On my first visit, I automatically felt better but along came with soreness. I did continue treatment, I saw him (Dr. Alex Jimenez) maybe two or three times out of the week. Shortly after that I started noticing change.�
Denise
The shoulder consists of a number of joints which merge together with other complex structures, including muscles, tendons and ligaments, to provide a wide range of movement in the arm, like scratching your back.
This increased range of motion, however, can cause a variety of health issues. It might lead to problems with impingement or it might even result in instability on the bony structures or the soft tissues of the shoulder. Shoulder pain might be felt continuously or it might occur through movements of the shoulder. Moreover, shoulder pain can be temporary or it might become chronic and require proper diagnosis and treatment.
The article below describes a few of the common causes of shoulder pain and discusses various treatment approaches to help improve shoulder pain. A qualified and experienced healthcare professional may be able to provide you with more information regarding your shoulder pain.
Anatomy of the Shoulder
The shoulder is a complex structure which is made up of three bones: the upper arm bone, also known as the humerus, the shoulder blade, also known as the scapula, along the collarbone, also known as the clavicle.
The head of the upper arm bone fits into a round socket on the shoulder blade, called the glenoid. A variety of ligaments, tendons and muscles then function by holding the upper arm bone. These collection of soft tissues are referred to as the rotator cuff. The main function of the rotator cuff is to both attach and cover the head of the upper arm bone in the shoulder.
Causes of Shoulder Pain
Most health issues that cause shoulder pain fall into four big categories:
Tendon inflammation, bursitis and tendinitis, or a tendon tear
Instability
Arthritis
Fracture or broken bone
Other much less common causes of shoulder pain can include factors such as tumors, disease or aggravated conditions, and nerve-related problems. Below, we will discuss the common causes of shoulder pain in detail.
Bursitis
The bursae are small, fluid-filled sacs which are found between joints throughout the entire body, including the shoulder. These function by decreasing friction between the bone and the muscles as well as act as cushions between the soft tissues and the bones.
Occasionally, excessive utilization of the shoulder can contribute to the swelling and inflammation of the bursa between the rotator cuff and a part of the shoulder blade called the acromion. The outcome measure of this health issue is a condition known as bursitis.
Bursitis often occurs in association with rotator cuff tendinitis, discussed below. The soft tissues in the shoulder can then become painful and inflamed. As a result, daily tasks, such as cleaning or brushing your hair and getting dressed, can become challenging to perform.
Tendinitis
A tendon is a cord which connects the muscles to the bones at different sites. Tendinitis is a consequence of inflammation in this soft tissue.
Ordinarily, tendinitis is frequently categorized as one of two types:
Acute. Overhead physical activities or ball projecting during a sport game or work may result in acute tendinitis.
Chronic. Degenerative diseases like arthritis or degenerative wear and tear as a result of age, may lead to chronic tendinitis.
The joints in the shoulder most commonly affected with tendinitis include the four rotator cuff tendons, particularly the shoulder tendons. The rotator cuff consists of four muscles and their respective tendons which keep the shoulder stable and protect the head of the upper arm bone. The rotator cuff provides equilibrium and shoulder movement.
Tendon Tears
The splitting and tearing of the tendons may by caused by severe damage or trauma from an injury as well as from degenerative changes in the joints due to the normal aging process, long-term overuse and the general wear-and-tear of the joints. These tears may divide the tendon completely out of its attachment or they may only be partial. Normally of tears, the tendon is entirely separated from the bone. Rotator cuff and biceps tendon injuries are among the most common types of tendon tears.
Impingement
Shoulder impingement happens when the cap of the shoulder blade, known as the acromion, places pressure on the underlying soft tissues once the arm is raised away from the torso. When the arm is raised, the acromion rubs, or “impinges” on, the rotator cuff tendons and bursa. This may result in tendinitis and bursitis, restricting motion and causing pain.
Instability
Shoulder instability occurs when the head of the upper arm bone is forced out from the shoulder socket. This can occur as a consequence of a sudden injury or even due to the excessive use of the shoulder.
Shoulder dislocations may only be partial, where only a part of the head of the upper arm may come out partially from the socket. This is also referred to as a subluxation. A complete dislocation usually means that the ball of the upper arm at the shoulder comes out all of the way from the socket.
When the ligaments, tendons, and muscles around the shoulder become torn or loose, dislocations can happen differently. Dislocations, which might be complete or partial, cause unsteadiness and pain when the arm is moved or lifted. Episodes of dislocations or subluxations result in an increased chance of developing arthritis in the shoulder joint, among others.
Arthritis
Health issues resulting in shoulder pain may also lead to arthritis. There are various kinds of arthritis. The most common kind of arthritis in the shoulder is osteroarthritis, also called the “wear-and-tear” arthritis. Osteoarthritis symptoms can include pain, stiffness and swelling which may begin during the day and may worsen throughout the day.
Osteoarthritis might also be associated with work or sports accidents as well as chronic wear-and-tear problems. Other kinds of arthritis could be linked to rotator cuff tears or an inflammation of the joint lining.
Many times, individuals who already have arthritis in the shoulder joints will attempt to prevent moving their shoulder in an effort to reduce arthritis pain and discomfort, However,�this often contributes to the stiffening or the tightening of the soft tissues surrounding the shoulder joints, leading to a painful restriction of movement.
Fracture
Fractures are frequently referred to as broken bones. Shoulder fractures commonly involve the clavicle, or the collarbone, the humerus, or the upper arm bone, and the scapula, or the shoulder blade.
Shoulder fractures in elderly patients are frequently the consequence of a fall from standing height. In the average person, harm from a motor vehicle accident or a sports accident often causes shoulder fractures.
Fractures frequently cause acute pain, swelling, and bruising concerning the shoulder. If a shoulder fracture is suspected, it’s important for the person to seek immediate medical attention by a healthcare professional.
Diagnosis for Shoulder Pain
In the instance of any of the health issues mentioned above resulting in extreme shoulder pain, seek medical attention as soon as possible to receive a proper diagnosis. While many cases of shoulder pain may resolve on their own, make sure to see a doctor if symptoms persist or worsen.
A healthcare professional will conduct a comprehensive evaluation so as to ascertain the cause of the patient’s shoulder pain before providing them with the appropriate treatment options for their health issues.
Medical History
The first step for diagnosis is a comprehensive look at the patient’s medical history. The doctor will ask how the problem has been previously treated and how the pain began, if they are aware of that information. Moreover, additional questions will help determine the causes of the patient’s shoulder pain. Since certain actions may improve or worsen symptoms, a record may be an important tool in discovering the origin of shoulder pain.
Physical Evaluation
A thorough examination will help to discover the source of a patient’s shoulder pain. A doctor will assess for tender places and will try to find physical abnormalities, swelling, deformity or muscular fatigue. They will also observe the shoulder’s strength, flexibility and movement.
Tests
The healthcare professional may additionally order certain tests to help identify the reason for the patient’s shoulder pain and help determine if the symptoms are due to other health issues. The following list demonstrates the variety of tests which can help determine the diagnosis.
X-rays. These images will reveal bone injuries.
Magnetic resonance imaging, or MRI and ultrasound. These imaging studies produce images of soft tissues. MRI can help your doctor identify injuries to the ligaments and tendons.
Computed tomography, or CT, scan. This instrument joins computer technologies and x-rays to make a better, much detailed image of the bones located in the shoulder region.
Electrical studies. The doctor may order an evaluation, including an EMG, or electromyogram, to assess neural function.
Arthrogram. In this study, dye is injected to show the joint and its surrounding soft tissues. It might be used together with an MRI.
Arthroscopy. During this procedure, a doctor looks inside the joint using a camera. Arthroscopy may reveal soft tissue injuries that aren’t apparent in evaluations along with the exam. Arthroscopy can be used to fix the problem and help find the reason for symptoms.
Dr. Alex Jimenez’s Insight
As the most mobile joint in the human body, the shoulder joint is often vulnerable to experience a variety of problems which can result in shoulder pain. Shoulder pain can tremendously affect an individual’s ability to perform everyday tasks and, if lest untreated, it can progress into neck and back pain as well as cause other severe symptoms. Understanding the cause of a patient’s shoulder pain can help diagnose their problem in order to recommend the best treatment option.
Treatment for Shoulder Pain
Chiropractic Care
Chiropractic care is a safe and effective, alternative treatment option which can help manage shoulder pain by relieving discomfort and swelling, among other painful symptoms. A chiropractor will utilize chiropractic adjustments and manual manipulations to reduce joint restrictions and correct spinal misalignments, in an effort to improve function.
Lifestyle Modifications
Furthermore, a doctor of chiropractic, or chiropractor, will recommend a series of lifestyle modifications to help promote a faster recovery process. Changing a patient’s actions through a balance of rest and physical therapeutics can help improve shoulder endurance. Avoiding overexertion can also help prevent further harm and shoulder pain.�
Drugs & Medications
A doctor may also prescribe drugs and/or medications to decrease shoulder pain and inflammation. It needs to be taken only as directed, however, if medicine is prescribed to ease pain. A physician can also recommend shots of numbing steroids to alleviate pain.
Surgery
Surgical interventions can be used to help treat the causes attributing to shoulder pain, however, it should only be considered as a last resort. A majority of patients will react positively to alternative treatment options like chiropractic care and through lifestyle modifications.�
For certain types of shoulder problems, like recurring dislocations and a few rotator cuff tears, alternative treatment options may not be recommended and surgery may be considered, in this instance.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
45 million Americans suffer headaches on a regular basis. There are the traditional methods used to treat them, which include taking over the counter medications or taking pharmaceutical concoctions to eliminate pain and reduce swelling. However, none of these solutions provide permanent relief that address the core of the problem.
Alternative Treatment
In recent years, people throughout the country are seeking alternative forms of therapy for all types of conditions, especially headaches. One treatment that is promising for physical and other types of pain is chiropractic treatment.
This form of alternative care has been used for over a hundred years and is a regular part of the American healthcare delivery system. Insurance providers are growing and are willing to pay for chiropractic because of its effectiveness.
Chiropractic school begins by studying human anatomy in great detail, like other medical professionals. In addition to looking at how the body works together physically, training primarily revolves around the diagnosis and treatment of misalignments in the spine known as subluxations.
Theses subluxations compress nerve tissue that affects organ function, soft tissue like muscle, ligaments and tendons and can eventually manifest as other health problems if not treated.
Once the nerves are disrupted pain will result. While it usually manifests itself as physical pain, this is not always the case. In some instances, the person may experience difficulties with sleep or other routine habits.
�How Does Chiropractic Help People Who Suffer From Headaches
On the first visit with a chiropractor, a review of health history will be completed. These include x-rays (if they are needed), in order to determine the type of nerve blockage that may be occurring. They will listen to the patient, make an assessment, and determine what type/s of treatment is best.
With headaches, there is usually a misalignment (subluxation) in the cervical spine. This may be accompanied by muscles that are tight in the neck, shoulders and surrounding area. Pressure on the nerves can cause sharp stabbing pain or a continual throbbing pain in the region.
The chiropractor will assess the area and then begin treatment, known as a chiropractic adjustment. The adjustment is what relieves the pressure and pain. The relief is usually instantaneous, with an increase in positive symptoms for the following few hours.
Chiropractors don�t just focus on relieving symptoms but getting to the root cause and correcting the problem. That is why additional treatments/adjustments are often required, as one adjustment is usually not enough. A chiropractor will take time to educate patients on treatment, therapy exercises, fitness, nutrition, sleep, and regular adjustments.
If you’re tired and no longer want to suffer from headaches, see how beneficial chiropractic care can be, then please give us a call to schedule an appointment!
Injury Medical Clinic:�Chiropractic Care Migraines & Headaches
Dr. Alex Jimenez has helped me a lot. The pain is less, it’s not painful. My back is able to loosen up, I’ve started to walk better and the pain is gone, not completely but it’s on its way. It’s helped me tremendously to where I couldn’t bend at times and now I can easily bend down and stretch. The sessions that I’ve been here, every time it has helped a lot. – David Garcia
Arthritis is medically defined as the inflammation of the joints, where it may affect a single or multiple joints in the body. There are over 100 kinds of arthritis, each with various causes and symptoms that may require distinct treatment procedures to relieve them. Some of the most common kinds of arthritis include osteoarthritis, abbreviated as OA, and rheumatoid arthritis, abbreviated as RA.
The signs and symptoms of arthritis generally develop gradually over time, however, they might also appear unexpectedly. Arthritis is most frequently found in older adults, mostly over the age of 65, but it may also develop in young adults, teenagers, and children. Arthritis is more common to develop in individuals that are overweight and it has been found to be more prevalent in women than in men.
What are the Symptoms of Arthritis?
Joint pain, stiffness, and swelling are the most frequent symptoms of arthritis. People with arthritis may also experience reduced range of movement as well as redness of the skin around the joint, where symptoms have been described to be worse in the daytime. In the case of RA, or rheumatoid arthritis, an autoimmune disease where the body’s own immune system attacks the joints, patients can also feel exhausted or experience a loss of appetite because of the inflammation that the immune system’s response triggers. Moreover, because RA can cause a fever, an individual’s blood cell count can drop, leading to anemia. If left untreated, deformity can be caused by severe rheumatoid arthritis.
What are the Causes of Arthritis?
Cartilage is a firm but elastic connective tissue on your joints which shields the joints from stress and pressure caused by movement. A decline in the quantity of the cartilage tissue due to age, however, can trigger some kinds of arthritis. Regular wear and tear of the joints causes OA, or osteoarthritis, among one of the most frequent types of arthritis. An injury or condition to the joints may exacerbate this breakdown of cartilage. Your risk of OA might also be greater if you’ve got a family history with the disease.
As mentioned above, another common type of arthritis, RA, is an autoimmune disease, which happens when your body’s own immune system attacks the body’s cells. These attacks often impact the tissues on your joints that produce a fluid which lubricates them and also nourishes the cartilage, the synovium. RA is a disease of the synovium which will greatly affect a joint. It may cause the destruction of cartilage and bone within the joint. The precise reason for the immune system’s attacks is still unknown.
How is Arthritis Diagnosed?
Visiting a qualified and experienced healthcare professional should be the first step to get an arthritis diagnosis. They will initially conduct a physical examination to test joints that are red or warm as well as evaluate the fluid around the joints and anaylyze restricted mobility. If necessary, a healthcare professional can refer you to another doctor for further diagnosis. If you are experiencing severe symptoms, you might need to visit a rheumatologist first.
Extracting and assessing inflammation levels in your bloodstream and joint fluids can help your doctor determine what sort of arthritis you have. Blood tests which check for particular kinds of compounds, such as anti-CCP, or anti-cyclic citrullinated peptide, RF, or rheumatoid factor, and ANA, or antinuclear antibody, can also be common diagnostic evaluations. Healthcare professionals normally utilize imaging scans like X-ray, MRI, and CT scans to check your cartilage and bones, so that they could rule out other causes of the symptoms.
Dr. Alex Jimenez’s Insight
Arthritis is commonly referred to as a group of symptoms, rather than a single disease. From pain and discomfort to swelling and inflammation, the symptoms associated with arthritis can tremendously affect an individual’s quality of life. Fortunately, a number of different types of treatment approaches are available to help manage arthritis pain. Chiropractic care can help reduce pain and discomfort, through the use of spinal adjustments and manual manipulations without the need for drugs and/or medications as well as surgery, by decreasing stress and pressure on the joints. A chiropractor may also recommend a series of lifestyle modifications to help promote healing.
What is the Treatment for Arthritis?
The most important goal of treatment is to lessen the quantity of pain you are experiencing and prevent further damage to the joints. A healthcare professional can find out what works best for you in terms of pain and they may also recommend a series of home remedies which could help you manage your pain at home. Many people with arthritis find heating pads and ice packs can help relieve symptoms. Others utilize a walking aid apparatus, such as walkers or canes, to take pressure of the joints. Enhancing the strength, mobility and flexibility of your joints is also significant. A healthcare professional may prescribe you with a combination of treatment approaches to attain the best outcomes.
By way of instance, chiropractic care and physical therapeutics can help manage painful symptoms associated with arthritis. Chiropractic care is a safe and effective, alternative treatment option which utilizes spinal adjustments and manual manipulations, among other treatment approaches, to diagnose, treat and prevent a variety of injuries and conditions affecting the musculoskeletal and nervous system, including arthritis. Spinal adjustments and manual manipulations can help reduce pain as well as decrease stress and pressure on the joints by carefully correcting any spinal misalignments, or subluxations, along the length of the spine. Furthermore, a doctor of chiropractic, or chiropractor, may recommend a series of lifestyle changes to help promote healing.
What Lifestyle Changes can Help People with Arthritis?
If you’re like the one in four older adults that suffer with arthritis symptoms, you may have already visited a healthcare professional, such as a chiropractor, to address your pain. While a doctor can help provide treatment to improve your symptoms, there are also a variety of lifestyle changes which can help promote a decrease in these often painful symptoms. Below, we will discuss several lifestyle changes which can help manage your arthritis pain at home.
First of all, since most arthritis symptoms are affected by obesity, weight loss is among the very best approaches to deal with these symptoms without the need for drugs and/or medications. Many chiropractors are proficient at engaging patients in weight loss or weight maintenance programs. Weight loss can help take pressure off the joints, ultimately decreasing pain from those joints which would have had to support more weight.
Together with weight loss, many people with arthritis, especially in the knees and feet, don’t understand how essential getting the right footwear can be for those painful symptoms. Whether it’s buying special footwear or incorporating orthotics or insoles to your shoes, this fix can help relieve the strain on the body’s joints. As an additional bonus, the footwear makes it a lot more easy to walk or engage in physical activities without pain.
In regards to arthritis pain itself, a lot of individuals find that a warm bath or heat package helps alleviate arthritis pains and aches. Other people have found that cold or ice packs can also alleviate pain and discomfort as well as implemented on a basis to decrease swelling at the joints. Alternating between both has been demonstrated to present cold’s properties to the relaxation of warmth. It’s important to consult a healthcare professional, however, regarding the proper procedures of these so as to prevent skin irritation from employing both cold and heat.
As tempting as it is to rest when you’re feeling pain and discomfort, there’s nothing better for handling arthritis symptoms than participating in exercise or physical activities on a regular basis. A lot of individuals are hesitant to start a workout program because of fear of injuring themselves or even worsening their symptoms due to arthritis. A chiropractor can show you the appropriate techniques as well as demonstrate how to utilize accessories or wraps if needed.
What is the Prognosis for People with Arthritis?
Arthritis shouldn’t keep you from living the life you deserve. The combination of appropriate treatment, such as chiropractic care or physical therapeutics, as well as the use of a weight reduction plan, proper footwear, cold and heat therapies, and the participation in exercise and physical activities, will be able to help you handle your painful symptoms.� While there is no cure for arthritis, the ideal treatment can manage your symptoms. Along with treatment, you may create numerous lifestyle changes that can improve your quality of life. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Nothing had really worked until I started seeing Dr. Alex Jimenez. The way he cares about his patients, that is what keeps on bringing me back. He does a great job and he really cares about his patients. – Araceli Pizana
Arthritis is considered to be quite a common health issue, however, it’s still not very well understood by many healthcare professionals today. As a matter of fact, arthritis isn’t a single disorder, but rather, it is an informal way of referring to joint pain or a joint disorder. There are approximately more than 100 distinct kinds of arthritis and associated problems. People of all ages, sexes and races can develop arthritis as it is the chief cause of disability in the United States. Over 50 million adults and 300,000 children have some type of arthritis while it often happens and is most common among women.
Common arthritis joint symptoms include pain, swelling and inflammation, stiffness and decreased range of movement. Symptoms of arthritis may come and go where these can range from mild, moderate or severe. They may also remain about the exact same for many years or it might advance and become worse over time. Arthritis may result in chronic pain which can make it difficult to perform tasks. Arthritis can additionally cause joint alterations. Frequently, although these modifications may be visible, such as knobbly finger joints, the extent of the health issue can be observed on x-rays. Some kinds of arthritis have an effect on skin, eyes, lungs, kidneys and the heart as well as the joints.
Common Types of Arthritis
The two most common types of arthritis which result in pain are osteoarthritis and rheumatoid arthritis. Osteoarthritis generally occurs in people over the age of 60, however, it may also be a consequence of trauma from an injury, overuse and improper body movement mechanics. This sort of arthritis is characterized by the loss of cartilage that’s responsible for lubricating joints and distributing forces of motion. When you don’t have enough of it, the bones can begin to rub together and cause pain. Moreover, bone fragments may break away and may cause bone spurs to grow.�The hands, knees, hips and back are the most common sites for osteoarthritis.
Being the most common type of arthritis, osteoarthritis is considered to be one of the most prevalent causes for chronic pain symptoms. Common causes which can ultimately increase the risk of developing osteoarthritis�include: excess weight, family history, age and previous injury, such as an anterior cruciate ligament, or ACL, tear, for instance. Osteoarthritis can be prevented by avoiding injury and repetitive movements, maintaining a healthy weight and remaining active.
Rheumatoid arthritis generally occurs when the human body’s own immune system strikes; in other words, it’s an autoimmune disease.�A healthy immune system functions by protecting the human body from intruders that can cause disease.�Researchers believe that a combination of environmental factors and genetics can cause autoimmunity. Smoking is an illustration of an ecological risk factor that can cause arthritis in people with specific genes.
Nevertheless, in the case of an autoimmune disease, the immune system may go mistakenly attacking the joints, causing uncontrolled inflammation and potentially causing erosion of the cartilage in the bones.�With this kind of arthritis, the lining of the joints become irritated and inflamed. Moreover, rheumatoid arthritis might damage other parts of the human body, including the eyes and internal organs. Symptoms include pain, swelling and soreness, inflammation, stiffness, and tenderness. Rheumatoid arthritis is found in the hands, wrists and toes, even in the hips and knees, if not treated properly. Other symptoms of rheumatoid arthritis include: fever, weight loss, diminished appetite and continual exhaustion.
While there is no cure for osteoarthritis or rheumatoid arthritis, a variety of treatment approaches can help people manage the symptoms of those afflictions. As a matter of fact, research studies have shown that chiropractic care can help manage arthritis. Chiropractic care consists of both passive and active treatment modalities. With these common types of arthritis, early diagnosis and treatment are fundamental. Slowing down the progress of the disease can help decrease and prevent permanent damage.�Remission is the goal and it might be accomplished via the utilization of a combination of therapies. The objective of treatment is to decrease pain, improve functioning, and prevent joint damage.
Through chiropractic care, a doctor of chiropractic, or chiropractor, will review goals together with the patient as well as perform a full assessment of their condition to develop a specific treatment plan to meet their individual requirements and needs. A specialized treatment program for arthritis will help manage pain and improve strength, flexibility and mobility. Below, we will discuss the types of chiropractic treatment modalities and how these can help with arthritis.
Dr. Alex Jimenez’s Insight
Before, arthritis was considered to be a natural consequence of aging, however, patients today can find a variety of treatment options to help manage the symptoms associated with this painful disease. Arthritis is simply defined as the swelling or inflammation of the joints. Osteoarthritis is the most common type of arthritis and it is most prevalent in older patients. Rheumatoid arthritis is the second most common type of arthritis, characterized as an autoimmune disease where the patient’s own immune system attacks the joints. This type of arthritis is most prevalent in younger patients. Chiropractic care is a safe and effective, alternative treatment option which can help manage the symptoms associated with arthritis.
Chiropractic Care for Arthritis Pain
Chiropractic care is a great treatment approach to manage and relieve pain caused by arthritis. Chiropractic care is a well-known, alternative treatment option which focuses on the diagnosis, treatment and prevention of a variety of injuries and conditions associated with the musculoskeletal and nervous system, including osteoarthritis and rheumatoid arthritis. Routine chiropractic care offers arthritis patients a safe and effective, non-invasive, non-addictive alternative treatment option to prescription opioids or over-the-counter pain drugs, or OTCs, that are generally given to patients to help them manage their own arthritis pain.
Chiropractic care utilizes spinal adjustments and manual manipulations, among other treatment approaches. Chiropractic spinal adjustments and manual manipulations reduce misalignments of the spine, also referred to as subluxations, as well as joint restrictions in the spinal column and other joints, improving the functioning of the bones, joints and nervous system. By enhancing your nervous system function, spinal health and increasing mobility, your body gets the ability to better manage symptoms caused by arthritis or rheumatoid arthritis. Furthermore, chiropractic care may use passive treatment methods to help manage symptoms associated with arthritis.�The passive treatment methods for arthritis are:
Transcutaneous electric nerve stimulation (TENS)
Electrical stimulation
Ultrasound
Superficial heat
Cryotherapy or ice packs
TENS can considerably help reduce pain from arthritis, tricking the brain into believing there’s no pain. Pain, muscle spasms, inflammation and soft tissue edema is reduced by electric stimulation. Ultrasound is a deep heating modality which helps deep joint tissues. It assists with swelling and inflammation as well as improving the structure of connective tissue. Heat reduces inflammation and swelling. Ice or cryotherapy packs will also be effective for arthritic pain. It’s useful for swelling and decreasing local inflammation. These passive treatment methods may be used alongside other alternative treatment options.
A doctor of chiropractor, or chiropractor, may even recommend a series of lifestyle changes to help promote healing and speed up the recovery process. If you are afflicted with pain, an exercise or physical activity program will address any impairments that could be contributing to the patient’s painful symptoms. Moreover, a chiropractor may also recommend nutritional advice. Research studies have found that some types of foods may cause pain and inflammation in arthritis patients.
Nobody should be living with pain. If you are experiencing challenges when performing daily tasks due to your arthritis pain, make sure to seek immediate medical attention from a qualified and experienced chiropractor, to achieve relief from your symptoms.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
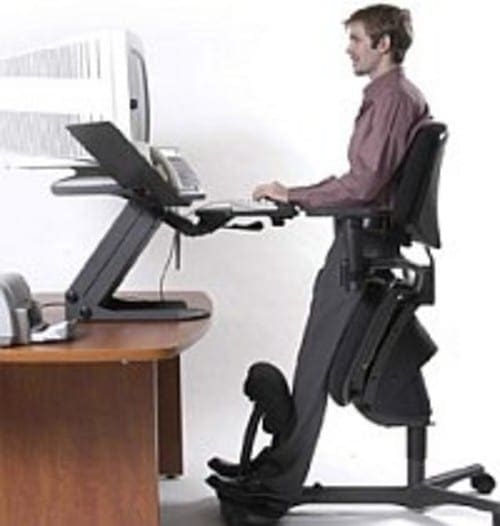
Sitting at a desk for extended periods of time is not healthy and can lead to a host of health problems. As more and more studies show the detriments of prolonged sitting, some companies are taking action to protect their employees� health by installing upright work stations. These desks take the person from a seated position and move them into one where they are leaning. As a result, most of the workers are enjoying several health benefits.
Health Benefits
It Facilitates Healthy Postural Transitions
Simply put, postural transitions are the body movements made when changing positions. There are large movements like going from sitting to standing, standing to leaning, and standing to sitting, but also small movements like adjusting arm placement or moving a foot.
Ergonomists suggest that a person should be making postural transitions several time an hour. They also recommend that people avoid any static position such as standing, sitting, or leaning for an extended period of time, instead advocating a transition or movement every 20 minutes when possible.
Static positioning has been linked to obesity, heart disease, and other health conditions. When the body is positioned in such a way that facilitates healthy movement, the body moves more often and in a more natural way. This is not likely to happen with static positioning, especially prolonged sitting.
It Improves Spine Health
Sitting or standing for long periods of time is not good for the spine. When a person stands or sits without any healthy postural transitions the spine can begin to compact and the discs become hard. This undermines the spines ability to adequately support the body, leading to loss of mobility, decreased flexibility, and pain.
The spine is made up of small bones, vertebrae, which are cushioned by spongy, fluid filled discs. In a healthy spine, the discs are filled with fluid providing a good cushion for the vertebrae as they move and support the body. However, the discs need movement to encourage blood flow so they can continue working as they should. Working upright facilitates those movements, thus decreasing the likelihood of spinal problems.
It Discourages Painful Posture
Standing and sitting for prolonged periods of time can cause pain and certain mobility problems. While they share some pain points, each brings its own problems. A strained neck and stiff, sore shoulders are often associated with sitting and standing, usually due to improper computer monitor placement. Poor leg circulation, tight hips, and lower back pain are also common problems of people who do a lot of standing or sitting on their jobs.
Using an upright workstation moves the body into a more natural, healthier posture that encourages natural, frequent movement. The spine is properly aligned over the hips, the hips are open, and the feet are adequately supported. It promotes posture that is completely contrary to being hunched over a desk � the typical posture for a sitting workstation.
It Keeps Core Muscles Engaged
When in a seated position, the core muscles are mostly lax and rarely engaged. Over time, these muscles can actually be trained to become weak, or lazy and not engage as they should. This means that they stop supporting the back and body which leads to poor posture, loss of balance, lack of mobility, decrease in flexibility, and pain.
Working upright encourages micro movements that engage the core. It�s not like crunches at the gym, but more like an ongoing mini-workout that keeps the core muscles toned and supportive. The results are a healthier spine, fewer gastrointestinal problems, better posture, and improved circulation.
Other health benefits of working upright include a decreased risk of certain cancers like colon cancer and breast cancer, improved circulation, better brain function, and a decreased risk of health conditions like diabetes, heart disease, and hypertension. Working upright is the most natural position for the body�s best function and health.
Health Benefits: Chiropractic Care Crossfit Rehabilitation
It’s going very, very well. I do feel a lot of relief. What I like about here is that he genuinely cares about his patients and he educates you. He’s constantly talking to you about why he’s doing what he’s doing. He’s very good as a doctor, he’s awesome. – Araceli Norte
Low back pain is a common health issue for many people. Nearly everybody will experience lower back pain at any moment in their own lives. This pain can differ from mild to severe and it might be short-term or long-term. When it happens, low back pain can make many everyday tasks difficult to participate and engage in. That all too familiar annoyance, however, can tremendously limit time spent relaxing, working, and even that of relationships.
Moreover, low back pain might also lead to irritability as well as a whole onslaught of additional medical health issues if not treated appropriately. The prevalence of low back pain has become a common problem, amounting to one of the most common reasons for doctor office visits each year. Before considering what type of treatment approach to follow for your back pain, it’s important to understand the anatomy of the spine and how low back pain occurs.
Understanding the Spine
The World Health Organization estimates that in the United States alone, approximately 149 million days of work are lost as a consequence of low back pain. Back pain is considered to be one of the main sources of disability and shortage of work, and it appears in 60 to 70 percent of people in industrialized nations. Understanding your spine and the way it works can help you know some of the problems which exist from aging or injury, including spinal conditions.
Many demands are placed on your own spine. It holds up your head, shoulders, and upper body. It supplies you with the necessary components to help the human body stand up right, and provides flexibility and mobility to bend and twist. Furthermore, it protects your spinal cord. Back pain differs from one person to another. The pain might have a slow beginning or come on suddenly. The pain may be continuous or irregular. Usually, back pain resolves on its own in a few weeks. However, if you’re experiencing persistent low back pain, then you may have already realized how important it is to look for treatment. Chiropractic care is a well-known treatment option which can help offer relief from your low back pain.
What is Chiropractic Care?
Chiropractic care is a popular, alternative treatment approach which primarily focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions, associated with the musculoskeletal and nervous systems. Through the use of specific treatment modalities, including spinal adjustments and manual manipulations, among others, a qualified and experienced chiropractor can help relieve low back pain by carefully correcting spinal misalignments, or subluxations.
By realigning the spine, chiropractic care can help promote the human body’s natural healing capabilities, without the need for drugs and/or medications as well as surgical interventions. Although low back pain can happen due to a variety of causes, chiropractic care can include various treatment modalities which are devoted to the management of numerous injuries and disabilities or conditions, including low back pain.
A chiropractor will perform specific treatments based on the individual’s needs, treating the body as a whole rather than simply reducing the symptoms. Many healthcare professionals recommend seeking chiropractic care for low back pain first before considering other, more aggressive treatment approaches. There are two components for chiropractic care techniques and methods: passive treatments to lower the patient’s pain in sequence to it becoming more manageable, and active treatments that the patient participates in independently.
Passive Treatment
If you’re experiencing low back pain, then it could be debilitating, making it difficult for you to go about your day normally. For that reason, it’s very important to seek immediate medical attention from a qualified and experienced healthcare professional, such as a chiropractor or physical therapist, to reduce your pain as much as possible so that you can actively participate in your treatment. These tools are often referred to as passive treatment because they are performed to a patient by the healthcare professional, including:
Electrical stimulation, such as TENS Units
Heat/ice packs
Ultrasound
Iontophoresis
Dry needling
Manual remedies
Massage
Hydrotherapy
Healthcare professionals use some of the methods, such as hot/cold packs and massage therapy, to improve blood flow to the affected area, thus reducing swelling and stiffness. Additionally, a chiropractor may utilize electric stimulation therapy, a painless remedy that gives miniature electric waves through your nervous system to relieve pain, reduce muscle strain, and encourage your body to create hormones which are anabolic. A variety of patients may also benefit from hydrotherapy. This involves executing low-intensity moves in water which alleviates strain on muscles while allowing you to move your joints without any distress.
Active Treatment
Active treatment involves exercises performed by the person and are often utilized at the following phases of chiropractic and passive treatments following the very low back pain has subsided enough so that the patient may perform them without any excessive distress. There are numerous different kinds of exercises that a chiropractor or professional physical therapist may recommend, like extending, balance training, and strength training. A variety of them can assist you with your strength, flexibility, mobility and range of motion, but a few help build the muscles around the painful region to provide those regions of the human body collectively with support to reduce low back pain.
Dr. Alex Jimenez’s Insight
A doctor of chiropractic, or chiropractor, will make sure to properly evaluate a patient before making any form of diagnosis or developing a treatment plan. An assessment can include analyzing the patient’s health history, a physical examination, including orthopedic and neurological tests, as well as advanced diagnostic tests. A chiropractor, or doctor of chiropractic, will then perform a variety of treatment modalities to treat a patient’s low back pain, depending on the specific cause of their symptoms.
What to Expect During a Chiropractor Visit
After you initially visit a chiropractor’s office, your doctor may ask you a couple of questions concerning your health, history, and lower back pain particularly. With this information, you will help your chiropractor provide you with the best treatment plan possible so that you see long-term results for your low back pain as quickly as possible.
Your doctor of chiropractic, or chiropractor, can also offer you an extensive examination. Depending upon your symptoms, your chiropractor may assess your own strength, coordination, flexibility, balance, posture, blood pressure, and heart and respiration rates. This may include using their hands to palpate your spine and surrounding area, along with a visual analysis of your movements.
You are going to learn excellent exercises to perform in your home so you may decrease your low back pain, stop re-injury, decrease strain, and accelerate your healing period. Your chiropractor will recommend specific equipment and will devote a good deal of time educating you about your source of pain and pain management plans. They’ll also implement hands-on exercises to supply you immediate relief.
When you’re well prepared to alleviate or remove your own pain, then seek immediate medical attention, so that a qualified and experienced chiropractor or professional physical therapist can help you live a pain-free life. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
I came to him (Dr. Alex Jimenez) and he’s been doing work on me and it’s been like, we’re going on 7 days, and I seem to be improving a lot more with him than what I’ve done with other therapists that I’ve been going to in almost a year. I would recommend him very highly, he’s good at what he does. – Leticia
According to the National Institute of Neurological Diseases and Stroke, or NINDS, lower back pain is one of the most common reasons for premature disability, often amounting to many doctor office visits and missed days at work. Based on these statistics, at least 80 percent of individuals in the world will experience low back pain at some point in their lifetimes, a majority of which could have been prevented.
Most lower back pain results from an injury, such as muscle sprains or strains due to abrupt movements or poor body mechanics while lifting heavy things. Low back pain may also be caused by certain ailments, such as a ruptured or herniated disc, sciatica, arthritis, kidney infections, diseases of the spinal column or cancer of the spinal cord,. Acute back pain can last anywhere from a few days to a few weeks while chronic back pain can last over three weeks to even months.
Low back pain is significantly more likely to happen in people between the ages of 30 and 50. This is partly as a consequence of changes that develop within the whole body with age. As you grow older, the fluid-like substance of the intervertebral discs in the spine reduces. This means that the discs in the spine experience stress more easily. You also lose muscle tone, which makes the spine more vulnerable to harm.
Ask any healthcare professional and you’ll get confirmation that low back pain is the most frequent health issue they are asked to look after. Strengthening your muscles and using good body mechanics are beneficial in preventing lower back pain. Often back pain can decrease on its own, especially through the use of the “RICE” treatment. But whilst rest, ice, compression and elevation can reduce back pain, its important to also seek treatment from a healthcare professional to treat the true underlying cause of your lower back pain.
What are the Symptoms of Low Back Pain?
Low back pain can be different for everyone. It might be sharp or stabbing. It may be dull, achy, or feel as a sort of cramp. The kind of pain you have will be based on the root cause of your low back pain. Many individuals discover that reclining or lying down can enhance their lower back pain, regardless of the underlying reason. Individuals with low back pain might experience a number of these, including:
Back pain that worsens with lifting and bending.
Worsening symptoms when sitting down.
Symptoms that become worse when walking.
Back pain which comes and goes, frequently following an up and down path.
Pain that extends from the back to the buttocks or outer hip, and travels down the leg.
Sciatica, including buttock and leg pain which travels into the foot, along with numbness, weakness or tingling sensations. It’s likely to get sciatica without low back pain.
Because low back pain can develop due to a variety of underlying health issues, symptoms commonly associated with lower back pain may differ from person to person. Irrespective of your age or symptoms, even if your low back pain doesn’t get better over a couple weeks, or is associated with fever, chills, or sudden weight loss, it’s fundamental for you to contact a healthcare professional immediately.
How is Low Back Pain Diagnosed?
Most doctors begin by conducting a physical examination to determine where you’re feeling the pain. A physical exam may also ascertain whether pain is affecting other structures and functions of your body. Your doctor may check your reflexes and your response to certain senses. This determines if your low back pain is affecting your nerves. If you do not have such debilitating symptoms, your doctor will probably monitor your condition before sending you for testing.
Certain symptoms like lack of bowel control, fever, fatigue, and weight loss might demand additional testing. Likewise, if your low back pain persists following home treatment, your doctor may also most likely want to send you for tests. Seek medical attention immediately at the event you observe any of these symptoms in addition to lower back pain.
Imaging evaluations such as X-rays, CT scans, ultrasound, and MRI may be needed in order for your doctor to evaluate bone issues, disk difficulties, or problems with the joints and ligaments in your spine. If your doctor suspects a matter with all the bones in your spine, they could send you to have a bone loss or bone density test. Electromyography, or EMG, as well as nerve conduction tests can help identify a problem with your own nerves.
How Can I Prevent Low Back Pain?
There are plenty of methods to prevent lower back pain. Practicing prevention techniques may also help reduce the seriousness of the symptoms once you have lower back pain. Prevention involves exercising the muscles in your core and back, losing weight if you are overweight or obese, lifting items properly by bending at the knees and lifting with the legs, and maintaining proper posture. Among the most common causes of lower back pain is a misalignment of the spine, or a subluxation, originating from improper posture.
Most office setups don’t provide ergonomic or support positioning desk chairs, while poor work habits prevents us from providing our spines with the much-needed relief we deserve throughout the day. Non-desk jobs also have their own perils. Standing daily, especially when combined with heavy lifting or routine bending, may also cause low back pain. The muscles surrounding the lumbar spine may not acquire the support they need when bending and lifting, resulting in low back pain. In either circumstance, strengthening these back muscles is fundamental to reducing the probability of chronic lower back pain.
Insist on an ergonomic desk chair, or have the opportunity to stand and move around more frequently. If you’re a cashier, invest in shoes with good arch support, which may help keep your entire body aligned. If needed, put on a technical brace to help support heavy lifting. Good habits at home to prevent low back pain can involve sleeping on a firm surface and having seats that are in the proper height. Steer clear from high-heeled shoes. If you smoke, then you may need to quit. Smoking causes the degeneration of spinal discs and reduces blood flow. But when you already have low back pain, a variety of treatment options, such as chiropractic care, can help treat lower back pain.
Dr. Alex Jimenez’s Insight
Many health issues can ultimately affect the spine, causing low back pain. Because of this, an individual’s symptoms are always different, often characterized by the underlying problem affecting them. A chiropractor can diagnose the source of a patient’s symptoms over a series of tests and evaluations, to determine the best treatment approach for the individual’s cause of low back pain. Chiropractic care focuses on naturally correcting any spinal misalignments, or subluxations, to reduce low back pain.
How Can Chiropractic Care Treat Low Back Pain?
Chiropractic care is one of the most well-known treatment options for relieving lower back pain. Medical practitioners normally recommend their patients to consider alternative treatment options before turning to prescription drugs and/or medications or surgery. The reasons are obvious: Many medications and/or drugs can have long-term health consequences. Whatever the advantages of providing temporary pain relief may be, these carry risks of complication throughout the recovery period.
Chiropractic care is a treatment approach which focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Through the use of spinal adjustments and manual manipulations, a chiropractor can carefully restore the natural alignment of the spine, reducing stress in the complex structures of the spine and improving function. Chiropractic care may also include other treatment techniques and methods to help reduce low back pain.�Lower back pain may also need the two-pronged way of using both active and passive physical therapeutics, unless the healthcare professional has a reason to recommend one over another.
Passive treatments includes using ice packs and heating pads. The healthcare professional may also use many different forms of pulsing equipment, which triggers nerves and releases pain.
Active treatments comprises the individual to perform stretches and exercises that build the type of flexibility and strength necessary to stop future flare-ups and reduce current pain. Lots of them are done with a chiropracto’s supervision, on specialized equipment, though some might be performed at the patient’s home after they learns the principles.
Chiropractic care can help treat low back pain through the treatment approaches mentioned above. Furthermore, a chiropractor may suggest lifestyle modifications to help promote a faster recovery, including physical activities and nutritional guidelines. It you’re experiencing low back pain, make sure to seek immediate medical attention, in order to receive a proper diagnosis and be able to continue with treatment. Moreover, preventing lower back pain can help avoid future episodes. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine