Detecting Hidden Traumatic Brain Injury: How Chiropractors and Nurse Practitioners Work Together for Better Recovery
Patient answers the doctor’s traumatic brain injury questions.
Traumatic brain injuries (TBIs) affect millions each year, often in ways that are hard to spot right away. These injuries happen from falls, car crashes, sports hits, or other sudden jolts to the head or body. While severe cases show clear signs like unconsciousness or seizures, milder ones can hide in plain sight. This can lead to ongoing problems with thinking, feelings, and daily life if not caught early. Healthcare providers like chiropractors and nurse practitioners play key roles in spotting these hidden signs through careful talks with patients. By asking the right questions, they uncover subtle clues that point to brain damage.
An integrative approach combines chiropractic adjustments with nurse-led medical care. This team effort targets both the body’s frame and the brain’s wiring, helping people heal better after a TBI. Treatments include gentle spine work, muscle therapies, and custom exercises to fix imbalances and boost brain power. Nurse practitioners add layers of support for mood, energy, and overall health. Advanced tools help confirm diagnoses, starting from simple checks to high-tech scans. Missing a TBI is easy because symptoms mimic stress or fatigue, but thorough checks and treatments can change lives. This article dives into how to detect, treat, and recover from these “invisible” wounds.
The Sneaky Nature of Traumatic Brain Injuries
TBIs disrupt brain function through direct hits or shaking forces. Mild forms, like concussions, might seem minor at first but can linger. According to the Mayo Clinic, symptoms can start right after the injury or pop up days later (Mayo Clinic, 2023). This delay makes them tricky. For example, someone might walk away from a car accident feeling fine, only to struggle with focus at work weeks later. Without prompt care, these issues can worsen, leading to long-term changes in how a person thinks or feels.
The brain controls everything from movement to emotions, so damage shows up in varied ways. Physical signs include headaches that won’t quit or a constant feeling of tiredness. Cognitive hints involve forgetting simple things or zoning out during talks. Emotional shifts, like sudden anger bursts, strain relationships. Sensory changes, such as a weird metallic taste in food or a loss of smell, add to the puzzle. These aren’t always dramatic, which is why they’re often ignored. Friends or family might notice first, saying, “You’ve been off since the fall.” Early spotting is vital because the brain can rewire itself if helped soon (Hauger et al., 2024).
Statistics paint a stark picture: About 1.7 million TBIs occur yearly in the U.S., with many going undiagnosed (Reis, 2022). Military personnel and athletes face higher risks, but anyone can be hit. Children and older adults show unique signs, such as kids losing interest in play or elders stumbling more often. The key? Listen to the body’s quiet signals. Untreated TBIs raise the chances of depression, job loss, or even repeat injuries. But with awareness, recovery paths open up.
Spotting Hidden Signs: A Step-by-Step Guide for Providers
Chiropractors and nurse practitioners are on the front lines for catching TBIs. They start with a deep dive into the patient’s story. This isn’t a quick chat—it’s a series of targeted questions to peel back layers. For instance, a chiropractor might ask, “Have you noticed foods tasting off, or smells fading since your accident?” This uncovers sensory shifts linked to brain areas involved in taste and smell (Fisher Stark, P.C., n.d.). Such details often slip past standard checkups.
A thorough history covers the injury event, immediate aftermath, and ongoing quirks. Questions probe cognitive slips: “Do tasks that used to take 10 minutes now drag on for hours?” This flags concentration woes common in TBIs (BrainLine, 2023). Emotional probes include, “Have small frustrations sparked big anger lately?” Irritability or mood swings signal disrupted emotional centers (U.S. Air Force, 2017). Balance checks ask, “Do you feel wobbly in crowds or after standing quickly?” These point to coordination hits.
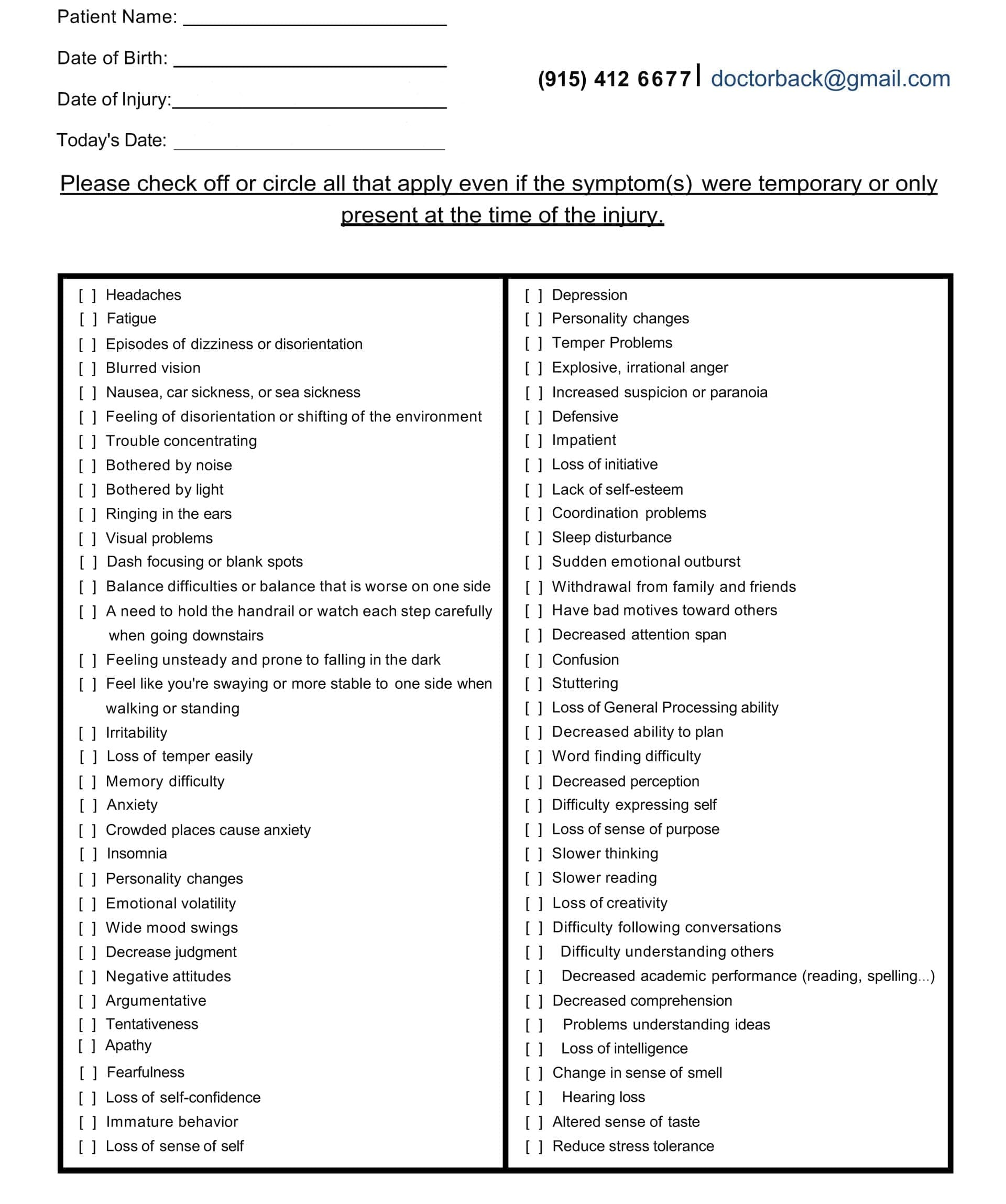
Symptom questionnaire:
Nurse practitioners layer in health checks, asking about sleep: “Are you crashing early but waking foggy?” Disturbed rest is a red flag (Mayo Clinic, 2023). Fatigue questions follow: “Does everyday stuff leave you wiped out?” Together, these inquiries build a full picture. Dr. Alexander Jimenez, a chiropractor and nurse practitioner, stresses personalized histories in his practice. He notes that linking subtle symptoms to past traumas helps tailor care, drawing from his work in integrative injury recovery (Jimenez, n.d.a). By cross-checking answers, providers spot patterns missed in rushed visits.
This method shines in real cases. One patient described headaches as “just stress,” but questions revealed post-accident timing, leading to TBI confirmation (Denver Chiropractic, LLC, n.d.). Multiple angles—physical, mental, sensory—ensure nothing hides. It’s simple yet powerful: Listen actively, ask openly, and connect dots.
Nuanced Symptoms: What to Watch For
TBI signs aren’t always obvious; they whisper through daily life. Cognitive disturbances top the list. Trouble focusing might mean rereading the same page over and over or missing deadlines. Memory lapses, like forgetting recent chats, disrupt routines (BrainLine, 2023). These stem from damaged brain pathways handling attention and recall.
Emotional turbulence follows closely. Anger flares over minor things, or flat moods replace joy. Depression creeps in, with unexplained sadness (U.S. Air Force, 2017). Loved ones often spot this first, as the injured person might downplay it. Dr. Jimenez observes in his clinic that these shifts strain families, urging early emotional screens (Jimenez, n.d.b).
Sensory oddities add intrigue. Taste changes turn meals bland or metallic; smells vanish, making cooking a chore (Fisher Stark, P.C., n.d.). Vision blurs, or lights sting eyes. These links to brain regions processing senses are hit hard by jolts.
Physical clues include relentless headaches, pulsing behind the eyes. Fatigue hits like a wall, even after rest. Sleep goes haywire—too much or too little, with nightmares or insomnia (Mayo Clinic, 2023). Balance falters, turning walks into teeters; coordination slips, fumbling keys or tripping.
In kids, signs differ: cranky spells, play changes, or nap shifts (BrainLine, 2023). Elders might show confusion mimicking dementia. These nuances demand vigilance. As one source notes, symptoms overlap with those of stress, delaying help-seeking (Reis, 2022). Recognizing them early prevents cascades, like poor sleep fueling more fatigue.
Building an Integrative Recovery Team
Recovery thrives on teamwork. Chiropractic care fixes body mechanics, while nurse practitioners oversee whole-body health. This blend heals the brain’s hardware and software. Spinal tweaks ease nerve pressure, boosting signals to damaged areas (Northwest Florida Physicians Group, LLC, n.d.). Nurses handle meds, nutrition, and mood support, creating balance.
Dr. Jimenez embodies this, merging his DC and APRN roles for seamless care. His clinic uses functional assessments to link spine health to brain function, echoing collaborative models (Jimenez, n.d.a). Studies back this: Teams reduce recovery time by addressing root causes (Holden et al., 2010).
Chiropractic Tools for Brain and Body Healing
Chiropractors target the spine-brain link. Adjustments realign vertebrae, improving fluid flow and nerve flow (Pinnacle Health Chiropractic, 2023). This cuts headaches and fog. Soft-tissue work kneads tight muscles, easing tension from impacts (Calibration Mansfield, n.d.).
Targeted exercises build strength and balance. Simple drills, like ball tosses, retrain coordination (HML Functional Care, n.d.). Vestibular therapies steady dizziness. Low-level lasers reduce swelling, aiding neuron repair (Reis, 2022).
Benefits stack: Better circulation delivers oxygen to the brain; balanced nerves sharpen focus (Apex Chiropractic, n.d.). One case saw a survivor return to EMT work after such care (Reis, 2022). It’s drug-free, focusing on the body’s own fixes.
Nurse Practitioners: Holistic Health Guardians
Nurses round out the plan with metabolic and emotional aid. They monitor blood sugar and electrolytes, preventing crashes that slow healing (Kim et al., 2024). Nutrition plans help fight inflammation, a key factor in TBI recovery.
Mental support includes therapy referrals and family coaching. Sedation eases agitation; family visits calm nerves (Kim et al., 2024). Dr. Jimenez integrates this, using coaching for stress and hormones (Jimenez, n.d.b). This full-spectrum care lifts mood, energy, and resilience.
Diagnostic Tools: From Basics to High-Tech
Diagnosis starts simple, scaling with needs. Basic tools include the Glasgow Coma Scale (GCS), scoring eye, verbal, and motor responses for quick severity checks (Mayo Clinic, 2023). Vital signs track blood pressure and heart rate, spotting brain pressure rises.
Next, CT scans image bleeds or swells—fast for emergencies (Mayo Clinic, 2023). MRIs detail soft tissue damage, revealing axon tears invisible on CT.
Advanced options: EEGs catch hidden seizures via brain waves (Kim et al., 2024). Neuropsychological tests probe memory and focus. Functional MRIs map active brain areas; diffusion tensor imaging traces nerve paths (HML Functional Care, n.d.).
Eye-tracking tools like RightEye assess gaze for subtle deficits (Calibration Mansfield, n.d.). Blood tests measure biomarkers for the extent of damage. Order matters: Basics rule out crises; advanced confirm and guide plans.
Why TBIs Slip Through Cracks—and How to Fix It
Traumatic Brain Injuries (TBIs) often go unnoticed because their symptoms can be mistaken for everyday life stresses. A headache? Blame work. Irritability? “Bad day.” This oversight delays care, worsening outcomes (BrainLine, 2023). Providers miss them without deep histories, as one study shows that up to 50% of mild cases go undiagnosed (Reis, 2022).
Meticulous evaluation changes this. Multi-question intakes and team huddles catch clues. Treatment urgency: Early adjustments prevent scarring; holistic plans build lasting gains. Paula’s story proves it— from bedbound to marathon training via integrated care (Reis, 2022).
In military settings, recognition cuts long-term woes (U.S. Air Force, 2017). For all, it means reclaiming life. Push for thorough checks; the brain deserves it.
Holden, C. Q., et al. (2010). Chiropractors and collaborative care: An overview illustrated with a case report. Chiropractic & Osteopathy, 18(21). https://doi.org/10.1186/1746-1340-18-21
Kim, J., et al. (2024). Nursing interventions to prevent secondary injury in critically ill patients with traumatic brain injury: A scoping review. Journal of Clinical Medicine, 13(8), 2396. https://doi.org/10.3390/jcm13082396
Chiropractic & Manual Therapies. (2018). Be good, communicate, and collaborate: A qualitative analysis of stakeholder perspectives on adding a chiropractor to the multidisciplinary rehabilitation team. Chiropractic & Manual Therapies, 26(17). https://doi.org/10.1186/s12998-018-0200-4
Overcoming Sciatic Nerve Pain: Expert Insights from El Paso Back Clinic® in El Paso, TX
At El Paso Back Clinic®, located in the heart of El Paso, Texas, we specialize in helping people get back to their active lives without the constant burden of pain. Led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, our team combines chiropractic care with modern wellness strategies to treat conditions like sciatic nerve issues. Whether you’re dealing with sharp leg pain from a work injury or numbness after a car accident, our clinic offers personalized plans to ease your symptoms and promote long-term health. We focus on non-invasive methods that address the root causes, not just the signs. If you’re in El Paso and searching for effective sciatica relief, our integrated approach could be the key to feeling better.
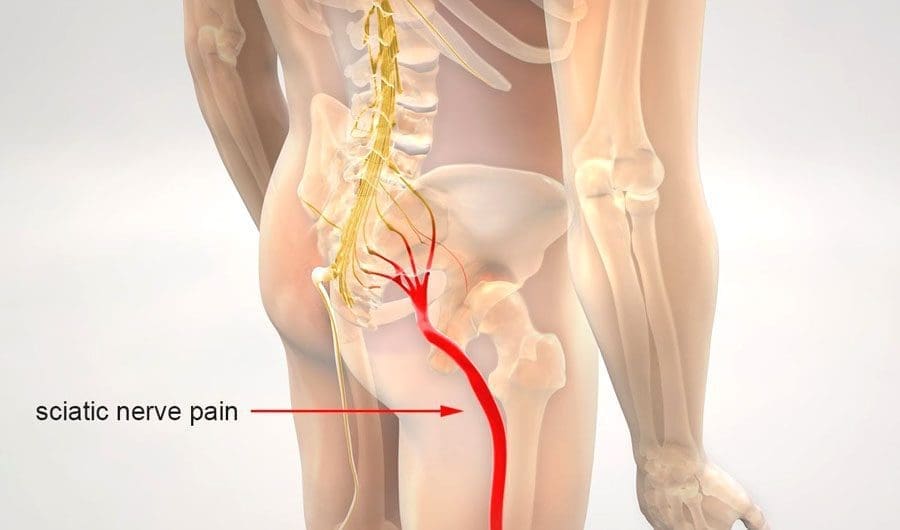
Sciatica isn’t just a back problem—it’s a nerve issue that can disrupt your daily routine. The sciatic nerve, which is like a thick cable running from your lower spine down each leg, gets irritated or squeezed, causing discomfort that travels far. At our clinic, we’ve seen how this affects everyone from athletes to office workers. In this guide, we’ll dive into what sciatica really is, why it happens, and how our team at El Paso Back Clinic® uses proven techniques to help. We’ll cover the physical side of nerve damage, common triggers, signs to watch for, and recovery steps. Plus, we’ll share how our chiropractic integrative care stands out in treating these issues right here in El Paso.
The Basics of the Sciatic Nerve and How Pressure Affects It
The sciatic nerve is your body’s main pathway for signals between the brain and legs. It begins at the lower back, where several nerve roots join, then branches through the buttocks and down to the feet. This nerve handles movement in your hamstrings, calves, and feet, as well as sensation in those areas. When something, like a slipped disk or tight muscle, presses on it, problems start.
When the sciatic nerve is compressed, pinched, or crushed, it suffers physical damage that disrupts its ability to transmit signals, leading to pain, numbness, and muscle weakness. The severity of the physical changes depends on the nature and duration of the pressure. Inside the nerve, axons carry messages, protected by myelin sheaths for fast travel. Pressure squishes these, causing swelling and blocking blood flow, which starves cells of oxygen—a state called ischemia (Verywell Health, 2023). In mild squeezes, like poor posture, the myelin gets worn but regrows. But harder crushes break axons, triggering degeneration where the nerve falls apart below the spot (Menorca et al., 2013).
Think of it like a garden hose: a light kink slows water, but a stomp cuts it off. Short pressure might cause temporary numbness, but ongoing force leads to scarring and chronic issues. At El Paso Back Clinic®, we use advanced checks to spot these changes early, helping prevent lasting harm.
Recognizing the Signs of Sciatic Nerve Trouble
Sciatica shows up in ways that can sneak up on you. The classic sign is radiating pain—starting in the lower back and zipping down one leg like an electric shock. It might burn, tingle, or feel sharp, worse when you sit, stand, or sneeze (Penn Medicine, n.d.). Numbness follows, making parts of your leg feel asleep or prickly. Weakness hits muscles, causing limps or trouble with stairs (Align Wellness Center, n.d.).
In our El Paso clinic, patients often describe it as a “leg giving out” or a constant ache. Severe cases bring muscle shrinking or even bladder issues if nerves are badly pinched (ADR Spine, n.d.). We see this in folks from all walks—drivers with long hauls, athletes pushing limits, or those in desk jobs. Early signs? Pay attention to one-sided pain that doesn’t fade with rest.
What Causes Sciatic Nerve Compression in Everyday Life
Life in El Paso means active days, but that can lead to sciatica triggers. A herniated disk, where the cushy part bulges and presses on the spinal cord roots, is common from lifting heavy boxes at work (Mayo Clinic, 2023). Aging narrows the spine in stenosis, squeezing nerves (Physio Pretoria, n.d.). Tight piriformis muscles in the butt can pinch the sciatic nerve, too, especially in runners or cyclists.
Accidents amp it up—car crashes crush nerves directly (MedStar Health, n.d.). Bone growths from arthritis add pressure, and extra weight strains everything (Advanced Orthopaedics & Sports Medicine, n.d.). Double crush? That’s when two spots squeeze, such as the back and leg, worsening the condition (Southwest Regional Wound Care Center, n.d.). At our clinic, we trace these in locals from border commutes to sports fields.
How We Diagnose Sciatica at El Paso Back Clinic®
Getting the right diagnosis is step one to relief. At our El Paso locations, we start with a full chat about your history—when the pain started and what makes it worse. Then, during hands-on exams, we test reflexes, strength, and perform the leg raise to pinpoint nerve irritation (Penn Medicine, n.d.).
We use top tools like MRI for disk views, EMG for signal checks, and X-rays for bones (ICliniq, 2023). Dr. Jimenez’s dual training as a chiropractor and nurse practitioner allows for a dual-scope diagnosis—blending medical tests with chiropractic insights for a full picture (Jimenez, n.d.). This helps link injuries to symptoms accurately, especially in complex cases from MVAs or sports.
Physical Damage from Compression: A Closer Look
Diving deeper, compression physically alters the nerve. Mild pressure causes neurapraxia: myelin dents, slowing signals without axon breaks. You feel weak but recover fast (Menorca et al., 2013). Stronger pinches lead to axonotmesis: axons snap, walls degenerate, and swelling builds. Healing takes time as new growth crawls along (Horton Mendez, n.d.).
Crushes bring neurotmesis: full sever, with scars blocking regrowth (Bhatia, 2023). Pressure cuts off blood, causing ischemia and cell death (Verywell Health, 2023). Chronic? Fibrosis hardens tissue (Mackinnon, 1998). Our clinic spots these via imaging, guiding treatments to reduce pressure and aid repair.
Integrative Chiropractic Care: Our Approach at El Paso Back Clinic®
We believe in whole-body healing. Our chiropractic integrative care combines spinal adjustments, soft tissue work, and exercises to correct alignment, enhance muscle function, and improve nerve signals. Adjustments ease pressure on the sciatic nerve, while massage loosens tight spots (AMTA, n.d.). Rehab builds strength to prevent repeats (Byington, n.d.).
This holistic method tackles pain now and builds stability for tomorrow. We add nutrition and stress tips, as gut health and emotions affect recovery. For El Paso folks, it’s about getting back to hikes or family time pain-free.
Dr. Alexander Jimenez’s Clinical Observations and Clinic Breakdown
With over 30 years, Dr. Jimenez brings unique insights. His dual credentials allow clinical correlations: linking injuries to assessments via advanced imaging like MRI for neuromusculoskeletal views (LinkedIn, n.d.). We treat work strains, sports sprains, personal slips, and MVAs with tailored plans.
Our process: Dual-scope diagnosis merges chiropractic and medical for thorough checks. Treatments include adjustments, non-surgical decompression, acupuncture, and functional medicine. We handle legal documents for accident claims, ensuring smooth care (Jimenez, n.d.). Observations? Stress worsens posture, and gut issues slow healing—we address all.
Recovery and Prevention Tips from Our El Paso Team
Recovery varies: Mild cases heal in weeks with rest and therapy, while severe cases require months (ADR Spine, n.d.). We guide with exercises, avoiding surgery when possible.
Prevent? Good posture, regular moves, and weight control. At our clinic, we teach these in sessions.
In El Paso, sciatica doesn’t have to hold you back. El Paso Back Clinic® offers expert, local care to restore your life.
Your Spine, Your Life: An El Paso-Ready Guide to Strong, Flexible, Pain-Resistant Backs
A young woman is performing a spine checkup at a vertebra clinic.
What “spinal health” means (and why it matters here in El Paso)
Spinal health refers to the proper structure, alignment, and function of the spine, enabling it to support the body, facilitate movement, and protect the spinal cord—the pathway for nerve signals between the brain and the body. Good spinal health comes from regular exercise, posture awareness, a nutrient-dense diet, steady hydration, and a healthy weight. Poor spinal health can lead to chronic pain, nerve irritation or damage, and a lower quality of life (Raleigh Orthopaedics, 2024; Orthopedic Specialists of Southwest Florida [OSSWF], 2024; National Spine Health Foundation, 2024).
How a healthy spine supports your whole body
Support & alignment: Your spine acts like a central pillar that shares load with the hips and legs and keeps you upright (Premier Spine & Sports Medicine, n.d.).
Movement & shock absorption: Curves, discs, and joints allow for safe bending and twisting, enabling you to lift, reach, and play (Raleigh Orthopaedics, 2024).
Nerve protection: The spinal column shields the spinal cord and nerve roots, so signals move clearly. Irritation can cause pain, tingling, or weakness (Cary Orthopaedics, 2023).
Quality of life: Ongoing spine issues can lead to fatigue, poor sleep, headaches, and reduced participation in work or sports (Raleigh Orthopaedics, 2024).
Common problems we see—and why early action helps
Strains/sprains and facet irritation from long sitting, poor lifting form, or sudden loads
Disc problems that can press on nearby nerves and create radiating symptoms
Spinal stenosis (narrowing) that pinches nerves
Degenerative changes related to age, low activity, smoking, or extra weight
Most cases respond to conservative care when initiated early, including movement, postural changes, targeted exercises, and load management (OSSWF, 2024).
Red flags—don’t wait: radiating pain, numbness, weakness, headaches, or loss of function. Seek a prompt exam (Cary Orthopaedics, 2023; Suarez Physical Therapy, n.d.).
An El Paso Back Clinic–style plan: simple steps that fit your day
1) Movement you can keep
20–30 minutes of low-impact cardio most days (e.g., walking, cycling, swimming).
Core & hip strength 2–3 days/week: planks, side planks, glute bridges, and bird-dogs.
Mobility after warm-ups: thoracic open-books, hip-flexor, and hamstring stretches (National Spine Health Foundation, 2024; Mobility Project PT, 2024).
2) Posture that holds up at work and home
Sit: feet flat, hips back in the chair, lumbar support, screen at eye level.
Stand: weight balanced, knees soft, ears over shoulders.
Micro-breaks: move every 30–45 minutes (National Spine Health Foundation, 2024).
3) Ergonomics you actually feel
The chair is high enough so the hips are level with or slightly above the knees.
Keyboard and mouse close; forearms supported; shoulders relaxed.
Lift with a hip hinge, keep the load close, and exhale as you stand.
4) Sleep & stress recovery
Neutral neck/back with a supportive mattress and the right pillow height.
Side sleepers: pillow between knees. Back sleepers: pillow under knees.
Use breathing drills, short walks, and stretch breaks to lower tension (Raleigh Orthopaedics, 2024).
5) Hydration & healthy weight
Steady water intake supports disc hydration and tissue recovery (Centeno-Schultz Clinic, n.d.).
A healthy body weight lowers compressive load on joints and discs (Raleigh Orthopaedics, 2024).
Nutrition for a stronger spine (simple and local-friendly)
Protein for muscle and connective-tissue repair
Omega-3s (salmon, trout, walnuts) to help regulate inflammation
Calcium & vitamin D for bone strength
Magnesium for nerve and muscle function
Colorful fruits/vegetables for antioxidants that support recovery
Water for disc hydration and nutrient transport These habits reduce inflammation and support healing (Watkins Family Chiropractic, 2023; OSSWF, 2024).
Four-week “Borderland Back Reset” (minimal gear, steady progress)
Week 1 — Start easy
Daily: 10-minute walk + 5 minutes mobility (open-books, hip-flexor, hamstrings).
Core set (3x/week): plank 20 s, side plank 15 s/side, glute bridge 10 reps.
Posture: Raise the screen and add a small lumbar roll.
Week 2 — Build consistency
Daily: 15–20 minutes walk/cycle + mobility.
Core set (3x/week): plank 25–30 s, side plank 20 s/side, bridge 12 reps; add bird-dog 6/side.
Nutrition: add one serving of leafy greens and one serving of lean protein to each meal (Watkins Family Chiropractic, 2023).
Week 3 — Strength + recovery
Cardio most days: 20–25 minutes.
Light hinge pattern (backpack or kettlebell) 1–2 days/week; focus on form.
Before bed, do slow breathing for 5 minutes.
Week 4 — Re-test & adjust
Compare flexibility, pain, and energy levels with those of Week 1.
Keep what helps; trim what doesn’t.
If numbness, weakness, or radiating pain persists, book an exam (Cary Orthopaedics, 2023; Suarez Physical Therapy, n.d.).
Real-world injuries: work, sports, and motor-vehicle accidents (MVAs)
Work: Desk roles need posture breaks and lumbar support; physical jobs need task rotation, hip-hinge training, and planned recovery.
Sports: Combine mobility, core/hip strength, and gradual return to play.
MVAs: Even “minor” collisions can cause whiplash or soft-tissue injury. A stepwise evaluation, along with imaging when necessary, guides safe return and documentation (OSSWF, 2024).
Inside our integrative approach in El Paso
(Clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC, Nurse Practitioner and Chiropractor)
Dual-scope diagnosis: We blend chiropractic and medical perspectives. Your exam includes a detailed history, movement, and neurological screens, as well as, when necessary, advanced imaging to clarify the problem and rule out potential red flags (Jimenez, n.d.; see Imaging/Diagnostics and Personal-Injury topics).
Evidence-based conservative care:
Chiropractic adjustments to restore motion and reduce joint irritation
Therapeutic exercise to build core/hip strength and mobility
Manual therapy/massage for tight or sensitive tissues
Acupuncture as part of an integrative plan when appropriate
Lifestyle coaching on posture, lifting, sleep, and stress (Prestige Health & Wellness, n.d.; Mobility Project PT, 2024; Raleigh Orthopaedics, 2024)
Documentation & advocacy: For work, sports, personal, and MVA cases, we document the mechanism of injury, exam findings, functional limits, and response to care. When claims or legal issues arise, clear records and appropriate imaging support decision-making (Jimenez, n.d.; Rangeline Chiropractic, n.d.).
Myths vs. facts (short and clear)
Myth: “If my back hurts, I should rest all day.” Fact: Gentle movement and short walks often speed recovery; long bed rest adds stiffness (National Spine Health Foundation, 2024).
Myth: “Only heavy lifting causes back pain.” Fact: Prolonged sitting, poor ergonomics, stress, and sleep problems also drive pain (National Spine Health Foundation, 2024; Raleigh Orthopaedics, 2024).
The El Paso Back Clinic checklist
☐ Break up sitting every 30–45 minutes
☐ Screen at eye level; use lumbar support
☐ 10–15 minutes daily core + mobility
☐ 20–30 minutes low-impact cardio most days
☐ Hydrate across the day
☐ Build meals around protein + produce + healthy fats
☐ Sleep with neutral neck/back alignment
☐ Seek care quickly for red flags or lasting symptoms
Strumming Without Pain: Chiropractic Solutions for Guitarists and Bassists at El Paso Back Clinic
Playing guitar or bass fills life with rhythm and joy. The thrill of strumming chords or plucking deep notes creates unforgettable moments. But for many string players in El Paso, Texas, this passion can lead to pain. Hours of practice can strain hands, wrists, forearms, elbows, and shoulders, leading to repetitive strain injuries (RSIs) such as tendonitis. These injuries bring swelling, stiffness, and aches that make playing tough. At El Paso Back Clinic, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, we offer integrative chiropractic care to tackle these issues, helping musicians heal naturally and keep the music alive.
This article explains why guitarists and bassists are prone to RSIs, how tendonitis affects key areas, and how our clinic’s holistic approach—combining chiropractic adjustments, massage, acupuncture, and nutrition—restores health. With insights from Dr. Jimenez’s 30+ years of expertise, we’ll show how El Paso Back Clinic helps local musicians recover from injuries and prevent future pain, so they can strum and pluck without worry.
Why String Players Face Repetitive Strain Injuries
Guitarists and bassists repeat the same motions for hours: fretting chords, strumming strings, or plucking heavy bass lines. These actions stress tendons—the tough bands connecting muscles to bones. Over time, small tears form, which can lead to inflammation or tendonitis. Unlike a one-time injury, RSIs develop gradually from overuse, making them common among musicians (Pianucci et al., 2021).
The fretting hand curls tightly to press strings, while the strumming or plucking arm moves fast. Bassists face extra strain from thicker strings that need more force. Poor posture, like slouching over a guitar, adds pressure to the shoulders and neck. Heavy instruments—guitars at 7-10 pounds and basses up to 12—strain the body more during gigs (Pain Free NY, n.d.). Cold El Paso nights or long jam sessions at local venues like Lowbrow Palace can worsen symptoms by stiffening muscles.
Other factors increase risks. Older players over 40 have less flexible tendons (Bend Total Body Chiropractic, n.d.). Poor habits, such as gripping picks too hard or skipping warm-ups, can speed up strain. Diet matters too—sugary or fatty foods fuel inflammation, slowing recovery (Healthline, 2022). El Paso’s active music scene, with frequent gigs and rehearsals, means local players often push their limits, increasing the risk of RSI.
Where It Hurts: Tendonitis in Musicians’ Bodies
Tendonitis hits specific spots based on how guitarists and bassists play. Here’s where pain strikes:
Hands and Fingers: Fretting chords strains finger tendons, especially at the thumb base. Thumb tendonitis (De Quervain’s) causes sharp pain when gripping the neck. Swelling or a gritty feel signals trouble (Guitar Strength Project, n.d.).
Wrists: Strumming and plucking bend wrists repeatedly, inflaming tendons on top (extensor) or below (flexor). Stiffness after waking or a weak grip are signs. Carpal tunnel syndrome may add tingling or numbness (Rawlogy, n.d.).
Forearms: Constant flexing causes the forearm muscles to burn. Redness, warmth, or lumps show tendonitis. Bassists feel it more from forceful plucks (Healthline, 2022).
Elbows: “Guitar elbow” mimics tennis elbow, with pain on the outer elbow from strained tendons. Inner elbow pain (golfer’s elbow) also hits. Both weaken grip, making it hard to hold picks or instruments (Tennis Elbow Classroom, n.d.).
Shoulders: Holding arms out for chords strains the rotator cuff tendons, causing aches that spread down the arm. Slouching worsens it (Smithsonian Folkways, n.d.).
These areas link up. Hand pain can trigger elbow issues, and shoulder misalignment can strain wrists. Catching early signs—such as soreness or fatigue—prevents more severe problems.
Symptoms That Stop the Show
Tendonitis symptoms creep in but hit hard. Pain starts as a dull ache during play, then sharpens at rest. Swelling puffs up joints, and stiffness locks fingers, especially in the morning. Numbness or tingling buzzes in cold venues, sometimes with fingers turning blue from poor blood flow (Pain Free NY, n.d.). Weakness, drops, and fatigue, as well as burning or throbbing sensations, often linger after gigs. A grating sensation hints at the presence of scar tissue.
For El Paso musicians, long practices for gigs at Tricky Falls or house shows can exacerbate symptoms. Stress from late-night sets or cold weather can cause muscles to tighten, exacerbating pain. If symptoms last for weeks, it’s time to visit El Paso Back Clinic for expert care.
Quick Relief at Home
Before professional help, try these steps to ease tendonitis:
RICE Method: Rest by avoiding play and using splints. Ice for 15 minutes, wrapped, several times daily. Compress with elastic wraps, not too tight. Elevate arms on pillows (Mayo Clinic, 2023).
Meds: Ibuprofen reduces swelling, but ask a doctor first.
Stretches: Gentle wrist circles, finger spreads, or forearm pulls, held 15-30 seconds (Healthline, 2022).
Massage: Use massage balls to roll out knots gently (Rawlogy, n.d.).
Diet: Eat berries, fish, and leafy greens to help combat inflammation. Avoid sugary snacks common at El Paso food trucks.
These help, but don’t address the root cause. For lasting relief, see the experts at El Paso Back Clinic.
Chiropractic Care at El Paso Back Clinic
At El Paso Back Clinic, Dr. Alexander Jimenez and his team utilize chiropractic care to effectively treat RSIs. Adjustments realign joints in the wrist, elbow, or shoulder, freeing nerves and boosting blood flow. For elbow tendonitis, specific adjustments reduce pain and swelling, with patients often regaining full motion in weeks (Stamford Spine, n.d.).
Our clinic checks the whole body. A misaligned shoulder can strain wrists, so we adjust the entire chain. Soft tissue work, such as Graston therapy, breaks down scar tissue in the wrists. Laser therapy reduces inflammation, and taping supports joints during physical activity (Pinnacle Hill Chiropractic, 2024). Regular visits help keep the body aligned, reducing the risk of re-injury by up to 50% (Chiro One, n.d.).
Dr. Jimenez’s dual training as a chiropractor and nurse practitioner ensures precise diagnosis and treatment. Using advanced imaging like MRIs, we pinpoint tendon tears or nerve issues. Treatments are safe, with only mild soreness possible, and tailored to each musician’s needs (Bend Total Body Chiropractic, n.d.).
Integrative Healing for El Paso Musicians
Our integrative approach goes beyond adjustments. We combine:
Massage Therapy: Kneads forearm knots, easing tension from long sets (Beech Street Health, n.d.).
Acupuncture: Calms nerves, reducing wrist tingling for smoother playing.
Exercises: Wrist curls with light weights or finger bands build strength (Chiro One, n.d.).
Nutrition: Collagen supplements and omega-3 fatty acids accelerate tendon repair. We guide patients to local El Paso markets for healthy foods.
Ergonomics: Adjust guitar straps or use lighter picks. Take breaks every 20 minutes during practice (Smithsonian Folkways, n.d.).
This mix helps heal faster and prevents future pain, allowing musicians to stay on stage.
Dr. Jimenez’s Expertise at El Paso Back Clinic
Dr. Alexander Jimenez brings over 30 years of experience to El Paso Back Clinic. His dual-scope approach—combining chiropractic and functional medicine—targets the root causes of injuries. We provide personalized plans for musicians, workers, athletes, and individuals who have experienced accidents. Advanced tools, such as neuromusculoskeletal imaging, can reveal hidden damage, while assessments also consider lifestyle and genetics (Jimenez, n.d.a).
For a local guitarist who was injured in a car accident, we utilized adjustments, massage, and nutrition to restore their fretting ability. Our clinic also handles legal documentation for injury claims, ensuring smooth insurance processes (Jimenez, n.d.b). From whiplash to wrist strain, we help El Paso’s music community heal naturally.
Preventing Pain for Lifelong Playing
Prevention keeps musicians playing. Try these:
Exercises: Wrist stretches, towel twists, or 1-pound weight curls, 10 reps, three times weekly (Healthline, 2022).
Warm-Ups: 10-minute finger flexes and arm circles before gigs.
Technique: Use loose grips and neutral wrists. Alternate hands for songs (No Treble, 2011).
Gear: Ergonomic straps and lighter instruments ease shoulder strain.
Breaks: Rest every 20 minutes. Relax with meditation to cut stress.
El Paso Back Clinic offers tailored plans to keep your body gig-ready.
Keep the Music Playing
Tendonitis doesn’t have to silence your strings. At El Paso Back Clinic, Dr. Jimenez and our team use chiropractic and integrative care to heal RSIs and prevent pain. From hands to shoulders, we address the root causes so you can play without fear. Visit us in El Paso to get back to strumming and plucking with ease.
Contact El Paso Back Clinic at 915-850-0900 or dralexjimenez.com to schedule your consultation today.
What is a bone density test, how is it performed, and what do the results mean?
Bone Density Test
A bone density test examines bone mass, which indicates overall bone strength. Assessing bone density or mass is necessary for diagnosing osteopenia or osteoporosis, conditions that increase the risk of broken bones. The scan is performed through dual-energy X-ray absorptiometry (DEXA), which examines the thickness of the bones. Results from DEXA scans are compared to standardized values to determine whether bone density is lower than normal and whether osteopenia or osteoporosis is present.
Examination
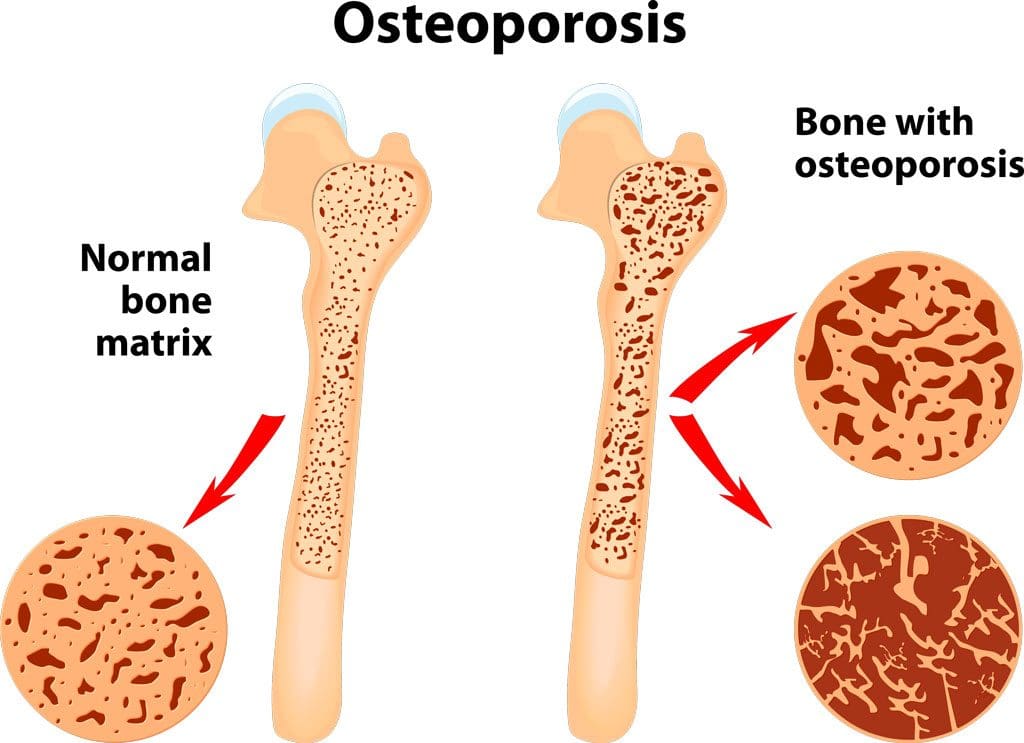
The procedure examines bone density, or bone mass. The bones’ density, or mass, is an overall indicator of bone strength. The greater the bone density, the thicker and stronger the bones are. The test is used to diagnose osteoporosis, a condition characterized by brittle bones at risk of breaking due to significantly low bone density. A bone density test can also diagnose osteopenia, a condition characterized by lower than normal bone mass that can lead to osteoporosis. (National Institute of Arthritis and Musculoskeletal and Skin Diseases, 2025) It is recommended that all women aged 65 and older and all men aged 70 and older have a bone density scan to screen for bone loss to help prevent fractures. (Kling J. M., Clarke B. L., & Sandhu N. P. 2014)
Bone density scans can establish a baseline level of bone density and track changes over time.
For individuals with osteoporosis or osteopenia, a bone density scan can help track how well their bones respond to treatment.
During a DEXA scan, the patient will lie on their back on a table with their legs elevated on a padded platform.
An X-ray scanner will pass over the spine and hips while another scans beneath.
While the scan takes place, the patient will be asked to hold very still to obtain an accurate image.
The scan will obtain bone density readings from the spine and hip, the two most commonly fractured bones, and generally takes less than 30 minutes.
Results
A DEXA scan measures bone density in grams per centimeter squared (g/cm²). This number indicates how densely bone cells are packed together in a specific area of bone. This bone density reading is then compared to a standardized value to determine if bone density is within a normal range or lower than average.
Between minus 1.0 and minus 2.5: Low bone density (osteopenia)
Equal to minus 2.5 or below: Osteoporosis
Bone density values are reported as a Z score for women who have not undergone menopause and men under 50 years old.
Z scores are compared to bone density levels of individuals of the same age and sex.
A Z score of minus 2.0 or lower indicates low bone density, which can be caused by factors other than aging, such as medication side effects, nutritional deficiencies, or thyroid problems.
Arthritis Diagnosis
Because a DEXA scan only measures the thickness of bones, it doesn’t work to diagnose arthritis. An X-ray of the affected joint is currently the most accurate way to diagnose arthritis. The Kellgren-Lawrence classification system categorizes the extent of arthritis based on the severity of joint damage seen on an X-ray. According to this system, arthritis can be classified as: (Kohn M. D., Sassoon A. A., & Fernando N. D. 2016)
Grade 1 (minor)
Minimal or no joint space narrowing, with possible bone spur formation.
Grade 2 (mild)
Possible joint space narrowing, with definite bone spur formation.
Grade 3 (moderate)
Definite joint space narrowing, moderate bone spur formation, mild sclerosis (abnormal thickening of bone), and possible deformation of bone ends.
Grade 4 (severe)
Severe joint space narrowing, large bone spur formation, marked sclerosis, and definite deformation of bone ends.
Injury Medical Chiropractic & Functional Medicine Clinic
Exercise can be incredibly beneficial for improving bone density, joint mobility, and the strength of surrounding muscles, which support and protect joints and bones. Talk to a healthcare provider to learn what interventions and available treatment options would be the most effective. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Osteoporosis
References
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2025). Bone mineral density tests: what the numbers mean. Retrieved from https://www.niams.nih.gov/health-topics/bone-mineral-density-tests-what-numbers-mean
Kling, J. M., Clarke, B. L., & Sandhu, N. P. (2014). Osteoporosis prevention, screening, and treatment: a review. Journal of women’s health (2002), 23(7), 563–572. https://doi.org/10.1089/jwh.2013.4611
Kohn, M. D., Sassoon, A. A., & Fernando, N. D. (2016). Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clinical orthopaedics and related research, 474(8), 1886–1893. https://doi.org/10.1007/s11999-016-4732-4
How are MRIs used to help diagnose bulging and herniated discs and help healthcare providers develop effective treatment programs for individuals experiencing back pain symptoms?
Herniated Bulging Disc MRI
A herniated bulging disc is often identified during magnetic resonance imaging (MRI); however, it’s usually an incidental finding that was done for other reasons where spinal problems and/or injuries are found. A bulging disc is relatively common, even in individuals who experience no symptoms. A herniated or bulging disc in the back can be identified with an MRI test, typically recommended when someone experiences back pain symptoms for at least six weeks. (American Academy of Neurological Surgeons, 2024) Normal wear and tear and age cause changes in the spinal disc/s cushion to bulge and become misaligned with the spine. (Brinjikji W. et al., 2015) And with a herniated disc, it can press against the spinal cord and nerves. Repeated heavy lifting, practicing unhealthy postures, a history of back injuries, or underlying health conditions are common causes.
Bulging Disc
Bulging discs are common even in healthy individuals but can be difficult to interpret independently on an MRI, so other symptoms and findings are as important in diagnosis.
Causes
A bulging disc is usually considered age-related degenerative changes that cause the disc to bulge downward with gravity. (Penn Medicine, 2018)
A significant bulge is expected to cause leg pain due to irritation to the nerves going down the legs. (Amin R. M., Andrade N. S., & Neuman B. J. 2017) As the condition progresses, more than one disc can be affected, leading to other spinal conditions, including spinal stenosis.
A Bulging Disc On MRI
A disc bulge will measure over 25% of the total disc circumference. Its displacement is usually 3 millimeters or less from the normal shape and position of the disc. (Radiopaedia, 2024)
Herniated Disc
A herniated disc shifts out of its correct position and compresses nearby spinal nerves, causing pain and mobility issues.
Herniated discs will measure less than 25% of the total disc circumference. However, herniation is based on the type and can include: (Wei B., & Wu H. 2023)
Disc Protrusion – the displacement is limited, and the ligaments are intact.
Disc Extrusion – part of the disc remains connected but has slipped through the annulus or outer covering of the disc.
Disc Sequestration – a free fragment has separated and broken off from the main disc.
Candidates For Spinal MRI
The MRI is generally safe for most, including those with implanted cardiac devices like newer-model pacemakers. (Bhuva A. N. et al., 2020) However, it’s important to ensure that the healthcare team is aware of cochlear implants or other devices so that necessary precautions can be taken. It is recommended for all individuals that symptoms be present for six weeks before an MRI. A specialist may want to see MRI results sooner, especially if symptoms include: (American Academy of Neurological Surgeons, 2024)
A specific injury, like a fall that caused the pain
Recent or current infection or fever with spinal symptoms
Significant weakness in arms or legs
Loss of pelvic sensation.
A history of metastatic cancer.
Loss of bladder or bowel control
An MRI may be needed if symptoms are rapidly worsening. However, many with a disc bulge don’t have symptoms at all. In most cases, an MRI is an outpatient procedure that can be completed in an hour or less but can take longer if contrast dye is used. The healthcare provider will provide specific instructions about MRI preparation.
Treatment
Treatment for a herniated or bulging disc depends on the cause and severity of symptoms.
Over-the-counter pain relief, including nonsteroidal anti-inflammatory drugs (NSAIDs).
Physical therapy
In rare cases that have not resolved with conservative treatment, surgery may be recommended.
Remember that the MRI findings may not identify or rule out all conditions, including muscle strains or ligament injuries, which may require different treatments, such as targeted stretches and exercises. (Brinjikji W. et al., 2015) (Fujii K. et al., 2019)
Herniated Disc
Treatment depends on the cause and severity of symptoms, if any. It can include stand-alone or a combination of physical therapy, medication, and steroid injections. Cases usually resolve in six to 12 weeks (Penn Medicine, 2018). Electrical nerve stimulation may be performed through specialized devices and/or acupuncture to help with nerve compression. (National Institute of Neurological Disorders and Stroke, 2020) Surgery may be recommended if conservative treatments fail to achieve significant pain relief and healing. (Wang S. et al., 2023)
Injury Medical Chiropractic and Functional Medicine Clinic
A healthcare provider can discuss treatment options such as pain medication, physical therapy, and surgery. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Root Causes of Spinal Stenosis
References
American Academy of Neurological Surgeons. (2024). Herniated disc. https://www.aans.org/patients/conditions-treatments/herniated-disc/
Brinjikji, W., Diehn, F. E., Jarvik, J. G., Carr, C. M., Kallmes, D. F., Murad, M. H., & Luetmer, P. H. (2015). MRI Findings of Disc Degeneration are More Prevalent in Adults with Low Back Pain than in Asymptomatic Controls: A Systematic Review and Meta-Analysis. AJNR. American journal of neuroradiology, 36(12), 2394–2399. https://doi.org/10.3174/ajnr.A4498
Penn Medicine. (2018). Bulging Disc vs. Herniated Disc: What’s The Difference? Penn Musculoskeletal and Rheumatology Blog. https://www.pennmedicine.org/updates/blogs/musculoskeletal-and-rheumatology/2018/november/bulging-disc-vs-herniated-disc
Wu, P. H., Kim, H. S., & Jang, I. T. (2020). Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. International journal of molecular sciences, 21(6), 2135. https://doi.org/10.3390/ijms21062135
Amin, R. M., Andrade, N. S., & Neuman, B. J. (2017). Lumbar Disc Herniation. Current reviews in musculoskeletal medicine, 10(4), 507–516. https://doi.org/10.1007/s12178-017-9441-4
American Academy of Orthopaedic Surgeons. (2022). Herniated disk in the lower back. https://orthoinfo.aaos.org/en/diseases–conditions/herniated-disk-in-the-lower-back/
Wei, B., & Wu, H. (2023). Study of the Distribution of Lumbar Modic Changes in Patients with Low Back Pain and Correlation with Lumbar Degeneration Diseases. Journal of pain research, 16, 3725–3733. https://doi.org/10.2147/JPR.S430792
Bhuva, A. N., Moralee, R., Moon, J. C., & Manisty, C. H. (2020). Making MRI available for patients with cardiac implantable electronic devices: growing need and barriers to change. European radiology, 30(3), 1378–1384. https://doi.org/10.1007/s00330-019-06449-5
Brinjikji, W., Luetmer, P. H., Comstock, B., Bresnahan, B. W., Chen, L. E., Deyo, R. A., Halabi, S., Turner, J. A., Avins, A. L., James, K., Wald, J. T., Kallmes, D. F., & Jarvik, J. G. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR. American journal of neuroradiology, 36(4), 811–816. https://doi.org/10.3174/ajnr.A4173
Fujii, K., Yamazaki, M., Kang, J. D., Risbud, M. V., Cho, S. K., Qureshi, S. A., Hecht, A. C., & Iatridis, J. C. (2019). Discogenic Back Pain: Literature Review of Definition, Diagnosis, and Treatment. JBMR plus, 3(5), e10180. https://doi.org/10.1002/jbm4.10180
Wang, S., Zhao, T., Han, D., Zhou, X., Wang, Y., Zhao, F., Shi, J., & Shi, G. (2023). Classification of cervical disc herniation myelopathy or radiculopathy: a magnetic resonance imaging-based analysis. Quantitative imaging in medicine and surgery, 13(8), 4984–4994. https://doi.org/10.21037/qims-22-1387
National Institute of Neurological Disorders and Stroke. (2020). Low back pain fact sheet. Retrieved from https://www.ninds.nih.gov/sites/default/files/migrate-documents/low_back_pain_20-ns-5161_march_2020_508c.pdf
How do healthcare professionals in a chiropractic clinic provide a clinical approach to preventing medical errors for individuals in pain?
Introduction
Medical errors resulted in 44,000–98,000 hospitalized American deaths annually, and many more caused catastrophic injuries. (Kohn et al., 2000) This was more than the number of people who died annually from AIDS, breast cancer, and auto accidents at the time. According to later research, the actual number of deaths may be closer to 400,000, placing medical errors as the third most common cause of death in the US. Frequently, these mistakes are not the product of medical professionals who are inherently bad; rather, they are the outcome of systemic issues with the health care system, such as inconsistent provider practice patterns, disjointed insurance networks, underutilization or absence of safety protocols, and uncoordinated care. Today’s article looks at the clinical approach to preventing a medical error in a clinical setting. We discuss associated medical providers specializing in various pretreatments to aid individuals suffering from chronic issues. We also guide our patients by allowing them to ask their associated medical providers very important and intricate questions. Dr. Alex Jimenez, DC, only utilizes this information as an educational service. Disclaimer
Defining Medical Errors
Determining what medical error is the most crucial step in any conversation about preventing medical errors. You might assume this is a very easy chore, but that is only until you delve into the vast array of terminology utilized. Many terms are used synonymously (sometimes mistakenly) since some terminology is interchangeable, and occasionally, the meaning of a term depends on the specialty being discussed.
Even though the healthcare sector stated that patient safety and eliminating or reducing medical errors were priorities, Grober and Bohnen noted as recently as 2005 that they had fallen short in one crucial area: determining the definition of “perhaps the most fundamental question… What is a medical error? A medical error is a failure to complete a planned action in a medical setting. (Grober & Bohnen, 2005) However, none of the terms that one would often identify expressly with a medical error—patients, healthcare, or any other element—are mentioned in this description. Despite this, the definition offers a solid framework for further development. As you can see, that specific definition consists of two parts:
An execution error: A failure to complete a planned action as intended.
A planning error: is a technique that, even with perfect execution, does not produce the desired results.
The concepts of faults of execution and planning errors are insufficient if we are to define a medical error adequately. These may occur anywhere, not only at a medical establishment. The component of medical management must be added. This brings up the idea of unfavorable occurrences, known as adverse events. The most common definition of an adverse event is unintentional harm to patients brought about by medical therapy rather than their underlying disease. This definition has gained international acceptance in one way or another. For example, in Australia, the term incidents are defined as in which harm resulted in a person receiving health care. These consist of infections, injury-causing falls, and issues with prescription drugs and medical equipment. Certain unfavorable occurrences might be avoidable.
Common Types of Medical Errors
The only issue with this notion is that not all negative things happen accidentally or intentionally. Because the patient may ultimately benefit, an expected but tolerated adverse event may occur. During chemotherapy, nausea and hair loss are two examples. In this instance, refusing the recommended treatment would be the only sensible approach to prevent the unpleasant consequence. We thus arrive at the concept of preventable and non-preventable adverse occurrences as we further refine our definition. It isn’t easy to categorize a choice to tolerate one impact when it is determined that a favorable effect will occur simultaneously. But purpose alone isn’t necessarily an excuse. (Patient Safety Network, 2016, para.3) Another example of a planned mistake would be a right foot amputation due to a tumor on the left hand, which would be accepting a known and predicted unfavorable event in the hopes of a beneficial consequence where none has ever arisen before. There is no evidence to support the anticipation of a positive outcome.
Medical errors that cause harm to the patient are typically the focus of our research. Nonetheless, medical mistakes can and do occur when a patient is not harmed. The occurrence of near misses could provide invaluable data when planning how to reduce medical errors in a healthcare facility. Still, the frequency of these events compared to the frequency clinicians report them needs to be investigated. Near misses are medical errors that could have caused harm but did not to the patient, even if the patient is doing well. (Martinez et al., 2017) Why would you acknowledge something that could potentially result in legal action? Consider the scenario where a nurse, for whatever reason, had just been looking at photographs of different medications and was about to provide a medication. Maybe something lingers in her memory, and she decides that’s not how a specific medication looks. Upon checking, she found that the incorrect medicines had been administered. After checking all the paperwork, she fixes the mistake and gives the patient the right prescription. Would it be possible to avoid an error in the future if the administration record included photographs of the proper medication? It is easy to forget that there was a mistake and a chance for harm. That fact remains true regardless of whether we were fortunate enough to find it in time or suffer any negative consequences.
Errors of Outcomes & Process
We need complete data to develop solutions that improve patient safety and decrease medical errors. At the very least, when the patient is in a medical facility, everything that can be done to prevent harm and put them in danger should be reported. Many doctors have determined that using the phrases errors and adverse events was more comprehensive and suitable after reviewing mistakes and adverse events in health care and discussing their strengths and weaknesses in 2003. This combined definition would increase data gathering, including mistakes, close calls, near misses, andactive and latent errors. Additionally, the term adverse events includes terms that usually imply patient harm, such as medical injury and iatrogenic injury. The only thing that remains is determining whether a review board is a suitable body to handle the separation of preventable and non-preventable adverse events.
A sentinel event is an occurrence where reporting to the Joint Commission is required. The Joint Commission states that a sentinel event is an unexpected occurrence involving a serious physical or psychological injury. (“Sentinel Events,” 2004, p.35) There isn’t a choice, as it needs to be documented. Most healthcare facilities, however, do keep their records outlining sentinel incidents and what to do in the event of one to guarantee that the Joint Commission standards are met. This is one of those situations when it’s better to be safe than sorry. Since “serious” is a relative concept, there may be some wriggle room when defending a coworker or an employer. On the other hand, reporting a sentinel event incorrectly is better than failing to report a sentinel event. Failing to disclose can have serious consequences, including career termination.
When considering medical errors, people frequently make the mistake of focusing just on prescription errors. Medication errors are undoubtedly frequent and involve many of the same procedural flaws as other medical errors. Breakdowns in communication, mistakes made during prescription or dispensing, and many other things are possible. But we would be gravely misjudging the issue if we assumed that drug errors are the only cause of harm to a patient. One major challenge in classifying the different medical errors is determining whether to classify the error based on the procedure involved or the consequence. It is acceptable to examine those classifications here, given numerous attempts have been made to develop working definitions that incorporate both the process and the outcome, many of which are based on Lucian Leape’s work from the 1990s.
Enhance Your Lifestyle Today- Video
Analyzing & Preventing Medical Errors
Operative and nonoperative were the two main categories of adverse events that Leape and his colleagues distinguished in this study. (Leape et al., 1991) Operative problems included wound infections, surgical failures, non-technical issues, late complications, and technical difficulties. Nonoperative: headings such as medication-related, misdiagnosed, mistreated, procedure-related, fall, fracture, postpartum, anesthesia-related, neonatal, and a catch-all heading of the system were included under this category of adverse occurrences. Leape also classified errors by pointing out the point of process breakdown. He also categorized these into five headings, which include:
System
Performance
Drug Treatment
Diagnostic
Preventative
Many process faults fall under more than one topic, yet they all help to pinpoint the exact cause of the issue. If more than one physician was engaged in determining the precise areas that need improvement, then additional questioning might be required.
Technically, a medical error can be made by any staff member at a hospital. It is not limited to medical professionals like physicians and nurses. An administrator may unlatch a door, or a cleaning crew member could leave a chemical within a child’s grasp. What matters more than the identity of the perpetrator of the mistake is the reason behind it. What before it? And how can we make sure that doesn’t occur again? After gathering all the above data and much more, it’s time to figure out how to prevent similar errors. As for sentinel events, the Joint Commission has mandated since 1997 that all of these incidents undergo a procedure called Root Cause Analysis (RCA). However, using this procedure for incidents that need to be reported to outside parties would need to be corrected.
What Is A Root Cause Analysis?
RCAs “captured the details as well as the big picture perspective.” They make evaluating systems easier, analyzing whether remedial action is necessary, and tracking trends. (Williams, 2001) What precisely is an RCA, though? By examining the events that led to the error, an RCA can focus on events and processes rather than reviewing or placing blame on specific people. (AHRQ,2017) This is why it is so crucial. An RCA frequently makes use of a tool called the Five Whys. This is the process of continuously asking yourself “why” after you believe you have determined the cause of an issue.
The reason it’s called the “five whys” is because, while five is an excellent starting point, you should always question why until you identify the underlying cause of the problem. Asking why repeatedly could reveal many process faults at different stages, but you should keep asking why about every aspect of the issue until you run out of other things that could be adjusted to provide a desirable result. However, different tools besides this one can be utilized in a root cause investigation. Numerous others exist. RCAs must be multidisciplinary and consistent and involve all parties involved in the error to avoid misunderstandings or inaccurate reporting of occurrences.
Conclusion
Medical errors in healthcare institutions are frequent and mostly unreported events that seriously threaten patients’ health. Up to a quarter of a million individuals are thought to pass away each year as a result of medical blunders. These statistics are unacceptable in a time when patient safety is supposedly the top priority, but not much is being done to alter practices. If medical errors are accurately defined and the root cause of the problem is found without assigning blame to specific staff members, this is unnecessary. Essential changes can be made when fundamental causes of system or process faults are correctly identified. A consistent, multidisciplinary approach to root cause analysis that uses frameworks like the five whys to delve down until all issues and defects are revealed is a helpful tool. Although it is now necessary for the wake of sentinel events, the Root Cause Analysis may and should be applied to all mistake causes, including near misses.
Kohn, L. T., Corrigan, J., Donaldson, M. S., & Institute of Medicine (U.S.). Committee on Quality of Health Care in America. (2000). To err is human : building a safer health system. National Academy Press. http://books.nap.edu/books/0309068371/html/index.html
Leape, L. L., Brennan, T. A., Laird, N., Lawthers, A. G., Localio, A. R., Barnes, B. A., Hebert, L., Newhouse, J. P., Weiler, P. C., & Hiatt, H. (1991). The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med, 324(6), 377-384. https://doi.org/10.1056/NEJM199102073240605
Martinez, W., Lehmann, L. S., Hu, Y. Y., Desai, S. P., & Shapiro, J. (2017). Processes for Identifying and Reviewing Adverse Events and Near Misses at an Academic Medical Center. Jt Comm J Qual Patient Saf, 43(1), 5-15. https://doi.org/10.1016/j.jcjq.2016.11.001
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine