Spinal stenosis is the term used to describe a narrowing spine. Treatments vary because everybody’s case is different. Some individuals experience mild symptoms, while others experience severe symptoms. Can knowing treatment options help the patient and healthcare team customize and personalize a treatment plan to the individual’s condition?
Spinal Stenosis Treatments
Spaces within the spine can become narrower than they’re supposed to be, which can cause pressure on nerve roots and the spinal cord. Anywhere along the spine can be affected. The narrowing can cause pain, burning, and/or aching in the back and weakness in the legs and feet. Spinal stenosis has several primary treatments. When working through spinal stenosis treatments, a healthcare provider will assess symptoms and start treatment with first-line therapy, such as pain medication and/or physical therapy. These are often the first among individuals with the disease.
Medication
Chronic pain is one of the main symptoms. The first-line treatment often involves using pain-relieving medication/s. Commonly prescribed medications are nonsteroidal anti-inflammatories or NSAIDs. These medications reduce pain and inflammation. However, NSAIDs are not recommended for long-term use, and other medications may need to be used to relieve pain that includes: (Sudhir Diwan et al., 2019)
Tylenol – acetaminophen
Gabapentin
Pregabalin
Opioids for severe cases
Exercise
Exercise can reduce spinal stenosis symptoms by taking pressure off the nerves, which can reduce pain and improve mobility. (Andrée-Anne Marchand et al., 2021) Healthcare providers will recommend the most effective exercises for the individual. Examples include:
Another primary spinal stenosis treatment is physical therapy, which is often used alongside pain medications. Typically, individuals undergo six to eight weeks of physical therapy, with sessions two to three times a week. Utilizing physical therapy has been shown to (Sudhir Diwan et al., 2019)
Reduce pain
Increase mobility
Reduce pain medications.
Reduce mental health symptoms like anger, depression, and mood changes.
For severe cases, physical therapy following surgery can reduce recovery times.
Back Braces
Back braces can help reduce movement and pressure on the spine. This is helpful because even small spinal movements can lead to nerve irritation, pain, and worsening symptoms. Over time, the bracing can lead to a positive increase in mobility. (Carlo Ammendolia et al., 2019)
Injections
Epidural steroid injections may be recommended to relieve severe symptoms. Steroids act as anti-inflammatories to reduce pain and swelling caused by inflammation and irritation of the spinal nerves. They are considered nonsurgical medical procedures. According to research, injections can effectively manage pain for two weeks and up to six months, and some research has found that after a spinal injection, relief can last 24 months. (Sudhir Diwan et al., 2019)
Thickened Ligaments Decompression Procedure
Some individuals may be recommended to undergo a decompression procedure. This procedure involves using a thin needle tool inserted into the back. The thickened ligament tissue is removed to reduce the pressure on the spine and nerves. Research has found that the procedure can reduce symptoms and the need for more invasive surgery. (Nagy Mekhail et al., 2021)
Alternative Treatments
In addition to first-line treatments, individuals may be referred to alternative therapies for symptom management, including:
Acupuncture
This involves the insertion of thin-tipped needles into various acupoints to relieve symptoms.
Some research has found that acupuncture may be more effective at reducing symptoms than physical therapy alone. Both options are viable and can improve mobility and pain. (Hiroyuki Oka et al., 2018)
Chiropractic
This therapy reduces pressure on nerves, maintains spinal alignment, and helps to improve mobility.
Massage
Massage helps to increase circulation, relax the muscles, and reduce pain and stiffness.
New Treatment Options
As spinal stenosis research continues, new therapies are emerging to help relieve and manage symptoms in individuals who don’t respond to traditional medicine or cannot partake in conventional therapies for various reasons. However, some evidence presented is promising; medical insurers may consider them experimental and not offer coverage until their safety has been proven. Some new treatments include:
Acupotomy
Acupotomy is a form of acupuncture that uses thin needles with a small, flat, scalpel-type tip to relieve tension in painful areas. Research on its effects is still limited, but preliminary data shows it could be an effective complementary treatment. (Ji Hoon Han et al., 2021)
Stem Cell Therapy
Stem cells are the cells from which all other cells originate. They act as the raw material for the body to create specialized cells with specific functions. (National Institutes of Health. 2016)
Individuals with spinal stenosis can develop soft tissue damage.
Stem cell therapy uses stem cells to help repair injured or diseased tissues.
Stem cell therapy can help repair or improve the damaged areas and provide symptom relief.
Clinical studies for spinal stenosis report that it could be a viable treatment option for some.
However, more research is needed to confirm whether the therapy is effective enough to be widely used. (Hideki Sudo et al., 2023)
Dynamic Stabilization Devices
LimiFlex is a medical device undergoing research and analysis for its ability to restore mobility and stability in the spine. It is implanted into the back through a surgical procedure. According to research, individuals with spinal stenosis who receive the LimiFlex often experience a higher reduction in pain and symptoms than with other forms of treatment. (T Jansen et al., 2015)
Lumbar Interspinous Distraction Decompression
Lumbar interspinous distraction decompression is another surgical procedure for spinal stenosis. The surgery is performed with an incision above the spine and places a device between two vertebrae to create space. This reduces movement and pressure on the nerves. Preliminary results show positive short-term relief from symptoms; long-term data is not yet available as it is a relatively new spinal stenosis treatment option. (UK National Health Service, 2022)
Surgical Procedures
There are several surgical procedures are available for spinal stenosis. Some include: (NYU Langone Health. 2024) Surgery for spinal stenosis is often reserved for individuals with severe symptoms, like numbness in the arms or legs. When these symptoms develop, it indicates a more notable compression of the spinal nerves and the need for a more invasive treatment. (NYU Langone Health. 2024)
Laminectomy
A laminectomy removes part or all of the lamina, the vertebral bone covering the spinal canal.
The procedure is designed to reduce pressure on nerves and the spinal cord.
Laminotomy and Foraminotomy
Both surgeries are used if an individual’s spinal stenosis negatively affects an opening in the vertebral foramen.
Ligaments, cartilage, or other tissues that constrict the nerves are removed.
Both reduce pressure on the nerves traveling through the foramen.
Laminoplasty
A laminoplasty relieves pressure on the spinal cord by removing parts of the spinal canal’s lamina.
This surgical procedure involves removing herniated or bulging discs that are placing pressure on the spinal cord and nerves.
Spinal fusion
Spinal fusion involves joining two vertebrae using metal pieces like rods and screws.
The vertebrae are more stable because the rods and screws act as a brace.
Which Treatment Is The Right One?
Because all treatment plans differ, determining the most effective is best suited for a healthcare provider. Each approach will be personalized to the individual. To decide what therapy is best, healthcare providers will assess: (National Institute of Arthritis and Musculoskeletal and Skin Diseases. 2023)
The severity of symptoms.
The current level of overall health.
The level of damage that’s occurring in the spine.
The level of disability and how mobility and quality of life are affected.
Injury Medical Chiropractic and Functional Medicine Clinic will work with an individual’s primary healthcare provider and/or specialists to help determine the best treatment options and concerns regarding medications or other forms of treatment.
Unlocking Wellness
References
Diwan, S., Sayed, D., Deer, T. R., Salomons, A., & Liang, K. (2019). An Algorithmic Approach to Treating Lumbar Spinal Stenosis: An Evidenced-Based Approach. Pain medicine (Malden, Mass.), 20(Suppl 2), S23–S31. https://doi.org/10.1093/pm/pnz133
Marchand, A. A., Houle, M., O’Shaughnessy, J., Châtillon, C. É., Cantin, V., & Descarreaux, M. (2021). Effectiveness of an exercise-based prehabilitation program for patients awaiting surgery for lumbar spinal stenosis: a randomized clinical trial. Scientific reports, 11(1), 11080. https://doi.org/10.1038/s41598-021-90537-4
Ammendolia, C., Rampersaud, Y. R., Southerst, D., Ahmed, A., Schneider, M., Hawker, G., Bombardier, C., & Côté, P. (2019). Effect of a prototype lumbar spinal stenosis belt versus a lumbar support on walking capacity in lumbar spinal stenosis: a randomized controlled trial. The spine journal : official journal of the North American Spine Society, 19(3), 386–394. https://doi.org/10.1016/j.spinee.2018.07.012
Mekhail, N., Costandi, S., Nageeb, G., Ekladios, C., & Saied, O. (2021). The durability of minimally invasive lumbar decompression procedure in patients with symptomatic lumbar spinal stenosis: Long-term follow-up. Pain practice : the official journal of World Institute of Pain, 21(8), 826–835. https://doi.org/10.1111/papr.13020
Oka, H., Matsudaira, K., Takano, Y., Kasuya, D., Niiya, M., Tonosu, J., Fukushima, M., Oshima, Y., Fujii, T., Tanaka, S., & Inanami, H. (2018). A comparative study of three conservative treatments in patients with lumbar spinal stenosis: lumbar spinal stenosis with acupuncture and physical therapy study (LAP study). BMC complementary and alternative medicine, 18(1), 19. https://doi.org/10.1186/s12906-018-2087-y
Han, J. H., Lee, H. J., Woo, S. H., Park, Y. K., Choi, G. Y., Heo, E. S., Kim, J. S., Lee, J. H., Park, C. A., Lee, W. D., Yang, C. S., Kim, A. R., & Han, C. H. (2021). Effectiveness and safety of acupotomy on lumbar spinal stenosis: A pragmatic randomized, controlled, pilot clinical trial: A study protocol. Medicine, 100(51), e28175. https://doi.org/10.1097/MD.0000000000028175
Sudo, H., Miyakoshi, T., Watanabe, Y., Ito, Y. M., Kahata, K., Tha, K. K., Yokota, N., Kato, H., Terada, T., Iwasaki, N., Arato, T., Sato, N., & Isoe, T. (2023). Protocol for treating lumbar spinal canal stenosis with a combination of ultrapurified, allogenic bone marrow-derived mesenchymal stem cells and in situ-forming gel: a multicentre, prospective, double-blind randomised controlled trial. BMJ open, 13(2), e065476. https://doi.org/10.1136/bmjopen-2022-065476
National Institutes of Health. (2016). Stem cell basics. U.S. Department of Health and Human Services. Retrieved from https://stemcells.nih.gov/info/basics/stc-basics
Jansen, T., Bornemann, R., Otten, L., Sander, K., Wirtz, D., & Pflugmacher, R. (2015). Vergleich dorsaler Dekompression nicht stabilisiert und dynamisch stabilisiert mit LimiFlex™ [A Comparison of Dorsal Decompression and Dorsal Decompression Combined with the Dynamic Stabilisation Device LimiFlex™]. Zeitschrift fur Orthopadie und Unfallchirurgie, 153(4), 415–422. https://doi.org/10.1055/s-0035-1545990
UK National Health Service. (2022). Lumbar decompression surgery: How It’s performed. https://www.nhs.uk/conditions/lumbar-decompression-surgery/what-happens/
NYU Langone Health. (2024). Surgery for spinal stenosis. https://nyulangone.org/conditions/spinal-stenosis/treatments/surgery-for-spinal-stenosis
Columbia Neurosurgery. (2024). Cervical laminoplasty procedure. https://www.neurosurgery.columbia.edu/patient-care/treatments/cervical-laminoplasty
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Spinal stenosis: Diagnosis, treatment and steps to take. Retrieved from https://www.niams.nih.gov/health-topics/spinal-stenosis/diagnosis-treatment-and-steps-to-take
For individuals living with cyclical or chronic endometriosis symptoms, can incorporating support therapies help in disease management?
Support Therapies
Endometriosis is a disorder in which tissue similar to the uterine lining begins to grow outside the uterus where it does not belong. Endometriosis support therapies involve a comprehensive approach to treatment. It involves non-invasive treatments to help manage symptoms that can include:
A physical therapist uses various pressures, stretching, and/or trigger point release. This helps: (Sylvia Mechsner, 2022)
Release muscle tension
Lower cortisol – stress hormone
Improve circulation
Release endorphins – the body’s natural painkillers
Medications
Nonsteroidal anti-inflammatory drugs or NSAIDs and hormonal contraceptives – birth control are the first line of treatment. Advil and Motrin are over-the-counter NSAIDs. If those don’t manage pain effectively, a healthcare provider may recommend prescription NSAIDs. (Sylvia Mechsner, 2022) Hormonal suppression agents or estrogen modulators are a second line of treatment for endometriosis and can include: (Christian M. Becker et al., 2022)
Hormonal contraceptives suppress or regulate periods. They are effective for management, but not everyone can take them because of medical history, side effects, or fertility disorders and conditions. (Mert Ilhan et al., 2019) A healthcare provider can recommend alternative support therapies.
Transcutaneous Electrical Nerve Stimulation
A transcutaneous electrical nerve stimulation utilizes a battery-operated device that delivers low-voltage electrical stimulation to nerve fibers through electrodes placed on the skin.
Sessions are usually 15 to 30 minutes and work by disrupting pain signals. (Sylvia Mechsner, 2022)
Acupuncture
Acupuncture is a therapy in which a practitioner inserts thin needles into specific acupoints on the body to promote the flow of energy and alleviate pain. (Nora Giese et al., 2023)
Chiropractic
Chiropractic care focuses on spinal adjustments and alignment to enhance nervous system function, help alleviate pelvic discomfort and nerve pain – sciatica – and improve overall well-being. (Robert J. Trager et al., 2021)
Non-surgical decompression could be recommended to gently stretch the spine, relieve pressure, and flood the spine with added nutrients.
Movement Medicine: Chiropractic Care
References
Mansfield, C., Lenobel, D., McCracken, K., Hewitt, G., & Appiah, L. C. (2022). Impact of Pelvic Floor Physical Therapy on Function in Adolescents and Young Adults with Biopsy-Confirmed Endometriosis at a Tertiary Children’s Hospital: A Case Series. Journal of pediatric and adolescent gynecology, 35(6), 722–727. https://doi.org/10.1016/j.jpag.2022.07.004
Mechsner S. (2022). Endometriosis, an Ongoing Pain-Step-by-Step Treatment. Journal of clinical medicine, 11(2), 467. https://doi.org/10.3390/jcm11020467
Ilhan, M., Gürağaç Dereli, F. T., & Akkol, E. K. (2019). Novel Drug Targets with Traditional Herbal Medicines for Overcoming Endometriosis. Current drug delivery, 16(5), 386–399. https://doi.org/10.2174/1567201816666181227112421
Becker, C. M., Bokor, A., Heikinheimo, O., Horne, A., Jansen, F., Kiesel, L., King, K., Kvaskoff, M., Nap, A., Petersen, K., Saridogan, E., Tomassetti, C., van Hanegem, N., Vulliemoz, N., Vermeulen, N., & ESHRE Endometriosis Guideline Group (2022). ESHRE guideline: endometriosis. Human reproduction open, 2022(2), hoac009. https://doi.org/10.1093/hropen/hoac009
Endometriosis Foundation of America. (2015). Seeking a doctor: finding the right endometriosis specialist. https://www.endofound.org/preparing-to-see-a-doctor
Pereira, A., Herrero-Trujillano, M., Vaquero, G., Fuentes, L., Gonzalez, S., Mendiola, A., & Perez-Medina, T. (2022). Clinical Management of Chronic Pelvic Pain in Endometriosis Unresponsive to Conventional Therapy. Journal of personalized medicine, 12(1), 101. https://doi.org/10.3390/jpm12010101
Giese, N., Kwon, K. K., & Armour, M. (2023). Acupuncture for endometriosis: A systematic review and meta-analysis. Integrative medicine research, 12(4), 101003. https://doi.org/10.1016/j.imr.2023.101003
Trager, R.J., Prosak, S.E., Leonard, K.A. et al. (2021). Diagnosis and management of sciatic endometriosis at the greater sciatic foramen: a case report. SN Comprehensive Clinical Medicine, 3. https://doi.org/doi:10.1007/s42399-021-00941-0
For individuals having difficulty moving or functioning normally due to injury, surgery, or illness, can a chiropractic and physical therapy team help expedite recovery?
Friction Massage
Individuals may develop scar tissue or tissue adhesions that limit normal motion after injury or surgery. A pain management team may use various treatments and modalities and may incorporate friction massage as part of a rehabilitation treatment plan. Friction massage, also known as transverse friction or cross friction massage, is a technique used to help improve scar tissue and adhesion mobility to move better and decrease the negative effects. The therapist uses their fingers to massage the scar in a direction that is at right angles to the scar line. It is a specialized technique that breaks up tissue adhesions that are limiting normal movement in the skin and underlying tissues. (Haris Begovic, et al., 2016)
Scar Tissue and Adhesions
For individuals who require surgery due to an injury or an orthopedic condition, their doctor will cut into the skin, tendons, and muscle tissue during the operation. Once sutured and healing has begun, scar tissue forms. Healthy tissue is made up of collagen that is comprised of cells that are arranged in a regular pattern. Healthy collagen is strong and can resist forces when tissues are pulled and stretched. (Paula Chaves, et al., 2017)
During the healing process after an injury, the collagen cells are laid down in a haphazard pattern and form scar tissue. The random accumulation of cells becomes tight and does not react well to tension and stretching forces. (Qing Chun, et al., 2016) The body can form scar tissue after a soft tissue injury, like a muscle or tendon strain. (Qing Chun, et al., 2016)
If a muscle or tendon gets strained the body will generate new collagen during the healing. The new collagen is laid down in a random fashion, and scar tissue or tissue adhesions can form that can limit the normal range of motion. Healthy tissue stretches and glides as the body moves. Scar tissue is rigid. At the site of the scar tissue, there can be some movement, but it is tight, less pliable, and can be painful. If scar tissue or adhesions are limiting motion, cross-friction massage can improve tissue gliding and sliding. This process is referred to as remodeling.
Massage Objectives
The objectives and goals of friction massage to adhesions or scar tissue may include:
Stimulation of nerve fibers to decrease and relieve pain.
The entire area of scar tissue or adhesion should be treated.
If the scar tissue is in a muscle, it should be relaxed.
If the scar tissue is in a tendon sheath, that tendon should be slightly stretched during the procedure.
The therapist places two or three fingers over the scar or adhesion and moves their fingers perpendicular to the scar to smooth the collagen fibers down.
The fingers and underlying tissues move together.
The massage should feel deep and uncomfortable but not painful.
There may be some pain, but should remain within the individual’s tolerance.
If the massage is too painful, less pressure may be used.
After several minutes the therapist will assess the tissue mobility.
Specific stretches may be done to elongate the scar tissue or adhesions.
At-home exercises and stretches may be prescribed to maintain flexibility.
Contraindications
There are situations where friction massage should not be used and can include: (Paula Chaves, et al., 2017)
Around an active open wound.
If there is a bacterial infection.
Areas with decreased sensation.
If calcification is present in the muscle or tendon tissue.
The therapist will explain the procedure and inform of the goals and risks associated with it.
Adhesive capsulitis in the shoulder/frozen shoulder.
Joint contracture.
Ligament tears.
Scar tissue buildup after surgery or trauma.
Friction massage is a popular technique used in physical therapy, but some research suggests it is not any more effective than other rehabilitation techniques. One study found that static stretches and exercises were more effective than massage in improving tissue length and strength in uninjured soccer players. Other studies have supported this, but individuals may find that the massage helps improve injured tissues’ movement as well. (Mohammed Ali Fakhro, et al. 2020)
The main goal of any treatment in physical therapy is to help the individual regain movement and flexibility. Friction massage, combined with targeted stretches and exercises, can help individuals expedite recovery and get back to normal.
Chiropractic Care After Accidents and Injuries
References
Begovic, H., Zhou, G. Q., Schuster, S., & Zheng, Y. P. (2016). The neuromotor effects of transverse friction massage. Manual therapy, 26, 70–76. https://doi.org/10.1016/j.math.2016.07.007
Chaves, P., Simões, D., Paço, M., Pinho, F., Duarte, J. A., & Ribeiro, F. (2017). Cyriax’s deep friction massage application parameters: Evidence from a cross-sectional study with physiotherapists. Musculoskeletal science & practice, 32, 92–97. https://doi.org/10.1016/j.msksp.2017.09.005
Chun, Q., ZhiYong, W., Fei, S., & XiQiao, W. (2016). Dynamic biological changes in fibroblasts during hypertrophic scar formation and regression. International wound journal, 13(2), 257–262. https://doi.org/10.1111/iwj.12283
Fakhro, M. A., Chahine, H., Srour, H., & Hijazi, K. (2020). Effect of deep transverse friction massage vs stretching on football players’ performance. World journal of orthopedics, 11(1), 47–56. https://doi.org/10.5312/wjo.v11.i1.47
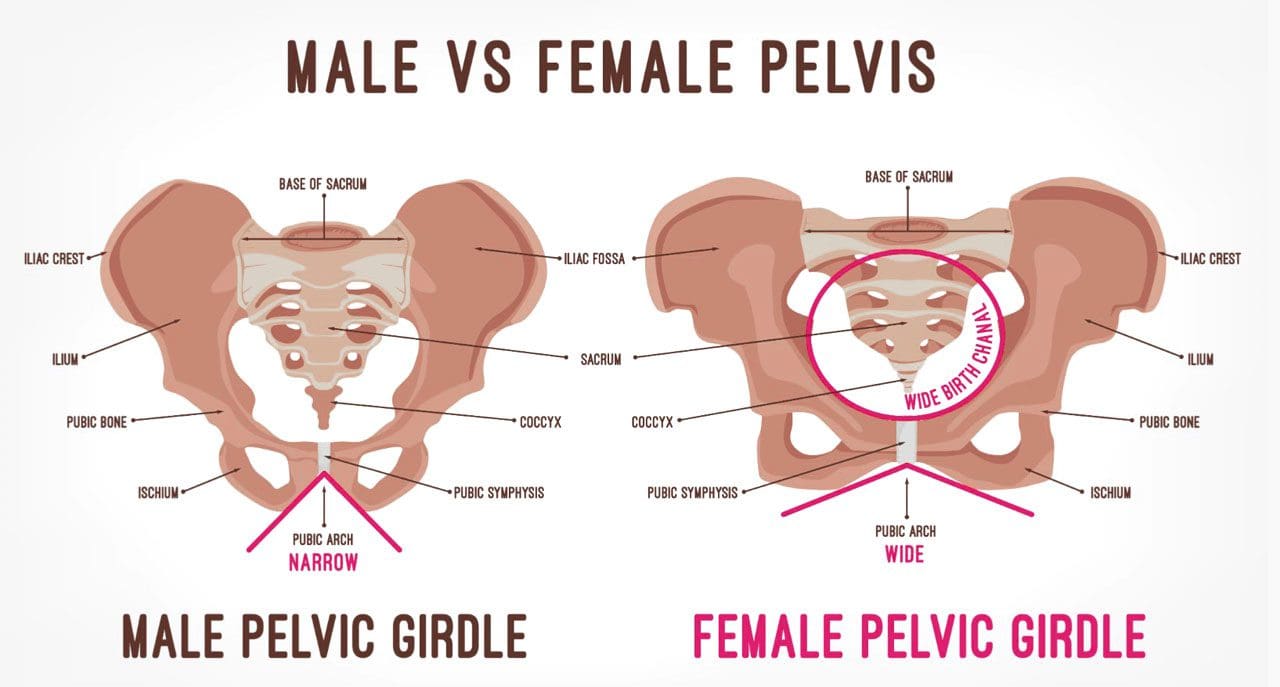
For women experiencing lower back and pelvic pain, could understanding symptoms help in the diagnostic process, treatment options, and prevention?
Low Back and Pelvic Pain In Women
In women, lower back and hip pain that radiates to the front pelvis area can have a variety of causes. The pain can feel dull, sharp, or burning. The main causes of lower back and pelvic pain in women fall into two categories. (William S. Richardson, et al., 2009)
Musculoskeletal and nervous system
Related causes of pain affect how your muscles, nerves, ligaments, joints, and bones move.
Examples include sciatica, arthritis, and injury.
Other organ system-based
Causes may stem from the following:
Acute/chronic conditions or infections
Kidneys – stones, infection, and other ailments or conditions.
Reproductive system – such as the ovaries.
Gastrointestinal system – inguinal hernias or appendix.
Musculoskeletal and Nervous System Causes
Musculoskeletal and nervous system-related causes can be from injuries like a fall or practicing unhealthy posture.
Overuse Injuries and Trauma
Frequent use and repetitive movements can lead to overuse injuries to the muscles, ligaments, and joints. :
Exercises, sports, and physical activities that require repetitive twisting and bending.
Lifting, carrying, and placing objects that require movements that are repeated regularly.
Trauma from vehicle collisions, accidents, falls, or sports accidents can inflict acute and chronic bodily injuries, like strained muscles or broken bones.
Depending on the type of trauma, healing and recovery time and treatment vary.
Both types of injuries can lead to numbness, tingling, pain, stiffness, popping sensations, and/or weakness in the legs.
Mobility Problems
Over time, a decreased range of motion and mobility in muscles and joints can cause discomfort and pain. Causes include:
Long periods of time spent in the same position.
Sitting for extended periods.
The pain often feels dull, achy, and stiff.
It can also lead to muscle spasms characterized by quick episodes of sharp and intense pain.
Posture
Posture while sitting, standing, and walking affects the body’s range of motion.
It can affect the nerves and blood circulation to the back and pelvic region.
Prolonged unhealthy postures can contribute to lower back pain and muscle strain.
Posture-related symptoms can feel achy and stiff and lead to quick episodes of severe or intense pain, depending on the position.
Sciatica and Nerve Compression
A bulging or herniating vertebral disc most commonly causes sciatica and pinched or compressed nerves.
The sensations can be sharp, burning, electrical, and/or radiating pain along the nerve pathway.
Arthritis
Arthritis inflammation causes swelling, stiffness, pain, and the breakdown of cartilage that cushions the joints.
Hip arthritis causes groin pain that can radiate to the back and becomes more intense when standing or walking.
Thoracic and lumbar spine arthritis, or degenerative disc disease, are other common causes of back pain.
Sacroiliac Joint Dysfunction
The sacroiliac joints connect the lower spine and pelvis.
When these joints move too much or too little, it can cause sacroiliac joint pain, leading to a burning sensation in the lower back and pelvic area. (Daisuke Kurosawa, Eiichi Murakami, Toshimi Aizawa. 2017)
Renal and Urinary Causes
Kidney Stones
Kidney stones are the build-up of minerals and salts, which form into hard stones in the kidneys.
When the kidney stone begins to move to the bladder, pain symptoms will present.
It can trigger severe back and side pain that radiates to the pelvic region.
Other symptoms include – a change in urine color, pain when urinating, nausea, and vomiting.
Kidney Infection and Urinary Tract Infections
Urinary tract and kidney infections are also causes of lower back and pelvic pain in women.
They cause fever, continued urge to urinate, and painful urination.
Gynecological Causes
Pelvic Inflammatory Disease
Infections, known as pelvic inflammatory disease, occur when sexually transmitted bacteria spread through the vagina, womb, fallopian tubes, or ovaries. Symptoms include:
Pain during intercourse.
Bleeding between periods.
Vaginal discharge.
Pain in the lower abdomen or groin.
Fever.
Ovarian Cysts
The cyst can be a solid or fluid-filled sac on the surface or within an ovary.
Small ovarian cysts are unlikely to cause pain.
Large cysts or those that rupture can cause mild to severe pain.
The pain can occur during menstruation or intercourse and present acutely in the back, pelvis, or lower abdomen.
During Pregnancy
Back pain and discomfort in the pelvis area are common.
As the body adjusts, the bones and round ligaments in the pelvis move and stretch, which can cause discomfort.
Symptoms are usually normal but should be discussed with a healthcare provider during check-ups.
Pain in the lower back and groin can be a sign of miscarriage or labor – including preterm labor.
Sexually Transmitted Infection
Sexually transmitted infections, like chlamydia or gonorrhea, can cause lower back and groin pain.
Other symptoms can include – painful urination, vaginal discharge, intercourse pain, and bleeding between periods.
Yeast Infection
A yeast infection – overgrowth of the fungus candidiasis.
A common vaginal infection with symptoms including – itching, swelling, irritation, and pelvic pain.
Other Causes
Appendicitis
When the appendix becomes blocked, infected, and inflamed.
In most cases, a major symptom is pain that starts near or around the belly button.
In other cases, it can start in the lower back and radiate to the right side of the pelvic area. (Johns Hopkins Medicine. 2023)
Associated pain can worsen over time or when coughing, moving, or taking deep breaths.
It involves soft tissue and part of the intestine, pushing through weak groin muscles.
Pain presents in the abdomen, lower back, or pelvis, especially when bending or lifting objects.
Pancreatitis
Inflammation in the pancreas.
Infection, bile stones, or alcohol can cause it.
One symptom is abdominal pain that radiates to the back.
The pain becomes worse during and after eating.
Other symptoms include nausea, vomiting, and fever.
Enlarged Lymph Nodes
Lymph nodes lie in the internal and external regions of the iliac artery in the pelvis.
These can become enlarged by infection, injury, and, in rare cases, cancer.
Symptoms include pain, swelling, redness, skin irritation, and fever.
Enlarged Spleen
The spleen is located behind the left side of the rib cage.
It filters the blood and supports new blood cell creation.
Infections and diseases can cause the spleen to become enlarged.
An enlarged spleen – a condition known as splenomegaly – causes pain in the upper left part of the belly and sometimes the left shoulder and upper back.
However, some individuals with an enlarged spleen experience abdominal symptoms – not being able to eat without discomfort. (Mount Sinai. 2023)
Diagnosis
Depending on the cause of your pain, a healthcare provider may be able to diagnose it with a physical exam and by asking questions about your condition.
Other tests may be needed to find the cause, particularly blood work and imaging (X-ray or magnetic resonance imaging).
Treatment
Treatment of symptoms depends on the cause.
Once a diagnosis is made, an effective treatment plan will be developed and contain a combination of therapies:
Lifestyle Adjustments
For injuries caused by muscle strains, joint sprains, overuse, and smaller traumas, pain can be resolved with:
Rest
Ice therapy
Over-the-counter pain relievers – acetaminophen or ibuprofen.
Braces or compression wraps can help support the body and alleviate symptoms during healing and recovery.
Exercises to improve posture
Paying attention to form when lifting objects
Stretching can help ease the pain.
Medication
Medications can be used in a variety of ways to help in the treatment of lower back and pelvic pain. If an infection is the cause, medications will be prescribed to remove the infection and resolve the symptoms, which can include:
Antibiotics
Antifungals
Antivirals
Medications may also be prescribed to help manage pain symptoms and may include:
Medication to relieve nerve pain
Muscle relaxants
Steroids
Physical Therapy
A physical therapist can help to correct problems with:
Posture
Decreased mobility
Walking gait
Strengthening
A physical therapist will provide exercises to help increase and maintain strength, range of motion, and flexibility.
Pelvic Floor Therapy
This is physical therapy that focuses on the muscles, ligaments, and connective tissues in the pelvis.
It helps with pain, weakness, and dysfunction in the pelvic area.
A treatment plan will be developed to help with strength and range of motion in the pelvic muscles.
Chiropractic Care
Chiropractors offer spinal and hip adjustments to realign the joints of the spine.
Some more severe conditions could require surgery.
Ovarian cysts, hernias, and other infections sometimes require surgery to remove infected or unhealthy tissue – ruptured ovarian cysts or appendicitis.
Recommended surgeries can include:
A hernia repair.
Hip replacement.
Gallbladder removal to prevent recurring pancreatitis.
Prevention
Not all conditions and diseases cause lower back and pelvic pain. Symptoms can be prevented and reduced by adopting lifestyle changes. Prevention recommendations can include:
Staying hydrated.
Using proper bending and lifting techniques.
Eating healthy foods.
Regularly engaging in some form of physical activity – walking, swimming, yoga, cycling, or strength training.
Maintaining a healthy weight.
Pregnancy and Sciatica
References
Richardson, W. S., Jones, D. G., Winters, J. C., & McQueen, M. A. (2009). The treatment of inguinal pain. Ochsner journal, 9(1), 11–13.
Kurosawa, D., Murakami, E., & Aizawa, T. (2017). Groin pain associated with sacroiliac joint dysfunction and lumbar disorders. Clinical neurology and neurosurgery, 161, 104–109. https://doi.org/10.1016/j.clineuro.2017.08.018
Santilli, V., Beghi, E., & Finucci, S. (2006). Chiropractic manipulation in the treatment of acute back pain and sciatica with disc protrusion: a randomized double-blind clinical trial of active and simulated spinal manipulations. The spine journal : official journal of the North American Spine Society, 6(2), 131–137. https://doi.org/10.1016/j.spinee.2005.08.001
Individuals’ feet will heat up when walking or running; however, burning feet could be a symptom of medical conditions like athlete’s foot or a nerve injury or damage. Can awareness of these symptoms help identify solutions to relieve and heal the underlying condition?
Burning Feet
Walkers and runners often experience heat in their feet. This is natural from the increased circulation, heart rate, warm or hot sidewalks, and pavement. But the feet could experience an abnormal hot or burning sensation. Usually, the overheating is caused by socks and shoes and fatigue after a long workout. The first self-care steps include trying new or specialized footwear and workout adjustments. If burning feet persist or there are signs of infection, tingling, numbness, or pain, individuals should see their healthcare provider. (Mayo Clinic. 2018)
Footwear
The shoes and how they are worn may be the cause.
First, look at the material of the shoes. They could be shoes and/or insoles that don’t circulate air. They can get hot and sweaty without proper air circulation around the feet.
When choosing running shoes, consider a mesh material that allows airflow to keep the feet cool.
Consider getting fitted for shoes that are the right size, as the feet swell when running or walking.
If the shoes are too small, air can’t circulate, creating more friction between the foot and the shoe.
Shoes that are too large can also contribute to friction as the feet move around too much.
Insoles could also contribute.
Some insoles can make the feet hot, even if the shoes are breathable.
Swap the insoles from another pair of shoes to see if they are contributing, and if so, look into new insoles.
Tips to help prevent hot feet:
Topical Ointments
Use an anti-blister/chafing topical cream to lubricate and protect the feet.
This will reduce friction and prevent blisters.
Lace Properly
Individuals may be lacing the shoes too tight, constricting circulation, or irritating the nerves at the top of the foot.
Individuals should be able to slide one finger under the knot.
Remember that the feet will swell as walking or running commences
Individuals may need to loosen their laces after warming up.
Individuals are recommended to learn lacing techniques that will ensure they are not too tight over the sensitive areas.
Cushioning
Fatigue from long workouts or long days standing/moving can result in burning feet.
Individuals may need added cushioning in the shoes.
Look for work and athletic shoes that have added cushioning.
Shoe Allergies
Individuals may have an allergic reaction or a sensitivity to the fabric, adhesives, dyes, or other chemicals. (Cleveland Clinic. 2023) The chemicals used in production vary for leather compared to fabric and are different by brand and manufacturer.
A shoe material allergy may also result in burning, itching, and swelling.
It’s recommended to note whether symptoms only happen when wearing a specific pair of shoes.
Recommendations are to try different kinds and brands of shoes.
Socks
The sock fabric could be contributing to hot or burning feet. Steps to take can include:
Avoid cotton
Cotton is a natural fiber but is not recommended for walking and running as it holds sweat that can keep the feet wet.
It is recommended to use socks made of Cool-Max and other artificial fibers that wick sweat away and cool them down.
Wool
Wool socks can also cause itching and burning sensations.
Consider athletic socks made from itch-free wool.
Mindfulness
Individuals could be sensitive to other fabrics or dyes in socks.
Take note of which socks cause hot or burning feet symptoms.
Individuals could also be sensitive to laundry products and are recommended to try a different brand or type.
Medical Conditions
In addition to shoes and socks, medical conditions could cause and contribute to symptoms.
Athlete’s Foot
Athlete’s foot is a fungal infection.
Individuals may feel a burning sensation in the affected area.
Typically, it is itchy, red, scaling, or cracking.
Rotate shoes.
The fungus grows in damp places, therefore, it is recommended to rotate shoes to allow them to dry out between workouts.
Wash and dry the feet after walking or running.
Try home and over-the-counter solutions, powders, and remedies to treat athlete’s foot.
Peripheral Neuropathy
Individuals frequently experiencing burning feet apart from when they have been exercising could be due to nerve damage known as peripheral neuropathy. (National Institute of Neurological Disorders and Stroke. 2023) Peripheral neuropathy symptoms include pins and needles, numbness, tickling, tingling, and/or burning sensations.
Examination
Diabetes is one of the most common causes of peripheral neuropathy.
Diabetes can come on at any age.
Individuals need to learn how to protect their feet, as exercise is recommended for diabetes.
Other conditions that can produce peripheral neuropathy include:
Vitamin B-12 deficiency
Alcohol abuse
Circulatory disorders
AIDS
Heavy metal poisoning
Massage and Movement
Massaging the feet also increases circulation.
Exercise such as walking is recommended for peripheral neuropathy as it improves circulation to the feet.
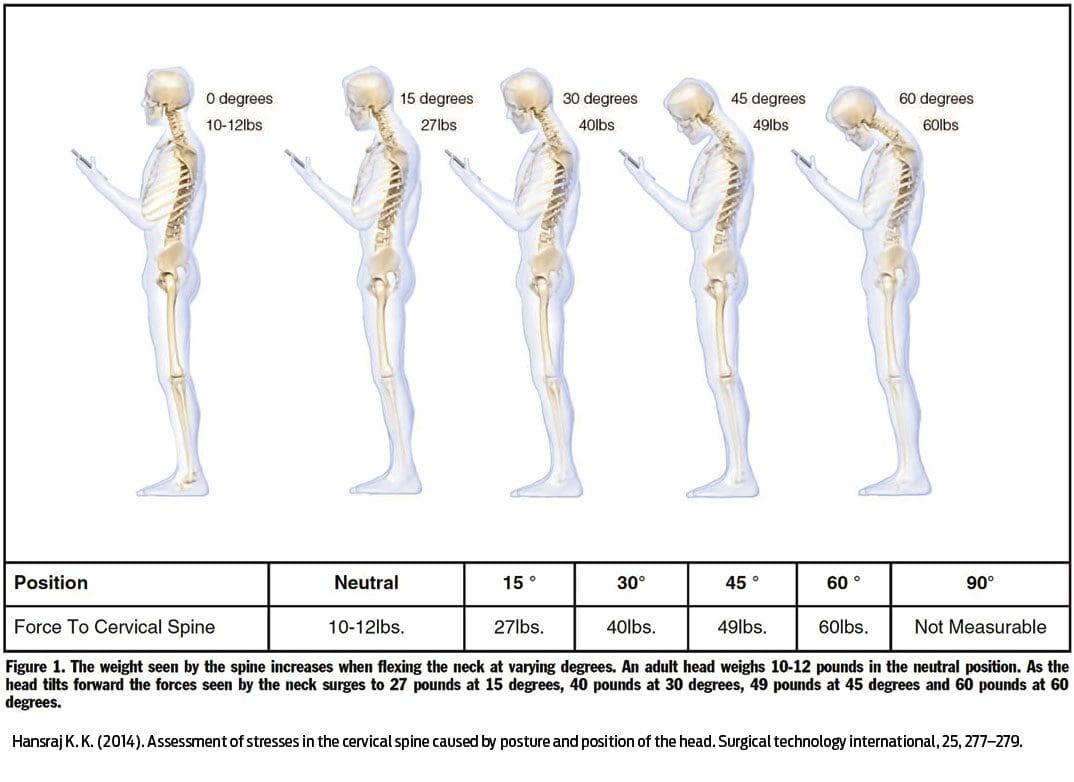
Individuals that sit at a desk/workstation for hours for work or school, or drive for a living, could be fostering a long-term condition known as forward head posture. Can understanding the signs and symptoms help to prevent the condition?
Forward Head Posture
Neck pain often causes or is caused by misalignment in the area between the shoulders and head. Forward head posture is a common problem that can strain the neck muscles, leading to pain and worsening neck, shoulder, and back posture. (Jung-Ho Kang, et al., 2012) For individuals who are at risk of developing or are already showing signs/symptoms, it’s important to get medical attention to prevent complications, such as chronic neck pain or compressing a nerve. Individuals can continue to do the work that they need to do but may need some postural adjustments and re-training so as not to continue straining the neck while working.
Postural Deviation
The head is in a healthy alignment with the neck when the ears line up with the gravity line.
The gravity line is an imaginary straight line that represents gravity’s downward pull.
It is used in posture assessments as a reference for noting the positions of the body and determining the presence of any postural misalignment or deviation.
A forward head posture occurs when the head begins to position forward of the gravity line when looking at the body from the side.
Forward head posture is a postural deviation because the head varies from the reference line. (Jung-Ho Kang, et al., 2012)
Muscle Imbalances
Forward head posture often results in a strength imbalance between muscles that support and move your neck, shoulders, and head. (Dae-Hyun Kim, et al., 2018)
The muscles in the back of the neck become shortened and overactive as they flex forward, while the muscles in the front become lengthened, weaker, and strained when they relax.
Kyphosis
Kyphosis also known as hunchback is when the shoulders round forward, and the head is also brought forward. (Jung-Ho Kang, et al., 2012) After many hours sitting at a desk, computer, or driving, kyphosis can also cause and/or worsen forward head posture.
This occurs because the upper back area supports the neck and head.
When the upper back moves or changes position, the head and neck follow.
The majority of the head’s weight is in the front, and this contributes to the forward movement.
An individual with kyphosis has to lift their head to see.
Treatment
A chiropractic injury specialist team can develop a personalized treatment plan to relieve pain symptoms, provide postural retraining, realign the spine, and restore mobility and function.
Standing and sitting using a healthy posture, along with exercises to strengthen the neck muscles, can help get the spine in alignment. (Elżbieta Szczygieł, et al., 2019)
Targeted stretching can help if the neck muscles are tight.
At-home stretches may also relieve pain
Risk Factors
Pretty much everyone is at risk of developing a forward head posture. Common risk factors include:
Constantly looking down at a phone and staying in this position for a long time aka text neck.
Desk jobs and computer use can significantly round the shoulders and upper back, leading to a forward head posture. (Jung-Ho Kang, et al., 2012)
Driving for a living causes prolonged back, neck, and shoulder positioning.
Sleeping or reading with a large pillow under the head can contribute to forward head posture.
Doing work that requires dexterity and close-up positions, like a seamstress or technician can cause over-positioning of the neck.
Individuals who regularly carry a significant amount of weight in front of their body may begin to develop kyphosis.
An example is carrying a child or another load in front of the body.
Large breasts can also increase the risk of kyphosis and forward head posture.
Neck Injuries
References
Kang, J. H., Park, R. Y., Lee, S. J., Kim, J. Y., Yoon, S. R., & Jung, K. I. (2012). The effect of the forward head posture on postural balance in long time computer based worker. Annals of rehabilitation medicine, 36(1), 98–104. https://doi.org/10.5535/arm.2012.36.1.98
Kim, D. H., Kim, C. J., & Son, S. M. (2018). Neck Pain in Adults with Forward Head Posture: Effects of Craniovertebral Angle and Cervical Range of Motion. Osong public health and research perspectives, 9(6), 309–313. https://doi.org/10.24171/j.phrp.2018.9.6.04
Szczygieł, E., Sieradzki, B., Masłoń, A., Golec, J., Czechowska, D., Węglarz, K., Szczygieł, R., & Golec, E. (2019). Assessing the impact of certain exercises on the spatial head posture. International journal of occupational medicine and environmental health, 32(1), 43–51. https://doi.org/10.13075/ijomeh.1896.01293
Hansraj K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical technology international, 25, 277–279.
As research increases in regenerative medicine with the potential of being able to regrow thyroid tissue, could regeneration therapy eliminate the need for patients to take thyroid replacement hormones?
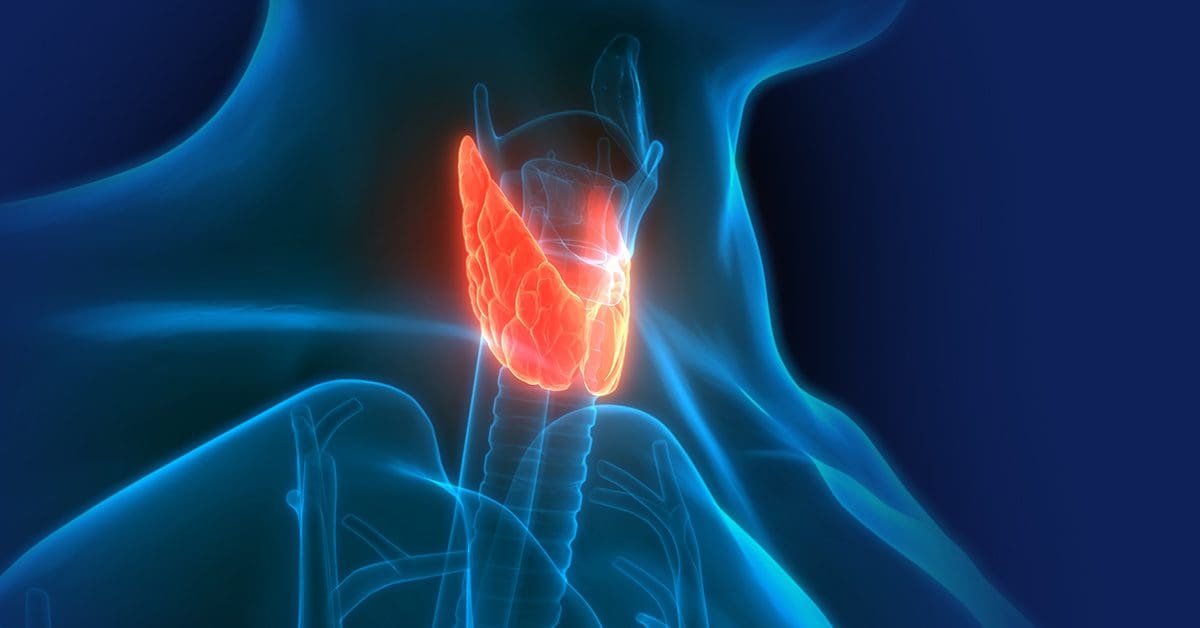
Thyroid Regenerative Therapy
A great hope for regenerative therapy is the ability to grow healthy organs. One of the organs being looked at is the thyroid gland. The goal is to re-grow thyroid tissue in:
Individuals who had to have the gland removed because of thyroid cancer.
Individuals who were born without a fully developed gland.
As science advances and research has expanded from laboratory and animal experiments to test tube human thyroid cell studies, the use of stem cell therapy for this purpose is not there yet, as more extensive research is needed for human consideration.
Human Research
Research on the use of thyroid regenerative therapy for thyroid disease has not published studies in which stem cell therapy has been attempted in human thyroid patients.
The studies that have been done were conducted in mice, and any findings of this research cannot automatically be applied to humans. (H. P. Gaide Chevronnay, et al., 2016)
In human thyroid tissue in test tube studies, the stimulation of cells was achieved in a way that raised the question of making cancerous transformations more likely if it were to be attempted in humans. (Davies T.F., et al., 2011)
Recent Studies
Current research involves advances in embryonic stem cell – ESC and induced pluripotent stem cell – iPSC. (Will Sewell, Reigh-Yi Lin. 2014)
ESCs, also known as pluripotent stem cells, can increase any type of cell in the body.
They are harvested from embryos that were produced, but not implanted, during IVF procedures.
iPSCs are pluripotent cells that have been developed using a reprogramming process of adult cells.
Follicular cells are thyroid cells that make thyroid hormones – T4 and T3 and have been produced from the embryonic stem cells of mice.
In a study published in the journal Cell Stem Cell in 2015, these cells had the ability to grow and were also able to start making thyroid hormone within two weeks. (Anita A. Kurmann, et al., 2015)
After eight weeks, cells that were transplanted into mice that did not have thyroid glands had normal amounts of thyroid hormone.
New Thyroid Gland
Investigators at Mount Sinai Hospital induced human embryonic stem cells into thyroid cells.
They were looking at the possibility of creating a new-like thyroid gland in individuals who have had their thyroid surgically removed.
The future looks promising for the ability to regrow thyroid tissue and eliminate thyroid replacement hormone. However, far more research is needed for this to even be considered a possibility.
Cracking the Low Thyroid Code Assessment Guide
References
Gaide Chevronnay, H. P., Janssens, V., Van Der Smissen, P., Rocca, C. J., Liao, X. H., Refetoff, S., Pierreux, C. E., Cherqui, S., & Courtoy, P. J. (2016). Hematopoietic Stem Cells Transplantation Can Normalize Thyroid Function in a Cystinosis Mouse Model. Endocrinology, 157(4), 1363–1371. https://doi.org/10.1210/en.2015-1762
Davies, T. F., Latif, R., Minsky, N. C., & Ma, R. (2011). Clinical review: The emerging cell biology of thyroid stem cells. The Journal of clinical endocrinology and metabolism, 96(9), 2692–2702. https://doi.org/10.1210/jc.2011-1047
Sewell, W., & Lin, R. Y. (2014). Generation of thyroid follicular cells from pluripotent stem cells: potential for regenerative medicine. Frontiers in endocrinology, 5, 96. https://doi.org/10.3389/fendo.2014.00096
Kurmann, A. A., Serra, M., Hawkins, F., Rankin, S. A., Mori, M., Astapova, I., Ullas, S., Lin, S., Bilodeau, M., Rossant, J., Jean, J. C., Ikonomou, L., Deterding, R. R., Shannon, J. M., Zorn, A. M., Hollenberg, A. N., & Kotton, D. N. (2015). Regeneration of Thyroid Function by Transplantation of Differentiated Pluripotent Stem Cells. Cell stem cell, 17(5), 527–542. https://doi.org/10.1016/j.stem.2015.09.004
Tuttle, R. M., & Wondisford, F. E. (2014). Welcome to the 84th annual meeting of the American Thyroid Association. Thyroid : official journal of the American Thyroid Association, 24(10), 1439–1440. https://doi.org/10.1089/thy.2014.0429
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine