Can individuals relieve back pain by incorporating core strength training to reduce pain and discomfort in their lower backs?
Introduction
Many individuals worldwide have dealt with back issues that make it difficult to complete any task that they are doing. Many often feel pain and discomfort radiating from the three sections of the back and can radiate from the neck, shoulders, and hips. When these areas of the musculoskeletal system are being affected, it can lead to a life of pain and chronic conditions that cause overlapping risk profiles. At the same time, some causes of back pain often correlate with environmental factors and weak core muscles. When a person is dealing with weak core muscles, they will experience instability and pain when they are mobile, leading to back pain. In today’s article, we look at what the core muscles are, how they are connected to back pain, and how strengthening them can reduce the effects of back pain. We discuss with certified medical providers who inform our patients how strengthening the core muscles can reduce back pain. While asking informed questions to our associated medical providers, we advise patients to incorporate various core strengthening exercises to prevent overlapping risk profiles correlated with back pain. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
What Are The Core Muscles?
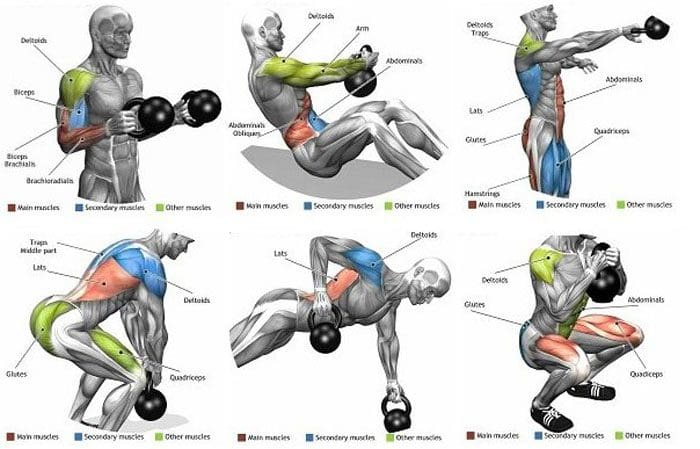
Do you feel a constant ache or pain in your back after lifting or carrying objects in a hunched position? Do you experience muscle weakness in your torso that you can’t stay in a plank position for a few seconds? Or do you experience radiating pain from your lower back to your leg? The core muscles are a group of muscles wrapped around the torso like a support belt that helps with stability, balance, and protecting the lumbar from injuries. The core muscles are found in the lower body’s front, back, and sides. At the same time, the core muscles can help generate intrabdominal pressure while moving the vertebral column. (Flynn & Vickerton, 2024) In the core muscles, the transverse abdominis muscle or the seatbelt muscle. This muscle works with the inspiratory muscles through elastic loading to evoke transversus expiratory activity when breathing and functioning in motion. (De Troyer et al., 1990)
Core Muscles & Back Pain
The core muscles, especially the transverse abdominis muscles, are often overlooked as many individuals frequently deal with numerous factors that cause low back pain. Common core muscles are associated with back pain because environmental factors can neglect the transverse abdominis muscles. Fatigue in the core muscles can cause repetitive asymmetric loading on the spine, which enhances susceptibility to back pain and other injuries. (Zemkova & Zapletalova, 2021) Since back pain is a multifactorial condition that is one of the leading causes of hospital visits and socio-economic issues, many individuals start to neglect the core muscles over time, causing them to be weak. Some symptoms correlated with weak core muscles include:
When this happens, many people start looking for treatment to reduce their back pain and help strengthen their core muscles.
Discover The Benefits Of Chiropractic Care- Video
Strengthening Core Muscles
Before people reduce their back pain and return to their daily routine, they would have to be assessed by a pain specialist like a chiropractor to assess fully what environmental factors are causing the back pain. After the assessment, a chiropractor can work with a physical therapist to reduce back pain and strengthen the core muscles to prevent back pain from returning. When it comes to core strengthening exercises, they focus on either the deep or superficial muscles of the torso, which might produce different effects on lumbar motion. (Puntumetakul et al., 2021) Additionally, core stability exercises can reduce pain in the back and disability reduction and improve a person’s quality of life. (Kanwal et al., 2021) Engaging the muscles through core strengthening exercises can help achieve optimal strength with twisting and side-bending movements to reduce back pain.
Pay Attention To Engaged Core Muscles
However, individuals need to pay attention to engaging their core muscles while maintaining a neutral spine position for stability and preventing back pain. (Cigdem Karacay et al., 2022) This allows individuals to be consistent with strengthening their core and to commit to short workouts incorporated as part of not only their routine but also as part of their customized treatment plan. When it comes to reducing back pain, it is important to ensure that the core muscles are engaged to help build strength and stability, decrease back pain, and improve functionality. When people start strengthening their core muscles, they will be able to be more mindful about how to present themselves and live healthier lives.
References
Cigdem Karacay, B., Sahbaz, T., Gurtekin, B., Yildiz, S., & Ozcan, E. (2022). Effectiveness of whole-body vibration exercise and core stabilization exercise in chronic non-specific low back pain: A randomized-controlled study. Turk J Phys Med Rehabil, 68(2), 184-194. https://doi.org/10.5606/tftrd.2022.7060
De Troyer, A., Estenne, M., Ninane, V., Van Gansbeke, D., & Gorini, M. (1990). Transversus abdominis muscle function in humans. J Appl Physiol (1985), 68(3), 1010-1016. https://doi.org/10.1152/jappl.1990.68.3.1010
Kanwal, S., Yaqoob, I., Shakil-Ur-Rehman, S., Ghous, M., Ghazal, J., & Namroz, N. (2021). Effects of core muscle stability on low back pain and quality of life in post-menopausal women: A comparative study. J Pak Med Assoc, 71(1(A)), 37-40. https://doi.org/10.47391/JPMA.151
Puntumetakul, R., Saiklang, P., Tapanya, W., Chatprem, T., Kanpittaya, J., Arayawichanon, P., & Boucaut, R. (2021). The Effects of Core Stabilization Exercise with the Abdominal Drawing-in Maneuver Technique versus General Strengthening Exercise on Lumbar Segmental Motion in Patients with Clinical Lumbar Instability: A Randomized Controlled Trial with 12-Month Follow-Up. Int J Environ Res Public Health, 18(15). https://doi.org/10.3390/ijerph18157811
Wattananon, P., Sinsurin, K., & Somprasong, S. (2020). Association between lumbopelvic motion and muscle activation in patients with non-specific low back pain during forward bending task: A cross-sectional study. Hong Kong Physiother J, 40(1), 29-37. https://doi.org/10.1142/S1013702520500043
Zemkova, E., & Zapletalova, L. (2021). Back Problems: Pros and Cons of Core Strengthening Exercises as a Part of Athlete Training. Int J Environ Res Public Health, 18(10). https://doi.org/10.3390/ijerph18105400
Can individuals incorporate the beneficial properties of l-theanine into their routines to reduce stress and improve brain function?
Introduction
More often than not, many people worldwide are constantly in stressful situations. People worry about the smaller things, from deadlines to piles and errands that must be done as soon as possible. Now, when environmental factors start to cause overlapping risk profiles associated with stress, it can lead to neurocognitive dysfunction and other comorbidities affecting the body, which is why there are numerous ways for people to reduce their stress and function in a healthier lifestyle. One of the ways to reduce stress can be found in a local grocery store, incorporating L-theanine. Today’s article focuses on how stress can affect the brain and how L-theanine can combat stress and help improve brain function. We discuss with certified medical providers who inform our patients how L-theanine can help reduce chronic stress that is affecting the body and how it can affect their brain function. While asking informed questions to our associated medical providers, we advise patients to incorporate mindful techniques and L-theanine as part of their routine to improve their brain function and prevent chronic stress from reoccurring. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
How Stress Affects The Brain
Have you experienced the 2 p.m. slumps that you constantly run on low energy after a hectic work or school day? How often do you experience brain fog that makes you unable to function properly? Or are you constantly stressed and feeling muscle aches and pains? Everyone knows stress is a major influence on their daily lives and can impact their mood, well-being, and health. (Schneiderman et al., 2005) Hence, stress comes in two forms: acute and chronic. Depending on the situation that the person is experiencing, stress can affect not only the body but also the brain. Short-term or acute stress can help enhance the immune response to the body, giving it a little boost of energy; however, in its long-term or chronic form, it can dysregulate the immune system and affect the brain function of the body. (Dhabhar, 2014)
Now, many people are thinking, how does stress affect brain function? The brain is the main organ for stress reactivity and helps distribute neural circuitry that determines what threats are coming that cause stress to the individual. (McEwen & Gianaros, 2010) When a person is dealing with a highly stressful situation, the brain determines that this situation is threatening and causes the individual to deal with stress cortisol levels. Hence why, many individuals are dealing with headaches, general aches, and pain around the neck and shoulders; stress causes issues with brain function; it can disrupt the neuron signals in the body, which leads to the development of inflammation, chronic illnesses, and neurological conditions to arise. Fortunately, there are numerous ways to reduce stress to prevent brain dysfunction and enhance the body while relaxing it.
Secrets Of Optimal Wellness- Video
How Does L-Theanine Combat Stress?
When finding natural ways to reduce stress, many people will search for different ways to relax and ease the stress. One of the ways many people can reduce stress is by sipping some green tea. Green tea contains polyphenolic compounds and about 1 to 3% L-theanine that can positively affect stress and mental health consequences in individuals. (Almudhi & Gabr, 2022) Additionally, drinking green tea or taking L-theanine supplements as part of a daily routine can be combined with relaxing hobbies to lower stress and boost energy levels. L-theanine is also an amino acid with stress-relieving effects that can improve glutamine and dampen inflammatory effects. (Unno et al., 2024)
How Does L-Theanine Improve Brain Function?
L-theanine can help improve brain function when consumed in tea form and decrease the risk for neurodegenerative disorders as a potential therapeutic agent. (Valverde-Salazar et al., 2023) Additionally, when individuals start to consume L-theanine, it can provide positive neuroprotective effects and cognitive function, which helps increase alertness and reduces brain fog. (Sokary et al., 2023) When individuals start thinking about their health and wellness by consuming L-theanine in tea form, it can provide beneficial properties combined with therapeutic options to help reduce chronic stress levels and improve brain function so they can have a healthier and stress-free life.
References
Almudhi, A., & Gabr, S. A. (2022). Green tea consumption and the management of adrenal stress hormones in adolescents who stutter. Biomed Rep, 16(4), 32. https://doi.org/10.3892/br.2022.1515
Dhabhar, F. S. (2014). Effects of stress on immune function: the good, the bad, and the beautiful. Immunol Res, 58(2-3), 193-210. https://doi.org/10.1007/s12026-014-8517-0
McEwen, B. S., & Gianaros, P. J. (2010). Central role of the brain in stress and adaptation: links to socioeconomic status, health, and disease. Ann N Y Acad Sci, 1186, 190-222. https://doi.org/10.1111/j.1749-6632.2009.05331.x
Schneiderman, N., Ironson, G., & Siegel, S. D. (2005). Stress and health: psychological, behavioral, and biological determinants. Annu Rev Clin Psychol, 1, 607-628. https://doi.org/10.1146/annurev.clinpsy.1.102803.144141
Sokary, S., Al-Asmakh, M., Zakaria, Z., & Bawadi, H. (2023). The therapeutic potential of matcha tea: A critical review on human and animal studies. Curr Res Food Sci, 6, 100396. https://doi.org/10.1016/j.crfs.2022.11.015
Unno, K., Taguchi, K., Matsuda, T., & Nakamura, Y. (2024). Stress-Relieving Effects of Green Tea Depend on the Ratio of Its Special Ingredients and the Infusion Conditions. Molecules, 29(19). https://doi.org/10.3390/molecules29194553
Valverde-Salazar, V., Ruiz-Gabarre, D., & Garcia-Escudero, V. (2023). Alzheimer’s Disease and Green Tea: Epigallocatechin-3-Gallate as a Modulator of Inflammation and Oxidative Stress. Antioxidants (Basel), 12(7). https://doi.org/10.3390/antiox12071460
Can individuals utilize chiropractic care to reduce sciatica pain and help restore mobility to their lower back and legs?
Introduction
Many individuals are always on the move and utilize the lower half of the body to go from one location to another. From the lower back to the feet, many individuals do repetitive movement that causes the lower back muscles to be constantly stretched. This, in turn, can lead to overlapping risk profiles that can affect the lower back and a long nerve connected to the lower back, known as the sciatic nerve. When numerous issues affect the sciatic nerve, many individuals experience pain and discomfort over time, which can develop into something chronic without treatment. Luckily, when individuals begin to think about their health and wellness, it reduces the chances of pain and discomfort from returning. Today’s article looks at the causes of sciatica and how non-surgical treatments like chiropractic care can help relieve sciatica pain and restore mobility to the lower back and legs. We discuss with certified medical providers who inform our patients how sciatica pain correlates with the lower back. While asking informed questions to our associated medical providers, we advise patients to incorporate non-surgical treatments like chiropractic care to reduce sciatica pain and help realign the body. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
What Causes Sciatica?
Do you feel numbness or tingling sensations in your legs, making walking unbearable? Do you experience pain or discomfort in your lower back after lifting a heavy object? Or how long have you stretched your body after sitting down or standing excessively at work? Many of these scenarios are often correlated with low back pain. However, low back pain is always connected with sciatica and can impact the body. While the sciatic nerve plays a huge role in direct motor function to the hamstrings and lower extremities, sciatica is when environmental factors impact or compress the sciatic nerve, causing pain-like symptoms to the lower extremities. (Davis et al., 2024) Since the sciatic nerve is large and travels down to the feet, it allows mobility to the lower extremities. When many individuals experience low back pain, they will also experience sciatica.
Sciatica also means that pain will always be transmitted along the sciatic nerve root, leading to various impairments and socioeconomic consequences and affecting a person’s quality of life. (Siddiq et al., 2020) Many of the causes of sciatica pain can vary as they are all correlated with low back pain. Some of the various environmental factors that can cause sciatica include:
Physical inactivity
Excessive sitting or standing
Poor posture
Musculoskeletal conditions
Another environmental factor that leads to the development of sciatica is disc degeneration. This can cause the nerves to be irritated due to herniation and cause asymptomatic overlapping risk profiles (Zhou et al., 2021). When people are dealing with the overlapping risk profiles of sciatica, many often seek treatment to reduce the pain and restore mobility to the lower extremities.
Sciatica: Causes, Symptoms, & Tips- Video
How Chiropractic Care Reduces Sciatica
Since sciatica is commonly experienced as a frequent symptom cause of low back and leg pain, the symptoms can range from a mild tingling sensation to a burning sensation, and treatment is needed. Many individuals will seek out non-surgical treatments to reduce the pain caused by sciatica. Non-surgical treatments are non-invasive, affordable, and customizable to the individual. One of the non-surgical treatments is chiropractic care, which can help many individuals dealing with sciatica. A chiropractor can diagnose a person’s sciatica and assess the root cause of the symptoms to provide the most appropriate form of treatment. The main goal for chiropractic care is to restore the natural mobility of the spine and provide progressive relief from pain and stiffness in the lower extremities while improving a person’s daily living. (Kruse et al., 2019)
Chiropractic Care Restores Lower Back & Leg Mobility
Chiropractors utilize manual and mechanical spinal manipulation to increase lumbar spinal mobility and flexibility and improve the legs biomechanically. (Siciliano et al., 2024) Chiropractic treatments can also use various methods like neural mobilization intervention to decrease the pain and restore nerve function in the lower extremities and lower back. (Peacock et al., 2023) This allows individuals to have a reduced disability from sciatica associated with low back pain, and it is possible to prevent sciatica from occurring in the future. As many people begin to become more mindful of what is causing their sciatica, they can find effective ways to improve their spine’s well-being and prevent sciatica symptoms from affecting the lower extremities.
Kruse, R. A., White, B. A., & Gudavalli, S. (2019). Management of Lumbar Radiculopathy Associated With an Extruded L4-L5 Spondylolytic Spondylolisthesis Using Flexion-Distraction Manipulation: A Case Study. J Chiropr Med, 18(4), 311-316. https://doi.org/10.1016/j.jcm.2019.02.001
Peacock, M., Douglas, S., & Nair, P. (2023). Neural mobilization in low back and radicular pain: a systematic review. J Man Manip Ther, 31(1), 4-12. https://doi.org/10.1080/10669817.2022.2065599
Siciliano, T. B., Gudavalli, M. R., & Kruse, R. (2024). Spinal manipulation and mobilization forces delivered treating sciatica: a case report. Front Integr Neurosci, 18, 1356564. https://doi.org/10.3389/fnint.2024.1356564
Siddiq, M. A. B., Clegg, D., Hasan, S. A., & Rasker, J. J. (2020). Extra-spinal sciatica and sciatica mimics: a scoping review. Korean J Pain, 33(4), 305-317. https://doi.org/10.3344/kjp.2020.33.4.305
Zhou, J., Mi, J., Peng, Y., Han, H., & Liu, Z. (2021). Causal Associations of Obesity With the Intervertebral Degeneration, Low Back Pain, and Sciatica: A Two-Sample Mendelian Randomization Study. Front Endocrinol (Lausanne), 12, 740200. https://doi.org/10.3389/fendo.2021.740200
What are the treatment options for individuals dealing with foot overpronation when the foot and ankle move too much downward and inward?
Overpronation
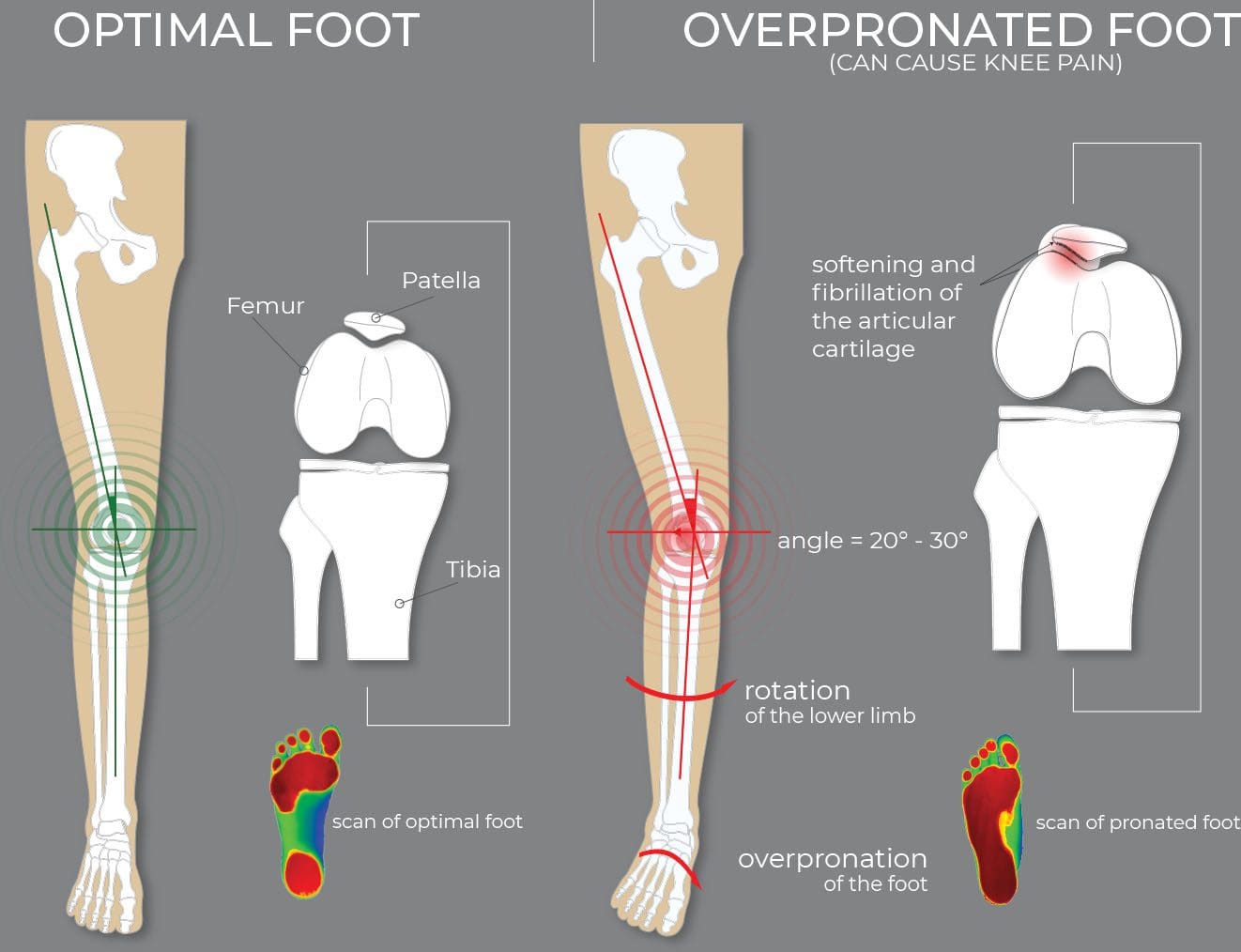
Pronation is the normal foot and ankle movement when taking a step and is usually associated with flat feet. Overpronation is a movement pattern in which the ankle rolls inward and downward, causing the foot’s arch to collapse with each stride. Overpronation can strain the muscles and ligaments in the feet and legs, leading to heel pain, ankle pain, shin splints, and low-back pain. (Pedorthic Association of Canada, 2023) Orthotic inserts for shoes, prescribed stretches, ankle braces, physical therapy, and surgery can all help alleviate the impact of overpronation. (Sánchez-Rodríguez, R. et al., 2020)
Signs and Symptoms
Some individuals with overpronation can have no symptoms at all. (Pedorthic Association of Canada, 2023) while others experience pain or other symptoms in their legs and feet. Overpronation is not a medical condition but a movement pattern that, if left untreated, can increase the risk for certain medical conditions because it strains the feet and leg muscles, joints, and ligaments. (Sánchez-Rodríguez, R. et al., 2020) Certain medical conditions can be a sign of overpronation and include: (Pedorthic Association of Canada, 2023)
Bunions
Heel pain
Plantar fasciitis
Achilles tendon pain
Posterior tibial tendonitis
Shin splints
Knee pain, including patellofemoral pain syndrome
Pain in the iliotibial or IT band
Lower back pain
Arthritis in foot and ankle joints
Stress fractures
Individuals may also experience pain in the midfoot or hips, which can be a symptom of flat feet.
Underpronation
Pronation refers to the normal movement of the foot and ankle while walking. Overpronation and underpronation are both abnormal movement patterns.
Overpronation – when the ankle rolls too much inward and downward.
Underpronation – occurs when an individual’s foot lacks flexibility and moves too little. This condition is called supination and is often associated with a high-arch foot type.
Overpronation can be caused or worsened by flatfeet. However, some individuals have overpronation because their feet and ankles are very flexible, so they tend to move more. Risk factors for flatfeet can also increase the chances of developing overpronation and include:
Age, especially individuals over 40.
Wearing shoes like high heels and shoes with a narrow-toe box.
Women are more prone to overpronate because of the various shoes and high heels worn.
Being overweight
Doing repetitive, impactful movements like running.
Correction and Treatment
Treating overpronation focuses on alleviating strain on muscles in the foot, ankle, and leg to relieve symptoms in the heel, ankle, knees, hips, or back. Common treatments are wearing supportive shoes and/or using foot orthotics. Exercises and stretches are also recommended to maintain flexibility and strength. Surgery is rare, but correcting flat feet that can cause overpronation may be recommended. (Sánchez-Rodríguez, R. et al., 2020) Individuals with overpronation are advised to see a podiatrist who can explain the best treatment options.
Supportive Shoes
The first course of treatment is to wear added supportive footwear. This can include specialized shoes or inserts that support the foot and reduce ankle movement. Individuals are advised to use shoes with firm heel and midfoot support to help prevent disproportionate movement. (Pedorthic Association of Canada, 2023)
Orthotics
A healthcare provider can recommend orthotics for individuals with moderate overpronation. These are meant to support the foot, especially the arch, and reduce overpronation. (Naderi A. Degens H. and Sakinepoor A. 2019) Individuals can purchase orthotics from shoe stores and elsewhere, but those with severe overpronation may need custom orthotics molded to the foot to provide individualized support.
Exercises and Stretches
Exercises and stretches can also help. A study found that exercises targeting the feet, core, and hips helped correct pronation over nine weeks. The exercises included: (Sánchez-Rodríguez, R. et al., 2020)
Toe pickups in which the individuals grab small objects with their toes and move them from one position to another.
Flexing and pointing the toes using a resistance band placed around the toes.
Hip abduction exercises to target the hip and glutes.
Abdominal and oblique muscle exercises to stabilize the torso.
Short-foot exercise raises the foot arch off the ground, drawing the toes toward the heel. (Sulowska I. et al., 2016)
Surgery
Rarely will surgery be needed to treat flat feet and severe overpronation. But if necessary, reconstruction realigns the bones to support the arch better and reduce overpronation. A metal implant is used for flatfeet to stabilize the area. Surgery can also repair torn tendons or other damage contributing to overpronation. (Healthline, 2020)
Injury Medical Chiropractic and Functional Medicine Clinic
Individuals with overpronation but no symptoms don’t necessarily have to see a healthcare provider since this may be the body’s natural movement pattern. But if the feet, legs, hips, or back begin to present with pain and other symptoms, see a healthcare provider who can evaluate gait and recommend treatment options. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Enhance Performance with Functional Foot Orthotics
References
Pedorthic Association of Canada. (2023). Overpronation and Underpronation Correction. https://pedorthic.ca/services/foot-health/pronation/
Sánchez-Rodríguez, R., Valle-Estévez, S., Fraile-García, P. A., Martínez-Nova, A., Gómez-Martín, B., & Escamilla-Martínez, E. (2020). Modification of Pronated Foot Posture after a Program of Therapeutic Exercises. International journal of environmental research and public health, 17(22), 8406. https://doi.org/10.3390/ijerph17228406
Naderi, A., Degens, H., & Sakinepoor, A. (2019). Arch-support foot orthoses normalize dynamic in-shoe foot pressure distribution in medial tibial stress syndrome. European journal of sport science, 19(2), 247–257. https://doi.org/10.1080/17461391.2018.1503337
Sulowska, I., Oleksy, Ł., Mika, A., Bylina, D., & Sołtan, J. (2016). The Influence of Plantar Short Foot Muscle Exercises on Foot Posture and Fundamental Movement Patterns in Long-Distance Runners, a Non-Randomized, Non-Blinded Clinical Trial. PloS one, 11(6), e0157917. https://doi.org/10.1371/journal.pone.0157917
Healthline. (2020). All About Surgery for Flat Feet: Pros and Cons. https://www.healthline.com/health/flat-feet-surgery
Can individuals with nerve injuries incorporate non-surgical treatments to reduce pain sensations and restore motor function to their bodies?
Introduction
The human body is a complex machine of nerves, bones, organs, tissues, and muscles that help the individual be mobile, flexible, and stable during various activities without pain and discomfort. However, when numerous factors start to hurt the body, it can lead to multiple overlapping risk profiles that can affect the body’s extremities and nerve injuries. Dealing with nerve injuries can lead to referred pain in the musculoskeletal system, and many people think it is muscle pain instead of nerve injury. When that happens, many individuals will begin to seek treatment to reduce not only the symptoms of nerve injuries but also reduce the pain associated with the nerves. In today’s article, we will look at what causes nerve injuries and how non-surgical treatments like chiropractic care and acupuncture can help with reducing the overlapping symptoms of nerve injuries and provide relief to the body. We discuss with certified medical providers who inform our patients about how nerve injuries can impact the musculoskeletal system. While asking informed questions to our associated medical providers, we advise patients to incorporate non-surgical treatments like chiropractic care and acupuncture to restore motor function to the body. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
What Causes Nerve Injuries?
Do you constantly feel tingling or numbness in your legs, arms, feet, and hands? Do your muscles feel so weak that holding objects seems difficult? Or do you feel pain in your extremities, making it difficult to do everyday tasks? The body has trillions of nerves that branch out from the central nervous system and are intertwined with the muscles, tissues, and organs for motor-sensory function. Traumatic injuries, accidents, and normal environmental factors impact the nerves and cause overlapping risk profiles. More often than not, many individuals deal with non-mechanical and mechanical nerve injuries that can occur to the body. With nerve injuries, many individuals can feel various symptoms depending on the severity. Neuropraxia, a moderate form of nerve injury, causes nerve compression in the upper and lower extremities that causes motor dysfunction. (Carballo Cuello & De Jesus, 2024)
Additionally, neuropraxia can lead to functional impairment to the motor-sensory dysfunction that disrupts the peripheral nervous system, signaling this blocks nerve conduction and transient weakness or paresthesia. (Biso & Munakomi, 2024) When this happens, many individuals dealing with peripheral nerve injury that is associated with neuropraxia can experience structural and functional impairment to the sensory-motor skills in the extremities, which leads to physical disability and neuropathic pain, thus affecting a person’s quality of life. (Lopes et al., 2022) Many individuals dealing with nerve injuries can have various recovery periods depending on the severity. Many people often think they are dealing with musculoskeletal pain in their neck, shoulders, back, and extremities, but it is associated with nerve injury. When this happens, many individuals can seek out treatment to reduce the pain-like symptoms from nerve injuries.
Is Motion The Key To Healing?- Video
Non-Surgical Treatments For Nerve Injuries
When it comes to treating nerve injuries, it depends on the severity of the symptoms they cause. Surgical options are recommended to restore motor-sensory function if severe mechanical factors cause nerve injury. However, many individuals will opt out of surgical treatments due to their high cost and will often take over-the-counter medication to ease the pain. However, if the nerve injury is non-mechanical, many individuals can seek non-surgical treatments to reduce the nerve injury affecting the musculoskeletal system. Many non-surgical treatments are preferable to many people because they are cost-effective and can ultimately enhance a person’s care and improve their recovery outcome. (El Melhat et al., 2024) Non-surgical treatments can come in many forms, from chiropractic care to acupuncture, to help reduce the effects of non-mechanical nerve injuries and help restore the sensory-motor function of the musculoskeletal system.
Chiropractic Care
Chiropractic care is one of the many non-surgical therapies that use mechanical and manual manipulation of the spine to realign the body and help restore the sensory-motor function to the extremities. With nerve injuries, chiropractic care can help with neural mobilization to release trapped nerves in the affected muscle areas, thus reducing pain-like symptoms of tingling sensations. (Jefferson-Falardeau & Houle, 2019) Additionally, chiropractic care can help increase ROM (range of motion) in the extremities and reduce numbing and tingling sensations.
Acupuncture
Acupuncture is another non-surgical treatment that can also help reduce non-mechanical nerve injuries to the body. When a professional acupuncturist uses small, thin needles at different pressure points to rewire the neuron signaling and restore the body’s energy flow, acupuncture can help improve the clinical efficacy of nerve pain intensity and help enhance the person’s quality of life. (Li et al., 2023) Additionally, acupuncture can help improve nerve injury’s emotional and cognitive function and can be combined with other non-surgical treatments. (Jang et al., 2021) When it comes to reducing pain-like symptoms correlated with nerve injury, non-surgical treatments can provide the relief many individuals seek and lead to a happier, healthier life.
El Melhat, A. M., Youssef, A. S. A., Zebdawi, M. R., Hafez, M. A., Khalil, L. H., & Harrison, D. E. (2024). Non-Surgical Approaches to the Management of Lumbar Disc Herniation Associated with Radiculopathy: A Narrative Review. J Clin Med, 13(4). https://doi.org/10.3390/jcm13040974
Jang, J. H., Song, E. M., Do, Y. H., Ahn, S., Oh, J. Y., Hwang, T. Y., Ryu, Y., Jeon, S., Song, M. Y., & Park, H. J. (2021). Acupuncture alleviates chronic pain and comorbid conditions in a mouse model of neuropathic pain: the involvement of DNA methylation in the prefrontal cortex. Pain, 162(2), 514-530. https://doi.org/10.1097/j.pain.0000000000002031
Jefferson-Falardeau, J., & Houle, S. (2019). Chiropractic Management of a Patient With Radial Nerve Entrapment Symptoms: A Case Study. J Chiropr Med, 18(4), 327-334. https://doi.org/10.1016/j.jcm.2019.07.003
Li, X., Liu, Y., Jing, Z., Fan, B., Pan, W., Mao, S., & Han, Y. (2023). Effects of acupuncture therapy in diabetic neuropathic pain: A systematic review and meta-analysis. Complement Ther Med, 78, 102992. https://doi.org/10.1016/j.ctim.2023.102992
Lopes, B., Sousa, P., Alvites, R., Branquinho, M., Sousa, A. C., Mendonca, C., Atayde, L. M., Luis, A. L., Varejao, A. S. P., & Mauricio, A. C. (2022). Peripheral Nerve Injury Treatments and Advances: One Health Perspective. Int J Mol Sci, 23(2). https://doi.org/10.3390/ijms23020918
For individuals trying to retrain their body movements for back health improvement, what is the spinal area that helps the body twist, bend, and stand upright?
Lumbosacral Joint L5-S1
The L5-S1, also called the lumbosacral joint, is a term used to describe a part of the spine. It is where the lumbar spine ends and the sacral spine begins, and it connects these bones. The lumbosacral joint is also susceptible to misalignment and injury, such as disc herniation or a spinal disorder called spondylolisthesis.
The spinal column is the structure that allows the body to stand upright and helps you twist, bend, and alter trunk and neck position. Typically, 24 movable bones in the spine connect to the sacrum and the coccyx, or the tailbone. The sacrum and the coccyx each have multiple bones that fuse over time. L5-S1 consists of the last bone in the lumbar spine, called L5, and the triangle-shaped bone under it, known as the sacrum. S1 is at the top of the sacrum and comprises five fused bones.
Risk of Injury
Each area of the spine has a curve that goes in opposite directions. The places where the spinal curve directions change are junctional levels. The risk of injuries may be higher at junctional levels because the body weight shifts direction as the curves shift. The L5-S1 junction is located between the lumbar curve and the sacral curve. The lumbar curve sweeps forward, and the sacral curve goes backward.
The lumbosacral joint L5-S1 junction is highly vulnerable to misalignment, wear and tear, and injury. This is because the top of the sacrum is positioned at an angle for most individuals. Aging and injury increase the vulnerability of the L5-S1 junction even more. Pain coming from L5-S1 is usually treated with:
Heat and/or ice
Over-the-counter anti-inflammatory medications
Prescription pain medications
Muscle relaxers
Physical therapy
Chiropractic adjustments
Epidural steroid injections
If these therapies do not help, surgery may be recommended. L5-S1 is one of the two most common sites for back surgery.
Conditions
Disc herniation at L5-S1 is a common injury and cause of sciatica, which can cause pain and other issues (MedlinePlus, 2024). The L5-S1 junction is often the site of a condition known as spondylolisthesis.
Disc Herniation
Discs separate the vertebrae, cushioning the spinal column and allowing movement between vertebrae. A disc herniation means the disc slips out of place. (MedlinePlus, 2022) A disc herniation at L5-S1 is a common cause of sciatica. Symptoms of sciatica include:
Burning
Numbness
Pain or tingling that radiates from the buttock down the leg to the knee or foot.
Disc herniation can also cause chronic back pain and stiffness and trigger painful muscle spasms. Bowel problems are also possible with disc issues at L5-S1. Research links irritable bowel syndrome to herniated discs in the lower back. (Bertilson BC, Heidermakr A, Stockhaus M. 2015) Additional studies found disc problems at L5-S1 can lead to difficulty with sphincter control. (Akca N. et al., 2014) Initial treatments for disc herniation include rest and pain relievers to reduce inflammation and swelling, then physical therapy. Most recover with conservative interventions, and those who don’t may require a steroid injection or surgery. (MedlinePlus, 2022)
Spondylolisthesis
Spondylolisthesis occurs when a vertebra slips forward relative to the bone below it. The most common form of this condition is degenerative spondylolisthesis, which generally begins when the spine wears down with age. Isthmic spondylolisthesis is another common variation and starts as a tiny fracture in the pars interarticularis, a bone that connects the adjoining parts of the facet joint. (American Academy of Orthopaedic Surgeons, 2020) These fractures often occur before age 15, but symptoms do not develop until adulthood. Degeneration of the spine in later adulthood can further worsen the condition.
The angle of the sacrum can also contribute to spondylolisthesis. This is because the S1 tips down in the front and up in the back rather than being horizontal. Individuals with a greater tilt are usually at a higher risk of spondylolisthesis. (Gong S. et al., 2019) However, individuals with spondylolisthesis may not have any symptoms. Those who do may experience: (American Academy of Orthopaedic Surgeons, 2020)
Back stiffness
Standing difficulties
Walking difficulties
Lower back pain
Hamstring tightness
Spondylolisthesis is typically treated with non-surgical interventions that can include:
Pain medications
Heat and/or ice application
Physical therapy
Epidural steroid injections
Usually, non-surgical care is tried for at least six months. If pain and symptoms persist, surgery may be an option. Spinal fusion surgery can be effective but requires a long recovery time and can have additional risks.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Healing After Trauma
References
MedlinePlus. (2024). Sciatica. Retrieved from https://medlineplus.gov/sciatica.html
MedlinePlus. (2022). Herniated disk. Retrieved from https://medlineplus.gov/ency/article/000442.htm
American Association of Neurological Surgeons. (2024). Herniate disc. https://www.aans.org/patients/conditions-treatments/herniated-disc/
Bertilson, B. C., Heidermark, A., & Stockhaus, M. (2015). Irritable Bowel Syndrome–a Neurological Spine Problem. Journal of Advances in Medicine and Medical Research, 4(24), 4154–4168. https://doi.org/10.9734/BJMMR/2014/9746
Akca, N., Ozdemir, B., Kanat, A., Batcik, O. E., Yazar, U., & Zorba, O. U. (2014). Describing a new syndrome in L5-S1 disc herniation: Sexual and sphincter dysfunction without pain and muscle weakness. Journal of craniovertebral junction & spine, 5(4), 146–150. https://doi.org/10.4103/0974-8237.147076
American Academy of Orthopaedic Surgeons. (2020). Spondylolysis and spondylolisthesis. https://orthoinfo.aaos.org/en/diseases–conditions/spondylolysis-and-spondylolisthesis/
Gong, S., Hou, Q., Chu, Y., Huang, X., Yang, W., & Wang, Z. (2019). Anatomical factors and pathological parts of isthmic fissure and degenerative lumbar spondylolisthesis.
Can individuals with body pain incorporate Pilates to reduce general aches and pains while strengthening muscles in the body?
Introduction
Environmental factors like poor posture, improper steps, mechanical overload, physical inactivity, and poor dieting can affect a person’s health and wellness, leading to body pains in the neck, shoulders, and back. When this happens, the surrounding muscles become weak and overstretched over time, causing pain and discomfort in different body areas. However, many individuals thinking about their health and wellness can seek various treatment options to reduce the pain and discomfort in their bodies and help improve their muscle strength. Today’s article looks at how body pain can affect posture, what Pilates is, how this exercise regime can be incorporated for body pain, and its benefits. We talk with certified associated medical providers who inform our patients about how incorporating Pilates can reduce body pain. While asking associated medical providers intricate questions, we advise patients to incorporate Pilates as part of their routine and how it can improve their muscle strength. Dr. Alex Jimenez, D.C., includes this information as an academic service. Disclaimer.
How Body Pain Can Affect Posture
Do you experience stiffness or general aches and pains in different muscle areas? Do you often feel constantly tired throughout the entire day? Or do you notice your posture worsening after looking at a computer or phone screen? Many of these environmental factors can lead to pain and discomfort in the body, which then can cause issues that many individuals will tend to ignore until it becomes too much. For instance, environmental factors like obesity are commonly associated with musculoskeletal problems and incorrect body posture, which can be represented as a causal factor for impairment to the body. (Calcaterra et al., 2022) This is because many individuals don’t realize that improper posture can be associated with body pain and, if not corrected, can lead to overlapping risk factors in the musculoskeletal system. Hence, many individuals start seeking treatments to improve postural alignment, but it can also be used to prevent and treat musculoskeletal pain. (Matsutani et al., 2023)
The Non-Surgical Approach To Wellness- Video
What Is Pilates?
While many people seek treatment for their body pain and improve muscle strength, many have started exercising to reduce the stress and discomfort caused by body pains associated with the musculoskeletal system. Since everyone knows that exercising is excellent for health and wellness, it can also help make the body healthier. Many individuals looking for an exercise routine have various options, including Pilates.
Developed in the early 20th century, Joseph Pilates created a system of exercises primarily focused on controlled muscle movement, stretching, and breathing known as Pilates. It has become popular later in the years not only as a physical fitness routine but also as a rehabilitation program. (Byrnes et al., 2018) Pilates uses a combination of repetitive exercises to create muscular exertion and is designed to increase muscle strength and endurance, enhance flexibility, and improve posture and balance. (Kloubec, 2011)
How Is It Incorporated For Body Pain?
While many people are dealing with body pain, some may wonder how Pilates is incorporated into a health and wellness treatment plan. Well, when environmental factors like poor posture and body pain associated with the musculoskeletal system start to cause pain and discomfort to the body. At the same time, that pain and discomfort, if not treated, will also affect the spine’s alignment, causing more musculoskeletal problems. (Shadi et al., 2024) Additionally, Pilates can be combined with non-surgical treatments like chiropractic care to help improve musculoskeletal pain and restore a person’s strength, flexibility, and mobility. This, in turn, promotes mindfulness and a faster recovery. Many individuals will begin to notice that combining a therapeutic exercise method like Pilates and non-surgical treatments can allow the individual to be pain-free and experience additional benefits. This will enable people to understand the impact of stretching exercises caused by Pilates on the components of musculoskeletal fitness aimed at rehabilitation or physical conditioning. (Dos Reis et al., 2024)
The Benefits Of Pilates
Many people will notice how Pilates can help their bodies through these benefits. This includes:
Adapting Pilates to your fitness level and needs: Anyone can start Pilates at any fitness level and go at their own pace.
Core strength increases: Pilates can help strengthen the core muscles, which correlates to improved posture and a strong body.
Strengthening muscles: Pilates can help strengthen and elongate muscles to help individuals look toned.
Natural energy booster: Like many exercise routines, Pilates can give people an energy boost through focus breathing. This increases circulation, stimulating the muscles and spine.
Utilizing Pilates for rehabilitation combined with non-surgical treatment can allow individuals to be more mindful of their bodies and to make tiny changes in their routines. This allows the chances of pain and discomfort from returning, allowing individuals to have a healthier lifestyle.
References
Byrnes, K., Wu, P. J., & Whillier, S. (2018). Is Pilates an effective rehabilitation tool? A systematic review. J Bodyw Mov Ther, 22(1), 192-202. https://doi.org/10.1016/j.jbmt.2017.04.008
Calcaterra, V., Marin, L., Vandoni, M., Rossi, V., Pirazzi, A., Grazi, R., Patane, P., Silvestro, G. S., Carnevale Pellino, V., Albanese, I., Fabiano, V., Febbi, M., Silvestri, D., & Zuccotti, G. (2022). Childhood Obesity and Incorrect Body Posture: Impact on Physical Activity and the Therapeutic Role of Exercise. Int J Environ Res Public Health, 19(24). https://doi.org/10.3390/ijerph192416728
Dos Reis, A. L., de Oliveira, L. C., & de Oliveira, R. G. (2024). Effects of stretching in a pilates program on musculoskeletal fitness: a randomized clinical trial. BMC Sports Sci Med Rehabil, 16(1), 11. https://doi.org/10.1186/s13102-024-00808-6
Matsutani, L. A., Sousa do Espirito Santo, A., Ciscato, M., Yuan, S. L. K., & Marques, A. P. (2023). Global posture reeducation compared with segmental muscle stretching exercises in the treatment of fibromyalgia: a randomized controlled trial. Trials, 24(1), 384. https://doi.org/10.1186/s13063-023-07422-w
Shadi, N., Khalaghi, K., & Seyedahmadi, M. (2024). Comparing the effects of Pilates, corrective exercises, and Alexander’s technique on upper cross syndrome among adolescent girls student (ages 13-16): a six-week study. BMC Sports Sci Med Rehabil, 16(1), 143. https://doi.org/10.1186/s13102-024-00933-2
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine