Can individuals dealing with neck pain find relief with electroacupuncture therapy while reducing pain symptoms to restore neck function?
Introduction
The cervical region of the body consists of the neck region, which allows the head to be mobile and stabilized from discomfort or pain. The neck has numerous muscles, ligaments, and tendons surrounding the cervical facet joints and spinal discs. However, when the neck muscles are overstretched or ached from environmental factors or traumatic injuries that cause the head and the neck muscles to whip back and forth rapidly, it can force individuals to deal with not only pain and discomfort from the neck but also the head and shoulders are affected as well. When this happens, many individuals try to find various relief methods to reduce the pain and its associated symptoms. Today’s articles look at how the pain symptoms are associated with the neck, how there are non-surgical treatments for neck pain, and how electroacupuncture can help restore neck function. We talk with certified medical providers who consolidate our patients’ information to understand better why they are experiencing neck pain. We also inform and guide patients on how non-surgical treatments like electroacupuncture can help restore neck function to the body. We encourage our patients to ask their associated medical providers intricate and important questions about reducing the impact of neck pain while trying to incorporate various therapeutic reliefs into their bodies. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
How Are Pain Symptoms Associated with the Neck?
Do you experience stiffness or pain on your neck’s left or right side? Do you constantly get headaches that you have to lie in a dark room to reduce the pain? Or do you experience numbness or tingling sensations on your shoulders and arms? Many of these pain-like scenarios are associated with neck pain. Now similar to back pain, neck pain is a multifactorial musculoskeletal condition that can lead to a socio-economic burden that causes many people to have reduced productivity and job-related problems that can be an issue. (Kazeminasab et al., 2022) Neck pain can be in acute or chronic stages as multiple factors can play the developmental part of neck pain. Some of the environmental factors and traumatic injuries associated with neck pain include:
Poor posture
Whiplash
Degenerative issues
Slouching/hunching position
Sprains or strains
Spinal fractures
When these environmental and traumatic injury factors start to cause issues in the neck region of the body, they can cause pain-like symptoms.
So, how is pain associated with the neck? Well, many individuals dealing with neck pain can either have specific or non-specific neck pain with various symptoms depending on the severity of the pain. While specific neck pain deals with the cervical spine, non-specific neck pain deals with the surrounding muscles and ligaments. To that point, many individuals who are dealing with neck pain are also experiencing somatic referred pain and radicular pain that is associated with neurological signs that make a diagnosis difficult to classify. (Misailidou et al., 2010) This can cause many individuals to experience referred pain in their shoulders and arms or have neurological issues like headaches and tension within their upper body regions, which then causes personal discomfort, disability, and impaired quality of life. (Ben Ayed et al., 2019) But all is not lost, as many individuals seek treatment to reduce the effects of neck pain.
Movement As Medicine- Video
Non-Surgical Treatments For Neck Pain
When it comes to reducing neck pain from environmental factors or traumatic injuries, many people will seek treatments that are affordable and effective in not only decreasing neck pain but also its associated pain-like symptoms. Non-surgical treatments are an excellent way to reduce the effects of neck pain, and they can be combined with other therapies. Some of the non-surgical treatments that are suitable for neck pain include:
Chiropractic care
Acupuncture
Electroacupuncture
Spinal decompression
Massage therapy
Physical therapy
Many individuals dealing with acute neck pain can incorporate non-surgical treatments since they are not only effective through consecutive treatment but are affordable as well. (Chou et al., 2020) This allows many individuals to be more mindful of what factors affect the neck and make small changes to prevent them from returning.
Electroacupuncture Restoring Neck Function
One of the oldest forms of non-surgical treatment is through acupuncture, which originates from China and is performed by highly trained professionals. Depending on how severe the pain is in the neck, many individuals seek out acupuncture therapy or electroacupuncture to reduce the pain. The difference between the two is that acupuncture incorporates thin, solid needles to the specific acupoints in the body that involve the central nervous system. In contrast, electroacupuncture incorporates electric stimulation to become a transformation of energy to block the pain signals that are causing pain in the neck region. (Liu et al., 2022)
Additionally, when the cervical area of the spine has been affected by traumatic forces, it can cause the neck to lose functionality. So, when people incorporate electroacupuncture to restore neck functionality, it has analgesic and anti-inflammatory properties that regulate the endocannabinoid system. (Wang et al., 2021) This means that the pain receptors from the nerve roots are blocked, and relief forms in the neck. Depending on the severity, many people with neck pain can utilize electroacupuncture consecutively to regain neck mobility and reduce the pain-like effects that are causing them to be miserable. When people think about their health and wellness, they can make small changes to reduce their environmental factors and start living life to the fullest extent possible.
References
Ben Ayed, H., Yaich, S., Trigui, M., Ben Hmida, M., Ben Jemaa, M., Ammar, A., Jedidi, J., Karray, R., Feki, H., Mejdoub, Y., Kassis, M., & Damak, J. (2019). Prevalence, Risk Factors and Outcomes of Neck, Shoulders and Low-Back Pain in Secondary-School Children. J Res Health Sci, 19(1), e00440. https://www.ncbi.nlm.nih.gov/pubmed/31133629
Chou, R., Wagner, J., Ahmed, A. Y., Blazina, I., Brodt, E., Buckley, D. I., Cheney, T. P., Choo, E., Dana, T., Gordon, D., Khandelwal, S., Kantner, S., McDonagh, M. S., Sedgley, C., & Skelly, A. C. (2020). In Treatments for Acute Pain: A Systematic Review. https://www.ncbi.nlm.nih.gov/pubmed/33411426
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Liu, R., Li, S., Liu, Y., He, M., Cao, J., Sun, M., Duan, C., & Li, T. (2022). Acupuncture Analgesia in Patients with Postoperative Neck Pain: A Protocol for Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med, 2022, 1226702. https://doi.org/10.1155/2022/1226702
Misailidou, V., Malliou, P., Beneka, A., Karagiannidis, A., & Godolias, G. (2010). Assessment of patients with neck pain: a review of definitions, selection criteria, and measurement tools. J Chiropr Med, 9(2), 49-59. https://doi.org/10.1016/j.jcm.2010.03.002
Wang, J., Zhang, J., Gao, Y., Chen, Y., Duanmu, C., & Liu, J. (2021). Electroacupuncture Alleviates Hyperalgesia by Regulating CB1 Receptor of Spinal Cord in Incisional Neck Pain Rats. Evid Based Complement Alternat Med, 2021, 5880690. https://doi.org/10.1155/2021/5880690
Can individuals dealing with headaches find the relief they are looking for from acupuncture to reduce pain-like symptoms?
Introduction
As part of the musculoskeletal system, the neck is part of the upper body portions and allows the head to be mobile through full rotations without pain and discomfort. The surrounding muscles, ligaments, and tendons help protect the cervical spinal region and have a fantastic relationship with the shoulders. However, the neck area can succumb to injuries, leading to pain-like symptoms that can cause pain and discomfort in the upper regions. One of the pain-like symptoms that correlates with neck pain is headaches. Headaches can vary in acute to chronic stages as they affect many individuals and the various factors that correlate with them. When headaches start to form, many individuals will look at multiple treatments to reduce the pain-like symptoms that correlate with headaches and have the relief they deserve. Today’s article looks at the various factors that correlate with headaches, how headaches cause overlapping risk profiles with neck pain, and how treatments like acupuncture can reduce headaches. We talk with certified medical providers who consolidate our patients’ information to provide treatments like acupuncture to minimize headaches. We also inform and guide patients on how acupuncture can benefit many individuals dealing with neck pain associated with headaches. We encourage our patients to ask their associated medical providers intricated and important questions about their pain-like symptoms that correlate with headaches and neck pain. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Various Factors Correlating Headaches
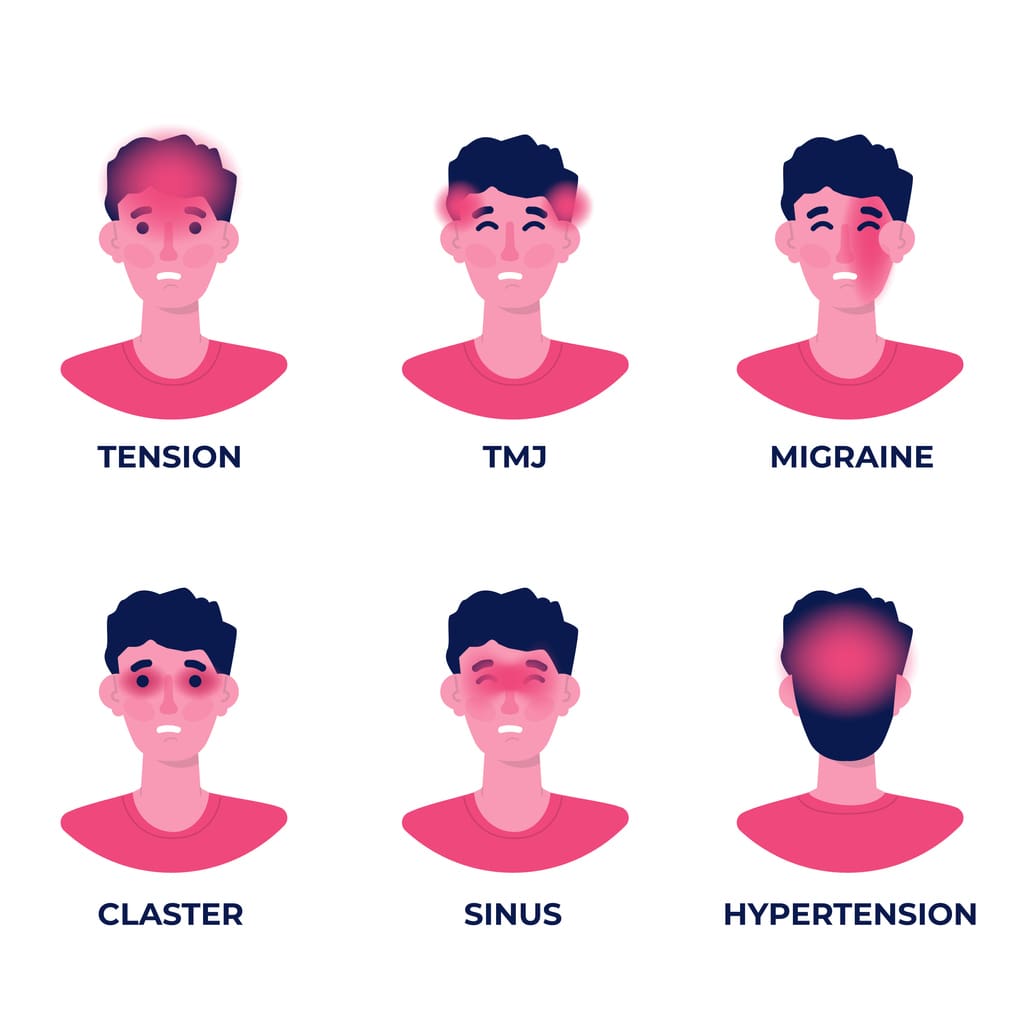
Have you been experiencing tension around the back of your neck after a long day? Do you feel a dull ache after staring at the computer or phone screen? Or do you feel a pounding sensation that you must lie down for a few minutes? Many of these pain-like scenarios are associated with headaches that affect many individuals from time to time. Headaches are correlated with various biochemical and metabolic risk profiles or changes that cause central sensitization and neuronal dysfunction. (Walling, 2020) This causes many individuals to develop acute or chronic pain-like symptoms that affect their heads and various locations around the face and the neck area. Some of the multiple factors that can lead to the development of headaches include:
Stress
Allergies
Tension
Inability to sleep
Lack of water and food
Traumatic injuries
Bright strobing lights
Additionally, other factors like obesity can become a strong risk factor for secondary headaches like migraines to have symptoms of intracranial hypertension impact the body. (Fortini & Felsenfeld Junior, 2022) This could lead to the development of neck pain caused by headaches.
Headaches & Neck Pain
When it comes to headaches associated with neck pain, many individuals will experience tension and pain in the surrounding muscles and the ongoing symptoms. Neck pain can cause overlapping risk profiles to muscles, ligaments, facet joints, and visceral structures of the neck that can trigger the development of a headache or become a symptom that co-exists with a neck disorder. (Vicente et al., 2023) Additionally, neck pain and headaches are strongly associated as muscular pain plays a role in headache development as they provide negative consequences within their social lives. Headaches can hinder a person’s ability to concentrate, while neck pain causes limited mobility and stiffness. (Rodriguez-Almagro et al., 2020)
Tension Headaches Overview- Video
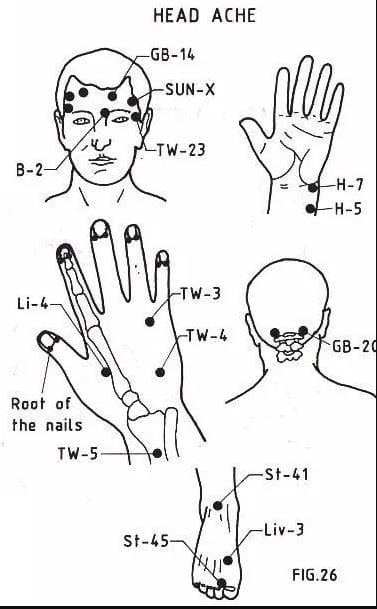
Acupuncture Reducing Headaches
When individuals are dealing with headaches, many will incorporate home remedies to reduce the tension they are experiencing from the various factors. This can provide temporary relief to mitigate the effects of the pain-like symptoms associated with headaches. However, when the pain from headaches becomes unbearable with neck pain in the mix, that is where non-surgical treatments could be the answer. Non-surgical treatments are effective on pain caused by headaches and customized to the person’s pain. For example, acupuncture could help with headaches and neck pain. Acupuncture is one of the oldest forms of non-surgical treatments; highly trained professionals use solid thin needles to be placed in various acupoints in the body to restore energy flow and reducing pain associated with headaches. (Turkistani et al., 2021)
Acupuncture can even help reduce the frequency and duration of headaches while disrupting the pain signals and help provide insight into the positive effects of pain reduction. (Li et al., 2020) When people start incorporating acupuncture as part of their health and wellness treatment plan, they will feel their headaches reduced and their neck mobility back to normal. Through consecutive treatment, they will feel much better and become more aware of the various factors pertaining to headache production while making small changes to reduce their chances of returning.
Li, Y. X., Xiao, X. L., Zhong, D. L., Luo, L. J., Yang, H., Zhou, J., He, M. X., Shi, L. H., Li, J., Zheng, H., & Jin, R. J. (2020). Effectiveness and Safety of Acupuncture for Migraine: An Overview of Systematic Reviews. Pain Res Manag, 2020, 3825617. https://doi.org/10.1155/2020/3825617
Rodriguez-Almagro, D., Achalandabaso-Ochoa, A., Molina-Ortega, F. J., Obrero-Gaitan, E., Ibanez-Vera, A. J., & Lomas-Vega, R. (2020). Neck Pain- and Unsteadiness-Inducing Activities and their Relationship to the Presence, Intensity, Frequency, and Disability of Headaches. Brain Sci, 10(7). https://doi.org/10.3390/brainsci10070425
Turkistani, A., Shah, A., Jose, A. M., Melo, J. P., Luenam, K., Ananias, P., Yaqub, S., & Mohammed, L. (2021). Effectiveness of Manual Therapy and Acupuncture in Tension-Type Headache: A Systematic Review. Cureus, 13(8), e17601. https://doi.org/10.7759/cureus.17601
Vicente, B. N., Oliveira, R., Martins, I. P., & Gil-Gouveia, R. (2023). Cranial Autonomic Symptoms and Neck Pain in Differential Diagnosis of Migraine. Diagnostics (Basel), 13(4). https://doi.org/10.3390/diagnostics13040590
Can individuals dealing with neck pain incorporate acupuncture as part of their health and wellness treatment to relieve headaches?
Introduction
As part of the musculoskeletal system, the neck allows the head to go into full rotation without feeling discomfort or pain. The neck is part of the cervical spine region and is surrounded by numerous ligaments, muscles, and tissues that help protect the spinal cord and the spinal column. However, the neck is also the most susceptible to injury neck to back pain as it is one the top three complaints many individuals suffer from at some point in their lives. When people experience neck pain, numerous causes can contribute to developing neck pain, while pain-like symptoms like headaches contribute to the body. This causes many individuals to seek treatment and find the relief they are looking for to reduce neck pain while continuing their daily routine. Today’s article looks at how neck pain is associated with headaches and how treatments like acupuncture can help with neck pain and reduce the painful effects of headaches. We talk with certified medical providers who utilize our patients’ information to provide acupuncture treatments to lessen the impact of headaches caused by neck pain. We also inform patients how multiple non-surgical treatments can help reduce headaches and pain-like symptoms associated with neck pain. We encourage our patients to ask their associated medical providers intricated and important questions about the pain-like symptoms they are experiencing from neck pain. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
Neck Pain & Headaches
Have you been experiencing unexplained stiffness along the sides of your neck? Do you feel a dull ache at the base of your neck or skull after looking down at your phone for an extended period? Or do you experience frequent headaches that are constant throughout the day? Many people dealing with these pain-like issues are associated with neck pain that is affecting their quality of life. Neck pain is amongst the top three complaints many people have experienced at some point. Neck pain has common presenting symptoms that are diagnosed, and the prevalence is much higher in older adults due to degenerative spinal changes in the facet joints and spinal discs. (Childress & Stuek, 2020) Many individuals experience common musculoskeletal pain conditions like muscle strains and stiffness when this happens. At the same time, neck pain can also be associated with neurological conditions that cause overlapping risk profiles, forcing many individuals to miss out on important events. Neck pain is a multifactorial musculoskeletal condition affecting many individuals as it induces them to miss work. This is because various modifiable and non-modifiable risk factors contribute to developing neck pain. (Kazeminasab et al., 2022) These risk factors can range from physical inactivity to poor posture, causing overlapping risk profiles that can trigger neck pain to advance over time.
So, how are headaches associated with neck pain? When a person is experiencing a headache, many would often think that the headaches are caused by not eating enough food or drinking enough water. Those are some of the factors that contribute to headaches, but they can also be due to the stress and comorbidities that are associated with neck pain. This is due to the risk factors many individuals don’t realize contribute to neck pain. Factors like the forward head position from smartphone usage cause tension on the cervical structures, generating potential degeneration and tearing of the neck structures. (Maayah et al., 2023) As repetitive motions affect the neck structure more over time, the nerve roots that surround the spine and spread through the upper extremities can become aggravated, and cause referred pain to different areas of the body, leading to headaches. When dealing with headaches associated with neck pain, they will feel stress, affecting their productivity. The headaches can range from acute to chronic, depending on the severity. Fortunately, many individuals dealing with headaches associated with neck pain will seek treatment to reduce the pain-like symptoms and feel the relief to return to their daily routine.
Healing After Trauma- Video
Many individuals who are dealing with neck pain often deal with headaches as a sign that risk factors are in play, like poor posture, slouching, or traumatic injuries that can affect their ability to work or participate in activities. This can cause many people to feel miserable and decrease their quality of life, thus causing them to seek out treatment for their pain, hence why many individuals opt for non-surgical treatments due to them being affordable and personalized. Non-surgical treatments range from chiropractic care to acupuncture, depending on the severity and location of where the pain is in the body. The video above shows how non-surgical treatments can help many individuals positively influence healing after a traumatic injury and restore a person’s well-being.
Acupuncture For Neck Pain
Non-surgical treatments are excellent for individuals trying to find the relief they seek in their neck pain. As stated earlier, non-surgical treatments are cost-effective and tailored to the person’s pain. Acupuncture is a form of non-surgical treatment that can help reduce the comorbidities associated with neck pain. Acupuncture is a medical practice in which highly trained, licensed, and certified professionals use solid, super-thin needles to be placed at specific points to treat the body. What this does is that when the needles are penetrating the points, it will begin to open any blockage or excess energy to flow correctly, restore balance to the body, and relieve the individual’s symptoms. (Berger et al., 2021) Some of the beneficial results that acupuncture can provide individuals with neck pain is a reduction of pain and disability to the neck while treating referred pain that is causing overlapping risk profiles to induce headaches. (Peron et al., 2022)
Acupuncture Relieving Headaches
Since headaches are associated with neck pain, acupuncture can help relieve the headaches from progressing further and enable many individuals to get back to their routine. Some overlapping risk profiles contributing to headaches include trigger points on the neck muscles that can cause non-dermatomal referral pain and discomfort. (Pourahmadi et al., 2019) When an acupuncturist is treating individuals for their headaches, many individuals will begin to feel the relief after a few consecutive sessions, and, combined with physical therapy to strengthen neck and shoulder muscles, will notice that the pain has been reduced significantly. Acupuncture is a safe, helpful, and available alternative treatment that is beneficial for many individuals dealing with headaches associated with neck pain. (Urits et al., 2020) By incorporating acupuncture as part of a person’s treatment plan, they can begin to feel the relief they deserve while also being more mindful of how they are treating their bodies to prevent pain-like symptoms from returning.
References
Berger, A. A., Liu, Y., Mosel, L., Champagne, K. A., Ruoff, M. T., Cornett, E. M., Kaye, A. D., Imani, F., Shakeri, A., Varrassi, G., Viswanath, O., & Urits, I. (2021). Efficacy of Dry Needling and Acupuncture in the Treatment of Neck Pain. Anesth Pain Med, 11(2), e113627. https://doi.org/10.5812/aapm.113627
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Maayah, M. F., Nawasreh, Z. H., Gaowgzeh, R. A. M., Neamatallah, Z., Alfawaz, S. S., & Alabasi, U. M. (2023). Neck pain associated with smartphone usage among university students. PLOS ONE, 18(6), e0285451. https://doi.org/10.1371/journal.pone.0285451
Peron, R., Rampazo, E. P., & Liebano, R. E. (2022). Traditional acupuncture and laser acupuncture in chronic nonspecific neck pain: study protocol for a randomized controlled trial. Trials, 23(1), 408. https://doi.org/10.1186/s13063-022-06349-y
Pourahmadi, M., Mohseni-Bandpei, M. A., Keshtkar, A., Koes, B. W., Fernandez-de-Las-Penas, C., Dommerholt, J., & Bahramian, M. (2019). Effectiveness of dry needling for improving pain and disability in adults with tension-type, cervicogenic, or migraine headaches: protocol for a systematic review. Chiropr Man Therap, 27, 43. https://doi.org/10.1186/s12998-019-0266-7
Urits, I., Patel, M., Putz, M. E., Monteferrante, N. R., Nguyen, D., An, D., Cornett, E. M., Hasoon, J., Kaye, A. D., & Viswanath, O. (2020). Acupuncture and Its Role in the Treatment of Migraine Headaches. Neurol Ther, 9(2), 375-394. https://doi.org/10.1007/s40120-020-00216-1
Can various therapeutic options provide relief for individuals with upper crossed syndrome to restore muscle strength?
Introduction
Many individuals often suffer neck and shoulder pain from poor posture, improper heavy lifting, musculoskeletal conditions, auto accidents, whiplash, etc. The surrounding muscles that connect the neck and shoulders help protect the cervical and thoracic region of the spine and can succumb to injuries that can cause pain-like symptoms causing discomfort to the individual. Neck, shoulder, and back pain are the three most common issues many individuals have experienced. These musculoskeletal disorders can also correlate with pre-existing conditions; many people will feel pain and discomfort while trying to find the relief they seek. One of the most common issues people often experience is upper crossed syndrome, which can be associated with neck and shoulder pain. Today’s article explains what upper cross syndrome is and how it affects the neck and shoulders while also diving into how different therapeutic options like spinal decompression and chiropractic care can reduce the effects of upper cross syndrome. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to mitigate upper-crossed syndrome in the neck and shoulders. We also inform our patients that there are many therapeutic options, like chiropractic care and spinal decompression, to minimize muscle pain in the neck and shoulders. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with upper-crossed syndrome. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer
What Is Upper Crossed Syndrome?
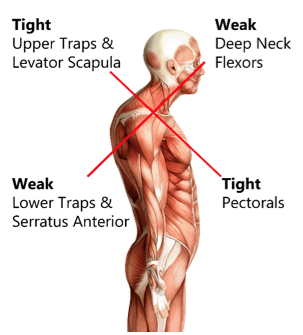
Have you been dealing with muscle pain in your shoulders or neck after being on the computer for a while? Do you feel stiffness in your shoulders that rotating them causes temporary relief? Or does it hurt when you turn your head from side to side? Many of these pain-like scenarios are often associated with upper-cross syndrome. Many people don’t often realize that upper crossed syndrome is a musculoskeletal condition that affects the neck, shoulder, and chest muscles and causes them to be weak and tight due to poor posture. The upper crossed syndrome can cause referred pain to the upper extremities, leading to cervicogenic headaches, limited range of motion, trigger points in the muscles, and muscle imbalance. (Moore, 2004) When many people are dealing with upper crossed syndrome due to poor posture, it can lead to many issues in the neck and shoulders.
How Does It Affect The Neck & Shoulders?
Now, why does upper crossed syndrome affect the neck and shoulders? Many people unintentionally hunched over when looking at their phones, being on the computer, or relaxing at home. This causes specific muscles in the neck and shoulder region, like the serratus and lower trapezius muscles, to become weak while the pectoral and neck muscles are tight. (Chu & Butler, 2021) This, in turn, causes the shoulders to be more rounded and hunched, causing the neck and head to crane forward. When people are dealing with upper crossed syndrome, many would often complain about pain-like symptoms like:
Headaches
Neck Strain
Muscle tightness
Upper back pain
Restricted range of motion
Numbness/Tingling sensations in the arms
The upper crossed syndrome can also occur gradually over time and cause nerve compression to the upper extremities. When the upper neck and shoulder muscles start to affect the surrounding nerve roots, which then leads to nerve dysfunction in the sensory and motor skills when a person picks up an object. (Lee & Lim, 2019) However, many individuals dealing with upper-crossed syndrome can seek treatment to relieve muscle pain in their neck and shoulders.
An Overview Of Upper Crossed Syndrome- Video
Since upper cross syndrome is a musculoskeletal condition that affects the neck and shoulders, it can result in muscle imbalance and pain in the individual. Many people, especially in the working field, develop this syndrome by being hunched over for an extended period. (Mujawar & Sagar, 2019) This causes the head to be more forward, the neck posture to be curved and hunched, and the shoulders to be rounded. The video above explains upper-crossing syndrome, its causes, and how it is treated.
Numerous treatments can help restore muscle strength and reduce muscle pain in the neck and shoulders. Treatments like spinal decompression can help reduce upper crossed syndrome by slowly using gentle traction to the cervical spine region and gently stretching the neck muscles to provide relief. Spinal decompression is one of the non-surgical treatments that many individuals with headaches associated with upper crossed syndrome can find the comfort they seek through pain reduction and improve their quality of life. (Eskilsson et al., 2021) At the same time, spinal decompression can be part of a personalized treatment plan that many individuals can add to their daily routine to prevent the pain from returning. (Saunders, 1983)
Chiropractic Care Restoring Muscle Strength
Just like spinal decompression, chiropractic care is a non-surgical treatment that can be combined with various stretching techniques to restore the neck’s range of motion and reduce pain associated with upper-crossed syndrome. (Mahmood et al., 2021) Chiropractic care incorporates manual and mechanical techniques like MET (muscle energy techniques) and spinal manipulation to realign the spine out of subluxation. When chiropractors integrate MET to manage upper crossed syndrome, many individuals find that their pain has decreased, their cervical range of motion is improved, and their neck disability is reduced. (Gillani et al., 2020) When many individuals start thinking about their health and wellness, they can make small changes to improve their posture and be more mindful of their bodies to reduce the chances of upper-cross syndrome returning.
References
Chu, E. C., & Butler, K. R. (2021). Resolution of Gastroesophageal Reflux Disease Following Correction for Upper Cross Syndrome-A Case Study and Brief Review. Clin Pract, 11(2), 322-326. https://doi.org/10.3390/clinpract11020045
Eskilsson, A., Ageberg, E., Ericson, H., Marklund, N., & Anderberg, L. (2021). Decompression of the greater occipital nerve improves outcome in patients with chronic headache and neck pain – a retrospective cohort study. Acta Neurochir (Wien), 163(9), 2425-2433. https://doi.org/10.1007/s00701-021-04913-0
Gillani, S. N., Ain, Q., Rehman, S. U., & Masood, T. (2020). Effects of eccentric muscle energy technique versus static stretching exercises in the management of cervical dysfunction in upper cross syndrome: a randomized control trial. J Pak Med Assoc, 70(3), 394-398. https://doi.org/10.5455/JPMA.300417
Mahmood, T., Afzal, W., Ahmad, U., Arif, M. A., & Ahmad, A. (2021). Comparative effectiveness of routine physical therapy with and without instrument assisted soft tissue mobilization in patients with neck pain due to upper crossed syndrome. J Pak Med Assoc, 71(10), 2304-2308. https://doi.org/10.47391/JPMA.03-415
Moore, M. K. (2004). Upper crossed syndrome and its relationship to cervicogenic headache. J Manipulative Physiol Ther, 27(6), 414-420. https://doi.org/10.1016/j.jmpt.2004.05.007
Mujawar, J. C., & Sagar, J. H. (2019). Prevalence of Upper Cross Syndrome in Laundry Workers. Indian J Occup Environ Med, 23(1), 54-56. https://doi.org/10.4103/ijoem.IJOEM_169_18
How does innovated non-surgical treatment help assist individuals with cervical spinal pain to reduce headaches?
Introduction
Do you or your loved ones often experience headaches that don’t disappear? Do you often feel your shoulder and neck muscles ache after looking down at your cell phone? Or do you feel aches after being slouched for an extended period? Many of these scenarios correlate with referred pain in the cervical spinal region, which can develop into neck pain. The neck region is located in the upper body portion and provides mobility for the head without pain and discomfort. The neck region also has surrounding muscles and ligaments that support the spine and protects the thyroid and spinal cord. However, just like the back region, it is susceptible to pain as many individuals can overstretch the neck muscles, and it can cause referred pain to the shoulders and head, leading to pain-like symptoms that can lead to a life of disability. However, non-surgical treatments can minimize the pain and help strengthen the surrounding muscles in the neck region. Today’s article focuses on how cervical spinal pain connects with headaches and how decompression can reduce headaches while relieving neck pain. Additionally, we communicate with certified medical providers who incorporate our patients’ information to reduce cervical spinal pain associated with headaches, causing many musculoskeletal issues in the upper body portion. We also inform them that non-surgical treatments can help relieve headaches and provide relief to the neck region. We encourage our patients to ask amazing educational questions for our associated medical providers about their symptoms correlating with cervical spinal pain. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer
Cervical Spinal Pain & Headache Connection
Throughout the world, neck pain (cervical spinal pain) is the second most common problem that can affect many individuals throughout their lives. It can lead to a life of disability and pain if not treated immediately. Many individuals often experience non-specific neck pain, as it can be through a postural or mechanical basis that can cause muscle strain in the surrounding muscles or compress the spinal canal to cause headaches that can last throughout the entire day. (Binder, 2008) Additionally, neck pain, like back pain, is a multifactorial disease with common risk factors like lack of physical activity, duration of computer usage, and perceived stress. (Kazeminasab et al., 2022) Many of these risk factors are normal as they can also affect the surrounding muscles in the lower back region and shoulder region, as many people often do repetitive motions that can naturally be overstretched and cause pain-like issues to the neck region. With neck pain connected with headaches, it can cause overlapping risk profiles and be costly. Neck pain associated with headaches can be a frequent and expensive occupational health problem as symptoms of pain, disability, reduced life quality, and, for adults, time lost for work. (Ben Ayed et al., 2019)
The correlation between headaches and neck pain is that the spinal canal is compressed from traumatic forces that can lead to cervicogenic headaches. Cervicogenic headaches usually aggravate neck mobility, thus reducing the ROM of the neck. (Verma, Tripathi, & Chandra, 2021) This can lead to many individuals suffering from migraine-like headaches and muscle stiffness in the upper regions of the body. When many individuals are dealing with headaches associated with cervical spinal pain, many will find treatments to mitigate the pain-like symptoms affecting the upper body region.
The Benefits Of Stretching-Video
When it comes to neck pain, it can be either acute or chronic depending the factors that cause it or the severity of the pain. Many individuals sought treatment that can alleviate the pain in the upper regions that are non-surgical and beneficial to their health and well-being. Non-surgical treatments can help stretch the tight and short muscles in the neck region and can reduce headaches affecting the person. Additionally, having the neck muscles professionally stretched by a massage therapist can relieve the neck and reduce headaches. The video above explains the benefits of stretching and describes how many people don’t stretch their bodies often to prevent pain-like issues from reoccurring in the future.
Spinal Decompression For Cervical Pain
Non-surgical treatments are excellent when it comes to reducing neck pain. When relieving neck pain, healthcare professionals must use the best available evidence to enhance clinical decision-making and improve the quality of care for people with neck pain. (Misailidou et al., 2010) Spinal decompression can help many people with neck pain by reducing the issues through gentle spinal traction. What spinal decompression does for the cervical spine is that it can realign the disc that is aggravating the neck region and causing headaches by stretching the surrounding muscles. This causes muscle improvement for the neck as it can change the patient’s pain outcome. (Youssef et al., 2019) Additionally, spinal decompression is safe, cost-effective, and gentle on the spine as it can be combined with other therapies to mitigate any residual pain that can relieve the neck and back. (Flynn, 2020) Many people who incorporate spinal decompression as part of their routine can benefit from their outcome as they return to their routine.
References
Ben Ayed, H., Yaich, S., Trigui, M., Ben Hmida, M., Ben Jemaa, M., Ammar, A., Jedidi, J., Karray, R., Feki, H., Mejdoub, Y., Kassis, M., & Damak, J. (2019). Prevalence, Risk Factors and Outcomes of Neck, Shoulders and Low-Back Pain in Secondary-School Children. J Res Health Sci, 19(1), e00440. https://www.ncbi.nlm.nih.gov/pubmed/31133629
Flynn, D. M. (2020). Chronic Musculoskeletal Pain: Nonpharmacologic, Noninvasive Treatments. American Family Physician, 102(8), 465-477. https://www.ncbi.nlm.nih.gov/pubmed/33064421
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Misailidou, V., Malliou, P., Beneka, A., Karagiannidis, A., & Godolias, G. (2010). Assessment of patients with neck pain: a review of definitions, selection criteria, and measurement tools. J Chiropr Med, 9(2), 49-59. https://doi.org/10.1016/j.jcm.2010.03.002
Verma, S., Tripathi, M., & Chandra, P. S. (2021). Cervicogenic Headache: Current Perspectives. Neurol India, 69(Supplement), S194-S198. https://doi.org/10.4103/0028-3886.315992
Youssef, J. A., Heiner, A. D., Montgomery, J. R., Tender, G. C., Lorio, M. P., Morreale, J. M., & Phillips, F. M. (2019). Outcomes of posterior cervical fusion and decompression: a systematic review and meta-analysis. Spine J, 19(10), 1714-1729. https://doi.org/10.1016/j.spinee.2019.04.019
Many people experience neck and back pain due to various factors that affect their daily routine. These pain conditions are common and can be caused by repetitive motions that impact the surrounding muscles, tissues, ligaments, and spinal discs. Chronic pain can develop depending on the severity and duration of the condition. People with demanding jobs, pre-existing conditions, or older adults may seek medical attention to reduce the pain-like symptoms of neck and back pain. However, treatment costs can be high. There are safe, cost-effective, and non-invasive treatments to relieve neck and back pain. This article will explore why neck and back pain is expensive and why non-surgical treatments are cost-effective. It will also discuss how non-surgical therapies like spinal decompression can alleviate back and neck pain. We work with certified medical providers who use our patients’ valuable information to treat individuals suffering from back and neck pain while informing them about non-surgical treatments like spinal decompression that can help relieve their neck and back pain. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
Why Does Back & Neck Pain Cost More?
Many people report to their primary doctors that they are experiencing radiating pain from the neck or lower back, which affects their upper or lower extremities. For neck pain, they may experience headaches or shoulder pain that causes pain-like symptoms like numbness or tingling sensations down to their arms and fingers. For back pain, they may experience muscle soreness in their lumbar region, which can result in numbness in the glute muscles or cause sciatic nerve pain, affecting their walking ability. Research studies reveal that cognitive, affective, and lifestyle factors all affect the neck and back. High-demanding jobs, stress, or trauma from an accident can develop neck and back pain. As a result, the body takes more overbearing loads, tightening the surrounding muscles in the neck and back. If not treated right away, it can lead to problematic issues that disrupt their routine.
Based on the book “The Ultimate Spinal Decompression” by Dr. Eric Kaplan D.C., FIAMA, and Dr. Perry Bard, D.C., humans’ evolution to walk upright has strained their stability, leading to axial overload and potential neck and back pain. The book also highlights that the human body was not meant to remain sedentary, which can also contribute to the development of such pain. Research studies revealed that neck and back pain can be nociceptive with neuropathic components, making treatment costly and time-consuming. This economic burden can discourage individuals from seeking treatment despite the pain and expense involved.
Fighting Inflammation Naturally- Video
Are you experiencing persistent neck and back pain? Do your upper or lower extremities feel stiff or tingly? Or is your mobility limited, interfering with your daily activities? These issues are often associated with neck and back pain, disrupting a person’s routine and preventing them from enjoying life. Neck and back pain are common ailments that can be expensive to treat. Research studies revealed that they can also influence individuals’ ability to return to work, increasing treatment costs.
Additionally, pain-like symptoms often accompany neck and back pain, leading some individuals to spend nearly a billion dollars on treatment. However, cost-effective treatments are available that can help alleviate these symptoms. The video above explains how non-surgical treatments can reduce neck and back pain and relieve pain-like symptoms.
Why Non-Surgical Treatments Are Cost Effective?
Research studies have shown that non-surgical treatments are a cost-effective and effective solution for neck and back pain. Many individuals can utilize these treatments combined with various therapies to improve their quality of life and reduce pain symptoms. Non-surgical treatments offer personalized plans as healthcare providers work together to find solutions. They provide individuals with a positive approach to regaining their health and wellness by informing them about their bodies and how to be more mindful of how pain affects their daily routines. Some non-surgical treatments that can relieve neck and back pain include:
Chiropractic care
Physical therapy
Spinal Decompression
Acupuncture
Massage therapy
How Spinal Decompression Can Alleviate Back & Neck Pain
You might be interested in non-surgical treatments like spinal decompression if you suffer back or neck pain. This technique uses gentle traction on the spinal column to alleviate pain while helping your body heal naturally. Research studies have found that cervical spinal decompression can increase disc height and reduce pain caused by compressed cervical discs. This treatment can also alleviate residual pain symptoms like headaches or muscle stiffness and restore mobility to the neck. For back pain, research suggests that spinal decompression can reduce the effects of compressed spinal discs, which can aggravate nerve roots like the sciatic nerve in the lumbar region. Many people who try spinal decompression feel relief after just a few sessions and become more mindful of what triggers their pain. This can help them make small lifestyle changes to continue their journey toward health and wellness.
Conclusion
Many people struggle with neck and back pain, which can be caused by multiple normal and traumatic factors and can be costly. Individuals often prefer to endure the pain rather than subject themselves to invasive treatments. However, non-surgical therapies that are cost-effective and gentle on the body are available. Spinal decompression therapy is one such treatment that can help alleviate pain and promote the body’s natural healing processes. By reducing pain symptoms, many individuals who undergo spinal decompression therapy can return to their daily routines pain-free.
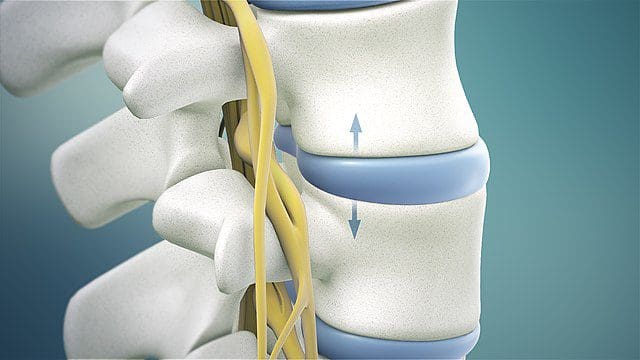
The neck is an extremely flexible part of the upper body that allows the head to move without causing pain or discomfort. It is part of the musculoskeletal system‘s cervical spinal region, which supports the spinal column and is surrounded by various muscles, tissues, and ligaments that protect the spinal cord. However, poor posture, spending too much time hunched over a computer, or looking down at our cellphones can cause neck muscles to become overstretched, leading to compression of the cervical spinal discs. This can cause the cervical discs to bulge or herniate, aggravating the spinal cord and causing neck pain and other associated conditions. This post will discuss how cervical disc compression affects neck pain and how decompression surgery and spinal decompression can help alleviate this condition. We work with certified medical providers who use our patients’ valuable information to treat individuals dealing with cervical disc compression affecting their necks and causes mobility issues. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
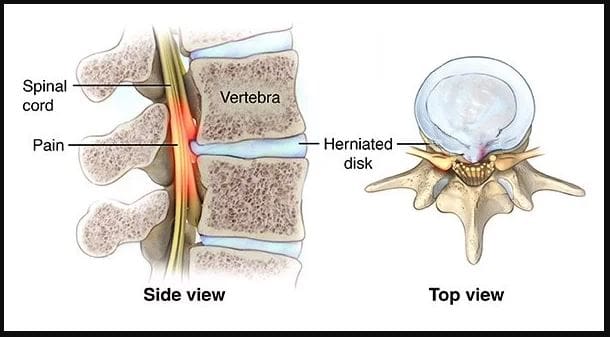
What Is Cervical Disc Compression?
Have you been experiencing neck pain or muscle aches in your shoulders? Do you feel numbness or tingling running down your arms and fingers? These symptoms may be signs of cervical disc compression. The cervical spinal discs act as shock absorbers for the spine, preventing unwanted pressure and mobility issues. Research studies revealed that age-related degenerative properties like dehydration could cause herniated and compressed cervical discs, leading to posterior disc protrusion into the spinal cord. Trauma can also cause extreme hyperflexion or hyperextension of the posterior neck muscles, resulting in various neck symptoms. Additional research studies stated cervical disc displacement could cause compression or impingement on spinal nerve roots, leading to inflammation and neck pain.
How Is It Associated With Neck Pain?
When the spinal cord and nerve roots in the cervical region are affected by cervical disc compression, the pain can be dull or sharp, depending on how it affects many individuals. According to research studies, many people are unaware that repetitive normal factors or traumatic forces can cause a challenge in determining the origin of the pain from symptomatic or asymptomatic disc compression. Additional research studies mentioned that cervical disc compression could cause upper and lower extremities abnormalities, such as loss of deep tendon reflexes in the arms and legs, loss of motor function in the hands and feet, muscle weakness, headaches, and gait imbalances. However, various treatments can alleviate the pain-like symptoms associated with cervical disc compression and help the body’s natural healing process.
From Inflammation To Healing-Video
Are you experiencing inflammation and pain in your neck? Do you notice a tingling or numb sensation in your hands or feet? Or do you feel stiffness in your shoulders or neck? These symptoms can be caused by compressed cervical discs, which many people are unaware of. The compression of cervical discs is a common source of neck pain and can even cause referred pain in the upper and lower extremities. Repetitive motions to the neck can cause the posterior neck muscles to overstretch and lead to pain. Normal or traumatic factors can also lead to neck pain associated with cervical disc compression, resulting in disc herniation. Fortunately, non-surgical therapies like chiropractic care and spinal decompression can help alleviate the symptoms of pain, discomfort, and inflammation caused by cervical disc compression. Check out the video above for more information on these treatments.
Posterior Cervical Disc Decompression Surgery
If you experience cervical compression on your neck, it can lead to persistent neck pain and discomfort if left untreated. Many people opt for posterior cervical disc decompression surgery to alleviate the effects of disc herniation. According to “The Ultimate Spinal Decompression” by Dr. Perry Bard, D.C., and Dr. Eric Kaplan, D.C., FIAMA, cervical disc herniation can sometimes affect the back of the neck and cause persistent pain. In such cases, decompression surgery is often performed. During the procedure, a small incision is made at the back of the neck, and a portion of the damaged disc is removed to ease the irritated nerve. This brings relief to the individual suffering from neck pain.
Non-Surgical Decompression For Compressed Cervical Disc
If you’re not interested in surgery for cervical disc compression, consider non-surgical spinal decompression instead. Studies have shown that spinal decompression is a safe, non-invasive treatment involving gentle cervical spine traction to reposition the herniated disc. This treatment can also help rehydrate the spinal disc by bringing in nutrients and oxygenated blood to promote natural healing. Additionally, spinal decompression can alleviate any remaining symptoms of neck pain.
Conclusion
The neck is a highly flexible area that enables smooth head movement without discomfort or pain. However, it is also a part of the musculoskeletal cervical region that can be prone to injuries. Compression of the disc due to normal or traumatic factors can result in herniation, causing pain if left untreated. Fortunately, several treatments are available to alleviate neck pain caused by cervical compression and make the neck mobile again.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine