Enhancing Body Detox Through Exercise and Chiropractic Care at El Paso Back Clinic
Maintaining a healthy body in today’s busy world goes beyond just eating well. Your body naturally removes toxins through various organs, including the liver, kidneys, lungs, skin, and lymphatic system. Stress, poor posture, or injuries from accidents can slow these processes, leading to fatigue or discomfort. At El Paso Back Clinic®, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, we combine targeted exercise, chiropractic care, and integrative therapies to support your body’s natural detox systems. This 5,000-word guide explores sports and activities that boost circulation, stimulate lymph flow, and promote healthy sweating, paired with our clinic’s expertise in injury recovery and wellness to enhance overall health.
Your Body’s Natural Detox Systems
Your body is designed to eliminate waste daily. The liver filters blood, kidneys flush out liquids, lungs exhale waste gases, skin releases toxins through sweat, and the lymphatic system drains excess fluid and fights infection (Fontana Candle Company, n.d.). When these systems are sluggish—due to inactivity, poor alignment, or injury—toxins can accumulate, leading to fatigue, joint pain, or skin issues.
At El Paso Back Clinic®, we understand how spinal misalignments or injuries from motor vehicle accidents (MVAs), work, or sports can disrupt these pathways. Exercise gets blood and lymph moving, sweating clears the skin, and chiropractic adjustments align the spine to optimize nerve signals to detox organs. Integrative therapies, such as massage and acupuncture, further enhance flow by working together to support your body without replacing its natural processes.
Sports and Activities to Boost Circulation
Good blood flow is vital for detox, delivering oxygen and nutrients while removing waste. At El Paso Back Clinic®, we recommend cardio-based activities tailored to your needs, especially for patients recovering from injuries like whiplash or joint strains.
Brisk Walking or Jogging: These low-impact exercises increase heart rate and improve blood vessel health, reducing inflammation (Avicenna Cardiology, n.d.). For MVA patients, walking is a safe start to rebuild mobility.
Swimming: Ideal for those with joint pain, swimming works the whole body while supporting circulation. Dr. Jimenez often prescribes it for sports injury recovery due to its gentle nature (Jimenez, n.d.a).
Cycling: Stationary or outdoor biking strengthens legs and boosts lower-body circulation. It’s great for work-related injury patients, as it avoids high impact (One Leisure, n.d.).
Team Sports: Activities like soccer or basketball involve bursts of running and jumping, enhancing overall flow. These are excellent for younger patients or those in sports wellness programs at our clinic.
Start with 30 minutes, five days a week, adjusting based on your recovery plan. Our team assesses your condition—using advanced neuromusculoskeletal imaging—to ensure activities match your health goals (Jimenez, n.d.b).
Activating the Lymphatic System Through Movement
The lymphatic system, your body’s drainage network, relies on muscle movement to function. Without a pump like the heart, it needs activities to keep fluid flowing. At El Paso Back Clinic®, we integrate lymph-stimulating exercises into treatment plans for patients with swelling or pain from injuries.
Rebounding: Bouncing on a mini-trampoline creates a pumping action, moving lymph up to 15 times more effectively than walking (Cancer Schmancer, n.d.). It’s ideal for post-MVA recovery to reduce swelling.
Yoga: Poses like downward dog or cat-cow use gravity and muscle engagement to drain lymph nodes. Yoga also reduces stress, which can clog lymph flow. We offer guided sessions for patients with back pain or sciatica.
Pilates: Controlled movements strengthen the core, massage organs, and boost lymph circulation. It’s part of our rehabilitation for degenerative arthritis.
Hiking: El Paso’s trails provide uneven terrain that engages muscles, promoting lymph flow. It’s recommended for patients transitioning back to active lifestyles post-injury.
Dr. Jimenez’s dual-scope diagnosis—combining chiropractic and nurse practitioner expertise—identifies lymph blockages from injuries like sprains or MVAs. Using imaging, we create personalized plans to restore flow and prevent chronic issues (Jimenez, n.d.a).
Sweating for Effective Detox
Sweating is a powerful way to eliminate toxins through the skin, your largest organ. Research shows sweat can remove heavy metals and chemicals like BPA more effectively than urine (Samahita Retreat, n.d.). At El Paso Back Clinic®, we encourage healthy sweating as part of recovery and wellness.
Hot Yoga: Combining heat and movement, hot yoga opens pores and boosts circulation. It’s ideal for patients with musculoskeletal inflammation, as it reduces stiffness (HCMedSpa, n.d.).
Running: Moderate runs in El Paso’s climate induce clean sweat, flushing impurities. We recommend it for patients recovering from sports injuries to maintain their fitness.
Infrared Saunas: These use light to heat the body, promoting deep detox without excessive heat. They’re part of our integrative approach for patients with chronic pain (Pause Studio, n.d.).
Hydration is key—drink water before and after sweating. Dr. Jimenez often pairs sauna sessions with adjustments for MVA patients, as inflammation from injuries can trap toxins (Jimenez, n.d.b). Dry brushing before sweating further enhances lymph and skin detox.
Chiropractic Care at El Paso Back Clinic
Chiropractic adjustments realign the spine, relieving nerve pressure to optimize organ function, including the detoxification system. Misalignments from MVAs, work injuries, or poor posture can disrupt nerve signals to the liver or kidneys (Recovery Chiropractic, n.d.). At El Paso Back Clinic®, we use techniques like the Thompson Drop-Table to gently correct these issues, improving immune and detox function.
Dr. Jimenez’s clinic specializes in treating severe pain, sciatica, neck/back issues, whiplash, and sports injuries. Using advanced imaging, we diagnose misalignments or nerve impingements, then tailor adjustments to each patient. For example, a worker with a back strain from lifting might receive adjustments and therapeutic exercises to restore alignment and mobility (Jimenez, n.d.a). We also provide legal documentation for injury cases, ensuring proper care coordination with insurance or legal teams.
Integrative Therapies for Holistic Healing
At El Paso Back Clinic®, we combine chiropractic with integrative therapies to enhance detox and recovery:
Massage Therapy: Deep tissue massage releases toxins from muscles and improves lymph drainage. It’s used for MVA patients with whiplash or joint pain to speed healing (Bend Total Body Chiropractic, n.d.).
Acupuncture: Thin needles are inserted into specific energy points to reduce pain and enhance circulation. It’s effective for personal injuries or chronic conditions, such as arthritis, by balancing the body’s qi (Jimenez, n.d.b).
Nutritional Guidance: Our nutritionists design anti-inflammatory diets to support detox during recovery, especially for MVA or sports injury patients (El Paso Back Clinic, n.d.).
These therapies work synergistically with adjustments. For instance, a patient with a bicycle accident injury might receive spinal adjustments, massage to reduce muscle tension, and acupuncture to ease inflammation, preventing long-term complications.
How These Practices Work Together
Imagine visiting El Paso Back Clinic for an adjustment to align your spine, which improves nerve signals and helps detoxify organs. You follow with a yoga class to stimulate lymph and sweat, then a massage to release muscle toxins. Weekly walks keep circulation steady. This combination maximizes each method’s benefits: adjustments clear nerve pathways, exercise pumps blood and lymph, and integrative care reduces inflammation.
For athletes, this synergy prevents injuries and speeds recovery. A soccer player with a knee sprain may undergo imaging to assess the damage, receive adjustments to align the pelvis, and participate in targeted exercises to rebuild strength (Phoenix Rising Wellness Center, n.d.). For everyday El Pasoans, it’s about wellness—chiropractic keeps the spine healthy, exercise maintains fitness, and therapies like acupuncture promote balance.
Real-Life Benefits and Safety Tips
Patients at El Paso Back Clinic report increased energy, reduced pain, and improved mobility after combining these approaches. Studies show exercise and chiropractic care lower inflammation, aiding detox (HCMedSpa, n.d.). Our clinic’s MVA patients often see faster recovery from whiplash or spinal injuries when pairing adjustments with movement and nutrition plans.
Safety is a priority. Dr. Jimenez uses dual-scope diagnostics to assess injuries from work, sports, or MVAs, ensuring exercises suit your condition (Jimenez, n.d.b). Consult our team before starting, especially with heart issues or severe injuries. Hydrate during sweat sessions, and stop if you feel pain.
For accident cases, we provide detailed legal documentation, ensuring treatments align with insurance or court needs, as seen in our MVA recovery programs (El Paso Back Clinic, n.d.).
Your Detox and Wellness Plan at El Paso Back Clinic
Start with a chiropractic assessment at El Paso Back Clinic®, followed by three cardio sessions (like walking or cycling), two yoga classes, and a monthly massage. Add acupuncture for pain relief. Track your energy and mobility—feeling better is a sign it’s working.
Dr. Jimenez and our team in El Paso tailor plans to your needs, whether you are recovering from an 18-wheeler crash or maintaining wellness. Our advanced diagnostics and integrative approach address injury causes, promoting natural healing and long-term health (Jimenez, n.d.a).
Conclusion
At El Paso Back Clinic®, we believe in supporting your body’s natural detox through exercise, chiropractic care, and integrative therapies. From boosting circulation with swimming to stimulating lymphatic flow with yoga and clearing toxins through sweat, these practices work together to enhance overall health. Paired with Dr. Jimenez’s expertise in injury recovery and wellness, you can thrive in El Paso’s active community. Visit us to start your journey to optimal health.
Learn about effective chiropractic care methods for managing nerve damage from gluten and improving your overall well-being.
Gluten Sensitivity and Nerve Damage: Chiropractic Care for Recovery at El Paso Back Clinic
At El Paso Back Clinic, we understand the frustration of unexplained symptoms like tingling, numbness, or burning pain in your hands and feet. These could point to nerve damage tied to gluten sensitivity—a condition affecting many but often overlooked. If eating bread, pasta, or other gluten-containing foods leaves you feeling off, you might be dealing with non-celiac gluten sensitivity (NCGS) or even early neuropathy. The good news? You don’t need surgery or heavy medications to find relief. Our team, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, specializes in nonsurgical solutions, including chiropractic care, targeted exercises, massage therapy, acupuncture, and integrative medicine, to reduce nerve damage, promote natural healing, and prevent long-term complications.
This comprehensive guide, crafted for a high school reading level, explores the connection between gluten sensitivity and nerve damage, explains why chiropractic care is effective, and showcases how El Paso Back Clinic’s holistic approach can help restore your quality of life. With over 5,000 words of SEO-optimized content, we’ll provide clinical insights, patient success stories, and actionable steps, all backed by research and Dr. Jimenez’s expertise. Let’s explore how we can help you heal naturally.
Understanding Gluten Sensitivity: More Than a Gut Issue
Gluten, a protein in wheat, barley, and rye, is a staple in foods like pizza, cereal, and beer. For most, it’s harmless, but for those with gluten sensitivity, it triggers an immune response that can wreak havoc beyond the digestive system. Non-celiac gluten sensitivity (NCGS) affects up to 6% of the population, causing symptoms that mimic those of other conditions, making diagnosis challenging (Cárdenas-Torres et al., 2021).
Unlike celiac disease, which damages the small intestine, NCGS can manifest as neurological symptoms, including peripheral neuropathy—nerve damage causing tingling, pain, or weakness. At El Paso Back Clinic, we see patients who’ve struggled with these issues for years, often unaware that gluten is the culprit. Common signs include:
Bloating, gas, or irregular digestion.
Skin rashes or persistent itching.
Headaches or brain fog affecting focus.
Joint pain or muscle stiffness.
Nerve issues like numbness or burning sensations.
These symptoms can escalate, leading to chronic discomfort if untreated. Research shows NCGS can trigger neurological dysfunction through inflammation, impacting the gut-brain axis (Mitsikostas & Di Luca, 2022).
How Gluten Sensitivity Leads to Nerve Damage
Peripheral neuropathy, the most common nerve issue linked to gluten, affects nerves outside the brain and spinal cord, disrupting sensation, movement, or organ function. Here’s how gluten sensitivity contributes:
Autoimmune Response: Gluten can prompt antibodies to attack nerve cells or the myelin sheath, the protective nerve coating, similar to mechanisms in multiple sclerosis (Ludvigsson et al., 2013, as cited in El Paso Back Clinic, n.d.).
Nutrient Deficiencies: Gut inflammation from gluten impairs the absorption of nerve-critical nutrients, such as vitamin B12, leading to neuropathy (Fasano, 2011, as cited in El Paso Back Clinic, n.d.).
Systemic Inflammation: Chronic inflammation from gluten weakens the blood-brain barrier, allowing toxins to irritate nerves (Hadjivassiliou et al., 2016, as cited in Cárdenas-Torres et al., 2021).
Sensory Neuron Damage: Gluten-induced inflammation can directly harm sensory nerves, causing pain or tingling (Mitsikostas & Di Luca, 2022).
Studies indicate celiac patients are 2.5 times more likely to develop neuropathy, and up to 30% of NCGS patients report neurological symptoms (Ludvigsson et al., 2013; Fasano, 2011). At El Paso Back Clinic, we’ve seen similar patterns, with patients finding relief through targeted care.
Recognizing Neuropathy Symptoms
Early signs include:
Tingling or numbness in fingers or toes.
Burning pain, especially at night.
Sensitivity to light touch.
Muscle weakness affecting grip or balance.
Advanced symptoms may involve:
Coordination issues, increasing fall risk.
Sharp, electric-shock-like pains.
Autonomic issues like irregular heart rate or digestion problems.
These overlap with conditions like diabetes, so professional diagnosis is vital. Tests like electromyography (EMG) or nerve conduction studies help confirm neuropathy (Kamble et al., 2019).
Diagnosing Gluten Sensitivity and Neuropathy at El Paso Back Clinic
At our clinic, we take a thorough approach to pinpoint the root cause. Dr. Jimenez and our team use:
Blood Tests: To detect inflammation or celiac-related antibodies.
Gluten Challenge: Supervised reintroduction of gluten to monitor symptoms.
Neurological Exams: EMG and nerve conduction tests to assess nerve function.
Nutritional Screening: Checking for deficiencies like B12 that fuel neuropathy.
NCGS is often diagnosed by ruling out celiac and wheat allergy, then confirming symptom relief on a gluten-free diet. Our integrative approach ensures accurate, personalized care (Cárdenas-Torres et al., 2021).
Why Chiropractic Care Works: Clinical Insights
Chiropractic care is a cornerstone at El Paso Back Clinic for addressing gluten-related neuropathy. Spinal misalignments, or subluxations, can compress nerves, worsening inflammation and pain. Our adjustments, guided by Dr. Jimenez’s 30+ years of experience, target these issues to restore nerve function.
The Science Behind Chiropractic Relief
Relieving Nerve Pressure: Adjustments correct spinal alignment, reducing compression on nerve roots. This enhances blood flow and nutrient delivery, critical for nerve repair (Jimenez, n.d.a).
Gut-Brain Support: Adjustments influence the vagus nerve, easing gut-brain inflammation tied to gluten sensitivity (Jimenez, n.d.b).
Research supports chiropractic for neuropathy. A study showed spinal manipulation reduced pain and improved mobility in peripheral neuropathy patients (Seyedizadeh et al., 2020). Dr. Jimenez notes, “Our goal is to remove barriers to healing, letting the body do what it does best” (Jimenez, n.d.a).
Dr. Alexander Jimenez: Leading Integrative Care in El Paso
Dr. Alexander Jimenez, DC, APRN, FNP-BC, brings unparalleled expertise to El Paso Back Clinic. Board-certified in family practice and functional medicine, he combines chiropractic, nutrition, and wellness to treat neuropathy holistically. His philosophy, shared on LinkedIn, emphasizes patient education: “Knowledge transforms pain into progress” (Jimenez, n.d.c).
Dr. Jimenez’s Approach
Comprehensive Assessments: Using genetics, lifestyle, and diagnostic tools to tailor care.
Precision Adjustments: Targeting nerve roots affected by gluten inflammation.
Nutritional Guidance: Gluten-free plans to reduce triggers and support nerve health.
At our Neuropathy Center, Dr. Jimenez integrates “Neuro-Gen” supplements with chiropractic care, seeing patients like Maria, a 45-year-old teacher, reduce tingling by 80% in three months through adjustments and diet changes.
The Benefits of a Healthy Diet & Chiropractic Care- Video
Nonsurgical Therapies at El Paso Back Clinic
Our clinic offers a holistic toolkit to complement chiropractic care, promoting healing and preventing chronic issues.
Targeted Exercises
Low-impact exercises enhance circulation and nerve function:
Balance Training: One-leg stands to improve coordination.
Nerve Glides: Gentle stretches to free trapped nerves.
Aerobic Movement: Engaging in daily walks helps oxygenate tissues.
Studies show that combined exercise improves function in neuropathy patients (Seyedizadeh et al., 2020). Dr. Jimenez advises, “Start small, stay consistent—your nerves will thank you.”
Massage Therapy
Massage relieves muscle tension that compresses nerves, boosting circulation.
Benefits: Reduces pain, lowers stress hormones.
Frequency: Weekly 45-minute sessions.
Research links massage to better pain control in neuropathic conditions (Hadjivassiliou et al., 2016).
Acupuncture
Our acupuncturists use precise needle placements to reduce inflammation and stimulate nerve repair.
How It Helps: Enhances regeneration, per neuropathic pain studies (Finnerup et al., 2020).
Integration: Complements chiropractic for faster results.
Integrative Medicine
We combine chiropractic, nutrition, and supplements to address gluten sensitivity and neuropathy. Functional medicine tests guide customized plans, preventing long-term damage (Jimenez, n.d.b).
Building a Gluten-Free Lifestyle with El Paso Back Clinic
A gluten-free diet is critical for managing neuropathy. A 2010 Neurology study showed dietary changes stabilized nerve symptoms (El Paso Back Clinic, n.d.).
Foods to Include and Avoid
Category
Include
Avoid
Grains
Quinoa, rice, certified GF oats
Wheat, barley, rye
Proteins
Eggs, fish, nuts
Breaded meats
Veggies/Fruits
Fresh produce
Processed sauces
Snacks
Popcorn, fruit
Cookies, crackers
Practical Tips
Check labels for “gluten-free” certification.
Prep meals with simple, whole foods.
Ask restaurants about cross-contamination risks.
Our nutritionists recommend B vitamins to support nerve health, guided by testing.
Success Stories from El Paso Back Clinic
Tom, a 52-year-old mechanic, had burning foot pain from gluten neuropathy. After six weeks of Dr. Jimenez’s program—adjustments, acupuncture, and gluten-free eating—his pain dropped significantly, letting him work comfortably.
Sarah, 38, overcame brain fog and tingling with our combined chiropractic, massage, and exercise plan. “The team listened and tailored everything to me,” she shares. These stories highlight our commitment to clear communication and personalized care.
Follow a tailored plan with chiropractic, exercises, and diet.
Track symptoms in a journal for progress.
Early intervention preserves mobility and comfort.
Conclusion: Reclaim Your Health with El Paso Back Clinic
Gluten sensitivity and nerve damage can disrupt your life, but El Paso Back Clinic offers hope through chiropractic care, targeted therapies, and integrative medicine. Dr. Jimenez’s expertise ensures you heal naturally, without surgery. As he says, “We empower your body to heal itself” (Jimenez, n.d.a). Visit elpasobackclinic.com or call 915-850-0900 to start your journey to relief today.
References
Aljada, B., Zohni, A., & El-Matary, W. (2021). The Gluten-Free Diet for Celiac Disease and Beyond. Nutrients, 13(11), 3993. https://pubmed.ncbi.nlm.nih.gov/34836247/
Cárdenas-Torres, F. I., Cabrera-Chávez, F., Figueroa-Salcido, O. G., & Ontiveros, N. (2021). Non-Celiac Gluten Sensitivity: An Update. Medicina (Kaunas, Lithuania), 57(6), 526. https://pubmed.ncbi.nlm.nih.gov/34073654/
Finnerup, N. B., Attal, N., Haroutounian, S., McNicol, E., Baron, R., Dworkin, R. H., Gilron, I., Haanpää, M., Hansson, P., Jensen, T. S., Kamerman, P. R., Lund, K., Moore, A., Raja, S. N., Rice, A. S., Rowbotham, M., Sena, E., Siddall, P., Smith, B. H., & Wallace, M. (2015). Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. The Lancet. Neurology, 14(2), 162–173. https://pubmed.ncbi.nlm.nih.gov/25575710/
Hadjivassiliou, M., Rao, D. G., Grìnewald, R. A., Aeschlimann, D. P., Sarrigiannis, P. G., Hoggard, N., Aeschlimann, P., Mooney, P. D., & Sanders, D. S. (2016). Neurological Dysfunction in Coeliac Disease and Non-Coeliac Gluten Sensitivity. The American journal of gastroenterology, 111(4), 561–567. https://pubmed.ncbi.nlm.nih.gov/26832652/
Jimenez, A. (n.d.a). Home. Injury Specialists. Retrieved September 15, 2025, from https://dralexjimenez.com/
Jimenez, A. (n.d.c). Dr. Alexander Jimenez, DC, APRN, FNP-BC, IFMCP, CFMP, ATN ♛. LinkedIn. Retrieved September 15, 2025, from https://www.linkedin.com/in/dralexjimenez/
Kamble, N., Shukla, D., & Bhat, D. (2019). Peripheral Nerve Injuries: Electrophysiology for the Neurosurgeon. Neurology India, 67(6), 1419–1422. https://pubmed.ncbi.nlm.nih.gov/31857526/
Mitsikostas, D. D., Moka, E., Orrillo, E., Aurilio, C., Vadalouca, A., Paladini, A., & Varrassi, G. (2022). Neuropathic Pain in Neurologic Disorders: A Narrative Review. Cureus, 14(2), e22419. https://pubmed.ncbi.nlm.nih.gov/35345699/
Rosenberger, D. C., Blechschmidt, V., Timmerman, H., Wolff, A., & Treede, R. D. (2020). Challenges of neuropathic pain: focus on diabetic neuropathy. Journal of neural transmission (Vienna, Austria: 1996), 127(4), 589–624. https://pubmed.ncbi.nlm.nih.gov/32036431/
Seyedizadeh, S. H., Cheragh-Birjandi, S., & Hamedi Nia, M. R. (2020). The Effects of Combined Exercise Training (Resistance-Aerobic) on Serum Kinesin and Physical Function in Type 2 Diabetes Patients with Diabetic Peripheral Neuropathy (Randomized Controlled Trials). Journal of diabetes research, 2020, 6978128. https://pubmed.ncbi.nlm.nih.gov/32215272/
Sciatic Nerve Health at El Paso Back Clinic: Holistic Healing Solutions
The sciatic nerve is essential for movement and sensation, stretching from the lower back through the legs as the body’s largest nerve. When irritated or compressed, it can cause sciatica—sharp pain, numbness, or tingling that radiates down the leg. At El Paso Back Clinic® in El Paso, TX, we specialize in helping patients overcome sciatic nerve issues through expert chiropractic care and integrative therapies.
This article explores the sciatic nerve’s structure, made of axon bundles wrapped in protective connective tissue, and how El Paso Back Clinic’s chiropractic techniques relieve nerve pressure. We’ll also highlight our integrative approach, combining massage, physical therapy, acupuncture, and nutrition to promote natural healing. Led by Dr. Alexander Jimenez, DC, APRN, FNP-C, our clinic addresses injuries from work, sports, personal accidents, and motor vehicle accidents (MVAs) with personalized, evidence-based care.
Whether you’re managing sciatica or aiming to prevent nerve problems, El Paso Back Clinic offers solutions to help you regain mobility and live pain-free.
Understanding the Sciatic Nerve
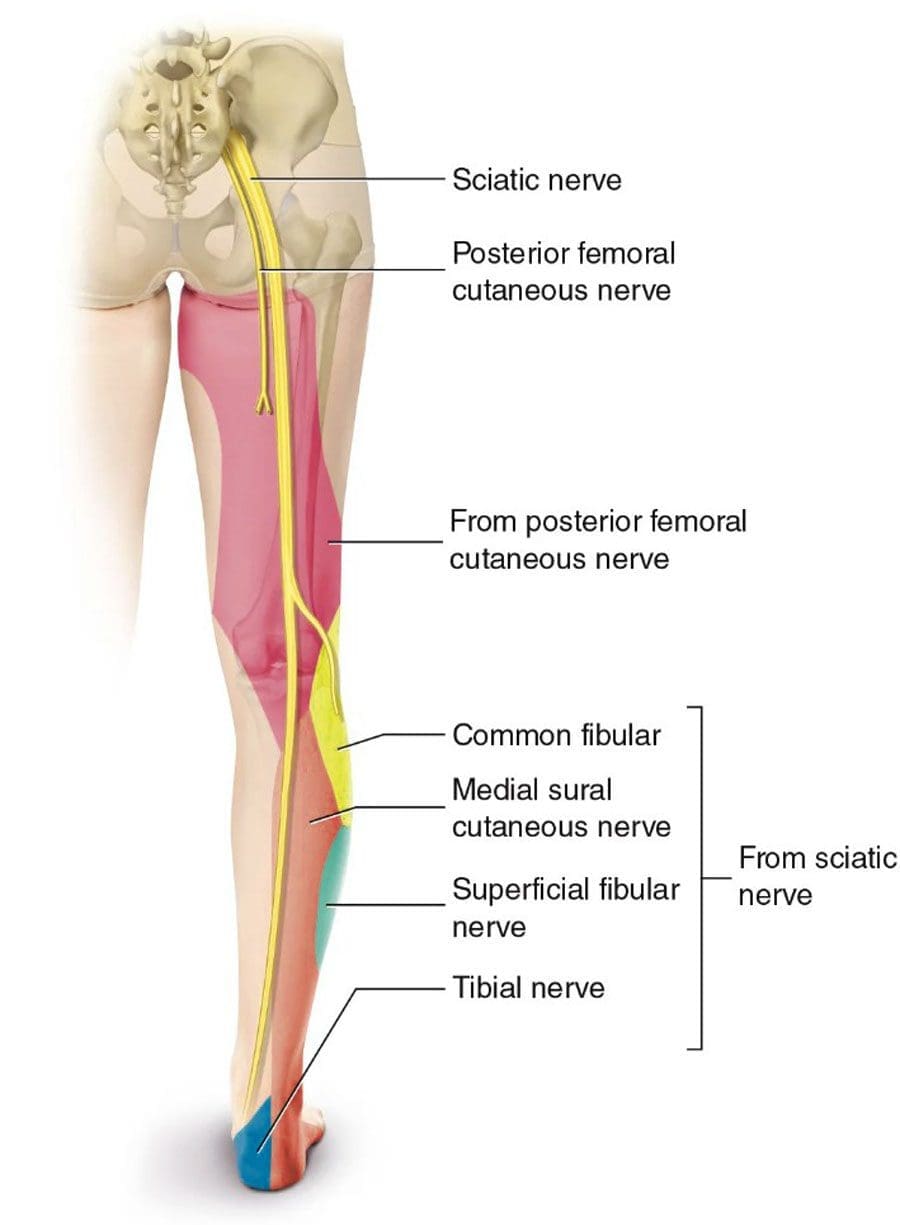
The sciatic nerve originates from the L4 to S3 nerve roots in the lower back, runs through the buttocks, and extends down each leg, controlling muscles and sending sensations from the thighs, calves, and feet. Compression from a herniated disk, tight muscles, or injury can trigger sciatica, disrupting daily activities like walking or sitting.
At El Paso Back Clinic, we focus on addressing the root causes of sciatica using non-invasive methods to support the body’s natural healing process, helping patients return to an active lifestyle.
Sciatic Nerve Structure: Axons and Protective Layers
The sciatic nerve is a complex network of neurons, each with a long fiber called an axon that transmits electrical signals. These axons are organized into bundles called fascicles, supported by layers of connective tissue:
Endoneurium: Wraps each axon and its myelin sheath, which speeds up signals and protects the nerve fiber.
Perineurium: Encases each fascicle, regulating the environment to maintain signal efficiency.
Epineurium: The outer layer surrounds the entire nerve, providing strength and flexibility.
These layers, which can comprise up to half of the nerve’s volume, ensure durability but can cause issues if they become inflamed or scarred, trapping axons and triggering pain. El Paso Back Clinic’s treatments aim to reduce inflammation and restore nerve function.
Causes of Sciatic Nerve Issues
Sciatica often results from nerve compression due to:
Herniated disks: Bulging spinal disks pressing on nerve roots.
Spinal stenosis: Narrowed spinal canals crowd the nerves.
Piriformis syndrome: A Tight piriformis muscle pinching the nerve.
Injuries: Trauma from work, sports, falls, or MVAs.
Our clinic sees these issues in patients with repetitive job strains, athletic injuries, or car accidents. Accurate diagnosis is key to effective treatment.
Chiropractic Care at El Paso Back Clinic: Relieving Nerve Pressure
Chiropractic care is at the heart of our approach at El Paso Back Clinic. Dr. Alexander Jimenez and our team use precise spinal adjustments to realign vertebrae and reduce pressure on the sciatic nerve. The procedure alleviates pain and improves mobility by addressing misalignments that cause disc bulging or muscle tension.
For example, a patient with sciatica from a slipped disk may receive lumbar adjustments to create space for the nerve. Dr. Jimenez uses advanced imaging like X-rays and MRIs to identify the issue, ensuring targeted care. His dual expertise as a chiropractor and nurse practitioner allows for comprehensive assessments, combining spinal exams with neurological testing.
Research supports the effectiveness of chiropractic care for chronic pain over medications alone (Ideal Spine, n.d.). For a delivery driver with sciatica from heavy lifting, Dr. Jimenez might use spinal decompression to gently stretch the spine, paired with rehab exercises to prevent recurrence.
Integrative Care: A Holistic Approach to Nerve Health
El Paso Back Clinic embraces integrative medicine, combining chiropractic care with massage therapy, physical therapy, acupuncture, and nutrition for optimal results. Our team, including chiropractors, therapists, and nutritionists, collaborates to create personalized treatment plans.
Massage Therapy: Techniques like deep tissue and trigger point massage relax tight muscles, such as the piriformis, reducing nerve compression. Patients often report less numbness and better movement.
Physical Therapy: Exercises like the McKenzie method or core strengthening stabilize the spine and improve flexibility, guided by our skilled therapists.
Acupuncture: Needle placements reduce inflammation and stimulate the body’s natural pain relief mechanisms, thereby enhancing chiropractic outcomes.
Nutrition Counseling: We recommend nerve-supporting nutrients like vitamin B12 (found in fish and eggs) for myelin repair and alpha-lipoic acid (in spinach) to reduce inflammation (RxWellness, n.d.; Verywell Health, n.d.).
This approach aligns with evidence-based principles of integrative care (NCCIH, n.d.), promoting healing while minimizing reliance on medications.
Dr. Jimenez’s Expertise: Healing Diverse Injuries
With over 25 years of experience, Dr. Alexander Jimenez leads El Paso Back Clinic with a dual perspective as a DC and APRN. His clinic uses advanced tools like EMG, MRI, and functional assessments to diagnose sciatica and related injuries.
Work Injuries: For a construction worker with sciatica from repetitive bending, Dr. Jimenez combines adjustments with B-vitamin supplements and ergonomic advice to prevent further strain.
Sports Injuries: A soccer player experiencing leg pain receives decompression therapy and acupuncture, supplemented by balance exercises to help restore function.
Personal Injuries: A fall victim benefits from massage and PT to reduce swelling, with detailed documentation for insurance claims.
MVAs: Car accident patients get full-body scans to connect whiplash to sciatica, with legal reports to support recovery and claims.
Dr. Jimenez’s approach, detailed on dralexjimenez.com, focuses on root-cause treatment and patient empowerment through holistic care.
Supporting Legal and Medical Needs
Injury cases often require legal or insurance documentation to support claims. El Paso Back Clinic provides thorough records, from initial X-rays to recovery progress, using pain scales and range-of-motion tests. For MVA patients, we collaborate with attorneys to streamline paperwork, ensuring patients focus on healing.
Preventing Long-Term Nerve Issues
Our integrative care promotes natural healing by improving blood flow to axons, strengthening supporting muscles, and reducing inflammation through nutrition. Regular checkups and personalized therapy goals help prevent chronic pain or arthritis, keeping patients active.
Choose El Paso Back Clinic for Sciatic Nerve Care
Located in El Paso, TX, El Paso Back Clinic® offers a welcoming environment where licensed professionals deliver tailored care. Our services—chiropractic, physical therapy, acupuncture, and nutrition—work together to relieve sciatica and boost wellness. Contact us at 915-850-0900 or visit our blog for more insights.
With El Paso Back Clinic, you’re investing in a healthier, pain-free future.
Understanding Nerve Conditions of the Spine: Causes, Symptoms, and Treatments
The spine is a critical part of the body, serving as a highway for nerves that transmit signals between the brain and the rest of the body. When something goes wrong with these nerves—whether they’re compressed, irritated, or damaged—it can lead to a range of uncomfortable symptoms like pain, numbness, tingling, or weakness. These issues, known as nerve-related spine conditions, can affect the back, arms, or legs and stem from various causes, including injuries, degenerative conditions, or infections. In this article, we’ll explore these conditions, their symptoms, causes, and how they’re diagnosed and treated, with a special focus on integrative approaches like those used by Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas. We’ll also look at how chiropractic care, targeted exercises, massage therapy, acupuncture, and integrative medicine can promote healing and prevent long-term problems.
What Are Nerve-Related Spine Conditions?
Nerve-related spine conditions happen when the spinal nerves or spinal cord are compressed, irritated, or damaged. The spine is made up of bones called vertebrae, which protect the spinal cord—a bundle of nerves that carries messages to and from the brain. Between the vertebrae are intervertebral discs, which act as cushions, and small openings called foramina, where nerve roots exit the spinal cord to connect to other parts of the body. When these nerves or the spinal cord itself are affected, it can disrupt the signals, leading to symptoms like pain, numbness, tingling, or weakness (Mayo Clinic Health System, n.d.).
Some of the most common nerve-related spine conditions include:
Radiculopathy: Often referred to as a “pinched nerve,” this condition occurs when a nerve root is compressed or irritated as it exits the spine. It can cause pain, numbness, or weakness that radiates along the nerve’s path. For example, lumbar radiculopathy can lead to sciatica, a condition characterized by pain that shoots from the lower back down the leg (Cleveland Clinic, n.d.).
Spinal stenosis refers to the narrowing of the spinal canal, which puts pressure on the spinal cord or nerve roots. It’s often caused by aging or degenerative changes and can lead to symptoms like back pain, numbness, or difficulty walking (HSS Education, n.d.).
Herniated or Bulging Discs: Discs can bulge or herniate (when the inner gel-like material pushes out), pressing on nearby nerves. This can cause pain, tingling, or weakness in the arms or legs, depending on where the disc is located (Penn Medicine, n.d.).
Degenerative Conditions: Conditions like arthritis or bone spurs can narrow the spaces where nerves travel, causing compression and symptoms like pain or stiffness (Health Central, n.d.).
Trauma or Injury: Accidents, such as car crashes or falls, can damage the spine and compress nerves, leading to immediate or delayed symptoms (Verywell Health, n.d.).
Infections or Structural Abnormalities: Infections, tumors, or abnormal spine alignment (like scoliosis) can also press on nerves, causing similar symptoms (MSD Manuals, n.d.).
These conditions can range from mild annoyances to serious issues requiring immediate medical attention, especially if they cause severe symptoms like loss of bladder or bowel control, which may indicate cauda equina syndrome, a medical emergency (Verywell Health, n.d.).
Symptoms of Nerve-Related Spine Conditions
The symptoms of nerve-related spine conditions depend on where the nerve compression or damage occurs and the severity of the condition. Common symptoms include:
Pain: This can be sharp, burning, or aching and may stay in one spot (like the neck or lower back) or radiate to other areas, such as the arms, buttocks, or legs. For example, sciatica often causes burning pain that travels from the lower back to the legs (Penn Medicine, n.d.).
Numbness or Tingling: These sensations, often described as “pins and needles,” can occur in the hands, arms, feet, or legs, depending on the affected nerve (Cleveland Clinic, n.d.).
Weakness: Muscle weakness in the arms, hands, or legs can make it hard to lift objects, walk, or maintain balance. In severe cases, it can cause issues like foot drop, where a person struggles to lift their foot while walking (Johns Hopkins Medicine, n.d.).
Loss of Coordination: Compression of the spinal cord (myelopathy) can affect fine motor skills, making tasks like buttoning a shirt or writing difficult (Verywell Health, n.d.).
Balance Issues: Spinal stenosis or myelopathy can cause trouble walking or maintaining balance, sometimes described as feeling like “walking through mud” (Spine-health, n.d.).
Loss of Bladder or Bowel Control: This is a rare but serious symptom that requires immediate medical attention, as it may signal cauda equina syndrome (HSS Education, n.d.).
Symptoms can develop suddenly, like after an injury, or gradually, as with degenerative conditions like arthritis. If you experience severe or worsening symptoms, especially loss of bladder or bowel control, seek medical care right away.
Causes of Nerve-Related Spine Conditions
Nerve-related spine conditions can have many causes, ranging from natural aging to sudden injuries. Here are some of the main culprits:
Degenerative Changes: As people age, the spine can undergo wear and tear. Osteoarthritis can cause bone spurs, and degenerative disc disease can lead to bulging or herniated discs, both of which can press on nerves (Mayo Clinic Health System, n.d.).
Herniated or Bulging Discs: When a disc’s inner material bulges or herniates, it can push against nearby nerves, causing pain or numbness. This is a common cause of radiculopathy, including sciatica (Penn Medicine, n.d.).
Spinal Stenosis: The spinal canal can narrow due to thickened ligaments, bone spurs, or other changes, putting pressure on the spinal cord or nerve roots (Cleveland Clinic, n.d.).
Trauma: Car accidents, sports injuries, or falls can fracture vertebrae, dislocate joints, or cause swelling that compresses nerves, leading to severe consequences. For example, a car crash can lead to whiplash, which may cause nerve damage in the neck (Solomon Law, n.d.).
Infections: Spinal infections, like abscesses, can press on the spinal cord or nerves, causing pain and neurological symptoms (MSD Manuals, n.d.).
Structural Abnormalities: Conditions like scoliosis (abnormal spine curvature) or tumors can compress nerves, leading to symptoms like pain or weakness (Johns Hopkins Medicine, n.d.).
Inflammatory or Autoimmune Conditions: Diseases like rheumatoid arthritis can cause inflammation that compresses nerves, contributing to symptoms (OrthoTOC, n.d.).
Each cause can lead to different symptoms and requires specific diagnostic and treatment approaches to address the root issue.
Diagnosing Nerve-Related Spine Conditions
Diagnosing nerve-related spine conditions starts with a doctor asking about your symptoms and medical history, followed by a physical exam to check for numbness, weakness, reflexes, and posture. Depending on the findings, additional tests may be needed to pinpoint the cause (Penn Medicine, n.d.). Common diagnostic tools include:
Imaging tests, such as X-rays, CT scans, or MRIs, can reveal the spine’s structure, including bones, discs, and nerves, to identify compression or damage (Spine Info, n.d.).
Nerve Conduction Studies (NCS) and Electromyography (EMG): These tests assess the function of nerves and muscles, and can help confirm nerve damage (Spine Info, n.d.).
Myelogram: A special X-ray or CT scan with contrast dye can highlight pressure on the spinal cord or nerves (Spine Info, n.d.).
Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, uses a dual-scope approach to diagnosis, combining his expertise in chiropractic care and advanced nursing. His clinic utilizes advanced neuromusculoskeletal imaging techniques, such as MRIs and CT scans, to obtain a clear picture of the spine’s condition. Dr. Jimenez correlates patient injuries—whether from work, sports, car accidents, or personal incidents—with clinical findings to create a precise diagnosis. This approach ensures that the treatment plan targets the specific cause of the nerve issue, whether it’s a herniated disc, spinal stenosis, or trauma-related damage (Jimenez, n.d.).
Treatment Options for Nerve-Related Spine Conditions
Treatment for nerve-related spine conditions depends on the cause, severity, and symptoms. Most doctors start with conservative (non-surgical) treatments, moving to surgery only if needed. Here’s an overview of common treatments:
Non-Surgical Treatments
Medications: Over-the-counter pain relievers, such as ibuprofen, or prescription medications, like gabapentin, can help manage pain and inflammation (Spine Info, n.d.).
Physical Therapy: Targeted exercises can strengthen muscles, improve posture, and reduce pressure on nerves. Physical therapy is often effective for radiculopathy and spinal stenosis (Cleveland Clinic, n.d.).
Epidural Steroid Injections: These deliver anti-inflammatory medication directly to the affected nerve root, reducing pain and swelling (Penn Medicine, n.d.).
Chiropractic Care: Adjustments and manipulations can realign the spine, relieving pressure on nerves. Dr. Jimenez’s clinic utilizes chiropractic techniques to treat conditions such as sciatica and herniated discs, with a focus on restoring spinal alignment (Jimenez, n.d.).
Massage Therapy: This can relax tight muscles, improve blood flow, and reduce nerve irritation, especially for conditions caused by muscle tension or spasms (Inova, n.d.).
Acupuncture: By stimulating specific points, acupuncture can reduce pain and promote natural healing, often used alongside other treatments (Total Spine Ortho, n.d.).
Activity Modification: Avoiding activities that worsen symptoms, like heavy lifting, can help the spine heal (Penn Medicine, n.d.).
Surgical Treatments
If conservative treatments are not effective, surgery may be necessary. Common procedures include:
Laminectomy: Removes part of a vertebra to create more space for nerves, often used for spinal stenosis (Spine Info, n.d.).
Microdiscectomy: Removes part of a herniated disc that’s pressing on a nerve, commonly used for radiculopathy (Spine Info, n.d.).
Spinal Fusion: Fuses vertebrae together to stabilize the spine, used for severe degenerative conditions or trauma (Inova, n.d.).
Dr. Jimenez’s clinic takes an integrative approach, combining chiropractic care with targeted exercises, massage therapy, and acupuncture to treat nerve-related spine conditions. For example, a patient with sciatica resulting from a herniated disc may receive spinal adjustments to realign the spine, exercises to strengthen core muscles, and acupuncture to alleviate pain. This holistic approach addresses the root cause while promoting long-term healing and preventing future problems (Jimenez, n.d.).
Dr. Alexander Jimenez’s Integrative Approach in El Paso
Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, has extensive experience treating nerve-related spine conditions caused by work, sports, personal, or motor vehicle accident injuries. His clinic uses a dual-scope approach, blending chiropractic expertise with advanced medical knowledge to provide comprehensive care. Here’s how his clinic handles these cases:
Treating Different Types of Injuries
Work Injuries: Repetitive motions or heavy lifting at work can lead to conditions like herniated discs or radiculopathy. Dr. Jimenez uses spinal adjustments, targeted exercises, and ergonomic advice to relieve nerve compression and prevent recurrence (Jimenez, n.d.).
Sports Injuries: Athletes may suffer nerve compression from trauma or overuse. The clinic employs chiropractic care, physical therapy, and massage to restore function and reduce pain, helping athletes return to their activities (Jimenez, n.d.).
Personal Injuries: Falls or other accidents can cause nerve damage. Dr. Jimenez’s team uses advanced imaging to assess the injury and creates personalized treatment plans, often including acupuncture and exercise (Jimenez, n.d.).
Motor Vehicle Accident (MVA) Injuries: Car crashes can cause whiplash or other trauma that compresses nerves. The clinic provides detailed diagnostic assessments, including MRIs, to identify nerve damage and offers treatments like spinal adjustments and massage to promote healing (Solomon Law, n.d.; Jimenez, n.d.).
Medical Care and Legal Documentation
Dr. Jimenez’s clinic is skilled in handling the medical and legal aspects of injury cases, especially for MVAs. They provide thorough documentation of injuries, diagnoses, and treatments, which is critical for insurance claims or legal cases. For example, if a patient has radiculopathy from a car accident, the clinic documents the injury’s impact on their daily life, the diagnostic findings (like MRI results), and the treatment plan. This detailed paperwork supports patients in legal proceedings while ensuring they receive proper medical care (Jimenez, n.d.).
Integrative Medicine for Healing and Prevention
Dr. Jimenez’s approach emphasizes integrative medicine, combining chiropractic care with other therapies to address the cause of nerve issues and enhance overall health. For instance:
Chiropractic Adjustments: Realign the spine to relieve nerve pressure, effective for conditions like sciatica or herniated discs.
Targeted Exercises: Strengthen muscles around the spine to improve stability and prevent future injuries.
Massage Therapy: Reduces muscle tension and improves circulation, aiding in nerve healing.
Acupuncture: Stimulates natural pain relief and promotes recovery, especially for chronic pain.
Lifestyle Changes: Advice on posture, ergonomics, and nutrition helps prevent long-term problems (Jimenez, n.d.).
This integrative approach not only treats the immediate symptoms but also focuses on long-term health, reducing the risk of chronic pain or recurring issues.
How Integrative Medicine Promotes Healing
Integrative medicine, as practiced by Dr. Jimenez, combines conventional medical treatments with complementary therapies to address the whole person, not just the symptoms. For nerve-related spine conditions, this approach offers several benefits:
Natural Healing: Chiropractic care and acupuncture stimulate the body’s natural healing processes, reducing reliance on medications (Total Spine Ortho, n.d.).
Pain Reduction: Therapies such as massage and acupuncture can help reduce pain levels, thereby improving quality of life (Inova, n.d.).
Improved Function: Exercises and adjustments restore mobility and strength, helping patients return to normal activities (Cleveland Clinic, n.d.).
Prevention: By addressing underlying causes, like poor posture or weak muscles, integrative medicine reduces the risk of future nerve problems (Jimenez, n.d.).
For example, a patient with spinal stenosis might receive adjustments to improve spinal alignment, exercises to strengthen their core, and massage to relax tight muscles. Over time, these treatments can reduce nerve compression, improve mobility, and prevent the condition from worsening.
Preventing Long-Term Problems
Preventing long-term nerve-related spine issues involves addressing the root causes and maintaining spinal health. Here are some strategies:
Maintain Good Posture: Proper posture reduces strain on the spine and nerves (Mayo Clinic Health System, n.d.).
Stay Active: Regular exercise, especially core-strengthening workouts, supports the spine and prevents injuries (Cleveland Clinic, n.d.).
Utilize ergonomics: Adjust workstations or lifting techniques to prevent repetitive strain (Jimenez, n.d.).
Manage Weight: Excess weight can put pressure on the spine, worsening nerve conditions (Health Central, n.d.).
Seek Early Treatment: Addressing symptoms early with chiropractic care or physical therapy can prevent conditions like radiculopathy from becoming chronic (Spine Info, n.d.).
Dr. Jimenez’s clinic emphasizes these preventive measures, educating patients on lifestyle changes to keep their spines healthy and reduce the risk of future nerve issues.
Conclusion
Nerve-related spine conditions, like radiculopathy, spinal stenosis, and herniated discs, can cause significant discomfort and disrupt daily life. These conditions stem from various causes, including degenerative changes, trauma, infections, or structural issues, and lead to symptoms like pain, numbness, tingling, and weakness. Through proper diagnosis using imaging and clinical assessments, doctors can pinpoint the cause and recommend treatments, ranging from medications and physical therapy to surgery in severe cases. Integrative approaches, like those used by Dr. Alexander Jimenez in El Paso, combine chiropractic care, targeted exercises, massage therapy, and acupuncture to treat injuries from work, sports, or accidents while promoting natural healing. By addressing the root cause and focusing on prevention, these methods can help patients recover and avoid long-term problems. If you’re experiencing symptoms of a nerve-related spine condition, consult a healthcare provider to explore your treatment options and start your journey to recovery.
How Massage Therapy Supports El Paso Back Clinic’s Integrative Back & Injury Care
Massage therapy is far more than relaxation. In places like El Paso Back Clinic, it is a central part of healing after injury, especially when combined with advanced diagnostics, chiropractic care, and functional medicine. This article explains how therapists are trained to use proper body mechanics and a range of techniques to deliver variable pressure safely and effectively—and how that fits specifically within the services and philosophy at El Paso Back Clinic.
El Paso Back Clinic: Philosophy & Local Context
El Paso Back Clinic is led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP. The clinic offers injury care, sports wellness, functional medicine, nutritional labs, accident & trauma rehabilitation, and more. Their goal is not only to reduce pain but also to restore function, improve long-term health, and empower patients. (El Paso Back Clinic® • 915-850-0900)
Given El Paso’s climate, traffic patterns, high incidence of work and motor vehicle injuries, and populations often facing musculoskeletal stresses (from physical labor, commute, environmental heat), having a clinic that combines hands-on care (like massage and chiropractic) plus diagnostics, nutrition, and rehabilitation gives patients a more complete path to recovery.
How Massage Therapists Are Trained at El Paso Back Clinic
At El Paso Back Clinic, massage therapists (or hands-on therapists) receive training in:
Anatomy & injury types: Understanding soft tissue, fascia, muscles, ligaments, joint mechanics, nerve irritation, and the healing stages after trauma.
Techniques with varying pressure levels include Swedish massage for light pressure, myofascial release, trigger point work, deep tissue strokes, and sports massage. The therapist must know when to adjust pressure and technique based on the patient’s needs.
They also learn body mechanics, which includes:
Using stable positions (such as lunges, with aligned shoulders and hips, and a stable base) to deliver pressure using body weight instead of relying purely on arm strength.
Keeping joints aligned to avoid strain: wrists, elbows, shoulders, and hips.
Engaging core muscles and using forearms or elbows when deeper pressure is needed, rather than overusing small muscles or risking repetitive strain injuries.
These practices help ensure therapists can deliver light, medium, or very deep pressure safely and consistently.
Variable Pressure: Light, Medium, and Deep
One of the strengths of El Paso Back Clinic is tailoring the pressure to the patient’s condition. Key considerations:
Stage of injury
Immediately after injury (e.g., whiplash, auto collision, work accident), there is often swelling, sensitivity, nerve irritation, or inflammation. Therapists start with lighter pressure to ease muscle guarding and improve circulation without causing further trauma.
As healing progresses, they gradually increase to medium or deeper pressure to break down adhesions, improve tissue mobility, release trigger points, and facilitate proper alignment.
Patient feedback
Therapists continually check with the patient (pain levels, comfort, tolerance). If pressure hurts more than helps, it is adjusted.
The use of pain or discomfort scales, or sometimes comparison between sides, helps map out what level of pressure works.
Treatment goals
For relaxation, circulation, or early healing: lighter pressure;
For chronic tightness, scar tissue, longer-term dysfunction: deeper work;
For preparing for chiropractic adjustments or rehabilitation exercises, pressure is sufficient to loosen soft tissue tension without aggravation.
Tools & technique
Use of elbows, forearms, or specialized tools when deeper pressure is needed so the therapist avoids wearing out hands and joints.
Sustained pressure (holding a spot) vs. lighter strokes; slow increments rather than sudden, strong force.
How Massage Fits into El Paso Back Clinic’s Injury & Rehabilitation Protocols
El Paso Back Clinic integrates massage therapy into its broader care model, which includes:
Chiropractic adjustments: After a massage relaxes tight muscles and soft tissue, chiropractic manipulation or spinal adjustments can be more effective because tissues are less resistant and joints can move more freely.
Diagnostic imaging & functional assessments: Before and during treatment, the clinic utilizes imaging (X-ray, MRI if necessary), laboratory and blood studies, functional movement assessments, and neurological examinations. These help identify which tissues to treat, where deeper pressure might be risky, and how far to push therapy. (El Paso Back Clinic® • 915-850-0900)
Functional Medicine & Nutrition: Pain, inflammation, and healing are influenced not only by what happens at the injury site but also by systemic factors, including nutrition, inflammation, metabolic health, sleep, and stress. The clinic evaluates these and includes them in plans, so massage and chiropractic care are supported from the inside. (El Paso Back Clinic® • 915-850-0900)
Rehabilitation & Movement Training: A range of exercises, including range of motion, strength training, posture correction, flexibility, and agility work, all help maintain gains from therapy and prevent re-injury. Massage reduces muscle tightness and improves mobility, which makes rehab exercises more effective.
Auto Injury / Trauma / Legal Documentation: For patients with motor vehicle accidents, whiplash, or other collision injuries, the clinic documents condition (soft tissues, alignment, neurologic signs), imaging findings, treatment plans, responses to massage, and other modalities. This documentation is essential to support insurance or legal claims. (El Paso Back Clinic® • 915-850-0900)
Clinical Observations & Outcomes at El Paso Back Clinic
From Dr. Jimenez’s experience and the clinic’s outcomes:
Patients who start hands-on therapy (massage) early, combined with chiropractic and functional medicine, often show quicker reduction in pain and better range of motion.
Deep pressure techniques are only introduced when imaging or assessment indicates it is safe (i.e., no unresolved inflammation, no acute nerve compression).
Many patients report better sleep, less muscle soreness, improved posture, and fewer flare-ups when massage is integrated regularly rather than used only in emergency phases.
Use of body mechanics in massage therapy helps therapists avoid fatigue and maintain consistency over a full course of care, which helps patient outcomes remain steady.
Safety, Communication, & Patient Empowerment
Safety is a big priority. The clinic ensures that:
Therapists communicate: asking about pressure, pain, any aggravations, or sensitivities.
Pressure is adjusted immediately if something doesn’t feel right.
Therapists use posture, leverage, and tools properly — so patients are treated safely and therapists avoid injury.
Patients are educated on self-care, stretches, ergonomics, and posture to sustain the benefits of therapy.
Conclusion
El Paso Back Clinic uses massage therapy not as an add-on, but as a vital part of an integrative, evidence-based healing pathway. Through professional training, variable pressure techniques, good body mechanics, diagnostics, chiropractic care, functional medicine, and legal documentation, the clinic offers patients in El Paso a full spectrum of recovery—not just temporary pain relief, but restored function, strength, and long-term wellness.
If you are recovering from a back injury, auto accident, work or sports trauma, or chronic pain, El Paso Back Clinic’s model may be what helps you return to normal life safely and fully.
Transform your well-being with chiropractic care for the gluteus medius. Experience targeted solutions for enhanced movement and relief.
Comprehensive Guide to Chiropractic Care for Gluteus Medius Injuries and Hip Pain
Key Points
Gluteus Medius Role: This muscle stabilizes your pelvis and keeps you upright during movement, preventing you from wobbling like a poorly balanced skeleton.
Hip Pain Causes: Environmental factors like prolonged sitting, poor posture, or a car accident can strain the gluteus medius, leading to pain that feels like a grim reminder of mortality.
Chiropractic Benefits: Chiropractic care, combined with non-surgical treatments, can reduce hip pain by realigning joints and strengthening muscles, offering relief without the scalpel’s cold embrace.
Dr. Jimenez’s Expertise: In El Paso, Dr. Alexander Jimenez utilizes advanced imaging and diagnostics to connect injuries to legal claims, serving as a bridge between pain and justice.
Lifestyle Adjustments: Small changes, like better posture or targeted exercises, can prevent hip pain from haunting your daily life.
Understanding Hip Pain and the Gluteus Medius
Hip pain can sneak up like a shadow in the night, turning simple tasks like walking or sitting into a grim ordeal. The gluteus medius, a key muscle in the hip, plays a crucial role in maintaining lower-body stability. When it’s injured—whether from a car accident, poor posture, or just life’s relentless grind—pain can radiate, making you feel like you’re starring in your own personal horror show. Chiropractic care, as practiced by experts like Dr. Alexander Jimenez in El Paso, offers a non-invasive way to tame this beast, restoring function and easing discomfort.
Why Chiropractic Care Matters
Chiropractic care isn’t just about cracking backs; it’s a calculated dance to restore balance to your body’s structure. For gluteus medius injuries, chiropractors use adjustments, soft tissue therapy, and targeted exercises to realign joints and strengthen muscles. This approach can reduce inflammation and pain, helping you move without feeling like you’re auditioning for a role as a creaky old gate.
Dr. Jimenez’s Role in Personal Injury Cases
In El Paso, Dr. Jimenez stands out as a beacon for personal injury victims, particularly those reeling from motor vehicle accidents (MVAs). His ability to connect clinical findings—through advanced imaging like MRI and dual-scope diagnostic procedures—to legal documentation makes him a vital ally. Whether it’s whiplash or a strained gluteus medius, his expertise ensures injuries are thoroughly assessed and properly reported for legal claims, offering a lifeline to those navigating the murky waters of recovery and justice.
Small Changes, Big Impact
Simple tweaks to your daily routine can keep hip pain at bay. From standing desks to targeted stretches, Dr. Jimenez’s insights, available through El Paso Back Clinic and his LinkedIn profile, guide patients toward lasting relief. These changes are like small wards against the creeping specter of chronic pain.
The Gluteus Medius: Your Hip’s Unsung Hero
Picture the gluteus medius as the grim, silent guardian of your hips. Nestled on the side of your pelvis, this muscle keeps you stable when you walk, run, or stand on one leg. Without it, you’d wobble like a poorly strung marionette, collapsing under the weight of your own existence. But when this muscle is injured, it’s like a betrayal from within, causing pain that can radiate from the hip to the lower back or even down the leg.
The Role of the Gluteus Medius in Lower Extremity Function
The gluteus medius is a key player in the lower extremities, acting as a stabilizer for the pelvis during movement. It abducts the hip (moves the leg away from the body) and assists in internal and external rotation. When you take a step, it prevents your pelvis from dropping on the opposite side, ensuring smooth, balanced motion. Studies show that a weak or injured gluteus medius can lead to issues such as Trendelenburg gait, where the pelvis tilts awkwardly, giving the appearance of an exaggerated posture, akin to auditioning for a role in a zombie flick (Mucha et al., 2019).
Weakness or tears in the gluteus medius can also contribute to lower back pain, knee issues, and even ankle instability. A systematic review found that individuals with low back pain often have impaired gluteus medius function, highlighting its role in the kinetic chain (Sadler et al., 2019). Essentially, if your gluteus medius is slacking, the rest of your lower body has to pick up the pieces, often with disastrous results.
References
Mucha, M. D., Caldwell, W., Schlueter, E. L., Walters, C., & Hassen, A. (2019). Gluteus medius tears of the hip: A comprehensive approach. Journal of the American Academy of Orthopaedic Surgeons, 27(3), 77–85. https://pubmed.ncbi.nlm.nih.gov/30278009/
Sadler, S., Cassidy, S., Peterson, B., Spink, M., & Chuter, V. (2019). Gluteus Medius Muscle Function in People with and without Low Back Pain: A Systematic Review. BMC Musculoskeletal Disorders, 20(1), 463. https://pubmed.ncbi.nlm.nih.gov/31640621/
Why Hip Pain Haunts: Environmental Culprits
Hip pain doesn’t just appear like a ghost in the night; the mundane horrors of daily life often summon it. Environmental factors—those sneaky, everyday villains—can wreak havoc on your gluteus medius and hips, turning your body into a creaky haunted house.
Prolonged Sitting: The Silent Killer
Sitting for hours, whether at a desk or in a car, is like sentencing your hips to a slow, torturous demise. It tightens the hip flexors and weakens the gluteus medius, creating an imbalance that screams for attention. Research shows that prolonged sedentary behavior is linked to musculoskeletal pain, including hip discomfort (Law et al., 2020). Imagine your gluteus medius, neglected and underused, plotting its revenge with every ache.
Poor Posture: The Slouch of Doom
Slouching isn’t just unflattering; it’s a biomechanical nightmare. Poor posture shifts your pelvis, overloading the gluteus medius and causing strain. Studies on posture and hip pain suggest that misaligned posture can exacerbate musculoskeletal issues, particularly in the hips and lower back (Smith et al., 2020).
Motor Vehicle Accidents: A Crash Course in Pain
Car accidents, even minor ones, can jolt the gluteus medius into dysfunction. The sudden force can strain or tear the muscle, leading to inflammation and pain. In El Paso, where rainy weather increases accident risks, the aftermath of MVAs often includes hip injuries (El Paso Back Clinic, n.d.). Whiplash-associated disorders (WAD) from accidents can also cascade into hip pain, as the body compensates for spinal misalignments (El Paso Back Clinic, n.d.).
Occupational Hazards: The Grind That Bites
Jobs requiring repetitive motions, heavy lifting, or prolonged standing can stress the gluteus medius. Construction workers, nurses, or even retail employees are at risk. A narrative review highlights that repetitive strain contributes to lateral hip pain, often tied to gluteus medius dysfunction (French et al., 2020).
Lifestyle Factors: The Everyday Terrors
Wearing high heels, carrying heavy bags on one shoulder, or even sleeping in awkward positions can damage your hips. These habits subtly strain the gluteus medius, leading to pain that feels like a cruel prank. Research on lifestyle and hip pain emphasizes the cumulative impact of these small stressors (French et al., 2020).
References
Law, D., Mark, J., & Smith, R. (2020). Hip Pain in Adults: Evaluation and Differential Diagnosis. American Family Physician, 101(2), 81–89. https://pubmed.ncbi.nlm.nih.gov/31939642/
Smith, J. A., Stabbert, H., & Bagwell, J. J. (2020). Posterior, lateral, and anterior hip pain due to musculoskeletal origin: A narrative literature review of history, physical examination, and diagnostic imaging. Journal of Chiropractic Medicine, 19(1), 1–14. https://pubmed.ncbi.nlm.nih.gov/33192189/
French, H. P., Woodley, S. J., & Schwank, A. (2020). Lateral hip pain: Relation to greater trochanteric pain syndrome. Current Reviews in Musculoskeletal Medicine, 13(5), 638–645. https://pubmed.ncbi.nlm.nih.gov/32748299/
El Paso Back Clinic. (n.d.). Auto accident insights for safe driving and recovering from WAD. Retrieved from https://elpasobackclinic.com/
Chiropractic Care: Banishing Hip Pain Without Surgery
Chiropractic care is like a well-aimed exorcism for hip pain, banishing discomfort without the need for invasive procedures. For gluteus medius injuries, chiropractors employ a multi-faceted approach that restores function and eases pain, all while keeping you out of the operating room’s cold embrace.
Why Chiropractic Works for Gluteus Medius Injuries
The gluteus medius thrives on proper alignment and balanced muscle function. Chiropractic adjustments realign the pelvis and spine, reducing stress on the muscles. According to a blog from El Paso Back Clinic, strengthening the gluteus medius post-injury involves targeted chiropractic interventions like spinal adjustments and soft tissue therapy, which improve blood flow and reduce inflammation (El Paso Chiropractor Blog, 2016). A randomized trial also found that core stability and hip exercises, often prescribed by chiropractors, improve function in patients with related pain (Jeong et al., 2020).
Non-Surgical Allies: A Team of Pain-Fighters
Chiropractic care doesn’t work alone; it’s backed by a grimly effective team of non-surgical treatments:
Massage Therapy: Loosens tight muscles and boosts circulation, like coaxing a grumpy ghost to leave. It’s particularly effective for post-MVA recovery (El Paso Back Clinic, n.d.).
Dry Needling: Targets trigger points in the gluteus medius, reducing pain with a precision that would make even Wednesday Addams nod approvingly (Gattie et al., 2021).
Rehabilitation Exercises: Progressive loading exercises strengthen the gluteus medius, preventing re-injury. A systematic review highlights their efficacy in restoring function (Moore et al., 2020).
Physical Therapy: Complements chiropractic care by improving mobility and strength, ensuring your hips don’t creak like an old coffin.
These treatments work together to address overlapping risk factors, like muscle imbalances or joint dysfunction, that amplify hip pain.
Dr. Jimenez’s Clinical Insights
Dr. Alexander Jimenez, DC, APRN, FNP-BC, brings a clinical rigor to hip pain treatment that’s as sharp as a guillotine. His approach, detailed at El Paso Back Clinic, emphasizes personalized treatment plans. Simple changes, such as using ergonomic chairs, correcting posture, or incorporating daily stretches, can help prevent hip pain from becoming a chronic issue. His LinkedIn profile showcases his expertise in integrating functional medicine with chiropractic care, providing patients with a holistic approach to recovery.
Jeong, U. C., Kim, J. S., Park, S. H., & Lee, J. H. (2020). Core stability and hip exercises improve physical function and activity in patients with non-specific low back pain: A randomized controlled trial. Journal of Back and Musculoskeletal Rehabilitation, 33(4), 581–589. https://pubmed.ncbi.nlm.nih.gov/31594203/
Gattie, E., Cleland, J. A., & Snodgrass, S. (2021). Effectiveness of dry needling and ischemic trigger point compression in the gluteus medius in patients with non-specific low back pain: A randomized short-term clinical trial. Journal of Bodywork and Movement Therapies, 27, 529–536. https://pubmed.ncbi.nlm.nih.gov/34391285/
Moore, D., Semciw, A. I., & Pizzari, T. (2020). A systematic review of rehabilitation exercises to progressively load the gluteus medius. Journal of Sport Rehabilitation, 29(2), 222–238. https://pubmed.ncbi.nlm.nih.gov/30676192/
El Paso Back Clinic. (n.d.). Trigger point therapy MVAs explained for patients. Retrieved from https://elpasobackclinic.com/
Chiropractic Care for Leg Instability- Video
Dr. Jimenez and Personal Injury Cases in El Paso
In El Paso, personal injury cases—especially those from MVAs—are as common as tumbleweeds in a desert storm. Dr. Alexander Jimenez stands out as a distinguished practitioner, offering hope to those who have been injured in accidents. His ability to connect the dots between injuries and legal claims is nothing short of macabre genius.
Advanced Diagnostics: Seeing the Invisible
Dr. Jimenez uses advanced imaging, like MRI and X-rays, to pinpoint gluteus medius injuries or other musculoskeletal damage. These tools reveal what the naked eye can’t, like a radiograph exposing a skeleton’s secrets. Dual-scope procedures, combining diagnostic and therapeutic techniques, allow him to assess and treat injuries with precision. This approach ensures that injuries are documented thoroughly, providing critical evidence for legal claims.
Bridging Medicine and Law
As a liaison between medical care and legal documentation, Dr. Jimenez ensures that personal injury victims receive comprehensive care while building a robust case. His detailed reports link clinical findings to accident-related injuries, helping attorneys secure fair compensation. This is especially vital in cases involving gluteus medius injuries, where pain can be debilitating but hard to prove without expert evaluation.
Why El Paso Needs Dr. Jimenez
El Paso’s busy roads and frequent accidents make practitioners like Dr. Jimenez invaluable. His work with MVA victims, detailed at El Paso Back Clinic, ensures that injuries like gluteus medius strains or tears are treated effectively while supporting legal outcomes. His reputation, reflected on LinkedIn, underscores his role as a trusted ally for those navigating the aftermath of personal injuries.
References
El Paso Back Clinic. (n.d.). Musculoskeletal injury treatment after car accidents. Retrieved from https://elpasobackclinic.com/
El Paso Back Clinic. (n.d.). Spinal injury rehabilitation tools for enhanced care. Retrieved from https://elpasobackclinic.com/
Small Changes, Big Relief: Practical Tips
Preventing hip pain doesn’t require a deal with the devil—just a few practical tweaks to your daily routine. Dr. Jimenez’s insights offer a roadmap to keep your gluteus medius happy and your hips pain-free.
Daily Adjustments
Ergonomic Seating: Use chairs that support proper posture to prevent hip strain. Think of it as giving your gluteus medius a comfy coffin to rest in.
Regular Movement: Stand and stretch every 30 minutes to prevent your hips from seizing up like a rusted gate.
Proper Footwear: Opt for supportive shoes instead of high heels to reduce stress on your hips and gluteus medius.
Targeted Exercises
Dr. Jimenez recommends exercises like side-lying leg lifts and clamshells to strengthen the gluteus medius. A systematic review supports progressive loading exercises to rebuild muscle strength (Moore et al., 2020). These moves are like training your hips to fend off pain’s ghostly grip.
Posture Correction
Stand tall and align your spine to reduce strain on the gluteus medius. Imagine you’re a gothic statue, poised and unyielding. Regular posture checks can prevent pain from creeping back.
Nutrition for Recovery
A diet rich in anti-inflammatory foods, like omega-3s and leafy greens, supports muscle healing. El Paso Back Clinic emphasizes nutrition’s role in MVA recovery, noting that a proper diet can reduce inflammation and speed recovery (El Paso Back Clinic, n.d.).
Table: Daily Tips for Hip Pain Prevention
Tip
Description
Benefit
Ergonomic Seating
Use chairs with lumbar support and proper height.
Reduces pelvic strain.
Regular Movement
Stand and stretch every 30 minutes during prolonged sitting.
Prevents muscle tightness.
Supportive Footwear
Wear flat, cushioned shoes instead of high heels.
Minimizes hip stress.
Gluteus Medius Exercises
Perform side-lying leg lifts and clamshells daily.
Strengthens stabilizing muscles.
Posture Correction
Maintain neutral spine alignment during sitting and standing.
Reduces biomechanical strain.
Anti-Inflammatory Diet
Include foods like salmon, walnuts, and spinach.
Supports muscle healing and reduces pain.
References
Moore, D., Semciw, A. I., & Pizzari, T. (2020). A systematic review of rehabilitation exercises to progressively load the gluteus medius. Journal of Sport Rehabilitation, 29(2), 222–238. https://pubmed.ncbi.nlm.nih.gov/30676192/
El Paso Back Clinic. (n.d.). Nutrition for accident injuries during recovery. Retrieved from https://elpasobackclinic.com/
The Bigger Picture: Chiropractic’s Role in Musculoskeletal Health
Chiropractic care isn’t just about fixing hips; it’s about restoring the body’s balance, like a grim ritual to banish chaos. For gluteus medius injuries, it addresses the root causes—misalignments, muscle imbalances, and inflammation—while preventing future issues.
Overlapping Risk Profiles
Hip pain often overlaps with other conditions, like low back pain or knee issues, due to the interconnected nature of the musculoskeletal system. A weak gluteus medius can destabilize the entire lower body, leading to a cascade of problems. Chiropractic care, combined with therapies like dry needling and massage, tackles these risks holistically, ensuring that one injury doesn’t summon a host of others (Gattie et al., 2021).
Long-Term Benefits
Regular chiropractic care can prevent chronic pain by maintaining proper alignment and muscle function. Studies show that core and hip exercises, often part of chiropractic plans, improve long-term physical function (Jeong et al., 2020). It’s like fortifying your body against the inevitable decay of time.
El Paso’s Unique Needs
In El Paso, where MVAs are a grim reality, chiropractic care is a lifeline. Dr. Jimenez’s integrative approach—combining adjustments, rehabilitation, and nutrition—addresses the unique needs of accident victims, ensuring they don’t just survive but thrive.
References
Gattie, E., Cleland, J. A., & Snodgrass, S. (2021). Effectiveness of dry needling and ischemic trigger point compression in the gluteus medius in patients with non-specific low back pain: A randomized short-term clinical trial. Journal of Bodywork and Movement Therapies, 27, 529–536. https://pubmed.ncbi.nlm.nih.gov/34391285/
Jeong, U. C., Kim, J. S., Park, S. H., & Lee, J. H. (2020). Core stability and hip exercises improve physical function and activity in patients with non-specific low back pain: A randomized controlled trial. Journal of Back and Musculoskeletal Rehabilitation, 33(4), 581–589. https://pubmed.ncbi.nlm.nih.gov/31594203/
Conclusion: A Serious Note
While we’ve danced with dark humor to lighten the mood, hip pain and gluteus medius injuries are no laughing matter. They can disrupt your life, limit your mobility, and cast a shadow over your daily routine. Chiropractic care, as championed by Dr. Alexander Jimenez in El Paso, offers a proven, non-invasive path to recovery. By addressing the root causes of pain, integrating advanced diagnostics, and supporting legal claims, Dr. Jimenez helps patients reclaim their lives. Whether you’re recovering from an MVA or battling chronic hip pain, his expertise—rooted in clinical precision and holistic care—provides a beacon of hope.
Disclaimer: This blog post is for informational purposes only and should not be taken as medical advice. Always consult a qualified healthcare provider, such as Dr. Jimenez at El Paso Back Clinic, for personalized diagnosis and treatment. Hip pain can have serious underlying causes, and professional evaluation is essential for effective care.
Mucha, M. D., Caldwell, W., Schlueter, E. L., Walters, C., & Hassen, A. (2019). Gluteus medius tears of the hip: A comprehensive approach. Journal of the American Academy of Orthopaedic Surgeons, 27(3), 77–85. https://pubmed.ncbi.nlm.nih.gov/30278009/
Sadler, S., Cassidy, S., Peterson, B., Spink, M., & Chuter, V. (2019). Gluteus Medius Muscle Function in People with and without Low Back Pain: A Systematic Review. BMC Musculoskeletal Disorders, 20(1), 463. https://pubmed.ncbi.nlm.nih.gov/31640621/
Law, D., Mark, J., & Smith, R. (2020). Hip Pain in Adults: Evaluation and Differential Diagnosis. American Family Physician, 101(2), 81–89. https://pubmed.ncbi.nlm.nih.gov/31939642/
Smith, J. A., Stabbert, H., & Bagwell, J. J. (2020). Posterior, lateral, and anterior hip pain due to musculoskeletal origin: A narrative literature review of history, physical examination, and diagnostic imaging. Journal of Chiropractic Medicine, 19(1), 1–14. https://pubmed.ncbi.nlm.nih.gov/33192189/
French, H. P., Woodley, S. J., & Schwank, A. (2020). Lateral hip pain: Relation to greater trochanteric pain syndrome. Current Reviews in Musculoskeletal Medicine, 13(5), 638–645. https://pubmed.ncbi.nlm.nih.gov/32748299/
Jeong, U. C., Kim, J. S., Park, S. H., & Lee, J. H. (2020). Core stability and hip exercises improve physical function and activity in patients with non-specific low back pain: A randomized controlled trial. Journal of Back and Musculoskeletal Rehabilitation, 33(4), 581–589. https://pubmed.ncbi.nlm.nih.gov/31594203/
Gattie, E., Cleland, J. A., & Snodgrass, S. (2021). Effectiveness of dry needling and ischemic trigger point compression in the gluteus medius in patients with non-specific low back pain: A randomized short-term clinical trial. Journal of Bodywork and Movement Therapies, 27, 529–536. https://pubmed.ncbi.nlm.nih.gov/34391285/
Moore, D., Semciw, A. I., & Pizzari, T. (2020). A systematic review of rehabilitation exercises to progressively load the gluteus medius. Journal of Sport Rehabilitation, 29(2), 222–238. https://pubmed.ncbi.nlm.nih.gov/30676192/
Yogurt Probiotics and Holistic Recovery at El Paso Back Clinic
Introduction
Not all yogurts are the same. While true yogurt always begins with Lactobacillus bulgaricus and Streptococcus thermophilus, many brands add extra probiotic strains—like Lactobacillus acidophilus or Bifidobacterium lactis—which may boost digestion, immunity, or reduce inflammation (Healthline, n.d.; Medical News Today, 2019). But beware: some yogurts are heat-treated after culturing, which kills the live bacteria and removes any probiotic benefit (Everyday Health, n.d.). To get the benefits, look for the “Live and Active Cultures” seal or find specific strain names like LA-5 and BB-12 on the ingredient list (Walgreens, 2023).
At El Paso Back Clinic, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, IFMCP, patients receive a truly integrative healing experience. The clinic weaves chiropractic care, functional nutrition, advanced diagnostics, and rehab strategies into a whole-body recovery model (El Paso Back Clinic, 2025) (El Paso Back Clinic® • 915-850-0900).
Why Probiotic Strains Matter
Each probiotic strain does something a little different:
Lactobacillus acidophilus supports immune and gut health.
Bifidobacterium lactis aids in digestion and promotes bowel regularity.
And research shows benefits are strain-specific: for example, Lactobacillus rhamnosus GG may prevent diarrhea, while Bifidobacterium infantis might soothe IBS symptoms (NIH-PMC, 2023) (El Paso Back Clinic® • 915-850-0900).
At El Paso Back Clinic, they value this specificity—just like they customize adjustments, nutrition, and rehab plans to each patient.
Choosing Effective Probiotic Yogurt
Here’s how to pick yogurt that actually delivers health benefits:
Look for the “Live and Active Cultures” seal.
Check ingredients for specific strains like LA-5 or BB-12.
Avoid shelf-stable or heat-treated yogurts.
Choose plain and low-sugar options.
Select strains proven to support your health goals, such as those that reduce inflammation or aid digestion.
These principles align with the clinic’s functional nutrition philosophy—targeted, evidence-based, and personalized. (El Paso Back Clinic® • 915-850-0900)
Linking Gut Health to Recovery and Pain Relief
El Paso Back Clinic recognizes that healing isn’t just about realigning the spine—it’s about supporting the whole-body system.
Nutrition for mobility: Adjustments improve circulation and nerve function, while nutrients and probiotics support tissue repair (El Paso Back Clinic, 2025) (El Paso Back Clinic® • 915-850-0900).
Digestive support: A healthy gut helps reduce inflammation, improve energy, and enhance nutrient absorption—boosting recovery whether from sports injuries or auto accidents (El Paso Back Clinic, 2025) (El Paso Back Clinic® • 915-850-0900).
Probiotic-rich yogurt can play a key role—especially when it’s part of a chiropractic-driven plan.
Dr. Jimenez’s Dual-Scope, Evidence-Based Approach
Dr. Alexander Jimenez brings a distinct set of skills:
Chiropractic therapy: spinal adjustments, decompression, and rehab to restore function.
Functional nutrition and medicine: personalized diet plans, targeted supplements, and laboratory assessments to combat inflammation and promote tissue healing.
Advanced diagnostics, including imaging and laboratory work, are used to identify root causes and document progress (El Paso Back Clinic, 2025) (El Paso Back Clinic • 915-850-0900).
This integration enables comprehensive injury care—whether resulting from sports, work, or vehicle accidents. Patients benefit from reduced pain, faster healing, and stronger long-term outcomes.
Probiotic Yogurt: One Piece of a Complete System
Probiotics aren’t magic—but they are a powerful ally when combined with chiropractic care and functional nutrition:
They support digestion and reduce inflammation, improving the body’s ability to heal.
They enhance nutrient absorption, which is essential for rebuilding muscle and connective tissue.
When used alongside adjustments, rehab, and supplements, probiotics help create a supportive healing environment.
This holistic model reflects El Paso Back Clinic’s philosophy: address internal health while restoring physical structure.
Conclusion
Not all yogurts are created equal. To gain real probiotic benefits, look for yogurts with live cultures and clearly listed strain names. At El Paso Back Clinic, Dr. Jimenez blends this nutritional insight with chiropractic care, functional medicine, and rehab therapies to support healing from the inside out. Together, nutrients and structure form a complete recovery plan—and probiotics can play a meaningful role in that journey.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine