What is pseudoarthrosis of the cervical and lumbar spine?
Pseudoarthrosis of the cervical and lumbar spine
Individuals may need a spinal fusion to treat a fractured vertebra, scoliosis, or conditions like spinal stenosis, degenerative disc disease, and spondylolisthesis/slipped vertebrae. A spinal fusion reduces pain and stabilizes the spine by limiting movement between vertebrae. Pseudoarthrosis happens when the bones don’t heal after a fracture or bone surgery. When pseudoarthrosis affects the cervical or lumbar spine, it means that two vertebrae did not heal and grow together after spinal surgery to fuse them (spinal fusion). Reasons for a failed spinal fusion include:
Issues with the instruments used to stabilize the bone
Lack of bone growth
The number of vertebrae being fused.
The patient’s health and lifestyle play a role in failed fusions, which can include
Diabetes
Inflammatory health conditions increase the risk
Smoking
Long-term steroid use
In many cases, revision surgery is needed.
Surgery-Related
During a spinal fusion, surgeons insert a bone graft between two vertebrae and then apply spinal fixation hardware (instrumented spinal fusion) that includes:
Plates
Rods
Screws
The bone graft promotes growth between the two bones.
The hardware stabilizes the vertebrae and prevents movement while they fuse and grow together.
The hardware goes inside, or internal fixation.
Although rare, a severe spinal fracture or deformity may need external fixation.
A rigid frame secured outside the body helps to stabilize the bones.
If the fusion fails, it could be caused by one or more of the following surgical issues:
The surgeon must carefully plan and use the right hardware.
The type of hardware used during a spinal fusion may influence bone healing.
The instruments can come loose or break, interfering with the fusion process.
Spinal osteoporosis, having thin, weak bones, can affect fixation.
Even with the optimal surgical preparedness, weak bones significantly increase the chance of the instruments loosening and pseudoarthrosis developing.
Bone Graft
The type of bone graft used may affect the fusion.
For example, in cervical/neck spinal fusions, an autograft, which uses a small piece of bone from the patient’s body, has a higher success rate. (Verla T. et al., 2021)
Other graft options include specialized steel cages that fit between vertebrae and contain bone growth factors.
The surgeon recommends the optimal bone graft for the type of surgery, the number of vertebrae involved, and risk factors.
Risk Factors
The patient’s overall health and lifestyle impact the results of spinal fusion. Smoking increases the risk. (Berman D. et al., 2017)
Nicotine restricts blood circulation, decreases bone density, reduces new bone formation, and delays bone healing. (Hernigou J., & Schuind F., 2019)
The primary sign of pseudoarthrosis is pain in the same area as before the fusion surgery.
If the bones pinch a spinal nerve, one arm may experience pain, tingling, burning, or numbness.
Rarely does a pinched nerve affect both arms.
The pain may return shortly after the procedure.
The pain may develop gradually or not appear for many months.
However, it’s more likely to appear after several months when the individual returns to their usual activities.
Diagnosis
The healthcare provider will learn about symptoms and perform a physical exam to evaluate the back.
They’ll assess mobility and the type of movement that causes pain.
Then, they order diagnostic imaging to see the spine and identify the cause of pain.
Individuals may need a CT scan, MRI, and/or X-rays to evaluate the spinal structures and instrumentation fully.
Treatment
Treatment for pseudoarthrosis will likely start with:
Physical therapy
Pain management – especially in cases where it is important to rule out other sources of back or neck pain.
Medication
Injections
If symptoms don’t improve with conservative care or if there is severe pain, the healthcare provider may recommend revision surgery.
Revision surgery is another procedure to treat complications or correct issues that arise after the initial pseudoarthrosis surgery.
Injury Medical Chiropractic and Functional Medicine Clinic
As a Family Practice Nurse Practitioner, Dr. Jimenez combines advanced medical expertise with chiropractic care to address various conditions. Our clinic integrates Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine to create customized care plans that promote natural healing, mobility, and long-term wellness. By focusing on flexibility, agility, and strength, we empower patients to thrive, regardless of age or health challenges. At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately focus on treating patients after injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities. We use in-person and virtual health coaching and comprehensive care plans to ensure every patient’s personalized care and wellness outcomes.
Enhancing Health Together
References
Boonsirikamchai, W., Wilartratsami, S., Ruangchainikom, M., Korwutthikulrangsri, E., Tongsai, S., & Luksanapruksa, P. (2024). Pseudarthrosis risk factors in lumbar fusion: a systematic review and meta-analysis. BMC musculoskeletal disorders, 25(1), 433. https://doi.org/10.1186/s12891-024-07531-w
Verla, T., Xu, D. S., Davis, M. J., Reece, E. M., Kelly, M., Nunez, M., Winocour, S. J., & Ropper, A. E. (2021). Failure in Cervical Spinal Fusion and Current Management Modalities. Seminars in plastic surgery, 35(1), 10–13. https://doi.org/10.1055/s-0041-1722853
Berman, D., Oren, J. H., Bendo, J., & Spivak, J. (2017). The Effect of Smoking on Spinal Fusion. International journal of spine surgery, 11(4), 29. https://doi.org/10.14444/4029
Hernigou, J., & Schuind, F. (2019). Tobacco and bone fractures: A review of the facts and issues that every orthopaedic surgeon should know. Bone & joint research, 8(6), 255–265. https://doi.org/10.1302/2046-3758.86.BJR-2018-0344.R1
Scoliosis Research Society. (2023). Pseudoarthrosis. https://www.srs.org/Patients/Conditions/Pseudoarthrosis
Torres, H. M., Arnold, K. M., Oviedo, M., Westendorf, J. J., & Weaver, S. R. (2023). Inflammatory Processes Affecting Bone Health and Repair. Current osteoporosis reports, 21(6), 842–853. https://doi.org/10.1007/s11914-023-00824-4
Jiao, H., Xiao, E., & Graves, D. T. (2015). Diabetes and Its Effect on Bone and Fracture Healing. Current osteoporosis reports, 13(5), 327–335. https://doi.org/10.1007/s11914-015-0286-8
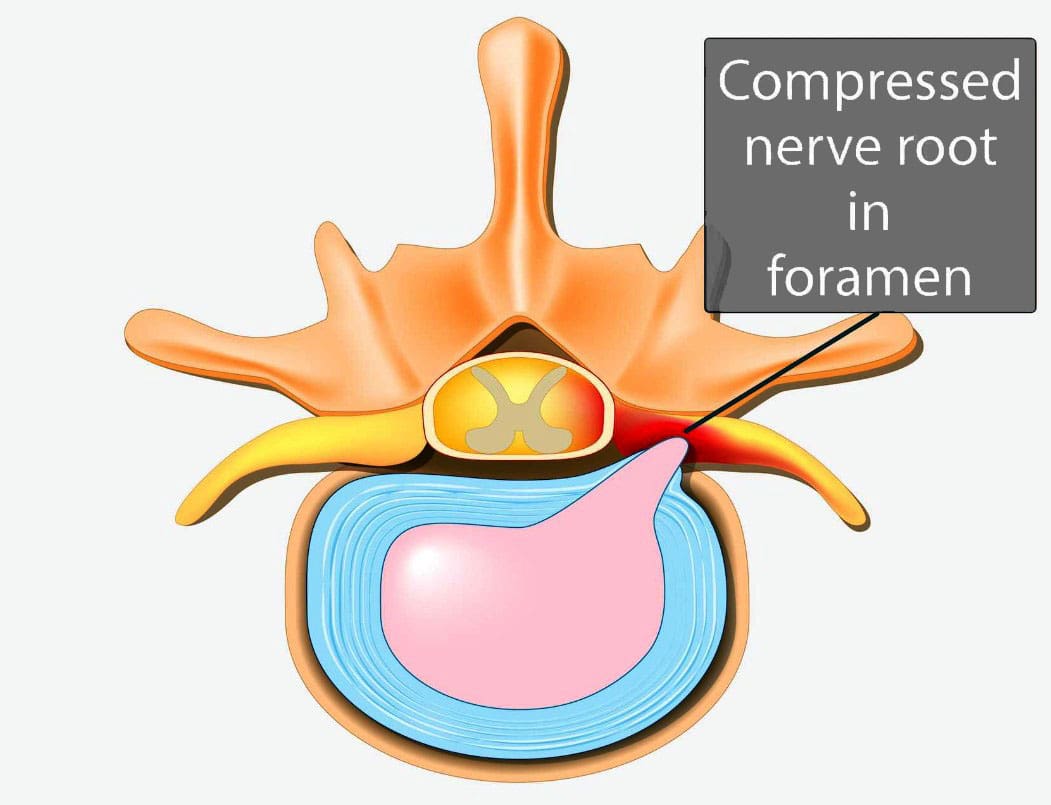
Individuals experiencing persistent pain, weakness, numbness, and tingling in the back could be suffering from nerve root encroachment. Could surgery ease nerve compression and improve symptoms for persistent and severe cases?
Surgical Decompression
The pain, weakness, numbness, and tingling associated with nerve root encroachment are usually first treated with non-surgical therapies that include:
Anti-inflammatory medications
Physical therapy
This can be enough to address the irritation of the spinal nerve root. But when cases become severe, surgical decompression may be recommended and necessary. It can be done in a couple of different ways.
Causes and Symptoms
Vertebrae are bones in the spine. Small openings called foramina allow a spinal nerve root to pass through on each side of the vertebra. When nerve root encroachment is present, the spinal nerve root gets compressed, pinched, and trapped, which can cause peripheral symptoms such as numbness, tingling, pain, or weakness to develop. Nerve root encroachment is typically caused by normal aging degenerative wear and tear changes in the vertebrae. (Choi Y. K. 2019) These degenerative changes can include:
Facet joint hypertrophy
Ligament and bone hypertrophy
Disc disorders
Formation of bone spurs or osteophytes.
If these degenerative changes progress, they can encroach and compress a nerve root, leading to peripheral symptoms. (Choi Y. K. 2019)
When Surgery Is Recommended
When symptoms occur, initial treatment will involve:
Physical therapy
Chiropractic realignment
Massage therapies
Rest
Lifestyle adjustments
Nonsteroidal anti-inflammatories – NSAIDs
Corticosteroid injections into the spine
If conservative therapies don’t fully heal or improve symptoms or there are neurological problems like difficulty with balance or walking, then surgery may be recommended. Severe pain that limits normal function is an indication for surgery, and rapidly progressive weakness of the arms and/or legs or signs of cauda equina syndrome are indications for emergency surgery.
Surgery Options
Different types of spinal surgery may be performed. A neurosurgeon will decide the best procedure for each patient based on their case, age, medical conditions, and other factors. Specific spinal surgical decompression depends on what is causing the nerve compression. In most cases, it involves removing bone or tissue to relieve nerve pressure or provide support to stabilize the joint. The most common types of surgical decompression include: (Mayo Clinic Health System, 2022)
Maintain the stability and alignment of the spine.
Improve the stability and alignment of the spine.
Anterior Surgery
The anterior approach to surgery means that the spine is accessed through the anterior/front of the spine. In this surgery, one or more discs and bone spurs may be removed through an incision in the front of the neck. (American Association of Neurological Surgeons, 2024) For example, an anterior cervical discectomy may alleviate pressure on one or more nerve roots in the neck. With an anterior lumbar interbody fusion, a surgeon removes a degenerative disc in the lower spinal area by going through a patient’s lower abdomen. (American Association of Neurological Surgeons, 2024) After the disc is removed, a structural device, usually made of bone, fills the space where it once was. This device encourages bone healing and helps the vertebrae’s bodies fuse.
Posterior Surgery
Posterior surgery means the spine is accessed through the posterior/back of the spine. An example is removing a thickened ligament, bone spur, or disc material in the neck. To do this, a small incision in the back of the neck may be made to remove part of the back of the vertebrae called the lamina. This is called a posterior cervical laminectomy. (American Association of Neurological Surgeons, 2024) A posterior lumbar interbody fusion removes a degenerative disc by going through the back. (American Association of Neurological Surgeons, 2024) Like the anterior approach, a structural device often contains bone to fill the space where the disc once was to fuse the bones.
Potential Risks
As with any surgery, it’s important that the individual and their healthcare provider carefully discuss the benefits and risks. Spinal surgical decompression includes: (Proietti L. et al., 2013)
Bleeding
Blood clots
Surgical site infection
Urinary tract infection
Lung infection
Intestinal blockage
There are also specific risks to the area of the spine being operated on and how it is surgically approached. For example, a cervical anterior procedure may injure the esophagus, trachea, or carotid artery. Likewise, damage to the C5 nerve root/C5 palsy can occur from cervical spinal decompressive surgery. This complication causes weakness, numbness, and pain in the shoulders. (Thompson S. E. et al., 2017) The spinal cord may also be injured during surgery and result in paralysis, although this is rare. (American Association of Neurological Surgeons, 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
The Non-Surgical Solution
References
Choi Y. K. (2019). Lumbar foraminal neuropathy: an update on non-surgical management. The Korean journal of pain, 32(3), 147–159. https://doi.org/10.3344/kjp.2019.32.3.147
Mayo Clinic Health System. (2022). Decompress and stabilize: understanding types of back surgery. Speaking of Health. https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/understanding-types-of-back-surgery
American Association of Neurological Surgeons. (2024). Cervical spine. https://www.aans.org/patients/conditions-treatments/cervical-spine/
American Association of Neurological Surgeons. (2024). Lumbar spinal stenosis. https://www.aans.org/patients/conditions-treatments/lumbar-spinal-stenosis/
Proietti, L., Scaramuzzo, L., Schiro’, G. R., Sessa, S., & Logroscino, C. A. (2013). Complications in lumbar spine surgery: A retrospective analysis. Indian journal of orthopaedics, 47(4), 340–345. https://doi.org/10.4103/0019-5413.114909
Thompson, S. E., Smith, Z. A., Hsu, W. K., Nassr, A., Mroz, T. E., Fish, D. E., Wang, J. C., Fehlings, M. G., Tannoury, C. A., Tannoury, T., Tortolani, P. J., Traynelis, V. C., Gokaslan, Z., Hilibrand, A. S., Isaacs, R. E., Mummaneni, P. V., Chou, D., Qureshi, S. A., Cho, S. K., Baird, E. O., … Riew, K. D. (2017). C5 Palsy After Cervical Spine Surgery: A Multicenter Retrospective Review of 59 Cases. Global spine journal, 7(1 Suppl), 64S–70S. https://doi.org/10.1177/2192568216688189
Can using a cane help individuals after an injury, living with chronic pain or balance issues, or post-surgery?
Walking With A Cane
A cane is an assistive device that can help individuals walk after injury or surgery and aids with balance and stability. It can be used for:
Balance or Stability Issues
Canes can help with minor balance or stability issues, such as weakness in the leg or trunk, or after an injury.
Pain
Canes can help reduce stress on painful joints or limbs.
Independence
Canes can help people continue living independently, especially the elderly.
There are different types of canes, including single-point and quad canes. Single-point canes are generally the least expensive. Quad canes have four points and can provide more stability. It is important to use it correctly to prevent falls and injuries.
Post-surgery or Injury
A cane can help reduce pressure on the leg or back after surgery or injury. Healthcare providers may recommend a cane as a step-down device after using a walker or crutches. Before walking with the cane, ensure it is at the right height. Hold the cane in the hand on the opposite side of the injury. Hold the cane’s handle at the level of the bend in the wrist when standing with the elbow slightly bent. (American Academy of Orthopaedic Surgeons, 2020) If there are issues in both legs or a cane is used after back surgery, keep the cane in the hand with the most support.
Step forward with the cane and injured leg at the same time.
Step the non-injured leg up with the cane firmly on the ground to meet the injured leg.
The feet should be side by side.
Walking Normally
Once comfortable taking practice steps, try walking normally with the cane. Step forward with the cane and injured leg simultaneously. The cane should be off the ground when the wounded leg is in the air. Firmly plant the cane when stepping onto the injured leg. Step forward with the cane and the injured leg first, then step past the injured leg with the good leg.
Step down with the injured leg while lowering the cane to the step below.
Make sure the cane is firmly on the stairs.
Bring the good leg down to the same step.
If a handrail is available, use it. Although doing so may require moving the cane to the other hand, even if it’s on the same side as the injured leg, it will improve stability and reduce the risk of falling. Once proficient on the stairs, individuals may alternate placing one foot on each step.
Walking With Chronic Pain
Walking with a cane with a chronic pain condition is similar to using it with an injury. The location of the pain will determine which hand the cane is held in. If the pain is on the right side of the body, keep the cane on the left side or vice versa. If chronic pain is not in the legs but, for example, back pain makes it difficult to walk, hold the cane on either side, whichever feels more supportive and comfortable. If there is weakness on one side of the body or decreased sensation/numbness in one of the legs or feet, hold the cane on the opposite side of the pain, weakness, or numbness. Walking with a cane can also benefit individuals with other medical conditions. For example, assistive devices may be recommended for those with balance issues. (National Library of Medicine, 2023)
Cane Types
There are two primary types of canes, characterized by their points, and choosing the right one depends on the reason it’s needed. (Arthritis Foundation, N.D.)
Single-point
Single-point canes have one tip at the end.
These are recommended for those who need to relieve some pressure off an injured leg or need support due to occasional difficulties with balance.
Quad
Quad canes have four tips or feet to provide more stability.
They provide more support and are recommended for those with significant weakness in one leg or difficulty maintaining their balance while walking.
The traditional cane has a rounded C handle. Other types have contoured handles for a more secure grip. Talk to a doctor, physical therapist, or other health care professional for suggestions on which cane is right for you.
Losing Balance
A potential risk of using a cane is losing balance. If unable to maintain balance with a cane, individuals may want to consider a different walking device, such as a walker or crutches. To reduce the risk of falls, consider the following tips (American Academy of Orthopaedic Surgeons, 2020)
Wear shoes with nonskid soles.
Add lighting so you can see where you are walking.
Remove throw rugs or objects that can cause tripping.
Arrange furniture to allow for wide walking paths throughout the home.
Carry objects in a backpack or fanny pack rather than holding them.
Injury Medical Chiropractic and Functional Medicine Clinic
Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other associated medical professionals to develop a personalized treatment plan to help relieve muscle pain, improve the body’s flexibility and mobility, resolve musculoskeletal issues, and prevent future pain symptoms from reoccurring.
Osteoporosis
References
American Academy of Orthopaedic Surgeons. (2020). How to use crutches, canes, and walkers. https://orthoinfo.aaos.org/en/recovery/how-to-use-crutches-canes-and-walkers/
Hirayama, K., Otaka, Y., Kurayama, T., Takahashi, T., Tomita, Y., Inoue, S., Honaga, K., Kondo, K., & Osu, R. (2022). Efficiency and Stability of Step-To Gait in Slow Walking. Frontiers in human neuroscience, 15, 779920. https://doi.org/10.3389/fnhum.2021.779920
National Library of Medicine. (2023). Using a cane. Retrieved from https://medlineplus.gov/ency/patientinstructions/000343.htm
Arthritis Foundation. (N.D.). How to choose the right cane. https://www.arthritis.org/health-wellness/healthy-living/managing-pain/joint-protection/how-to-choose-the-right-cane
Can learning about comminuted fracture symptoms and repair help individuals and healthcare providers develop effective treatment and rehabilitation programs?
Comminuted Fractures
A comminuted fracture is a severe break in which the bone splits into at least three pieces. Comminuted fractures typically happen in the long bones like those in the arms and legs. But they can also happen in other places, including the ribs. (Corinne Tarantino, 2022) They are usually caused by intense impact, like an automobile collision/accident or a severe fall. Depending on the location of the fracture, recovery from a comminuted fracture can take months and often involves:
Surgery – A surgeon will place screws and rods to hold the pieces of the bone in position. Sometimes, the hardware is left in permanently. (American Academy of Orthopaedic Surgeons, 2021)
Wearing a cast for several months.
Physical therapy.
Types
In these types of fractures, the bone is completely broken, not just cracked. The break is a highly comminuted fracture if the bone is broken into four or more pieces. (Corinne Tarantino, 2022)
Symptoms
The symptoms are the same as those of other broken bones, but they can be more intense because the bone is broken in multiple areas, which means there may also be more soft tissue injuries than with a simple fracture. Broken bone symptoms include: (MedlinePlus, 2024)
Persistent pain
Swelling
Bruising
Deformity – the bone looks out of place or is at an odd angle.
Tingling
Numbness
Difficulty moving the limb.
Causes
An intense force causes a comminuted fracture, often a car accident or a hard fall, but it can also result from sports injuries. (Corinne Tarantino, 2022)
Diagnosis
A comminuted fracture is diagnosed by X-ray, which shows where the bone has broken and how many pieces it has split into (MedlinePlus, 2024). Healthcare providers will diagnose any broken bones but also look for other injuries.
Treatment
Typically, broken bones can be treated with casts, braces, or a boot to keep them immobilized. (MedlinePlus, 2024) Because comminuted fractures are more severe, they often need other treatments, including surgery. Sometimes, the bone can be reset instead of surgery using a closed reduction technique, where the healthcare provider resets the bone manually. Surgery may be recommended if that’s not possible or doesn’t work.
Types of Surgery
Surgery allows the healthcare provider to correctly position all the pieces of the bone to heal in a strong, stable formation. The two types commonly used to treat comminuted fractures are: (American Academy of Orthopaedic Surgeons, 2021)
External Fixation
This surgery uses rods and screws outside the body to stabilize the bone.
This external frame is placed during surgery and later removed.
Open Reduction Internal Fixation – ORIF
During this surgery, the bone is stabilized with metal plates, screws, rods, and/or wires placed inside your body.
Sometimes, these are permanent, but in other cases, they are removed later.
An orthopedic surgeon performs these surgeries.
Casting
After surgery, a cast is usually needed to prevent the bone from moving and allow healing. Typically, the cast is worn for six to eight weeks, but it may need to be worn longer with comminuted fractures. Some need a cast for several months (American Academy of Orthopaedic Surgeons, 2021). Sometimes, those with an external fixation must continue wearing a cast after removing the pins and rods, giving the bone more time to stabilize. The healthcare provider will inform the patient how long the cast will need to be worn and which sports activities should be avoided even after the cast comes off.
Physical Therapy
The healthcare provider may recommend physical therapy to help treat the fracture. Usually, when the cast is removed, physical therapy is activated to help rebuild strength and range of motion. (Corinne Tarantino, 2022)
Prognosis
Although these fractures are severe, they are treatable. The prognosis is good for individuals who follow their healthcare provider’s treatment plan. Most don’t have lingering pain after the initial injury and can eventually return to regular activities. (American Academy of Orthopaedic Surgeons, 2021)
Recovery
Healing a comminuted fracture can take months. During that time, it’s helpful to focus on tasks that can be accomplished, like new hobbies that don’t involve physical injury. Talk to the healthcare provider about any problems with the cast or ongoing pain and what to expect during recovery.
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility programs to relieve pain and help individuals return to normal. Our providers create personalized care plans for each patient. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
The Path to Healing Personal Injury
References
Corinne Tarantino, MPH. Osmosis. (2022). Comminuted Fracture: What is it, Examples and More. https://www.osmosis.org/answers/comminuted-fracture
Throckmorton T.W. American Academy of Orthopaedic Surgeons. (2021). Fractures (broken bones). https://orthoinfo.aaos.org/en/diseases–conditions/fractures-broken-bones/
MedlinePlus. National Library of Medicine. (2024). Fractures Also called: Broken bone. Retrieved from https://medlineplus.gov/fractures.html
For individuals who have exhausted all other treatment options for low back pain and nerve root compression, can laser spine surgery help alleviate nerve compression and provide long-lasting pain relief?
Laser Spine Surgery
Laser spine surgery is a minimally invasive surgical procedure that uses a laser to cut through and remove spinal structures that are compressing nerves and causing intense pain. The minimally invasive procedure often results in less pain, tissue damage, and faster recovery than more extensive surgeries.
How It Works
Minimally invasive procedures result in less scarring and damage to surrounding structures, often reducing pain symptoms and a shorter recovery time. (Stern, J. 2009) Small incisions are made to access spinal column structures. With open-back surgery, a large incision is made down the back to access the spine. The surgery differs from other surgeries in that a laser beam, rather than other surgical instruments, is used to cut structures in the spine. However, the initial incision through the skin is made with a surgical scalpel. Laser is an acronym for Light Amplification Stimulated by Emission of Radiation. A laser can generate intense heat to cut through soft tissues, especially those with a high water content, like spinal column discs. (Stern, J. 2009) For many spine surgeries, the laser cannot be used to cut through bone as it generates instant sparks that can damage surrounding structures. Rather, laser spine surgery is primarily used to perform a discectomy, which is a surgical technique that removes a portion of a bulging or herniated disc that is pushing against the surrounding nerve roots, causing nerve compression and sciatic pain. (Stern, J. 2009)
Surgical Risks
Laser spine surgery may help resolve the cause of nerve root compression, but there is an increased risk of damage to nearby structures. Associated risks include: (Brouwer, P. A. et al., 2015)
Infection
Bleeding
Blood clots
Remaining symptoms
Returning symptoms
Further nerve damage
Damage to the membrane around the spinal cord.
Need for additional surgery
A laser beam is not precise like other surgical tools and requires practiced mastery and control to avoid damage to the spinal cord and nerve roots. (Stern, J. 2009) Because lasers cannot cut through bone, other surgical instruments are often used around corners and at different angles because they are more efficient and allow greater accuracy. (Atlantic Brain and Spine, 2022)
Purpose
Laser spine surgery is performed to remove structures that are causing nerve root compression. Nerve root compression is associated with the following conditions (Cleveland Clinic. 2018)
Bulging discs
Herniated discs
Sciatica
Spinal stenosis
Spinal cord tumors
Nerve roots that are injured or damaged and constantly send chronic pain signals can be ablated with laser surgery, known as nerve ablation. The laser burns and destroys the nerve fibers. (Stern, J. 2009) Because laser spine surgery is limited in treating certain spinal disorders, most minimally invasive spine procedures do not use a laser. (Atlantic Brain and Spine. 2022)
Preparation
The surgical team will provide more detailed instructions on what to do in the days and hours before surgery. To promote optimal healing and a smooth recovery, it is recommended that the patient stay active, eat a healthy diet, and stop smoking prior to the operation. Individuals may need to stop taking certain medications to prevent excess bleeding or interaction with anesthesia during the operation. Inform the healthcare provider about all prescriptions, over-the-counter drugs, and supplements being taken.
Laser spine surgery is an outpatient procedure at a hospital or outpatient surgical center. The patient will likely go home on the same day of the operation. (Cleveland Clinic. 2018) Patients cannot drive to or from the hospital before or after their surgery, so arrange for family or friends to provide transportation. Minimizing stress and prioritizing healthy mental and emotional well-being is important to lowering inflammation and aiding recovery. The healthier the patient goes into surgery, the easier the recovery and rehabilitation will be.
Expectations
The surgery will be decided by the patient and healthcare provider and scheduled at a hospital or outpatient surgical center. Arrange for a friend or family member to drive to the surgery and home.
Before Surgery
The patient will be taken to a pre-operative room and asked to change into a gown.
The patient will undergo a brief physical examination and answer questions about medical history.
The patient lies on a hospital bed, and a nurse inserts an IV to deliver medication and fluids.
The surgical team will use the hospital bed to transport the patient in and out of the operating room.
The surgical team will assist the patient in getting onto the operating table, and the patient will be administered anesthesia.
The patient may receive general anesthesia, which will cause the patient to sleep for the surgery, or regional anesthesia, injected into the spine to numb the affected area. (Cleveland Clinic. 2018)
The surgical team will sterilize the skin where the incision will be made.
An antiseptic solution will be used to kill bacteria and prevent the risk of infection.
Once sanitized, the body will be covered with sterilized linens to keep the surgical site clean.
During Surgery
For a discectomy, the surgeon will make a small incision less than one inch in length with a scalpel along the spine to access the nerve roots.
A surgical tool called an endoscope is a camera inserted into the incision to view the spine. (Brouwer, P. A. et al., 2015)
Once the problematic disc portion causing the compression is located, the laser is inserted to cut through it.
The cut disc portion is removed, and the incision site is sutured.
After Surgery
After surgery, the patient is brought to a recovery room, where vital signs are monitored as the effects of the anesthesia wear off.
Once stabilized, the patient can usually go home one or two hours after the operation.
The surgeon will determine when the individual is clear to resume driving.
Recovery
Following a discectomy, the individual can return to work within a few days to a few weeks, depending on the severity, but it can take up to three months to return to normal activities. Length of recovery can range from two to four weeks or less to resume a sedentary job or eight to 12 weeks for a more physically demanding job that requires heavy lifting. (University of Wisconsin School of Medicine and Public Health, 2021) During the first two weeks, the patient will be given restrictions to facilitate the spine’s healing until it becomes more stable. Restrictions can include: (University of Wisconsin School of Medicine and Public Health, 2021)
No bending, twisting, or lifting.
No strenuous physical activity, including exercise, housework, yard work, and sex.
No alcohol in the initial stage of recovery or while taking narcotic pain medications.
No driving or operating a motor vehicle until discussed with the surgeon.
The healthcare provider may recommend physical therapy to relax, strengthen, and maintain musculoskeletal health. Physical therapy may be two to three times weekly for four to six weeks.
Process
Optimal recovery recommendations include:
Getting enough sleep, at least seven to eight hours.
Maintaining a positive attitude and learning how to cope and manage stress.
Maintaining body hydration.
Following the exercise program as prescribed by the physical therapist.
Practicing healthy posture with sitting, standing, walking, and sleeping.
Staying active and limiting the amount of time spent sitting. Try to get up and walk every one to two hours during the day to stay active and prevent blood clots. Gradually increase the amount of time or distance as recovery progresses.
Do not push to do too much too soon. Overexertion can increase pain and delay recovery.
Learning correct lifting techniques to utilize the core and leg muscles to prevent increased pressure on the spine.
Discuss treatment options for managing symptoms with a healthcare provider or specialist to determine if laser spine surgery is appropriate. Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers. We focus on restoring normal body functions after trauma and soft tissue injuries using Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
The Non-Surgical Approach
References
Stern, J. SpineLine. (2009). Lasers in Spine Surgery: A Review. Current Concepts, 17-23. https://www.spine.org/Portals/0/assets/downloads/KnowYourBack/LaserSurgery.pdf
Brouwer, P. A., Brand, R., van den Akker-van Marle, M. E., Jacobs, W. C., Schenk, B., van den Berg-Huijsmans, A. A., Koes, B. W., van Buchem, M. A., Arts, M. P., & Peul, W. C. (2015). Percutaneous laser disc decompression versus conventional microdiscectomy in sciatica: a randomized controlled trial. The spine journal : official journal of the North American Spine Society, 15(5), 857–865. https://doi.org/10.1016/j.spinee.2015.01.020
Atlantic Brain and Spine. (2022). The Truth About Laser Spine Surgery [2022 Update]. Atlantic Brain and Spine Blog. https://www.brainspinesurgery.com/blog/the-truth-about-laser-spine-surgery-2022-update?rq=Laser%20Spine%20Surgery
Cleveland Clinic. (2018). Can Laser Spine Surgery Fix Your Back Pain? https://health.clevelandclinic.org/can-laser-spine-surgery-fix-your-back-pain/
University of Wisconsin School of Medicine and Public Health. (2021). Home Care Instructions after Lumbar Laminectomy, Decompression or Discectomy Surgery. https://patient.uwhealth.org/healthfacts/4466
For individuals experiencing back pain from a herniated disc, can understanding the difference between surgery and chiropractic help individuals find the right treatment plan?
Surgery or Chiropractic
Living with back pain can be a nightmare, and yet many struggle without seeking care. Today, there are a vast number of surgeries and noninvasive techniques that are better at treating spine and back problems and managing symptoms. For individuals who may have a herniated disc or are curious about ways to relieve their back pain, a health care provider, physical therapist, spine specialist, and chiropractor can inform them of treatment options. Surgery and chiropractic therapy are popular treatments for a herniated, bulging, or slipped disc.
A herniated disc is when the cartilage discs that cushion the vertebrae shift out of position and leak out.
Surgery for a herniated disc involves removing or repairing the disc.
Chiropractic nonsurgically repositions the disc and realigns the spine.
Both treatments have the same goals with key differences.
Chiropractic Care
Chiropractic is a system of therapy that focuses on adjusting and maintaining spinal alignment to help with back and posture problems. Chiropractors are trained and licensed medical professionals who take a nonsurgical approach, a proven therapy for chronic pain, flexibility, and mobility issues.
The Way It Works
Chiropractic treatment encourages and supports the body’s natural healing processes. It is considered for joint pain in the back, neck, legs, arms, feet, and hands. It typically involves sessions in which the chiropractor physically and carefully adjusts the vertebrae by hand, also known as spinal manipulation or chiropractic adjustments. (MedlinePlus. 2023). A chiropractor performs a thorough medical evaluation and runs tests to establish a diagnosis. A chiropractor will develop a treatment plan that may involve a team of massage and physical therapists, acupuncturists, health coaches, and nutritionists to treat affected areas with various techniques, recommend targeted exercises, adjust lifestyle and nutrition to support the treatment, and monitor progress. Combined with stretching and sustained pressure, the multiple methods can increase joint mobility and relieve pain symptoms. (National Center for Complimentary and Integrative Health. 2019) Added protocols to support or enhance chiropractic therapy include:
Heating and ice therapies to reduce inflammation and increase blood circulation.
Using devices to stimulate muscles and nerves electrically.
Developing relaxation and deep breathing techniques.
Incorporating exercises to promote rehabilitation.
Establishing a regular fitness routine.
Making adjustments to diet and lifestyle.
Taking certain dietary supplements.
Spinal manipulation and chiropractic adjustments have been shown to improve symptoms and restore mobility in cases of chronic back pain. One review found that individuals with chronic lumbar/low back pain reported significant improvement after six weeks of chiropractic treatment. (Ian D. Coulter et al., 2018)
Prices
The out-of-pocket expenses of chiropractic treatment depend on a variety of factors.
Insurance may or may not cover the treatment, and the amount an individual has to pay can vary based on the severity of their case, what their plan covers, and where they live. One review found the cost can range between $264 and $6,171. (Simon Dagenais et al., 2015)
Surgery
There is a range of minimally invasive surgical procedures to treat herniated discs. These work to ease nerve compression by removing or replacing damaged discs or stabilizing the vertebrae, relieving pain and inflammation.
The Way It Works
A herniated disc can happen in any part of the spine but is more common in the lower back/lumbar spine and in the neck/cervical spine. Surgery is recommended when: (American Academy of Orthopaedic Surgeons. 2022)
More conservative treatments, like medications and physical therapy, are unable to manage symptoms.
The pain and symptoms impact daily life and functioning.
Standing or walking becomes difficult or impossible.
The herniated disc causes difficulty walking, muscle weakness, and bladder or bowel control loss.
The individual is reasonably healthy, without infection, osteoporosis, or arthritis.
Specific surgical procedures used include:
Fusion Surgery
Spinal fusion is the most common procedure for a lower back herniated disc.
It involves using artificial bone material to fuse vertebrae to increase stability and release and prevent nerve irritation and compression. (American Academy of Neurological Surgeons. 2024)
Laminotomy and Laminectomy
Herniated disc symptoms appear from compression placed on the nerves.
Laminotomy involves making a small cut in the lamina, or the arch of the spinal vertebrae, to release the pressure.
Another approach involves implanting an artificial disc.
This is most often used for hernia in the lower spine; the worn or damaged disc is removed, and a specialized prosthetic replaces the removed disc. (American Academy of Orthopaedic Surgeons. 2022)
This allows for more mobility.
The success of herniated disc surgery depends on different factors. Advances in minimally invasive techniques have significantly improved long-term outcomes, with one review finding that around 80% reported good—excellent results at a six-year follow-up. (George J. Dohrmann, Nassir Mansour 2015) However, there is the possibility of recurrence. About 20% to 25% of individuals with herniated lumbar discs experience re-herniation at some point. (American Academy of Neurological Surgeons. 2024)
Prices
Surgery for a herniated disc is specialized, and the costs depend on the scope and scale of the treatment.
The individual’s specific insurance plan also determines the expenses.
When choosing between chiropractic and surgery for a herniated disc, a number of factors can determine the decision, including:
Chiropractic is the less invasive nonsurgical option.
Chiropractic adjustments cannot help certain severe cases of herniated discs.
Chiropractic adjustments prevent the herniated disc from getting worse and ease symptoms.
Surgery provides pain and symptom relief faster than chiropractic or conservative treatment but requires significant recovery time and is expensive. (Anna N A Tosteson et al., 2008)
Surgery may not be appropriate for individuals with osteoarthritis or osteoporosis.
Chiropractic therapy is among the more conservative treatment options for a herniated disc and may be tried first before proceeding with surgery. Generally, surgery is only recommended when noninvasive methods haven’t been able to stop or manage the pain and symptoms. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution that fully benefits the individual to get back to normal.
Quick Patient Process
References
MedlinePlus.MedlinePlus. (2023). Chiropractic. Retrieved from https://medlineplus.gov/chiropractic.html
National Center for Complimentary and Integrative Health. (2019). Chiropractic: in depth. Retrieved from https://www.nccih.nih.gov/health/chiropractic-in-depth
Coulter, I. D., Crawford, C., Hurwitz, E. L., Vernon, H., Khorsan, R., Suttorp Booth, M., & Herman, P. M. (2018). Manipulation and mobilization for treating chronic low back pain: a systematic review and meta-analysis. The spine journal : official journal of the North American Spine Society, 18(5), 866–879. https://doi.org/10.1016/j.spinee.2018.01.013
Dagenais, S., Brady, O., Haldeman, S., & Manga, P. (2015). A systematic review comparing the costs of chiropractic care to other interventions for spine pain in the United States. BMC health services research, 15, 474. https://doi.org/10.1186/s12913-015-1140-5
American Academy of Orthopaedic Surgeons. (2022). Herniated disk in the lower back. https://orthoinfo.aaos.org/en/diseases–conditions/herniated-disk-in-the-lower-back/
American Academy of Neurological Surgeons. Surgeons, A. A. o. N. (2024). Herniated disc. https://www.aans.org/en/Patients/Neurosurgical-Conditions-and-Treatments/Herniated-Disc
Dohrmann, G. J., & Mansour, N. (2015). Long-Term Results of Various Operations for Lumbar Disc Herniation: Analysis of over 39,000 Patients. Medical principles and practice : international journal of the Kuwait University, Health Science Centre, 24(3), 285–290. https://doi.org/10.1159/000375499
Tosteson, A. N., Skinner, J. S., Tosteson, T. D., Lurie, J. D., Andersson, G. B., Berven, S., Grove, M. R., Hanscom, B., Blood, E. A., & Weinstein, J. N. (2008). The cost effectiveness of surgical versus nonoperative treatment for lumbar disc herniation over two years: evidence from the Spine Patient Outcomes Research Trial (SPORT). Spine, 33(19), 2108–2115. https://doi.org/10.1097/brs.0b013e318182e390
Progress can be challenging for individuals in post total ankle replacement surgery. How can physical therapy help in recovery and restoring leg function?
Total Ankle Replacement Post Surgery Physical Therapy
Total ankle replacement surgery is a major procedure that takes time to recover. A total ankle replacement surgery or arthroplasty can benefit individuals with chronic ankle pain or disability. This procedure can significantly improve an individual’s overall pain and function with time. Physical therapy is essential to regaining movement in the ankle and restoring full mobility. A physical therapist will work with the individual to control pain and swelling, restore the ankle’s range of motion, train on walking gait and balance, and rebuild strength in the leg. This will help maximize the chances of a successful outcome after surgery.
Total Ankle Replacement
The ankle joint is the section of the lower leg where the shinbone/tibia meets the talus bone on the top of the foot. What can happen is the slippery surface/articular cartilage that coats the ends of these bones begins to thin or deteriorate. As the deterioration progresses, it can lead to significant pain, disability, and difficulty walking. (Cleveland Clinic. 2021) This is where a specialist may recommend total ankle replacement for the best results. Various conditions can be helped by this procedure, including:
During an ankle replacement procedure, an orthopedic surgeon removes the damaged ends of the tibia and talus bones and replaces them with an artificial covering. A polyethylene component is also secured between the two structures to support the smooth movement of the new joint endings. (Massachusetts General Hospital. N.D.) Following the procedure, individuals are typically placed in a protective boot or splint. The healthcare provider will recommend staying off the leg for 4 to 8 weeks to allow healing.
Physical Therapy
Outpatient physical therapy is usually initiated several weeks after the ankle operation. (UW Health Orthopedics and Rehabilitation. 2018) Physical therapy can last for five months or more, depending on the severity of the condition and injury. The physical therapist will focus on different areas to get the best results. (Cort D. Lawton et al., 2017)
Pain and Swelling Control
Post-operative pain and swelling are normal after a total ankle replacement. It is not unusual for an ankle to be swollen for even six to 12 months after the operation. (UW Health Orthopedics and Rehabilitation. 2018) The surgeon will normally prescribe medication to help manage discomfort early on, and physical therapy also plays an important role in addressing the symptoms. Treatments used can include:
Electrical stimulation – mild electrical pulses applied to the muscles.
Ice
Vasopneumatic compression, where an inflatable sleeve is used to create pressure around the area, is commonly utilized at the beginning of physical therapy to reduce pain or swelling.
Other modalities, such as stretching and targeted exercises, are combined with other treatments.
Range of Motion
Early after the procedure, the ankle will be very stiff and tight. This is due to several factors, including the inflammation and swelling after surgery and the time spent immobilized in a boot.
The physical therapist will employ various techniques to improve the ankle joint’s range of motion to rotate and flex.
The physical therapist may employ passive stretching induced by an outside force such as the therapist or a resistance band) to help improve mobility.
After multiple weeks of reduced movement and lack of bearing any weight on the ankle, the muscles that surround the ankle have often atrophied/weakened, which can impact balance.
When the individual can begin placing weight on the leg, the therapist will apply proprioceptive/sense of body position training to improve overall stability. (UW Health Orthopedics and Rehabilitation. 2018)
Balance exercises will be added to the home program and will progress from week to week.
Strength
The muscles in the leg, ankle, and foot become weak from the surgery and the time spent in a splint or boot. These structures have a significant role in balance, the ability to stand, walk, and go up or down the stairs.
Regaining the strength and power of these muscles is a critical goal of rehabilitation.
In the first weeks, the physical therapist will focus on gentle strengthening exercises.
Isometrics lightly activate the muscles but avoid irritating the surgical site.
As time passes and weight-bearing is allowed, these gentle moves are replaced with more challenging ones, like resistance bands and standing exercises, to accelerate strength gains.
Lawton, C. D., Butler, B. A., Dekker, R. G., 2nd, Prescott, A., & Kadakia, A. R. (2017). Total ankle arthroplasty versus ankle arthrodesis-a comparison of outcomes over the last decade. Journal of orthopaedic surgery and research, 12(1), 76. https://doi.org/10.1186/s13018-017-0576-1
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine