Fasting is associated with numerous health benefits; from weight loss to longevity. There are many different types of fasting methods, such as intermittent fasting. The fasting mimicking diet allows you to experience the benefits of traditional fasting without depriving your body of food. The main difference of the FMD is that instead of completely eliminating all food for several days or even weeks, you only restrict your calorie intake for five days out of the month. The FMD can be practiced once a month to promote well-being.
While anyone can follow the FMD on their own, the ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled for each day and it serves the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The purpose of the research study below is to demonstrate the molecular mechanisms and clinical applications of fasting in the FMD.
Fasting: Molecular Mechanisms and Clinical Applications
Fasting has been practiced for millennia, but only recently studies have shed light on its role in adaptive cellular responses that reduce oxidative damage and inflammation, optimize energy metabolism and bolster cellular protection. In lower eukaryotes, chronic fasting extends longevity in part by reprogramming metabolic and stress resistance pathways. In rodents intermittent or periodic fasting protects against diabetes, cancers, heart disease and neurodegeneration, while in humans it helps reduce obesity, hypertension, asthma and rheumatoid arthritis. Thus, fasting has the potential to delay aging and help prevent and treat diseases while minimizing the side effects caused by chronic dietary interventions.
Introduction
In humans, fasting is achieved by ingesting no or minimal amounts of food and caloric beverages for periods that typically range from 12 hours to three weeks. Many religious groups incorporate periods of fasting into their rituals including Muslims who fast from dawn until dusk during the month of Ramadan, and Christians, Jews, Buddhists and Hindus who traditionally fast on designated days of the week or calendar year. In many clinics, patients are now monitored by physicians while undergoing water only or very low calorie (less than 200 kcal/day) fasting periods lasting from 1 week or longer for weight management, and for disease prevention and treatment. Fasting is distinct from caloric restriction (CR) in which the daily caloric intake is reduced chronically by 20�40%, but meal frequency is maintained. Starvation is instead a chronic nutritional insufficiency that is commonly used as a substitute for the word fasting, particularly in lower eukaryotes, but that is also used to define extreme forms of fasting, which can result in degeneration and death. We now know that fasting results in ketogenesis, promotes potent changes in metabolic pathways and cellular processes such as stress resistance, lipolysis and autophagy, and can have medical applications that in some cases are as effective as those of approved drugs such as the dampening of seizures and seizure-associated brain damage and the amelioration of rheumatoid arthritis (Bruce-Keller et al., 1999; Hartman et al., 2012; Muller et al., 2001). As detailed in the remainder of this article, findings from well-controlled investigations in experimental animals, and emerging findings from human studies, indicate that different forms of fasting may provide effective strategies to reduce weight, delay aging, and optimize health. Here we review the fascinating and potent effects of different forms of fasting including intermittent fasting (IF, including alternate day fasting, or twice weekly fasting, for example) and periodic fasting (PF) lasting several days or longer every 2 or more weeks. We focus on fasting and minimize the discussion of CR, a topic reviewed elsewhere (Fontana et al., 2010; Masoro, 2005).
Lessons from Simple Organisms
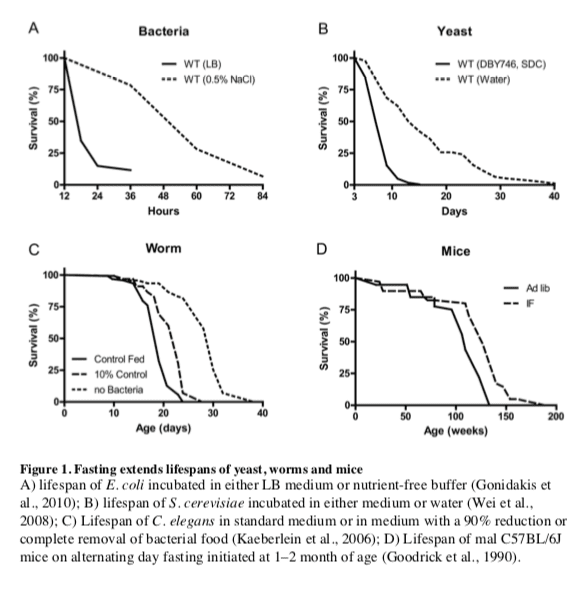
The remarkable effects of the typical 20�40% CR on aging and diseases in mice and rats are often viewed as responses evolved in mammals to adapt to periods of limited availability of food (Fontana and Klein, 2007; Fontana et al., 2010; Masoro, 2005; Weindruch and Walford, 1988). However, the cellular and molecular mechanisms responsible for the protective effects of CR have likely evolved billions of years earlier in prokaryotes attempting to survive in an environment largely or completely devoid of energy sources while avoiding age-dependent damage that could compromise fitness. In fact, E. coli switched from a nutrient rich broth to a calorie-free medium survive 4 times longer, an effect reversed by the addition of various nutrients but not acetate, a carbon source associated with starvation conditions (Figure 1A) (Gonidakis et al., 2010). The effect of rich medium but not acetate in reducing longevity raises the possibility that a ketone body-like carbon source such as acetate may be part of an �alternate metabolic program� that evolved billions of years ago in microorganisms and that now allows mammals to survive during periods of food deprivation by obtaining much of the energy by catabolizing fatty acids and ketone bodies including acetoacetate and ?-hydroxybutyrate (Cahill, 2006).
In the yeast S. cerevisiae, switching cells from standard growth medium to water also causes a consistent 2-fold chronological lifespan extension as well as a major increase in the resistance to multiple stresses (Figure 1B) (Longo et al., 1997; Longo et al., 2012). The mechanisms of food deprivation-dependent lifespan extension involve the down-regulation of the amino acid response Tor-S6K (Sch9) pathway as well as of the glucose responsive Ras-adenylate cyclase-PKA pathway resulting in the activation of the serine/threonine kinase Rim15, a key enzyme coordinating the protective responses (Fontana et al., 2010). The inactivation of Tor-S6K, Ras-AC-PKA and activation of Rim15 result in increased transcription of genes including superoxide dismutases and heat shock proteins controlled by stress responsive transcription factors Msn2, Msn4 and Gis1, required for the majority of the protective effects caused by food deprivation (Wei et al., 2008). Notably, when switched to food deprivation conditions, both bacteria and yeast enter a hypometabolic mode that allows them to minimize the use of reserve carbon sources and can also accumulate high levels of the ketone body-like acetic acid, analogously to mammals.
Another major model organism in which fasting extends lifespan is the nematode C. elegans. Food deprivation conditions achieved by feeding worms little or no bacteria, lead to a major increase in lifespan (Figure 1C) (Kaeberlein et al., 2006; Lee et al., 2006), which requires AMPK as well as the stress resistance transcription factor DAF-16, similarly to the role of transcription factors Msn2/4 and Gis1 in yeast and FOXOs in flies and mammals (Greer et al., 2007). Intermittent food deprivation also extends lifespan in C. elegans by a mechanism involving the small GTPase RHEB-1 (Honjoh et al., 2009).
In flies, most studies indicate that intermittent food deprivation does not affect lifespan (Grandison et al., 2009). However, food reduction or food dilution have been consistently shown to extend Drosophila longevity (Piper and Partridge, 2007) suggesting that flies can benefit from dietary restriction but may be sensitive to even short starvation periods.
Together these results indicate that food deprivation can result in pro-longevity effects in a wide variety of organisms, but also underline that different organisms have different responses to fasting.
Adaptive Responses to Fasting in Mammals
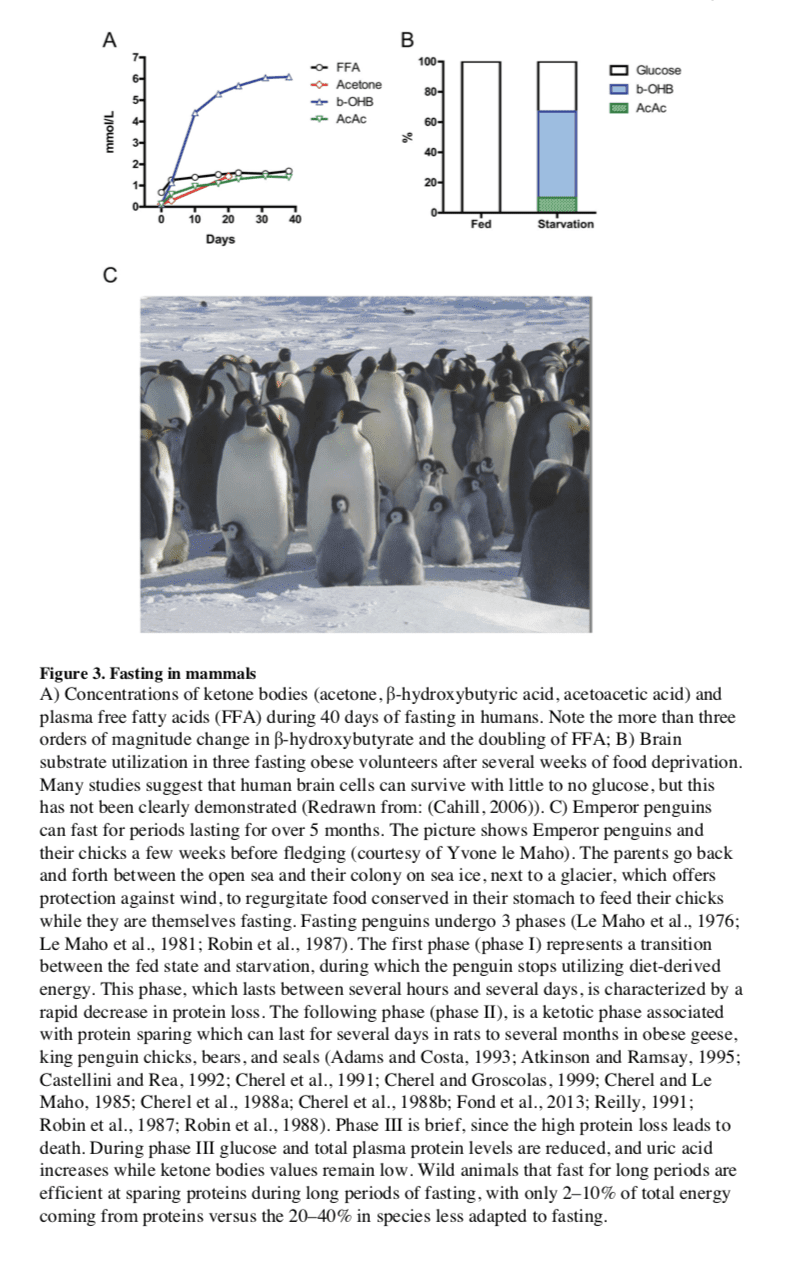
In most mammals, the liver serves as the main reservoir of glucose, which is stored in the form of glycogen. In humans, depending upon their level of physical activity, 12 to 24 hours of fasting typically results in a 20% or greater decrease in serum glucose and depletion of the hepatic glycogen, accompanied by a switch to a metabolic mode in which non-hepatic glucose, fat-derived ketone bodies and free fatty acids are used as energy sources (Figures 2 and 3). Whereas most tissues can utilize fatty acids for energy, during prolonged periods of fasting, the brain relies on the ketone bodies ?-hydroxybutyrate and acetoacetate in addition to glucose for energy consumption (Figure 3B). Ketone bodies are produced in hepatocytes from the acetyl-CoA generated from ? oxidation of fatty acids released into the bloodstream by adipocytes, and also by the conversion of ketogenic amino acids. After hepatic glycogen depletion, ketone bodies, fat-derived glycerol, and amino acids account for the gluconeogenesis-dependent generation of approximately 80 grams/day of glucose, which is mostly utilized by the brain. Depending on body weight and composition, the ketone bodies, free fatty acids and gluconeogenesis allow the majority of human beings to survive 30 or more days in the absence of any food and allow certain species, such as king penguins, to survive for over 5 months without food (Eichhorn et al., 2011) (Figure 3C). In humans, during prolonged fasting, the plasma levels of 3-?-hydroxybutyrate are about 5 times those of free fatty acids and acetoacetic acid (Figure 3A and 3B). The brain and other organs utilize ketone bodies in a process termed ketolysis, in which acetoacetic acid and 3-?- hydroxybutyrate are converted into acetoacetyl-CoA and then acetyl-CoA. These metabolic adaptations to fasting in mammals are reminiscent of those described earlier for E. coli and yeast, in which acetic acid accumulates in response to food deprivation (Gonidakis et al., 2010; Longo et al., 2012). In yeast, glucose, acetic acid and ethanol, but not glycerol which is also generated during fasting from the breakdown of fats, accelerate aging (Fabrizio et al., 2005; Wei et al., 2009). Thus, glycerol functions as a carbon source that does not activate the pro-aging nutrient signaling pathways but can be catabolized by cells. It will be important to understand how the different carbon sources generated during fasting affect cellular protection and aging. and to determine whether glycerol, specific ketone bodies or fatty acids can provide nourishment while reducing cellular aging in mammals, a possibility suggested by beneficial effects of a dietary ketone precursor in a mouse model of Alzheimer�s disease (Kashiwaya et al., 2012). It will also be important to study, in various model organisms and humans, how high intake of specific types of fats (medium- vs. long- chain fatty acids, etc.) in substitution of carbohydrates and proteins influences gluconeogenesis and glucose levels as well as aging and diseases.
Fasting and the Brain
In mammals, severe CR/food deprivation results in a decrease in the size of most organs except the brain, and the testicles in male mice (Weindruch and Sohal, 1997). From an evolutionary perspective this implies that maintenance of a high level of cognitive function under conditions of food scarcity is of preeminent importance. Indeed, a highly conserved behavioral trait of all mammals is to be active when hungry and sedentary when satiated. In rodents, alternating days of normal feeding and fasting (IF) can enhance brain function as indicated by improvements in performance on behavioral tests of sensory and motor function (Singh et al., 2012) and learning and memory (Fontan-Lozano et al., 2007). The behavioral responses to IF are associated with increased synaptic plasticity and increased production of new neurons from neural stem cells (Lee et al., 2002).
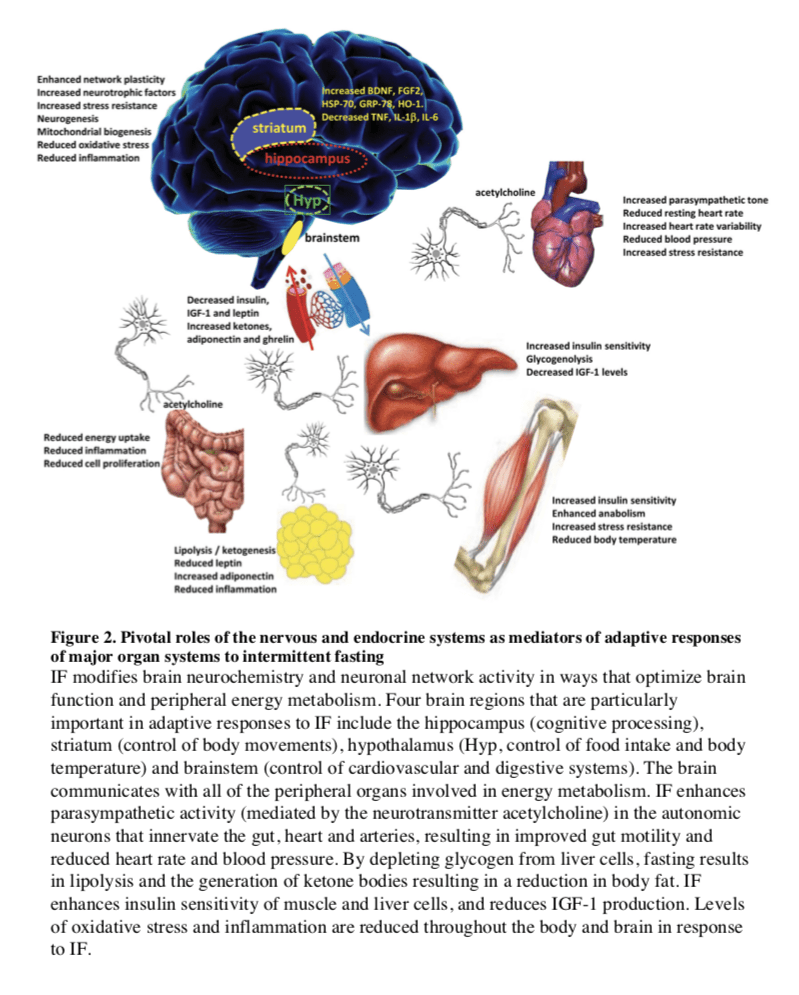
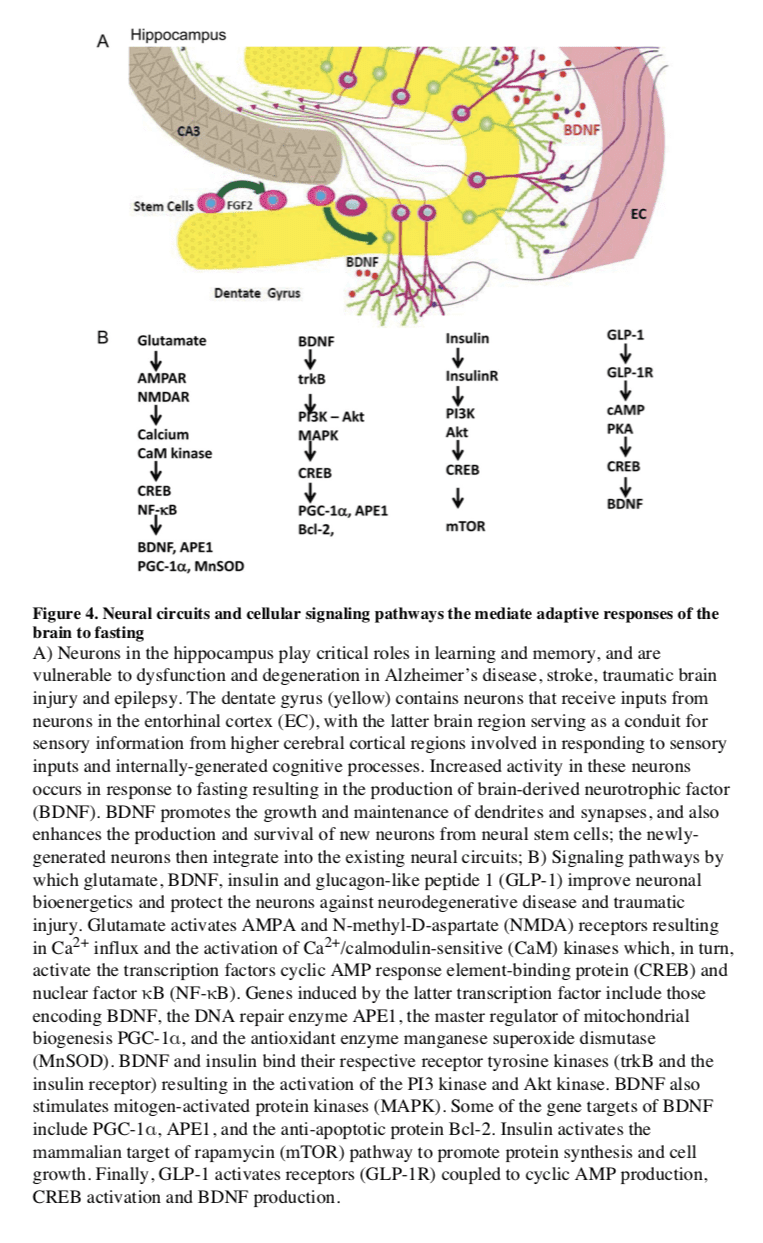
Particularly interesting with regards to adaptive responses of the brain to limited food availability during human evolution is brain-derived neurotrophic factor (BDNF). The genes encoding BDNF and its receptor TrkB appeared in genomes relatively recently as they are present in vertebrates, but absent from worms, flies and lower species (Chao, 2000). The prominent roles of BDNF in the regulation of energy intake and expenditure in mammals is highlighted by the fact that the receptors for both BDNF and insulin are coupled to the highly conserved PI3 kinase � Akt, and MAP kinase signaling pathways (Figure 4). Studies of rats and mice have shown that running wheel exercise and IF increase BDNF expression in several regions of the brain, and that BDNF in part mediates exercise- and IF-induced enhancement of synaptic plasticity, neurogenesis and neuronal resistance to injury and disease (see sections on fasting and neurodegeneration below). BDNF signaling in the brain may also mediate behavioral and metabolic responses to fasting and exercise including regulation of appetite, activity levels, peripheral glucose metabolism and autonomic control of the cardiovascular and gastrointestinal systems (Mattson, 2012a, b; Rothman et al., 2012).
Hunger is an adaptive response to food deprivation that involves sensory, cognitive and neuroendocrine changes which motivate and enable food seeking behaviors. It has been proposed that hunger-related neuronal networks, neuropeptides and hormones play pivotal roles in the beneficial effects of energy restriction on aging and disease susceptibility. As evidence, when mice in which the hypothalamic �hunger peptide� NPY is selectively ablated are maintained on a CR diet, the ability of CR to suppress tumor growth is abolished (Shi et al., 2012). The latter study further showed that the ability of CR to elevate circulating adiponectin levels was also compromised in NPY-deficient mice, suggesting a key role for the central hunger response in peripheral endocrine adaptations to energy restriction. Adiponectin levels increase dramatically in response to fasting; and data suggest roles for adiponectin in the beneficial effects of IF on the cardiovascular system (Wan et al., 2010). The hunger response may also improve immune function during aging as ghrelin-deficient mice exhibit accelerated thymic involution during aging, and treatment of middle age mice with ghrelin increases thymocyte numbers and improves the functional diversity of peripheral T cell subsets (Peng et al., 2012). In addition to its actions on the hypothalamus and peripheral endocrine cells, fasting may increase neuronal network activity in brain regions involved in cognition, resulting in the production of BDNF, enhanced synaptic plasticity and improved stress tolerance (Rothman et al., 2012). Thus, hunger may be a critical factor involved in widespread central and peripheral adaptive responses to the challenge of food deprivation for extended time periods.
Fasting, Aging, and Disease in Rodent Models
Different Fasting Methods and Aging
The major differences between IF and PF in mice are the length and the frequency of the fast cycles. IF cycles usually last 24 hours and are one to a few days apart, whereas PF cycles last 2 or more days and are at least 1 week apart, which is necessary for mice to regain their normal weight. One difference in the molecular changes caused by different fasting regimes is the effect on a variety of growth factors and metabolic markers, with IF causing more frequent but less pronounced changes than PF. It will be important to determine how the frequency of specific changes such as the lowering of IGF-1 and glucose affect cellular protection, diseases and longevity. The most extensively investigated IF method in animal studies of aging has been alternate day fasting (food is withdrawn for 24 hours on alternate days, with water provided ad libitum) (Varady and Hellerstein, 2007). The magnitude of the effects of alternate day fasting on longevity in rodents depends upon the species and age at regimen initiation, and can range from a negative effect to as much as an 80% lifespan extension (Arum et al., 2009; Goodrick et al., 1990). IF every other day extended the lifespan of rats more than fasting every 3rd or 4th day (Carlson and Hoelzel, 1946). Fasting for 24 hours twice weekly throughout adult life resulted in a significant increase in lifespan of black-hooded rats (Kendrick, 1973). In rats, the combination of alternate day fasting and treadmill exercise resulted in greater maintenance of muscle mass than did IF or exercise alone (Sakamoto and Grunewald, 1987). Interestingly, when rats were maintained for 10 weeks on a PF diet in which they fasted 3 consecutive days each week, they were less prone to hypoglycemia during 2 hours of strenuous swimming exercise as a result of their accumulation of larger intramuscular stores of glycogen and triglycerides (Favier and Koubi, 1988). Several major physiological responses to fasting are similar to those caused by regular aerobic exercise including increased insulin sensitivity and cellular stress resistance, reduced resting blood pressure and heart rate, and increased heart rate variability as a result of increased parasympathetic tone (Figure 2) (Anson et al., 2003; Mager et al., 2006; Wan et al., 2003). Emerging findings suggest that exercise and IF retard aging and some age-related diseases by shared mechanisms involving improved cellular stress adaptation (Stranahan and Mattson, 2012). However, in two different mouse genetic backgrounds, IF did not extend mean lifespan and even reduced lifespan when initiated at 10 months (Goodrick et al., 1990). When initiated at 1.5 months, IF either increased longevity or had no effect (Figure 1D) (Goodrick et al., 1990). These results in rodents point to conserved effects of fasting on lifespan, but also to the need for a much better understanding of the type of fasting that can maximize its longevity effects and the mechanisms responsible for the detrimental effects that may be counterbalancing its anti-aging effects. For example, one possibility is that fasting may be consistently protective in young and middle aged laboratory rodents that are either gaining or maintaining a body weight, but may be detrimental in older animals that, similarly to humans, begin to lose weight prior to their death. Notably, whereas bacteria, yeast and humans can survive for several weeks or more without nutrients, most strains of mice are unable to survive more than 3 days without food. The age-dependent weight loss may make this sensitivity to long periods of fasting worse.
Fasting and Cancer
Fasting can have positive effects in cancer prevention and treatment. In mice, alternate day fasting caused a major reduction in the incidence of lymphomas (Descamps et al., 2005) and fasting for 1 day per week delayed spontaneous tumorigenesis in p53-deficient mice (Berrigan et al., 2002). However, the major decrease in glucose, insulin and IGF-1 caused by fasting, which is accompanied by cell death and/or atrophy in a wide range of tissues and organs including the liver and kidneys, is followed by a period of abnormally high cellular proliferation in these tissues driven in part by the replenishment of growth factors during refeeding. When combined with carcinogens during refeeding, this increased proliferative activity can actually increase carcinogenesis and/or pre-cancerous lesions in tissues including liver and colon (Tessitore et al., 1996). Although these studies underline the need for an in depth understanding of its mechanisms of action, fasting is expected to have cancer preventive effects as indicated by the studies above and by the findings that multiple cycles of periodic fasting can be as effective as toxic chemotherapy in the treatment of some cancers in mice (Lee et al., 2012).
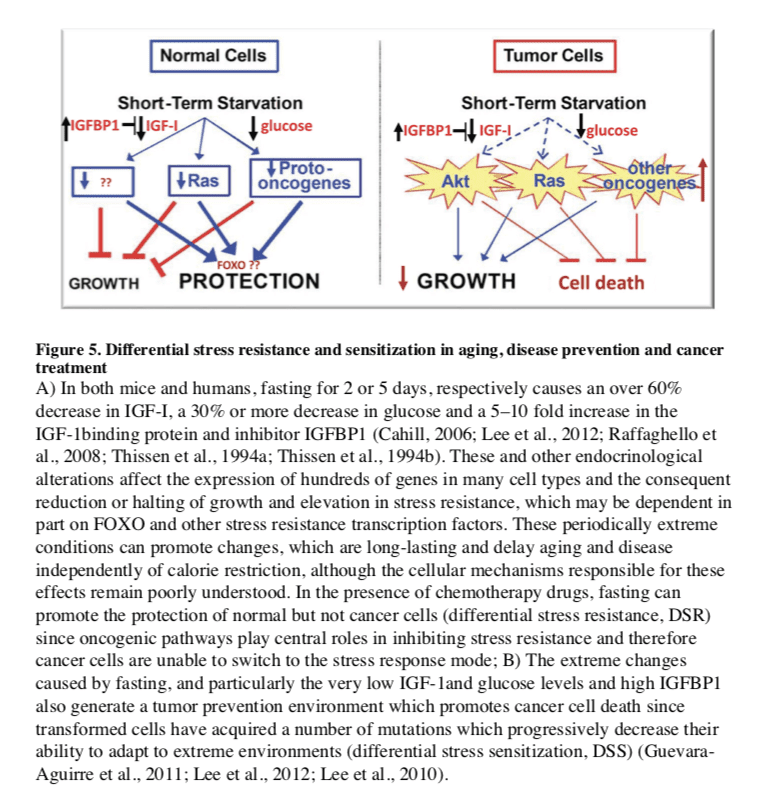
In the treatment of cancer, fasting has been shown to have more consistent and positive effects. PF for 2�3 days was shown to protect mice from a variety of chemotherapy drugs, an effect called differential stress resistance (DSR) to reflect the inability of cancer cells to become protected based on the role of oncogenes in negatively regulating stress resistance, thus rendering cancer cells, by definition, unable to become protected in response to fasting conditions (Figure 5) (Raffaghello et al., 2008). PF also causes a major sensitization of various cancer cells to chemo-treatment, since it fosters an extreme environment in combination with the stress conditions caused by chemotherapy. In contrast to the protected state entered by normal cells during fasting, cancer cells are unable to adapt, a phenomenon called differential stress sensitization (DSS), based on the notion that most mutations are deleterious and that the many mutations accumulated in cancer cells promote growth under standard conditions but render them much less effective in adapting to extreme environments (Lee et al., 2012). In mouse models of metastatic tumors, combinations of fasting and chemotherapy that cause DSR and DSS, result in 20 to 60% cancer-free survival compared to the same levels of chemotherapy or fasting alone, which are not sufficient to cause any cancer-free survival (Lee et al., 2012; Shi et al., 2012). Thus, the idea that cancer could be treated with weeks of fasting alone, made popular decades ago, may be only partially true, at least for some type of cancers, but is expected to be ineffective for other types of cancers. The efficacy of long-term fasting alone (2 weeks or longer) in cancer treatment will need to be tested in carefully designed clinical trials in which side effects including malnourishment and possibly a weakened immune system and increased susceptibility to certain infections are carefully monitored. By contrast, animal data from multiple laboratories indicate that the combination of fasting cycles with chemotherapy is highly and consistently effective in enhancing chemotherapeutic index and has high translation potential. A number of ongoing trials should soon begin to determine the efficacy of fasting in enhancing cancer treatment in the clinic.
Fasting and Neurodegeneration
Compared to ad libitum-fed controls, rats and mice maintained on an IF diet exhibit less neuronal dysfunction and degeneration, and fewer clinical symptoms in models of Alzheimer�s disease (AD), Parkinson�s disease (PD) and Huntington�s disease (HD). These models include transgenic mice expressing mutant human genes that cause dominantly inherited AD (amyloid precursor protein and presenilin-1) and frontotemporal lobe dementia (Tau) (Halagappa et al., 2007), PD (?-synuclein) (Griffioen et al., 2012) and HD (huntingtin) (Duan et al., 2003), as well as neurotoxin-based models pertinent to AD, PD and HD (Bruce-Keller et al., 1999; Duan and Mattson, 1999). Animals on an IF diet also fare better than ad libitum-fed controls after acute injury including severe epileptic seizures, stroke, and traumatic brain and spinal cord injuries (Arumugam et al., 2010; Bruce-Keller et al., 1999; Plunet et al., 2008).
Several interrelated cellular mechanisms contribute to the beneficial effects of IF on the nervous system including reduced accumulation of oxidatively damaged molecules, improved cellular bioenergetics, enhanced neurotrophic factor signaling, and reduced inflammation (Mattson, 2012a). The latter neuroprotective mechanisms are supported by studies showing that IF diets boost levels of antioxidant defenses, neurotrophic factors (BDNF and FGF2) and protein chaperones (HSP-70 and GRP-78), and reduce levels of pro- inflammatory cytokines (TNF?, IL-1? and IL-6) (Figure 4) (Arumugam et al., 2010). IF may also promote restoration of damaged nerve cell circuits by stimulating synapse formation and the production of new neurons from neural stem cells (neurogenesis) (Lee et al., 2002). Interestingly, while beneficial in models of most neurodegenerative conditions, there is evidence that fasting can hasten neurodegeneration in some models of inherited amyotrophic lateral sclerosis, perhaps because the motor neurons affected in those models are unable to respond adaptively to the moderate stress imposed by fasting (Mattson et al., 2007; Pedersen and Mattson, 1999).
Fasting and the Metabolic Syndrome
Metabolic syndrome (MS), defined as abdominal adiposity, combined with insulin resistance, elevated triglycerides and/or hypertension, greatly increases the risk of cardiovascular disease, diabetes, stroke and AD. Rats and mice maintained under the usual ad libitum feeding condition develop an MS-like phenotype as they age. MS can also be induced in younger animals by feeding them a diet high in fat and simple sugars (Martin et al., 2010). IF can prevent and reverse all aspects of the MS in rodents: abdominal fat, inflammation and blood pressure are reduced, insulin sensitivity is increased, and the functional capacities of the nervous, neuromuscular and cardiovascular systems are improved (Castello et al., 2010; Wan et al., 2003). Hyperglycemia is ameliorated by IF in rodent models of diabetes (Pedersen et al., 1999) and the heart is protected against ischemic injury in myocardial infarction models (Ahmet et al., 2005). A protective effect of fasting against ischemic renal and liver injury occurs rapidly, with 1 � 3 days of fasting improving functional outcome and reducing tissue injury and mortality (Mitchell et al., 2010). Six days on a diet missing just a single essential amino acid such as tryptophan can also elicit changes in metabolism and stress resistance, similar to those caused by fasting, which are dependent on the amino acid sensing kinase Gcn2 (Peng et al., 2012).
Multiple hormonal changes that typify MS in humans a re observed in rodents maintained on high fat and sugar diets including elevated levels of insulin and leptin and reduced levels of adiponectin and ghrelin. Elevated leptin levels are typically reflective of a pro- inflammatory state, whereas adiponectin and ghrelin can suppress inflammation and increase insulin sensitivity (Baatar et al., 2011; Yamauchi et al., 2001). Local inflammation in hypothalamic nuclei that control energy intake and expenditure may contribute to a sustained positive energy balance in MS (Milanski et al., 2012). Fasting results in a lowering of insulin and leptin levels and an elevation of adiponectin and ghrelin levels. By increasing insulin and leptin sensitivity, suppressing inflammation and stimulating autophagy, fasting reverses all the major abnormalities of the MS in rodents (Singh et al., 2009; Wan et al., 2010). Finally, in addition to its many effects on cells throughout the body and brain, IF may elicit changes in the gut microbiota that protect against MS (Tremaroli and Backhed, 2012). Naturally, the challenge of applying fasting-based interventions to treat MS in humans is a major one, as some obese individuals may have difficulties in following IF for long periods.
The ProLon� fasting mimicking diet is a 5-day meal program consisting of scientifically developed and clinically tested, natural ingredients which “trick” the human body into a fasting mode. The FMD is low in carbohydrates as well as proteins and it’s high in fats. The ProLon� fasting mimicking diet promotes a variety of healthy benefits, including weight loss and decreased abdominal fat, all while preserving lead body mass, improved energy levels, softer and healthier looking skin, as well as overall health and wellness. The FMD can promote longevity.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Fasting, Aging, and Disease in Humans
Fasting and Factors Implicated in Aging
Clinical and epidemiological data are consistent wit h an ability of fasting to retard the aging process and associated diseases. Major factors implicated in aging whose generation are accelerated by gluttonous lifestyles and slowed by energy restriction in humans include: 1) oxidative damage to proteins, DNA and lipids; 2) inflammation; 3) accumulation of dysfunctional proteins and organelles; and 4) elevated glucose, insulin and IGF-I, although IGF-1decreases with aging and its severe deficiency can be associated with certain pathologies (Bishop et al., 2010; Fontana and Klein, 2007). Serum markers of oxidative damage and inflammation as well as clinical symptoms are reduced over a period of 2�4 weeks in asthma patients maintained on an alternate day fasting diet (Johnson et al., 2007). Similarly, when on a 2 days/week fasting diet overweight women at risk for breast cancer exhibited reduced oxidative stress and inflammation (Harvie et al., 2011) and elderly men exhibited reductions in body weight and body fat, and improved mood (Teng et al., 2011). Additional effects of fasting in human cells that can be considered as potentially �anti-aging� are inhibition the mTOR pathway, stimulation of autophagy and ketogenesis (Harvie et al., 2011; Sengupta et al., 2010).
Among the major effects of fasting relevant to aging and diseases are changes in the levels of IGF-1, IGFBP1, glucose, and insulin. Fasting for 3 or more days causes a 30% or more decrease in circulating insulin and glucose, as well as rapid decline in the levels of insulin- like growth factor 1 (IGF-1), the major growth factor in mammals, which together with insulin is associated with accelerated aging and cancer (Fontana et al., 2010). In humans, five days of fasting causes an over 60% decrease in IGF-1and a 5-fold or higher increase in one of the principal IGF-1-inhibiting proteins: IGFBP1 (Thissen et al., 1994a). This effect of fasting on IGF-1is mostly due to protein restriction, and particularly to the restriction of essential amino acids, but is also supported by calorie restriction since the decrease in insulin levels during fasting promotes reduction in IGF-1(Thissen et al., 1994a). Notably, in humans, chronic calorie restriction does not lead to a decrease in IGF-1unless combined with protein restriction (Fontana et al., 2008).
IF can be achieved in with a minimal decrease in overall calorie intake if the refeeding period in which subjects overeat is considered. Thus, fasting cycles provide a much more feasible strategy to achieve the beneficial effects of CR, and possibly stronger effects, without the burden of chronic underfeeding and some of the potentially adverse effects associated with weight loss or very low BMIs. In fact, subjects who are moderately overweight (BMI of 25�30) in later life can have reduced overall mortality risk compared to subjects of normal weight (Flegal et al., 2013). Although these results may be affected by the presence of many existing or developing pathologies in the low weight control group, they underline the necessity to differentiate between young individuals and elderly individuals who may use CR or fasting to reduce weight or delay aging. Although extreme dietary interventions during old age may continue to protect from age-related diseases, they could have detrimental effects on the immune system and the ability to respond to certain infectious diseases, wounds and other challenges (Kristan, 2008; Reed et al., 1996). However, IF or PF designed to avoid weight loss and maximize nourishment have the potential to have beneficial effects on infectious diseases, wounds and other insults even in the very old. Nourishment of subjects can be achieved by complementing IF or PF with micro- and macro Studies to test the effect of IF or PF regimens on markers of aging, cancer, cognition and obesity are in progress (V. Longo and M. Mattson).
Fasting and Cancer
Fasting has the potential for applications in both cancer prevention and treatment. Although no human data are available on the effect of IF or PF in cancer prevention, their effect on reducing IGF-1, insulin and glucose levels, and increasing IGFBP1 and ketone body levels could generate a protective environment that reduces DNA damage and carcinogenesis, while at the same time creating hostile conditions for tumor and pre-cancerous cells (Figure 5). In fact, elevated circulating IGF-1 is associated with increased risk of developing certain cancers (Chan et al., 2000; Giovannucci et al., 2000) and individuals with severe IGF-1deficiency caused by growth hormone receptor deficiency, rarely develop cancer (Guevara-Aguirre et al., 2011; Shevah and Laron, 2007; Steuerman et al., 2011). Furthermore, the serum from these IGF-1deficient subjects protected human epithelial cells from oxidative stress-induced DNA damage. Furthermore, once their DNA became damaged, cells were more likely to undergo programmed cell death (Guevara-Aguirre et al., 2011). Thus, fasting may protect from cancer by reducing cellular and DNA damage but also by enhancing the death of pre-cancerous cells.
In a preliminary study of 10 subjects with a variety of malignancies, the combination of chemotherapy with fasting resulted in a decrease in a range of self-reported common side effects caused by chemotherapy compared to the same subjects receiving chemotherapy while on a standard diet (Safdie et al., 2009). The effect of fasting on chemotherapy toxicity and cancer progression is now being tested in clinical trials in both Europe and the US (0S-08-9, 0S-10-3).
Fasting and Neurodegeneration
Our current understanding of the impact of IF on the nervous system and cognitive functions is largely inferred from animal studies (see above). Interventional studies to determine the impact of fasting on brain function and neurodegenerative disease processes are lacking.
After 3�4 month, CR improved cognitive function (verbal memory) in overweight women (Kretsch et al., 1997) and in elderly subjects (Witte et al., 2009). Similarly, when subjects with mild cognitive impairment were maintained for 1 month on a low glycemic diet, they exhibited improved delayed visual memory, cerebrospinal fluid biomarkers of A? metabolism and brain bioenergetics (Bayer-Carter et al., 2011). Studies in which cognitive function, regional brain volumes, neural network activity, and biochemical analyses of cerebrospinal fluid are measured in human subjects before and during an extended period of IF should clarify the impact of IF on human brain structure and function.
Fasting, Inflammation and Hypertension
In humans, one of the best demonstrations of the beneficial effects of long-term fasting lasting one to 3 weeks is in the treatment of rheumatoid arthritis (RA). In agreement with the results in rodents, there is little doubt that during the period of fasting both inflammation and pain are reduced in RA patients (Muller et al., 2001). However, after the normal diet is resumed, inflammation returns unless the fasting period is followed by a vegetarian diet (Kjeldsen-Kragh et al., 1991), a combination therapy that has beneficial effects lasting for two years or longer (Kjeldsen-Kragh et al., 1994). The validity of this approach is supported by four differently controlled studies, including two randomized trials (Muller et al., 2001). Therefore, fasting combined with a vegetarian diet and possibly with other modified diets provides beneficial effects in the treatment of RA. Alternate day IF also resulted in significant reductions in serum TNF? and ceramides in asthma patients during a 2 month period (Johnson et al., 2007). The latter study further showed that markers of oxidative stress often associated with inflammation (protein and lipid oxidation) were significantly reduced in response to IF. Thus, for many patients able and willing to endure long-term fasting and to permanently modify their diet, fasting cycles would have the potential to not only augment but also replace existing medical treatments.
Water only and other forms of long-term fasting have also been documented to have potent effects on hypertension. An average of 13 days of water only fasting resulted in the achievement of a systolic blood pressure (BP) below 120 in 82% of subjects with borderline hypertension with a mean 20 mm Hg reduction in BP (Goldhamer et al., 2002). BP remained significantly lower compared to baseline even after subjects resumed the normal diet for an average of 6 days (Goldhamer et al., 2002). A small pilot study of patients with hypertension (140 mm and above systolic BP) also showed that 10�11 days of fasting caused a 37�60 mm decrease in systolic BP (Goldhamer et al., 2001). These preliminary studies are promising but underscore the need for larger controlled and randomized clinical studies that focus on periodic fasting strategies that are feasible for a larger portion of the population.
For both hypertension and RA it will be important to develop PF mimicking diets that are as effective as the fasting regimens described above but that are also tolerable by the great majority of patients.
Fasting and the Metabolic Syndrome
Periodic fasting can reverse multiple features of the metabolic syndrome in humans: it enhances insulin sensitivity, stimulates lipolysis and reduces blood pressure. Body fat and blood pressure were reduced and glucose metabolism improved in obese subjects in response to an alternate day modified fast (Klempel et al., 2013; Varady et al., 2009). Overweight subjects maintained for 6 months on a twice weekly IF diet in which they consumed only 500�600 calories on the fasting days, lost abdominal fat, displayed improved insulin sensitivity and reduced blood pressure (Harvie et al., 2011). Three weeks of alternate day fasting resulted in reductions in body fat and insulin levels in normal weight men and women (Heilbronn et al., 2005) and Ramadan fasting (2 meals/day separated by approximately 12 hours) in subjects with MS resulted in decreased daily energy intake, decreased plasma glucose levels and increased insulin sensitivity (Shariatpanahi et al., 2008). Subjects undergoing coronary angiography who reported that they fasted regularly exhibited a lower prevalence of diabetes compared to non-fasters (Horne et al., 2012). Anti- metabolic syndrome effects of IF were also observed in healthy young men (BMI of 25) after 15 days of alternate day fasting: their whole-body glucose uptake rates increased significantly, levels of plasma ketone bodies and adiponectin were elevated, all of which occurred without a significant decrease in body weight (Halberg et al., 2005). The latter findings are similar to data from animal studies showing that IF can improve glucose metabolism even with little or no weight change (Anson et al., 2003). It will be important to determine if longer fasting periods which promote a robust switch to a fat breakdown and ketone body-based metabolism, can cause longer lasting and more potent effects.
Conclusions and Recommendations
Based on the existing evidence from animal and human studies described, we conclude that there is great potential for lifestyles that incorporate periodic fasting during adult life to promote optimal health and reduce the risk of many chronic diseases, particularly for those who are overweight and sedentary. Animal studies have documented robust and replicable effects of fasting on health indicators including greater insulin sensitivity, and reduced levels of blood pressure, body fat, IGF-I, insulin, glucose, atherogenic lipids and inflammation. Fasting regimens can ameliorate disease processes and improve functional outcome in animal models of disorders that include myocardial infarction, diabetes, stroke, AD and PD. One general mechanism of action of fasting is that it triggers adaptive cellular stress responses, which result in an enhanced ability to cope with more severe stress and counteract disease processes. In addition, by protecting cells from DNA damage, suppressing cell growth and enhancing apoptosis of damaged cells, fasting could retard and/ or prevent the formation and growth of cancers.
However, studies of fasting regimens have not been performed in children, the very old and underweight individuals, and it is possible that IF and PF would be harmful to these populations. Fasting periods lasting longer than 24 hours and particularly those lasting 3 or more days should be done under the supervision of a physician and preferably in a clinic. IF- and PF-based approaches towards combating the current epidemics of overweight, diabetes and related diseases should be pursued in human research studies and medical treatment plans. Several variations of potential �fasting prescriptions� that have been adopted for overweight subjects revolve around the common theme of abstaining from food and caloric beverages for at least 12 � 24 hours on one or more days each week or month, depending on the length, combined with regular exercise. For those who are overweight, physicians could ask their patients to choose a fasting-based intervention that they believe they could comply with based upon their daily and weekly schedules. Examples include the �5:2� IF diet (Harvie et al., 2011), the alternate day modified fasting diet (Johnson et al., 2007; Varady et al., 2009), a 4�5 day fast or low calorie but high nourishment fasting mimicking diets once every 1�3 months followed by the skipping of one major meal every day if needed (V. Longo, clinical trial in progress). One of the concerns with unbalanced alternating diets such as those in which low calorie intake is only observed for 2 days a week are the potential effects on circadian rhythm and the endocrine and gastrointestinal systems, which are known to be influenced by eating habits. During the first 4 � 6 weeks of implementation of the fasting regimen, a physician or registered dietitian should be in regular contact with the patient to monitor their progress and to provide advice and supervision.
Fasting regimens could also be tailored for specific diseases as stand-alone or adjunct therapies. Results of initial trials of IF (fasting 2 days per week or every other day) in human subjects suggest that there is a critical transition period of 3 � 6 weeks during which time the brain and body adapt to the new eating pattern and mood is enhanced (Harvie et al., 2011; Johnson et al., 2007). Though speculative, it is likely that during the latter transition period brain neurochemistry changes so that the �addiction� to regular consumption of food throughout the day is overcome. Notably, the various fasting approaches are likely to have limited efficacy particularly on aging and conditions other than obesity unless combined with diets such as the moderate calorie intake and mostly plant-based Mediterranean or Okinawa low protein diets (0.8 g protein/Kg of body weight), consistently associated with health and longevity.
In the future, it will be important to combine epidemiological data, studies of long-lived populations and their diets, results from model organisms connecting specific dietary components to pro-aging and pro-disease factors, with data from studies on fasting regimens in humans, to design large clinical studies that integrate fasting with diets recognized as protective and enjoyable. A better understanding of the molecular mechanisms by which fasting affects various cell types and organ systems should lead to the development of novel prophylactic and therapeutic interventions for a wide range of disorders.
Take Home Message
The fasting mimicking diet provides the same benefits of traditional fasting by restricting your calorie intake for five days out of the month instead of completely eliminating all food for several days or even weeks. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled in precise quantities and combinations for each day. Although the research study above has demonstrated the health benefits of fasting, please make sure to talk to a healthcare professional before starting the ProLon� fasting mimicking diet, 5-day meal program to find out if the FMD, or any other diet, is right for you.
The published, final edited form of the research study referenced above was made available in the NIH Public Access Author Manuscript on PMC February 4, 2015. The scope of our information is limited to chiropractic, spinal health issues, and functional medicine topics. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
At El Paso Back Clinic, we want to help as many people as possible achieve optimal health, through the power of nutrition. The Fasting Mimicking Diet�is the first and only clinically tested, scientific breakthrough in Fasting Mimicking technology that gives your body the stem cell-based rejuvenation of a 5-day fast while eating real food. Dr. Jimenez discusses the biological effects of the ProLon� fast mimicking diet (FMD).
Fasting: Awakening the Rejuvenation from Within | Valter Longo | TEDxEchoPark
An enlightening and provocative presentation is given by Valter Longo updating audience on the benefits of fasting for life-extension.
Dr. Valter Longo is the Edna M. Jones Professor of Gerontology and Biological Sciences, and Director of the Longevity Institute at the University of Southern California � Davis School of Gerontology, Los Angeles. Dr. Longo�s studies focus on the fundamental mechanisms of aging in simple organisms, mice, and humans. The Longo laboratory has identified several genetic pathways that regulate aging in simple organisms and reduce the incidence of multiple diseases in mice and humans. His laboratory also described both dietary and genetic interventions that protect cells and improve the treatment and prevention of cancer and other diseases in mammals. He received his Ph.D. in Biochemistry from the University of California, Los Angeles (UCLA) in 1997 and his postdoctoral training in the Neurobiology of Aging and Alzheimer�s Diseases at USC. He started his independent career in 2000 at the University of Southern California, School of Gerontology.
Every day millions of people use chiropractic care to help manage pain, correct certain health conditions, and to live a healthier, more mobile life � and there are some very famous faces among them. A number of celebrities use chiropractic on a regular basis. Here are three very different people with very different reasons for seeing a chiropractor.
Lance Armstrong � 7 Time Tour de France Winner
Cycling takes a serious toll on the human body. The repetitive motion of pedaling, combined with the hunched posture as the cyclist leans over the handlebars can lead to back pain, hip lock, and knee problems as well as wrist problems.
Pro cyclist, Lance Armstrong knows well the beating that a body takes when cycling and keeps chiropractor Dr. Jeff Spencer on his staff. The 7 time Tour de France winner has been quoted as saying that the chiropractor is the most important person on the team staff. In fact, in his book, Every Second Counts, he said, �The guy who put us all back together was our chiropractor.�
Dr. Spencer, who toured with Armstrong and the United States Cycling Team, has work with other pro athletes including NASCAR drivers and PGA golfer Tiger Woods. He helps keep Armstrong on top of his game.
Montel Williams � Talk Show Host
One of the most profound testimonials from a celebrity regarding chiropractic comes from talk show host Montel Williams.
In 1999, Williams was diagnosed with Multiple Sclerosis (MS), a devastating chronic disease that affects the central nervous system. It often leads to disability in many of the people who have it. The symptoms can range from mild tingling to paralysis or blindness.
He endured severe pain that affected the way he moved, including how he walked. He tried many different treatments, including chiropractic. He credits chiropractic with reducing his pain and mobility issues.
When Williams tried chiropractic for MS, he found that his symptoms decreased significantly, especially his chronic pain. Regular chiropractic treatments help him to stay active which he finds very effective in managing his disease and pain. The whole-body approach that chiropractic offers gave Williams invaluable guidance regarding diet, exercise, and stress management in addition to spinal adjustments. It has made a significant difference in his life.
Gisele Bundchen � Victoria�s Secret Model
We may never know just what Victoria�s �secret� is, but Gisele Bundchen, one of the famous faces of the brand, has her own secret to a �painless� natural birth � good prenatal care that includes a top-notch doula/midwife and an exceptional chiropractor. The supermodel, who is married to Tom Brady, made regular visits to her chiropractor throughout her pregnancy.
She �wanted to be present� during the birth of her child so she opted for a more natural approach to her prenatal care as well as labor and delivery. When it came time for her son�s birth, she said that she �felt no pain.� The birth was reportedly quick and painless.
Chiropractic has long been used by expectant moms to counteract the many changes a woman�s body experiences throughout pregnancy. When the body is in balance and the spine is aligned, it does indeed make the birth much easier.
Bundchen is not the only supermodel who believes in chiropractic though. Cindy Crawford is also a believer. In fact, her twins have been seeing a chiropractor since they were very young. According to Crawford, she included chiropractic as part of their healthcare because she wanted her kids to be healthy.
Chiropractic can help anyone; you don�t have to be a celebrity to enjoy the health benefits. No matter what you do for work or play, it can make a difference in your life too.
Heard about fasting? It is defined as, “abstinence from eating.” What this diet has the potential for in medical benefits has increased quite substantially � both in animal and medical research. Inventor of the Fast Mimicking Diet (FMD) Dr. Longo is recognized as a leading expert on longevity and has done intense work in biochemical pathways. In other words the way cells and we as humans age. This diet can change all that!
What’s all the hype about the FMD?
After years of experimenting with FMD in animal models and showing its benefits on metabolism and life span, Dr. Longo�s team analyzed the effects in human clinical trials. One hundred healthy subjects participated�with half of them following the Prolon FMD five days a month for three months, while the other half ate their regular diet.
Increase in stem cell production, (this is a marker for cell regeneration).
This diet works by shifting the body�s metabolism and enhancing the power of cells to help protect against chronic diseases like type 2 diabetes and cardiovascular disease. This idea is beginning to catch on: according to a 2018 survey from the International Food Information Council Foundation, intermittent fasting was last year�s most popular diet. Dr. Longo is now studying if a fast-mimicking diet can improve cancer �outcomes and help prevent the disease.
Dr. Longo addresses the point that the more healthy food an individual chooses, the more one can eat. Individuals can still eat fats like pesto, and starches like pasta. The benefits happen when the individual loads up on produce. This brings in more nutrients, more fiber and the feeling of being more full. Dr. Longo is also working on the ability to train an individual’s body to eat within a 12-hour day, which acts as a quick fast overnight.
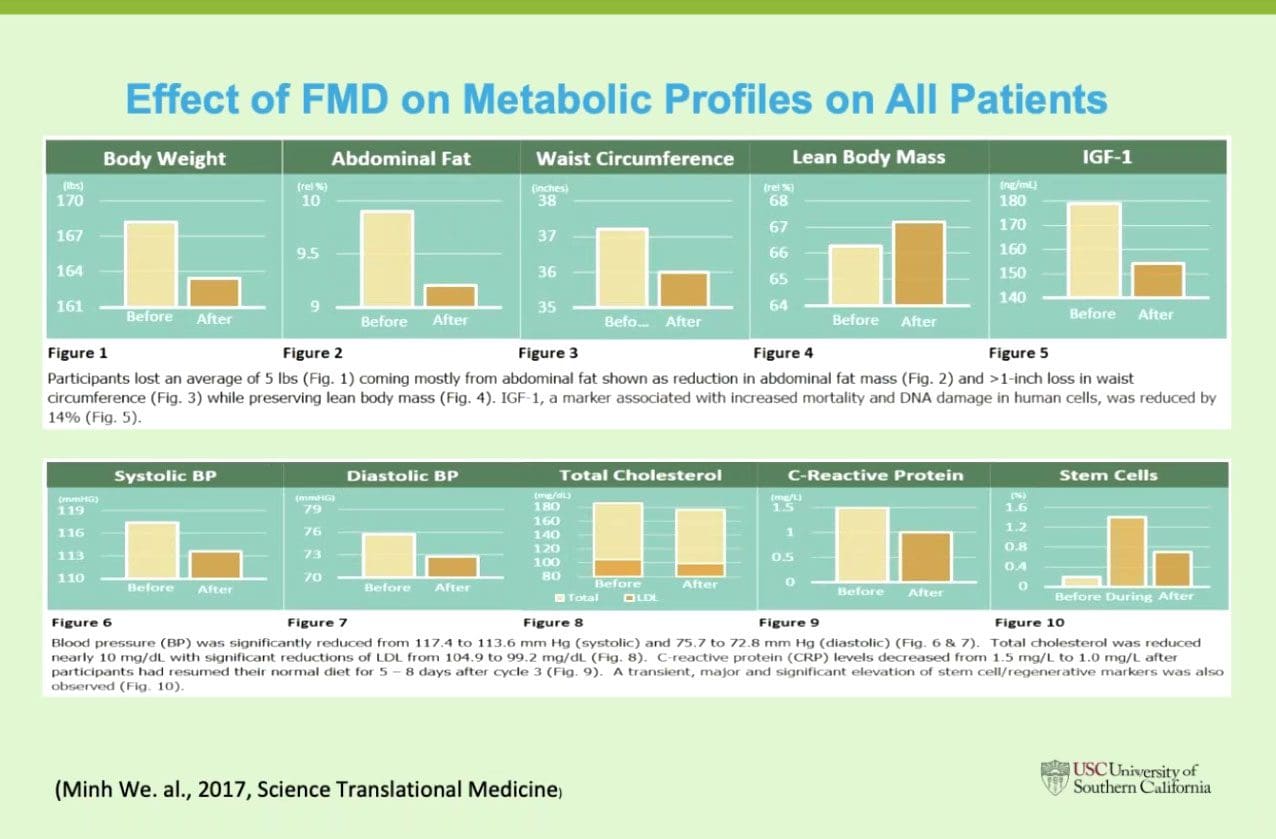
Los Angeles, Calif.�July 31, 2018�On July 10,�L-Nutra, Inc.�became the first company to market a product that has been granted a patent by the�United States Patent and Trademark Office (USPTO)�for optimizing human healthspan, the length of time that a person is healthy. This follows a landmark patent issued in 2016 for treating diabetes and multiple patents previously issued for cancer treatment, but this is the first patented protocol to address health and wellness prior to the onset of disease. The patent is for the Fasting Mimicking Diet� (FMD�), discovered and clinically tested by the�laboratory of Valter Longo�and�Keck Hospital�at the University of Southern California (USC), a nutrition technology that is proven to reduce markers for age-related disease as well as promote tissue regeneration. The Fasting Mimicking Diet is one of few nutri-technologies that has undergone extensive scientific research and clinical trials at major universities across the world. Last year, a landmark human trial published in�Science Translational Medicine�demonstrated that ProLon is clinically proven to reduce markers of the body�s aging process, optimize weight, and maintain healthy levels of multiple metabolic markers such as cholesterol, triglyceride, glucose, and CRP (an inflammatory marker). The secret to the Fasting Mimicking Diet relies on the body�s activation of the epigenetic, metabolic, and cellular reprogramming to survive prolonged periods of fasting. Fasting Mimicking Diet Is Awarded First-Ever Patent for Optimizing Human Healthspan
Interested?
Information
Diet Decreases Calorie Intake to 1,100 on Day One
Then Around 800 the Next Four Days
The program is rich in nuts � so not for those with a nut allergy
Nutrients are crucial and are plant-based whole foods:
Nuts
Olives�(note if don’t like olives)
Teas
Soup mixes – which are 80% fat, 10% protein, and 10% carbohydrate.
During the five days fast:
Exercise and Alcohol are prohibited
Coffee is limited to zero or one cup a day
How to Use ProLon FMD
Ready?
What to know. To achieve the published results, one will possibly need to go through three cycles at specific times, where they don’t conflict with family/social events like birthdays, weddings, quinceaneras, etc. After three months some will choose to do the program monthly or every other month for long-term health.
Increased Brain Power Study
Preliminary studies with FMD showed remarkable brain changes
FMD fed to mice four days in a row twice a month:
Extended longevity
Lowered visceral fat
Reduced cancer incidence and
Skin Lesions
Rejuvenated the immune system
Slowed down bone density loss
In old mice, FMD cycles promoted:
Brain growth
Demonstrate improved cognitive performance
It is possible that the best brains may result from the least caloric intake for five days a month
El Paso, TX. Chiropractor, Dr. Alexander Jimenez examines how the Fasting Mimicking diet works. What it does, how to take it and the optimal health benefits.
The Diet Where You Fast With Food!
The 5 DayFasting Mimicking Diet�, or FMD, is the first fasting meal program.
Made from natural ingredients.
Meals are consumed for five days.
The body’s ( cellular pathways) do not recognize the meals as food.
This keeps the body in a fasting mode.
This diet is proven to promote overall health.
Reduce excess fat.
Allows�you freedom.
Scientifically developed and clinically tested at the Longevity Institute at the University of Southern California. Led by Dr. Valter Longo, the USC Longevity Institute unites multidisciplinary aging research approaches to enhance the healthy years of life.
The FMD is the only meal program that provides the body with optimal nourishment, which keeps the body in fasting mode.
�
Take ProLon� What For?
ProLon� is clinically tested, an�easy-to-take 5-day meal program that enhances your health without dramatic lifestyle changes
Pre-Clinical Trials
In the first study from the Clinical and Translational Report, yeast deprived of food periodically were shown to have longer life expectancy than yeast fed normally.
The second study involved feeding a group of mice a specialized diet for four days a month.
The diet reduced both caloric intake and protein intake.
The scientists tested markers in the blood of the mice and found that the diet emulated prolonged water-only fasting.
After returning to regular feeding, the mice regained most, but not all of the lost weight.
Differences between the Fasting Mimicking Diet group and the control group include improved metabolism and cognitive function, gradual weight loss, muscle rejuvenation, higher bone density, 40% fewer malignant lymphomas, immune system regeneration, and longer average life expectancy.
A Third Study
There were nineteen participants and nineteen control participants with a broad range of ages (19-75).
Members of both sexes and various races so that the study represented a general cross-section of, adult population.
The individuals in the Fasting Mimicking Diet group were provided with the food they were required to eat during the five days.
Scientists were happy with the compliance level of the diet, and most reported only mild or no negative effects on the fast days.
Results showed that the FMD participants experienced an average:
Individuals diagnosed with serious medical condition or disease unless approved in writing by a physician appropriately trained to treat that condition
Individuals who have been severely weakened by a disease or medical procedure
Individuals who are taking medications which may not be safely consumed with a calorie restricted diet unless authorized in writing by a licensed physician
Individuals with Diabetes (type 1 and type 2), cardiovascular disease and cancer, unless approved in writing by a licensed physician. ProLon� should never be combined with glucose-lowering drugs, such as metformin or insulin
Fasting is prohibited for individuals with particular metabolic diseases, such as those affecting gluconeogenesis.
Individuals with a history of significant cardiac disease, particularly uncompensated congestive heart failure NYHA grade 2 or more or LVEF <40% on any prior assessment
Individuals with a history of syncope (fainting) with calorie restriction or other medical co-morbidities Individuals who have special dietary needs that are incompatible with the ProLon� meal plan
Individuals with liver or kidney disorders that may be affected by very low glucose and protein content of the diet
Chiropractic Weight Loss Treatment
ProLon� is clinically tested, an�easy-to-take 5-day meal program that enhances your health without dramatic lifestyle changes
Pre-Clinical Trials
In the first study from the Clinical and Translational Report, yeast deprived of food periodically were shown to have longer life expectancy than yeast fed normally.
The second study involved feeding a group of mice a specialized diet for four days a month.
The diet reduced both caloric intake and protein intake.
The scientists tested markers in the blood of the mice and found that the diet emulated prolonged water-only fasting.
After returning to regular feeding, the mice regained most, but not all of the lost weight.
Differences between the Fasting Mimicking Diet group and the control group include improved metabolism and cognitive function, gradual weight loss, muscle rejuvenation, higher bone density, 40% fewer malignant lymphomas, immune system regeneration, and longer average life expectancy.
A Third Study
There were nineteen participants and nineteen control participants with a broad range of ages (19-75).
Members of both sexes and various races so that the study represented a general cross-section of, adult population.
The individuals in the Fasting Mimicking Diet group were provided with the food they were required to eat during the five days.
Scientists were happy with the compliance level of the diet, and most reported only mild or no negative effects on the fast days.
Results showed that the FMD participants experienced an average:
Individuals diagnosed with serious medical condition or disease unless approved in writing by a physician appropriately trained to treat that condition
Individuals who have been severely weakened by a disease or medical procedure
Individuals who are taking medications which may not be safely consumed with a calorie restricted diet unless authorized in writing by a licensed physician
Individuals with Diabetes (type 1 and type 2), cardiovascular disease and cancer, unless approved in writing by a licensed physician. ProLon� should never be combined with glucose-lowering drugs, such as metformin or insulin
Fasting is prohibited for individuals with particular metabolic diseases, such as those affecting gluconeogenesis.
Individuals with a history of significant cardiac disease, particularly uncompensated congestive heart failure NYHA grade 2 or more or LVEF <40% on any prior assessment
Individuals with a history of syncope (fainting) with calorie restriction or other medical co-morbidities Individuals who have special dietary needs that are incompatible with the ProLon� meal plan
Individuals with liver or kidney disorders that may be affected by very low glucose and protein content of the diet
Chiropractic Weight Loss Treatment
The ProLon clinical trials protocol included three consecutive cycles of ProLon (5-day only per month over three consecutive months). It is up to the practitioner to decide the best method that he or she would like to use for each patient. It is suggested that for patients who are obese or overweight, to use ProLon for one three cycle protocol, and recommend that you check with your doctor to re-assess and determine if they have met their goals or if more cycles would be helpful. If a patient is not overweight and eats and exercises well, it is suggested to take the product 1-2 times a year.
Caution
Due to the low caloric nature of the ProLon� 5-day meal program, Individuals should not take ProLon� in combination with prescription or non-prescription drugs unless approved by your healthcare professional.
Drink at least 8 cups of water to minimize the risk of dehydration.
Avoid alcohol consumption, strenuous exercise, and exposure to high temperatures (e.g., saunas, spas, Jacuzzi) or cold environments and swimming.
Operate a motor vehicle and heavy machinery with care until it is known how ProLon� may affect you.
Clinical Methodology
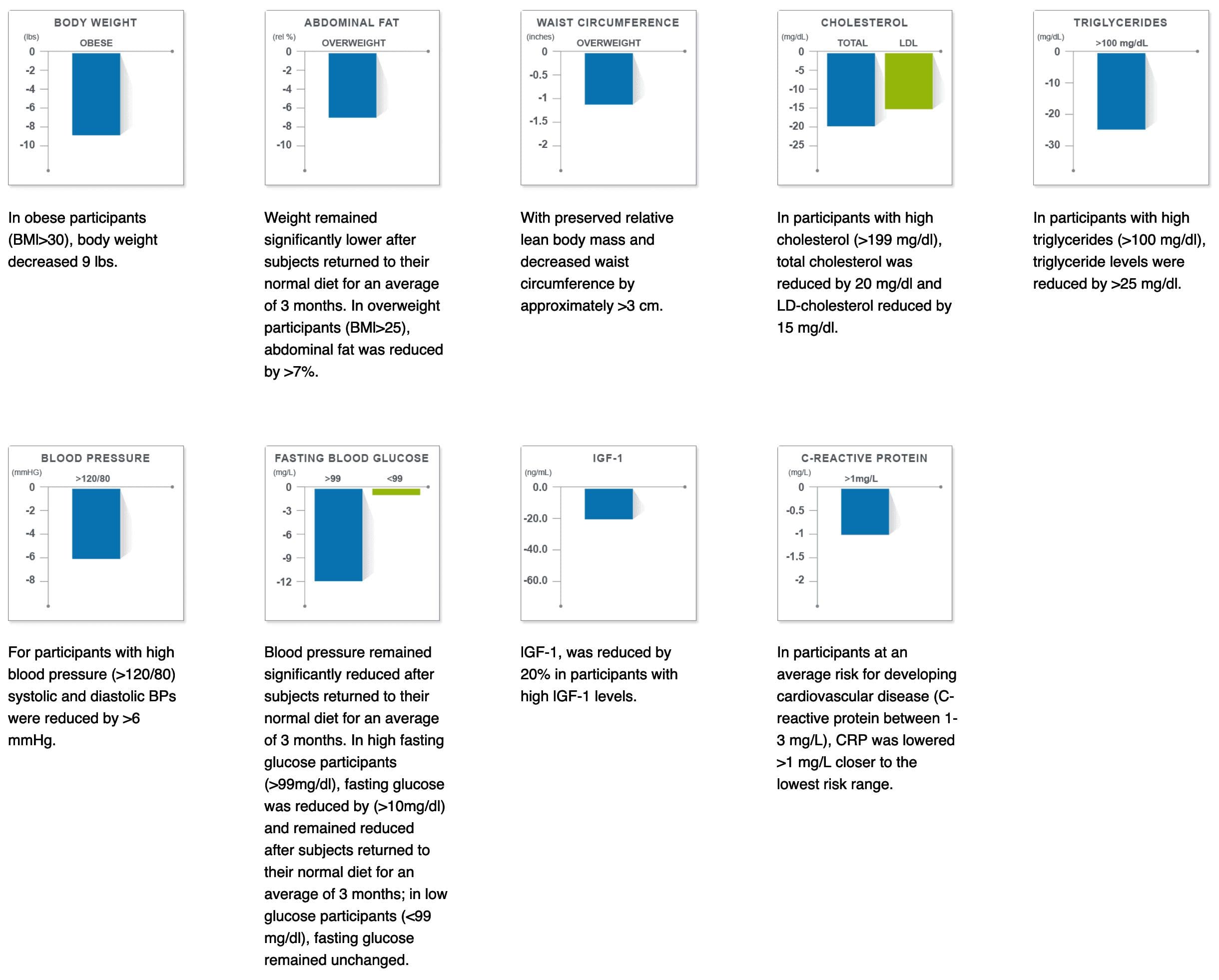
Pre-clinical and clinical studies have proven that periodic fasting, done for several days, is a very powerful intervention that our bodies learned to naturally cope with by protecting and rejuvenating itself. The 5-Day ProLon Fasting Mimicking Diet has been clinically tested and found to promote beneficial effects in a wide variety of conditions ranging from excess weight and fasting blood glucose, to growth factors associated with DNA damage and aging.
A randomized control trial of 100 subjects
71 completed 3 cycles of the ProLon� either in a randomized phase (N=39) or
After being crossed over from a control diet group to the FMD group (N=32)
Control subjects continued with a normal diet.
ProLon� participants consumed the fasting mimicking diet (FMD) for 5 days per month for 3 months.
Measurements were performed prior to the diet (Before) and (During) the recovery period and (After) the 3rd cycle.
�
Clinical Results
Elevated Risk Results
ProLon� is clinically tested, an�easy-to-take 5-day meal program that enhances your health without dramatic lifestyle changes
Pre-Clinical Trials
In the first study from the Clinical and Translational Report, yeast deprived of food periodically were shown to have longer life expectancy than yeast fed normally.
The second study involved feeding a group of mice a specialized diet for four days a month.
The diet reduced both caloric intake and protein intake.
The scientists tested markers in the blood of the mice and found that the diet emulated prolonged water-only fasting.
After returning to regular feeding, the mice regained most, but not all of the lost weight.
Differences between the Fasting Mimicking Diet group and the control group include improved metabolism and cognitive function, gradual weight loss, muscle rejuvenation, higher bone density, 40% fewer malignant lymphomas, immune system regeneration, and longer average life expectancy.
A Third Study
There were nineteen participants and nineteen control participants with a broad range of ages (19-75).
Members of both sexes and various races so that the study represented a general cross-section of, adult population.
The individuals in the Fasting Mimicking Diet group were provided with the food they were required to eat during the five days.
Scientists were happy with the compliance level of the diet, and most reported only mild or no negative effects on the fast days.
Results showed that the FMD participants experienced an average:
Individuals diagnosed with serious medical condition or disease unless approved in writing by a physician appropriately trained to treat that condition
Individuals who have been severely weakened by a disease or medical procedure
Individuals who are taking medications which may not be safely consumed with a calorie restricted diet unless authorized in writing by a licensed physician
Individuals with Diabetes (type 1 and type 2), cardiovascular disease and cancer, unless approved in writing by a licensed physician. ProLon� should never be combined with glucose-lowering drugs, such as metformin or insulin
Fasting is prohibited for individuals with particular metabolic diseases, such as those affecting gluconeogenesis.
Individuals with a history of significant cardiac disease, particularly uncompensated congestive heart failure NYHA grade 2 or more or LVEF <40% on any prior assessment
Individuals with a history of syncope (fainting) with calorie restriction or other medical co-morbidities Individuals who have special dietary needs that are incompatible with the ProLon� meal plan
Individuals with liver or kidney disorders that may be affected by very low glucose and protein content of the diet
Chiropractic Weight Loss Treatment
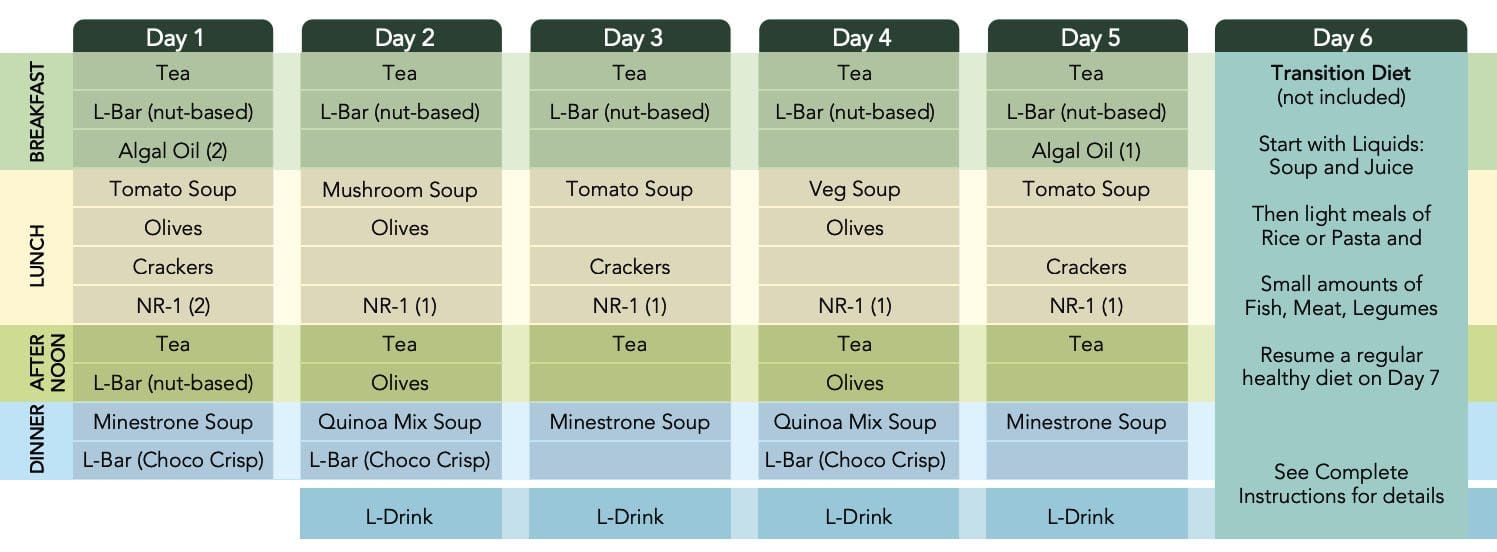
At the end of the program on Day 6
Liquid foods, such as soups and fruit juices
Light meals: rice, pasta, small portions of fish/meat/legumes
Avoid binge eating
Fast Performance
�
The Expectations?
Individuals taking ProLon� a have reported
Improved energy levels
Less fatigue
Softer and shinier skin
A positive impact on lifestyle
Making healthier choices and eating less
How Often Should Somebody Take The 5-Day ProLon� Diet?
The ProLon clinical trials protocol included three consecutive cycles of ProLon (5-day only per month over three consecutive months). It is up to the practitioner to decide the best method that he or she would like to use for each patient. It is suggested that for patients who are obese or overweight, to use ProLon for one three cycle protocol, and recommend that you check with your doctor to re-assess and determine if they have met their goals or if more cycles would be helpful. If a patient is not overweight and eats and exercises well, it is suggested to take the product 1-2 times a year.
Caution
Due to the low caloric nature of the ProLon� 5-day meal program, Individuals should not take ProLon� in combination with prescription or non-prescription drugs unless approved by your healthcare professional.
Drink at least 8 cups of water to minimize the risk of dehydration.
Avoid alcohol consumption, strenuous exercise, and exposure to high temperatures (e.g., saunas, spas, Jacuzzi) or cold environments and swimming.
Operate a motor vehicle and heavy machinery with care until it is known how ProLon� may affect you.
Clinical Methodology
Pre-clinical and clinical studies have proven that periodic fasting, done for several days, is a very powerful intervention that our bodies learned to naturally cope with by protecting and rejuvenating itself. The 5-Day ProLon Fasting Mimicking Diet has been clinically tested and found to promote beneficial effects in a wide variety of conditions ranging from excess weight and fasting blood glucose, to growth factors associated with DNA damage and aging.
A randomized control trial of 100 subjects
71 completed 3 cycles of the ProLon� either in a randomized phase (N=39) or
After being crossed over from a control diet group to the FMD group (N=32)
Control subjects continued with a normal diet.
ProLon� participants consumed the fasting mimicking diet (FMD) for 5 days per month for 3 months.
Measurements were performed prior to the diet (Before) and (During) the recovery period and (After) the 3rd cycle.
�
Clinical Results
Elevated Risk Results
ProLon� is clinically tested, an�easy-to-take 5-day meal program that enhances your health without dramatic lifestyle changes
Pre-Clinical Trials
In the first study from the Clinical and Translational Report, yeast deprived of food periodically were shown to have longer life expectancy than yeast fed normally.
The second study involved feeding a group of mice a specialized diet for four days a month.
The diet reduced both caloric intake and protein intake.
The scientists tested markers in the blood of the mice and found that the diet emulated prolonged water-only fasting.
After returning to regular feeding, the mice regained most, but not all of the lost weight.
Differences between the Fasting Mimicking Diet group and the control group include improved metabolism and cognitive function, gradual weight loss, muscle rejuvenation, higher bone density, 40% fewer malignant lymphomas, immune system regeneration, and longer average life expectancy.
A Third Study
There were nineteen participants and nineteen control participants with a broad range of ages (19-75).
Members of both sexes and various races so that the study represented a general cross-section of, adult population.
The individuals in the Fasting Mimicking Diet group were provided with the food they were required to eat during the five days.
Scientists were happy with the compliance level of the diet, and most reported only mild or no negative effects on the fast days.
Results showed that the FMD participants experienced an average:
Individuals diagnosed with serious medical condition or disease unless approved in writing by a physician appropriately trained to treat that condition
Individuals who have been severely weakened by a disease or medical procedure
Individuals who are taking medications which may not be safely consumed with a calorie restricted diet unless authorized in writing by a licensed physician
Individuals with Diabetes (type 1 and type 2), cardiovascular disease and cancer, unless approved in writing by a licensed physician. ProLon� should never be combined with glucose-lowering drugs, such as metformin or insulin
Fasting is prohibited for individuals with particular metabolic diseases, such as those affecting gluconeogenesis.
Individuals with a history of significant cardiac disease, particularly uncompensated congestive heart failure NYHA grade 2 or more or LVEF <40% on any prior assessment
Individuals with a history of syncope (fainting) with calorie restriction or other medical co-morbidities Individuals who have special dietary needs that are incompatible with the ProLon� meal plan
Individuals with liver or kidney disorders that may be affected by very low glucose and protein content of the diet
Chiropractic Weight Loss Treatment
Blood glucose
Blood pressure
Cholesterol
Triglycerides
C-reactive proteins
Stem cells Insulin-like growth factor 1 (IGF-1
Meals
The Program Itself
Consume the ProLon� meal program�s components for five consecutive days
Do not consume any additional food/liquid other than water or herbal teas without caffeine or additives
In order to maximize the benefits, you should minimize your consumption of caffeine to 1 cup of coffee or tea without additives or sweeteners per day during the 5-day program.
�
Resume Normal Healthy Diet
At the end of the program on Day 6
Liquid foods, such as soups and fruit juices
Light meals: rice, pasta, small portions of fish/meat/legumes
Avoid binge eating
Fast Performance
�
The Expectations?
Individuals taking ProLon� a have reported
Improved energy levels
Less fatigue
Softer and shinier skin
A positive impact on lifestyle
Making healthier choices and eating less
How Often Should Somebody Take The 5-Day ProLon� Diet?
The ProLon clinical trials protocol included three consecutive cycles of ProLon (5-day only per month over three consecutive months). It is up to the practitioner to decide the best method that he or she would like to use for each patient. It is suggested that for patients who are obese or overweight, to use ProLon for one three cycle protocol, and recommend that you check with your doctor to re-assess and determine if they have met their goals or if more cycles would be helpful. If a patient is not overweight and eats and exercises well, it is suggested to take the product 1-2 times a year.
Caution
Due to the low caloric nature of the ProLon� 5-day meal program, Individuals should not take ProLon� in combination with prescription or non-prescription drugs unless approved by your healthcare professional.
Drink at least 8 cups of water to minimize the risk of dehydration.
Avoid alcohol consumption, strenuous exercise, and exposure to high temperatures (e.g., saunas, spas, Jacuzzi) or cold environments and swimming.
Operate a motor vehicle and heavy machinery with care until it is known how ProLon� may affect you.
Clinical Methodology
Pre-clinical and clinical studies have proven that periodic fasting, done for several days, is a very powerful intervention that our bodies learned to naturally cope with by protecting and rejuvenating itself. The 5-Day ProLon Fasting Mimicking Diet has been clinically tested and found to promote beneficial effects in a wide variety of conditions ranging from excess weight and fasting blood glucose, to growth factors associated with DNA damage and aging.
A randomized control trial of 100 subjects
71 completed 3 cycles of the ProLon� either in a randomized phase (N=39) or
After being crossed over from a control diet group to the FMD group (N=32)
Control subjects continued with a normal diet.
ProLon� participants consumed the fasting mimicking diet (FMD) for 5 days per month for 3 months.
Measurements were performed prior to the diet (Before) and (During) the recovery period and (After) the 3rd cycle.
�
Clinical Results
Elevated Risk Results
ProLon� is clinically tested, an�easy-to-take 5-day meal program that enhances your health without dramatic lifestyle changes
Pre-Clinical Trials
In the first study from the Clinical and Translational Report, yeast deprived of food periodically were shown to have longer life expectancy than yeast fed normally.
The second study involved feeding a group of mice a specialized diet for four days a month.
The diet reduced both caloric intake and protein intake.
The scientists tested markers in the blood of the mice and found that the diet emulated prolonged water-only fasting.
After returning to regular feeding, the mice regained most, but not all of the lost weight.
Differences between the Fasting Mimicking Diet group and the control group include improved metabolism and cognitive function, gradual weight loss, muscle rejuvenation, higher bone density, 40% fewer malignant lymphomas, immune system regeneration, and longer average life expectancy.
A Third Study
There were nineteen participants and nineteen control participants with a broad range of ages (19-75).
Members of both sexes and various races so that the study represented a general cross-section of, adult population.
The individuals in the Fasting Mimicking Diet group were provided with the food they were required to eat during the five days.
Scientists were happy with the compliance level of the diet, and most reported only mild or no negative effects on the fast days.
Results showed that the FMD participants experienced an average:
Individuals diagnosed with serious medical condition or disease unless approved in writing by a physician appropriately trained to treat that condition
Individuals who have been severely weakened by a disease or medical procedure
Individuals who are taking medications which may not be safely consumed with a calorie restricted diet unless authorized in writing by a licensed physician
Individuals with Diabetes (type 1 and type 2), cardiovascular disease and cancer, unless approved in writing by a licensed physician. ProLon� should never be combined with glucose-lowering drugs, such as metformin or insulin
Fasting is prohibited for individuals with particular metabolic diseases, such as those affecting gluconeogenesis.
Individuals with a history of significant cardiac disease, particularly uncompensated congestive heart failure NYHA grade 2 or more or LVEF <40% on any prior assessment
Individuals with a history of syncope (fainting) with calorie restriction or other medical co-morbidities Individuals who have special dietary needs that are incompatible with the ProLon� meal plan
Individuals with liver or kidney disorders that may be affected by very low glucose and protein content of the diet
Chiropractic Weight Loss Treatment
Two decades of scientific discoveries at the University of Southern California.
Nutritional-Tech
All natural, plant-based, high-quality food and supplements
Experience the benefits of fasting, but with natural foods
Conveniently packaged in single-serve portions for each day of the program
ProLon� Can
Decrease body fat
Decrease body weight
Preserve lean body mass
60% weight loss maintained 3 months after resuming a normal diet
Maintain Levels
Blood glucose
Blood pressure
Cholesterol
Triglycerides
C-reactive proteins
Stem cells Insulin-like growth factor 1 (IGF-1
Meals
The Program Itself
Consume the ProLon� meal program�s components for five consecutive days
Do not consume any additional food/liquid other than water or herbal teas without caffeine or additives
In order to maximize the benefits, you should minimize your consumption of caffeine to 1 cup of coffee or tea without additives or sweeteners per day during the 5-day program.
�
Resume Normal Healthy Diet
At the end of the program on Day 6
Liquid foods, such as soups and fruit juices
Light meals: rice, pasta, small portions of fish/meat/legumes
Avoid binge eating
Fast Performance
�
The Expectations?
Individuals taking ProLon� a have reported
Improved energy levels
Less fatigue
Softer and shinier skin
A positive impact on lifestyle
Making healthier choices and eating less
How Often Should Somebody Take The 5-Day ProLon� Diet?
The ProLon clinical trials protocol included three consecutive cycles of ProLon (5-day only per month over three consecutive months). It is up to the practitioner to decide the best method that he or she would like to use for each patient. It is suggested that for patients who are obese or overweight, to use ProLon for one three cycle protocol, and recommend that you check with your doctor to re-assess and determine if they have met their goals or if more cycles would be helpful. If a patient is not overweight and eats and exercises well, it is suggested to take the product 1-2 times a year.
Caution
Due to the low caloric nature of the ProLon� 5-day meal program, Individuals should not take ProLon� in combination with prescription or non-prescription drugs unless approved by your healthcare professional.
Drink at least 8 cups of water to minimize the risk of dehydration.
Avoid alcohol consumption, strenuous exercise, and exposure to high temperatures (e.g., saunas, spas, Jacuzzi) or cold environments and swimming.
Operate a motor vehicle and heavy machinery with care until it is known how ProLon� may affect you.
Clinical Methodology
Pre-clinical and clinical studies have proven that periodic fasting, done for several days, is a very powerful intervention that our bodies learned to naturally cope with by protecting and rejuvenating itself. The 5-Day ProLon Fasting Mimicking Diet has been clinically tested and found to promote beneficial effects in a wide variety of conditions ranging from excess weight and fasting blood glucose, to growth factors associated with DNA damage and aging.
A randomized control trial of 100 subjects
71 completed 3 cycles of the ProLon� either in a randomized phase (N=39) or
After being crossed over from a control diet group to the FMD group (N=32)
Control subjects continued with a normal diet.
ProLon� participants consumed the fasting mimicking diet (FMD) for 5 days per month for 3 months.
Measurements were performed prior to the diet (Before) and (During) the recovery period and (After) the 3rd cycle.
�
Clinical Results
Elevated Risk Results
ProLon� is clinically tested, an�easy-to-take 5-day meal program that enhances your health without dramatic lifestyle changes
Pre-Clinical Trials
In the first study from the Clinical and Translational Report, yeast deprived of food periodically were shown to have longer life expectancy than yeast fed normally.
The second study involved feeding a group of mice a specialized diet for four days a month.
The diet reduced both caloric intake and protein intake.
The scientists tested markers in the blood of the mice and found that the diet emulated prolonged water-only fasting.
After returning to regular feeding, the mice regained most, but not all of the lost weight.
Differences between the Fasting Mimicking Diet group and the control group include improved metabolism and cognitive function, gradual weight loss, muscle rejuvenation, higher bone density, 40% fewer malignant lymphomas, immune system regeneration, and longer average life expectancy.
A Third Study
There were nineteen participants and nineteen control participants with a broad range of ages (19-75).
Members of both sexes and various races so that the study represented a general cross-section of, adult population.
The individuals in the Fasting Mimicking Diet group were provided with the food they were required to eat during the five days.
Scientists were happy with the compliance level of the diet, and most reported only mild or no negative effects on the fast days.
Results showed that the FMD participants experienced an average:
Individuals diagnosed with serious medical condition or disease unless approved in writing by a physician appropriately trained to treat that condition
Individuals who have been severely weakened by a disease or medical procedure
Individuals who are taking medications which may not be safely consumed with a calorie restricted diet unless authorized in writing by a licensed physician
Individuals with Diabetes (type 1 and type 2), cardiovascular disease and cancer, unless approved in writing by a licensed physician. ProLon� should never be combined with glucose-lowering drugs, such as metformin or insulin
Fasting is prohibited for individuals with particular metabolic diseases, such as those affecting gluconeogenesis.
Individuals with a history of significant cardiac disease, particularly uncompensated congestive heart failure NYHA grade 2 or more or LVEF <40% on any prior assessment
Individuals with a history of syncope (fainting) with calorie restriction or other medical co-morbidities Individuals who have special dietary needs that are incompatible with the ProLon� meal plan
Individuals with liver or kidney disorders that may be affected by very low glucose and protein content of the diet
Chiropractic Weight Loss Treatment
Two decades of scientific discoveries at the University of Southern California.
Nutritional-Tech
All natural, plant-based, high-quality food and supplements
Experience the benefits of fasting, but with natural foods
Conveniently packaged in single-serve portions for each day of the program
ProLon� Can
Decrease body fat
Decrease body weight
Preserve lean body mass
60% weight loss maintained 3 months after resuming a normal diet
Maintain Levels
Blood glucose
Blood pressure
Cholesterol
Triglycerides
C-reactive proteins
Stem cells Insulin-like growth factor 1 (IGF-1
Meals
The Program Itself
Consume the ProLon� meal program�s components for five consecutive days
Do not consume any additional food/liquid other than water or herbal teas without caffeine or additives
In order to maximize the benefits, you should minimize your consumption of caffeine to 1 cup of coffee or tea without additives or sweeteners per day during the 5-day program.
�
Resume Normal Healthy Diet
At the end of the program on Day 6
Liquid foods, such as soups and fruit juices
Light meals: rice, pasta, small portions of fish/meat/legumes
Avoid binge eating
Fast Performance
�
The Expectations?
Individuals taking ProLon� a have reported
Improved energy levels
Less fatigue
Softer and shinier skin
A positive impact on lifestyle
Making healthier choices and eating less
How Often Should Somebody Take The 5-Day ProLon� Diet?
The ProLon clinical trials protocol included three consecutive cycles of ProLon (5-day only per month over three consecutive months). It is up to the practitioner to decide the best method that he or she would like to use for each patient. It is suggested that for patients who are obese or overweight, to use ProLon for one three cycle protocol, and recommend that you check with your doctor to re-assess and determine if they have met their goals or if more cycles would be helpful. If a patient is not overweight and eats and exercises well, it is suggested to take the product 1-2 times a year.
Caution
Due to the low caloric nature of the ProLon� 5-day meal program, Individuals should not take ProLon� in combination with prescription or non-prescription drugs unless approved by your healthcare professional.
Drink at least 8 cups of water to minimize the risk of dehydration.
Avoid alcohol consumption, strenuous exercise, and exposure to high temperatures (e.g., saunas, spas, Jacuzzi) or cold environments and swimming.
Operate a motor vehicle and heavy machinery with care until it is known how ProLon� may affect you.
Clinical Methodology
Pre-clinical and clinical studies have proven that periodic fasting, done for several days, is a very powerful intervention that our bodies learned to naturally cope with by protecting and rejuvenating itself. The 5-Day ProLon Fasting Mimicking Diet has been clinically tested and found to promote beneficial effects in a wide variety of conditions ranging from excess weight and fasting blood glucose, to growth factors associated with DNA damage and aging.
A randomized control trial of 100 subjects
71 completed 3 cycles of the ProLon� either in a randomized phase (N=39) or
After being crossed over from a control diet group to the FMD group (N=32)
Control subjects continued with a normal diet.
ProLon� participants consumed the fasting mimicking diet (FMD) for 5 days per month for 3 months.
Measurements were performed prior to the diet (Before) and (During) the recovery period and (After) the 3rd cycle.
�
Clinical Results
Elevated Risk Results
ProLon� is clinically tested, an�easy-to-take 5-day meal program that enhances your health without dramatic lifestyle changes
Pre-Clinical Trials
In the first study from the Clinical and Translational Report, yeast deprived of food periodically were shown to have longer life expectancy than yeast fed normally.
The second study involved feeding a group of mice a specialized diet for four days a month.
The diet reduced both caloric intake and protein intake.
The scientists tested markers in the blood of the mice and found that the diet emulated prolonged water-only fasting.
After returning to regular feeding, the mice regained most, but not all of the lost weight.
Differences between the Fasting Mimicking Diet group and the control group include improved metabolism and cognitive function, gradual weight loss, muscle rejuvenation, higher bone density, 40% fewer malignant lymphomas, immune system regeneration, and longer average life expectancy.
A Third Study
There were nineteen participants and nineteen control participants with a broad range of ages (19-75).
Members of both sexes and various races so that the study represented a general cross-section of, adult population.
The individuals in the Fasting Mimicking Diet group were provided with the food they were required to eat during the five days.
Scientists were happy with the compliance level of the diet, and most reported only mild or no negative effects on the fast days.
Results showed that the FMD participants experienced an average:
Individuals diagnosed with serious medical condition or disease unless approved in writing by a physician appropriately trained to treat that condition
Individuals who have been severely weakened by a disease or medical procedure
Individuals who are taking medications which may not be safely consumed with a calorie restricted diet unless authorized in writing by a licensed physician
Individuals with Diabetes (type 1 and type 2), cardiovascular disease and cancer, unless approved in writing by a licensed physician. ProLon� should never be combined with glucose-lowering drugs, such as metformin or insulin
Fasting is prohibited for individuals with particular metabolic diseases, such as those affecting gluconeogenesis.
Individuals with a history of significant cardiac disease, particularly uncompensated congestive heart failure NYHA grade 2 or more or LVEF <40% on any prior assessment
Individuals with a history of syncope (fainting) with calorie restriction or other medical co-morbidities Individuals who have special dietary needs that are incompatible with the ProLon� meal plan
Individuals with liver or kidney disorders that may be affected by very low glucose and protein content of the diet
Fasting offers numerous health benefits, from increasing insulin sensitivity and promoting weight loss to enhancing the immune system. Although we all want the benefits of fasting, many of us can’t embrace the idea of not eating for extended periods of time. However, what if you could achieve all the healthy advantages of a fast without having to skip meals?
The fasting mimicking diet, sometimes abbreviated as FMD, is a nutritional regimen. It consists of eating natural ingredients for five days which “tricks” the human body into a fasting mode. Research studies have demonstrated the fasting mimicking diet’s ability to improve overall health and wellness. Below, we will discuss the benefits of the fasting mimicking diet.
How Does the Fasting Mimicking Diet Work?
By restricting the food you eat, the fasting mimicking diet can provide similar health benefits as traditional fasting like reduced inflammation and fat burning. The difference, however, is that instead of not eating any food for several days or weeks, you’re simply limiting your calorie intake for five days. You can do the FMD once a month or every other month to promote well-being.
The ProLon� fasting mimicking diet, 5-day meal program offers individually packed and labeled foods for each day in precise quantities and combinations. The meal program consists of ready-to-eat or easy-to-prepare, plant-based foods, such as bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting.
FMD Macronutrient Ratios
First, you will restrict your calories to 1,100 calories on day one of the FMD. Then, you will restrict your calories to 800 calories on the other four days. What you eat and in what ratios you eat those foods is fundamental in the fasting mimicking diet. Healthcare professionals will recommend different ratios of macronutrients, the three basic components of every diet.
The most common recommendation is to eat 1,100 calories following a macronutrient ratio of 34 percent carbohydrates, 10 percent proteins, and 56 percent fats on day one. For the remaining four days, the most common recommendation is to eat 800 calories following a macronutrient ratio of 47 percent carbohydrates, 9 percent proteins, and 44 percent fats.
Other healthcare professionals recommend a macronutrient ratio with as much as 80 percent of calories coming from fat, and 10 percent from carbohydrates and proteins, respectively. According to Dr. Valter Longo, creator of the FMD, “the fasting mimicking diet allows the natural process of starvation, including autophagy, and stem cell regeneration, to occur without interruption.
The Science Behind the FMD
Research studies have demonstrated that limiting calorie intake provides many benefits for the lifespan of animals. However, what does the science say about the benefits of the fasting mimicking diet on humans? A recent research study evaluated the effects of the FMD in people and found some promising outcome measures. The research study was conducted on 100 healthy participants.
Half of the participants followed the ProLon� fasting mimicking diet, 5-day meal program every month and the other half of the participants followed a regular diet. After three months, the FMD group experienced weight loss, including visceral fat reduction, as well as decreased blood glucose, blood pressure, and markers of inflammation. The FMD group also experienced a drop in insulin-like growth factor 1, more frequently known as 1GF-1, which is considered to be a biomarker for cancer development.
The ProLon� fasting mimicking diet, 5-day meal program provides numerous health benefits while providing balanced nourishment. The FMD can promote weight loss as well as maintain healthy levels of blood glucose, BP, cholesterol, and triglycerides, C-reactive proteins, stem cells, and insulin-like growth factor 1 or IGF-1. Following the FMD alongside healthy lifestyle modifications can help improve overall health and wellness. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Other Fasting Mimicking Diet Benefits
The FMD has been demonstrated to give you protective, regenerative, and rejuvenating advantages while continuing to provide you with the balanced nourishment you need. Below, we will discuss several other health benefits of the fasting mimicking diet.
Decreases Cholesterol
The same research study mentioned above also demonstrated that after three months, the FMD group experienced decreased levels of total and bad LDL cholesterol. When we have increased levels of cholesterol in our blood, it can cause plaque to build up in our arteries, causing the hardening, and the narrowing of the arteries. This may lead to a heart attack and coronary heart disease. If you combine the FMD with lifestyle modifications, you can lower and maintain healthy cholesterol levels and keep your heart healthy.
Reduces Inflammation
We already mentioned that the FMD research study demonstrated it could decrease inflammation. However, we should first discuss what inflammation is and what it can do to the human body. Inflammation is one of the human body’s defense mechanisms. Your inflammation is triggered by your immune system to protect you from foreign invaders that could cause infection, illness, or injury.
By way of instance, let’s imagine you get a splinter in your finger. Your finger will become red and inflamed almost immediately. Your body is utilizing inflammation to protect itself from this foreign object. When you get a cut or an insect bite, the same holds true. However, how does inflammation affect our well-being? Chronic inflammation can lead to many chronic diseases, such as heart disease, diabetes, multiple sclerosis, and cancer. The FMD has the potential to reduce the possibility of developing chronic diseases.
Improves Brain Health
The fasting mimicking diet can also help improve our brain health. In a 2015 animal research study, the FMD improved cognition and promoted the regeneration of neurons in the brains of mice. Additionally, it decreased the markers of aging in the subjects.
Can Help Reverse Diabetes
The FMD can positively affect insulin production. In another animal research study, blood glucose levels were preserved and more insulin-producing beta cells were produced in mice. The Science Translational Medicine research study also demonstrated that the participants following the FMD experienced a reduction in glucose levels. Although further evidence is required, there are strong indications that healthy lifestyle modifications can help control and even reverse diabetes.
How to Start the Fasting Mimicking Diet
I encourage you to work with your healthcare professional if you’re interested in the FMD. You will also need advice and guidance from a qualified healthcare professional to help you decide on your proper macronutrient ratios. In summary, you should be eating a diet full of plant-rich whole foods, with an emphasis on nuts and olives. You could also eat soups and broths as well as herbal teas.
Make sure you also avoid the consumption of alcohol and carbonated drinks. Instead, you can drink two cups of black tea or coffee. Furthermore, you shouldn’t exercise vigorously during those five days. Consider taking a gentle walk around the block.
Research studies have demonstrated promising results with the fasting mimicking diet. However, the FMD may not be for everyone. Pregnant women and older adults shouldn’t try the FMD. If you’d like to experience the health benefits of the FMD yourself, talk with your doctor and/or a nutritionist. Doing more than one cycle every month could ultimately affect your overall health and wellness.
The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Aracely Pisana saw Dr. Alex Jimenez, doctor of chiropractic in El Paso, Tx, for the very first time after many other treatment efforts were not able to supply her with the back pain relief she’d needed. Aracely Pisana describes how well Dr. Alex Jimenez and his staff have taken care of her and she adds that their services are what keeps her coming back to chiropractic care. Aracely Pisana has recovered her quality of life and she highly recommends Dr. Alex Jimenez as the non-surgical selection for back pain.
Chiropractic Treatment
�
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Now in the heart of the school year � new shoes, haircuts, homework, and their bulging backpacks. Think about the backpack your child is carrying. Sure, they load them up with books, but did you know that wearing a heavy backpack for a long time can actually hurt your child? The American Academy of Pediatrics (AAP) has provided some helpful guidelines for choosing a backpack for your child and avoiding the injury that can result from one that is too heavy.
What are the health risks of a heavy backpack?
Wearing a heavy backpack can strain the shoulders, back, and neck. As the child�s body tries to compensate for the extra weight, such as leaning forward, it can adopt positions that put the spine out of alignment. It can also cause the muscles to fatigue and weaken. This results in poor posture and a misaligned spine.
The longer he or she carries the extra weight, the worse it gets. Over time, the child can experience pain, stiffness, and problems with flexibility and range of motion. This can significantly increase the child�s potential for injury. The effects may include backache, sore or stiff neck, sore shoulders, and headaches.
How heavy is too heavy for a child�s backpack?
According to the AAP, a child�s backpack should weigh less than 10 to 20 percent of his or her body weight � and no more. However, a Consumer Reports survey showed that the lower end of the range, around 10 percent or less, is preferable. In short, the lighter the backpack, the healthier it is for your child. A good rule of thumb is to observe your child wearing the backpack. If they are stooped or leaning forward, it is too heavy.
Children who are shorter, as well as girls, may be more prone to back pain caused by carrying heavy backpacks. This means that for these children you need to aim for even lighter weights. Children who are overweight may also be at risk for injury. The excess weight already puts a strain on their joints and muscles; the heavy backpack exacerbates the situation.
Children who wear their backpack over one shoulder also increase their risk of injury. This puts all the weight on one side, causing the child to bend or lean in an effort to compensate for the off-kilter weight. This can strain the shoulder and back, eventually causing injury and pain.
Helping your child avoid carrying a heavy backpack.
If you notice that your child cannot stand up straight while wearing the backpack, then it is too heavy. You should inspect your child�s backpack on a regular basis to test the heaviness. When purchasing a backpack, aim for wide, padded straps that are adjustable. It should fit the child well and to be too big. The straps should not be too loose. You want it to fit close to your child�s body and should come to just below the waist � but not too far. Don�t allow your child to carry the backpack on one shoulder, encourage them to wear it on both shoulders. This distributes the weight more evenly.
If your child is carrying a heavy backpack, you may need to talk to their teacher to see what is necessary for him or her to carry daily, and what can be left at home or at school. Work together to find ways to lighten the load and avoid injury. Also, keep in mind, your child may not bring your attention to the fact that their backpack is too heavy. It is up to you to observe and intervene for them.
The fasting mimicking diet is an alternative to fasting. However, it can have several benefits for your overall health and wellness. We will discuss everything you need to know about the regimen. The article below describes how to do it, its benefits, and how it’s different from normal fasting. The benefits of the fast mimicking diet will have you wanting to try it for yourself.
What is the Fasting Mimicking Diet?
The fasting mimicking diet is a type of modified fasting. The regimen produces the same benefits of fasting by eating small amounts of food. The fast mimicking diet generally lasts about five days and it includes a healthy protocol of carbohydrates, proteins, and fats.
Calories are also maintained at approximately 40 percent of the average calorie intake. This permits the human body to remain nourished without the stress of normal fasting. Calorie restriction can cause health issues, however, the fast mimicking diet is safe and effective. Below, we will discuss just how much the fast mimicking diet differs from traditional fasting.
Traditional Fasting Vs Fast Mimicking Diet
The fasting mimicking diet is always compared to intermittent fasting. There are many myths about these types of modified fasts. Some claim that our muscles waste away while others claim that they change our metabolism, and that it’s downright unhealthy.
The health issues discussed above may be true for a person who’s actually restricting their calorie intake. Some types of fasting may cause metabolic damage which may not be recommended for people with underlying health conditions. However, the fast mimicking diet gives you all the advantages of fasting without the side effects. Below are the benefits of the fast mimicking diet.
Benefits of the Fast Mimicking Diet
The benefits of the fast mimicking diet are essentially the same as those of regular fasting. The benefits are listed below.
The fast mimicking diet “tricks” the human body into feeling as though it’s fasting. Now that we have discussed what this alternate form of fasting is and why it is worth doing, the following advice will demonstrate how to do the diet itself.
How to do the Fast Mimicking Diet
Research studies have found that the best results for the fasting mimicking diet occur in about five days or when your glucose ketone index drops below 1.0. Doing this regimen anywhere between 3 to 7 days is also beneficial. The regimen should also be repeated every month to fully experience its benefits, unless otherwise instructed by a healthcare professional.
If you’re interested in monitoring your fasting outcomes, you should consider quantifying specific biomarkers. This could be measured through lab tests before and after following the fasting mimicking diet. Measuring blood glucose, ketones, and weight changes every day can also be helpful to determine your biomarkers. You might also want to set up your environment by:
Telling friends and family about what you are doing and asking them for their support.
Eliminating any snack foods at home or work that might interrupt your regimen.
Giving yourself more time to sleep, as you will probably be more exhausted than usual.
Planning for exercise and physical activity every day. But keep away from intense workouts during this time.
Now that we discussed how you can do the diet, let’s discuss the basics of the fast mimicking diet.
The fasting mimicking diet provides the same great benefits of fasting while still providing your body with some nourishment. If you are following this regimen, make sure that you maintain a low-calorie intake and utilize appropriate supplements to achieve ketosis without experiencing health issues. Set up your environment for the diet. And if you decide to blend the ketogenic diet with this alternate form of fasting to get into ketosis faster, you can achieve the maximum advantages out of the two regimens. Be sure to consult a healthcare professional before following the fasting mimicking diet. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Fasting Mimicking Diet Basics
Some people today might eat a slightly higher amount of calories the first day as they ease into the fasting mimicking diet. They might then decrease their total caloric intake. You also want to make sure you eat smaller amounts of foods which are easy to digest.
ProLon� offers a pre-packaged box which contains all five days’ worth of meals for you to do the diet. The meals are all plant-based. One day, by way of instance, offers tea and a nut bar for breakfast, a small portion of vegetable soup and a few kale crackers for lunch, several olives in the afternoon, and finally another small portion of vegetable soup for dinner.
You can also do the fasting mimicking diet without the need for a pre-packaged box like ProLon�. Simply follow the right proportions and plan out how you will space them out every day. Macros for the fast mimicking diet are 34 percent carbohydrates, 10 percent protein, and 56 percent fat for the very first day and 47 percent carbohydrates, 9 percent protein, and 44 percent fat to the rest days.
A cup of black tea and coffee every day are generally allowed. Just make sure they don’t contain any added sugars or oils. Remember that people with health issues should consult a healthcare professional prior to doing the fast mimicking diet in your own home.
Foods
Dr. Anthony Gusting followed a four-day ketogenic fasting mimicking diet. Every day, he consumed different amounts of bone broth, coconut milk, coconut oil, BCAAs, and exogenous ketones. Avocados and grass-fed butter can also be included in the fast mimicking diet. This is a great way to combine the ketogenic diet with the fasting mimicking�diet to benefit from the two regimens.
Supplements
Taking nutritional supplements can also make the fasting mimicking diet easier by providing enough nutrition. These may include:
Electrolytes like magnesium and salt to replenish any lost during water loss
Grass-fed liver tablets to provide micronutrient support
Branch chain amino acids, or BCAAs, to help prevent loss of lean tissue
Greens powder to provide micronutrients
Algal oil or cod liver oil for omega-3s
You may also take exogenous ketones to achieve ketosis through the keto diet. The fast mimicking diet can also help you achieve ketosis before following a ketogenic diet. Below, we will discuss how the fast mimicking diet promotes ketosis.
Ketosis and the Fast Mimicking Diet
The fast mimicking diet is an excellent way to prepare you for the ketogenic diet. This is because it allows you to get into ketosis. Additionally, eating keto foods makes it possible to remain in ketosis throughout the regimen. To follow a ketogenic fasting mimicking diet you must maintain your macros over the suitable range of 5 to 10 percent of carbohydrates, 20 to 25percent of proteins, and 70 to 80 percent of fats. If you’re unsure about whether you’re properly maintaining your macros, always choose something with more fat.
The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
It is estimated that scoliosis affects anywhere from 2 to 3 percent of children and adults in the United States. That is roughly six to nine million people. While it seems to develop most commonly within specific age ranges for boys and girls, it can also develop in infancy. Every year, approximately 30,000 children are fitted with a scoliosis back brace while 38,000 people have spinal fusion surgery to correct the problem. Scoliosis screenings can have tremendous benefits by identifying both risk factors for scoliosis and allowing for early treatment.
The earlier you detect scoliosis, the easier it is to treat.
Scoliosis typically develops in childhood. For girls, it usually occurs between 7 and 14 years of age. Boys develop it a little later, between 6 and 16 years of age.
Getting a scoliosis screening each year during these critical age ranges allow doctors to identify the condition early and begin treating it before it gets serious. Advanced scoliosis can require extensive treatments, bracing, and even surgery.
Chiropractic has been shown to help scoliosis, as do stretching, special exercises, and physical therapy. There are spinal adjustments that chiropractors do that are specific to the treatment of scoliosis.
When addressing the condition early on, the Cobb angle can be stopped from progressing and even reduced so that the spine has a more natural curve. Non-surgical treatments tend to be much more effective in the earlier stages of scoliosis, so early detection and early diagnosis are critical.
Identifying high-risk cases early can address current issues and prevent future ones.
Chiropractors can identify certain scoliosis risk factors in children before the condition even develops. A scoliosis screening allows them to spot tension in a child�s spinal cord � a common sign that they will develop scoliosis.
When parents are aware that their child is in a high-risk category for developing scoliosis, they can take proactive measures with home monitoring for the signs of scoliosis as well as keeping up with the course of recommended screenings. They will know to look for the signs and can address them quickly so that treatment can be started at the earliest possible time.
Help researchers and doctors become more effective in treating scoliosis.
The early stages and development of scoliosis are still shrouded in mystery for researchers and doctors. While there have been great strides made in better understanding the condition, there is still much left to learn.
There have been many studies that have aided doctors in identifying high-risk children and making early stage diagnoses, such as how the�angle of the ankle and foot are linked to scoliosis. However, screening, diagnosis, and treatment are vital to maintaining the flow of data for more studies to be conducted and more research to be done.
More mainstream screenings mean�identifying more cases of scoliosis at the early stages. This would have a two-prong effect on research. It would provide more data to be reviewed and studied, and it would increase interest in the condition as more cases of early stage scoliosis is found. This would further spur research.
Avoid the �waiting game� of seeing if scoliosis will progress.
Any parent who has had to wait for the results of a test or to see if a condition will develop or worsen knows well the anxiety of playing that waiting game. A family is usually the first person to discover scoliosis in a child.
While they may suspect a problem, or know that a problem exists, they may take a �wait and see� approach in getting treatment. If the curve worsens they may eventually seek treatment, but the constant nagging of not knowing if the curve will get worse � and the anxiety it produces � can impact not only the parents� peace of mind�but the child�s as well.
Scoliosis screenings provide peace of mind and monitor the child�s development so that if their scoliosis does progress or become a problem it can be addressed in the quickest, most efficient way possible.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine