Dr. Alex Jimenez Discusses Exercise and Methylation
A personalized, moderate exercise plan can promote methylation support. According to research studies, exercise can affect metabolic methylation-related activity and biomarkers. According to a 2014 systematic review, exercise is associated with lower homocysteine levels. In animal models, exercise has been demonstrated to prevent folate deficiency-induced hyperhomocysteinemia through increased BHMT expression in the kidney.
However, several research studies have also demonstrated that exercise can cause a temporary increase in plasma homocysteine, especially in untrained people, which is believed to be due to the increased proteins during exercise to make amino acids available for gluconeogenesis in the liver. This effect can also be triggered by low folate and vitamin B12 status, which is why nutrient repletion is essential for overall health and wellness.
Regular and moderate exercise is an effective treatment for factors which can decrease methyl donors or affect methylation activity, such as psychological stress, oxidative stress, and inflammation. Aerobic exercise and resistance training have also been associated with increased cellular glucose uptake and reduced blood glucose, which can also reduce oxidative stress caused by higher AGE-promoting glucose levels, among other factors.
How Exercise Improves DNA Methylation
The increased production of reactive oxygen species and free radicals during exercise as well as the increased levels of pro-inflammatory cytokines has been demonstrated in a variety of research studies. However, the effects of these changes can depend on a person’s nutrition and lifestyle habits. High-intensity or anaerobic exercise may have pro-oxidative effects, especially in untrained individuals. Endurance exercise, by way of instance, may produce circulating levels of IL-6, up to 120 times that of baseline, as well as increases in other predominantly pro-inflammatory cytokines.
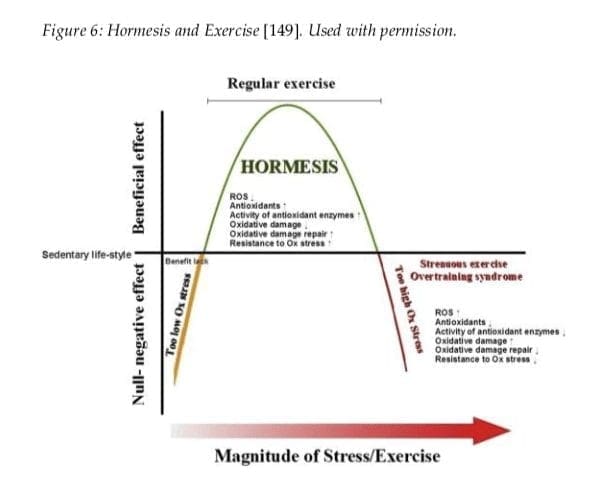
A 2013 systematic review demonstrated the effect of exercise on oxidative stress in the brain. The outcome measures determined that regular, moderate, aerobic exercise increase the brain�s antioxidant capacity, however, high-intensity, anaerobic exercise decreased the antioxidant response. The results can be explained by a hormesis model of exercise (Figure 6), which discusses that low or high levels of exercise can produce negative effects. The gradual build-up of exercise, through regular practice or training, can change the hormesis curve to the right, meaning that exercise tolerance and benefits are highly personalized for each person.
Recent research studies have discussed that antioxidants provided by a diet rich in natural plant phytochemicals, such as vegetables, fruits, whole grains, legumes and beans, sprouts and seeds, are also an effective way to meet the antioxidant needs of the general population and athletes who participate in exercise, physical activities, and/or sports. As a matter of fact, dietary intervention is a much safer and effective treatment than antioxidant supplementation because research studies utilizing supplementation demonstrated insufficient and mixed results. Several researchers even believe that antioxidant supplementation can affect the beneficial hormetic effects of exercise, ultimately affecting well-being.
Exercise can ultimately affect DNA methylation, according to a recent review of literature. By way of instance, in a retrospective research study of 647 women, regular exercise throughout their lifetimes helped preserve the age-related depletion of global methylation status, where exercise and physical activity like sports and daily movement, such as climbing stairs, housework, and yardwork, which was greater than or equal to the average in childhood, adolescence, and adulthood, did have a small yet considerable increase in global DNA methylation compared with participants who did not meet that level of exercise or physical activity in all three life stages.
Women who engaged in exercise or physical activity at or above the average in only one or two of those life stages also demonstrated increased DNA methylation, however, statistical importance was lost. The average level of exercise was determined at 9.8 hours per week in childhood, 5.9 hours per week in teenage years, and 12.5 hours per week in adulthood. Further research studies may be used to gather further outcome measures.
In a separate case-control research study of 500 females, long-term, tai-chi participants of at least one hour per week for 3 years or more, demonstrated a slowing of age-related DNA methylation losses, from 5 to 70 percent, compared with controls. During their research study, the researchers determined a considerable difference in methylation between the two groups at a number of specific sites which only occurred after 50 to 55 years of age, leading them to believe that tai-chi may be of particular benefit in this age-group. Further research studies are still required.
Although the effects of exercise on DNA methylation are not well understood, research studies have demonstrated that this may actually be true due to the inflammation-lowering effects of exercise and physical activity through changes in sex hormone levels that can affect DNA methylation. Mind-body exercises, such as tai-chi, may also be beneficial due to their effects on stress hormone levels and stress responsiveness.
Nutrition and lifestyle habits, such as exercise and physical activity, can help improve DNA methylation. Regardless of your age, research studies have demonstrated that participating in exercise, sports, or any other physical activity can enhance your overall health and wellness. Recent research studies have also determined that proper nutrition and lifestyle habits can improve methylation, a fundamental process of the human body involved in a variety of functions.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many healthcare professionals can recommend a variety of treatment options to help improve DNA methylation. Proper nutrition and lifestyle habits, such as exercise and physical activity, can ultimately help improve DNA methylation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Water is good for you. This is the message that we hear over and over, as we pursue optimal health, strive to lose weight, or overcome chronic conditions. Water is a vital part of life.
The problem is, every �expert� has an opinion of what is the best way to get this life substance. There are different messages about what is the best water source � what�s healthy, what isn�t. To cut through all the hype and get to the truth the answer isn�t as cut and dry as you might think.
Hydration Importance
Water is essential for our very survival. It keeps the functions of our organs properly, is a vital component of digestion, and it even helps us have a healthy spine. It helps to regulate body temperature and lubricates the joints. You may not realize it, but�most of your body is composed of water:
Lungs � 83%
Kidneys and muscles � 79%
Heart and brain � 73%
Skin � 64%
Bones � 31%
The average adult female requires around 2.2 liters of water per day, while the average adult male requires around 3 liters. Most of this comes from drinking fluids, but some come from food that is consumed. Dehydration is a serious condition and can cause serious damage to the body. Severe and prolonged (about 3 days) dehydration can be deadly.
Bottled Water Facts
There has been a lot of debate about bottled water in the past few years. At the center of the controversy are two main issues: much of the bottled water is said to be nothing more than tap water, and in the US alone, more than 60 million water bottles find their way to landfills every single day. Those are some pretty serious issues.
The truth is, studies show that almost half (around 40%) of bottled water is just tap water. So, what�s the big deal about tap water? It is largely known to contain chemicals that are not only toxic to humans, but many are also linked to certain cancers. Chlorine, arsenic, and fluoride are some of the more common chemicals found in tap water. Things aren�t looking good for tap water, but if so much bottled water is tap, then what can you do?
The Bottles
Before we explore the safer water options, it is worth taking a look at the plastic bottles that are used. The materials used to make water bottles are widely known to contain deadly, cancer-causing carcinogens like Bisphenol A (BPA), polyethylene terephthalate (PET), and phthalates. Each of these poses significant risks to your health.
Even if you choose a bottle that is BPA free (like PET bottles) you could be exposing yourself to other hazardous substances. For instance, PET bottles are made of a soft plastic that is extremely difficult, if not impossible, to clean. This can leave some unsavory residue like food, saliva, and even fecal matter to contaminate your water. The more the bottles are reused, the greater the risk of these and other contaminants making their way into your water.
Healthier Alternative To Bottled Water
Actually, tap water is the safer, healthier alternative to bottled water � but not straight out of the tap. All tap water should be run through a high-quality water filtration system before you use it. Without filtration, you run the risk of consuming contaminants like harmful chemicals, bacteria, and even heavy metals. So, what should you do?
Ditch the plastic bottles and choose glass or stainless steel instead. Next, filter your tap water using a high-quality carbon filter. Store your water in a ceramic or glass container. Do not heat or cook food or water in anything made of plastic or Styrofoam. In fact, avoid drinking or eating from plastic altogether. If you must though, do not cut into the plastic while you are eating or drinking and do not expose the food or water to a microwave, high heat, or the sun.
Drink your water, but make sure you are doing it in the healthiest way possible � on tap and filtered!
According to research studies, stress management can promote methylation support. High levels psychological and physiological stress can increase the production of the catecholamines epinephrine and norepinephrine, both of which depend on methylation for their biosynthesis, metabolism, and excretion. DNA methylation activity utilizes SAMe and it can lower the availability of this methyl donor for other processes. Stress management is, therefore, a fundamental treatment option to promote methylation support.
Stress can also affect DNA methylation status through different mechanisms rather than through the utilization of methyl donors. Although a variety of research studies have been conducted regarding the effects of stress on methylation, our understanding of the complex association between stress management and methylation support is still tremendously limited. Methylation of the promoter genes for glucocorticoid, an essential regulator of the HPA axis and stress response, has been demonstrated to be affected differently through various states of stress, including early-life stress, post-traumatic stress disorder, or PTSD, and chronic fatigue syndrome.
How Stress Affects Methylation
We do understand, however, that stress-mediated epigenetic “priming” through methylation during fundamental developmental stages has been associated with a variety of health issues. By way of instance, and as we’ve previously discussed, low levels of maternal nurturing can affect DNA methylation status in the glucocorticoid receptor promoter and gene expression. This ultimately suggests that traumatic experiences, especially during essential stages of development, may “prime” high levels of stress. Several researchers believe that the connection between stress and methylation may explain the association of health issues, such as asthma.
Furthermore, research studies determined that prenatal maternal stress, as evaluated after the January 1998 Quebec ice storm, correlates with increased central adiposity and BMI in offspring at age 13 1?2. These changes are regulated through DNA methylation. Traumatic childhood experiences, including maltreatment, and parental death or desertion, outside of the prenatal and perinatal stages of development can also affect methylation of the promoter genes for glucocorticoid, associated with increased cortisol production.
Research studies have also demonstrated that acute and chronic stress can increase circulating inflammatory factors, including IL-1?, CRP, and IL-6, which are commonly regulated through the NLRP3 inflammasome. This may be a considerable way in which stress affects epigenetic changes. The effects of inflammation on DNA methylation status and activity have been discussed in previous articles. Doctors and functional medicine practitioners can recommend stress management techniques for methylation support.
Stress is a natural response to any type of demand or threat, it is the human body’s way of protecting you. However, chronic stress can cause a variety of health issues and recent research studies have demonstrated that stress can even affect an individual’s DNA methylation status. Doctor and functional medicine practitioners can recommend several stress management techniques, whether through nutrition and/or lifestyle modifications, to help promote methylation support. According to the article above, stress can affect methylation in several ways.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many healthcare professionals can recommend a variety of treatment options to help with stress management and help prevent health issues associated with DNA methylation. Proper nutrition and lifestyle habits, can improve methylation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
People from all walks of life can have hormonal imbalances and don�t realize it. Medical tests for abnormal thyroid function don�t always pick up on a thyroid that isn’t working correctly.
Adrenals have the same issues. When overworked, the hormonal imbalance that follows can become a nightmare. Fortunately, there are excellent natural remedies for hormonal imbalance.
Hormones Not Balanced
Glands that are under-producing will have some symptoms that are different from glands that are over-producing. However, some symptoms are shared across the board. If you notice that you experience several of these symptoms, it could point to a hormonal imbalance:
Weight loss or gain (without trying or doing anything different)
Swelling
Confusion, difficulty finding the �right� word, lack of mental clarity
Your chiropractor, naturopath, or specialist can help you determine if you have a hormonal imbalance. Many medical doctors tend to prescribe medications, but in most cases, the problem can be corrected through natural means. These three treatments are very beneficial in treating hormonal imbalances in the body. They can be done separately or combined for added benefits.
Herbs and Essential Oils
There are several herbs and essential oils that are exceptional when it comes to balancing hormones. Ashwagandha tops the list for treating overactive or sluggish thyroid as well as overtaxed adrenals. You can take it as a tablet or capsule, in powder form, or as a liquid. Mixing � to � teaspoons of powder into some milk with honey and taking just before bedtime can help you sleep as well as calm your stress and balance your hormones.
Several essential oils like clary sage, lavender, and sandalwood help reduce stress and promote a sense of wellbeing. Hormonal balance is a natural result. To use essential oils, put 3 to 5 drops in a diffuser and breathe it in.
Nutrition Balances Hormones
Hormonal imbalance is often the result of stress, whether it is emotional stress from difficulties in life or physical stress from poor health habits like not getting enough sleep and not maintaining a healthy diet. Omega 3 and six fatty acids are vital for everything from heart health to vibrant skin to hormonal balance. Extra nutrients you should be getting include vitamin D, B complex, and magnesium. If you aren�t getting enough in the foods that you eat, then consider supplements. Yes, it�s that important.
You can also give your body a significant boost by taking probiotics and enjoying the marvelous healing properties of bone broth. Bone broth is available in powder or liquid � or you can make it yourself. It packs a serious nutritional punch so incorporating it into your diet is a brilliant move.
Chiropractic Balances Hormones
Chiropractic care is an excellent treatment for hormonal imbalance. It goes right to the heart of many of the factors that cause the body to get out of balance and treats the problem at its root.
It helps to relieve stress in the body and reduce or eliminate pain, both of which can contribute to hormonal imbalances. It is one of the best natural treatments for hormonal imbalance because it brings the body itself back into balance.
What�s more, the whole-body approach that chiropractic offers means that you get recommendations on healthy eating, exercise, and positive lifestyle changes. All of these things work together to balance your body and balance your hormones for a healthier, happier you.
Research has given us even more reasons to eat our veggies. Several studies have revealed that certain types of vegetables, specifically those known as cruciferous vegetables, have properties that could make them useful in preventing cancer.
What are Cruciferous Vegetables?
Some of the crunchiest, tastiest vegetables belong to the Cruciferae family. Typically cool weather vegetables, they are most notably characterized by four petal flowers somewhat resembling a cross.
These flower buds or the leaves are the parts of these plants that are most often consumed. However, the seeds or roots of some of these vegetables are also edible. Incorporating some of these cruciferous vegetables into your diet may help lower your risk for cancer:
Broccoli
Cabbage
Wasabi
Collard greens
Bok choi
Brussels sprout
Arugula
Cauliflower
Mustard (leaves and seeds)
Turnips
Horseradish
Rutabaga
Kale
Radish
Watercress
What is the Link Between Cruciferous Vegetables and Cancer?
Cruciferous vegetables are packed with nutrients that are believed to lower a person�s risk for several types of cancers, including prostate cancer, colorectal cancer, lung cancer, and breast cancer. This includes the carotenoids zeaxanthin, lutein, and beta-carotene as well as folate and vitamins C, E, and K. They are also rich in minerals and an excellent source of fiber which is well known for preventing colorectal cancer.
This group of vegetables is also a good dietary source of glucosinolates which also has cancer-fighting properties. When intact, the glucosinolates are not effective, but when they are broken down through chewing, processing, and pests, they then make contact with the myrosinase enzyme and initiate a process that releases specific chemicals that can prevent cancer.
How Cruciferous Vegetables Prevent Cancer
There are three primary ways that cruciferous vegetables can prevent cancer. Researchers have found substantial evidence that shows when they are part of a healthy, clean, low-fat diet, a person�s risk of cancer can be decreased.
Glucosinolates � These are chemicals that contain sulfur and are present in all cruciferous vegetables, giving them their trademark bitter flavor and pungent aroma. When this substance is broken down by chewing, preparation, or digestion, it forms certain compounds (indole-3-carbinol and sulforaphane) that scientists have identified as having �anticancer properties.� They do this by impeding the development or growth of cancer. Studies have looked at this effect on mice and rats and found that it is particularly useful in specific organs. Researchers are also looking at other ways the substances can prevent cancer. When working in the body, they:
Have anti-inflammatory properties
Aid in preventing DNA damage to cells
Inhibit the formation of blood vessels in tumors
Are antibacterial and antiviral
Inhibit the migration of tumor cells, thus halting metastasis
Cause cancerous cells to die
Aid in causing carcinogens to become inactiveBioactive components � Some studies have shown that the bioactive components of these veggies can affect the biomarkers of processes related to cancer in the human body such as decreasing abnormal cell growth. Genetic encoding of glutathione S-transferase � Glutathione S-transferase is an enzyme that helps the body metabolize and eliminate isothiocyanates. This is important because isothiocyanates prevent the activation of carcinogens, increase the speed at which the carcinogens are removed from the body, and counteract the dangerous effects of active carcinogens.
Best Ways to Consume Cruciferous Vegetables
Cruciferous vegetables are at their most nutritious and have the greatest cancer-fighting properties when they are raw. When the vegetables are chopped and chewed they release the most cancer-fighting chemicals. Likewise, when they are cooked, they lose a great deal of those properties. Steaming or cooking the vegetables very lightly for less than 5 minutes will allow them to retain some of those cancer-fighting properties.
Most people now acknowledge just how bad sugar is. The problem is, many are not willing to give it up. The evidence is clear though, over the last three decades chronic disease like diabetes, cancer, and heart disease have grown exponentially in occurrences that correlate strongly with Americans� ever-increasing intake of sugar.
But while this may not be new information, people are still unwilling to make the changes necessary � even with the threat of poor or worsening health (and even death) hanging over their heads.
One of the problems is that it is very difficult to get away from. Pick up almost any product on your grocery store shelves and read the ingredients. Sugar is there most of the time.
It is found in most processed foods including spaghetti sauce, salad dressings, dried fruit, fruit juices, even so-called �healthy� foods like frozen quinoa blends and �diet� frozen dinners. Sugar is everywhere and people are consuming it without even realizing that they are doing so.
Sugar is Addictive
Again, this is not new information, but many people don�t realize just how addictive sugar really is. One research article compared sugar addiction to drug addiction. The authors even went so far as to say sugar is as addictive as cocaine (or more so).
There is strong evidence to support this; sugar does affect a person at the neurobiological level. It activates the brain�s reward center, similar to what drugs do. Regular exposure provokes cravings similar to drug addiction and withdrawal symptoms when it is stopped.
The real problem here is that it is 1) legal, and 2) available for anyone to purchase- even children. There is a huge push to market sugar to children through heavily sugared cereals, drinks, and snack foods.
The children want it because they saw it on TV, the parents buy it, and the children end up cognitively impaired, obese, and chronically ill. It�s time to start connecting the dots and making significant changes in not only what we eat, but what we feed our children.
But Why is Sugar so Bad?
In its pure form, right out of the sugar cane, the juice has nutritional properties. However, all of that nutrition is destroyed when it is processed and refined as sugar (even “raw,” turbinado, and other forms – it’s still sugar). It becomes something that may be edible but isn�t really food. It is just a substance with absolutely no nutritional value � but lots of potential for damage.
The moment sugar enters your bloodstream your body begins secreting insulin. Insulin is produced in the pancreas and its function is to regulate sugar in the blood, to keep it balanced. When you overwhelm your body with sugar it keeps producing more and more insulin. A diet that is high in sugar can result in insulin resistance which can lead to obesity, diabetes, high blood pressure, and other dangerous conditions.
The more sugar you consume, the harder your body has to work to process it. It gets stored in the liver, leading to a fatty, enlarged liver, high glucose levels, and even affect the function of your organs including your kidneys. If you have conditions like heart disease, diabetes, or high blood pressure, the risk of damage to your organs is increased even more.
High glucose levels have also been linked to impaired cognitive function, loss of memory, depression, and anxiety as well as an increased risk of dementia. It can cause difficulty in concentration and the inability to focus or stay on task.
The solution here is to avoid sugar or make low sugar choices. Read labels! Take the time to think about what you are putting into your body and how it will affect you. If you make a conscious effort to reduce your sugar intake, over time your body will stop craving it.
*Detox Your Body* | Detox Doctor | El Paso, TX (2019)
The ketogenic diet, also known as a low carb diet is being talked about in various circles. And while science has proven over and over about the numerous health benefits, there are still those that want to disclaim it. This guide will explain the ketogenic diet, ketones, and the many health benefits that this way of eating provides.
What are Exogenous Ketones?
In order to understand exogenous ketones, it is important to first know what ketones are. Simply put, ketones are carbon-based, organic compounds that are produced in the liver. They are used by the mitochondria within the body to generate energy and can replace glucose as a fuel source, putting the body in a state of ketosis.
Exogenous ketones are ketones that are taken into the body as nutritional supplements. Endogenous ketones are produced in the body, specifically, the liver. Exogenous ketones are not produced in the body, rather are introduced into the body through supplements.
What is a Ketogenic Diet?
A ketogenic diet is characterized by three primary markers:
Low carbohydrate
Adequate protein
High fat
It is designed to put the body into a state of ketosis which means that instead of burning carbohydrates for energy, it is forced to burn fat.
When the body consumes foods that are high in carbs, it begins to produce insulin and glucose. Glucose happens to be the path of least resistance when it comes to energy conversion and usage, so the body will opt for that route before any utilizing another energy source.
What are the Benefits of a Ketogenic Diet?
There are several significant health benefits of a ketogenic diet. It was developed to be a way of life (WOL), not just a temporary diet and this was primarily due to the health benefits it provides. In fact, ketone diets were created to help allay or improve the symptoms of certain chronic health conditions, including epilepsy. Other benefits of the ketogenic diet include:
Weight loss
Lower insulin levels and reduced blood sugar
Lower triglycerides
Effectively treats metabolic syndrome
Forces the body to burn fat
Increased HDL (�good� cholesterol) levels
Improve LDL
Prevention of certain cancers
Potential to kill certain cancer cells
Lowered blood pressure
Improve epilepsy symptoms
Help treat Parkinson�s Disease
Reverse and treat symptoms of Alzheimer�s
The weight loss occurs from a ketogenic diet is largely fat loss – particularly abdominal fat (visceral fat). It is visceral fat that increases the risk of heart disease, type 2 diabetes, and other health conditions.
A ketogenic diet helps to reduce many of the risks of some of the most debilitating and even deadly chronic health conditions that are so prevalent today. Exogenous ketones provide a powerful supplementation to the diet, improving its effectiveness.
A ketogenic diet is not a quick fix or fad diet; it is indeed a way of life. While many people do see very noticeable results quite quickly, the substantial health benefits that it provides make it worthy of a lifelong commitment. By adhering to this low carb lifestyle, you can reverse many health conditions and avoid others. In short, you will enjoy increased energy and better health for years to come.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine