How Integrative Sports Chiropractic Speeds Injury Recovery at the Mechanical and Cellular Levels
Athletes push their bodies hard. A sudden twist, a hard landing, or repeated stress can leave them with sprains, disc problems, tendon issues, or lingering pain. Traditional rest and pain pills often only quiet the symptoms. Integrative sports chiropractic takes a different path. It treats the injury at both the mechanical level—how bones, joints, and soft tissues line up and move—and the cellular level—how cells repair, reduce swelling, and rebuild tissue.
This approach combines spinal decompression, precise chiropractic adjustments, MLS laser therapy, shockwave therapy, and peptide support. Together, they create a non-invasive plan that moves athletes from simply managing pain toward faster, more complete tissue regeneration.
Why Mechanical and Cellular Care Matter Together
Injuries create two problems at once. Mechanically, a disc may bulge and press on a nerve, or joints may shift out of place. Soft tissues tighten or form scar tissue, limiting motion. At the cellular level, inflammation increases, blood flow decreases, and cells lack the energy and building blocks needed to heal effectively.
Treating only one side leaves the other unfinished. Aligning the spine without calming inflammation or feeding the cells often leads to slow progress or return of symptoms. Addressing cells without fixing alignment allows the mechanical problem to keep stressing the tissues. Integrative care solves both.
Spinal Decompression: Creating Space and Delivering Nutrients
Spinal decompression uses a specialized table that gently and controllably stretches the spine. This creates a mild negative pressure inside the disc. The pressure pulls bulging or herniated material away from nerves and draws nutrient-rich fluid back into the disc.
Discs have a limited blood supply, so they depend on this fluid exchange for oxygen and nutrients. When decompression restores that flow, the disc environment becomes more conducive to repair. Athletes with lower back or neck disc issues often experience reduced nerve pressure and improved mobility after a series of sessions. The treatment is comfortable and requires no downtime.
Chiropractic adjustments carefully restore normal position and motion to the spine and joints. When vertebrae sit correctly, nerve pathways stay open, and muscles no longer work overtime to compensate. Adjustments also help maintain the space created by decompression so the disc does not quickly return to its previous stressed state.
For sports injuries, proper alignment improves how force travels through the body during running, jumping, or throwing. This reduces secondary strain on tendons and ligaments. The combination of decompression and adjustments addresses the mechanical foundation of the injury.
MLS Laser Therapy: Energizing Cells to Heal
MLS laser therapy delivers specific, synchronized wavelengths of light deep into tissue. One wavelength helps calm inflammation. The other supports pain relief and cellular activity. The light energy reaches the mitochondria inside cells and boosts ATP production, the main energy source cells use for repair.
Higher ATP levels allow cells to work more efficiently. Swelling decreases, blood flow improves, and collagen production rises. Sessions are short and painless. Athletes often notice reduced soreness and faster return of function when laser is added to mechanical care. Research and clinical use show that combining laser with chiropractic shortens recovery time compared with either method alone.
Shockwave Therapy: Breaking Scar Tissue and Restarting Healing
Shockwave therapy sends focused acoustic waves into injured soft tissue. These waves increase local blood flow, break down dense scar tissue and calcifications, and release growth factors that restart stalled healing.
Chronic tendon problems—such as tennis elbow, Achilles issues, or rotator-cuff irritation—respond especially well. The waves create a controlled micro-stimulus that tells the body to rebuild stronger tissue rather than leave restrictive scar behind. When used with adjustments, shockwave improves the way muscles and tendons glide over newly aligned joints.
Certain peptides act as signaling molecules that encourage the body’s own repair systems. Peptides such as BPC-157 and TB-500 have been studied for their ability to support blood-vessel growth, modulate inflammation, and promote organized collagen deposition in tendons, ligaments, and muscle.
In the setting of disc or joint injury, these signals can help create a more favorable environment for tissue recovery. They work alongside the mechanical and energy-based therapies rather than replacing them. Clinical protocols often include peptides as part of a broader regenerative plan under medical oversight. Evidence is strongest in preclinical models and growing in human musculoskeletal use, with careful patient selection and monitoring.
How the Full Combination Accelerates Recovery
A typical integrated plan might begin with evaluation of posture, joint motion, nerve function, and soft-tissue quality. Spinal decompression and adjustments restore mechanical balance. Laser and shockwave then address inflammation and scar tissue at the cellular and tissue levels. Peptides supply additional regenerative signals.
The result is more than pain relief. Blood flow improves, cells receive energy and nutrients, restrictive scars soften, and new tissue forms under better biomechanical conditions. Athletes often progress faster through rehabilitation exercises because the underlying tissues are better prepared to handle load.
Key advantages include:
Non-invasive nature with little or no downtime
Simultaneous treatment of structure and cellular function
Reduced need for long-term medication or invasive procedures
Support for both acute sports injuries and chronic overuse problems
Multidisciplinary Care at Injury Medical Clinic PA in El Paso
In El Paso, Texas, Injury Medical Clinic PA brings these therapies together under one coordinated team. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CCST, CFMP, IFMCP, ATN, provides chiropractic and functional medicine care focused on sports injuries, personal injury recovery, and whole-person restoration. His clinical observations, detailed on dralexjimenez.com and his professional profile, emphasize identifying root mechanical and metabolic contributors to pain rather than masking symptoms. He notes that many athletes and active patients improve when alignment, soft-tissue health, nutrition, and cellular support are addressed together.
Medical direction and collaborative oversight are provided by Dr. Maria Guadalupe Cardenas, MD. She is board-certified in internal medicine (NPI #1164426749, Texas MD License #J2933) and brings more than 40 years of experience as an internist. As Medical Director and Collaborative Physician, Dr. Cardenas works alongside Dr. Jimenez to ensure medical safety, appropriate diagnostic correlation, and integrated planning. This MD–DC partnership is common in modern integrative and injury-focused clinics. It allows seamless blending of chiropractic adjustments, spinal decompression, laser and shockwave therapies, functional-medicine strategies, personal-injury documentation, and regenerative options such as peptides—all under physician collaboration.
The clinic’s multidisciplinary model also incorporates rehabilitation exercises, nutritional support, and careful monitoring so that mechanical corrections and cellular therapies reinforce one another. Patients receive coordinated care that respects both the structural demands of sport and the biological processes of healing.
Moving from Symptom Control to Active Tissue Regeneration
Symptom management keeps pain low enough for daily life. Active tissue regeneration aims higher: it restores the quality and resilience of injured structures, enabling athletes to return to training with confidence. Spinal decompression and adjustments handle the mechanical framework. MLS laser supplies cellular energy. Shockwave clears barriers of scar tissue. Peptides amplify the body’s repair signals. When these tools are used in sequence under experienced clinical guidance, recovery becomes more efficient and complete.
Athletes who once faced months of limited activity often regain function sooner and with less residual restriction. The same principles apply to active people of all ages who want durable results without surgery.
Integrative sports chiropractic offers a clear path: fix the structure, feed the cells, clear the obstacles, and support the body’s own regenerative capacity. The combination delivers a practical, non-invasive route back to performance from injury.
Repairing Your Spine from the Inside Out: How Chiropractic and Regenerative Therapies Work Together
Chronic back or neck pain can make everyday life feel challenging. Many people try rest, pain pills, or physical therapy, but the pain often returns. Surgery is one option, yet it comes with risks and long recovery times. There is a better path for many people. Combining chiropractic care with regenerative therapies helps repair the spine from the inside out. Chiropractic adjustments fix the structure and alignment. Treatments such as PRP injections and shockwave therapy help heal the soft tissues around the bones. Together, they stop chronic pain and help rebuild strength without surgery.
This approach treats the whole picture. It is like fixing a house with problems in both the frame and the interior.
Your Spine Is Like a House
Think of your spine like the wooden frame of a house. The bones (vertebrae) are the main beams. The discs, ligaments, tendons, and muscles are the wood, pipes, and supports that hold everything together.
If the frame leans or shifts, the whole house feels off. Chiropractic adjustments gently move the bones back into better position. This straightens the frame and takes pressure off nerves.
But what if the wood is rotting or the pipes are leaking? Straightening the frame alone will not last. The house will lean again. The same thing happens with the spine. If the soft tissues stay damaged or inflamed, pain and weakness return even after effective adjustments.
Regenerative therapies, laser treatments, and shockwave therapy act like a skilled repair crew. They go into damaged areas, reduce swelling, and help new, healthy tissue grow. Massage and spinal decompression then remove daily stress so the repairs hold strong over time. This comprehensive plan delivers lasting results for many people with ongoing spinal problems.
Chiropractic Care: Fixing the Structural Frame
Chiropractic care focuses on the bones and joints of the spine. A chiropractor uses gentle, hands-on adjustments to correct misalignments. These shifts can happen from poor posture, old injuries, car accidents, or years of sitting and bending.
Adjustments help in simple ways:
They restore normal movement in stiff joints.
They reduce pressure on nerves that cause pain, numbness, or tingling.
They improve blood flow and support the body’s natural healing ability.
They help improve posture so daily activities feel easier.
According to reliable health information, chiropractic adjustments aim to correct alignment problems, ease pain, and support the body’s natural ability to heal itself (MedlinePlus, n.d.). Many people use it for low back pain, neck pain, and headaches. It is a hands-on method that does not rely on drugs or surgery.
When the frame is straight, the rest of the spine can heal better. But adjustments work even better when paired with treatments that fix the soft tissues around the bones.
Regenerative Therapies: The Repair Crew for Soft Tissues
Regenerative therapies use the body’s own materials to heal damaged areas. They target the “rotting wood” parts — inflamed discs, torn ligaments, irritated nerves, and weak tendons. These treatments send growth signals that tell cells to repair and rebuild.
Common options include:
PRP (platelet-rich plasma): A small amount of your blood is spun in a machine to concentrate the healing platelets. These are injected into painful spots. Growth factors signal damaged tissues to calm down and grow stronger (El Paso Back Clinic, n.d.).
Shockwave therapy: Special sound waves reach deep into sore muscles and tendons. They increase blood flow, break up scar tissue, and wake up the body’s repair process (Sleppy Chiropractic, n.d.).
MLS laser therapy: Safe light energy gives cells more power (ATP) to reduce inflammation and speed healing at the deepest level (Sleppy Chiropractic, n.d.).
Spinal decompression: Gentle stretching creates space between vertebrae. This relieves pressure on bulging discs, allows nutrient-rich fluid to flow in, and helps discs rehydrate and repair (Sleppy Chiropractic, n.d.).
These therapies help stop the cycle of chronic pain. They reduce swelling, support new tissue growth, and strengthen the areas that hold the spine in place. Many patients notice reduced pain and improved mobility within weeks when these treatments are used as part of a comprehensive plan.
How Chiropractic and Regenerative Therapies Work Together
The real power comes when the two approaches work together. Chiropractic adjustments create the right alignment so new tissue can form correctly. Regenerative treatments create a healing environment within tissues so that repairs last (El Paso Back Clinic, n.d.).
Here is how the full plan usually flows:
First, a careful exam and imaging find the exact problems.
Chiropractic adjustments straighten the frame and improve motion.
Regenerative injections or shockwave therapy target the damaged soft tissues and nerves.
Spinal decompression and soft-tissue work (such as massage or rehab exercises) reduce daily stress and protect healing areas.
Functional medicine support — nutrition, sleep, and inflammation control — helps the whole body recover.
One clinical observation notes, “When regenerative injections and chiropractic care happen together, the results often last longer. The injections create a better healing environment inside the tissues. The adjustments keep the joints moving correctly so that new tissue forms properly and does not become stressed again” (El Paso Back Clinic, n.d.).
Another insight suggests that a combined approach using chiropractic care, spinal decompression, regenerative injections, and supportive therapies, such as shockwave and laser therapy, often works better. These treatments create both mechanical and biological conditions that help the body heal and maintain better alignment (Personal Injury Doctor Group, 2026).
Patients often report meaningful drops in pain, better strength, and the ability to return to work or activities they enjoy. The goal is not just short-term relief. It is lasting repair that helps people avoid surgery and strong medications.
Expert Multidisciplinary Care in El Paso, Texas
In El Paso, this type of care happens in a true team setting. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, brings over 30 years of chiropractic experience plus his training as a board-certified family nurse practitioner. His clinical observations show that patients with old injuries, car accident damage, sciatica, and posture-related spine pain improve when care targets both tissue repair and nervous system function. He sees people regain mobility, reduce chronic pain, and return to daily life through personalized, non-invasive plans that combine adjustments, regenerative therapies, rehabilitation, and functional medicine support (Dr. Alexander Jimenez, n.d.; Injury Medical Clinic PA, n.d.).
Working alongside him is Dr. Maria Guadalupe Cardenas, MD. She is a board-certified internal medicine physician (NPI #1164426749, Texas MD License #J2933) with over 40 years of experience. She serves as medical director and collaborative physician at Injury Medical Clinic PA. In this multidisciplinary setup — common in integrative and injury care clinics — the MD provides medical oversight, ensures procedural safety, reviews complex health factors, and adds an internal medicine perspective. Dr. Jimenez delivers the hands-on chiropractic and regenerative care. Together with functional medicine, personal injury documentation, and rehabilitation services, the team creates one coordinated plan under one roof.
This collaboration means patients receive complete care. The structural work (chiropractic), the biological repair (regenerative therapies), and the medical guidance all support each other. It is especially helpful for people with personal injuries, sciatica, chronic back pain, or posture problems that have not fully healed with other approaches.
Breaking the Pain Cycle and Rebuilding Strength
Poor posture or old injuries often create a cycle: misalignment stresses soft tissues, tissues become inflamed or torn, pain limits movement, and weakness worsens. The combined approach breaks this cycle at every level.
Chiropractic restores alignment and motion. Regenerative therapies heal and strengthen the supporting tissues. Decompression and soft tissue care protect the repairs from daily stress. Over time, many people feel less pain, stand taller, move more freely, and enjoy activities again.
This path focuses on root causes instead of just masking symptoms. It supports the body’s natural ability to heal while giving it the right tools and environment to succeed.
If ongoing spine pain is limiting your life, learning more about this integrative approach may open new options. Many people in El Paso and surrounding areas have found real relief and lasting improvement through careful, combined care that repairs the spine from the inside out.
Speeding and Aggressive Driving Motor Vehicle Accidents: Causes, Dangers, and How Integrative Care Supports Recovery
Speeding and aggressive driving cause thousands of serious crashes every year. These collisions occur when drivers ignore traffic laws, putting other people’s safety at risk. The results often include painful injuries to the neck, back, and spine that can last for months or years if not treated properly.
This article explains what these dangerous behaviors are, why they happen, and the real risks they create. It also shows how integrative chiropractic clinics use a team approach to help people heal from the physical damage these crashes cause. Understanding the problem is the first step. Knowing your recovery options is next.
What Are Speeding and Aggressive Driving?
These terms describe different but related problems on the road.
Speeding means driving faster than the posted speed limit or faster than conditions safely allow. This includes going too fast in heavy rain, at night, or on wet roads. Nearly one in three traffic deaths across the country involves speeding. It remains one of the most common and deadly driving mistakes.
Aggressive driving is a pattern of moving violations that endanger other drivers or property. The National Highway Traffic Safety Administration describes it as a combination of two or more risky actions, such as tailgating, improper passing, running red lights, or weaving through traffic. These behaviors show a clear disregard for the rules and for other people’s safety.
Road rage is different. While aggressive driving is a traffic violation, road rage involves intentional violent acts with a vehicle or weapon. It often starts from a traffic dispute but turns into a criminal assault. Examples include ramming another car or forcing someone off the road.
Why Do These Crashes Happen?
Most people do not plan to drive dangerously. Several common factors push drivers into these behaviors:
Feeling rushed or late for work, appointments, or family obligations
Frustration from sitting in traffic congestion
The feeling of being anonymous inside a vehicle, which can lower normal social inhibitions
Stress from daily life that spills over into driving
Traffic jams are a major trigger. Drivers may make sudden lane changes or accelerate to pass slower vehicles, creating dangerous situations for everyone nearby.
When these actions combine with high speed, reaction time drops sharply. A driver going much faster than surrounding traffic has far less time to stop or steer away from trouble.
The Real Hazards of Speed and Aggression
Higher speeds make crashes much more severe. The chance of dying or suffering serious injury rises quickly as speed increases. Research shows this risk can double for every 10 miles per hour over 50 mph. At higher speeds, the force of impact grows dramatically, and safety features like guardrails and seat belts become less effective at protecting people.
Aggressive moves such as tailgating and erratic lane changes further reduce the time everyone has to react. These crashes often produce stronger forces on the body, leading to more serious damage to muscles, ligaments, discs, and nerves.
In Texas and across the country, officials track these behaviors because they contribute to a large share of serious injury and fatal crashes. Resources from the Texas Department of Insurance and the Governors Highway Safety Association offer practical tips for staying safe and reporting dangerous drivers.
Common Injuries After Speeding and Aggressive Driving Crashes
High-impact collisions frequently cause:
Whiplash and neck strain
Herniated or bulging discs in the spine
Soft tissue damage to muscles, tendons, and ligaments
Pinched nerves that send pain, numbness, or tingling into the arms or legs
Joint injuries in the shoulders, hips, or back
These injuries can feel minor at first but often worsen over days or weeks. Without proper care, scar tissue can form, leading to long-term stiffness, chronic pain, and reduced mobility.
How Integrative Chiropractic Clinics Support Healing
Integrative clinics focus on restoring the body’s natural function rather than masking symptoms. They combine structural care with advanced tissue repair therapies. This approach helps people recover from the specific trauma caused by high-speed and aggressive driving crashes.
At Injury Medical Clinic PA (also known as El Paso Back Clinic) in El Paso, Texas, care is built around a multidisciplinary model. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, brings more than 30 years of experience treating thousands of patients with neck, back, and soft-tissue injuries resulting from car accidents. His clinical observations show that combining precise chiropractic adjustments with regenerative and rehabilitative therapies often helps patients regain mobility and reduce pain while lowering the chance of long-term problems.
Dr. Maria Guadalupe Cardenas, MD, a board-certified internal medicine physician with over 40 years of experience (NPI #1164426749, Texas MD License #J2933), serves as Medical Director and Collaborative Physician. She provides medical oversight for the entire care team. This setup is common in integrative injury clinics. The MD ensures that treatments are safe for patients with other health conditions, while the chiropractor focuses on alignment and nervous system function. Together with functional medicine, personal injury documentation, and rehabilitation services, the team creates personalized plans that address both the immediate injury and the whole person.
Specific Therapies Used for High-Impact Accident Recovery
Clinics like this one use several proven methods together:
Spinal Decompression gently creates negative pressure in the spine. This helps relieve pressure on compressed discs and pinched nerves in the neck and back, easing both local and radiating pain.
MLS Laser Therapy uses specific wavelengths of light to support cellular repair. It can reduce inflammation and calm damaged soft tissues without surgery or drugs.
Shockwave Therapy delivers deep acoustic waves to injured muscles and tendons. It helps break up painful scar tissue and encourages fresh blood flow to the area, speeding the body’s natural repair process.
Regenerative Therapies (PRP, PFP, and MFAT) use the patient’s own healing elements. Platelet-Rich Plasma (PRP) and Platelet-Poor Plasma (PFP) concentrate growth factors from blood to support ligament and tendon repair. Micro-Fragmented Adipose Tissue (MFAT) uses processed fat tissue to provide cushioning and healing signals to damaged joints. These treatments are especially beneficial after the forceful impacts common in speeding-related crashes.
Epidural Spinal Injections, administered under direct medical supervision, deliver anti-inflammatory medication to the area around irritated nerves. They can calm severe spinal inflammation when other steps need extra support.
IV Infusion Therapy delivers hydration, vitamins, and minerals straight into the bloodstream. This supports the body’s internal healing environment and helps combat the fatigue that often follows major trauma.
Chiropractic Care uses targeted manual adjustments to restore proper joint movement, ease nervous system stress, and improve range of motion. It forms the foundation for structural recovery.
When these therapies work together under coordinated medical and chiropractic oversight, many patients experience faster relief and better long-term function.
Why a Team Approach Matters
Recovering from injuries caused by speeding or aggressive drivers is rarely simple. Pain in one area can affect posture, sleep, and daily movement. An integrated team addresses these connections.
Dr. Cardenas’s medical direction helps guide care for patients with complex health histories. Dr. Jimenez’s dual training as a chiropractor and nurse practitioner allows seamless blending of structural correction with functional and rehabilitative strategies. The result is care that treats the whole injury, not just the painful spot. Early intervention is especially important because it can limit scar tissue formation and help prevent chronic pain patterns.
Staying Safe and Starting Recovery
Prevention remains the best protection. Simple habits help: leave extra space in front of your vehicle, avoid tailgating, use turn signals, and manage stress before getting behind the wheel. If another driver acts aggressively, do not engage. Stay calm, keep distance, and report serious threats to authorities when it is safe.
If you have already been in a crash involving speeding or aggressive driving, even a “minor” one, get evaluated promptly. Delayed symptoms are common with whiplash and spinal injuries. A thorough assessment can catch problems before they become harder to treat.
Integrative clinics in El Paso and similar communities offer coordinated care that combines chiropractic precision, regenerative support, and medical oversight. This approach gives many people a clearer path back to comfortable movement and daily life.
Car Accident Shoulder and Arm Injury Care in El Paso
Motor vehicle accidents happen suddenly and can have a lasting impact on your body. Seatbelts save lives, but the forces involved often cause arm and shoulder injuries. These problems range from strains that heal with time to more serious tears that affect work, sleep, and daily activities. At El Paso Back Clinic, patients receive caring, complete support to address these injuries and get back to feeling like themselves.
This guide explains common arm and shoulder injuries from car crashes, why they occur, which symptoms to watch for, and how an integrative approach can help with healing. The focus is on clear, practical steps for recovery right here in El Paso.
How Car Accidents Lead to Shoulder and Arm Problems
In a crash, your body stops or changes direction rapidly. Seatbelts hold you in place but can press hard across the shoulder. Your arms may hit the steering wheel, dashboard, or door. Bracing for impact by gripping the wheel tightly adds strain. Even whiplash from the neck can send pain into the shoulders and arms.
Main causes include:
Direct impact from inside the vehicle.
Seatbelt restraint pulling on the shoulder.
Sudden jarring or twisting motions.
Airbag deployment or bracing reactions.
The shoulder is a complex ball-and-socket joint. It allows a wide range of motion but becomes vulnerable in accidents. At El Paso Back Clinic, experts understand these patterns and create personalized plans for El Paso residents and visitors.
Common Types of Injuries After a Crash
A diverse array of arm and shoulder injuries results from auto accident trauma. The precise nature of the harm depends on how the body is jolted and where impact occurs.
Rotator Cuff Tears: These involve the muscles and tendons that stabilize the shoulder. Tears cause pain when lifting the arm, weakness, and nighttime discomfort. Partial or full tears are common in crashes.
Fractures: The collarbone, upper arm bone, or shoulder blade can break. Symptoms include sharp pain, swelling, and trouble moving the arm. Proper imaging and care are essential.
Dislocations and Instability: The upper arm bone may shift out of the socket. This leads to severe pain and limited motion. Follow-up care prevents future problems.
Sprains, Strains, and Soft Tissue Damage: Ligaments, muscles, and tendons can stretch or tear. Bruising and inflammation add to the pain. Nerve irritation may cause numbness or tingling down the arm.
Early diagnosis at a local clinic like El Paso Back Clinic helps prevent small issues from becoming long-term problems.
Symptoms That Should Not Be Ignored
Pain might not show up immediately due to the body’s stress response. Delayed symptoms are very common.
Typical warning signs:
Aching or sharp pain in the shoulder or upper arm.
Weakness or difficulty raising the arm.
Swelling, bruising, or stiffness.
Clicking or grinding feelings during movement.
Pain that worsens at night or with overhead activities.
Numbness or tingling in the arm or hand.
If these appear after an accident, seek evaluation soon. Prompt care supports better healing and stronger documentation for insurance or personal injury needs.
Comprehensive Care at El Paso Back Clinic
Motor vehicle accidents frequently result in arm and shoulder trauma. These collisions can lead to debilitating pain that needs multifaceted treatment. El Paso Back Clinic offers a full continuum of care by blending chiropractic adjustments with advanced regenerative and supportive therapies.
Chiropractic Adjustments: Gentle, precise movements realign the spine and joints. This reduces pressure on nerves, eases muscle tension, and improves overall mobility—key for accident recovery.
Regenerative and Advanced Therapies
Platelet-Rich Plasma (PRP), Platelet-Fibrin Products (PFP), and Microfragmented Adipose Tissue (MFAT) use the body’s own materials to promote natural repair.
Shockwave therapy, MLS laser therapy, spinal decompression, Graston technique, and cupping reduce inflammation and support tissue healing.
IV infusion therapies deliver nutrients to speed recovery.
Targeted injections and physical rehabilitation rebuild strength and function.
This integrative model works well for personal injury cases common in El Paso, including whiplash, work-related issues, and auto accidents.
Collaborative Medical Leadership in El Paso
At Injury Medical Clinic PA / El Paso Back Clinic, care is provided by a coordinated team. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CCST, CFMP, IFMCP, ATN, leads with deep experience in chiropractic and advanced practice. His clinical insights emphasize whole-person recovery that addresses root causes rather than just symptoms.
Dr. Maria Guadalupe Cardenas, MD (Board Certified in Internal Medicine, NPI #1164426749, Texas MD License #J2933), with over 40 years of experience, serves as Medical Director and Collaborative Physician. This multidisciplinary setup is standard in quality integrative clinics. The MD provides medical oversight and internal medicine expertise, while chiropractic and regenerative services focus on alignment, repair, and rehabilitation. The team also supports functional medicine, personal injury documentation, and tailored rehab plans for patients in El Paso.
Patients benefit from convenient, comprehensive care at one location in El Paso, Texas—reducing the need to visit multiple offices.
Steps Toward Better Recovery
Healing takes patience, but the right support makes it achievable. Many people at El Paso Back Clinic regain strength and comfort through consistent care.
Practical tips for recovery:
Follow your personalized treatment plan.
Do recommended home exercises to maintain progress.
Use ice or heat as advised for pain and swelling.
Eat nutrient-rich foods and stay hydrated.
Communicate openly with your care team about progress or concerns.
Whether your injury is recent or lingering from an older crash, integrative options can help when standard approaches plateau.
Moving Forward After an Accident in El Paso
Shoulder and arm injuries from car accidents are common but manageable with expert help. El Paso Back Clinic combines proven chiropractic methods with modern regenerative therapies to support cellular repair, relieve pain, and restore function.
If you or someone you know is dealing with post-accident shoulder or arm pain, reach out to the team at El Paso Back Clinic. Their experienced staff understands local needs and focuses on getting patients back to the activities they love. Early action often leads to the best outcomes.
Contact El Paso Back Clinic today to schedule an evaluation and start your personalized recovery journey.
How PRP Therapy, Chiropractic Adjustments, and Spinal Decompression Can Help Fix Poor Posture Issues in El Paso, TX
Poor posture is a common problem for many adults. Long hours at a desk, looking down at phones, past injuries, or even stress can pull the body out of alignment. Over time, this extra stress does more than cause discomfort. It can weaken muscles, tighten ligaments, and create small tears in the tissues that support the spine.
When these supporting structures break down, it becomes harder to hold good posture without pain or fatigue. Simple stretches or exercises may not be enough if the underlying tissues are damaged. That is where a combined approach using regenerative treatments, chiropractic care, spinal decompression, and supportive therapies can make a real difference. These methods work on both the mechanical alignment of the spine and the biological repair of the tissues that hold everything in place.
How Poor Posture Affects Muscles and Ligaments
Poor posture places uneven pressure on the spine and surrounding tissues. Muscles that should stay balanced often become tight on one side and weak on the other. Ligaments, the strong bands that connect bones and stabilize joints, can stretch beyond their normal range or develop tiny tears from ongoing strain.
This creates a cycle. Weak or damaged tissues make it difficult to maintain proper alignment. The body then compensates with increased tension or guarding, leading to greater pain and stiffness. Many people notice neck tension, low back ache, headaches, or radiating discomfort that makes daily activities harder.
Research on posture and spinal health shows that these changes in muscles and ligaments often contribute to ongoing instability (Darlington Chiropractic Care, n.d.; Square One Health, n.d.). Without addressing both the alignment and the tissue health, progress can stall.
Regenerative Medicine Options Such as PRP Therapy
Regenerative treatments focus on helping the body repair itself at the tissue level. Platelet-Rich Plasma (PRP) therapy is one common option. It uses a small sample of the patient’s own blood, which is processed to concentrate platelets and growth factors. When injected near damaged ligaments or spinal tissues, these concentrated elements send signals that encourage natural healing and new tissue growth.
Similar approaches include Platelet-Free Plasma (PFP) and micro-fragmented adipose tissue (mFAT or MFAT) from the patient’s own fat. These provide growth factors or a natural scaffolding that supports repair in areas worn down by long-term poor posture.
The goal is to strengthen the ligaments so they can better hold the vertebrae in proper position. This biological support is especially helpful when pain or tissue damage has made it difficult to maintain proper alignment through exercise or adjustments alone (Apex Biologix, n.d.; El Paso Chiropractor Blog, 2026).
Chiropractic Adjustments for Better Spinal Alignment
Chiropractic care uses precise, hands-on techniques to gently move vertebrae and joints back toward better alignment. This restores normal motion, reduces pressure on nerves, and helps tight muscles relax. Adjustments also improve the body’s sense of position, called proprioception, making it easier to maintain optimal posture without constant conscious effort.
When tissues are supported by regenerative treatments, chiropractic adjustments often hold their results longer. The mechanical correction works together with the biological repair occurring in the ligaments and muscles (Apex Biologix, n.d.; Darlington Chiropractic Care, n.d.).
Spinal Decompression Therapy
Spinal decompression uses a gentle, controlled pulling force to create more space between the vertebrae. This relieves pressure on bulging discs, pinched nerves, and irritated structures that often result from years of poor posture or compression.
Improved space allows better fluid movement and nutrient flow into the discs. Many patients report that it reduces radiating pain or sciatica-like symptoms, making it easier to participate in rehabilitation and daily movement. Decompression pairs well with other therapies because it relieves pressure on the spine while regenerative treatments promote tissue repair (El Paso Chiropractor Blog, 2026; Square One Health, n.d.).
Supportive Therapies: Shockwave and MLS Laser
Two advanced modalities often enhance results. Shockwave therapy delivers targeted sound waves that increase blood flow, break down scar tissue, and stimulate the body’s repair processes. It is frequently used to “prime” an area before PRP injections or to continue remodeling tissue afterward.
MLS laser therapy uses specific wavelengths of light to reduce inflammation and swelling while boosting cellular energy to support healing. It is particularly beneficial after regenerative injections or adjustments to keep post-treatment soreness low and speed overall recovery. Together, these therapies create a more favorable environment for the main treatments to succeed (CELasers, n.d.; OSpine Medical, n.d.; Carolina Non-Surgical Ortho, n.d.).
How the Therapies Work Together for Better Outcomes
No single treatment fixes posture by itself. The power comes from combining them in a thoughtful sequence.
Regenerative injections such as PRP first deliver growth factors directly to weakened ligaments and damaged tissues. This initiates the biological repair process, allowing the structures that support the spine to become stronger and more stable.
Chiropractic adjustments then provide the mechanical realignment, helping vertebrae sit in better positions while the tissues heal. Spinal decompression creates the necessary space and reduces nerve pressure, allowing the regenerative signals to work without constant compression interfering.
Shockwave therapy improves circulation and tissue responsiveness, helping the PRP or similar treatments reach their full effect. MLS laser therapy calms any temporary inflammation from injections or adjustments, so patients can stay consistent with care and rehabilitation.
Epidural injections may be added in cases of severe nerve inflammation or radiating pain. They calm irritated nerves enough for the patient to safely engage in adjustments, decompression, and exercises.
The result is a supportive environment where the body can heal both structurally and biologically. Patients often report less daily pain first, followed by easier movement and a gradual return to better posture that requires less effort to maintain. This integrated approach is especially useful when underlying tissue damage has made it difficult to progress with conservative care alone (Personal Injury Doctor Group, 2026; El Paso Chiropractor Blog, 2026).
Integrated Care at Injury Medical Clinic in El Paso
At Injury Medical Clinic PA in El Paso, Texas, patients have access to this type of coordinated care under one roof. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, and CCST, brings extensive clinical experience in chiropractic care, regenerative procedures, functional medicine, personal injury support, and rehabilitation. His observations show that many people with posture-related pain from desk work, old injuries, or daily habits benefit when both alignment and tissue health are addressed together.
Working closely with him is Dr. Maria Guadalupe Cardenas, MD, a board-certified internal medicine physician with over 40 years of experience. She serves as Medical Director and Collaborative Physician at the clinic (NPI #1164426749, Texas MD License #J2933). Her role provides medical oversight and direction, ensuring comprehensive evaluation and safe coordination of care.
This collaboration between chiropractic and regenerative expertise (Dr. Jimenez) and internal medicine leadership (Dr. Cardenas) is a common model in integrative and injury-focused clinics. The team also incorporates functional medicine, rehabilitation, soft tissue work, and detailed documentation for personal injury or insurance needs. Patients receive personalized plans that consider the whole picture—structural alignment, tissue repair, inflammation control, and overall function—rather than isolated treatments (El Paso Chiropractor Blog, 2026; LinkedIn pulse on integrated injury care, n.d.; DrAlexJimenez.com, n.d.).
What to Expect from a Combined Treatment Plan
Care usually begins with a thorough evaluation, including a history, an examination, and any necessary imaging or tests. The team then designs a plan that may include regenerative injections, a series of chiropractic adjustments, decompression sessions, shockwave or laser therapy, and guided rehabilitation exercises for posture and core strength.
Progress is monitored closely. Many people notice reduced pain and stiffness within the first few weeks, with continued improvement in mobility and posture comfort over several months. Results vary based on the severity of tissue damage, overall health, and consistency with home exercises and ergonomic changes. The goal is lasting functional improvement, not just temporary relief.
Taking Steps Toward Better Posture and Comfort
Poor posture can create a frustrating cycle of pain and limitation, but addressing both the mechanical alignment of the spine and the biological health of supporting tissues offers a promising path forward. Therapies like PRP and related regenerative options, combined with chiropractic adjustments, spinal decompression, shockwave, and MLS laser therapy, work together to create the conditions the body needs to heal and maintain better alignment.
In El Paso, the integrated team at Injury Medical Clinic PA, led by Dr. Alex Jimenez and under the medical direction of Dr. Maria Guadalupe Cardenas, provides a multidisciplinary approach for patients dealing with posture problems, personal injuries, and related spinal concerns. If ongoing posture discomfort is affecting your daily life, exploring these combined options with experienced providers may help you move toward lasting relief and improved function.
Sciatica Pain Relief: How PRP, PFP, mFAT, and Regenerative Epidurals Help Heal Your Spine
If you feel sharp pain shooting down one leg, tingling in your foot, or weakness that makes standing or walking difficult, you may be dealing with sciatica. This happens when something in the lower back presses on or irritates the long sciatic nerve that runs from the spine down each leg. Common causes include bulging or torn spinal discs, tight or damaged ligaments, or swollen tissues that pinch the nerve.
The body wants to heal these problems. However, spinal discs and ligaments have very poor natural blood flow. Healing signals move slowly, and inflammation can last a long time. Treatments such as PRP, Platelet-Fibrin Products (PFP), mFAT, and certain epidural injections deliver concentrated help straight to the irritated areas. They calm nerve inflammation and support the repair of the discs and ligaments that keep the sciatic nerve aggravated.
In El Paso, Texas, Dr. Alexander Jimenez, DC, APRN, FNP-BC, CCST, CFMP, IFMCP, ATN, and his team at Injury Medical Clinic PA use these options as part of a full care plan. They work closely with Dr. Maria Guadalupe Cardenas, MD, a board-certified internal medicine physician with over 40 years of experience (NPI #1164426749, Texas MD License #J2933). She serves as Medical Director and Collaborative Physician, providing medical oversight for safety and whole-person health. This team approach combines chiropractic care, functional medicine, personal injury support, rehabilitation, and regenerative procedures under one roof.
Here is how each treatment works and why combining them with chiropractic care often brings better, longer-lasting results.
PRP Injections: Your Body’s Own Healing Cells at Work
PRP stands for Platelet-Rich Plasma. A small sample of your blood is centrifuged to concentrate the platelets. These platelets release natural growth factors—proteins that tell the body to reduce swelling and start repair. The concentrated PRP is then injected near the irritated sciatic nerve or into damaged disc or ligament areas, often with image guidance for precision.
The growth factors help lower inflammation around the nerve, support repair of small tears in spinal discs, and aid nerve recovery. Many people experience longer pain relief compared with traditional steroid shots because PRP works on the actual tissue damage instead of only masking symptoms. It is considered very safe because it uses your blood components.
Key benefits of PRP for sciatica include:
Reduces nerve root inflammation
Supports disc and ligament healing
Often provides relief that lasts longer than steroids alone
Minimally invasive with low risk of side effects
Patients frequently notice gradual improvement over weeks to months as the tissues stabilize and the pressure on the sciatic nerve decreases (Naples Regenerative Institute, n.d.; Integrative Rehab Medicine, n.d.).
PFP: A Natural Scaffold for Steady, Long-Term Support
PFP, or Platelet-Fibrin Products, builds on PRP by adding something extra. It forms a natural, gel-like “scaffold” or framework from components in your blood. Once placed in the damaged area, this scaffold slowly and steadily releases healing growth factors.
Think of it as a built-in slow-release system. Instead of a one-time burst of signals, the scaffold provides ongoing support to ligaments and discs that have been stretched, torn, or weakened. This sustained action helps restore structure and strength in the tissues that may be rubbing or pressing on the sciatic nerve.
PFP is especially beneficial when longer-term tissue rebuilding is needed. It provides a supportive environment while the body works to repair itself (Health Coach Clinic, n.d.).
mFAT: Using Your Own Fat Tissue for Cushioning and Repair
mFAT stands for Microfragmented Adipose Tissue. A small amount of fat is gently taken from an area such as the abdomen or thigh through a minor procedure. The fat is then cleaned and broken into tiny pieces that can be injected into worn or degenerated areas of the spine or nearby joints.
Fat tissue naturally contains special repair cells and supportive factors. When processed into microfragments, these cells and signals can act as both a protective cushion and active helpers. They help calm long-term inflammation and support rebuilding of damaged discs or joints.
mFAT is often chosen for cases where discs or joints have worn down over the years. It delivers cushioning plus regenerative signals in one treatment. Improvement can appear gradually over several weeks to months as inflammation decreases and tissue quality improves (Fu & Wang, 2025; University of Iowa Health Care, n.d.).
Common advantages of mFAT include:
Uses your own tissue
Provides both cushioning and repair support
Helps with chronic inflammation in degenerated areas
Minimally invasive alternative to more aggressive options
Traditional Epidural Injections vs. Regenerative Epidurals
Epidural injections place medicine into the space surrounding the spinal nerves.
Traditional epidurals usually contain a corticosteroid (strong anti-inflammatory) and a numbing medicine. They work quickly to shrink swelling around irritated nerve roots. This can bring fast relief from severe sciatica pain, allowing people to move more comfortably and begin other therapies. However, these shots mainly reduce symptoms. They do not repair torn discs or weakened ligaments, and repeated use can carry risks such as tissue weakening or blood sugar changes (Orthopedic Specialists of the St. Louis Region, 2026).
Regenerative epidurals take a different approach. Instead of steroids, physicians may use platelet lysate—a processed form of PRP factors—or other orthobiologics. These calm nerve inflammation while also delivering healing signals to the surrounding tissues. The goal is faster comfort plus actual support for tissue repair, without the typical downsides of repeated steroid exposure (Integrative Rehab Medicine, n.d.).
Why Combining Chiropractic Care with Regenerative Treatments Works So Well
Injections deliver powerful healing materials directly to the problem spots. Yet spinal discs and ligaments have a limited blood supply, so these tissues need help reaching deep tissues effectively. This is where chiropractic care adds important value.
Dr. Alex Jimenez performs gentle spinal adjustments to improve joint movement and alignment. These adjustments can quickly reduce mechanical pressure on the sciatic nerve caused by misaligned vertebrae or tight muscles. Better movement also increases local blood flow and nutrient delivery.
When injections and adjustments work together, the results are often stronger than either alone. The injections provide concentrated repair signals. Chiropractic care and supportive therapies (such as shockwave) improve circulation, so those signals penetrate more deeply into low-blood-flow areas like discs and ligaments. This combination addresses both the mechanical pressure on the nerve and the biological inflammation and tissue damage.
Dr. Jimenez’s clinical observations from helping thousands of patients with back and leg pain show that this integrated method helps many people move better and experience lasting relief. It focuses on restoring function rather than only covering symptoms.
At Injury Medical Clinic PA in El Paso, this care happens in a true multidisciplinary setting. Chiropractic expertise from Dr. Jimenez pairs with medical oversight from Dr. Maria Guadalupe Cardenas, MD. As an experienced internist and Medical Director, she ensures procedures are appropriate for each person’s overall health, coordinates with other treatments, and supports safe, personalized plans. The team also includes functional medicine, personal injury documentation and care, and rehabilitation services—all working together for comprehensive support.
A Clear Path Forward
Sciatica does not have to mean ongoing pain or limited activity. By calming inflammation, supporting tissue repair, and restoring proper spinal mechanics, these treatments help the body overcome its natural healing challenges in the spine.
Many people in El Paso and surrounding areas have found meaningful improvement through this combined approach. A careful evaluation, including history, exam, and any needed imaging, helps determine the best starting plan for your specific situation.
If sciatica is affecting your daily life, work, or sleep, consider reaching out to a team experienced in both regenerative injections and integrative chiropractic care. The goal is simple: help your spine heal so the sciatic nerve can calm down and you can return to the activities you enjoy.
Hip Injuries in Motor Vehicle Accidents: Understanding the Trauma and Finding Healing
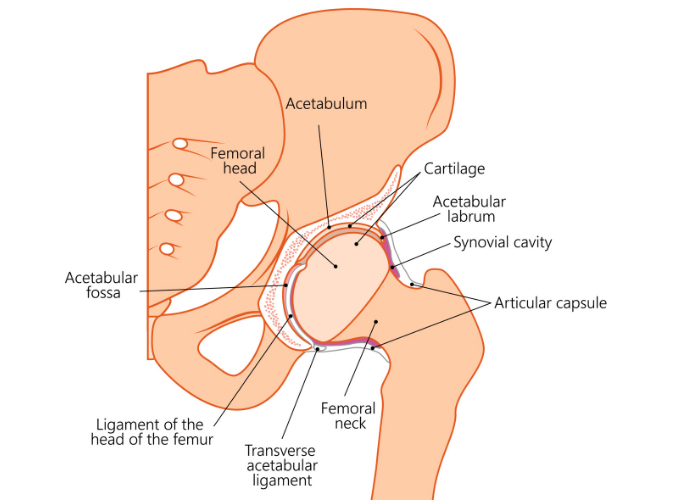
Car accidents send powerful forces through the body in seconds. The hips often absorb much of that energy because they connect the legs to the pelvis and spine. Even when the crash does not look severe, hip injuries can appear right away or develop days later. These injuries range from bone fractures and dislocations to tears in soft tissues such as cartilage and muscle.
The hip works as a ball-and-socket joint. The ball is the rounded top of the thigh bone. The socket is a deep cup in the pelvis. Strong ligaments and muscles, along with a ring of special cartilage called the labrum, keep the joint stable and smooth. It takes considerable force to damage this sturdy setup. That is why hip problems after a crash are often serious and need careful attention.
Understanding what can happen helps you know when to seek care and what options are available for recovery.
Common Hip Injuries from Motor Vehicle Accidents
The exact injury often depends on body position at impact. Legs braced, knees hitting the dashboard, or side forces from a T-bone crash all create different patterns of damage.
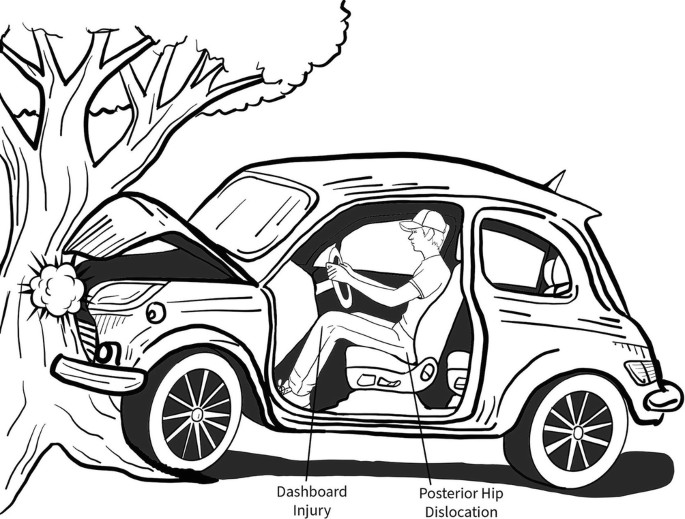
A classic dashboard injury happens in head-on crashes. The knee slams forward into the dashboard. This drives the thigh bone backward and pops the ball out of the socket. This is called a posterior hip dislocation. It causes immediate, severe pain. The leg may look shorter or rotated. You usually cannot put weight on it (American Academy of Orthopaedic Surgeons, n.d.).
Quick medical help is needed to put the joint back in place. Even after reduction, the labrum, ligaments, or blood supply to the ball can be damaged. Some people later face arthritis or bone death in the ball if blood flow is interrupted.
Acetabular Fractures
The socket itself can crack or shatter. High-energy dashboard hits or side impacts drive the ball forcefully into the cup. These breaks change the smooth surface the ball glides on. Many need surgery to restore the socket shape so the joint moves correctly again (OrthoInfo – AAOS, n.d.).
Femoral Head Fractures
The ball on top of the thigh bone can crack, crush, or break into pieces. This often occurs with a dislocation from the same dashboard force. The ball shears against the socket rim as it pops out or gets driven back in. These injuries raise the risk of long-term joint problems.
Labral Tears
The labrum is the cartilage rim that deepens the socket and helps seal joint fluid. A sudden dislocation, twist, or even strong bracing against the floor or seatbelt can tear it. People experience groin pain, clicking or catching, or a sensation that the hip gives way. Pain often worsens with sitting, walking, or twisting (Mayo Clinic, n.d.).
Muscle Strains, Sprains, and Soft Tissue Damage
Not every injury breaks a bone. Violent jerking or bracing can strain the hip flexor muscles or sprain ligaments around the joint. Seatbelt pressure or direct impact can inflame the bursa (a fluid-filled sac) on the side of the hip, causing trochanteric bursitis. These bring pain with movement, swelling, stiffness, and weakness. They heal more slowly when walking patterns are avoided due to pain (High Mountain Orthopedics, n.d.).
Why These Injuries Matter Long-Term
The hip joint is deep and well-protected, but damage here can affect walking, standing, and balance. Untreated dislocations or fractures can lead to arthritis years later. Labral tears and chronic muscle imbalance change how you move and stress the low back, knees, and opposite hip. Early care reduces these risks.
Doctors diagnose with physical exams plus imaging. X-rays show bone position and breaks. CT scans give detailed fracture pictures. MRI reveals labral tears, muscle damage, and soft tissue injury.
How Integrative Chiropractic Care Supports Recovery
Many hip injuries, especially soft-tissue and labral problems, or those requiring support after initial bone care, respond well to non-surgical approaches. An integrative chiropractic clinic combines hands-on structural work with regenerative therapies that use your body’s own healing tools. The goal is to reduce inflammation, repair tissue, and restore smooth movement without surgery when possible.
Chiropractic adjustments gently realign the pelvis, spine, and hip. This improves joint motion, eases tight muscles, and reduces nerve irritation. Better alignment helps blood flow and healing signals reach the injured area more effectively.
Regenerative therapies add biological support:
PRP (Platelet-Rich Plasma): A small amount of your blood is spun to concentrate platelets rich in growth factors. The concentrate is injected into the hip area to signal repair in tendons, ligaments, the labrum, and cartilage while calming inflammation.
PFP (Platelet-Fibrin Products): Similar to PRP but includes fibrin for slower, longer release of healing factors. This gives sustained support during recovery.
MFAT (Microfragmented Adipose Tissue): A tiny amount of your fat tissue is processed into micro pieces containing healing cells and natural cushioning material. It is injected to support regeneration and provide padding in the joint or around damaged tissues.
These injections are often guided by ultrasound for accuracy. When paired with chiropractic adjustments, they address both structure and biology. Adjustments keep the joint moving correctly so new tissue forms in the right pattern. Regenerative support reduces pain and swelling, so adjustments work better and last longer (Health Coach Clinic, n.d.).
Patients often notice gradual improvement over weeks as tissues rebuild. Many regain mobility and return to daily activities with less pain and lower risk of future problems.
The Collaborative Care Team
At Injury Medical Clinic PA in El Paso, Texas, care is built on teamwork. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, brings extensive experience treating personal injury and motor vehicle accident cases. His clinical observations show that patients with hip trauma from crashes often achieve better long-term function and less chronic pain when structural corrections and regenerative support are started early. He focuses on whole-person recovery, including rehabilitation exercises and addressing posture or gait changes that develop after an accident.
Dr. Maria Guadalupe Cardenas, MD, board-certified in Internal Medicine with more than 40 years of experience, serves as Medical Director and Collaborative Physician. She provides medical oversight for the practice. This includes reviewing complex cases, ensuring safety for regenerative procedures and injections, managing any underlying medical factors that affect healing, and collaborating on care plans. This MD-DC partnership is common in quality integrative and injury clinics. It combines precise medical direction with specialized chiropractic and regenerative expertise.
The broader team integrates functional medicine, rehabilitation, and personal injury support. This multidisciplinary setup helps patients heal thoroughly by addressing root causes rather than only symptoms.
What to Expect on the Road to Healing
Recovery time depends on the type and severity of the injury. Simple strains may improve in a few weeks with adjustments and guided movement. Labral tears or post-reduction care often take several months. Regenerative injections typically show progressive benefits over 4 to 12 weeks. The focus stays on restoring comfortable movement, strength, and daily function.
Early attention matters. Waiting can allow scar tissue or changed movement patterns to set in, making later recovery harder. A thorough evaluation helps create a clear plan tailored to your injury and goals.
Moving Forward After a Crash
Hip injuries from motor vehicle accidents do not have to mean ongoing pain or major surgery. Many people regain good function through integrative care that works with the body’s natural healing abilities—proper alignment, regenerative signals from your tissues, and expert guidance every step of the way.
If hip pain continues after a car accident, consider a clinic experienced in these injuries and equipped with both structural and regenerative options. In El Paso, the team at Injury Medical Clinic PA provides this comprehensive approach. Knowing what happened to your hip is the first step toward restoring your mobility and quality of life.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine