Sports or Crash? The Body Needs the Same Healing Strategy
Injuries from sports and motor vehicle accidents (MVAs) often share remarkable similarities due to the high-impact forces, sudden deceleration, or forceful twisting motions involved. Whether it’s a sprain from a basketball game or whiplash from a car crash, the body experiences comparable stress that results in similar injuries. At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, Dr. Alex Jimenez, DC, APRN, FNP-BC, and our team of chiropractors, nutritionists, and medical professionals provide holistic, patient-centered care using chiropractic techniques, functional medicine, and advanced diagnostics. The severity of these injuries depends on the force and specific circumstances, and our clinic is dedicated to helping patients recover naturally while preventing long-term complications.
Common Injuries in Sports and MVAs
Both sports and MVAs can lead to traumatic brain injuries (TBIs), fractures, sprains, and strains due to intense forces. Concussions, a type of TBI, are common in contact sports like football, where a sudden hit causes the brain to move within the skull, resulting in symptoms like headaches or confusion (Skinner Firm, n.d.). Similarly, MVAs can cause concussions when the head strikes an object or moves violently during a collision (Boohoff Law, n.d.). These shared mechanisms demonstrate how rapid forces affect the brain in both contexts.
Fractures are another frequent injury. A fall during a soccer game or a car accident can break bones, with severity depending on the force and impact direction (National Institute of Arthritis and Musculoskeletal and Skin Diseases [NIAMS], n.d.). For instance, rib fractures vary based on individual anatomy and the angle of impact, as noted in biomechanics research (National Highway Traffic Safety Administration [NHTSA], n.d.). Our clinic uses advanced imaging to assess fractures and design targeted rehabilitation plans.
Sprains and strains, involving stretched or torn ligaments, muscles, or tendons, are prevalent in both scenarios. In sports, twisting motions during activities like soccer often lead to ankle or knee sprains (Therasport, n.d.; Dubuque Physical Therapy, n.d.; The Smith Clinic, n.d.). In MVAs, rapid deceleration can cause similar sprains, particularly in the neck, resulting in whiplash (Indiana Department of Health, n.d.). Neck sprains are common in both cycling accidents and car crashes, especially rear-end collisions (PubMed Central [PMC], 2011; Stroud Law, n.d.).
The severity of these injuries depends on specific factors. In sports, protective gear like helmets can reduce concussion risk, while in MVAs, seatbelts and airbags can lessen damage (Brown Health, n.d.; Advanced Ortho, n.d.). The force’s intensity, speed, and body positioning all influence outcomes. Our clinic tailors treatments to these factors, ensuring care aligns with each patient’s unique injury profile.
Dr. Alex Jimenez, a board-certified chiropractor and family nurse practitioner, leads our El Paso clinic with a passion for helping patients recover from MVAs and sports injuries. His dual expertise in chiropractic care and functional medicine allows him to address both immediate injuries and their underlying causes, promoting natural healing and long-term wellness for patients of all ages.
Dual-Scope Diagnosis and Personalized Treatment
Dr. Jimenez employs a dual-scope diagnosis to link injuries to the mechanics of an accident or activity. For example, he might connect neck pain to whiplash from a rear-end collision or a sports-related sprain to a twisting motion, assessing both visible symptoms and underlying issues like spinal misalignment. This approach informs personalized treatment plans that integrate chiropractic adjustments, acupuncture, nutrition counseling, and functional medicine. Our team of chiropractors, nutritionists, and medical professionals collaborates to ensure comprehensive care tailored to each patient’s needs.
Advanced Diagnostics and Imaging
Our clinic uses advanced diagnostic tools, including X-rays, MRIs, and functional health assessments, to identify injuries such as fractures, disc herniations, or soft tissue damage. These assessments guide precise treatment plans, ensuring care matches the injury’s severity. For instance, imaging might reveal a hidden spinal issue contributing to chronic pain, which Dr. Jimenez targets with specific therapies. This thorough approach supports both recovery and legal documentation for personal injury cases.
Medical and Legal Expertise
Dr. Jimenez’s unique ability to manage both medical treatment and legal paperwork sets our clinic apart. After an MVA, patients often face insurance disputes or lawsuits. He meticulously documents injuries, linking them to the accident, and prepares detailed reports to support legal claims. This dual expertise simplifies the process, enabling patients to concentrate on their recovery while receiving accurate medical evidence to support their claims.
Holistic Recovery Through Integrative Medicine
Our clinic combines chiropractic care, acupuncture, nutrition counseling, and functional medicine to promote natural healing. Chiropractic adjustments correct spinal and joint misalignments, addressing issues like whiplash or back pain. Acupuncture reduces pain and inflammation naturally, while nutrition counseling supports tissue repair and overall health. Functional medicine evaluates lifestyle, environmental, and genetic factors to prevent chronic issues like pain or reduced mobility.
For example, an MVA patient with a sprained ankle might receive chiropractic adjustments to restore alignment, acupuncture for pain relief, nutrition advice to support healing, and tailored exercises to rebuild strength. This integrative approach, rooted in our commitment to functional wellness, ensures faster recovery and long-term health. By addressing both the injury and its broader impact, we help patients return to a pain-free, active lifestyle in El Paso’s vibrant community.
Dr. Alex Jimenez: Pioneering Integrative Care as a Chiropractor and Nurse Practitioner
Dr. Alex Jimenez, a licensed chiropractor and board-certified nurse practitioner based in El Paso, Texas, brings over 25 years of expertise to his Injury Medical & Chiropractic Clinic practice. His dual licensure provides unique insights into the etiologies, pathogenesis, and treatment of complex clinical conditions, enabling him to deliver patient-centered, integrative care that bridges physical medicine, functional medicine, and advanced diagnostics. Combining chiropractic expertise with nurse practitioner-driven medical management, Dr. Jimenez offers comprehensive treatment protocols tailored to acute and chronic conditions, promoting metabolic resilience, longevity, and whole-person wellness.
Dual Expertise: Chiropractic and Nurse Practitioner Roles
Dr. Jimenez’s practice stands out due to his ability to integrate the biomechanical focus of chiropractic care with a nurse practitioner’s diagnostic and therapeutic scope. As a chiropractor, he specializes in restoring musculoskeletal function, particularly after trauma, neck, back, spine, and soft tissue injuries. His chiropractic interventions emphasize non-invasive techniques, such as spinal decompression, manual adjustments, and functional rehabilitation, to alleviate pain and enhance mobility.
As a board-certified nurse practitioner, Dr. Jimenez employs evidence-based medicine to address systemic and metabolic dysfunctions. His expertise extends to managing chronic degenerative disorders, hormonal imbalances, weight loss, sexual health, and pain syndromes. This dual perspective allows him to identify underlying disease causes, from biomechanical misalignments to physiological imbalances, and design treatment regimens that address symptoms and root causes.
The synergy of these roles enables Dr. Jimenez to offer a holistic approach that is particularly effective for complex conditions such as sciatica, fibromyalgia, disc herniation, spondylolisthesis, and chronic neck or back pain. His integrative protocols combine functional medicine assessments, lifestyle interventions, and advanced diagnostics to achieve homeostasis and physiological balance.
Treatment Protocols: Evidence-Based and Patient-Centered
Drawing from integrative protocols outlined on his website, www.chiromed.com, Dr. Jimenez employs a multidisciplinary approach to patient care. His treatment plans are grounded in evidence-based medicine, functional medicine, and lifestyle wellness strategies, tailored to each patient’s unique health profile, lifestyle, and medical history. Below are key components of his integrative care model:
1. Chiropractic Care and Functional Rehabilitation
Spinal Decompression: Non-surgical decompression therapy is used to relieve pressure on spinal discs, addressing conditions like disc herniation, sciatica, and spinal stenosis. This modality promotes healing by improving blood flow and nutrient delivery to affected areas.
Manual Adjustments: Targeted adjustments correct spinal misalignments, reduce nerve compression, and restore joint mobility. These are particularly effective for whiplash, scoliosis, and poor posture.
Functional Strength Training: Dr. Jimenez designs conditioning programs to enhance recovery and prevent re-injury. These programs are tailored for athletes and individuals seeking optimal performance and incorporate mobility, flexibility, and agility training.
2. Functional Medicine Assessments
Functional medicine tools evaluate metabolic, hormonal, and nutritional status. These assessments identify the root causes of conditions such as fatigue, weight gain, or chronic pain, enabling precise interventions.
Advanced diagnostic protocols, including blood panels and imaging, provide data-driven insights into etiologies and pathogenesis. This allows Dr. Jimenez to address underlying dysfunctions rather than merely masking symptoms.
3. Lifestyle and Nutritional Interventions
Weight Loss and Metabolic Resilience: Dr. Jimenez integrates nutritional counseling and metabolic optimization strategies to support sustainable weight loss and prevent chronic diseases like diabetes or cardiovascular disorders.
Hormone and Sexual Health: Personalized regimens address hormonal imbalances and sexual dysfunction, improving quality of life and overall wellness.
Pain Management: Nutritional and lifestyle modifications complement physical therapies to manage chronic pain syndromes, reducing reliance on pharmaceuticals.
4. Specialized Care for Complex Conditions
Sciatica and Disc Injuries: Dr. Jimenez employs targeted decompression and rehabilitation protocols to alleviate nerve compression and restore function.
Chronic Degenerative Disorders: Conditions like fibromyalgia, arthritis, and spondylolisthesis are managed through integrative plans that combine physical therapy, nutritional support, and metabolic optimization.
Sports and Auto Accident Injuries: Tailored rehabilitation programs address soft tissue damage, shoulder injuries, and whiplash, ensuring rapid recovery and long-term resilience.
5. Advanced Wellness Programs
Dr. Jimenez’s clinic offers comprehensive wellness programs on longevity, skin care, and hair loss. These programs integrate nutritional supplementation, lifestyle coaching, and cutting-edge therapies to promote vitality and aesthetic health.
High-level conditioning programs optimize performance for athletes, incorporating functional strength training and recovery-focused interventions.
Integrative Team and Clinic Highlights
Injury Medical & Chiropractic Clinic is El Paso’s largest mobility, flexibility, and agility center, integrating chiropractors, nurse practitioners, registered nurses, nutritionists, and physical performance trainers. The clinic’s multidisciplinary team collaborates to deliver personalized care, ensuring patients achieve measurable health outcomes. Key services include:
Acupuncture: A Complementary therapy to reduce pain and promote relaxation.
Advanced Nutritional Programs: Evidence-based dietary plans to support metabolic health and recovery.
Physical Performance Training: Programs to enhance fitness, prevent injuries, and optimize athletic performance.
The clinic accepts major insurances, including Aetna, Blue Cross Blue Shield, Cigna, and First Health, making care accessible to a broad patient base.
Insights from Dual Licensure
Dr. Jimenez’s licensure as both a chiropractor and nurse practitioner provides him with a comprehensive understanding of disease processes and treatment modalities. His chiropractic training equips him to address biomechanical dysfunctions, while his nurse practitioner expertise allows him to manage systemic conditions with a medical lens. This dual perspective enhances his ability to:
Clarify Etiologies: By combining musculoskeletal assessments with metabolic and hormonal evaluations, Dr. Jimenez identifies multifactorial causes of conditions, ensuring targeted interventions.
Understand Pathogenesis: His knowledge of disease progression informs proactive treatment plans that halt or reverse degenerative processes.
Design Appropriate Regimens: Integrating physical, nutritional, and medical therapies, Dr. Jimenez creates synergistic treatment plans that address both symptoms and underlying dysfunctions.
This integrative approach is particularly valuable for patients with chronic or multifactorial conditions, as it addresses the interplay between physical, metabolic, and lifestyle factors.
Patient-Centered Care: In-Person and Online
Dr. Jimenez’s practice emphasizes personalized attention, whether patients visit in person at 11860 Vista Del Sol, Suite 128, El Paso, TX 79936, or engage through telehealth. His functional medicine series, accessible via www.dralexjimenez.com, educates patients on holistic health principles, covering topics from spinal health to metabolic optimization. The website features:
Informative Content: Blog posts, articles, and videos provide insights into chiropractic care, functional medicine, and injury rehabilitation.
Patient Testimonials: Success stories highlight the transformative impact of Dr. Jimenez’s care, showcasing outcomes for conditions like sciatica, sports injuries, and chronic pain.
Appointment Booking: A user-friendly interface allows patients to schedule in-person or online consultations, with clear guidance on what to expect during their first visit.
Commitment to Education and Community Health
Dr. Jimenez is dedicated to empowering patients through education. His website is comprehensive, offering evidence-based information on health conditions, treatment options, and wellness strategies. By fostering health literacy, Dr. Jimenez enables patients to make informed decisions and take charge of their well-being.
His commitment extends to the El Paso community, where he aims to expand access to integrative care. Dr. Jimenez promotes proactive health management and preventive care through workshops, online content, and community outreach.
Conclusion
Dr. Alex Jimenez’s dual expertise as a chiropractor and nurse practitioner positions him as a leader in integrative medicine. His ability to bridge physical medicine with systemic health management allows him to address complex clinical issues with precision and compassion. Dr. Jimenez delivers personalized care that promotes healing, resilience, and longevity by leveraging evidence-based protocols, advanced diagnostics, and lifestyle interventions.
For more information or to schedule an appointment, visit www.dralexjimenez.com or contact the clinic at +1-915-412-6677.
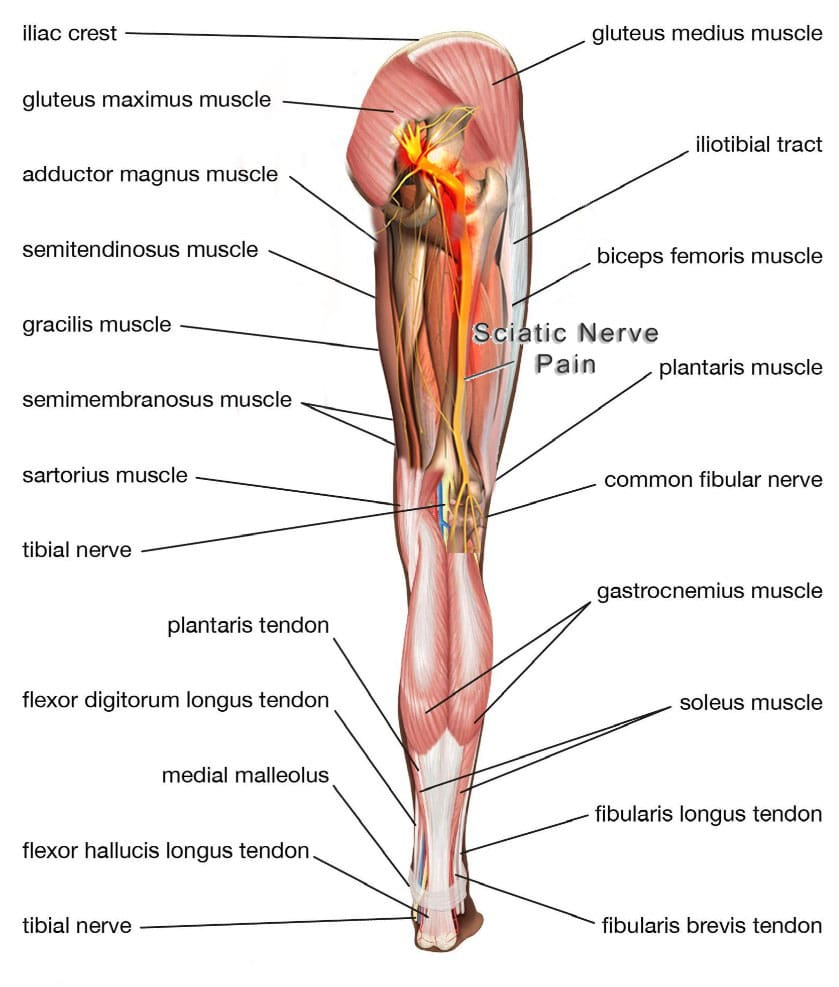
Individuals dealing with pain in the buttocks and in the back of the thigh, along with numbness and tingling down to the bottom of the foot, may be experiencing hamstring syndrome, a condition caused by pressure on the sciatic nerve. What is the recommended treatment?
Hamstring-Syndrome Relief
The hamstrings are three muscles in the back of the thigh, extending from the pelvis or upper thigh across the back of the knee to the leg. This muscle group is important for bending the knee, straightening the hip, and stabilizing the knee. The sciatic nerve is a large nerve that runs from the lower back down the legs. It usually passes near or through these muscles, and the pelvis then runs under these muscles in the thigh. Hamstring syndrome refers to pain in the buttock and back of the thigh, often radiating down the leg, caused by compression or irritation of the sciatic nerve at the hamstring-insertion point on the ischial tuberosity, typically due to tight or scarred tissue. (Sakari Orava, 1997)
Pain Location
The pain is primarily felt in the buttock and back of the thigh, sometimes extending down the leg. It’s characterized by pressure on the sciatic nerve, which runs through the buttock and into the back of the thigh, where it supplies the hamstring muscles. (Kaiser Permanente, 2024)
In some cases, injections with cortisone and numbing medicine may be used to reduce nerve inflammation and pain. (Lower Limb Surgery, 2024)
Surgery
In severe cases, surgery may be necessary to release the compressing bands and free the sciatic nerve. (Lower Limb Surgery, 2024)
Injury Medical Chiropractic & Functional Medicine Clinic
Talk to a healthcare provider about what interventions would help the most. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Kaiser Permanente. (2024). Hamstring Syndrome: Care Instructions. https://healthy.kaiserpermanente.org/health-wellness/health-encyclopedia/he.hamstring-syndrome-care-instructions.abr3618
Puranen, J., & Orava, S. (1988). The hamstring syndrome. A new diagnosis of gluteal sciatic pain. The American Journal of Sports Medicine, 16(5), 517–521. https://doi.org/10.1177/036354658801600515
Zion Physical Therapy. (2023). Hamstring Tendinitis Vs. Hamstring Syndrome. https://www.zionpt.com/post/hamstring-tendinitis-vs-hamstring-syndrome
Finger pulley injuries are unique digital injuries distinct from sprains or dislocations. They occur specifically in rock climbers and occasionally in baseball pitchers. What are the symptoms, diagnoses, and treatments available?
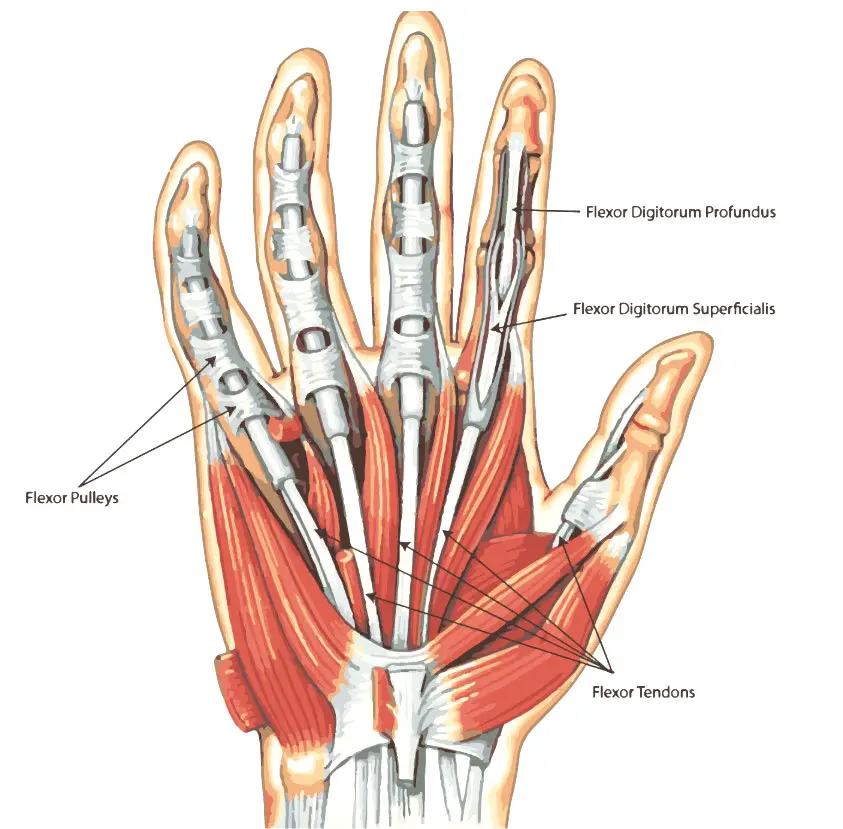
Finger Pulley Injury
A finger pulley injury, common in activities like climbing, involves damage to the fibrous bands (pulleys) that hold tendons against bones. This causes pain, swelling, and potentially bowstringing of the tendons.
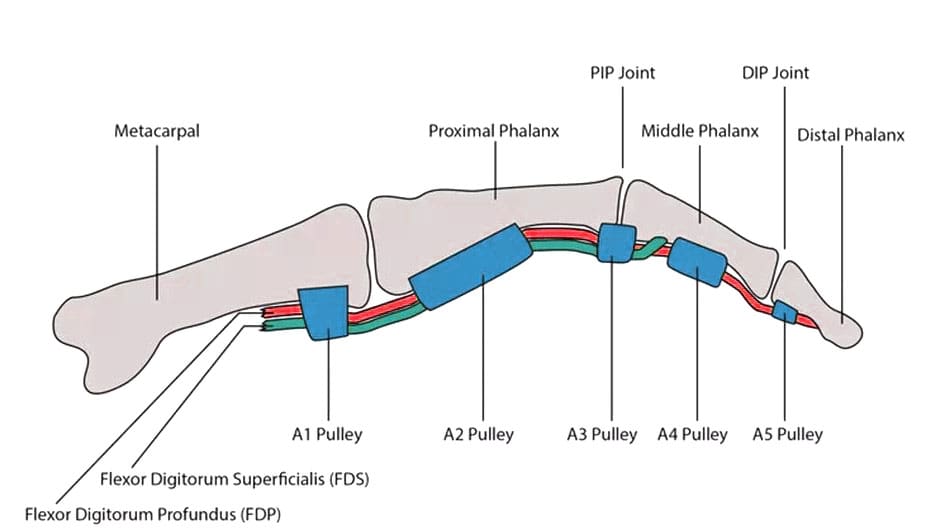
Finger pulleys are structures that hold tendons against the bones of the fingers.
Injury symptoms include pain, swelling, and a popping sound heard at the time of the injury.
Finger pulley injuries, or ruptures of the digital pulley, are seen almost exclusively in rock climbers. (Miro P. H. et al., 2021)
This activity stresses the digits when maneuvering along uneven surfaces while supporting the entire body’s weight. The injuries result from the mechanics of the finger tendons and joints and the position the fingers hold while rock climbing. Rock climbing has grown in popularity. The only other sport in which this injury has been described is baseball, in pitchers. The forces acting on the finger are very different in these activities, but both place high stress on the finger pulleys.
Digital Pulleys
Everyone has structures in their fingers called digital pulleys. These pulleys hold the tendons against the bones of the fingers. Each finger has eight pulleys, but only two are considered critical to prevent the finger tendons’ bowstringing (when one pulley gives out or ruptures). This can result in various injury outcomes, from a simple strain of the pulley to ruptures of multiple pulleys in a single digit. Pain, stiffness, and an inability to fully flex the finger can occur. (Carruthers K. H., Skie M., & Jain M. 2016) In severe situations, when the tendons are bowstringing, the tendon may lift away from the finger when making a fist.
Symptoms
Pain and Tenderness
Localized pain and tenderness at the finger’s base, particularly when gripping or bending. Pain on the palm side of finger and tenderness with pressure
Swelling
Swelling and bruising around the affected finger joint, especially on the palm side.
Stiffness and pain when bending the fingers or difficulty gripping. Difficulty forming a fist
Bowstringing
Visible displacement of the tendon from its normal position, causing a bulge at the finger’s base.
Most commonly, the middle or index digit is the injured finger. The two critical pulleys in the finger are designated the A2 and A4. (Carruthers K. H., Skie M., & Jain M. 2016) Individuals may see swelling, redness, and inflammation at the base of the finger (A2) and/or in the space between the two finger joints closest to the tip of the finger (A4). In rock climbers, either or both of those pulleys may be injured. In baseball pitchers, the injury is typically isolated to the A4 pulley.
Causes
Overuse and Repetitive Strain: Frequent or intense gripping or crimping, common in rock climbing and other activities, can cause pulley injuries.
Dynamic or Sudden Movements: Desperate or dynamic moves or poor technique can lead to injury.
Excessive Force: Pulleys can rupture when the force exerted on them is too great.
Mechanism of injury: The A2 pulley is the most commonly injured, followed by the A4 pulley.
Diagnosis
Emergency treatment is generally unnecessary. However, it is important to have suspected digital pulley injuries examined by a specialist within several days to a week after the injury. The most important aspect of an evaluation is determining whether the injury has caused the bowstringing of the tendons. Imaging tests may be performed to help with the diagnosis and plan treatment. An ultrasound is recommended as the initial imaging technique. (Miro P. H. et al., 2021)
If an ultrasound is inconclusive, an MRI may be advised. Sometimes, an MRI is performed with the finger held straight and then bent to see if the tendons are bowstringing. An X-ray can also help exclude other causes of finger pain, including sprains and fractures.
Treatment
Conservative Care
Immobilization, physical therapy, and pulley-protective measures, such as splints or taped fingers, are often used.
Surgery
Surgery may be necessary for severe grade IV injuries where conservative care fails.
Only in situations where there are multiple pulley ruptures or if there is delayed treatment should surgery be necessary.
Rehabilitation
Focuses on regaining flexibility, strength, and grip function through exercises and physical therapy.
If the tendons do not bowstring, treatment usually protects the injured finger until swelling and pain subside. If there is bowstringing of the tendons, more careful management of the injury is needed. Individuals who suspect a pulley injury rest or splint the finger and use nonsteroidal anti-inflammatory drugs as necessary for pain until they can get a medical evaluation. (Carruthers K. H., Skie M., & Jain M. 2016) Physical therapy, along with immobilization, the H-tape method, and a protective pulley splint, are recommended for most injuries. (Miro P. H. et al., 2021) Specialized splints and therapy techniques can allow the pulleys to heal properly.
Returning to activity varies significantly with the severity of the injury. With mild pulley strains, full activity can be resumed as soon as swelling and pain have subsided. Treatment for full ruptures being treated non-surgically is typically between one and three months. For individuals requiring surgical reconstruction of a pulley injury, restrictions may apply up to a year after the surgery.
Injury Medical Chiropractic & Functional Medicine Clinic
To prevent complications, a healthcare provider should evaluate pulley injuries as soon as possible. Treatment most often consists of physical therapy, but surgery may be necessary. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Sports Injury Treatments
References
Miro, P. H., vanSonnenberg, E., Sabb, D. M., & Schöffl, V. (2021). Finger Flexor Pulley Injuries in Rock Climbers. Wilderness & environmental medicine, 32(2), 247–258. https://doi.org/10.1016/j.wem.2021.01.011
Carruthers, K. H., Skie, M., & Jain, M. (2016). Jam Injuries of the Finger: Diagnosis and Management of Injuries to the Interphalangeal Joints Across Multiple Sports and Levels of Experience. Sports Health, 8(5), 469–478. https://doi.org/10.1177/1941738116658643
In females, hernia symptoms are often smaller and deeper without a noticeable lump and can mimic gynecological issues, with misdiagnoses being common. Can knowing the risk factors and how female hernias are treated help women get relief?
Female Hernia
A hernia occurs when an internal structure pushes through a weak spot in the abdominal wall, the muscles, and the tissue covering the front of the torso. The more common include:
Groin hernia, known as an inguinal hernia.
Upper thigh or femoral hernia.
However, a hernia can develop anywhere from the ribcage to the upper thigh. Hernias are less common in women, have different symptoms than in men, and are often misdiagnosed. Lower abdominal and pelvic hernias present differently in women than men, who typically have a visible bulge. Instead, female hernias tend to be smaller, deeper, and less noticeable. They can also cause chronic pelvic pressure or pain that can be mistaken for gynecological problems.
Hernia Symptoms For a Woman
Hernias in women tend to be smaller and deeper than male hernias, with no lump showing. Instead, female hernias can cause chronic, deep pelvic pain and occasional sharp, stabbing pain that comes on fast and lingers. (Köckerling F., Koch A., & Lorenz R. 2019) Hernia pain worsens with exercise, laughing, coughing, or straining to evacuate the bowels. The pain is often described as:
Dull
Aching
Pinching
Sharp
Shooting
Burning
Inguinal hernia pain is usually felt at or above the groin and may radiate to the hip, lower back, vulva, or thigh. Many women find the pain increases during their menstrual cycle. The pain can also be exacerbated by any activity that generates extra pressure on the pelvic floor, including:
Prolonged sitting or standing.
Bending
Getting in or out of bed.
Getting in or out of a car.
Sexual intercourse
Emergency
Hernias in the pelvic area are at risk of becoming incarcerated hernias. An incarcerated hernia occurs when a portion of the intestine or other abdominal tissue becomes trapped in the hernial sac, making it impossible to push it back into place. If this gets trapped or strangulated, it can cause tissue death. Strangulated hernias are a medical emergency. Symptoms include:
Deep red or purple tissues.
The hernia bulge does not shrink when you lie down.
Contact a healthcare provider or the emergency room if experiencing any of the above symptoms.
Types
Hernias can occur anywhere on the abdominal wall. They may be caused by:
Internal pressure, such as during pregnancy.
A sports injury
Tissue weakness
Hernias in the lower abdomen or groin are typically indirect inguinal hernias. The inguinal canal comprises multiple layers of muscles and fascia that the thin round ligament threads through. Other groin and pelvic hernias include:
A direct inguinal hernia
A femoral hernia at the top of the inner thigh.
An obturator hernia in the front upper thigh, although this type is rare.
Other common hernias in women are:
Incisional hernia – at the site of a surgical incision
Pregnancy and repeated pregnancies are linked to an increased risk of hernia. Types that are more common in pregnancy include:
Umbilical hernia
Ventral hernia
Inguinal hernia
Umbilical hernias are the most common. However, only a small percentage of pregnant individuals get them. (Kulacoglu H. 2018)
Diagnosis
A hernia diagnosis is made with a physical examination and, if needed, imaging studies. Patients are asked to describe their symptoms precisely, where the pain is located, and any activities that exacerbate it. To check for a hernia, the healthcare provider will palpate for a hernia while the patient sits, stands, or coughs. Imaging tests can include:
Ultrasound
CT scan
Endoscopy – a camera is used to see inside the esophagus and stomach.
Misdiagnoses
Female hernia symptoms can be vague, which often points healthcare providers in the wrong direction. Female hernias are commonly misdiagnosed as: (Köckerling F., Koch A., & Lorenz R. 2019)
Cysts in the reproductive organs
Endometriosis
Fibroid tumors
Treatment
A small hernia that does not cause problems or pain may be treated with a wait-and-evaluate protocol. A hernia often worsens over time and could eventually require surgery. (University of Michigan Health, 2024) Self-care treatments include:
Medical treatments usually start with conservative measures, including physical therapy, stretching, exercise, and rest. Physical therapists often use myofascial release techniques to relieve muscle spasms. Surgery may be needed to repair the weak area of the abdominal wall to relieve symptoms. (University of Michigan Health, 2024) Hernia repair surgery is typically performed as a laparoscopic surgery. (Köckerling F., Koch A., & Lorenz R. 2019) Most patients heal quickly from the surgery and can return to regular activities in a week or two.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Lumbar Spine Injuries in Sports: Chiropractic Healing
References
Köckerling, F., Koch, A., & Lorenz, R. (2019). Groin Hernias in Women-A Review of the Literature. Frontiers in surgery, 6, 4. https://doi.org/10.3389/fsurg.2019.00004
Johns Hopkins Medicine. (2025). How to tell if you have a hernia. https://www.hopkinsmedicine.org/health/conditions-and-diseases/how-to-tell-if-you-have-a-hernia
Kulacoglu H. (2018). Umbilical Hernia Repair and Pregnancy: Before, during, after…. Frontiers in surgery, 5, 1. https://doi.org/10.3389/fsurg.2018.00001
University of Michigan Health. (2024). Inguinal hernia: Should I have surgery now, or should I wait? https://www.uofmhealth.org/health-library/za1162
American Academy of Orthopaedic Surgeons. (2022). Sports hernia. https://orthoinfo.aaos.org/en/diseases–conditions/sports-hernia-athletic-pubalgia/
Northeast Georgia Health System. (2022). Living with a hernia. Northeast Georgia Health System Improving the health of our community in all we do. https://www.nghs.com/2022/02/15/living-with-a-hernia
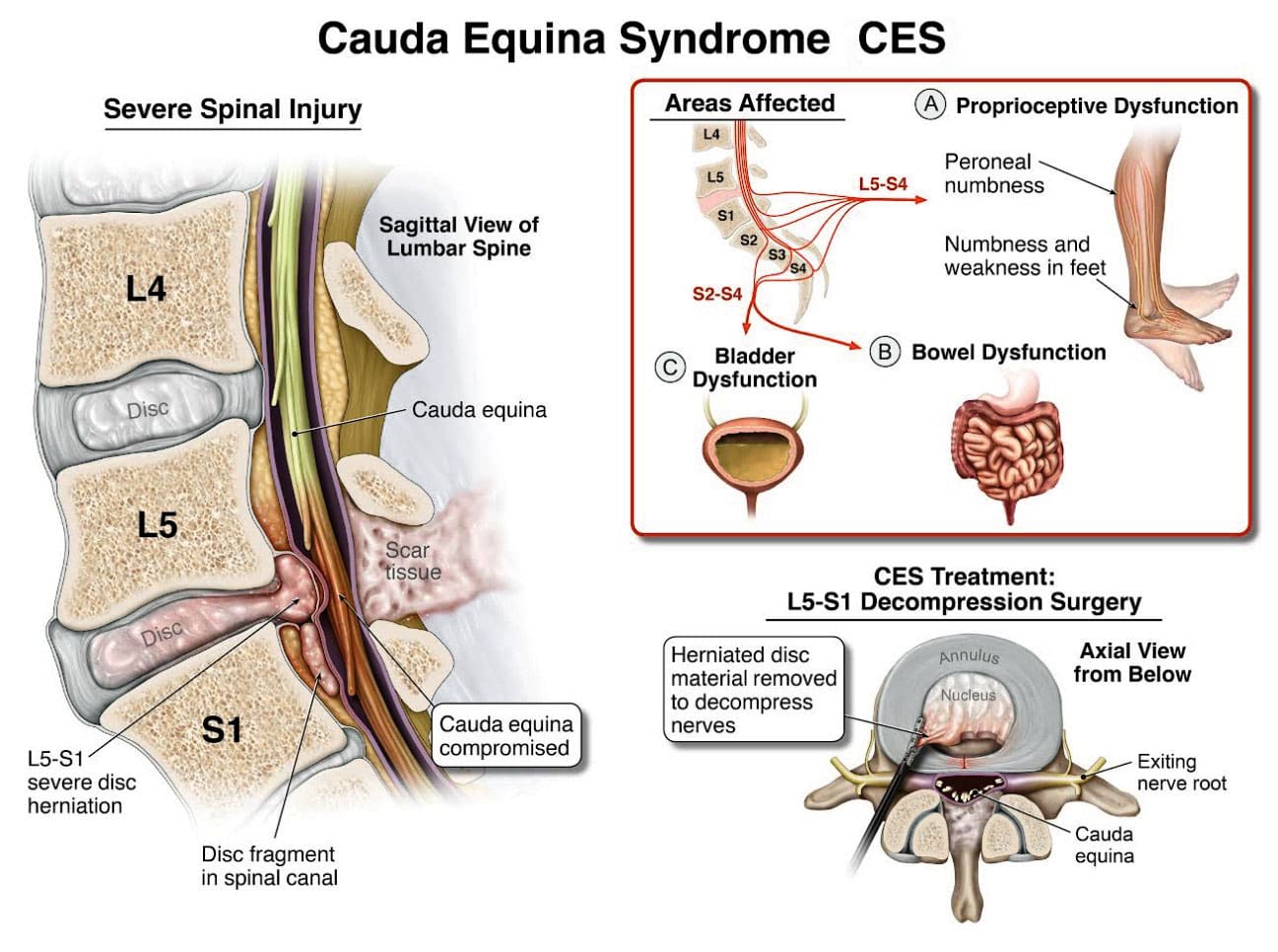
Cauda equina syndrome/CES is a rare condition in which the nerves in the lower back are compressed. It can include sciatica as one of its symptoms. Individuals presenting with symptoms that could be CES are advised to see a healthcare provider as soon as possible, as delaying treatment can lead to permanent damage.
Cauda Equina Syndrome
A cluster of nerve roots called the cauda equina, Latin for horse’s tail, sends and receives messages to the legs, bladder, and other body parts. Cauda equina syndrome is a rare condition in which nerve roots in the lower spinal cord are compressed. This compresses the nerves and disrupts motor and sensory function in the bladder and lower extremities. The most common cause is a ruptured or herniated disc in the lumbar area. This usually occurs when a severe disc herniation compresses the nerve bundle at the base of the spinal cord, causing significant neurological dysfunction like bladder/bowel issues and numbness in the saddle area. If found early, it is treated with surgery within 24 to 48 hours of symptom onset.
This is characterized by symptoms that include unusual urinary sensation, loss of desire to urinate, poor urinary stream, and having to strain to urinate. (Gardner A., Gardner E., & Morley T. 2011)
Pott’s paralysis is a neurological complication of tuberculosis (TB) of the spine.
TB is a bacterial infection that usually affects the lungs but can spread to the spine.
Iatrogenic Side Effects
Injuries or illnesses that result from medical or surgical treatment
Spinal Lesions or Malignant Tumors
A spinal lesion refers to any abnormal growth or damage within the spine.
It can include benign (noncancerous) and malignant (cancerous) tumors.
A malignant tumor is a cancerous growth within the spine; essentially, a malignant tumor is a type of spinal lesion with the potential to spread to other parts of the body.
Spinal Infection, Inflammation, Hemorrhage, or Fracture
A spinal infection refers to a bacterial, fungal, or viral infection that occurs within the bones of the spine (vertebrae) or the surrounding tissues, potentially causing pain, inflammation, and, in severe cases, neurological complications like weakness or paralysis;
Spinal inflammation is a general term for swelling or irritation within the spinal column.
Spinal hemorrhage” indicates bleeding within the spinal canal.
A spinal fracture refers to a break in one or more of the vertebrae in the spine.
Spinal Arteriovenous Malformations (AVMs)
A spinal arteriovenous malformation (AVM) is a rare condition in which the arteries and veins in the spinal cord tangle abnormally.
This can damage the spinal cord over time.
Complications from Lumbar Surgery
Lumbar surgery can have several complications, including infections, blood clots, nerve damage, and spinal fluid leaks.
Spinal Anesthesia
Spinal anesthesia is a regional anesthesia that blocks pain and sensation in the lower body.
It involves injecting a local anesthetic medication into the subarachnoid space surrounding the spinal cord.
The exact cause is not fully understood, but it can involve direct nerve root injury from the needle, inflammation caused by the anesthetic, or a spinal hematoma compressing the nerve roots.
Infection of the tissues (meninges) that cover the cauda equina and spinal cord.
An abscess pressing on the cauda equina.
Diagnosis
Diagnosis requires a medical history of symptoms, general health, activity level, and a physical exam to assess strength, reflexes, sensation, stability, alignment, and motion. (American Association of Neurological Surgeons, 2024) Testing includes:
X-ray or computerized tomography (CT) imaging is enhanced by the injection of contrast material into the cerebrospinal fluid spaces, which can show displacement of the spinal cord or spinal nerves.
Specialized Nerve Testing
This could be nerve conduction velocity tests and testing electrical activity in muscles or electromyography.
Treatment
The extent of urinary problems can determine treatment protocols. A CES diagnosis is usually followed by emergency surgery within 24 to 48 hours to relieve compression of the nerves. Moving quickly is essential to prevent permanent complications such as nerve damage, incontinence, or leg paralysis. (American Association of Neurological Surgeons, 2024)
Depending on the cause, corticosteroids also may be prescribed to reduce swelling.
Antibiotics may be needed if an infection is responsible for CES.
For situations in which a tumor is the cause, surgery to remove it may be necessary, followed by chemotherapy and/or radiation.
The outcome with CES-I during surgery is generally favorable.
Those whose CES has deteriorated to CES-R tend to have a less favorable prognosis.
Post Surgery Therapy
After surgery, CES can be challenging to deal with. If bladder function has been impaired, recovery of control can take time.
Frequent urinary infections are also a potential complication.
Loss of bladder or bowel control can be psychologically distressing, impacting social life, work, and relationships.
Sexual dysfunction can also occur, contributing to relationship difficulties or depression.
Therapy with a mental health professional may be recommended. When damage is permanent, it will be important to include family and friends in the adjustment to living with a chronic condition. Psychological counseling and/or a support group can be helpful. Other specialists who can help include: (American Academy of Orthopaedic Surgeons, 2024)
Occupational therapist
Physical therapist
Physiotherapist
Sex therapist
Social worker
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and mitigate issues through adjustments that help the body realign itself. The clinic can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Disc Herniation
References
American Association of Neurological Surgeons. (2024). Cauda Equina Syndrome. https://www.aans.org/patients/conditions-treatments/cauda-equina-syndrome/
Gardner, A., Gardner, E., & Morley, T. (2011). Cauda equina syndrome: a review of the current clinical and medico-legal position. European Spine Journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 20(5), 690–697. https://doi.org/10.1007/s00586-010-1668-3
Fairbank, J., & Mallen, C. (2014). Cauda equina syndrome: implications for primary care. The British journal of general practice: the journal of the Royal College of General Practitioners, 64(619), 67–68. https://doi.org/10.3399/bjgp14X676988
American Academy of Orthopaedic Surgeons. (2024). Cauda equina syndrome. https://orthoinfo.aaos.org/en/diseases–conditions/cauda-equina-syndrome
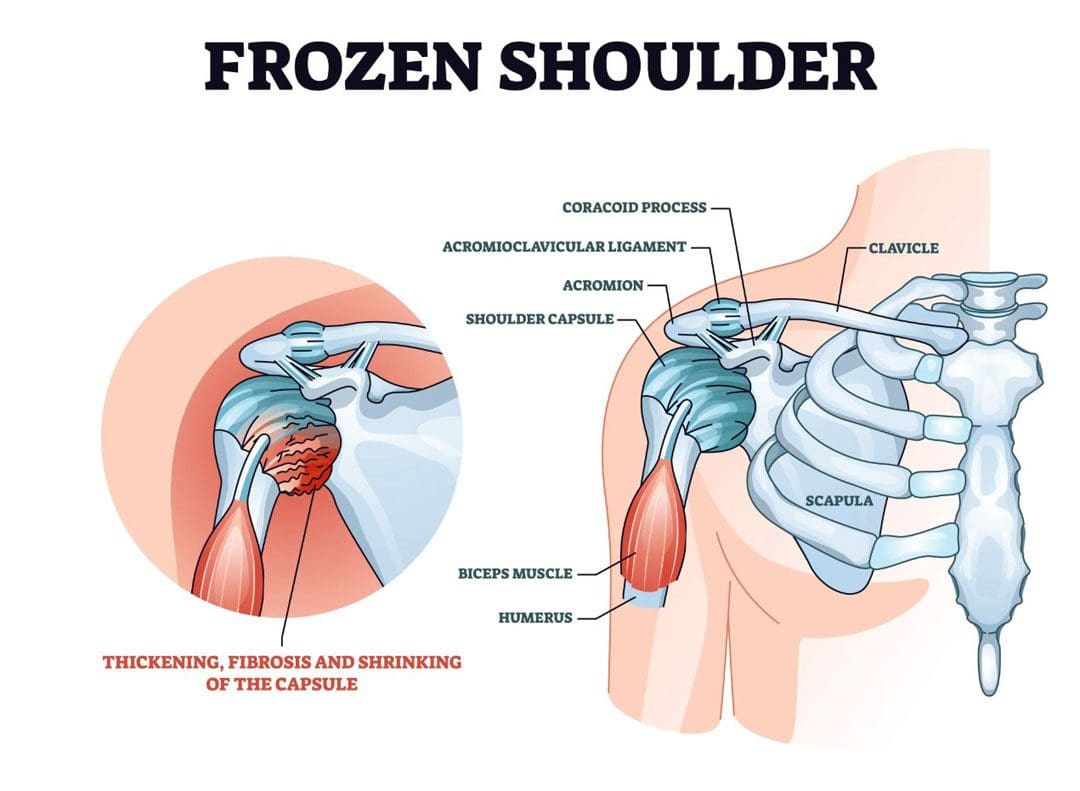
For individuals with shoulder pain and problems, what are the stages of a frozen shoulder, how long do they last, and what can be done to relieve pain?
Frozen Shoulder Stages
A frozen shoulder, also called adhesive capsulitis, is a very common cause of shoulder pain. It causes severe pain and limited mobility. The condition progresses through stages and can take up to two years to resolve completely. The stages of frozen shoulder include pre-freezing, freezing, freezing, and thawing.
Stage 1
Pre-Freezing – 1 month to 3 months
Pre-freezing describes the earliest stage of a frozen shoulder. This is when individuals first start to notice pain in their shoulder. (Soussahn, S. et al., 2024) Many in this stage will first experience the pain at night while changing sleeping positions. As the condition progresses, individuals may notice pain when they move their shoulders, especially when raising their arms or reaching behind them. Individuals may also find reduced mobility in that shoulder and may ache even when not using it. Because motion may be only slightly restricted in this stage, an early frozen shoulder can be mistaken for a rotator cuff problem. (Chan H. B. Y., Pua P. Y., & How C. H. 2017)
Root Cause
A frozen shoulder happens when there is inflammation in the tissue that surrounds the shoulder joint. Although the specific causes aren’t known, immobilization after an injury and other shoulder conditions, like bursitis, may play a role. (Johns Hopkins Medicine, 2025)
Stage 2
Freezing – 10 weeks to 8 months
The freezing stage is the most painful. The shoulder capsule becomes inflamed and can thicken and stiffen. As this happens, shoulder movements become increasingly difficult and painful. (Soussahn, S. et al., 2024)
Stage 3
Frozen – 4 months to 12 months
The third stage of a frozen shoulder is known as the frozen phase, where the shoulder is stiff. The examination finding confirming the frozen shoulder diagnosis is that neither the individual nor another person can move the shoulder. (UpToDate, 2024) With a rotator cuff issue, a patient cannot move their arm normally, but the healthcare provider can. This distinguishes between a frozen shoulder and a rotator cuff injury. The frozen stage is typically much less painful than freezing, but pain can result from simple activities. (Soussahn, S. et al., 2024) Rotation of the shoulder joint is limited, making activities like washing hair or reaching painful or difficult.
Stage 4
Thawing – 5 months to 2 years
In this phase, the shoulder joint capsule becomes thickened and stiff but gradually loosens with time. (Soussahn, S. et al., 2024) Stretching the shoulder capsule, even allowing for some discomfort, is important to ensure the shoulder joint’s mobility continues to recover. Not having the extreme pain associated with freezing the joint and seeing gradual gains in mobility make this stage tolerable.
Treatment
Frozen shoulder treatment starts with physical therapy and joint stretching. Anti-inflammatory medications, ice and heat application, and alternative therapies can all help manage the discomfort. A healthcare provider may also recommend a corticosteroid injection to reduce inflammation, relieve pain, and expedite improved mobility. Redler L. H. & Dennis E. R. 2019)
Surgery is seldom needed but is an option for treating a frozen shoulder. It is usually only considered if prolonged efforts at therapy have failed to improve symptoms. One of the problems is that surgery could worsen shoulder problems. (Le H. V., Lee S. J., Nazarian A., & Rodriguez E. K. 2017)
Prognosis
The timeline for recovery can be long, measured in months and possibly years. (Le H. V., Lee S. J., Nazarian A., & Rodriguez E. K. 2017) Expecting a quick recovery can cause more frustration. However, individuals can take steps to speed their recovery and reduce discomfort. Physical therapy can be beneficial, and a healthcare provider can suggest treatments to help alleviate pain while recovering. Over time, almost all patients will find complete relief and a normal or near-normal range of motion in their shoulder joints.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Motion Key To Healing
References
Soussahn, S., Hu, D., Durieux, J., Kosmas, C., & Faraji, N. (2024). Adhesive capsulitis: Utility of magnetic resonance imaging as a primary diagnostic tool and clinical management support. Current problems in diagnostic radiology, 53(4), 464–469. https://doi.org/10.1067/j.cpradiol.2024.03.005
Chan, H. B. Y., Pua, P. Y., & How, C. H. (2017). Physical therapy in the management of frozen shoulder. Singapore Medical Journal, 58(12), 685–689. https://doi.org/10.11622/smedj.2017107
UpToDate. (2024). Patient education: Frozen shoulder (beyond the basics). https://www.uptodate.com/contents/frozen-shoulder-beyond-the-basics
Redler, L. H., & Dennis, E. R. (2019). Treatment of Adhesive Capsulitis of the Shoulder. The Journal of the American Academy of Orthopaedic Surgeons, 27(12), e544–e554. https://doi.org/10.5435/JAAOS-D-17-00606
Le, H. V., Lee, S. J., Nazarian, A., & Rodriguez, E. K. (2017). Adhesive capsulitis of the shoulder: review of pathophysiology and current clinical treatments. Shoulder & elbow, 9(2), 75–84. https://doi.org/10.1177/1758573216676786
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 Digital Pulleys
Digital Pulleys