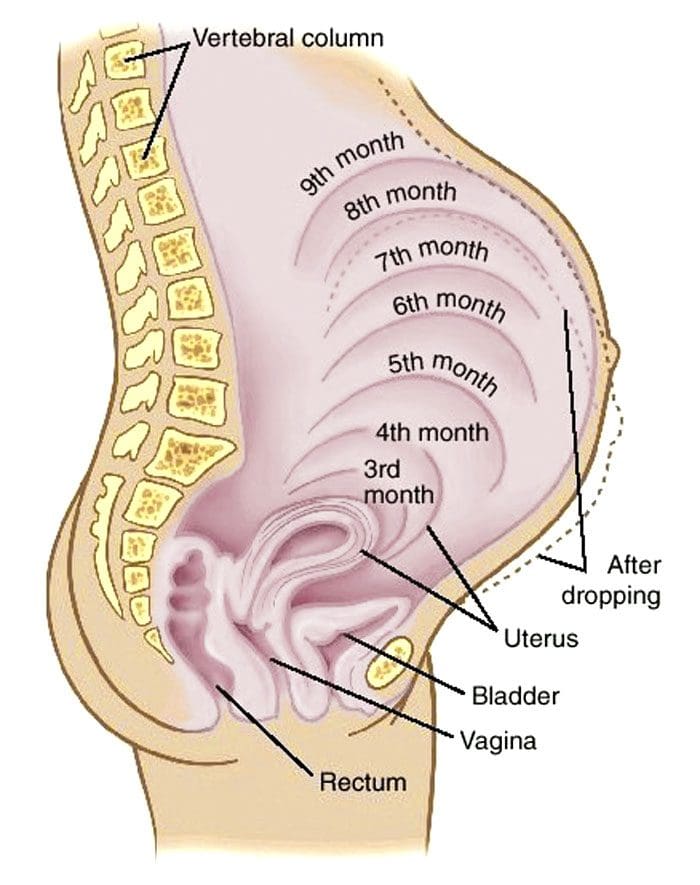
Pregnant and Chiropractic: Many women experience back/pelvis/leg/feet swelling, soreness, achiness, and pain during pregnancy. A growing belly added weight and changes in connective tissue can cause a variety of musculoskeletal strains and misalignments. Chiropractic care provides health maintenance of the spinal column, discs, nerves, joints, muscles, and bones. It is an art and science of adjusting a misaligned body, reducing stress, and promoting health throughout the body.
Pregnant and Chiropractic
With a primary doctor’s clearance, chiropractic can provide safe adjustments. Chiropractors trained to work with pregnant women utilize techniques that avoid applying pressure on or around the abdomen. Benefits of chiropractic during pregnancy include:
Restores and maintains spinal alignment and balance.
Helps control symptoms of nausea.
Improves energy levels.
Relieves body pain.
Helps reduce labor time and delivery.
Restores pelvic positioning and balance, improving standing, sitting, and walking mechanics.
A chiropractor trained in the needs of pregnant women will also provide exercises and stretches that are safe during pregnancy. A chiropractor will discuss/recommend treatment options, patient concerns, and a complete medical history assessment. They will monitor symptoms to customize treatments to the individual’s specific needs to get the most relief.
Body Composition
Gestational Hypertension
Gestational hypertension develops during pregnancy. It is not preventable and returns to normal levels postpartum. However, there is an increased risk of developing chronic hypertension later if gestational hypertension begins to develop. According to Mayo Clinic, gestational hypertension is diagnosed by the following:
Blood pressure is higher than 140/90 on at least two occasions.
Must be more than four hours apart.
There is no other organ damage present.
References
Gutke, Annelie et al. “Treatments for pregnancy-related lumbopelvic pain: a systematic review of physiotherapy modalities.” Acta Obstetricia et Gynecologica Scandinavica vol. 94,11 (2015): 1156-67. doi:10.1111/aogs.12681
Poděbradská, R et al. “The effect of physiotherapy intervention on the load of the foot and low back pain in pregnancy.” “Vliv fyzioterapeutických postupů na zatížení plosky a bolesti zad v těhotenství.” Ceska gynekologie vol. 84,6 (2019): 450-457.
Schreiner, Lucas et al. “Systematic review of pelvic floor interventions during pregnancy.” International journal of gynecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics vol. 143,1 (2018): 10-18. doi:10.1002/ijgo.12513
For older individuals, experiencing frequent low back pain could turn out to be a sacral fracture. They tend to occur in individuals over the age of 60 often because there has been a degree of bone loss. Sacral fractures tend not to be the first thing doctors think of when low back pain symptoms are presenting. They are often not picked up on X-rays and are either not diagnosed early enough to take steps or not diagnosed at all. However, they are common.
Sacrum
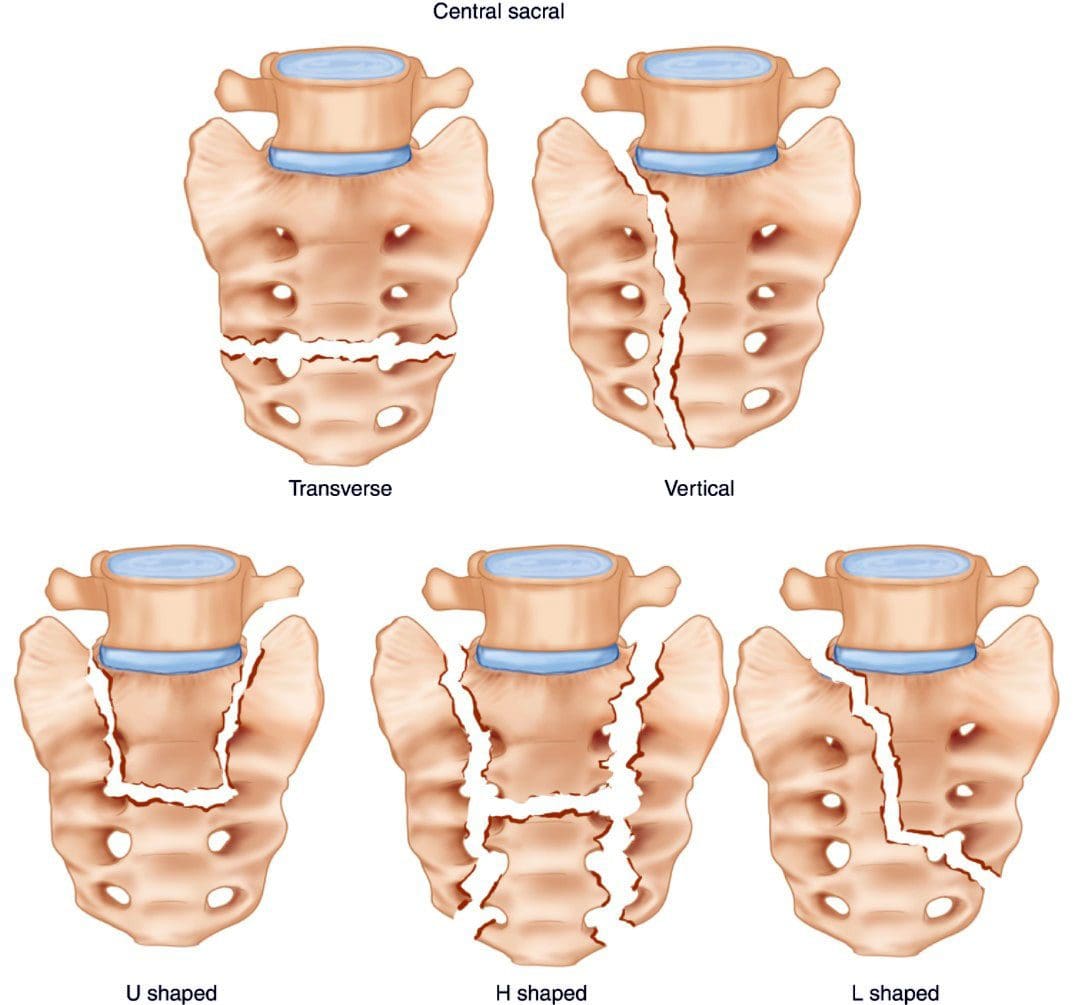
The sacrum is shaped like a triangle and comprises five segments fused into one large bone. It sits at the base of the spine, between the two halves of the pelvis, connecting the spine to the lower half of the body. It stabilizes the body when walking, sitting, or standing. The nerves in the lower spine control the bowels bladder and provide sensation to the region.
The two dimples that can be seen on individuals’ backs are where the sacrum joins the hipbones or the sacroiliac joint.
The point where the low back joins the sacrum can develop discomfort, soreness, and pain.
This area experiences stress from bending, twisting, reaching, lifting, carrying during physical activities or sitting for long periods.
Sacral Fracture
Most sacral fractures result from trauma, like slips, falls, and automobile accidents. Stress fractures that happen without a specific injury are also called insufficiency fractures.
Types of Sacral Fractures
Low-energy fractures usually happen to older individuals with weak bones due to osteoporosis.
An individual trips on something, lands hard on their butt, lifts a heavy object awkwardly, or over-exerts themselves from some physical activity.
Then persistent back or buttock pain begins to present.
The pain is often centered in the lower back, the hips, and butt.
It is more than just back achiness.
The individual goes to the doctor, and X-rays are ordered.
A lot of the time, these fractures are missed on X-rays.
The doctor may diagnose a sprain, but the pain symptoms do not improve.
Sometimes there is no apparent cause for the pain.
It can be misdiagnosed as a lower back compression fracture or urinary tract infection.
High-energy fractures are due to trauma and are more common among the young.
The individual sustains injuries from an auto accident, has fallen from a significant height, or suffers a sports injury.
It results in severe pain.
A woman who has just had a baby and gone through some bone loss because of the pregnancy can experience a sacral stress fracture.
For individuals that have been to a doctor and had an X-ray that reveals no fracture, and there is no improvement after 5 to 7 days, it is recommended to schedule another appointment and ask for a CAT scan or MRI, which is highly effective at finding a sacral fracture.
Treatment
Treatment consists of resting the bone but still being safely active in most cases.
Medication is prescribed for pain relief.
Many individuals have been found to do well with anti-inflammatory medications, topical medications, and lidocaine patches.
Older individuals may be recommended to use a walker during the treatment/healing process.
Depending on the severity, crutches may be recommended.
Engaging in regular exercise is not recommended, but too much bed rest is also not recommended.
Too much rest may not allow the injury to heal correctly, worsen the injury, and/or cause new injuries.
Chiropractic and physical therapy are not recommended to let the sacrum naturally heal.
After the pain subsides, chiropractic and physical therapy can be implemented to maintain agility and flexibility and strengthen the pelvic and core muscles.
In some cases, if the bone does not heal correctly or some other issue, sacroplasty could be recommended. This is a minimally invasive procedure that injects bone cement into the fracture. It offers quick and long-lasting pain relief with a low percentage of complications. It is considered low risk and can be done by an interventional radiologist or spine surgeon.
Prevention
To minimize the risk of a sacral fracture, it is highly recommended to maintain bone strength. This consists of:
Try to keep moving with different exercise stretches, or take a lap around the building.
References
Gibbs, Wende Nocton, and Amish Doshi. “Sacral Fractures and Sacroplasty.” Neuroimaging clinics of North America vol. 29,4 (2019): 515-527. doi:10.1016/j.nic.2019.07.003
Holmes, Michael W R, et al. “Evaluating Abdominal and Lower-Back Muscle Activity While Performing Core Exercises on a Stability Ball and a Dynamic Office Chair.” Human factors vol. 57,7 (2015): 1149-61. doi:10.1177/0018720815593184
Santolini, Emmanuele et al. “Sacral fractures: issues, challenges, solutions.” EFORT open reviews vol. 5,5 299-311. 5 May. 2020, doi:10.1302/2058-5241.5.190064
Post spine surgery physical therapy or PT is the next phase after a discectomy, laminectomy, fusion, etc., to gain optimal mobility and ease the transition for a full recovery. A chiropractor and physical therapist team will help with proper muscle training and activation, pain and inflammation relief, postural training, exercises, stretches, and educate the individual on an anti-inflammatory diet. Physical therapy post spine surgery reduces:
Scar tissue
Inflammation
Muscle weakness
Muscle tightness
Joint stiffness
The therapy also identifies and treats any issues that caused or contributed to the spinal damage/injury. A study found physical therapy to improve postoperative ambulation, pain, disability, and decreased surgical complications.
Post Spine Surgery Physical Therapy Goals
Physical therapy goals are to return the individual to full function before chronic pain or injury. These include:
Decrease pain and stress around the surgical site.
Loosen and stretch the muscles surrounding the surgical site.
Strengthen the back and neck muscles.
Stabilize the back and neck muscles.
Learn to move around safely.
Prepare for everyday physical activities like standing up or sitting down, lifting, and carrying objects.
Improve posture.
The therapy team will develop a customized treatment/rehabilitation plan as well as post-surgical recovery at home to help the individual and family to understand what to expect, including psychological factors like not wanting to perform the exercises or stretches to avoid pain, frustration, anger, depression, and wanting to give up. However, individuals can maximize the benefits to ensure an optimal outcome before surgery by pre-conditioning identifying structural and functional issues contributing to the injury.
Physical Therapy Involves
Therapy can be done at home, in a hospital or rehab setting, or at a chiropractic/physical therapy clinic. Therapists use:
A physical therapy session can last 45 minutes to an hour. It’s essential to discuss hopes and expectations post-surgery and after the therapy has finished. The therapists will explain the healing process, the treatment progression, and any questions a patient may have. Understanding the treatment process will help the individual want to engage in the treatment plan. The therapist team will also interface with the surgeon to prevent adverse outcomes.
Optimal Health
The physical therapy team will help the individual feel better with each session and stay motivated. Having a solid relationship with the therapy team makes it easier to share goals, worries, and challenges that the team can adapt to as progress is made. To gain the most from the therapy:
Try working with a therapist that the surgeon recommends can be helpful as they already have a working relationship.
Keep communication open between the surgeon and team.
Adhere to any precautions and restrictions set by the surgeon and therapy team.
Maintain recommended exercises at home between sessions.
Ease into activity and avoid overexertion.
Post spine surgery physical therapy helps accelerate the healing process and serves to help individuals regain their quality of life.
Body Composition
Power Of Protein
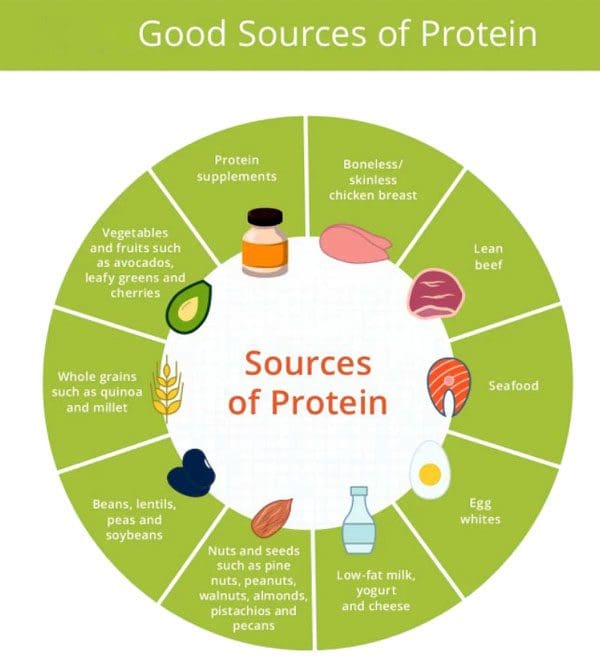
Protein is an essential component of muscle development, bone density, muscle mass, and lean tissue when building a healthy body. Protein is necessary for all the body’s physiological functions.
References
Adogwa, Owoicho et al. “Assessing the effectiveness of routine use of postoperative in-patient physical therapy services.” Journal of spine surgery (Hong Kong) vol. 3,2 (2017): 149-154. doi:10.21037/jss.2017.04.03
Atlas, S J, and R A Deyo. “Evaluating and managing acute low back pain in the primary care setting.” Journal of general internal medicine vol. 16,2 (2001): 120-31. doi:10.1111/j.1525-1497.2001.91141.x
Gellhorn, Alfred Campbell et al. “Management patterns in acute low back pain: the role of physical therapy.” Spine vol. 37,9 (2012): 775-82. doi:10.1097/BRS.0b013e3181d79a09
Jack, Kirsten et al. “Barriers to treatment adherence in physiotherapy outpatient clinics: a systematic review.” Manual therapy vol. 15,3 (2010): 220-8. doi:10.1016/j.math.2009.12.004
Lindbäck, Yvonne et al. “PREPARE: Pre-surgery physiotherapy for patients with degenerative lumbar spine disorder: a randomized controlled trial protocol.” BMC musculoskeletal disorders vol. 17 270. 11 Jul. 2016, doi:10.1186/s12891-016-1126-4
Sciatica motor vehicle crash. After an automobile crash/accident, symptoms of pain and discomfort can immediately follow the force of impact, indicating an injury. Many injuries and symptoms appear right away, like:
Pain from high-impact trauma and cuts.
Bone fractures.
Dislocations.
Neck whiplash.
Back pain.
The sciatic nerve is the largest in the body, and any damage can cause pain in one or both sides of the body. Pressure and compression on the nerves, ligaments, and muscles accompanied by weakness or numbness in the lower back, legs, or feet could cause delayed sciatica symptoms hours, days, even weeks later. It is critical to meet with a doctor and auto accident chiropractor after any type of accident, large or small, to develop a thorough personalized treatment plan.
Sciatica Motor Vehicle Crash
Sciatica can be brought on by a pinched nerve, which is often the result of the spine shifting out of place, causing herniation and compression on the sciatic nerve. The trauma from a motor vehicle accident can cause the spinal discs to be knocked out of place, rupture, and leak out, irritating the surrounding tissue and nerve endings. Back injuries are among the most common forms of damage/injury resulting from a motor vehicle accident/crash that can lead to sciatica. Broken and/or fractured vertebral, hip, or pelvis bone fragments can compress the sciatic nerve. Even when the initial result of the impact does not result in sciatica, over time, an untreated back injury could lead to sciatica symptoms.
Symptoms
Motor vehicle crashes often activate or aggravate pre-existing conditions like asymptomatic degenerative disc disease, affecting the sciatic nerve causing discomfort and pain. Common symptoms include:
Mild discomfort or achiness.
Tingling sensations from the lower back and down the back of the leg.
Weakness, numbness, or difficulty moving the leg and foot.
Inability to bend the foot upward at the ankle- known as foot drop.
Constant pain in one side of the buttocks or leg.
Sharp pain that makes it difficult to stand up and walk
Difficulty sitting.
Burning or tingling in one leg can worsen when sitting.
Intense pain.
Sharp burning and/or what feels like shooting electricity pain.
Diagnosis
A spine doctor and chiropractor will use diagnostic imaging tools like X-rays, and CT scans to see the scope of the injured area.
An X-ray will show a detailed image of the spine and affected bones in the area.
A CT scan will include a 3D image that shows the surrounding musculature, tissues, and nerves that could be damaged/injured.
Treatment
The doctor and chiropractor will then develop an appropriate and personalized treatment plan that could utilize various methods and techniques.
Chiropractic is commonly the first treatment to realign the spine and relieve pressure on the nerve.
A pain management specialist or physical therapist will be brought in for rehabilitation/recovery as adjustments progress.
Orthopedists and neurologists may be brought in for less conservative treatment in more severe cases, including surgical options.
Other treatments can include steroid injections or anti-inflammatory medicines to relieve nerve pressure.
Body Composition
Injury Rehabilitation Phase
Current in-clinic methods of measuring the composition of an injured body are indirect, while medically advanced techniques limit the frequency of testing. InBody provides cost-effective, comprehensive, and timely measurements that identify areas of weakness from damage, injury, or recent surgery and develop a customized rehabilitation program to improve functional status.
During the rehabilitation phase, increased sedentary behavior and/or immobilization causes muscle loss in the injured or operated region. By independently evaluating lean mass in each segment of the arms, legs, and torso, a chiropractor or physical therapist gathers baseline information on the body segments with restricted mobility.
InBody can help provide further insight into an individual’s body composition to analyze long-term health risks and develop a personalized exercise intervention to improve overall health and reduce health risks. This provides beneficial information for identifying potential imbalances related to muscle loss post-injury/surgery that can be targeted and improved. Identifying these imbalances allows the therapists to increase functional fitness and mobility, helping the individual reduce the risk of re-injury or new injuries.
References
Defouilloux, B et al. “A propos de trois observations chez des polytraumatisées de la route présentag une fracture du bassin associée à des signes neurologiques” [Apropos of 3 cases of multiple traffic injuries presenting pelvic fractures associated with neurologic signs]. Journal de radiologie, d’electrologie, et de medecine nucleaire vol. 48,8 (1967): 505-6.
Noble, J et al. “Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries.” The Journal of trauma vol. 45,1 (1998): 116-22. doi:10.1097/00005373-199807000-00025
Walsh, K et al. “Risk of low back pain in people admitted to hospital for traffic accidents and falls.” Journal of epidemiology and community health vol. 46,3 (1992): 231-3. doi:10.1136/jech.46.3.231
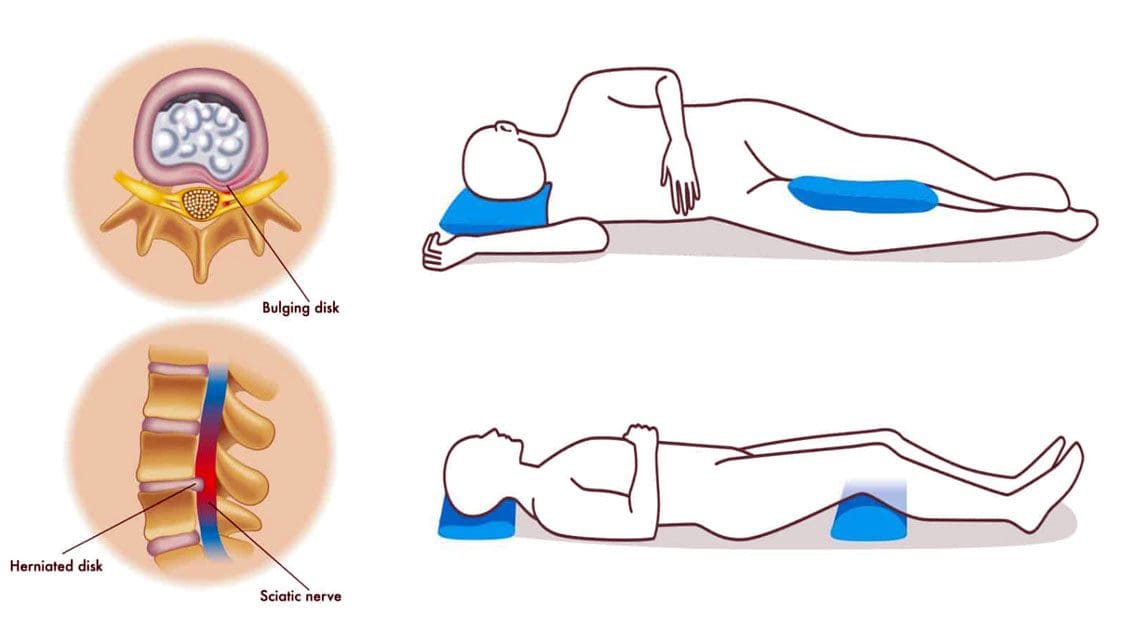
Sleeping with a bulging disc can be challenging for the body to achieve the proper rest. And sleeping in an awkward position can add stress to the spine, making the bulge worse, which can cause tingling, numbness, pain, and digestive problems. This can disrupt the sleep cycle and prevent proper healing of the spinal injury.
Sleeping With a Bulging Disc
When sleeping, most back pain occurs in the lumbar or lower back, in one of two places where the spine meets the pelvis. Around 95% of lower back herniations happen in the L4-L5 spinal segment or the L5-S1 Lumbosacral joint. Any back pain can turn into a vicious cycle of:
Sleeping with a bulging disc requires maintaining the ears, shoulders, and hips aligned to keep the spine aligned.
Sleeping on The Back
Back sleeping done correctly is the best way to sleep for the spine’s health. The important thing is to ensure the entire back is supported when sleeping. If there is a gap or space between the mattress and the back, the weight and gravity force the spine to lower in an unnatural way to fill the space. This can cause back muscle soreness, injury, and sciatica. A thin pillow, blanket, or towel can be used to fill the space, giving the spine the support it needs. Back sleepers can also benefit from a pillow or two under the knees to elevate the legs and help maintain the natural curve of the pine.
Sleeping on The Side
Side sleepers can try pulling the legs up toward the chest, and placing a pillow between the knees can provide relief when sleeping with a bulging disc. Pulling the legs up in the fetal position can relieve pressure on the discs. It is recommended to switch sides to keep the spine balanced. This helps maintain hip alignment, which helps keep the spine in a neutral position.
Sleeping On The Stomach
It is recommended to avoid sleeping on the stomach. This pulls the spine down into an unnatural curve that can cause and exacerbate back pain. For individuals that naturally stomach sleep, it is recommended to place a pillow under the hips and lower abdomen to prevent unnatural spinal positioning.
Chiropractic Relief
Utilizing the right sleeping position can provide pain relief and thorough rest. However, sleeping with a herniated disc is far from what is needed to get back to a normal healthy sleeping pattern. This depends on the location of the bulging disc, severity, and cause. A chiropractor can:
Help the individual develop an optimal sleeping routine and positioning.
Body Composition
Sleep and Growth Hormone In Children
Growth, in all ages, is primarily controlled by growth hormone. The hormone is regulated by the hypothalamus and pituitarygland which plays an important role in sleep. Growth hormone has been found:
It peaks during the beginning of deep sleep.
There are multiple smaller peaks during the other stages of sleep.
Those who have a delay at the beginning of deep sleep have delayed rises in growth hormone levels.
For children to grow they need to have proper levels of growth hormone. This means they need to have the proper amount of sleep for proper body composition. Research has found that increased levels of sleep resulted in less overall fat mass and a reduced percentage of body fat allowing their bodies to grow.
References
Al Qaraghli MI, De Jesus O. Lumbar Disc Herniation. [Updated 2021 Aug 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560878/
Desouzart, Gustavo et al. ‘Effects of Sleeping Position on Back Pain in Physically Active Seniors: A Controlled Pilot Study. 1 Jan. 2016: 235 – 240.
Kose, Gulsah et al. “The Effect of Low Back Pain on Daily Activities and Sleep Quality in Patients With Lumbar Disc Herniation: A Pilot Study.” The Journal of neuroscience nursing: Journal of the American Association of Neuroscience Nurses vol. 51,4 (2019): 184-189. doi:10.1097/JNN.0000000000000446
Sener, Sevgi, and Ozkan Guler. “Self-reported data on sleep quality and psychologic characteristics in patients with myofascial pain and disc displacement versus asymptomatic controls.” The International Journal of prosthodontics vol. 25,4 (2012): 348-52.
Setting spinal goals is important for an individual’s treatment plan to ensure a thorough and successful recovery following:
Surgery
Trauma
Spinal condition
When developing goals with a surgeon or spine specialist, utilizing a well-known method known as SMART is recommended. Individuals are encouraged to set goals to accomplish personal growth and improvement. It is a model for forming goals and objectives that for medical purposes include:
This could be fitness trackers, daily journaling – writing, video, health coach, etc.
Attainable
Determine if the goal is achievable.
Figure out what tools or skill sets are needed to reach the goal.
Realistic
Results-oriented goals.
Measure results or output, including accomplishments.
Time Frame
Set goals within a doable time frame.
Goal setting helps individuals monitor their progress when recovering from injury, surgery, and/or spinal conditions. Making goals smaller makes it easier to achieve improvements. It’s recommended to have a partner assistant during the goal-setting because the pain can compromise decision-making. Pain affects the mind’s abilities to assess improvement and treatment response rationally. Taking the most important goals and focusing on small building blocks helps individuals maintain motivation during a long recovery process.
Difference Between Goal Setting and Treatment
A standard treatment plan is structured for a specific result and is not set up for adjusting the way goal setting does. A treatment plan is created and prescribed to a patient with little patient input. Goal setting is a collaboration between a patient and a doctor setting objectives as stepping-off points to achieve goals. Goal setting empowers patients with education, skillsets, and tools to succeed and continue that mindset as their lives move on. Achieving short-term goals helps individuals reflect positively on small gains that set a solid foundation for more challenging future goals.
Spinal Treatment Goals
Goals are personalized/custom-tailored to the individual’s case and condition. For example, a patient could set a goal of returning to weekend sports activities. Therefore, achieving the goal could require the individual to engage in exercise five days a week for the next two weeks that could include physical therapy rehabilitation:
These activities are small goals that help the body adapt to handling additional physical stress.
Goal Setting When In Recovery
Spinal issues are dealt with by creating reasonable small objectives to reach a goal. SMART goal setting is an instrumental framework for medical providers to help identify what is important to the patient. Modifications on SMART goals can be done to adjust to the individual’s needs. Spinal goals help patients accomplish what is necessary, keeping them empowered and motivated.
Body Composition
Too Comfortable With Goals
An individual may have a great deal of success doing the same workouts initially but then notice they’re getting easier and are not seeing the same rate of progression. That same workout routine, same weights, and equipment will only go so far in goal achievement. In recovery, as the body gets stronger and fitness levels improve, it is recommended to consistently challenge yourself to avoid falling into a rehabilitation fitness plateau. Part of the recovery process is to change up workouts to challenge the body to achieve optimal health and healing. Individuals are recommended to:
Increase weight and or reps
Increase the amount of weight or the number of reps in each set.
Increase or decrease the tempo
Shorten the rest period between sets to keep the heart rate high or slow down to focus on muscle contraction.
Experiment with different types of workout sets
If you’ve been doing the same kinds of lifts, try drop sets, supersets, or AMRAP (as many reps as possible) to challenge your muscles differently.
Individuals doing high-intensity interval training are recommended to incorporate a long run or bike ride.
Changing the workout routine will keep challenging the body, which is great for health progress.
References
Alexanders, Jenny et al. “Goal setting practices used within anterior cruciate ligament rehabilitation: An exploration of physiotherapists understanding, training, and experiences.” Musculoskeletal care vol. 19,3 (2021): 293-305. doi:10.1002/msc.1535
Bovend’Eerdt, Thamar J H et al. “Writing SMART rehabilitation goals and achieving goal attainment scaling: a practical guide.” Clinical rehabilitation vol. 23,4 (2009): 352-61. doi:10.1177/0269215508101741
Haas, B et al. “Rehabilitation goals of people with spinal cord injuries can be classified against the International Classification of Functioning, Disability and Health Core Set for spinal cord injuries.” Spinal cord vol. 54,4 (2016): 324-8. doi:10.1038/sc.2015.155
The thoracic spine, also known as the upper or middle back, is designed for stability to anchor the rib cage and protect the organs in the chest. It is highly resistant to injury and pain. However, when thoracic back pain does present, it is usually from long-term posture problems or an injury. Thoracic back pain is less common than lower back and neck pain, but it does affect up to 20% of the population, particularly women. Treatment options include chiropractic for quick and long-term pain relief.
Thoracic Back Pain and Soreness
The thoracic area is vital for various functions related to:
Upper back pain usually feels like a sharp, burning pain localized to one spot or a general achiness that can flare up and spread out to the shoulder, neck, and arms.
Types of Upper Back Pain
These include:
Myofascial pain
Spine degeneration
Joint dysfunction
Nerve dysfunction
General spinal misalignments
Depending on what specific tissues are affected, pain can occur with breathing or arm use. It is recommended to have a healthcare professional perform an examination and get an accurate diagnosis. A chiropractor understands the delicate balance and functions that the thoracic spine provides and can develop a proper treatment plan.
Chiropractic
Treatment options will depend on the symptoms, underlying dysfunctions, and individual preferences. Recommendations for treatment often include:
Spine adjustments to improve alignment and nerve integrity.
Posture training to maintain spinal alignment.
Therapeutic massage.
Exercise training to restore muscular balance.
Non-invasive pain-relieving techniques.
Health coaching.
Body Composition
Plant-Based Diets for Weight Loss
Individuals who follow vegan, vegetarian, and semivegetarian diets have reported and shown they are less likely to be overweight or obese. This can indicate that reducing intake of meat and animal products is beneficial for weight loss. Studies have found that individuals who follow a vegan diet may lose more weight than individuals on a more conventional weight loss diet, even with similar calories consumed, and often have significant improvements in blood sugar and inflammation markers.
Plant-Based Protein and Muscle Gain
Some plant-based proteins are just as effective as animal protein at promoting muscle gain. A study found that supplementing rice protein following resistance training had similar benefits to whey protein supplementation. Both groups had:
Briggs AM, Smith AJ, Straker LM, Bragge P. Thoracic spine pain in the general population: prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskelet Disord. 2009;10:77.
Cichoń, Dorota et al. “Efficacy of Physiotherapy in Reducing Back Pain and Improve Joint Mobility in Older Women.” Ortopedia, traumatologia, rehabilitacja vol. 21,1 (2019): 45-55. doi:10.5604/01.3001.0013.1115
Fouquet N, Bodin J, Descatha A, et al. Prevalence of thoracic spine pain in a surveillance network. Occup Med (Lond). 2015;65(2):122-5.
Jäger, Ralf et al. “Comparison of rice and whey protein isolate digestion rate and amino acid absorption.” Journal of the International Society of Sports Nutrition vol. 10,Suppl 1 P12. 6 Dec. 2013, doi:10.1186/1550-2783-10-S1-P12
Joy, Jordan M et al. “The effects of 8 weeks of whey or rice protein supplementation on body composition and exercise performance.” Nutrition journal vol. 12 86. 20 Jun. 2013, doi:10.1186/1475-2891-12-86
Medawar, Evelyn et al. “The effects of plant-based diets on the body and the brain: a systematic review.” Translational psychiatry vol. 9,1 226. 12 Sep. 2019, doi:10.1038/s41398-019-0552-0
Newby, PK et al. “Risk of overweight and obesity among semivegetarian, lactovegetarian, and vegan women.” The American journal of clinical nutrition vol. 81,6 (2005): 1267-74. doi:10.1093/ajcn/81.6.1267
Pope, Malcolm H et al. “Spine ergonomics.” Annual review of biomedical engineering vol. 4 (2002): 49-68. doi:10.1146/annurev.bioeng.4.092101.122107
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine