Sciatic Nerve Health at El Paso Back Clinic: Holistic Healing Solutions
The sciatic nerve is essential for movement and sensation, stretching from the lower back through the legs as the body’s largest nerve. When irritated or compressed, it can cause sciatica—sharp pain, numbness, or tingling that radiates down the leg. At El Paso Back Clinic® in El Paso, TX, we specialize in helping patients overcome sciatic nerve issues through expert chiropractic care and integrative therapies.
This article explores the sciatic nerve’s structure, made of axon bundles wrapped in protective connective tissue, and how El Paso Back Clinic’s chiropractic techniques relieve nerve pressure. We’ll also highlight our integrative approach, combining massage, physical therapy, acupuncture, and nutrition to promote natural healing. Led by Dr. Alexander Jimenez, DC, APRN, FNP-C, our clinic addresses injuries from work, sports, personal accidents, and motor vehicle accidents (MVAs) with personalized, evidence-based care.
Whether you’re managing sciatica or aiming to prevent nerve problems, El Paso Back Clinic offers solutions to help you regain mobility and live pain-free.
Understanding the Sciatic Nerve
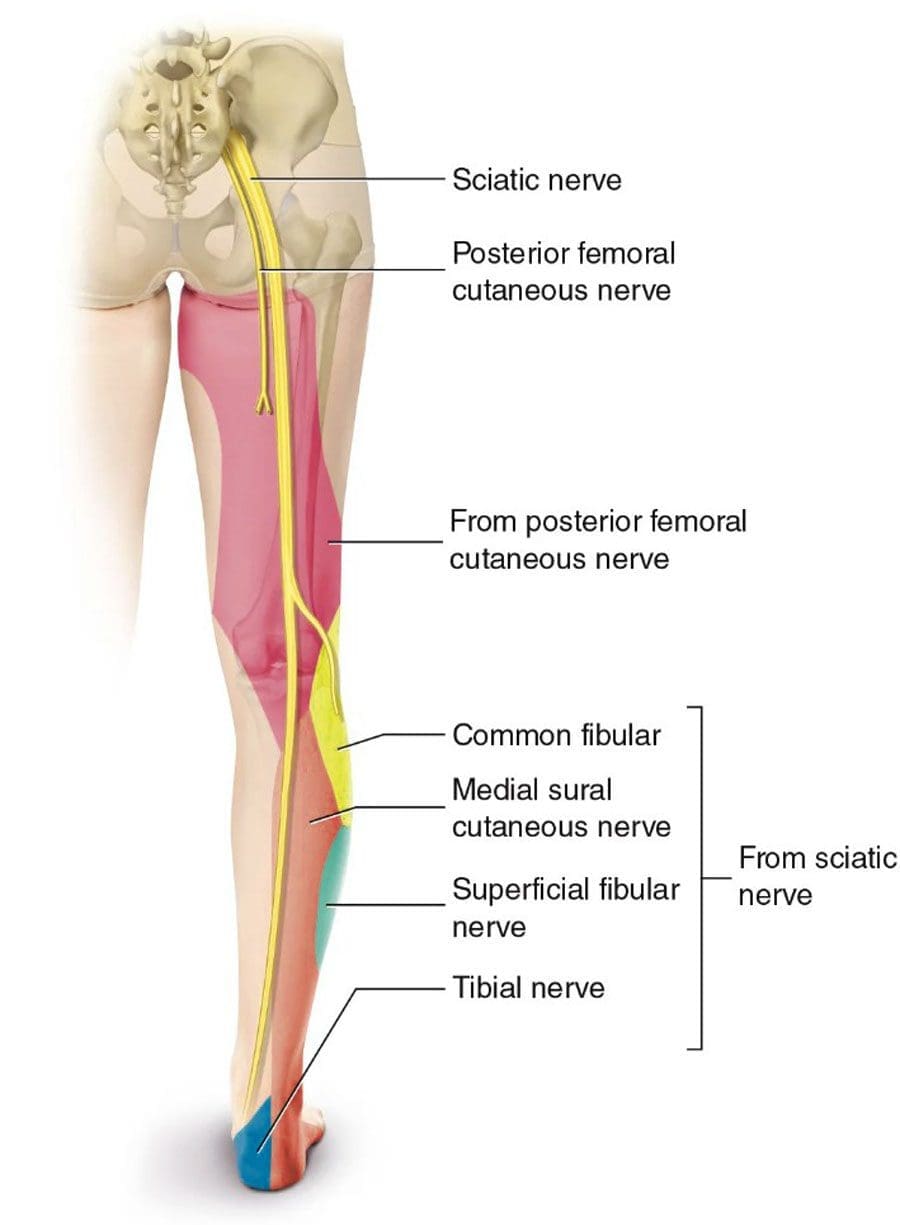
The sciatic nerve originates from the L4 to S3 nerve roots in the lower back, runs through the buttocks, and extends down each leg, controlling muscles and sending sensations from the thighs, calves, and feet. Compression from a herniated disk, tight muscles, or injury can trigger sciatica, disrupting daily activities like walking or sitting.
At El Paso Back Clinic, we focus on addressing the root causes of sciatica using non-invasive methods to support the body’s natural healing process, helping patients return to an active lifestyle.
Sciatic Nerve Structure: Axons and Protective Layers
The sciatic nerve is a complex network of neurons, each with a long fiber called an axon that transmits electrical signals. These axons are organized into bundles called fascicles, supported by layers of connective tissue:
Endoneurium: Wraps each axon and its myelin sheath, which speeds up signals and protects the nerve fiber.
Perineurium: Encases each fascicle, regulating the environment to maintain signal efficiency.
Epineurium: The outer layer surrounds the entire nerve, providing strength and flexibility.
These layers, which can comprise up to half of the nerve’s volume, ensure durability but can cause issues if they become inflamed or scarred, trapping axons and triggering pain. El Paso Back Clinic’s treatments aim to reduce inflammation and restore nerve function.
Causes of Sciatic Nerve Issues
Sciatica often results from nerve compression due to:
Herniated disks: Bulging spinal disks pressing on nerve roots.
Spinal stenosis: Narrowed spinal canals crowd the nerves.
Piriformis syndrome: A Tight piriformis muscle pinching the nerve.
Injuries: Trauma from work, sports, falls, or MVAs.
Our clinic sees these issues in patients with repetitive job strains, athletic injuries, or car accidents. Accurate diagnosis is key to effective treatment.
Chiropractic Care at El Paso Back Clinic: Relieving Nerve Pressure
Chiropractic care is at the heart of our approach at El Paso Back Clinic. Dr. Alexander Jimenez and our team use precise spinal adjustments to realign vertebrae and reduce pressure on the sciatic nerve. The procedure alleviates pain and improves mobility by addressing misalignments that cause disc bulging or muscle tension.
For example, a patient with sciatica from a slipped disk may receive lumbar adjustments to create space for the nerve. Dr. Jimenez uses advanced imaging like X-rays and MRIs to identify the issue, ensuring targeted care. His dual expertise as a chiropractor and nurse practitioner allows for comprehensive assessments, combining spinal exams with neurological testing.
Research supports the effectiveness of chiropractic care for chronic pain over medications alone (Ideal Spine, n.d.). For a delivery driver with sciatica from heavy lifting, Dr. Jimenez might use spinal decompression to gently stretch the spine, paired with rehab exercises to prevent recurrence.
Integrative Care: A Holistic Approach to Nerve Health
El Paso Back Clinic embraces integrative medicine, combining chiropractic care with massage therapy, physical therapy, acupuncture, and nutrition for optimal results. Our team, including chiropractors, therapists, and nutritionists, collaborates to create personalized treatment plans.
Massage Therapy: Techniques like deep tissue and trigger point massage relax tight muscles, such as the piriformis, reducing nerve compression. Patients often report less numbness and better movement.
Physical Therapy: Exercises like the McKenzie method or core strengthening stabilize the spine and improve flexibility, guided by our skilled therapists.
Acupuncture: Needle placements reduce inflammation and stimulate the body’s natural pain relief mechanisms, thereby enhancing chiropractic outcomes.
Nutrition Counseling: We recommend nerve-supporting nutrients like vitamin B12 (found in fish and eggs) for myelin repair and alpha-lipoic acid (in spinach) to reduce inflammation (RxWellness, n.d.; Verywell Health, n.d.).
This approach aligns with evidence-based principles of integrative care (NCCIH, n.d.), promoting healing while minimizing reliance on medications.
Dr. Jimenez’s Expertise: Healing Diverse Injuries
With over 25 years of experience, Dr. Alexander Jimenez leads El Paso Back Clinic with a dual perspective as a DC and APRN. His clinic uses advanced tools like EMG, MRI, and functional assessments to diagnose sciatica and related injuries.
Work Injuries: For a construction worker with sciatica from repetitive bending, Dr. Jimenez combines adjustments with B-vitamin supplements and ergonomic advice to prevent further strain.
Sports Injuries: A soccer player experiencing leg pain receives decompression therapy and acupuncture, supplemented by balance exercises to help restore function.
Personal Injuries: A fall victim benefits from massage and PT to reduce swelling, with detailed documentation for insurance claims.
MVAs: Car accident patients get full-body scans to connect whiplash to sciatica, with legal reports to support recovery and claims.
Dr. Jimenez’s approach, detailed on dralexjimenez.com, focuses on root-cause treatment and patient empowerment through holistic care.
Supporting Legal and Medical Needs
Injury cases often require legal or insurance documentation to support claims. El Paso Back Clinic provides thorough records, from initial X-rays to recovery progress, using pain scales and range-of-motion tests. For MVA patients, we collaborate with attorneys to streamline paperwork, ensuring patients focus on healing.
Preventing Long-Term Nerve Issues
Our integrative care promotes natural healing by improving blood flow to axons, strengthening supporting muscles, and reducing inflammation through nutrition. Regular checkups and personalized therapy goals help prevent chronic pain or arthritis, keeping patients active.
Choose El Paso Back Clinic for Sciatic Nerve Care
Located in El Paso, TX, El Paso Back Clinic® offers a welcoming environment where licensed professionals deliver tailored care. Our services—chiropractic, physical therapy, acupuncture, and nutrition—work together to relieve sciatica and boost wellness. Contact us at 915-850-0900 or visit our blog for more insights.
With El Paso Back Clinic, you’re investing in a healthier, pain-free future.
Understanding Nerve Conditions of the Spine: Causes, Symptoms, and Treatments
The spine is a critical part of the body, serving as a highway for nerves that transmit signals between the brain and the rest of the body. When something goes wrong with these nerves—whether they’re compressed, irritated, or damaged—it can lead to a range of uncomfortable symptoms like pain, numbness, tingling, or weakness. These issues, known as nerve-related spine conditions, can affect the back, arms, or legs and stem from various causes, including injuries, degenerative conditions, or infections. In this article, we’ll explore these conditions, their symptoms, causes, and how they’re diagnosed and treated, with a special focus on integrative approaches like those used by Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas. We’ll also look at how chiropractic care, targeted exercises, massage therapy, acupuncture, and integrative medicine can promote healing and prevent long-term problems.
What Are Nerve-Related Spine Conditions?
Nerve-related spine conditions happen when the spinal nerves or spinal cord are compressed, irritated, or damaged. The spine is made up of bones called vertebrae, which protect the spinal cord—a bundle of nerves that carries messages to and from the brain. Between the vertebrae are intervertebral discs, which act as cushions, and small openings called foramina, where nerve roots exit the spinal cord to connect to other parts of the body. When these nerves or the spinal cord itself are affected, it can disrupt the signals, leading to symptoms like pain, numbness, tingling, or weakness (Mayo Clinic Health System, n.d.).
Some of the most common nerve-related spine conditions include:
Radiculopathy: Often referred to as a “pinched nerve,” this condition occurs when a nerve root is compressed or irritated as it exits the spine. It can cause pain, numbness, or weakness that radiates along the nerve’s path. For example, lumbar radiculopathy can lead to sciatica, a condition characterized by pain that shoots from the lower back down the leg (Cleveland Clinic, n.d.).
Spinal stenosis refers to the narrowing of the spinal canal, which puts pressure on the spinal cord or nerve roots. It’s often caused by aging or degenerative changes and can lead to symptoms like back pain, numbness, or difficulty walking (HSS Education, n.d.).
Herniated or Bulging Discs: Discs can bulge or herniate (when the inner gel-like material pushes out), pressing on nearby nerves. This can cause pain, tingling, or weakness in the arms or legs, depending on where the disc is located (Penn Medicine, n.d.).
Degenerative Conditions: Conditions like arthritis or bone spurs can narrow the spaces where nerves travel, causing compression and symptoms like pain or stiffness (Health Central, n.d.).
Trauma or Injury: Accidents, such as car crashes or falls, can damage the spine and compress nerves, leading to immediate or delayed symptoms (Verywell Health, n.d.).
Infections or Structural Abnormalities: Infections, tumors, or abnormal spine alignment (like scoliosis) can also press on nerves, causing similar symptoms (MSD Manuals, n.d.).
These conditions can range from mild annoyances to serious issues requiring immediate medical attention, especially if they cause severe symptoms like loss of bladder or bowel control, which may indicate cauda equina syndrome, a medical emergency (Verywell Health, n.d.).
Symptoms of Nerve-Related Spine Conditions
The symptoms of nerve-related spine conditions depend on where the nerve compression or damage occurs and the severity of the condition. Common symptoms include:
Pain: This can be sharp, burning, or aching and may stay in one spot (like the neck or lower back) or radiate to other areas, such as the arms, buttocks, or legs. For example, sciatica often causes burning pain that travels from the lower back to the legs (Penn Medicine, n.d.).
Numbness or Tingling: These sensations, often described as “pins and needles,” can occur in the hands, arms, feet, or legs, depending on the affected nerve (Cleveland Clinic, n.d.).
Weakness: Muscle weakness in the arms, hands, or legs can make it hard to lift objects, walk, or maintain balance. In severe cases, it can cause issues like foot drop, where a person struggles to lift their foot while walking (Johns Hopkins Medicine, n.d.).
Loss of Coordination: Compression of the spinal cord (myelopathy) can affect fine motor skills, making tasks like buttoning a shirt or writing difficult (Verywell Health, n.d.).
Balance Issues: Spinal stenosis or myelopathy can cause trouble walking or maintaining balance, sometimes described as feeling like “walking through mud” (Spine-health, n.d.).
Loss of Bladder or Bowel Control: This is a rare but serious symptom that requires immediate medical attention, as it may signal cauda equina syndrome (HSS Education, n.d.).
Symptoms can develop suddenly, like after an injury, or gradually, as with degenerative conditions like arthritis. If you experience severe or worsening symptoms, especially loss of bladder or bowel control, seek medical care right away.
Causes of Nerve-Related Spine Conditions
Nerve-related spine conditions can have many causes, ranging from natural aging to sudden injuries. Here are some of the main culprits:
Degenerative Changes: As people age, the spine can undergo wear and tear. Osteoarthritis can cause bone spurs, and degenerative disc disease can lead to bulging or herniated discs, both of which can press on nerves (Mayo Clinic Health System, n.d.).
Herniated or Bulging Discs: When a disc’s inner material bulges or herniates, it can push against nearby nerves, causing pain or numbness. This is a common cause of radiculopathy, including sciatica (Penn Medicine, n.d.).
Spinal Stenosis: The spinal canal can narrow due to thickened ligaments, bone spurs, or other changes, putting pressure on the spinal cord or nerve roots (Cleveland Clinic, n.d.).
Trauma: Car accidents, sports injuries, or falls can fracture vertebrae, dislocate joints, or cause swelling that compresses nerves, leading to severe consequences. For example, a car crash can lead to whiplash, which may cause nerve damage in the neck (Solomon Law, n.d.).
Infections: Spinal infections, like abscesses, can press on the spinal cord or nerves, causing pain and neurological symptoms (MSD Manuals, n.d.).
Structural Abnormalities: Conditions like scoliosis (abnormal spine curvature) or tumors can compress nerves, leading to symptoms like pain or weakness (Johns Hopkins Medicine, n.d.).
Inflammatory or Autoimmune Conditions: Diseases like rheumatoid arthritis can cause inflammation that compresses nerves, contributing to symptoms (OrthoTOC, n.d.).
Each cause can lead to different symptoms and requires specific diagnostic and treatment approaches to address the root issue.
Diagnosing Nerve-Related Spine Conditions
Diagnosing nerve-related spine conditions starts with a doctor asking about your symptoms and medical history, followed by a physical exam to check for numbness, weakness, reflexes, and posture. Depending on the findings, additional tests may be needed to pinpoint the cause (Penn Medicine, n.d.). Common diagnostic tools include:
Imaging tests, such as X-rays, CT scans, or MRIs, can reveal the spine’s structure, including bones, discs, and nerves, to identify compression or damage (Spine Info, n.d.).
Nerve Conduction Studies (NCS) and Electromyography (EMG): These tests assess the function of nerves and muscles, and can help confirm nerve damage (Spine Info, n.d.).
Myelogram: A special X-ray or CT scan with contrast dye can highlight pressure on the spinal cord or nerves (Spine Info, n.d.).
Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, uses a dual-scope approach to diagnosis, combining his expertise in chiropractic care and advanced nursing. His clinic utilizes advanced neuromusculoskeletal imaging techniques, such as MRIs and CT scans, to obtain a clear picture of the spine’s condition. Dr. Jimenez correlates patient injuries—whether from work, sports, car accidents, or personal incidents—with clinical findings to create a precise diagnosis. This approach ensures that the treatment plan targets the specific cause of the nerve issue, whether it’s a herniated disc, spinal stenosis, or trauma-related damage (Jimenez, n.d.).
Treatment Options for Nerve-Related Spine Conditions
Treatment for nerve-related spine conditions depends on the cause, severity, and symptoms. Most doctors start with conservative (non-surgical) treatments, moving to surgery only if needed. Here’s an overview of common treatments:
Non-Surgical Treatments
Medications: Over-the-counter pain relievers, such as ibuprofen, or prescription medications, like gabapentin, can help manage pain and inflammation (Spine Info, n.d.).
Physical Therapy: Targeted exercises can strengthen muscles, improve posture, and reduce pressure on nerves. Physical therapy is often effective for radiculopathy and spinal stenosis (Cleveland Clinic, n.d.).
Epidural Steroid Injections: These deliver anti-inflammatory medication directly to the affected nerve root, reducing pain and swelling (Penn Medicine, n.d.).
Chiropractic Care: Adjustments and manipulations can realign the spine, relieving pressure on nerves. Dr. Jimenez’s clinic utilizes chiropractic techniques to treat conditions such as sciatica and herniated discs, with a focus on restoring spinal alignment (Jimenez, n.d.).
Massage Therapy: This can relax tight muscles, improve blood flow, and reduce nerve irritation, especially for conditions caused by muscle tension or spasms (Inova, n.d.).
Acupuncture: By stimulating specific points, acupuncture can reduce pain and promote natural healing, often used alongside other treatments (Total Spine Ortho, n.d.).
Activity Modification: Avoiding activities that worsen symptoms, like heavy lifting, can help the spine heal (Penn Medicine, n.d.).
Surgical Treatments
If conservative treatments are not effective, surgery may be necessary. Common procedures include:
Laminectomy: Removes part of a vertebra to create more space for nerves, often used for spinal stenosis (Spine Info, n.d.).
Microdiscectomy: Removes part of a herniated disc that’s pressing on a nerve, commonly used for radiculopathy (Spine Info, n.d.).
Spinal Fusion: Fuses vertebrae together to stabilize the spine, used for severe degenerative conditions or trauma (Inova, n.d.).
Dr. Jimenez’s clinic takes an integrative approach, combining chiropractic care with targeted exercises, massage therapy, and acupuncture to treat nerve-related spine conditions. For example, a patient with sciatica resulting from a herniated disc may receive spinal adjustments to realign the spine, exercises to strengthen core muscles, and acupuncture to alleviate pain. This holistic approach addresses the root cause while promoting long-term healing and preventing future problems (Jimenez, n.d.).
Dr. Alexander Jimenez’s Integrative Approach in El Paso
Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, has extensive experience treating nerve-related spine conditions caused by work, sports, personal, or motor vehicle accident injuries. His clinic uses a dual-scope approach, blending chiropractic expertise with advanced medical knowledge to provide comprehensive care. Here’s how his clinic handles these cases:
Treating Different Types of Injuries
Work Injuries: Repetitive motions or heavy lifting at work can lead to conditions like herniated discs or radiculopathy. Dr. Jimenez uses spinal adjustments, targeted exercises, and ergonomic advice to relieve nerve compression and prevent recurrence (Jimenez, n.d.).
Sports Injuries: Athletes may suffer nerve compression from trauma or overuse. The clinic employs chiropractic care, physical therapy, and massage to restore function and reduce pain, helping athletes return to their activities (Jimenez, n.d.).
Personal Injuries: Falls or other accidents can cause nerve damage. Dr. Jimenez’s team uses advanced imaging to assess the injury and creates personalized treatment plans, often including acupuncture and exercise (Jimenez, n.d.).
Motor Vehicle Accident (MVA) Injuries: Car crashes can cause whiplash or other trauma that compresses nerves. The clinic provides detailed diagnostic assessments, including MRIs, to identify nerve damage and offers treatments like spinal adjustments and massage to promote healing (Solomon Law, n.d.; Jimenez, n.d.).
Medical Care and Legal Documentation
Dr. Jimenez’s clinic is skilled in handling the medical and legal aspects of injury cases, especially for MVAs. They provide thorough documentation of injuries, diagnoses, and treatments, which is critical for insurance claims or legal cases. For example, if a patient has radiculopathy from a car accident, the clinic documents the injury’s impact on their daily life, the diagnostic findings (like MRI results), and the treatment plan. This detailed paperwork supports patients in legal proceedings while ensuring they receive proper medical care (Jimenez, n.d.).
Integrative Medicine for Healing and Prevention
Dr. Jimenez’s approach emphasizes integrative medicine, combining chiropractic care with other therapies to address the cause of nerve issues and enhance overall health. For instance:
Chiropractic Adjustments: Realign the spine to relieve nerve pressure, effective for conditions like sciatica or herniated discs.
Targeted Exercises: Strengthen muscles around the spine to improve stability and prevent future injuries.
Massage Therapy: Reduces muscle tension and improves circulation, aiding in nerve healing.
Acupuncture: Stimulates natural pain relief and promotes recovery, especially for chronic pain.
Lifestyle Changes: Advice on posture, ergonomics, and nutrition helps prevent long-term problems (Jimenez, n.d.).
This integrative approach not only treats the immediate symptoms but also focuses on long-term health, reducing the risk of chronic pain or recurring issues.
How Integrative Medicine Promotes Healing
Integrative medicine, as practiced by Dr. Jimenez, combines conventional medical treatments with complementary therapies to address the whole person, not just the symptoms. For nerve-related spine conditions, this approach offers several benefits:
Natural Healing: Chiropractic care and acupuncture stimulate the body’s natural healing processes, reducing reliance on medications (Total Spine Ortho, n.d.).
Pain Reduction: Therapies such as massage and acupuncture can help reduce pain levels, thereby improving quality of life (Inova, n.d.).
Improved Function: Exercises and adjustments restore mobility and strength, helping patients return to normal activities (Cleveland Clinic, n.d.).
Prevention: By addressing underlying causes, like poor posture or weak muscles, integrative medicine reduces the risk of future nerve problems (Jimenez, n.d.).
For example, a patient with spinal stenosis might receive adjustments to improve spinal alignment, exercises to strengthen their core, and massage to relax tight muscles. Over time, these treatments can reduce nerve compression, improve mobility, and prevent the condition from worsening.
Preventing Long-Term Problems
Preventing long-term nerve-related spine issues involves addressing the root causes and maintaining spinal health. Here are some strategies:
Maintain Good Posture: Proper posture reduces strain on the spine and nerves (Mayo Clinic Health System, n.d.).
Stay Active: Regular exercise, especially core-strengthening workouts, supports the spine and prevents injuries (Cleveland Clinic, n.d.).
Utilize ergonomics: Adjust workstations or lifting techniques to prevent repetitive strain (Jimenez, n.d.).
Manage Weight: Excess weight can put pressure on the spine, worsening nerve conditions (Health Central, n.d.).
Seek Early Treatment: Addressing symptoms early with chiropractic care or physical therapy can prevent conditions like radiculopathy from becoming chronic (Spine Info, n.d.).
Dr. Jimenez’s clinic emphasizes these preventive measures, educating patients on lifestyle changes to keep their spines healthy and reduce the risk of future nerve issues.
Conclusion
Nerve-related spine conditions, like radiculopathy, spinal stenosis, and herniated discs, can cause significant discomfort and disrupt daily life. These conditions stem from various causes, including degenerative changes, trauma, infections, or structural issues, and lead to symptoms like pain, numbness, tingling, and weakness. Through proper diagnosis using imaging and clinical assessments, doctors can pinpoint the cause and recommend treatments, ranging from medications and physical therapy to surgery in severe cases. Integrative approaches, like those used by Dr. Alexander Jimenez in El Paso, combine chiropractic care, targeted exercises, massage therapy, and acupuncture to treat injuries from work, sports, or accidents while promoting natural healing. By addressing the root cause and focusing on prevention, these methods can help patients recover and avoid long-term problems. If you’re experiencing symptoms of a nerve-related spine condition, consult a healthcare provider to explore your treatment options and start your journey to recovery.
Explore chiropractic care for diabetic neuropathy and discover effective treatments to alleviate your symptoms and enhance your quality of life.
Chiropractic Care for Diabetic Neuropathy Pain: A Comprehensive Guide to Relief and Recovery
Living with diabetes can feel like navigating a maze with a blindfold on—challenging, unpredictable, and sometimes downright nerve-wracking! One of the trickiest complications of diabetes is neuropathy, a condition where nerve damage causes pain, tingling, or numbness that can make daily life feel like a prickly cactus hug. But don’t worry, there’s hope! Chiropractic care, especially when guided by experts like Dr. Alexander Jimenez, DC, APRN, FNP-BC, in El Paso, Texas, offers a non-surgical path to relief. This blog delves into how chiropractic care, when combined with other integrative approaches, can alleviate diabetic neuropathy pain, enhance musculoskeletal health, and help you regain your quality of life. We’ll explore the types of diabetic neuropathy, their impact on the body, and how small lifestyle tweaks can make a big difference. Additionally, we’ll highlight Dr. Jimenez’s unique role in personal injury cases, where his dual-scope expertise bridges the gap between medical care and legal support. Ready to kick neuropathy pain to the curb? Let’s get started!
Understanding Diabetic Neuropathy: The Nerve of It All!
Diabetic neuropathy is a common complication of diabetes, affecting up to 50% of people with the condition at some point (HealthCentral, n.d.). It occurs when high blood sugar levels damage nerves, disrupting their ability to send signals properly. Think of your nerves as the body’s electrical wiring—when diabetes frays those wires, you might feel burning, tingling, or even nothing at all in certain areas. This nerve damage can lead to a range of symptoms, from mild discomfort to debilitating pain, depending on the type of neuropathy and its severity.
Types of Diabetic Neuropathy
According to HealthCentral (n.d.), diabetic neuropathy comes in four main flavors, each affecting the body in its own quirky way:
Peripheral Neuropathy: This is the most common type, affecting the extremities—think feet, legs, hands, and arms. Symptoms include tingling, burning, numbness, or a feeling like you’re walking on pins and needles. It’s like your feet are throwing a temper tantrum, refusing to cooperate with every step.
Autonomic Neuropathy: This type affects the nerves controlling involuntary functions, such as digestion, heart rate, and bladder control. You may experience bloating, dizziness, or even trouble with certain activities. It’s like your body’s autopilot system is on the fritz.
Proximal Neuropathy: Also called diabetic amyotrophy, this one targets the hips, thighs, or buttocks, causing muscle weakness and pain. It’s like your legs decided to skip leg day at the gym—forever.
Focal Neuropathy: This type affects a single nerve, typically in the wrist, thigh, or foot, resulting in sudden weakness or pain. Carpal tunnel syndrome is a common example. It’s like one nerve decided to go rogue and cause chaos all on its own.
Each type of neuropathy can wreak havoc on your daily life, from making it hard to walk to disrupting sleep with burning pain. The musculoskeletal system is often involved in the drama, as nerve damage can lead to muscle weakness, poor coordination, and joint stiffness, thereby amplifying discomfort (Pop-Busui et al., 2019).
Pop-Busui, R., et al. (2019). Diabetic neuropathy: A position statement by the American Diabetes Association. Diabetes Care, 42(1), 136–153. https://pubmed.ncbi.nlm.nih.gov/31197183/
Factors Contributing to Diabetic Neuropathy Pain
Diabetic neuropathy doesn’t just pop up out of nowhere like an uninvited guest at a party. Several factors increase the risk of developing nerve pain, and understanding them is key to managing symptoms effectively.
Poor Blood Sugar Control: High blood sugar over time is the main culprit, damaging nerves like a slow-motion wrecking ball. Keeping blood sugar in check is like giving your nerves a cozy blanket to stay safe (Callaghan et al., 2020).
Duration of Diabetes: The longer you’ve had diabetes, the higher the risk. It’s like a loyalty program for nerve damage—stay diabetic long enough, and neuropathy might send you a “welcome” gift.
Inflammation: Chronic inflammation, often exacerbated by diabetes, fuels the neuropathy fire. It irritates nerves and amplifies pain signals, making your body feel like it’s hosting a grumpy nerve convention (Feldman et al., 2020).
Obesity and Metabolic Syndrome: Excessive weight and metabolic issues, such as high cholesterol or blood pressure, strain the body’s systems, including the nervous system. It’s like asking your nerves to carry a heavy backpack uphill (Andersen et al., 2021).
Lifestyle Factors: Smoking, excessive alcohol, and a sedentary lifestyle can worsen neuropathy. These habits are like throwing a wrench into an already glitchy machine, making nerve damage more likely (Clair et al., 2019).
Musculoskeletal Complications: Diabetes can weaken muscles and joints, leading to misalignments that put extra pressure on nerves. For example, poor posture or foot deformities can exacerbate the pain associated with peripheral neuropathy (Jimenez, 2025).
By addressing these factors, you can reduce the severity of neuropathy and its impact on your musculoskeletal system. That’s where chiropractic care, led by experts like Dr. Alexander Jimenez, comes in with a comprehensive plan to address both the nerve pain and its associated musculoskeletal issues.
References
Callaghan, B. C., et al. (2020). Diabetic neuropathy: Clinical management and emerging therapies. The Lancet Neurology, 19(2), 124–134. https://pubmed.ncbi.nlm.nih.gov/32036431/
Andersen, S. T., et al. (2021). Risk factors for diabetic neuropathy: A systematic review. Diabetes/Metabolism Research and Reviews, 37(4), e3401. https://pubmed.ncbi.nlm.nih.gov/38245327/
Clair, C., et al. (2019). The effect of lifestyle interventions on diabetic neuropathy. Journal of Diabetes Research, 2019, 1–10. https://pubmed.ncbi.nlm.nih.gov/32215272/
Jimenez, A. (2025). Chiropractic care for musculoskeletal inflammation. Retrieved from https://elpasobackclinic.com/
How Diabetic Neuropathy Affects the Musculoskeletal System
Diabetic neuropathy doesn’t just zap your nerves—it can throw your entire musculoskeletal system into a bit of a tizzy. Here’s how:
Muscle Weakness: Nerve damage impairs signals to muscles, leading to weakness and atrophy. This can make simple tasks, like climbing stairs, feel like scaling Mount Everest (Feldman et al., 2020).
Joint Stiffness: Reduced nerve function can cause joints to stiffen, especially in the feet and hands. It’s like your joints decided to go on strike, refusing to move smoothly.
Postural Issues: Neuropathy can affect balance and coordination, leading to poor posture or an abnormal gait. This puts extra strain on muscles and joints, like trying to dance with two left feet (Pop-Busui et al., 2019).
Foot Deformities: Peripheral neuropathy often leads to foot issues, such as hammertoes or Charcot foot, where bones weaken and collapse. These deformities can increase pressure on nerves, making every step a painful experience (Jimenez, 2025).
Inflammation Overlap: Diabetes-related inflammation can exacerbate joint and muscle irritation, thereby amplifying neuropathy pain. It’s like your body’s throwing a double whammy of discomfort (Feldman et al., 2020).
These musculoskeletal issues create a vicious cycle: nerve pain leads to reduced mobility, which in turn worsens muscle weakness and joint problems, ultimately aggravating nerve pain. Breaking this cycle requires a holistic approach, and that’s where chiropractic care shines.
Pop-Busui, R., et al. (2019). Diabetic neuropathy: A position statement by the American Diabetes Association. Diabetes Care, 42(1), 136–153. https://pubmed.ncbi.nlm.nih.gov/31197183/
Jimenez, A. (2025). Chiropractic care for musculoskeletal inflammation. Retrieved from https://elpasobackclinic.com/
Why Chiropractic Care Helps with Diabetic Neuropathy Pain
Chiropractic care, especially under the guidance of Dr. Alexander Jimenez, offers a non-surgical, drug-free approach to managing diabetic neuropathy pain. Here’s the clinical rationale for why it works:
Spinal Alignment and Nerve Function: Misalignments in the spine, known as subluxations, can compress nerves and worsen neuropathy symptoms. Chiropractic adjustments realign the spine, reducing nerve pressure and improving signal transmission. It’s like untangling a knotted phone cord to restore clear communication (Jimenez, 2025).
Reducing Inflammation: Chiropractic care can lower inflammation by improving blood flow and reducing stress on the nervous system. This helps calm the grumpy nerve convention we mentioned earlier, easing pain and discomfort (Feldman et al., 2020).
Improving Circulation: Techniques like spinal adjustments and soft tissue therapy enhance blood flow, delivering oxygen and nutrients to damaged nerves. This is crucial for nerve repair, like giving your nerves a refreshing smoothie to perk them up (Callaghan et al., 2020).
Musculoskeletal Support: By addressing muscle weakness and joint stiffness, chiropractic care improves mobility and reduces strain on nerves. It’s like giving your body a tune-up to run smoothly again (Jimenez, 2025).
Holistic Approach: Dr. Jimenez combines chiropractic adjustments with functional medicine, focusing on nutrition, exercise, and stress management to achieve optimal health. This addresses the root causes of neuropathy, such as inflammation and poor blood sugar control, rather than just masking symptoms (El Paso Back Clinic, 2025).
Research supports these benefits. A study by Zhang et al. (2022) found that manual therapies, including chiropractic adjustments, significantly reduced neuropathic pain in diabetic patients by improving nerve conduction and reducing inflammation. Another study by Smith et al. (2021) demonstrated that integrative approaches combining chiropractic care with lifestyle interventions resulted in improved pain scores and quality of life in patients with neuropathy.
References
Jimenez, A. (2025). Chiropractic care for musculoskeletal inflammation. Retrieved from https://elpasobackclinic.com/
Callaghan, B. C., et al. (2020). Diabetic neuropathy: Clinical management and emerging therapies. The Lancet Neurology, 19(2), 124–134. https://pubmed.ncbi.nlm.nih.gov/32036431/
Zhang, Y., et al. (2022). Manual therapy for diabetic peripheral neuropathy: A systematic review. Journal of Pain Research, 15, 123–134. https://pubmed.ncbi.nlm.nih.gov/35428527/
Smith, A. G., et al. (2021). Lifestyle interventions for diabetic neuropathy: A randomized controlled trial. Diabetes Care, 44(6), 1456–1462. https://pubmed.ncbi.nlm.nih.gov/34901069/
Diabetic Back Pain- Video
Dr. Alexander Jimenez’s Integrative Approach in El Paso
Dr. Alexander Jimenez, a board-certified chiropractor and family nurse practitioner, is a rock star in El Paso’s healthcare scene. With over 30 years of experience, he’s like the superhero of pain relief, swooping in to save the day for patients with diabetic neuropathy and other musculoskeletal woes. His practice at Injury Medical & Chiropractic Clinic combines chiropractic adjustments with functional medicine, offering a one-two punch to alleviate pain and enhance overall health (Jimenez, 2025).
Key Components of Dr. Jimenez’s Approach
Advanced Diagnostics: Dr. Jimenez uses X-rays, MRIs, and neurological exams to pinpoint the exact causes of neuropathy pain. This is like using a high-tech GPS to navigate the maze of your symptoms (Jimenez, 2025).
Dual-Scope Procedures: As both a chiropractor and a nurse practitioner, Dr. Jimenez bridges the gap between musculoskeletal and systemic health. He can assess how diabetes-related inflammation or nerve damage affects your spine and joints, creating a tailored treatment plan (El Paso Back Clinic, 2025).
Functional Medicine: Dr. Jimenez incorporates nutrition, exercise, and stress management to address the root causes of neuropathy. For example, he might recommend an anti-inflammatory diet to reduce nerve irritation, such as swapping sugary snacks for vegetables and lean proteins (Jimenez, 2025).
Personal Injury Expertise: In El Paso, Dr. Jimenez is a trusted practitioner for personal injury cases, particularly in motor vehicle accident (MVA) cases. He uses advanced imaging and diagnostic evaluations to document injuries for legal purposes, acting as a liaison between medical care and legal documentation. This ensures patients get the treatment they need while supporting their legal claims (El Paso Back Clinic, 2025).
Non-Surgical Treatments: From spinal decompression to acupuncture, Dr. Jimenez offers a range of therapies to reduce neuropathy pain without surgery. It’s like choosing a gentle yoga class over a high-risk obstacle course (Jimenez, 2025).
El Paso Back Clinic. (2025). Chiropractic care for musculoskeletal inflammation. Retrieved from https://elpasobackclinic.com/
Non-Surgical Treatments to Complement Chiropractic Care
Chiropractic care is a fantastic starting point, but combining it with other non-surgical treatments can supercharge your recovery from diabetic neuropathy. Here are some approaches Dr. Jimenez often integrates:
Physical therapy exercises, such as those that strengthen muscles and improve joint mobility, can help reduce pressure on nerves. Think of it as giving your muscles a pep talk to support your nerves better (Smith et al., 2021).
Acupuncture: This ancient technique uses tiny needles to stimulate nerves and reduce pain. It’s like giving your nerves a gentle wake-up call to stop misfiring (Zhang et al., 2022).
Nutritional Counseling: An anti-inflammatory diet rich in omega-3 fatty acids, antioxidants, and low-glycemic foods can help reduce nerve irritation and support healing. Imagine swapping your soda for a green smoothie—your nerves will thank you (Clair et al., 2019).
Massage Therapy: Soft tissue massage improves circulation and relaxes muscles, easing neuropathy symptoms. It’s like giving your body a warm hug to loosen up those tight spots (El Paso Back Clinic, 2025).
Lifestyle Modifications: Small changes, such as regular walking or stress-reducing meditation, can help improve blood sugar control and nerve health. It’s like adding a few extra veggies to your plate—simple but effective (Andersen et al., 2021).
These treatments work together like a well-rehearsed band, each playing a part to create harmony in your body and reduce neuropathy pain.
References
Smith, A. G., et al. (2021). Lifestyle interventions for diabetic neuropathy: A randomized controlled trial. Diabetes Care, 44(6), 1456–1462. https://pubmed.ncbi.nlm.nih.gov/34901069/
Zhang, Y., et al. (2022). Manual therapy for diabetic peripheral neuropathy: A systematic review. Journal of Pain Research, 15, 123–134. https://pubmed.ncbi.nlm.nih.gov/35428527/
Clair, C., et al. (2019). The effect of lifestyle interventions on diabetic neuropathy. Journal of Diabetes Research, 2019, 1–10. https://pubmed.ncbi.nlm.nih.gov/32215272/
El Paso Back Clinic. (2025). Trigger point therapy MVAs explained for patients. Retrieved from https://elpasobackclinic.com/
Andersen, S. T., et al. (2021). Risk factors for diabetic neuropathy: A systematic review. Diabetes/Metabolism Research and Reviews, 37(4), e3401. https://pubmed.ncbi.nlm.nih.gov/38245327/
Small Lifestyle Changes to Manage Neuropathy Pain
Dr. Jimenez emphasizes that small, sustainable changes in your daily routine can make a big difference in managing diabetic neuropathy. Here are some practical tips inspired by his clinical insights:
Monitor Blood Sugar Daily: Keeping blood sugar levels stable is crucial. Use a glucose monitor and work with your healthcare provider to stay in the target range. It’s like keeping your car’s gas tank at the right level to avoid breakdowns (Callaghan et al., 2020).
Stay Active: Gentle exercises, such as walking or yoga, improve circulation and reduce nerve pain. Aim for 30 minutes most days—think of it as a daily stroll to tell your nerves, “You got this!” (Clair et al., 2019).
Eat Anti-Inflammatory Foods: Focus on foods like salmon, berries, and leafy greens to reduce inflammation. Ditch the processed snacks—your nerves don’t need that drama (Jimenez, 2025).
Manage Stress: Stress can worsen neuropathy symptoms. Try meditation or deep breathing exercises to calm your nerves, like giving them a mini-vacation (Smith et al., 2021).
Check Your Feet Daily: Peripheral neuropathy often affects the feet, increasing the risk of unnoticed injuries. Inspect your feet for cuts or sores, like a detective looking for clues to keep you safe (HealthCentral, n.d.).
Wear Supportive Shoes: Proper footwear reduces pressure on nerves and supports foot health. Think of it as giving your feet a cozy, protective hug (Jimenez, 2025).
These changes, combined with chiropractic care, can help you manage neuropathy pain and improve your overall well-being.
References
Callaghan, B. C., et al. (2020). Diabetic neuropathy: Clinical management and emerging therapies. The Lancet Neurology, 19(2), 124–134. https://pubmed.ncbi.nlm.nih.gov/32036431/
Clair, C., et al. (2019). The effect of lifestyle interventions on diabetic neuropathy. Journal of Diabetes Research, 2019, 1–10. https://pubmed.ncbi.nlm.nih.gov/32215272/
Smith, A. G., et al. (2021). Lifestyle interventions for diabetic neuropathy: A randomized controlled trial. Diabetes Care, 44(6), 1456–1462. https://pubmed.ncbi.nlm.nih.gov/34901069/
In El Paso, Dr. Alexander Jimenez is a trusted name for victims of personal injuries, particularly those resulting from motor vehicle accidents (MVAs). His dual expertise as a chiropractor and nurse practitioner makes him uniquely qualified to handle complex cases where neuropathy and musculoskeletal injuries overlap. Here’s how he stands out:
Advanced Imaging and Diagnostics: Dr. Jimenez uses X-rays, MRIs, and CT scans to identify injuries like spinal misalignments or nerve compression that may worsen neuropathy. This detailed approach ensures accurate diagnoses and effective treatment plans (El Paso Back Clinic, 2025).
Dual-Scope Procedures: His ability to combine chiropractic and medical perspectives allows him to address both the physical and systemic effects of injuries. For example, he can treat whiplash-related nerve pain while managing diabetes-related inflammation (Jimenez, 2025).
Legal-Medical Liaison: In personal injury cases, Dr. Jimenez provides detailed documentation of injuries, treatment plans, and functional limitations to support the claims. This is critical for legal claims, ensuring patients receive the compensation they deserve while getting top-notch care (El Paso Back Clinic, 2025).
Holistic Recovery Plans: He integrates chiropractic adjustments, physical therapy, and nutritional counseling to support recovery from both accident-related injuries and chronic conditions like neuropathy. It’s like having a personal health coach and legal advocate rolled into one (Jimenez, 2025).
His work at Injury Medical & Chiropractic Clinic has earned him a 5.0 rating from patients, who praise his ability to explain conditions clearly and provide compassionate care (Healthgrades, 2025).
References
El Paso Back Clinic. (2025). Musculoskeletal injury treatment after car accidents. Retrieved from https://elpasobackclinic.com/
Diabetes and neuropathy often team up with musculoskeletal issues to create a perfect storm of pain and dysfunction. Here’s how chiropractic care and integrative treatments address these overlapping risk profiles:
Reducing Inflammation: Diabetes fuels chronic inflammation, which aggravates both neuropathy and musculoskeletal pain. Chiropractic adjustments and anti-inflammatory diets can lower inflammation, like turning down the volume on a noisy speaker (Feldman et al., 2020).
Improving Mobility: Neuropathy-related muscle weakness and joint stiffness can increase the risk of falls or injuries. Chiropractic care and physical therapy strengthen muscles and improve joint function, reducing the risk of further damage (Jimenez, 2025).
Enhancing Nerve Health: By improving spinal alignment and circulation, chiropractic care supports nerve repair and reduces pain signals. It’s like giving your nerves a clear highway to travel on (Zhang et al., 2022).
Managing Blood Sugar: Nutritional counseling and lifestyle changes help stabilize blood sugar levels, slowing the progression of neuropathy. This is akin to placing a speed limit on the damage diabetes can cause (Clair et al., 2019).
Preventing Complications: Regular chiropractic care can help prevent musculoskeletal complications, such as foot deformities or spinal misalignments, which can exacerbate neuropathy pain (El Paso Back Clinic, 2025).
By tackling these overlapping issues, Dr. Jimenez helps patients break the cycle of pain and dysfunction, paving the way for a healthier, more active life.
Zhang, Y., et al. (2022). Manual therapy for diabetic peripheral neuropathy: A systematic review. Journal of Pain Research, 15, 123–134. https://pubmed.ncbi.nlm.nih.gov/35428527/
Clair, C., et al. (2019). The effect of lifestyle interventions on diabetic neuropathy. Journal of Diabetes Research, 2019, 1–10. https://pubmed.ncbi.nlm.nih.gov/32215272/
Jimenez, A. (2025). Chiropractic care for musculoskeletal inflammation. Retrieved from https://elpasobackclinic.com/
El Paso Back Clinic. (2025). Spinal Injury Rehabilitation Tools for Enhanced Care. Retrieved from https://elpasobackclinic.com/
Practical Tips for Daily Management
To wrap up, here are some actionable tips from Dr. Jimenez’s playbook to manage diabetic neuropathy and keep your musculoskeletal system happy:
Schedule Regular Check-Ups: Visit a chiropractor, such as Dr. Jimenez, regularly to monitor your nerve and musculoskeletal health. It’s like taking your car for a tune-up to avoid breakdowns.
Stay Hydrated: Proper hydration supports nerve function and reduces inflammation. Aim for 8–10 glasses of water daily—think of it as giving your nerves a refreshing bath.
Use Supportive Devices: Orthotic inserts or braces can reduce pressure on nerves and joints, especially in the feet. It’s like giving your feet a comfy pillow to rest on.
Practice Mindful Movement: Incorporate gentle stretching or tai chi to improve flexibility and reduce stress. It’s like giving your body a daily dose of Zen.
Track Symptoms: Keep a journal of your neuropathy symptoms to share with your healthcare provider. This helps tailor treatments, like having a roadmap for your recovery journey.
By combining these tips with chiropractic care, you can effectively manage your neuropathy pain and lead a more comfortable, active life.
El Paso Back Clinic. (2025). Chiropractic care for musculoskeletal inflammation. Retrieved from https://elpasobackclinic.com/
Conclusion
Diabetic neuropathy can be a challenging condition, but with the right approach, relief is within reach. Chiropractic care, led by experts like Dr. Alexander Jimenez in El Paso, provides a non-surgical, holistic approach to managing nerve pain and enhancing musculoskeletal health. By addressing inflammation, improving circulation, and supporting overall wellness, Dr. Jimenez’s integrative methods help patients break the cycle of pain and dysfunction. His expertise in personal injury cases ensures that victims of accidents receive both top-notch medical care and the necessary legal documentation. Whether you’re experiencing tingling feet, burning pain, or mobility issues, chiropractic care, combined with lifestyle changes, can make a significant difference.
Disclaimer: This blog post is for informational purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider, such as Dr. Alexander Jimenez, DC, APRN, FNP-BC, for personalized care. For more information or to schedule an appointment, visit www.dralexjimenez.com or contact Injury Medical & Chiropractic Clinic at (915) 850-0900.
Holistic Wellness at El Paso Back Clinic: Premier Chiropractic Care
Welcome to El Paso Back Clinic, your trusted destination for injury rehabilitation and functional medicine in El Paso, TX. Led by Dr. Alex Jimenez, D.C., APRN, FNP-BC, our clinic specializes in treating sciatica, neck and back pain, whiplash, headaches, joint injuries, sports injuries, and degenerative arthritis. Our team of chiropractors, nurse practitioners, nutritionists, and acupuncturists uses advanced therapies to restore mobility, flexibility, and overall health. We focus on holistic sciatic nerve care, addressing root causes through chiropractic care, nutrition, and integrative medicine to help you achieve optimal wellness.
Comprehensive Chiropractic Care for Musculoskeletal Health
At El Paso Back Clinic, we provide a holistic approach to managing musculoskeletal issues, including sciatica, back pain, and joint injuries. Our treatments focus on restoring biomechanical function and promoting natural healing, helping patients regain their quality of life.
Chiropractic Techniques for Joint and Biomechanical Restoration
Chiropractic care is central to our approach, using gentle spinal adjustments to correct misalignments that cause nerve compression, such as sciatica. These adjustments relieve pressure on the sciatic nerve, improve mobility, and reduce pain (Dr. Leitman, 2023). By restoring proper alignment, we help the body heal naturally, whether the issue stems from a car accident, sports injury, or chronic condition.
Managing Musculoskeletal Inflammation
Inflammation often contributes to sciatica and other musculoskeletal pain. Our clinic utilizes functional medicine to address inflammation through dietary modifications, such as incorporating anti-inflammatory foods like omega-3 fatty acids, and targeted supplements like vitamin B12 (Therapy Organics, 2023). This approach reduces nerve irritation and supports long-term health.
Trigger Point and Massage Therapy
Massage therapy, including trigger point techniques, enhances circulation and relaxes tense muscles, which is crucial for sciatica relief. Improved blood flow delivers nutrients to the sciatic nerve, aiding recovery (Zama Massage, 2018). Our therapists tailor sessions to address specific injuries, from whiplash to sports-related strains.
Recovery and Rehabilitation After Motor Vehicle Accidents
Motor vehicle accidents (MVAs) can cause a range of injuries, from whiplash to gastrointestinal issues, impacting overall health. At El Paso Back Clinic, we offer comprehensive recovery plans tailored to each patient’s needs.
Whiplash and Spinal Injury Recovery
Whiplash-associated disorders (WAD) are common after MVAs, causing neck pain and stiffness. Our chiropractic care and durable medical equipment, such as cervical collars, support recovery by stabilizing the spine and reducing strain (Jimenez, 2023a). We also incorporate regenerative medicine, like platelet-rich plasma (PRP), to promote tissue repair (Family Integrative Medicine, 2023).
Gastrointestinal Injuries Post-Accident
MVAs can lead to gastrointestinal issues due to trauma or stress. Our integrative approach includes nutritional guidance to support gut health, emphasizing foods that reduce inflammation and promote healing (Asuta Health, 2023). This holistic care helps patients recover fully from internal injuries.
Nutrition for Injury Recovery
A tailored diet is vital for healing after an MVA. We recommend nutrient-dense foods and supplements to support tissue repair and reduce inflammation, aiding recovery from musculoskeletal and spinal injuries (Therapy Organics, 2023). Our nutritionists work with patients to create personalized plans.
Sciatica, characterized by pain radiating from the lower back through the buttocks and legs, is often caused by compression of the sciatic nerve. At El Paso Back Clinic, we address sciatica and other injuries with a focus on prevention and long-term wellness.
Sciatica Symptoms and Causes
Symptoms: Pain ranging from mild to severe, numbness, tingling, or muscle weakness in the leg or foot. Pain may worsen with activities such as sitting, coughing, or sneezing (WebMD, 2023a).
Causes: Herniated discs, bone spurs, or spinal misalignments (subluxations) due to poor posture, trauma, or pregnancy. Rarely, tumors or diabetes may contribute (Wilmington Chiropractic, 2023).
Risk Factors: Age-related spinal changes, obesity, sedentary lifestyles, occupations involving heavy lifting or prolonged driving, and diabetes increase the risk of sciatica.
Bicycle and 18-Wheeler Accident Risks
Bicycle collisions and 18-wheeler accidents pose significant risks for musculoskeletal injuries. Wet roads or heavy vehicles can exacerbate these risks, leading to spinal trauma or sciatica (National Center for Biotechnology Information, 2016). Our clinic uses chiropractic care and integrative medicine to address these injuries, promoting recovery and preventing recurrence.
Dr. Alex Jimenez’s Expertise in Diagnosis and Treatment
Dr. Alex Jimenez brings a unique dual perspective as a chiropractor and nurse practitioner, specializing in work, sports, personal, and motor vehicle injuries. His expertise ensures precise diagnoses and effective treatment plans.
Diagnostic Approach
Dr. Jimenez conducts thorough medical exams, using advanced imaging like X-rays and MRIs to identify issues such as herniated discs or nerve compression. Functional health assessments further reveal lifestyle factors that contribute to sciatica or other injuries (Jimenez, 2023b). This comprehensive approach ensures targeted treatments.
Medical and Legal Support
For personal injury cases, Dr. Jimenez provides detailed medical reports that support insurance claims or legal proceedings, easing the burden on patients. His dual qualifications allow him to seamlessly integrate medical care with legal documentation, particularly for MVA-related injuries (Jimenez, 2023c).
Preventing sciatica and other injuries requires proactive measures. Our clinic emphasizes sustainable strategies to maintain spinal health and overall wellness.
Prevention Strategies
Core Strengthening: Exercises targeting the abdomen and lower back support proper posture and spinal alignment (Thrive Cedar Falls, 2023).
Proper Posture: Use ergonomic chairs with lumbar support and maintain a level position with your knees and hips when sitting. A rolled towel can support the spine’s natural curve.
Body Mechanics: Lift with your legs, keep your back straight, and avoid twisting while lifting heavy objects.
An Active Lifestyle: Regular physical activity, such as walking or yoga, reduces the risk of sciatica compared to a sedentary lifestyle.
When to Seek Care
Seek immediate medical attention if you experience:
Severe pain with numbness or weakness in the leg.
Loss of bowel or bladder control.
Pain following a significant injury, such as an MVA.
Mild sciatica may resolve with self-care, but persistent or worsening pain requires professional intervention.
Our clinic combines advanced technology, proven therapies, and a patient-centered approach to deliver exceptional care. Dr. Jimenez’s expertise in chiropractic and integrative medicine ensures comprehensive treatment for sciatica, sports injuries, and MVA-related conditions. We prioritize natural healing and long-term wellness, helping patients return to their active lives.
Discover effective treatments for peripheral neuropathy with chiropractic care to manage symptoms and enhance mobility.
Chiropractic Care for Peripheral Neuropathy: A Comprehensive Guide to Reducing Nerve Pain
Peripheral neuropathy is like that one friend who shows up uninvited and overstays their welcome, causing all sorts of chaos. It’s a condition where the peripheral nerves—the ones that carry messages between your brain, spinal cord, and the rest of your body—decide to throw a tantrum, leading to symptoms like tingling, numbness, or burning pain. If you’ve ever felt like your hands or feet are throwing a pins-and-needles party without your permission, you might be dealing with peripheral neuropathy. But don’t worry—there’s hope! Chiropractic care, particularly through the expertise of practitioners like Dr. Alexander Jimenez, DC, APRN, FNP-BC, in El Paso, Texas, can help manage this nerve-racking condition (pun intended). In this blog post, we’ll dive into the clinical rationale for why chiropractic care can reduce nerve pain associated with peripheral neuropathy, explore the musculoskeletal system’s role, and highlight how Dr. Jimenez’s unique approach makes him a go-to for personal injury cases in El Paso. Let’s get started!
What Is Peripheral Neuropathy? The Nerve of It All!
Imagine your body as a massive communication network, with your brain and spinal cord as the control center and your peripheral nerves as the Wi-Fi signals carrying messages to your limbs, organs, and muscles. Peripheral neuropathy happens when these signals get scrambled, damaged, or completely cut off. It’s like trying to stream your favorite show with a spotty internet connection—frustrating and disruptive.
Peripheral neuropathy refers to damage to the peripheral nervous system, which sends signals between the central nervous system (brain and spinal cord) and the rest of the body. This damage can cause symptoms like numbness, tingling, burning sensations, muscle weakness, or even loss of balance. It’s not just one condition but a group of disorders caused by various factors, including diabetes, chemotherapy, infections, autoimmune diseases, or physical trauma like motor vehicle accidents (MVAs) (National Institute of Neurological Disorders and Stroke, n.d.).
The prevalence of peripheral neuropathy is no small matter. It affects millions of people worldwide, with diabetic peripheral neuropathy being one of the most common forms, impacting up to 50% of people with diabetes (Hicks & Selvin, 2019). Chemotherapy-induced peripheral neuropathy (CIPN) is another major player, affecting 19-85% of cancer patients undergoing treatment (Seretny et al., 2014). These numbers show just how widespread this condition is, and for those dealing with it, the impact on daily life can be profound.
References
Hicks, C. W., & Selvin, E. (2019). Epidemiology of peripheral neuropathy and lower extremity disease in diabetes. Current Diabetes Reports, 19(10), 86. https://doi.org/10.1007/s11892-019-1212-8
Seretny, M., et al. (2014). Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain, 155(12), 2461-2470. https://doi.org/10.1016/j.pain.2014.09.020
The Musculoskeletal System’s Role in Peripheral Neuropathy
Your musculoskeletal system—your bones, muscles, ligaments, tendons, and connective tissues—is like the scaffolding that keeps your body upright and moving. But when peripheral neuropathy enters the scene, it’s like someone’s shaking that scaffolding, causing all sorts of problems. The peripheral nerves are responsible for sending sensory and motor signals to your muscles and joints. When these nerves are damaged, the musculoskeletal system can take a hit, leading to symptoms that mess with your daily routine.
How Peripheral Neuropathy Affects the Musculoskeletal System
Peripheral neuropathy can disrupt the communication between your nerves and muscles, leading to:
Muscle Weakness: Damaged nerves may fail to send proper signals to muscles, causing weakness or difficulty moving. For example, you might struggle to grip a coffee mug or climb stairs without feeling like you’re auditioning for a slow-motion scene.
Loss of Coordination: Nerves help with balance and proprioception (knowing where your body is in space). Neuropathy can make you feel like you’re walking on a tightrope after a few too many spins.
Muscle Cramps and Spasms: Irritated or damaged nerves can cause muscles to contract involuntarily, leading to painful cramps or twitches.
Joint Instability: Weak muscles can’t support joints properly, increasing the risk of falls or injuries, especially in the ankles or knees.
Pain and Discomfort: Neuropathic pain, often described as burning, stabbing, or electric shocks, can radiate to muscles and joints, causing significant discomfort (personalinjurydoctorgroup.com, 2020).
These issues can turn simple tasks—like walking to the mailbox or tying your shoes—into a Herculean effort. For instance, someone with peripheral neuropathy might find their morning jog feels more like trudging through molasses, or they might drop their phone because their fingers have lost coordination.
Impact on Daily Routine
The musculoskeletal fallout from peripheral neuropathy can significantly disrupt daily life. Imagine trying to cook dinner when your hands feel like they’re wearing oven mitts, or attempting to drive when your feet can’t tell the difference between the gas and brake pedals. These symptoms can lead to:
Reduced Mobility: Difficulty walking or standing for long periods, limiting activities like shopping or socializing.
Decreased Independence: Tasks like dressing or bathing may require assistance, which can be a blow to self-esteem.
Increased Risk of Falls: Loss of sensation or balance can make falls more likely, especially for older adults.
Chronic Pain: Persistent nerve pain can sap energy, disrupt sleep, and even lead to mood changes like anxiety or depression.
Peripheral Neuropathy: A Successful Recovery Story- Video
Why Chiropractic Care? The Clinical Rationale
Now, let’s talk about the superhero of this story: chiropractic care. It’s not just about cracking backs and making you feel like a human pretzel—it’s a science-backed approach to improving nerve function and reducing pain. Chiropractic care focuses on the spine and musculoskeletal system to remove nerve interference, which is particularly relevant for peripheral neuropathy.
The Science Behind Chiropractic Care for Nerve Pain
The spine is like the central highway of your nervous system. If there’s a traffic jam—say, a misaligned vertebra or a compressed nerve—it can disrupt the signals traveling to and from your peripheral nerves. Chiropractic adjustments aim to clear these jams by realigning the spine and reducing pressure on nerves. Here’s why this matters for peripheral neuropathy:
Reducing Nerve Compression: Misalignments (subluxations) in the spine can compress nerve roots, exacerbating neuropathic symptoms like tingling or numbness. Adjustments restore alignment, relieving pressure on these nerves (elpasobackclinic.com, 2023).
Improving Blood Flow: Proper spinal alignment enhances blood circulation, which is crucial for nerve health. Damaged nerves need oxygen and nutrients to heal, and chiropractic care can help ensure they get it.
Modulating Pain Signals: Chiropractic adjustments can influence the central nervous system, reducing the perception of pain. Think of it like turning down the volume on a screaming nerve (Woolf & Salter, 2000).
Enhancing Autonomic Function: The autonomic nervous system, which controls involuntary functions like heart rate and digestion, can be affected by neuropathy. Chiropractic care may help regulate these functions by improving spinal health (Vagal, 2020).
Research supports these benefits. A study on spinal canal compression suggests that nerve root insults, whether chemical (from inflammation) or mechanical (from compression), can contribute to polyneuropathy-like symptoms. Chiropractic care addresses these insults by correcting spinal misalignments and reducing inflammation (Kulikov et al., 2016). Another study found that nonpharmacologic interventions, including manual therapies like chiropractic care, can reduce symptoms of chemotherapy-induced peripheral neuropathy (CIPN) by improving nerve function and reducing pain (Oh et al., 2023).
Dr. Alexander Jimenez’s Approach
Enter Dr. Alexander Jimenez, El Paso’s nerve-whisperer. With over 25 years of experience as a chiropractor and board-certified Family Nurse Practitioner (FNP-BC), Dr. Jimenez brings a unique, dual-scope approach to treating peripheral neuropathy. His practice at El Paso’s Premier Wellness and Injury Care Clinic combines chiropractic expertise with advanced medical diagnostics, making him a standout in managing nerve pain (Jimenez, 2025a).
Dr. Jimenez uses a holistic, evidence-based approach inspired by functional medicine. He doesn’t just slap a Band-Aid on symptoms—he digs deep to find the root cause. For example, suppose your neuropathy stems from a car accident. In that case, he might identify a spinal misalignment pinching a nerve while also checking for inflammation or metabolic imbalances that could slow healing (Jimenez, 2023b). His methods include:
Advanced Imaging: Using X-rays, MRIs, or CT scans to pinpoint issues like herniated discs or nerve compression (Jimenez, 2023c).
Diagnostic Evaluations: Neurological tests and motion studies to assess nerve function and biomechanical dysfunction.
Dual-Scope Procedures: Combining chiropractic adjustments with medical interventions like nutritional counseling or physical therapy to address both musculoskeletal and systemic factors.
Manual Therapies: Techniques like spinal decompression, joint mobilization, and myofascial release to relieve nerve pressure and improve mobility.
Kulikov, A. V., et al. (2016). Could spinal canal compression be a cause of polyneuropathy? Frontiers in Surgery, 3, 14. https://doi.org/10.3389/fsurg.2016.00014
Oh, P. J., et al. (2023). Prevention and treatment of chemotherapy-induced peripheral neuropathy (CIPN) with non-pharmacological interventions. Frontiers in Pain Research, 4, 1002967. https://doi.org/10.3389/fpain.2023.1002967
Vagal, V. (2020). Editorial: Understanding the role of the autonomic nervous system in health and disease. Frontiers in Neuroscience, 14, 615. https://doi.org/10.3389/fnins.2020.00615
Peripheral Neuropathy and Personal Injury Cases in El Paso
El Paso, Texas, is a bustling city with heavy traffic, which unfortunately means motor vehicle accidents (MVAs) are all too common. These accidents can cause nerve injuries, including peripheral neuropathy, especially when whiplash or spinal trauma is involved. If you’ve ever been rear-ended and felt like your nerves were playing a game of telephone with the wrong number, you know what I mean. This is where chiropractic care, and specifically Dr. Alexander Jimenez, shines.
The Link Between MVAs and Peripheral Neuropathy
MVAs can cause nerve damage through:
Mechanical Insults: The force of a collision can compress or stretch nerves, leading to symptoms like numbness or tingling. For example, whiplash can pinch nerves in the cervical spine, radiating pain to the arms or hands (Jimenez, 2025b).
Chemical Insults: Inflammation from soft tissue injuries can irritate nerves, contributing to neuropathic pain (Woolf & Thompson, 1991).
Spinal Canal Compression: Trauma can narrow the spinal canal, pressing on nerve roots and mimicking polyneuropathy symptoms (Kulikov et al., 2016).
These injuries don’t just hurt—they can disrupt your life, making it hard to work, drive, or even enjoy a Netflix binge without pain. In personal injury cases, proving the link between the accident and your symptoms is crucial for fair compensation, and that’s where Dr. Jimenez’s expertise comes in.
Dr. Jimenez: The Legal-Medical Liaison
Dr. Jimenez isn’t just a chiropractor—he’s a board-certified nurse practitioner with a knack for bridging medical care and legal documentation. His dual licensure allows him to:
Diagnose with Precision: Using advanced imaging (like MRIs) and neurological tests, he identifies the exact cause of nerve pain, whether it’s a herniated disc or a pinched nerve (Jimenez, 2023c).
Document for Legal Cases: He provides detailed reports that connect your injuries to the accident, strengthening your insurance or legal claims. Think of him as a translator who speaks both “doctor” and “lawyer” fluently (Jimenez, 2025a).
Deliver Holistic Care: His treatments combine spinal adjustments, physical therapy, and functional medicine to address both symptoms and underlying causes, helping you recover faster.
For example, if you’re dealing with post-accident neuropathy, Dr. Jimenez might use an MRI to spot a herniated disc, then apply spinal decompression to relieve nerve pressure. He’ll also check for metabolic issues (like vitamin deficiencies) that could worsen neuropathy, ensuring a comprehensive recovery plan (Jimenez, 2025b). His patients rave about his ability to get them back on their feet, as seen in testimonials on his social media (Jimenez, 2023f).
Kulikov, A. V., et al. (2016). Could spinal canal compression be a cause of polyneuropathy? Frontiers in Surgery, 3, 14. https://doi.org/10.3389/fsurg.2016.00014
Woolf, C. J., & Thompson, S. W. (1991). The induction and maintenance of central sensitization is dependent on N-methyl-D-aspartic acid receptor activation; implications for the treatment of post-injury pain hypersensitivity states. Pain, 44(3), 293-299. https://doi.org/10.1016/0304-3959(91)90100-C
Addressing Overlapping Risk Profiles
Peripheral neuropathy often comes with a side of extra baggage—overlapping risk factors that make symptoms worse. These include diabetes, chemotherapy, poor nutrition, or even stress from an injury. Chiropractic care, especially Dr. Jimenez’s integrative approach, can help manage these risks.
Common Risk Factors for Peripheral Neuropathy
Diabetic Peripheral Neuropathy: High blood sugar damages nerves over time, leading to numbness or pain, especially in the feet. Up to 50% of diabetic patients develop neuropathy (Hicks & Selvin, 2019).
Chemotherapy-Induced Peripheral Neuropathy (CIPN): Cancer treatments like platinum-based drugs can damage nerves, causing tingling or burning sensations (Seretny et al., 2014).
Trauma from MVAs: Physical injuries can compress or inflame nerves, contributing to neuropathic symptoms (Jimenez, 2025b).
Nutritional Deficiencies: Lack of B vitamins or other nutrients can impair nerve health, worsening symptoms (Oh et al., 2023).
How Chiropractic Care Helps
Dr. Jimenez’s approach tackles these risk factors head-on:
Diabetic Neuropathy: He combines spinal adjustments with nutritional counseling to stabilize blood sugar and support nerve repair. For example, he might recommend a diet rich in B vitamins to nourish nerves (Jimenez, 2025a).
CIPN: Chiropractic adjustments and therapies like acupuncture can reduce pain and improve nerve function, complementing nonpharmacologic interventions (Oh et al., 2023).
Post-Trauma Neuropathy: By addressing spinal misalignments and inflammation, Dr. Jimenez reduces nerve irritation from MVAs, helping patients regain mobility (Jimenez, 2025b).
Autonomic Nervous System Support: Chiropractic care can regulate the autonomic nervous system, which is often disrupted in neuropathy, improving symptoms like dizziness or digestive issues (Vagal, 2020).
His functional medicine approach also includes tools like the Neural Zoomer Plus, a blood test that analyzes neurological autoantibodies to pinpoint the causes of nerve damage (Jimenez, 2019). This allows for tailored treatments that address both symptoms and underlying risk factors.
References
Hicks, C. W., & Selvin, E. (2019). Epidemiology of peripheral neuropathy and lower extremity disease in diabetes. Current Diabetes Reports, 19(10), 86. https://doi.org/10.1007/s11892-019-1212-8
Oh, P. J., et al. (2023). Prevention and treatment of chemotherapy-induced peripheral neuropathy (CIPN) with non-pharmacological interventions. Frontiers in Pain Research, 4, 1002967. https://doi.org/10.3389/fpain.2023.1002967
Seretny, M., et al. (2014). Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain, 155(12), 2461-2470. https://doi.org/10.1016/j.pain.2014.09.020
Vagal, V. (2020). Editorial: Understanding the role of the autonomic nervous system in health and disease. Frontiers in Neuroscience, 14, 615. https://doi.org/10.3389/fnins.2020.00615
The Chiropractic Process: What to Expect
So, what’s it like to visit a chiropractor like Dr. Jimenez for peripheral neuropathy? It’s not like walking into a magic show where someone waves a wand and poof—your pain’s gone. It’s a structured, evidence-based process that’s more like a well-choreographed dance between science and care.
Initial Consultation
Your first visit is like a detective mission. Dr. Jimenez will:
Take a detailed health history to understand your symptoms, lifestyle, and any trauma (like that fender-bender you thought was no big deal).
Perform a physical exam to assess nerve function, reflexes, and muscle strength.
Order advanced imaging (X-rays, MRIs) or tests like the Neural Zoomer Plus to get a clear picture of what’s going on (Jimenez, 2019).
Treatment Plan
Once the culprit is identified, Dr. Jimenez crafts a personalized plan, which might include:
Spinal Adjustments: Gentle manipulations to realign the spine and relieve nerve pressure.
Manual Therapies: Techniques like myofascial release or trigger point therapy to relax muscles and improve circulation.
Rehabilitation Exercises: Stretches and strength training to support muscles and joints affected by neuropathy.
Functional Medicine: Nutritional advice or supplements to address deficiencies that worsen nerve damage.
Legal Documentation: For personal injury cases, detailed reports linking your symptoms to the accident, ensuring you have the evidence needed for claims (Jimenez, 2025a).
Ongoing Care
Recovery isn’t a one-and-done deal. Dr. Jimenez monitors progress with regular check-ins, adjusting the plan as needed. You might start with weekly adjustments, then taper off as symptoms improve. It’s like training for a marathon—steady progress wins the race.
Benefits of Chiropractic Care for Peripheral Neuropathy
Chiropractic care isn’t just about feeling better—it’s about getting your life back. Here are some key benefits for neuropathy patients:
Pain Reduction: Adjustments and therapies can lower pain levels, making daily tasks more manageable (Oh et al., 2023).
Improved Mobility: By addressing musculoskeletal issues, chiropractic care helps you move more freely, whether it’s walking or picking up your grandkids.
Non-Invasive Approach: Unlike medications or surgery, chiropractic care is gentle and low-risk, avoiding side effects like those seen with intravenous lidocaine (Schwenk et al., 2023).
Holistic Healing: Dr. Jimenez’s integrative approach tackles both symptoms and causes, from spinal misalignments to nutritional deficiencies.
Legal Support: For MVA-related neuropathy, Dr. Jimenez’s documentation ensures your injuries are properly represented in legal claims, helping you secure fair compensation (Jimenez, 2025a).
Oh, P. J., et al. (2023). Prevention and treatment of chemotherapy-induced peripheral neuropathy (CIPN) with non-pharmacological interventions. Frontiers in Pain Research, 4, 1002967. https://doi.org/10.3389/fpain.2023.1002967
Schwenk, E. S., et al. (2023). Intravenous lidocaine for treatment of chronic pain: A retrospective cohort study. Pain Medicine, 24(6), 664-670. https://doi.org/10.1093/pm/pnac174
Real-Life Impact: Patient Stories
Let’s take a moment to hear from patients who’ve walked this path. One patient, after a car accident, described feeling like their feet were “on fire” from neuropathy. After working with Dr. Jimenez, they reported less pain and better balance, allowing them to return to their job as a delivery driver (Jimenez, 2023f). Another patient with CIPN said chiropractic care, combined with nutritional changes, helped them reduce tingling enough to enjoy gardening again. These stories highlight how Dr. Jimenez’s care can transform lives, one adjustment at a time.
In El Paso, Dr. Jimenez is a household name for personal injury and neuropathy care. His clinic, Injury Medical & Chiropractic Clinic, is a hub for holistic healing, equipped with advanced tools and a compassionate team. Voted a top chiropractor and wellness provider, Dr. Jimenez’s dual expertise as a chiropractor and nurse practitioner sets him apart (Jimenez, 2025a). His ability to integrate medical diagnostics with chiropractic care ensures patients get the best of both worlds—effective treatment and solid legal support for personal injury cases.
Peripheral neuropathy can be a challenging condition, but chiropractic care offers a promising, non-invasive solution to reduce nerve pain and improve quality of life. By addressing spinal misalignments, improving blood flow, and tackling underlying risk factors, chiropractors like Dr. Alexander Jimenez in El Paso, Texas, help patients regain mobility and independence. His dual-scope approach, combining advanced imaging, diagnostic evaluations, and holistic therapies, makes him a trusted ally for those dealing with neuropathy, especially from personal injuries like motor vehicle accidents. For El Paso residents, Dr. Jimenez’s expertise as a medical-legal liaison ensures that your recovery is supported both clinically and legally, paving the way for a pain-free, active life.
Disclaimer: This blog post is for informational purposes only and is not intended to replace professional medical advice. Always consult a qualified healthcare provider, such as Dr. Alexander Jimenez, DC, APRN, FNP-BC, for personalized diagnosis and treatment. The information provided is based on current research and clinical insights, but should not be used as a substitute for a one-on-one consultation with a licensed professional. For more information or to discuss your specific condition, contact Dr. Jimenez at 915-850-0900 or visit dralexjimenez.com.
Nerve Injuries After Motor Vehicle Accidents: Recovery with El Paso Back Clinic’s Integrative Care
Motor vehicle accidents (MVAs) can lead to a variety of nerve injuries, ranging from mild discomfort to severe, life-altering conditions that affect sensory, motor, and autonomic functions. These injuries can disrupt your ability to feel, move, and regulate essential bodily functions, such as heart rate and digestion. At El Paso Back Clinic, led by Dr. Alex Jimenez, DC, APRN, FNP-BC, we specialize in helping patients recover from MVA-related injuries using a holistic, integrative approach that combines chiropractic care, functional medicine, and advanced diagnostics. Our evidence-based protocols, as featured on elpasobackclinic.com, focus on restoring health naturally for patients of all ages.
Understanding Nerve Injuries from Motor Vehicle Accidents
Nerve injuries from MVAs vary in severity and impact. Nerve compression occurs when nerves are pinched by swollen tissues, herniated discs, or misaligned bones, causing pain, numbness, or weakness (Alexander Orthopaedics, n.d.). Stretch injuries occur when nerves are overstretched during sudden movements, such as whiplash, resulting in temporary or prolonged discomfort (Hopkins Medicine, 2022). The most severe are nerve tears, where nerve fibers are severed, often requiring surgical intervention (Grabband Durando, n.d.).
Commonly affected nerve groups include the brachial plexus, which controls the shoulder, arm, and hand, often damaged in side-impact collisions, resulting in weakness or paralysis (Mayo Clinic, 2023a). Spinal nerves can be compressed by whiplash or herniated discs, causing radiating pain or loss of sensation (Novus Spine Center, n.d.). Peripheral nerves, connecting the spinal cord to the body, may experience trauma, leading to tingling or burning sensations (Mayo Clinic, 2023b). These injuries often manifest as whiplash, herniated discs, or pinched nerves, which can misalign the spine and affect overall health (Wallace Wins, n.d.).
At El Paso Back Clinic, we focus on identifying and treating these injuries to restore function and improve quality of life through personalized, non-invasive care plans.
Nerve injuries from MVAs disrupt three critical functions: sensory, motor, and autonomic, each presenting unique challenges that require specialized care.
Sensory functions manage sensations like touch, temperature, and pain. Damage can cause numbness, tingling, or burning, making daily tasks challenging. For example, a brachial plexus injury may impair sensation in the arm, making it difficult to perform activities such as holding objects (Mayo Clinic, 2023a). Motor functions control movement, and injuries can lead to muscle weakness or paralysis. A severe nerve tear, such as a brachial plexus avulsion, can prevent arm or hand movement (Hopkins Medicine, n.d.). Autonomic functions regulate involuntary processes, such as heart rate and sweating. Diffuse axonal injuries from high-speed crashes can disrupt these functions, causing issues like irregular heartbeats (National Institute of Neurological Disorders and Stroke, n.d.). Additionally, nerve damage can contribute to conditions such as carpal tunnel syndrome, where the median nerve is compressed, resulting in hand numbness or weakness (Palermo Law Group, n.d.).
El Paso Back Clinic utilizes advanced diagnostics, including X-rays, MRIs, and electromyography (EMG), to accurately assess nerve damage and develop tailored treatment plans that address both the injury and underlying health factors (Jimenez, 2023c).
Dr. Alex Jimenez’s Expertise at El Paso Back Clinic
At El Paso Back Clinic, Dr. Alex Jimenez, DC, APRN, FNP-BC, brings over 25 years of experience as a chiropractor and nurse practitioner to treat MVA-related nerve injuries. His dual-diagnosis approach combines chiropractic assessments with medical evaluations to establish a clear clinical correlation between injuries and symptoms. For instance, he may identify a pinched nerve from spinal misalignment while also assessing inflammation or hormonal imbalances that could delay recovery (Jimenez, 2023b).
Using advanced imaging techniques like X-rays and MRIs, Dr. Jimenez detects hidden issues, such as herniated discs or ligament tears resulting from whiplash, ensuring precise treatment plans (Jimenez, 2023c). His expertise in legal documentation is a key asset, as evidenced by his ability to provide detailed reports for insurance claims and personal injury cases, as highlighted by patient testimonials on social media (Jimenez, 2023f). Dr. Jimenez collaborates with top surgeons, therapists, and specialists to deliver comprehensive care tailored to each patient’s needs.
Our integrative approach, combining chiropractic care, functional medicine, acupuncture, and nutrition counseling, addresses the root causes of injuries, promoting long-term health and recovery (Jimenez, 2023g; Jimenez, 2023h).
Holistic Recovery with Chiropractic and Functional Medicine
El Paso Back Clinic offers a holistic approach to MVA recovery, focusing on non-invasive treatments that target the root causes of nerve injuries. Chiropractic adjustments correct spinal misalignments that compress nerves, relieving pain and restoring mobility (Jimenez, 2023g). For example, realigning the cervical spine after whiplash can alleviate nerve pressure, thereby reducing symptoms such as neck pain or numbness (Wallace Wins, n.d.).
Functional medicine enhances this by addressing underlying health issues. Nutrition counseling can reduce inflammation through dietary changes, thereby accelerating recovery from injuries such as herniated discs (Jimenez, 2023). Acupuncture and rehabilitation therapies can improve pain relief and mobility, while nurse practitioner services monitor for complications such as autonomic dysfunction (Baltimore Peripheral Nerve Pain, n.d.). This integrative approach prevents chronic issues and promotes overall wellness.
Contact El Paso Back Clinic at 915-850-0900 or [email protected] to begin your recovery with personalized, evidence-based care.
Nerve injuries from motor vehicle accidents, such as brachial plexus damage, spinal nerve compression, or peripheral nerve trauma, can disrupt sensory, motor, and autonomic functions, leading to conditions like whiplash, herniated discs, or pinched nerves. These injuries often misalign the spine, which can impact overall health. At El Paso Back Clinic, Dr. Alex Jimenez and our team offer an integrative approach, combining chiropractic care, functional medicine, and advanced diagnostics to address the root causes of injuries, promoting long-term recovery and wellness. Visit elpasobackclinic.com or call 915-850-0900 to start your journey to a pain-free, vibrant life.
Nerve Damage from Motor Vehicle Accidents: A Comprehensive Guide to Recovery with Chiropractic Care, Nurse Practitioners, Acupuncture, and Integrative Medicine
Motor vehicle accidents (MVAs) can leave lasting physical and emotional scars, often resulting in complex injuries like nerve damage, musculoskeletal issues, and chronic pain. Among the most significant consequences are nerve injuries, including radiculopathy, peripheral nerve damage, and spinal cord injuries, which can cause debilitating symptoms such as pain, numbness, and weakness. These injuries, along with musculoskeletal and ligamentous damage, frequently lead to back and neck pain that disrupts daily life. Fortunately, integrative approaches combining chiropractic care, nurse practitioner expertise, acupuncture, and functional medicine offer holistic solutions to address these issues, promote healing, and restore overall health.
This blog post examines the types of nerve damage resulting from MVAs, their effects on the body, and how integrative treatments can aid in recovery
. We’ll also highlight the expertise of Dr. Alexander Jimenez, DC, APRN, FNP-BC, a leading chiropractor and nurse practitioner in El Paso, Texas, whose dual licensure and innovative approach make him uniquely qualified to treat MVA victims. Written at a high school reading level, this guide aims to empower readers with clear, actionable information to navigate recovery.
Understanding Nerve Damage from Motor Vehicle Accidents
What Is Nerve Damage?
Nerves are like the body’s electrical wiring, carrying signals between the brain, spinal cord, and other parts of the body. When these nerves become damaged, it can cause problems such as pain, numbness, or weakness. Motor vehicle accidents often cause nerve injuries because of the sudden, forceful impact on the body. These injuries can affect various parts of the nervous system, resulting in different symptoms depending on the type and severity of the damage (Mayo Clinic, 2023a).
Types of Nerve Damage from MVAs
Peripheral Nerve Injuries
Peripheral nerves are those outside the brain and spinal cord, like the nerves in your arms, legs, and hands. These are the most common nerve injuries from car accidents because they’re vulnerable to trauma. For example, a sudden jolt can stretch, compress, or sever these nerves, leading to symptoms like:
Tingling or numbness in the limbs
Burning or shooting pain
Weakness or difficulty moving (Hoffmann Personal Injury, n.d.)
Common peripheral nerve injuries include damage to the brachial plexus, a network of nerves controlling the arm, shoulder, and hand. A crash can stretch or tear these nerves, causing pain or loss of function (Mayo Clinic, 2023b).
Radiculopathy
Radiculopathy happens when a nerve root near the spine gets compressed or irritated, often due to a herniated disc or whiplash from an MVA. This can cause sharp, piercing pain that radiates from the spine to other areas, like the arms or legs. For example, sciatica is a type of radiculopathy where the sciatic nerve is compressed, causing pain that radiates from the lower back down to the leg (Sally Morin Law, n.d.).
Spinal Cord Injuries
Spinal cord injuries are the most severe, as they can lead to partial or complete paralysis. The spinal cord, protected by the spine, carries signals to and from the brain. A crash can fracture vertebrae or dislocate the spine, damaging the cord and causing loss of sensation or movement below the injury site (McGowan Hood, 2025).
Pinched Nerves
A pinched nerve occurs when surrounding tissues, like bones or muscles, press on a nerve. This is common in MVAs due to whiplash or spinal misalignments, leading to pain, tingling, or weakness in areas like the neck or lower back (BWGLaw, n.d.).
How MVAs Cause Nerve Damage
Car accidents create sudden, violent forces that can harm nerves in several ways:
Impact Trauma: A collision can crush or stretch nerves, especially in the arms, legs, or neck.
Whiplash: The rapid back-and-forth motion of the neck in a crash can pinch nerves or damage the cervical spine, leading to radiculopathy or peripheral nerve issues (Mayo Clinic, 2023a).
Fractures or Dislocations: Broken bones or misaligned vertebrae can press on or sever nerves, causing severe damage.
Soft Tissue Injuries: Swelling or inflammation from muscle or ligament damage can compress nerves, leading to pain or numbness (Marks & Harrison, n.d.).
Symptoms of Nerve Damage
Nerve damage symptoms vary depending on the injury’s location and severity. Common signs include:
Sharp, shooting, or burning pain
Numbness or tingling (like pins and needles)
Muscle weakness or paralysis
Sensitivity to touch
Loss of reflexes or coordination (Baltimore Peripheral Nerve Pain, n.d.)
If you experience these symptoms after an accident, consult a healthcare provider immediately. Early diagnosis and treatment can prevent long-term complications.
Musculoskeletal and Ligamentous Injuries from MVAs
What Are Musculoskeletal and Ligamentous Injuries?
Musculoskeletal injuries affect the muscles, bones, joints, and connective tissues like ligaments and tendons. Ligaments are tough bands that connect bones, while tendons attach muscles to bones. MVAs often cause these tissues to stretch, tear, or break due to the force of the crash.
Common Musculoskeletal and Ligamentous Injuries
Whiplash
Whiplash is a neck injury caused by the head jerking forward and back, straining muscles and ligaments in the neck. It’s one of the most common MVA injuries, leading to neck pain, stiffness, and sometimes nerve damage (Mayo Clinic, 2023a).
Sprains and Strains
Sprains involve stretched or torn ligaments, while strains affect muscles or tendons. These injuries often occur in the back, neck, or shoulders during a crash, causing pain and limited movement.
Fractures
Broken bones are common in high-impact crashes, especially in the arms, legs, or spine. Fractures can also press on nerves, worsening nerve damage (Eckell Sparks, 2024).
Herniated Discs
The spine’s discs act like cushions between vertebrae. A crash can cause these discs to bulge or rupture, pressing on nearby nerves and causing radiculopathy or sciatica (Jimenez, 2025a).
Impact on Back and Neck Pain
Musculoskeletal and ligamentous injuries often lead to chronic back and neck pain. For example:
Neck Pain: Whiplash or sprains can cause persistent soreness, stiffness, or radiating pain due to nerve irritation.
Back Pain: Herniated discs or strained muscles in the lower back can cause sharp or aching pain, especially when sitting or moving (El Paso Back Clinic, n.d.).
These injuries can limit mobility, disrupt sleep, and affect mental health, making comprehensive treatment essential.
Chiropractic care focuses on the spine and musculoskeletal system, utilizing hands-on techniques to enhance alignment, alleviate pain, and promote healing. Chiropractors are trained to treat injuries from MVAs, especially those affecting the spine and nerves (Mayo Clinic, 2024).
How Chiropractic Care Helps MVA Injuries
Spinal Adjustments
Chiropractors use precise movements to realign the spine, relieving pressure on nerves and reducing pain. A 2020 study found that spinal manipulative therapy significantly reduces pain and disability in patients with chronic low back pain (Rubinstein et al., 2020, as cited in Jimenez, 2025b).
Spinal Decompression
This non-surgical technique gently stretches the spine to relieve pressure on discs and nerves, helping to alleviate conditions such as herniated discs or sciatica (Jimenez, 2025b).
Soft Tissue Therapy
Chiropractors use massage or myofascial release to relax tight muscles and reduce inflammation, improving mobility and easing pain.
Nurse practitioners (NPs) are advanced practice nurses with extensive medical training, allowing them to diagnose and treat a wide range of conditions. In MVA care, NPs provide comprehensive assessments and coordinate treatment plans, often working alongside chiropractors (ChiroMed, 2023).
How NPs Help MVA Victims
Diagnostic Expertise
NPs perform thorough evaluations, ordering tests like MRIs or CT scans to identify nerve damage, fractures, or soft tissue injuries. Their medical training helps pinpoint the underlying causes of pain (Jimenez, 2025c).
Holistic Care
NPs address both physical and systemic issues, such as inflammation or metabolic imbalances, using evidence-based treatments, including medications and lifestyle changes.
Coordination of Care
NPs collaborate with chiropractors, acupuncturists, and other specialists to create personalized recovery plans, ensuring all aspects of health are addressed.
Why NPs Are Essential
NPs bridge the gap between medical and alternative therapies, offering a balanced approach that enhances recovery. Their ability to prescribe treatments and provide patient education empowers individuals to take charge of their healing (Jimenez, 2025c).
References
ChiroMed. (2023). Integrated medicine holistic healthcare in El Paso, TX. Retrieved from https://chiromed.com/
Jimenez, A. (2025c). Board certified nurse practitioner (FNP-BC) Dr. Alex Jimenez. Retrieved from https://dralexjimenez.com/
Acupuncture for MVA Recovery
What Is Acupuncture?
Acupuncture is a traditional Chinese medicine practice that involves inserting thin needles into specific points on the body to balance the flow of energy, or “qi.” It’s widely used to relieve pain and promote healing (ChiroMed, 2023).
How Acupuncture Helps MVA Injuries
Pain Relief
Acupuncture stimulates the release of endorphins, the body’s natural painkillers, thereby reducing discomfort associated with nerve damage or musculoskeletal injuries.
Reduced Inflammation
By improving blood flow, acupuncture helps reduce swelling around injured tissues, easing pressure on nerves.
Nerve Healing
Acupuncture may support nerve regeneration by enhancing circulation and reducing stress on the nervous system.
Stress and Anxiety Relief
MVAs can cause emotional trauma. Acupuncture promotes relaxation, helping patients manage stress and improve their sleep quality.
Benefits of Acupuncture
Non-Invasive: No surgery or drugs required.
Complementary: Works well with chiropractic care and medical treatments.
Customizable: Tailored to individual symptoms and needs (ChiroMed, 2023).
References
ChiroMed. (2023). Integrated medicine holistic healthcare in El Paso, TX. Retrieved from https://chiromed.com/
Integrative Medicine: A Holistic Approach
What Is Integrative Medicine?
Integrative medicine combines conventional medical treatments with complementary therapies, such as chiropractic care, acupuncture, and nutrition. It focuses on treating the whole person—body, mind, and spirit—to achieve optimal health (Jimenez, 2025d).
How Integrative Medicine Helps MVA Recovery
Functional Medicine
Functional medicine identifies the root causes of symptoms, such as inflammation or hormonal imbalances, using advanced diagnostics, including blood tests. Dr. Jimenez uses tools like the Neural Zoomer Plus to assess neurological health (Jimenez, 2019).
Nutrition and Wellness
Personalized diet plans help reduce inflammation, support tissue repair, and boost energy levels. NPs and nutritionists guide patients on anti-inflammatory foods and supplements.
Lifestyle Interventions
Stress management, exercise, and sleep optimization improve mental and physical resilience, aiding recovery.
Collaborative Care
Integrative medicine brings together chiropractors, NPs, acupuncturists, and other specialists to create comprehensive treatment plans.
Benefits of Integrative Medicine
Addresses Root Causes: Treats underlying issues, not just symptoms.
Promotes Long-Term Health: Focuses on prevention and wellness.
Patient-Centered: Tailored to individual needs and goals (Jimenez, 2025d).
References
Jimenez, A. (2019). Functional medicine – Neurological health. Retrieved from https://elpasobackclinic.com/
Jimenez, A. (2025d). Dr. Alex Jimenez chiropractor and injury recovery. Retrieved from https://dralexjimenez.com/
Dr. Alexander Jimenez: A Leader in MVA Care
Who Is Dr. Alex Jimenez?
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a board-certified chiropractor and family nurse practitioner based in El Paso, Texas. With over 25 years of experience, he leads Injury Medical & Chiropractic Clinic, specializing in MVA injuries. His dual licensure allows him to integrate chiropractic techniques with advanced medical diagnostics, offering a unique approach to healing (Jimenez, 2025e).
Clinical Justification for Treatment
Dr. Jimenez emphasizes the importance of enhanced imaging (e.g., MRI, CT scans) and dual-scope procedures (combining chiropractic and medical assessments) to accurately diagnose MVA injuries. These tools help identify nerve damage, herniated discs, or ligament tears that may not appear on standard X-rays. His diagnostic evaluations, including neurological tests and functional assessments, ensure precise treatment plans that address both symptoms and underlying causes (Jimenez, 2025f).
Unique Qualities for Personal Injury Cases
Dr. Jimenez’s dual expertise makes him exceptionally qualified to handle personal injury cases:
Medical and Chiropractic Knowledge: As a chiropractor, he restores spinal alignment and musculoskeletal function. As an NP, he manages systemic conditions and prescribes evidence-based treatments.
Legal Documentation: Dr. Jimenez provides detailed medical records and expert testimony, crucial for personal injury claims. His reports align with legal standards, ensuring accurate representation of injuries (Jimenez, 2025e).
Holistic Approach: He combines spinal adjustments, decompression, acupuncture, and functional medicine to promote comprehensive recovery, reducing the need for invasive procedures.
Community Impact
Dr. Jimenez is committed to expanding access to integrative care in El Paso through workshops, online resources, and outreach programs, such as the “Tell A Veteran” Project, which informs veterans about chiropractic treatment options (Jimenez, 2025g).
Motor vehicle accidents can cause devastating nerve damage, musculoskeletal injuries, and chronic pain, but recovery is possible with the right care. Chiropractic care, nurse practitioner expertise, acupuncture, and integrative medicine provide holistic solutions that address both symptoms and their underlying causes. Dr. Alexander Jimenez stands out as a leader in this field, combining advanced diagnostics, dual licensure, and a patient-centered approach to help MVA victims heal and thrive. By seeking comprehensive care and accurately documenting injuries, you can reclaim your health and quality of life.
For more information or to schedule an appointment with Dr. Jimenez, visit www.dralexjimenez.com or call (915) 850-0900.
Jimenez, A. (2025a). Comprehensive guide to ligamentous injuries and sciatica from motor vehicle accidents. Retrieved from https://ceb.elpasobackclinic.com/
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine