Knee Injuries
Dashboard impacts frequently cause more than one issue inside the knee:
PCL tear or rupture: This is the most common ligament injury from this type of crash. It can make the knee feel loose or unstable, especially when going down stairs, pivoting, or changing direction.
Patellar fractures: The kneecap takes the direct hit and can crack or break. This causes sharp pain in the front of the knee, swelling, and difficulty straightening the leg.
Cartilage damage: The protective covering on the joint surfaces can bruise, tear, or wear down. Untreated cartilage injuries raise the risk of arthritis later in life.
These problems can lead to long-term stiffness, weakness, and difficulty with daily tasks like walking, driving, or working if they are not addressed properly.
Signs and Symptoms to Watch For
After a car accident, pay attention to these possible signs of a dashboard knee injury:
Pain in the front or back of the knee that gets worse with movement
Swelling that may appear immediately or develop over 24–72 hours
A feeling that the knee is unstable or “gives way”
Trouble bending or straightening the knee fully
Pain when walking, climbing stairs, or standing for long periods
Stiffness or locking sensations
Some people notice only mild discomfort at first and assume it will go away. Because early signs can be subtle, many dashboard knee injuries are missed without proper imaging. If you were in a crash and your knee hit the dashboard, it is wise to get checked, even if the pain seems minor.
How Doctors Diagnose These Injuries
X-rays are usually the first step. They can reveal fractures in the kneecap or other bones. However, X-rays do not show ligaments or cartilage well.
An MRI scan is the best tool for detecting PCL tears, cartilage damage, and other soft-tissue injuries. MRI gives detailed pictures that help doctors understand exactly what is torn or bruised. In some cases, doctors also perform physical tests to check knee stability.
Getting the right diagnosis early helps prevent chronic pain and long-term joint problems. Diagnostic challenges exist because swelling can be minimal at first and range of motion may still look normal, which is why imaging is so important.
Standard Treatment Options
Treatment depends on how severe the damage is:
Mild to moderate PCL tears: Doctors often recommend bracing to support the knee, rest, ice, compression, elevation (RICE), anti-inflammatory medication, and physical therapy. Therapy focuses on strengthening the quadriceps and other muscles that support the knee.
Severe tears, fractures, or major cartilage damage: Surgery may be needed to reconstruct the PCL, repair the kneecap, or clean up damaged cartilage. Recovery after surgery usually includes months of physical therapy.
Ongoing rehabilitation: No matter the path, guided exercises help restore strength, balance, and movement.
Healing takes time. Rushing back to normal activities too soon can worsen the injury or lead to new problems in the hips, back, or ankles due to altered walking patterns.
How Integrative Care Supports Better Recovery
Many people benefit from care that goes beyond just the knee. Integrative clinics combine medical doctors, nurse practitioners, chiropractors, and regenerative therapies. This team looks at the whole body and how the injury affects movement, alignment, and healing.
Medical Oversight: A physician or nurse practitioner first assesses all injuries from the accident. They review imaging, identify ligament and cartilage tears, and coordinate any needed medical steps. This oversight ensures nothing is missed, and that care stays safe and appropriate.
Regenerative Injections Clinics may offer injections that use your body’s healing cells. Platelet-rich plasma (PRP) concentrates growth factors from your blood to support torn ligaments and damaged cartilage. PFP (platelet-free plasma) and MFAT (micro-fragmented adipose tissue) are other options that can help tissue repair in areas with limited blood supply. These treatments aim to speed healing and sometimes reduce the need for surgery.
Targeted Tissue Repair: Shockwave therapy uses sound waves to break up scar tissue and stimulate new blood flow and collagen production. MLS laser therapy reduces deep inflammation and encourages cellular repair. Both are non-invasive and can be added to the recovery plan to help tissues heal faster.
Spine and Joint Mechanics: When the knee hurts, people often limp or shift weight. This creates extra stress on the spine, hips, and ankles. Chiropractic adjustments restore proper alignment in these areas. Correcting compensatory movement patterns takes pressure off the healing knee and improves overall function. Many patients notice better knee stability and less pain once the whole lower body moves correctly again.
Dr. Alex Jimenez and Dr. Maria Guadalupe Cardenas: A Collaborative Team in El Paso
At Injury Medical Clinic PA in El Paso, Texas, Dr. Alexander Jimenez, DC, APRN, FNP-BC, provides chiropractic care, functional medicine, regenerative procedures, and personal injury rehabilitation. His clinical observations emphasize that addressing the entire chain of movement—from the spine to the ankles—leads to more complete recovery after car accident injuries, including dashboard knee problems.
Working alongside him is Dr. Maria Guadalupe Cardenas, MD, a board-certified internal medicine physician with over 40 years of experience (NPI #1164426749, Texas MD License #J2933). She serves as Medical Director and Collaborative Physician. In this multidisciplinary setup, Dr. Cardenas provides medical direction, helps evaluate complex cases, and supports the team with internal medicine expertise.
This model blends chiropractic adjustments and rehabilitation (led by Dr. Jimenez) with medical oversight and coordination (led by Dr. Cardenas). Functional medicine principles—looking at inflammation, nutrition, and whole-body factors—are also part of the care. The result is a personalized plan that treats the knee injury while supporting overall healing, especially useful for patients with personal injuries and motor vehicle accidents in the El Paso area.
Local Clinics Offering This Type of Integrated Care
In Horizon City and the broader El Paso region, clinics such as Injury Medical & Chiropractic Clinic and El Paso Chiropractic & Personal Injury Group specialize in medically integrated personal injury rehabilitation. These centers bring together medical oversight, regenerative options, chiropractic adjustments, and rehabilitation in one coordinated approach. Patients receive thorough evaluations, clear explanations of their options, and ongoing support to regain function and return to daily life.
Moving Forward After a Dashboard Knee Injury
Dashboard knee injuries from car accidents can affect your mobility, work, and quality of life. The combination of a PCL tear, possible kneecap fracture, and cartilage damage needs careful attention. Early diagnosis with MRI and a treatment plan that includes medical oversight, regenerative support, tissue repair therapies, and chiropractic alignment often leads to better outcomes than treating the knee in isolation.
If you have knee pain after a motor vehicle accident—especially if your knee hit the dashboard—consider an integrative evaluation. Clinics in El Paso that combine the expertise of physicians like Dr. Maria Guadalupe Cardenas and chiropractors like Dr. Alex Jimenez can guide you through diagnosis, treatment choices, and rehabilitation. With the right team, many people regain strength, stability, and confidence in their movement.
Healing takes patience and the right support. Addressing both the specific knee damage and how the rest of your body compensates provides you the best chance of lasting recovery.
Joint Pain Relief Through Regenerative Chiropractic
Abstract
In this educational post, I, Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, guide you through a practical, evidence-based approach to shoulder and knee care using integrative chiropractic methods, functional rehabilitation, ultrasound-guided procedures, and regenerative strategies. You will learn how we identify pain generators and biomechanical contributors, why we select specific manual therapies and corrective exercises, and how we safely use ultrasound to guide injections into targeted tissues. I also introduce our multidisciplinary team, led medically by Dr. Maria Guadalupe Cardenas, MD (Board Certified in Internal Medicine) (NPI #1164426749, Texas MD License #J2933), who serves as Medical Director and Collaborative Physician at Injury Medical Clinic PA (Mission Plaza Injury Medical Clinic) in El Paso, Texas. We show how chiropractic care, internal medicine oversight, functional medicine, personal injury care, rehab, and physical therapy combine to restore function and reduce pain, while keeping hormones and medications in the background for elpasobackclinic.com’s audience. Finally, I translate complex anatomy and physiology into clear, actionable steps and provide citations with linked references so you can explore the research behind each decision.
Chiropractic And Internal Medicine Collaboration In El Paso, Texas
At Injury Medical Clinic PA (Mission Plaza Injury Medical Clinic) in El Paso, Texas, our multidisciplinary model is designed for precision diagnostics, safe care, and sustainable outcomes.
Medical direction: Dr. Maria Guadalupe Cardenas, MD (Internal Medicine), brings over 40 years of clinical experience, ensuring medical safety, bi-directional care coordination, and evidence-based protocols across complex cases.
Chiropractic integration: I lead integrative chiropractic care, combining spinal biomechanics, regional joint assessment, soft-tissue methods, and functional rehabilitation targeted to the patient’s presentation.
Functional medicine lens: We prioritize nutrition, sleep, stress physiology, and metabolic health as supportive pillars for tissue healing, while minimizing reliance on hormones or medications unless medically indicated.
Physical therapy emphasis: Coordinated mobility, stability, motor control, and return-to-function plans are sequenced with chiropractic adjustments and soft-tissue care, including sports-specific and work-injury progressions.
Personal injury workflows: For PI cases, we document thoroughly, use validated outcome measures, and align care with imaging, guided procedures, and gradual load progressions to restore confidence and capacity.
Why This Integrative Model Matters
Safety first: Internal medicine oversight reduces procedural risk and guides comorbidity management.
Precision: Ultrasound-guided interventions and biomechanical assessments target the right tissue at the right dose.
Durability: Chiropractic care, physical therapy, and functional medicine together produce longer-lasting outcomes by addressing root causes.
Patient-centered: We build stepwise care pathways, educate patients, and align expectations to reduce fear and improve adherence.
Shoulder Pain: Anatomy, Biomechanics, And Why It Hurts
The shoulder is a dynamic, multi-planar joint system in which the glenohumeral joint, acromioclavicular (AC) joint, scapulothoracic articulation, and sternoclavicular joint must synchronize to ensure smooth function. The rotator cuff—supraspinatus, infraspinatus, teres minor, and subscapularis—stabilizes the humeral head to prevent excessive superior or anterior translation during elevation.
Key physiology driving pain:
Tendinopathy: Repetitive load and poor scapular control foster collagen disorganization, neovascularization, and nociceptive sensitization within cuff tendons, especially the supraspinatus footprint on the greater tuberosity.
Subacromial space mechanics: Limited thoracic extension or scapular upward rotation narrows the subacromial space, increasing bursal and tendinous stress.
AC joint degeneration: Microinstability and load transfer through the clavicle result in capsular irritation, osteophytes, and localized pain with cross-body movements.
Biceps-labral interface: The long head of the biceps traverses the bicipital groove and contributes to anterior shoulder pain when overloaded or in SLAP variants.
Neurovascular proximity: The neurovascular bundle in the anterior shoulder region requires meticulous mapping during procedures to avoid iatrogenic injury.
What I Look For During A Real Patient Encounter
Drawing from my clinical experience:
Visual and palpatory cues: I watch for asymmetry, protective guarding, and painful arcs. Palpation maps tenderness over the supraspinatus footprint, AC joint, subscapularis, and bicipital groove.
Functional patterns: I analyze bird-dog, superman, and scapular setting drills to identify deficits in anti-extension control and rotator cuff endurance. These tests help me see how trunk stability informs shoulder mechanics.
Ultrasound landmarks: I trace the humeral head, articular cartilage, supraspinatus footprint, subacromial bursa, AC joint, and biceps tendon sheath, maintaining a safe distance from neurovascular structures.
Load tolerance: I progress from low-load tasks to higher-load regions (e.g., triceps or deep cuff work), carefully managing patient expectations and discomfort.
Integrative Chiropractic Approach To Shoulder Care
Our shoulder pathway prioritizes chiropractic and physical therapy methods:
Thoracic mobility and rib mechanics
Why: Thoracic extension and rib mobility enable scapular upward rotation and posterior tilt, reducing impingement risk.
Methods: Thoracic spine manipulation and mobilization to improve segmental motion; breathing retraining for costovertebral rhythm.
Evidence: Manual therapy to the cervical-thoracic junction can reduce shoulder pain and improve function through regional interdependence (Domenech-Garcia et al., 2011).
Scapular motor control
Why: Proper serratus anterior and lower trapezius activation improves humeral head centering, decreasing superior migration under load.
Methods: Wall slides with lift-off, prone Y/T/W, serratus punches, anti-shrug carries to re-pattern scapular mechanics.
Evidence: Scapular-focused intervention enhances pain and function in shoulder disorders (Kibler et al., 2013).
Rotator cuff capacity building
Why: The cuff stabilizes micro-movements. Progressive isometrics and eccentrics remodel tendon integrity.
Methods: Isometric external rotation, eccentric abduction, side-lying ER, full-can holds; later closed-chain perturbations.
Evidence: Eccentric loading promotes tendon remodeling and reduces pain in tendinopathies (Rio et al., 2015).
Soft-tissue and fascia
Why: Myofascial restrictions elevate local shear and neural input.
Methods: Instrument-assisted soft-tissue mobilization, percussion, cupping, and nerve glides where appropriate.
Evidence: Soft-tissue approaches can modulate pain, improve ROM, and support exercise tolerance (Cheatham et al., 2015).
Patient education and pacing
Why: Expectation management reduces threat perception and enhances adherence.
Methods: Transparent planning, explaining why each step is chosen and how measurable progress is tracked.
Ultrasound-Guided Shoulder Procedures: What We Do And Why
When indicated, we use ultrasound to guide precise injections. While this post emphasizes chiropractic and physical therapy, understanding our interventional choices clarifies our iterative care model.
Subacromial bursa, supraspinatus footprint, and AC joint
Why: Pain may originate from bursitis, partial-thickness supraspinatus lesions, or AC joint capsular irritation. Ultrasound guidance ensures in-plane or out-of-plane needle control, keeping the needle away from neurovascular structures.
Technique: Identify bright cortical bone under the footprint; visualize bursal fluid and capsule integrity. Use small aliquots and reassess spread, avoiding intratendinous trauma unless intentionally performing a tendon fenestration or PRP in tendinopathic zones.
Evidence: Ultrasound-guided shoulder injections improve accuracy compared with landmark techniques and can more precisely target pathologic pain generators (Sibbitt et al., 2011).
Biceps tendon sheath
Why: Anterior shoulder pain often involves the long head of biceps. Sheath injection—distinct from intratendinous injection—reduces irritability and allows rehab to progress.
Technique: Map the groove, maintain longitudinal needle trajectory, and confirm spread along the sheath without tendon violation.
AC joint microvolume injection
Why: Small-volume injections can modulate capsular irritability. Cross-body adduction reproduction of pain is a clinical cue.
Technique: Orient to the joint cleft, avoid over-distention, and recheck cross-body ROM post-procedure.
Our Procedure Safety And Team Coordination
Pre-procedure planning: We plan labs, imaging, and rehab scheduling in advance. My nurse and lab tech process any biologics as needed, while I maintain room-side focus on mapping and safety.
Minimal staff burden: Our care flow allows other team members to handle follow-ups, therapy sessions, and patient education while I perform the procedure efficiently.
Internal medicine oversight: Dr. Cardenas reviews risk factors, comorbidities, contraindications, and post-procedural monitoring when warranted.
Rehabilitation Sequencing After Shoulder Interventions
We deliberately move from low-threat to higher-load tasks:
Start with what hurts least: Early sessions prioritize thoracic mobility, scapular setting, and isometric cuff work at angles that do not provoke pain.
Gradual load introduction: As irritability recedes, we add eccentrics, closed-chain stabilization, and overhead progressions using tempo, isometric holds, and pause reps.
Return-to-sport or work tasks: We simulate reach, lift, carry, and press patterns relevant to the patient’s goals, using pain-guided progression and rate of perceived exertion to keep tissues within safe adaptive ranges.
Knee Care: Integrative Chiropractic And Physical Therapy Emphasis
The knee often presents with MCL strain, medial meniscal involvement, and synovial irritability—themes echoed in the transcript. Our approach blends chiropractic, PT, and when appropriate, ultrasound guidance.
Knee Biomechanics And Physiology
Load transmission: The knee depends on hip control and ankle mobility for shock absorption and alignment. Poor hip abduction and external rotation strength elevate medial compartment stress.
Meniscal physiology: Menisci distribute load and contribute to joint stability. Intra-meniscal degeneration and synovial inflammation can perpetuate pain and mechanical symptoms.
MCL healing: The MCL typically responds to graded load and frontal-plane stability training. Excess valgus strain irritates healing tissue.
Chiropractic And PT Integration For The Knee
Pelvic and lumbar alignment
Why: Pelvic tilt and lumbar rotation alter femoral tracking and tibial alignment under dynamic load.
Methods: Lumbopelvic adjustments, hip mobilizations, and gluteal activation to normalize kinetic chain input.
Motor control and strength
Why: Stable knees require hip abductors, external rotators, hamstrings, and quadriceps working in harmony.
Methods: Side-steps with bands, split-squat isometrics, Spanish squats, hamstring bridges, and tempo squats to train tolerance and tissue remodeling.
Tendon and fascia support
Why: Tendinopathic tissues benefit from eccentric and isometric loading; fascia responds to improved glide and hydration.
Methods: Patellar tendon isometrics, eccentric decline squats as tolerated, and soft-tissue mobilization to quadriceps and adductors.
Progressive return to function
Why: Sequenced progressions reduce flare-ups and build confidence.
Methods: Low-impact conditioning, step-down drills, landings, and multi-directional gait under supervision.
Ultrasound-Guided Knee Procedures When Indicated
Intra-articular injections
Why: Targeted delivery to the joint space supports modulation of synovial irritation.
Technique: Short-axis or long-axis guidance to visualize needle entry and avoid neurovascular structures.
MCL and medial meniscus region
Why: Pain generators can localize to the MCL or posteromedial meniscus. High-precision mapping reduces the risk of non-target injections.
Technique: In-plane approach along the MCL with careful hydrodissection when necessary; avoid intrameniscal violation unless using a specialist technique aligned with current evidence.
Clinical Observations From Dr. Alex Jimenez
From practice patterns noted across my work at elpasobackclinic.com and shared on my LinkedIn profile, several themes consistently emerge:
Patients thrive when care is sequenced, explained, and measured. Clear progress markers—ROM, strength, pain thresholds—reduce anxiety and improve outcomes.
The shoulder and knee respond best when the spine and hip are addressed concurrently. Regional interdependence is not academic—it is observable daily in the clinic.
Education and expectation management are as therapeutic as manual care. When patients understand why a technique is used, adherence and results improve.
Small-aliquot injections with ultrasound guidance allow real-time adjustments based on tissue spread and patient feedback, enhancing comfort and safety.
We emphasize movement literacy, teaching patients how to maintain neutral positions, breathe, and move through ranges of motion without provoking symptoms.
How Our Team Coordinates Care
Intake and triage: Medical review by Dr. Cardenas for complex histories; chiropractic exam and movement analysis by me; imaging decisions based on need.
Plan creation: A written plan outlines manual therapy, exercise progression, imaging, procedural options, and follow-up cadence.
Execution: Therapy staff handles laser, shockwave, and exercise coaching; I manage manual and chiropractic care, as well as any ultrasound-guided procedures, as appropriate.
Reassessment: We use validated outcome scales, ROM, strength testing, and return-to-function checkpoints to iterate the plan.
Communication: Patients receive clear instructions on post-session expectations and a simple home exercise sequence.
Why We Prioritize Chiropractic and Physical Therapy for elpasobackclinic.com
For our web audience and community, practical hands-on care, exercise therapy, and movement education are the cornerstones of recovery. While medications and hormones are part of comprehensive medical practice, we keep them in the background here, emphasizing:
The power of adjustments to restore joint motion and relieve nociception.
The value of targeted strengthening and motor control to protect tissues.
The role of patient-guided progression to boost independence and long-term resilience.
Safety, Dosing, And Patient Comfort
Dosing matters: Whether we are adjusting, mobilizing, loading a tendon, or injecting, we dose according to irritability, stage of healing, and patient goals.
Comfort strategies: We start with low-pain tasks, use paced breathing, and deploy brief micro-breaks to maintain composure in procedures.
Monitoring: Signs of over-irritation (escalation of night pain, heat, swelling) prompt plan adjustments or a medical review.
Putting It All Together: An Easy-To-Follow Care Journey
Step 1: Assessment
Detailed history, movement analysis, palpation, and ultrasound mapping when indicated.
Step 2: Early Care
Thoracic and cervical-thoracic mobilization, scapular setting, isometric cuff work; knee lumbopelvic alignment, hip strength foundations.
Step 3: Load And Control
Eccentrics, closed-chain drills, perturbation training, and gait re-education.
Step 4: Targeted Procedures If Needed
Ultrasound-guided bursa, AC joint, or intra-articular knee injections based on clear indications, with medical oversight.
Step 5: Return To Function
Task-specific progressions, confidence building, and preventive strategies.
Evidence-Based References That Inform Our Practice
We continually incorporate high-quality research into decisions:
Ultrasound guidance improves injection accuracy and patient outcomes in shoulder pathology (Sibbitt et al., 2011).
Scapular-focused programs and regional interdependence considerations enhance the effectiveness of shoulder rehabilitation (Kibler et al., 2013).
Eccentric and isometric loading strategies reduce tendinopathy pain and remodel tissue (Rio et al., 2015).
Myofascial techniques can improve pain and functional outcomes, supporting active rehabilitation (Cheatham et al., 2015).
Practical Takeaways For Patients
Movement is medicine: Consistency beats intensity early on.
Pain-guided progression: Minor discomfort is normal; escalating night pain or swelling means you should check in with us.
Whole-system support: Sleep, nutrition, and stress management help tissues heal and adapt.
Team-based care: Chiropractic, physical therapy, and medical oversight ensure your pathway is safe, precise, and personalized.
How To Get Help
If you are in El Paso or nearby and dealing with shoulder or knee pain, our team can create a clear, step-by-step plan designed for your goals. We will explain why we select each technique, how it fits your stage of healing, and how we measure progress so you can return to life with confidence.
References
Domenech-Garcia, V., Palsson, T. S., Boudreau, S. A., & Arendt-Nielsen, L. (2011). Upper cervical and upper thoracic manipulation in patients with shoulder pain: A randomized clinical trial. Journal of Orthopaedic & Sports Physical Therapy. https://www.jospt.org/doi/10.2519/jospt.2011.3579
Kibler, W. B., Sciascia, A., & Wilkes, T. (2013). Scapular dyskinesis and its relation to shoulder pain. Journal of the American Academy of Orthopaedic Surgeons. https://journals.lww.com/jaaos/Abstract/2013/06000/Scapular_Dyskinesis_and_Its_Relation_to_Shoulder.3.aspx
Rio, E., Kidgell, D., Purdam, C., Gaida, J., Moseley, L. G., & Cook, J. (2015). Isometric exercise for pain relief in tendinopathy: Mechanisms and implications. British Journal of Sports Medicine. https://bjsm.bmj.com/content/49/10/645
Sibbitt, W. L., Band, P. A., Kettwich, S. C., et al. (2011). Does ultrasound-guided injection improve outcomes for shoulder pain? A randomized controlled trial. Journal of Rheumatology. https://www.jrheum.org/content/38/9/1917
Cheatham, S. W., Kolber, M. J., & Cain, M. (2015). Instrument-assisted soft tissue mobilization: A systematic review. Journal of the Canadian Chiropractic Association. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4566596/
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine