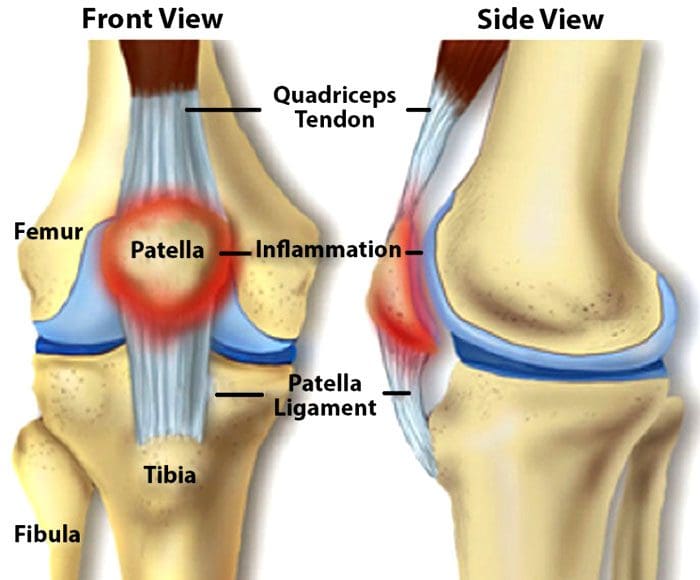
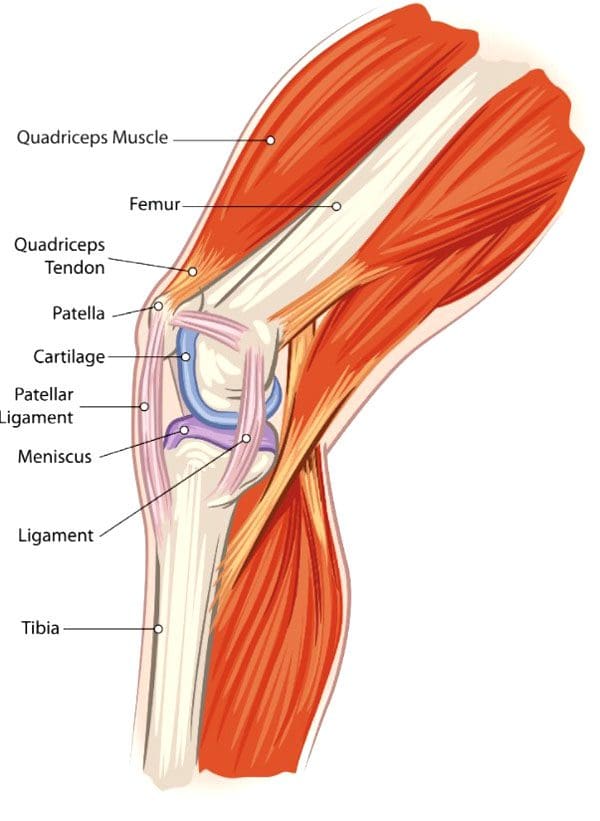
Knee Injuries, Surgeries, and Vitamin D Status. The knee joint is one of the largest and complex joints. It connects the thigh bone to the shinbone, which has a very important role in:
Supporting the body’s weight
Facilitating movement
Allowing the ability to bend the knee
Because of the complexity of the knee joint, it is highly susceptible to injuries. The most common injuries include tears in the:
Ligaments
Tendons
Cartilage
The kneecap itself can be fractured and/or dislocated.
Tears
Meniscal Tears
The meniscus is the cartilage between the knee joint that absorbs the impact/shock when running, playing sports, yard work, hiking, bicycling, etc. It cushions the joint and maintains stability.
Meniscus tears are common in sports that have a lot of jumping, starting/stopping quickly, changing direction suddenly, like volleyball, basketball, tennis, soccer, football. This is when the meniscus tears. Surgery can be required, depending on the severity/extent of the injury and tear.
Tendon Tears
The patellar tendon works with the knee muscles in the front of the thigh to straighten the leg. Tears in the patellar tendon are common among middle-aged individuals and those that participate in running or jumping sports.
A complete tear is considered a disabling injury that requires surgery for full functional recovery.
Fortunately, most tears are partial and require rest and chiropractic/physical therapy to heal.
Dislocation
Knee dislocations happen when the knee bones shift out of position. This can happen after a fall, car crash, or high-speed impact. It can also be caused by twisting the knee while the foot stays planted. Dislocations require relocation. However, sometimes a dislocated kneecap corrects itself and returns to the proper position. Other cases can require a mild sedative to allow a doctor to relocate the knee. Dislocations generally take around six weeks to fully heal.
Anterior Cruciate Ligament – ACL Injury
The anterior cruciate ligament or ACL is knee tissue that joins the upper and lower leg bones and maintains the knees’ stability. The ACL can be torn if the lower leg over-extends forward or if the leg gets twisted. ACL injuries are common knee injuries and account for around 40% of sports-related injuries. These injuries can range from a small tear in the ligament to a severe injury where the ligament tears completely or gets separated from the bone. Treatment depends on the severity of the injury. Depending on various factors including the severity of the tear, surgery could be required.
Knee Surgery
For most cases, surgery is done using arthroscopytechnology. This procedure uses small incisions to insert a camera and surgical instruments into the joint. Usually, two or three incisions are needed with recovery time being quicker than large incision surgery where the whole knee is opened. Minimally invasive arthroscopic surgery is preferred by sports medicine experts. With this procedure:
There is no need to cut the tendons or muscles
Bleeding is reduced
Small incisions decrease scarring
Recovery time is shorter
However, sometimes a large incision is required for complex surgical techniques. Common knee surgery procedures include:
Arthroscopy Surgery
This method allows the ability to see inside the knee joint. The procedure is often recommended for:
Diagnosis
Minor repairs to ligaments and/or tendons
Cartilage or bone that needs to be removed
Total Knee Replacement
A full knee replacement is known as arthroplasty. When the joint is damaged beyond repair from injury or disease, an implant is placed in the knee joint restoring function. A small amount of cartilage and bone from the shinbone and thigh bone gets removed for perfect placement of the new knee joint.
Revision Knee Replacement
Most knee replacements last around 15 – 20 years. For individuals that have knee replacement early, then a new operation for new implants could be required. Here, the surgeon removes the original prosthesis and replaces it with a new one.
Partial Knee Replacement
Some knee injuries do not require complete replacement. Here, only the worn-out portion of the joint is replaced. As an example, the cartilage that has been lost in an area of the knee can be repaired with a partial replacement.
Vitamin D Status
A study on athletes that underwent ACL surgery looked at their vitamin d status and how it affected their recovery.
The research concluded that vitamin D status had no effect on surgery outcomes.
However, those with the lowest vitamin D status had three times the failure rate than those with higher vitamin D
The average age of the individuals was around twenty-four and were healthy athletes.
Each of the patients in this study had their vitamin levels measured before the operation and were grouped based on their vitamin D status:
Group 1 vitamin D below 20 ng/mL – considered deficient
Group 2 vitamin D between 20-30 ng/mL – considered low but in a technical range
Group 3 vitamin D above 30 ng/mL – considered sufficient, but not optimal
All were followed for two years with their surgery recovery being measured with two systems.
The Lysholm score, which is a 100 point scoring system that looks at an individual’s knee functions that include:
Mechanical locking
Instability
Pain
Swelling
Stair climbing
Squatting
The WOMAC score is a scoring system that measures:
After 2 years, the Lysholm score and the WOMAC scores were similar.
However, there was a difference in the graft failure rate which was about 6% in group 1 with the lowest vitamin D and around 2% in groups 2 and 3. This shows that the lowest vitamin D status has three times the failure rate compared with those that had increased vitamin D levels. Vitamin D is a known anti-inflammatory with metabolic functions that are documented. Therefore, vitamin D does improve surgical success and recovery in healthy athletes.
Body Composition
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Brambilla, Lorenzo, et al. “Outcome of total hip and total knee arthroplasty and vitamin D homeostasis.” British medical bulletin vol. 135,1 (2020): 50-61. doi:10.1093/bmb/ldaa018
European Journal of Orthopedic Surgery and Traumatology, January 2021
Zhang, Hao et al. “Vitamin D Status and Patient Outcomes after Knee or Hip Surgery: A Meta-Analysis.” Annals of nutrition & metabolism vol. 73,2 (2018): 121-130. doi:10.1159/000490670
Individuals that have undergone spine surgery or spinal fusion for extreme low back pain caused by degeneration, herniated disks, sciatica, and other injuries could benefit from gentle chiropractic therapy post-surgery. Spinal fusion surgery is one of the last options after non-invasive treatment/s aren’t providing relief like:
Massage
Physical therapy
Chiropractic
Medications
However, many patients still experience pain/discomfort after the surgery and wonder which rehabilitation treatment options are available to them. Is chiropractic care still an option after major spinal surgery? Doctors will warn patients about the risks of receiving chiropractic treatment after surgery. This is true with high-velocity low-amplitude spinal adjustments/manipulation.
But incorporating gentle chiropractic therapy could benefit individuals still experiencing back pain after surgery. However, an individual needs to be adequately healed prior to beginning treatment. At Injury Medical Chiropractic and Functional Wellness Clinic, we regularly consult with patients post-surgery about the effectiveness of spinal rehabilitation therapy.
After the surgery wait time
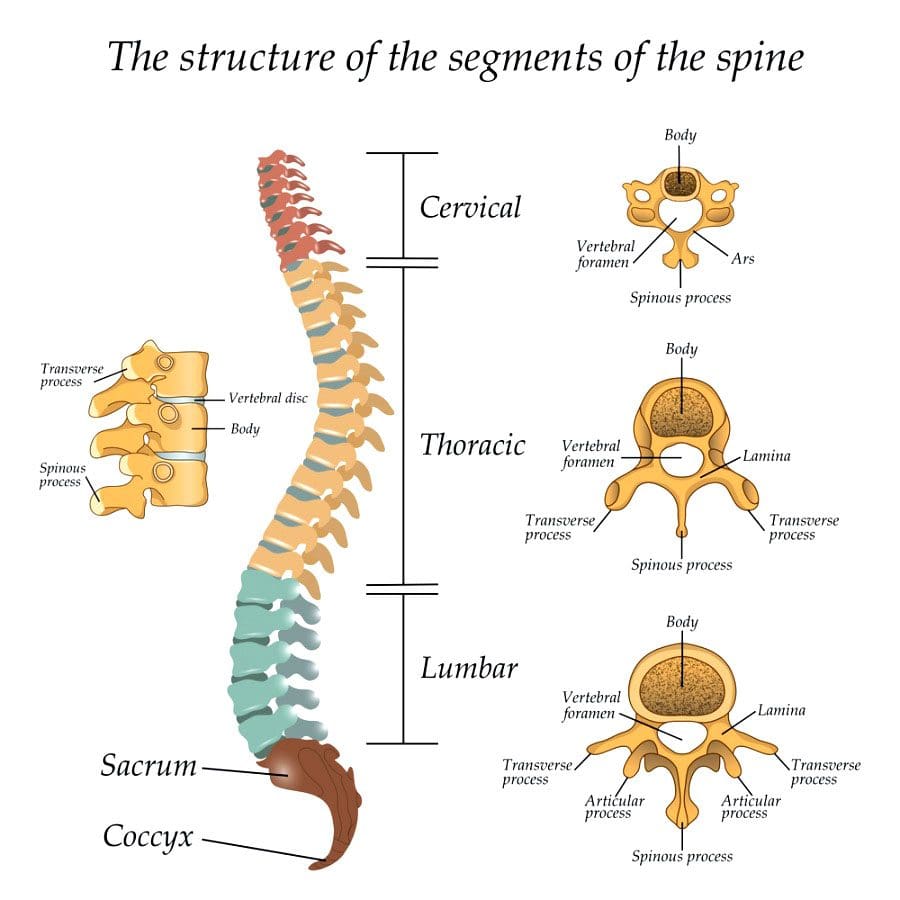
Spinal fusion surgeryremoves the discs between two or more vertebrae and fuses the bones together with screws and plates. The objective is to correct conditions like herniated discs and degenerative disc disease by immobilizing the spine in that area. It can take three months for the vertebrae to fuse together and create a complete immobilized graft. Once the graft is complete, physical therapy is brought in to strengthen the muscles around the graft. Patients are told to avoid any twisting and bending motions, or the graft could break.
How gentle chiropractic therapy can help
Spinal fusion surgery is not guaranteed to cure the problem causing an individual’s back pain. Gentle chiropractic therapy can help by therapeutically massaging the area/s keeping the muscles loose and flexible. Gentle manipulations are utilized to adjust or realign bones in the spine and other areas of the body. Because chiropractic treatment can involve intricate spinal manipulations, many individuals that have undergone back surgery can be hesitant to consider chiropractic treatment.
Discuss the possibility of receiving chiropractic therapy with a physician to determine whether the surgical graft is strong enough to withstand gentle spinal manipulations. A patient post-surgery is at greater risk of injury if they are not healed correctly before receiving chiropractic treatment. If the graft is adequately healed and a physician feels that the body is strong enough to endure mild spinal manipulations, reach out to a chiropractor to discuss treatment options.
Body Composition Clinic
Benefits of a cheat day
Cheat days can be a highly useful tool to help motivate sticking to a diet plan. Cheat days can help build a positive relationship with food. The goal is to see one’s favorite dessert/comfort food as a reward and not a coping mechanism. However, cheat days not a license to binge eat.
Binge eating can lead to eating-related issues and hurt an individual’s ability to self-regulate. Binge eating does not boost the body’s metabolism, but it can have the opposite effect. After a binge, the body’s system is overloaded with a rush of calories, sugar, and fat. In addition to causing hormone and energy levels to fluctuate, the excess of calories promotes:
Fat storage
Inflammation
Digestive discomfort
Bloating
Constipation
Cheat day frequency
Ultimately, cheat days depend on how well an individual self-regulates and what their short and long-term goals are. However, it can become very easy for a cheat day to become a cheat weekend, to a cheat week, and so on. Next thing an individual is back to old unhealthy eating habits. The objective is to understand what helps maintain motivation and develop a sustainable, long-term plan.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Perrucci, Rachel M, and Christopher M Coulis. �Chiropractic management of post-spinal cord stimulator spine pain: a case report.� Chiropractic & manual therapies�vol. 25 5. 6 Feb. 2017, doi:10.1186/s12998-017-0136-0
Fernandez, Matthew et al. �Surgery or physical activity in the management of sciatica: a systematic review and meta-analysis.� The European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society�vol. 25,11 (2016): 3495-3512. doi:10.1007/s00586-015-4148-y
O’Shaughnessy, Julie et al. �Chiropractic management of patients post-disc arthroplasty: eight case reports.��Chiropractic & osteopathy�vol. 18 7. 21 Apr. 2010, doi:10.1186/1746-1340-18-7
Spinal decompression surgery could be a treatment option discussion with a doctor to relieve nerve pain brought on by a spinal condition or disorder. Everything to know about the procedures straight from the experts.
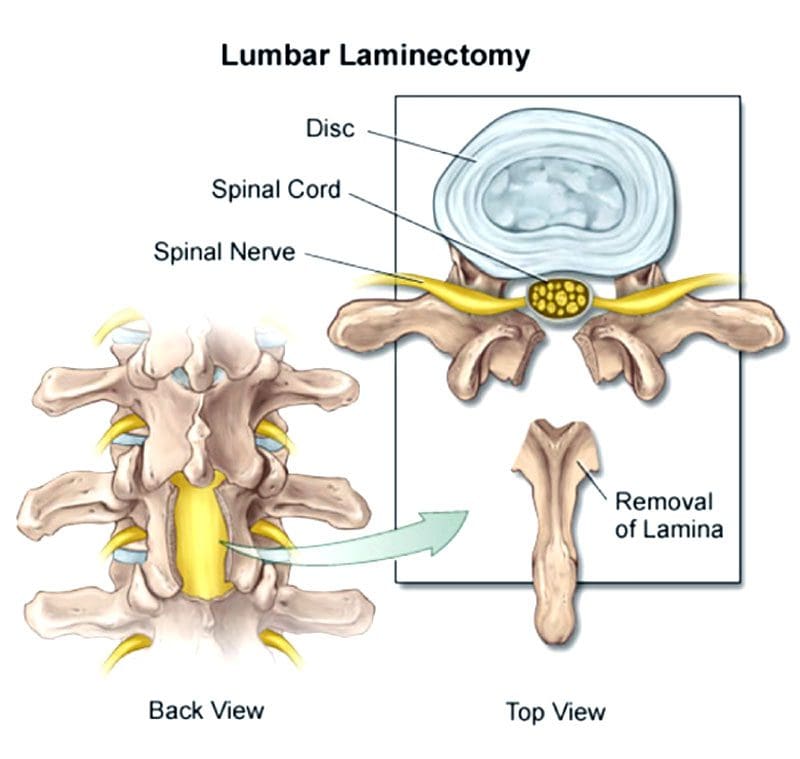
Spinal Decompression Surgery Types: Laminectomy or Laminotomy
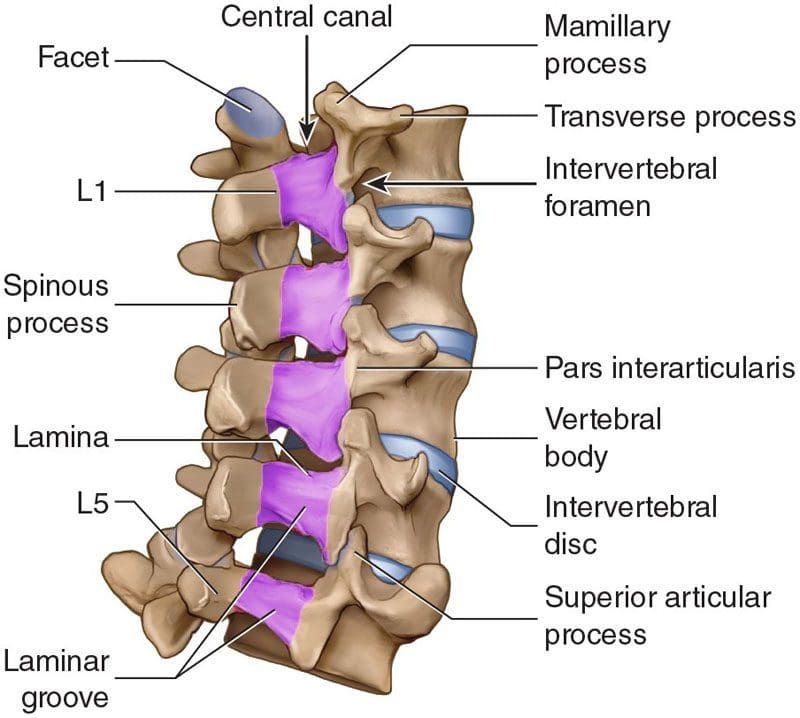
Both procedures involve the vertebrae�s lamina, which is an arch of bone that protects the spinal canal.
In a laminectomy, the lamina is removed almost entirely.
In a laminotomy, it is a partial removal.
Despite the removal, the large muscles of the back provide sustained protection for the nerves below. Therefore, the spinal nerves are still safe and secure following the procedures. Which one is right depends on the situation.
A laminectomy is usually performed to treat an arthritic condition of the spinal canal like spinal stenosis.
Laminotomy is used almost exclusively to remove a herniated disc.
A laminectomy removes more bone and sometimes the inner edge of the facet joint.
Ultimately, a surgeon will determine which of the two procedures is best for the individual’s needs and condition.
Decompression Surgery
Spinal stenosis or the narrowing of the spinal canal is usually caused by arthritis and overgrowth of the discs and joints. Similar compression issues respond well to non-surgical treatment. But sometimes surgery is necessary to treat uncommon but potentially severe cases. These include patients with:
Bowel or bladder problems caused by the pressure on the spinal nerves
Leg weakness that gets worse
Inability to walk or move for long periods and distance
The objective of spinal decompression surgery is to create space around the spinal cord and surrounding nerves by removing the compressing structure/s. When the cord and/or nerve/s are compressed, physical and neurological symptoms are experienced down the nerve�s pathway. This includes:
Tingling
Numbness
Electric shock sensations
Radiating/spreading pain
Weakness
Once the compressed nerves have space to relax and move around symptoms subside.
Laminectomy process
Lumbar laminectomy is the most common procedure to treat spinal stenosis in the low back.
It also helps treat herniated discs by allowing the surgeon to easily access the discs to repair any damage.
The surgeon removes the lamina and ligaments that have thickened and are causing problems to create more space in the canal.
The surgery enlarges the spinal canal so that pressure is relieved.
By removing the source of the pressure, the pain caused by the compressed nerves is alleviated.
An open laminectomy creates an incision of a couple of inches and exposes the spine.
The muscles of the spine and back are cut through to expose the bone.
Another technique that surgeons utilize is operating through a tube.
They’ve adapted these techniques to be able to decompress both the right and the left sides although they are only operating on one side.
Both procedures, minimal and traditional accomplish the same goals.
The difference is the minimally invasive approach involves one or more tiny incisions also known as skin punctures and small instruments designed to separate muscles and soft tissues instead of cutting through them.
The traditional approach requires a larger incision and instruments that retract, separate and cut tissues.
Laminectomy surgery
Laminectomies are performed under general anesthesia using a posterior approach/lying face down during the procedure.
It can be open or minimally invasive sometimes called a microlaminectomy.
In an open laminectomy, the surgeon makes an incision near the affected spinal area.
Once the incision is made, a retractor will move the skin, fat, and muscles to the side so the surgeon can access the spine.
Next, they remove or trim the lamina and thickened ligaments to enlarge the space surrounding the compressed nerves.
Once done, the retractor is removed and the incision is closed with sutures.
Minimally invasive surgery or MIS is performed using special instruments like endoscopes and tubular retractors.
These instruments allow for smaller incisions and less cutting.
They will also use special eyewear to have a detailed view of the surgical field.
Sometimes, the surgeon uses an endoscope or a microscope focused down the tube to perform the surgery.
The portion of the lamina is removed, along with any bone overgrowths/osteophytes and ligament tissue.
The tubular retractors are taken out so the soft tissue moves back into place, and the incision is closed with dissolving sutures.
Other spinal procedures performed alongside
Laminectomies and laminotomies are typically not performed together. However, a surgeon could perform both if the surgery affects multiple levels of the spine. They can also be combined with other spinal surgeries, that include:
Foraminotomy
A foraminotomy is also a decompression procedure. But instead of removing part or all the lamina, the surgeon accesses the nerves through the spine�s foramen or the passageway that nerves pass through on both sides.
Discectomy
This decompression surgery involves the removal of all or part of the damaged intervertebral disc and is utilized for herniated discs.
Spinal fusion
Fusion is often performed after spinal decompression surgery, as the space that was created by removing spinal structure/s can cause instability to the spine.
Candidates for spinal decompression surgery
Both are common procedures performed by neurosurgeons and orthopedic spine surgeons. Laminectomies are considered one of the most effective treatments for spinal stenosis and spinal canal issues like:
Tumors
Certain types of infections and abscesses
Spinal issues involving bowel/bladder dysfunction
The primary reason for laminectomy is spinal stenosis, most common in individuals over the age of 60.
Other considerations and conditions include:
Non-invasive treatments that don’t improve the condition that includes medication, massage, and physical therapy
Ask questions about the procedure to ensure you are comfortable with the operation. Here are some questions:
What are the risks associated?
Will the surgery relieve all symptoms?
Not having the surgery risks?
What is recovery like?
Recovery
Open or micro, recovery does take time. Following the doctor�s instructions carefully are essential to make a full, healthy recovery.
Individuals should be careful for about a month following the surgery. But does not mean laying down or being sedentary. Movement is crucial to recovery.
The patient should not stay in bed or lie on the sofa.
Wait a week or two before beginning physical therapy if necessary.
Most will have a weak core, poor posture, and poor body mechanics, the goal is to help develop and strengthen these areas.
Things to help with recovery include:
Ice/cold packs will help reduce swelling and pain.
Try not to sit for too long, as sitting is the least comfortable position after back surgery.
Body mechanic awareness means avoiding too much bending or lifting and using the right body mechanics when bending or lifting.
Especially before surgery. Quitting entirely or at least for at least six weeks before surgery will make recovery easier and healthier.
Losing weight
Speak with a doctor about weight. Just 5 pounds can make a significant difference during recovery.
Blood sugar
For individuals with diabetes, having an A1C under eight before surgery is ideal.
Every patient�s recovery is different. Recovery time depends on:
The complexity of the surgery
Personal medical history
Health issues
Recovery typically takes about two to four weeks after the surgery. However, it depends on the reason/s for the surgery.
Questions
Post-laminectomy syndrome
Post-laminectomy syndrome PLS also known as failed back surgery syndrome is a condition where an individual continues to have pain after surgery. Individuals still having symptoms after should speak with their doctor to determine the next phase of treatment.
How long before exercise?
Returning to the gym or getting into an exercise routine will take some time. It is important to follow the doctor�s recommendations and complete the full course of physical therapy before regular exercise activity can resume. Discuss workout plans with the doctor to determine the best timeline for the spine.
Full recovery?
Returning to some activity is possible around four weeks after surgery. Full recovery takes longer as each patient�s recovery is unique. Depending on the complexity of the surgery, most return to all activities within 6 to 9 months.
Body Composition Spotlight
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
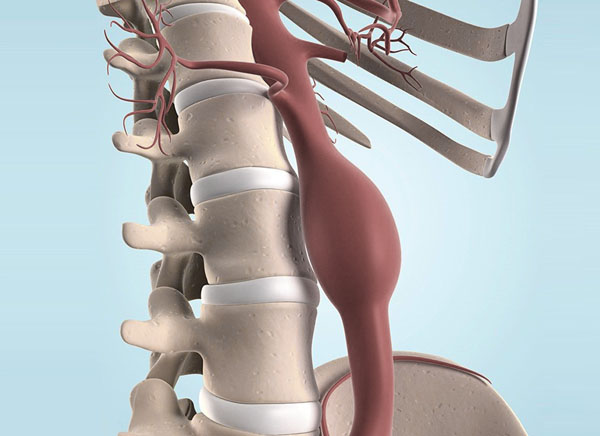
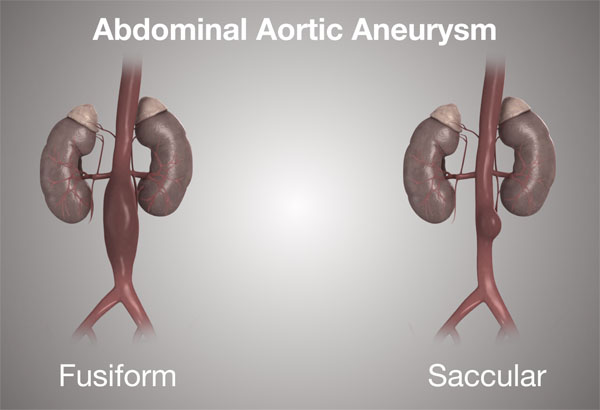
An abdominal aortic aneurysm refers to an enlargement of the abdominal aorta. If the blood vessel is enlarged and starts to leak blood or rupture, it will cause severe abdominal and lower back pain. This is a serious medical emergency that necessitates emergency surgery. Unfortunately, there is no way to reverse the damage. A prominent symptom from a rupture is severe, persistent low back pain, and pain in and around the abdomen. Treatment for an abdominal aortic aneurysmdepends on the possible complications that could develop. Approaches for treatment:
Nonsurgical treatments like anti-biotics calcium channel blockers and exercise along with monitoring are used for individuals that have a low risk of rupture.
If an aneurysm is not found until it becomes an emergency, then surgery to repair the ruptured artery is absolutely necessary. If ruptured or there is a high risk of rupturing is considered an emergency.
If a rupturing aneurysm has been diagnosed, some treatment/management will be implemented to prevent severe/fatal bleeding.
Cardiac
For low-risk cases, lifestyle changes and possible medication/s may be recommended to slow the development. Small aneurysms are monitored using ultrasound. This can be every 6 to 12 months depending on the size and growth rate of the artery.Medications for lowering blood pressure and cholesterol could be prescribed. This is to limit the amount of plaque buildup in the aorta and reduce any pressure on the arterial walls. Quitting smoking and removing tobacco altogether whether dip, chew, vape is a significant action an individual can do to minimize the risk of aortic rupture. Other lifestyle changes involve maintaining a healthy diet and regular exercise will help lower blood pressure and cholesterol levels decreasing the chance of rupture.
Surgery
Surgical treatment when necessary is to stop a rupture if leaking blood or to prevent a rupture. Surgery requires replacing the damaged portion of the aorta with a stent-graft. This is an artificial artery made from a high-tech mesh/fabric. There are two standard surgical treatments:
Open Repair
Open repair is the most common surgical treatment. It takes the enlarged portion of the aorta removes it and replaces it with a stent-graft. Open surgery repair consists of the following:
The incision is made in the abdomen at the site of the aneurysm.
The aorta gets clamped with the blood temporarily blocked from flowing through the damaged portion.
The damaged part is removed.
A tube graft is placed where the damaged portion was.
If the damage was not severe and does not require the removal and complete replacement, then less invasive options will be offered.
Endovascular Aortic Aneurysm Repair
EVAR endovascular aneurysm repair surgery is a minimally invasive procedure. There is no need for a large abdominal incision or removal of the damaged portion of the artery. This procedure does not require blood flow stoppage, which places less stress on the heart. Endovascular surgery involves:
A fluoroscopy or live X-ray is used. This is so the surgeon can look at the repair, and guide the stent into place.
2 small incisions are made in the groin.
A catheter is inserted into the femoral artery in the groin and guided to the abdominal aorta.
Through the catheter, the stent is guided to the aneurysm.
Once it reaches the aneurysm, it is compressed and closed.
The stent is placed in position, and the wireframe is expanded to fit the artery.
The stent is sewn/secured into place at both ends.
Once in place, the blood gets redirected from the enlarged area and flows only through the stent-graft. This takes the pressure off the artery’s walls and allows for size reduction over time, and decreases the risk of rupture.
The procedure is not an option for individuals with an aorta that cannot be accessed safely through the femoral arteries. Or if the artery is severely damaged that the aneurysm portion needs to be replaced. And if the aneurysm is too big or complex where an open repair is a more favorable option.
Follow Up
Follow-up monitoring is necessary after any aortic aneurysm surgical procedure. This is to ensure the stent works and the aorta is functioning without a high risk of rupture. Individuals will be advised to maintain a healthier heart and cardiovascular system. A surgeon/doctor will suggest:
Diet adjustments
Regular exercise
Quitting smoking/tobacco intake
Taking cholesterol and blood pressure medication
Chiropractic/Physical therapy for any spinal misalignment, herniation, sciatic nerve compression back pain relief.
Lower Back Pain
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Finding the right surgeon that specializes in an individual’s specific spinal conditions and physical health means doing some research. There are several types of procedures for spinal problems. The type of surgery depends on the condition and an individual’s medical history. If surgery is recommended for a lumbar herniated disc or LHD combined with sciatica here are a few things to think about.
Devotes at least 50% of their practice to spinal conditions
Specializes in treating herniated disc/s and sciatica. This means they will have added/specialized knowledge and expertise.
It is extremely important that an individual feels comfortable and feels they are able to communicate freely with the surgeon. A professionally qualified surgeon should:
Spend adequate time with the individual
Answer all questions
Provide all information needed about the condition and treatment
Listen to what the individual has to say
Is open-minded
Is not hard to get in contact with
Has experience in the latest methods and techniques
What to look at and think about
Individuals can feel uncomfortable asking questions, but thorough communication is key. Remember, it is your body, and it is your right to know the details of the spinal disorder, along with non-surgical and surgical approaches to treatment that are available. There is time to consider the options and make an informed decision about the treatment plan as most spinal procedures are elective. Ask the surgeon all the questions you have to help decide wisely and with confidence. Make sure they address all concerns, and any others not listed.
The surgeon’s specialization/focus
Orthopedic surgeons and neurosurgeons perform spinal procedures. Each will have a specific interest and expertise in certain spinal condition/s. For example, some surgeons may specialize in treating adult or pediatric patients, and some may only treat either lumbar/low back or cervical/neck conditions. Within those groups, some focus on:
Spinal deformities
Tumors
Myelopathy a spinal cord disease
Specific spinal cord diseases
Minimal invasive surgery option
Minimally invasive spine involves tiny incisions, that reduces the recovery time needed to heal. With this type, individuals can be up and walking within hours after surgery. Unfortunately, not all conditions can take this approach.
Is the surgery absolutely necessary, or can it be treated non-surgically?
Sciatica and herniated discs can be quite painful and cause disability. Never rush into surgery just to relieve symptoms. As surgery can cause other types of pain symptoms and issues. Herniation and sciatica can be resolved with:
Chiropractic
Physical therapy
Medications
Injections
Lifestyle changes
Diet adjustments
Regular exercise
Weight loss
However, if there are neurologic symptoms, like weakness in the leg, foot, numbness, or loss of bladder or bowel control – this is considered a medical emergency – then surgery is absolutely needed.
The number of similar procedures performed
The surgeon�s experience is very important. The more experienced, the better. Ask if they can refer to other patients who have had similar procedures.
Recovery time
Every patient is unique, as is the type of surgery, and recovery times. They all vary accordingly. General health, physical condition, and the severity of the disorder play a role in how long and how involved recovery time will be. Experienced surgeons can provide more specific answers concerning recovery/healing time.
Complication rate
All surgeries carry some risk of complication. Complication rates that are more than 10% is a red flag. Possible post-surgery complications.
Infection rate
Surgeons should have an infection rate lower than 10%. However higher rates do not always mean that surgeon is at fault as higher rates can come from performing highly complex procedures. Another reason for high infection rates could be the patients themselves like smokers or individuals with diabetes have increased risks for infection. However, do not feel uncomfortable asking the surgeon to explain a high infection rate.
Decide to not opt for spine surgery
As a surgeon produces a diagnosis, they should present a recommended treatment plan, including alternative treatments/therapies. Ask for another explanation of any part of the evaluation, diagnosis, or available treatment options.
Get a second opinion
A second opinion should be encouraged. A second opinion can reinforce the surgeon�s recommendations and offers a new perspective. The surgeon should be comfortable with a second opinion. This does not mean that the individual does not trust the surgeon. It does mean that there is considerable interest in achieving optimal health and making sure that surgery is the absolute right thing to do. Pass on surgeons that discourage or disapprove of second opinions and continue looking.
Whiplash Chiropractic Massage Therapy
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Whiplash injuries very rarely call for surgery. But with those rare occurrences, that are severe cases, surgery is considered appropriate when neck or shoulder pain worsens. Doctors recommend patients go through 4 to 6 weeks of non-surgical treatment. If there is no improvement or the condition is worsening then a doctor could recommend whiplash surgery as the best option.
A spine surgeon will recommend the best procedure for the specific injury. Ask all the questions you have to fully understand the exact process, the outcome, and the recovery time. Surgery is an individual’s decision. The surgeon can recommend it, but the patient has the final say. The procedure depends on what area/s the cervical spine is injured/damaged.
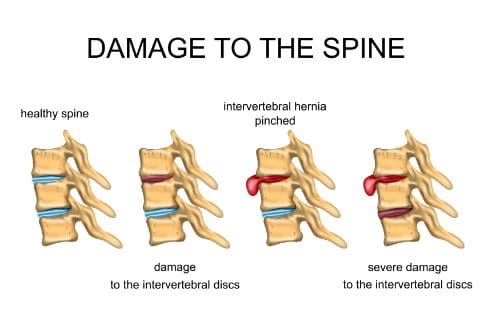
Disc Herniation
Depending on the type of trauma individuals can rupture or herniate the intervertebral disc/s, located between the vertebrae. This can generate constant pain, numbness, and weakness. With cases like this sometimes removal of the disc is necessary.
A surgeon will remove all or portion of the damaged disc through a process called a discectomy. After the discectomy, a doctor may have to permanently stabilize the area. This is because the spine becomes unstable and can move in abnormal ways. This increases the risk of a serious neurological injury. Therefore a discectomy is usually followed with a re-stabilization of the spine. Spinal stabilization techniques used:
Artificial Disc Replacement
Cervical artificial disc replacement also known as ADR could be performed instead of standard discectomy combined with spinal fusion. An artificial disc is implanted into the empty space following the procedure. Artificial disc replacement preserves or restores movement of the neck.
Fusion and Spinal Instrumentation
This form of spine stabilization can be done on its own or in combination with decompression surgery. The bones in the spine fuse together over time usually several months or longer depending on how the surgeon set up the fusion process. The surgeon will use a bone graft or a biological chemical that stimulates bone growth. A surgeon could use spinal instrumentation. These are:
Interbody device/s
Screws
Rods
Plates
These all are used to increase stability and help fuse the bones properly. The fusion prohibits movement between the vertebrae for long-term stability.
Stenosis
Whiplash surgery could also be necessary if the injury caused the spinal canal in the neck to narrow. Here a cervical corpectomy could be performed to remove part of the vertebra and intervertebral disc/s. This reduces the added pressure on the spinal cord and nerves.
A surgeon could also do a laminectomy or a laminoplasty. Both focus on the lamina, which is the bony plate at the back of each vertebra. The lamina protects the spinal cord and canal. The lamina could also present added pressure on the spinal cord. This is where the surgeon will create extra space for the cord by removing all or part of the lamina. This is a laminectomy.
A laminoplasty re-shapes the lamina to create more room for the spinal cord. If there is a narrowing of the space where the nerve exits the canal, a cervical foraminotomy could be utilized. The foramen is the area where the nerve roots exit the spinal canal. This is removed to allow for more space for the nerves to move through. A larger pathway is less likely to pinch/compress the nerve.
Complications
A doctor will discuss all the potential risks before being asked to sign a surgical consent form. Complications can include:
Injury to the spinal cord, nerves, esophagus, carotid artery, vocal cords
Pain and swelling in the leg veins known as phlebitis
Blood clots in the lung
Urination problems
Complications could lead to more surgery, so make sure there is a complete understanding of the surgery and the risks before proceeding. The final decision is up to the individual.
Whiplash Surgery Recovery
After surgery, things might not be great right away. More than likely individuals are out of bed within 24 hours, and on pain meds for 2 to 4 weeks. Individuals will receive instructions on how to sitting down, and standing up. The body needs time to heal, so the doctor will recommend restricting certain activities that involve moving the neck too much. Avoid sports, twisting, or heavy lifting during recovery. And report any problems like fever increased pain, or infection right away.
Whiplash Massage Therapy
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Different spinal surgical procedures use various types of spinal hardware to stabilize the spine. When this hardware breaks or gets infected sometimes it could have to be removed. The reason for this spinal hardware, whether from injury, disease, or a condition, that area of the spine needs added support other than the bone, collagen, ligaments, and other tissues. Surgeons utilize this hardware to:
Stabilize the spine
Correct deformities
Regain motion
Height restoration
Pain relief
Help heal another area of the spine
The hardware ranges from rods, plates, cages, wires, spacers, etc. There are many types and are employed in various operations. Many spine procedures involve some type of hardware. A surgeon relies on this spinal hardware to complete procedures involving realignment of the spine or spinal fusion.
Many patients undergo spine surgery without complications, however, some have problems with the hardware. The most common issues are the hardware loosening, breaking, or the development of an infection. Unfortunately, when this happens it can mean that another surgical procedure may be necessary to remove the hardware/device. �
�
Spinal Instrumentation
All of these pieces of equipment are designed to remain in the body permanently. The hardware can be made from stainless steel, titanium, and titanium alloy. Spinal fusion is common, involves hardware, and could be necessary to help/correct:
Spinal deformity/s
Degenerative condition/s
Heal fractures
Other issues causing back pain
The procedure involves the surgeon grafting bone between two vertebrae. Then the hardware is used to hold those vertebrae together. This eliminates motion between them. This is how the vertebrae fuse into a single bone, which reduces or eliminates the pain. Like with any surgical procedure complications can include hardware failure. �
�
Spinal Hardware Removal Reasons
If the hardware loosens, gets infected, or the patient can feel some of the hardware under the skin a surgeon will likely recommend removal. Intense, excessive pain is often a symptom of a loose screw and other hardware complications. If the hardware is protruding under the skin the patient could feel a bump that could cause pain when touched.
Loose hardware could irritate the surrounding tissues and nerves, resulting in the patient feeling pain or hearing a grating, crackling, or popping sound. Loosened instrumentation can be caused by the bones of the spine not healing or fusing correctly. The hardware can also shift and break from the bones not healing properly. Other reasons for hardware failure shortly after surgery.
Lifting heavy objects
Participation in high-impact activities
Trauma from accident, slip, fall, etc.
Health conditions especially osteoporosis and osteopenia can increase the risk of the instrumentation loosening, breaking, and shifting.
Quite uncommon but some patients develop infections right after or weeks following the surgery. When the hardware gets infected the patient could feel pain along with the site of the incision draining, and fever. Key indicators around the incision site are:
Chills
Redness
Swelling
Tenderness
Sometimes there are allergic reactions to the hardware itself. However, this has decreased significantly in recent years. This was common with stainless steel before the use of titanium. �
�
How The Removal Is Done
This type of removal surgery is typically not considered an emergency unless the nerves or spinal cord are at risk of being injured/damaged. The exact procedure depends on the individual’s specific situation and case. However, it will be easier than the first surgery. Removal is typically nowhere near the extensiveness of the initial instrumentation placement.
Before the procedure, the surgeon will advise preparation tips, just as with the original surgery. To optimize recovery, patients should ensure they are in the best possible health that they can be. This means no smoking, light exercise, and even breathing exercises for optimal lung function.
Patients should not begin any new medication regimen prior to the surgery and should ensure all medications are known to the surgical team. The procedure will go in through the original incision and remove any scar tissue around the hardware. Depending on the situation the hardware could be reinserted or left out entirely.
�
Post Removal
Hospital stay depends on the individual situation. Some patients go home the same day and some have to wait. If there was an infection it more than likely means an extended hospital stay to make sure the infection is gone and has not spread elsewhere. The healthcare team will give directions just as with the original surgery which can include detailed instructions on:
Sitting
Sleeping
Showering
Taking meds
Sex
Recovery from hardware removal depends on the extent of the surgery. Contact the surgical team if experience new or unusual symptoms after the procedure, including fever, pain beyond the surgical soreness, numbness, weakness, tingling, and for problems/issues around the incision area, like bleeding, redness, swelling, and draining.
�
Bottom Line
Spinal hardware helps the spine heal, and ultimately reduces or eliminates the back pain improving quality of life. Instrumentation and devices can be defective, causing them to break, loosen, etc and need to be replaced. It’s just in this case the replacement has to take place in and around the spine. A doctor will assess the damage and decide if removal surgery is necessary, which will prevent further problems.
18 Wheeler Accident Chiropractic Rehab
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine















 �
�








