Can irritable bowel syndrome cause back pain? Is there some relation, what are the treatment options, and can those therapies help with the aches, soreness, and overall discomfort? Irritable bowel syndrome (IBS) is not life-threatening but is definitely life-changing with the gas, bloating, abdominal pain and changes in bathroom habits. Many with IBS develop symptoms outside of the stomach. The most common is back pain. Here�s what to know.
Irritable Bowel Syndrome
Irritable bowel syndrome is a chronic disorder that affects the lower part of the digestive tract. The common symptoms are abdominal pain, diarrhea, and constipation. There could be some combination of the two. Individuals also experience cramping, gas and bloating. Symptoms can be mild or severe and come and go. Sometimes there are no symptoms at all. Around 10-20% of adults have IBS, and women are twice as likely to develop the syndrome. It’s usually diagnosed in people under 50, and if a family has a history of IBS, this increases the chances of also having it.
The exact cause of IBS is still unknown, but it is believed to involve the way the brain interacts with the gastrointestinal tract.
Anxiety
Hormone fluctuations
Certain foods
These can trigger or worsen symptoms. There is no single test to diagnose IBS. Doctors rely on medical history, physical exams and ruling out other illnesses. No cure exists for IBS but there is a variety of treatments that can help relieve symptoms. Many experience anxiety along with job, school and relationship disruptions, all that can begin to lower quality of life.
IBS and Back Pain
Individuals can develop extraintestinal symptoms or symptoms involving other areas of the body.
This includes:
Sleep problems
Headaches
Urination problems
Fatigue
Muscle pain
Pelvic pain
Jaw pain
Back pain
Backaches and pain are common with irritable bowel syndrome. Studies have shown it affects 28-81 percent of individuals with the syndrome. Some believe that it is what is known as referred pain that originates elsewhere in the body and is felt in the back. Gastrointestinal symptoms like gas and bloating have been linked to back pain.
Other health conditions associated with back pain can also present at the same time. Interstitial cystitis is a chronic illness that causes bladder pressure and pain, and also cause fibromyalgia. 3 in 10 individuals with irritable bowel syndrome check-off the criteria for fibromyalgia. Rheumatoid arthritis is another condition.
Treatment
Treatment is different for everyone. There are treatment options available. The best approach is usually a mix of these strategies. Treating the irritable bowel syndrome could also help ease back pain. Surgery is not needed for IBS-related back pain, as well as long-term painkillers. Speak with a healthcare provider to find the right combination for you.
Treatments include:
Dietary changes: There is no specific diet for IBS but your doctor could recommend changing fiber intake or keeping a food diary to pinpoint foods that trigger symptoms. Limiting citrus, carbonated drinks, and foods that contain carbohydrates linked to gastrointestinal troubles. These include:
Wheat
Dairy
Legumes/beans
Stress reduction: People who experience high levels of stress can feel pain more intensely, whether gastrointestinal or back pain. Deep breathing, meditation, progressive muscle relaxation, and guided imagery can help ease tensions. Exercise can also help like yoga, tai chi, walking, swimming, jogging, and biking are often recommended.
Therapy: Some individuals can benefit by speaking with a mental health professional. Studies have found that cognitive-behavioral therapy that shows you how to recognize and change stress response can be especially valuable for dealing with IBS and back pain.
Medication: Depending on the symptoms and underlying cause of the irritable bowel syndrome medication can help. Antidepressants are used to ease the pain for some patients, while anti-diarrheal loperamide is for reducing diarrhea in others. Discuss any medication you take with a doctor.
Functional medicine/Complementary health: Many find relief with alternative therapies. Hypnosis, for example, has been linked to improved gastrointestinal symptoms, lower levels of anxiety and other benefits.
Probiotics/supplements: Supplements are believed to help balance out beneficial gut bacteria. There is also evidence that probiotics can help relieve certain IBS symptoms. Ask your doctor if probiotics could help.
If you have irritable bowel syndrome along with back pain, get in touch with a healthcare provider. They can help you learn what is causing the uncomfortableness, test for other conditions and set up a treatment plan. The faster you reach out, the faster you can start to feel better.
Reduce stress, reduce pain. Life creates stress, and while some stress can be good, too much causes health problems. Everyone experiences stress. However, now it is becoming a new normal in today�s hectic, fast-paced, high-pressure society. Most individuals equate stress with high blood pressure, heart attacks, or stroke. However, neck and back pain, insomnia, and weight gain can be stress-related, as well. And a lot of stress can make already-existing back/neck pain worse.
73% of individuals report experiencing stress-related psychological symptoms including anxiety and depression. These are not accurate numbers because most do not seek help for their stress issues. Stress symptoms should not be taken lightly. It is important to address the symptoms and find ways to reduce stress. Chiropractic is an effective stress reliever.
Stress
Financial pressures, kids, long work weeks, and medical problems are common anxieties. Prolonged stress can become chronic, which results in muscle tension that can feel stiff, achy and uncomfortable. Stress can develop into neck or back pain.
Stress is the state of:
Emotional
Mental
Pressure
Tension
That results from difficulties, adverse situations, or extremely demanding circumstances. The very nature of stress by definition makes it very subjective. A “stressful” situation for one person might not phase another. This makes it difficult to pin down a precise definition.
More often, the term stress is more often used to describe the set of symptoms that are caused by stress and those symptoms can be as varied as the people who experience them.
Symptoms
Stress symptoms can affect the entire body physically and mentally. Common symptoms include:
Anxiety
Chest pain
Depression
Fatigue
Gastrointestinal problems
Irritability
Lower back pain
Muscle tension
Overeating
Headache
Restlessness
Sleep problems
Unable to focus
Undereating
Health
Technically, stress itself does not have a negative impact on health. Some individuals deal with situations that others would consider to be stressful, yet they never exhibit symptoms. This speaks to the subjective nature of stress. Different people experience different symptoms and are a combination of stress symptoms, how the person handles those symptoms that adversely affect health.
Ultimately, stress symptoms can lead to some very serious conditions including:
Heart disease
Hypertension
Diabetes
Obesity
Cancer/s
Psychologically, it can lead to social withdrawal and social phobias and is directly linked to alcohol and drug abuse.
Tips
These can help you reduce stress, and reduce pain.
Vital Signs
Get a medical checkup if possible through Telemedicine and talk to a doctor/therapist about your stress, along with medical history. Side effects from medications (prescription or over-the-counter), herbal products, or other supplements can cause restlessness, insomnia, and anxiety.
Physical therapy combines pain-relieving non-invasive treatments with therapeutic exercise, posture correction, and preventive body mechanics.
Consider conversational therapy with a stress counselor, psychologist, or support group online.
Get Moving
Yoga and relaxation movements help reduce stress and stretch muscles. Viniyoga blends breathing and movement together to quiet body and mind. These movements are less precise and adapted to a person’s physical condition. Talk to a doctor about trying yoga or other stretches.
Swimming combined with a sauna or steam bathing can relieve stress-induced pain.
Take frequent stretch breaks to loosen up tight neck or back muscles.
Go for short walks at break or lunchtime to get the circulation going.
Learn to Relax
Kick back, put your feet up, and empty your mind of everything.
Wrap an ice pack and hot pack (or hot water bottle) individually in towels. Apply the ice pack for 10 minutes and then the hot pack for 5 minutes. Alternate several times.
Massage, aromatherapy and spa treatments you can do at home.
Aromatic massage oils containing eucalyptus can help ease muscle pain.
Meditation or visualization therapy combines meditation practices that focus on breathing and calming the mind.
Visualization techniques combine imagery with breathing exercises.
Take Control of the Little Things
Break up problems into smaller manageable pieces and work on resolving the easier parts first.
Learn your limits, how to delegate responsibility and not take the entire load on your shoulders so as not to get overwhelmed.
Allow yourself to fail, we all have to fail in order to learn in order to apply what was learned.
Eat and Drink for Life
Make mealtime less stressful. Pick nourishing foods, eat slowly, and savor each other’s company.
Caffeinated coffee, soda, and other drinks do not help reduce stress or promote restful sleep.
Avoid drinking at night because it can make falling and staying asleep a challenge.
Proper sleep or naps can help relieve stress.
Dealing with Stress Is Good for Your Back
We may not be able to control life’s stressors, but don’t let everyday demands interfere with your health. Incorporate exercise, relaxation techniques, and healthy foods to reduce stress and pain and promote stress prevention.
Reduce stress reduce pain with chiropractic
Chiropractic cannot get rid of stress, but it can help relieve stress symptoms. The more stress the body endures, the more sensitive it becomes to pain and physical imbalances. Chiropractic helps by bringing the body back into balance, aligning the spine, and relieving pain.
The simple act of aligning the spine helps relieve stress in the body that you may not even be aware of. The physical stress of a misaligned spine can exacerbate symptoms and make a person more susceptible to stressful stimuli in their environment. Chiropractic helps to improve circulation which is essential in relieving muscle tension and helps shuts down the fight or flight response allowing the body to rest and heal.
Industrialization/modernization has impacted our food, the way we eat and our weight. Processed fast food can be purchased pretty much anywhere. We no longer expend physical energy to hunt and forage for food. Because of this back pain is probably the most common and most troublesome condition that individuals experience. Eight out of 10 will struggle with back pain at some point in their life. Low chronic back pain can become aggravated by a variety of triggers.
Mechanical stress
Excessive strain
Muscle weakness
Poor sleep position
No exercise
Excessive weight
These can all contribute to making back pain even worse. Obesity is defined as a disease. It is a serious disorder that affects adults and children. Being overweight can contribute to the development of coronary heart disease, diabetes, high blood pressure, and colon cancer. And it can also contribute to symptoms associated with:
Osteoporosis
Osteoarthritis
Rheumatoid arthritis
Degenerative disc disease
Spinal stenosis
Spondylolisthesis
Osteoporosis coupled with a sedentary lifestyle and an unhealthy diet can affect the density and the strength of the bones. When the structural integrity of the spine is compromised there is a higher risk for fracture. Vertebral fractures can be painful and disabling. Those diagnosed with osteoporosis probably have lost between 25% to 30% of bone density.
Being Overweight Affects the Spine
The spine carries the body’s weight and distributes the weight in an equal manner when resting and during activity. When there is excess weight the spine is forced to compromise which can lead to injuries and structural damage. The area of the spine that is the most vulnerable is the low back or lumbar spine.
Exercise is Important
When we don’t exercise it leads to:
Poor flexibility
Weak back muscles
Weak pelvis
Weak thighs
This can increase the lower back’s curve, which causes the pelvis to tilt forward in an unhealthy manner. This is detrimental to proper posture and when our posture weakens, the rest of the body follows.
Age Relation
These disorders of the spine might be thought of as the normal aging process. This is true that as we age, the body tissues begin to change and the spine’s disc wear down. But, if you are overweight, chances are you have, or will have pain in the back.
Weight Loss Reduces Back Pain
Weight loss can contribute to a partial or complete reduction in the back pain symptoms. The research between weight loss and back pain is still ongoing but numerous practitioners report cases of patients experiencing a serious reduction in pain after losing the excess weight. Because the extra weight is taken off the spine further stress is avoided. Especially when a chiropractor realigns the vertebral column. According to the American Spine Society, individuals that stay around 10 pounds of their proper weight are those least likely to experience back problems.
Back Health and Physical Activity
Chiropractic is one of the most popular treatments for back pain. With chiropractic adjustments, pain is alleviated but also the root cause of the problems is corrected. Spinal adjustments can help even more when combined with a proper diet and weight loss treatment program.
Besides weight loss, exercising and strengthening the core muscles can guarantee the proper distribution of the body�s weight. Stronger muscles, less weight, and better posture will provide amazing long-term benefits. If you want to know how to incorporate weight loss and exercise in your daily routine, speak to your chiropractor. They are ready to guide you along the way. If you aren�t currently seeing a chiropractor, give us a call. We�re here to help!
Chiropractic Weight Loss
NCBI Resources
While chiropractic adjustments and associated therapies can ease back pain symptoms and aid in healing, lifestyle changes like a healthy diet are just as important. The more a patient can get to their ideal weight, the easier it becomes to treat and eliminate the back pain.
Lumbago is a term that means mild to extreme pain in the muscles and joints of the lower spine/back. The pain can be acute or chronic and affects both young and older individuals. The spine is a very intricate structure and when one component fails to function properly it can affect the entire body, causing pain and loss of mobility. Back pain costs about $100 billion in medical bills, disability, and lost workdays.
Tiny bones, known as vertebrae, are stacked on top of each other, which forms the spine. The way these bones are joined facilitates movement, flexibility, and range of motion. In between�each vertebra are small, fluid-filled discs that are the padding/cushions between the bones. When these discs become damaged, injured, or shift out of place it can affect the surrounding nerves, muscles, and ligaments causing pain and making movement difficult.
At some point, an individual will experience some form of back pain. This could be a sore back from yard work, tough manual labor or hard workout, etc. This is a normal occurrence and can be taken care of at home. If you have a sprained or strained back but not a serious injury icing can help reduce swelling, muscle spasms, and pain for the first 24 to 48 hours after the injury. After 48 hours, switch to heat to warm and relax the sore muscle tissues.
Causes
There are a variety of conditions that can cause low back pain. The more common conditions:
Herniated Disc is one of the most common spinal disc issues.
Osteoarthritis or Spondylosis
Osteoporosis
Rheumatoid Arthritis
Scoliosis
Spinal Stenosis
Spinal Tumor
Factors that can contribute to back pain and can exacerbate the pain during episodes of lumbago.
Exposure to a cold damp environment
Poor posture
Sudden movement/s
Coughing
Sneezing
Lumbago Symptoms
Common symptoms of lumbago.
The pain can radiate into the buttocks, thigh/s, and the groin and can cause tingling/numbing/electrical sensations to be felt in the low back, buttocks, and legs and feet.
The pain can be aggravated when moving around. Bending forward, backward and side-to-side can limit mobility.
Spine muscle spasms can cause the back to feel stiff with a constant soreness.
The pain can affect proper posture, which causes individuals to walk bent or hunched to one side.
Lumbago rarely causes serious symptoms that need immediate medical attention.
See A Chiropractor
A chiropractor can help you create a natural, non-surgical treatment/exercise/health plan to control low back pain and prevent future episodes of lumbago. Treatments include physical therapy, chiropractic, supplements, and alternative medicine like acupuncture.
The “LIFE CHANGING” Foot Orthotics | El Paso, Tx (2020)
NCBI Resources
Everyone needs to take care of their back/spine because it is what holds us up as long as we keep it straight and strong.�Strengthening the core�can help prevent a weak and misaligned spine from getting worse�and helps to eliminate pain. Back safety should be priority one, as it affects all aspects of your life. Not only are you protecting your back, but preventing future injury.
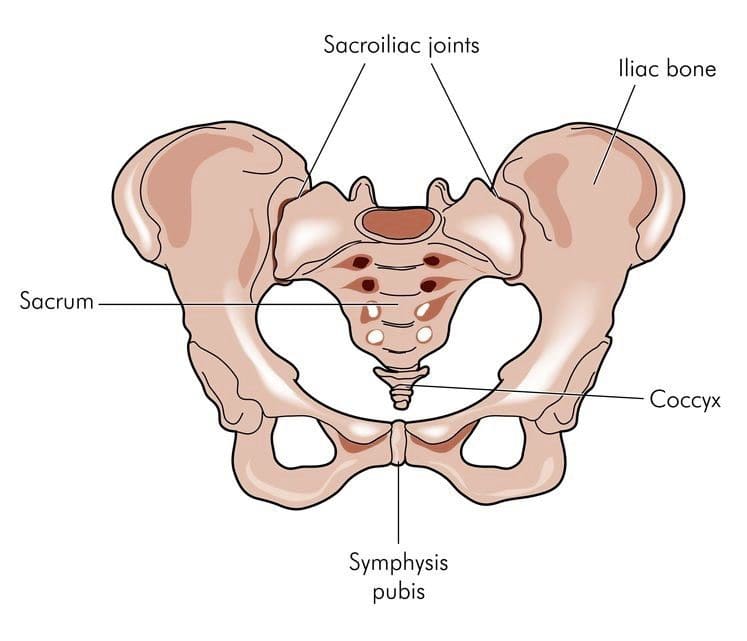
Sacroiliac joint dysfunction and its symptoms can also be a cause for low back pain conditions and disorders.
This condition is also known as:
Sacroiliitis
SI joint inflammation
SI joint syndrome
Sacroiliac joint dysfunction
SI joint strain
It can make regular activities like sitting, standing, walking, and sleeping frustrating, difficult and unbearable. It has been found in around 30-35% of individuals.�Many individuals can spend months or even years dealing with symptoms but are never aware that it’s not the correct diagnosis. Sacroiliac joint dysfunction can sometimes be difficult to diagnose. These joints are so close to the hip and low back, that it is common for sacroiliac joint dysfunction to be mistaken for other causes/conditions of low back pain, like a herniated, slipped or bulging disc.
Sacroiliac Joint Dysfunction Symptoms
When low back pain is present, it can be quite difficult for a doctor to figure out the exact source/cause of your pain.
These are a few recognizable symptoms of sacroiliac joint dysfunction.
Low back pain is the most common.
Pain could also present in the hips, buttocks, thighs, and possibly the groin area.
The pain can be so severe that just touching the area is unbearable.
Other activities that can cause symptoms:
Common movements like climbing stairs, sitting down/getting up out of a seat, can cause pain. Pain can also be aggravated from standing or walking for extended periods but improve when relaxed or lying down. Stiffness or a burning sensation in the pelvis can also present.
Causes of Joint Dysfunction
A variety of conditions can cause sacroiliac joint dysfunction. The most common:
Arthritis
Joint pain can be caused by spinal osteoarthritis because as the cartilage around the sacroiliac joint wears down, the bones can start to rub against each other. Ankylosing spondylitis is an inflammatory arthritis that affects the spine that can also cause joint dysfunction.
Pregnancy
Pregnant women can experience low back pain or pelvic pain from sacroiliac dysfunction because the joints get stretched and lose their elasticity during pregnancy. Hormone changes and added weight during pregnancy can place added stress on the sacroiliac joints.
Accident Trauma
High impact from an auto accident, slip and fall injury, or sports injury could damage the sacroiliac joint/s.
Viral Infection
Infections are extremely rare but could be another cause of joint pain.
There are a variety of treatment options that can help reduce and prevent low back pain.
Exercise/Physical Therapy
Exercise and physical therapy are therapies that doctors highly recommend before other treatments like pain medications or surgery. Exercise, chiropractic and physical therapy can help manage pain and other symptoms. Consult your doctor before starting any physical therapy or exercise program. Your doctor can recommend a chiropractor or therapist that can help get you started with the proper exercise treatment plan.
Physical Therapy
Physical therapy can help reduce stress on the joints, that are strained and tight. It also helps maintain joint flexibility. A physical therapist will perform passive and active treatment therapies to help manage joint pain.
Passive treatments – the physical therapist does the majority of the work. An example of passive treatment applying heat or ice along with massaging the area.
Active treatments – the patient participates in the treatment with at-home exercise routines is an example of active treatment.
A combination of passive and active treatment provides the best outcomes and offers the most benefits, as the patient has the know-how of proper posture, exercises that they can do and injury prevention. A chiropractor and physical therapist can build a physical therapy program to help address your symptoms.
Exercise
With sacroiliac joint dysfunction, you do not have to do hard intense exercise. The benefits come from a consistent gentle exercise routine with an emphasis on consistency. Exercising stretches and strengthens muscles of the low back muscles and helps maintain joint flexibility.
An overall exercise plan should incorporate the three main types:
Sacroiliac joint dysfunction is known to cause low back pain, but diagnosing can be hard for some doctors. Especially those that do not have a great deal of experience in sacroiliac joint pain. However,�chiropractors specialize in this area as the SI joint is an important part of the musculoskeletal system.
There are different types of topical medications, different ways of delivery and are available for patients with back and neck pain. A physician may combine one or more types of medication for maximum relief or as a way of�limiting the side effects of larger doses of only one medication. Strong dose compounds and controlled drugs are�only�available with a doctor’s prescription.
Medicines with a low potency and low risk of side effects are available at stores and local pharmacies over-the-counter. But remember medications sold over the counter without a prescription doesn’t mean they are safe to use as much as possible. Please read the label and follow the instructions. Taking higher doses, even acetaminophen e.g. Tylenol can cause liver damage. Discussing these medications with a doctor or pharmacist before purchase would be wise. Your physician should know if you plan to continue using over-the-counter medications.
Medicines with a low potency and low risk of side effects are available at stores and local pharmacies over-the-counter. But remember medications sold over the counter without a prescription doesn’t mean they are safe to use as much as possible. Please read the label and follow the instructions. Taking higher doses, even acetaminophen e.g. Tylenol can cause liver damage. Discussing these medications with a doctor or pharmacist before purchase would be wise. Your physician should know if you plan to continue using over-the-counter medications.
Inform your physician about all the products you take including herbal remedies to decrease the risk of side effects or potential severe drug interactions. When acute pain is present, injections either intravenous or intramuscular injected into the muscles are used. For chronic pain, medications are used and are typically in pill form. Both methods have limitations and different�delivery�approaches may be considered. This includes inhalation or topical on top of the skin applications.
Topical Pain Alleviators
These type of medications come prepared and are applied to the skin via:
Topical medications aim to reduce inflammation and soothe nerve and muscle pain. Some are available with a doctor’s prescription and others are over-the-counter. Medication administered�through the skin is becoming more popular.
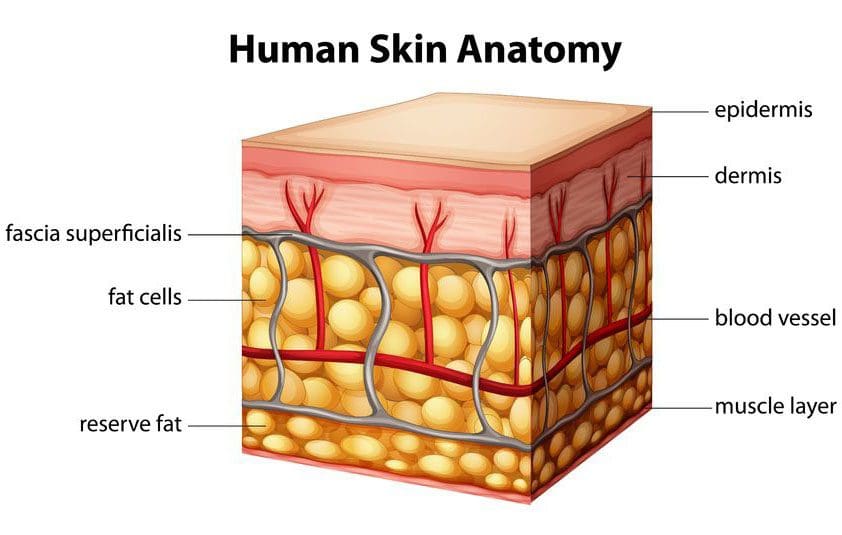
Skin Cells
The skin is the largest organ of the body. It serves as�water barrier protection, it regulates body temperature, controls fluid loss, and is important to homeostasis/healthy internal balance.
It is made up of many layers and is supported by a complex blood supply. The blood vessels are in a framework of connective tissue including fat and fascia that holds the tissues together. Below that layer is the bone and muscle. There are also nerve endings that relay touch, temperature, and pain signals from the skin to the spinal cord, to the brain.
Compounds�have been developed to safely carry the various medicines through the skin into the blood. These compound enhancers are able to penetrate the skin by opening normally closed channels for a quick time to help the skin absorb the medication/s and then close back up.
Spine Pain
Spine physicians and pain specialists often first recommend topical pain-relievers to help relieve the symptoms of back and neck pain/conditions.
Topical medicines may be used to treat the pain associated with:
Neck strain
Low back strain
Whiplash
Muscle inflammation
Spasms
Osteoarthritis
Rheumatoid arthritis
Certain types of nerve pain
Topical Advantages
Bases like creams, ointments, gels, and sprays make application easy.
Symptom relief is faster than oral medicines.
Symptoms reduce at a steady rate.
Relief can last longer.
Not as much medicine is needed when applied in topical form.
As the medication is diffused through the skin and enters the bloodstream, it bypasses the digestive system reducing any unwanted�side effects, like an irritated stomach.
Topical Disadvantages
Blood flows in different ways to different parts of the body. Education about the product is essential to know where to apply the product like the arm or abdomen and how often.
Blood flow to certain parts of the body can change over time. For example, when it’s cold the blood vessels in the skin contract which decreases the absorption of the medicine, while sweating can open the pores too much and allow too much medication to be absorbed too quickly or wash it away completely.
The skin could present a negative reaction. Therefore patients need to know what to do if an allergic or other reaction takes place.
The skin nerves are different from the spinal nerves, so certain types of neck/back pain may not respond well to topical treatment.
Spinal conditions/disorders deep in the body will not respond well to topical therapy.
Is it right
Are topical pain-alleviating medications the right for you? The best person to ask is your doctor or healthcare provider. Upon a final diagnosis and medical history, your doctor should offer various treatments/therapies for pain management.
Conclusion
Patches and creams can be used to deliver a wide variety of medications. These topicals are becoming popular because of their convenience and, reduction of negative side-effects.
For individuals with muscle or tendon inflammation, applying a topical to the affected area limits the amount of medication going to other areas of the body that do not need it.
For those that have stomach problems and find it difficult to digest anti-inflammatories, these topicals could be all they need to stay active.
Individuals with chronic neck or back pain should discuss these medications with their pain specialist, physician or chiropractor to see if one of these topicals might work for them.
El Paso, TX Neck Pain Chiropractic Treatment
NCBI Resources
Everyone needs to take care of their back/spine because it is what holds us up as long as we keep it straight and strong.�Strengthening the core�can help prevent�a weak and misaligned spine from getting worse�and helps to eliminate pain.
Back safety should be priority one, as it affects all aspects of your life. Not only are you protecting your back, but are preventing future injury. We all need to pay attention to proper body positioning and�body mechanics, as it will pay off in the long run.
Living in the desert means we don’t have to deal with digging/shoveling through snow and ice, but there are still proper techniques, tools, body mechanics, posture, and core strength that we should pay attention to and apply to guard our spines and general health. It is no surprise that when shoveling many individuals experience muscle fatigue, low back strain, vertebral disc damage (herniated disc), and even spinal fractures.
A great deal of these injuries come from excessive stress to spinal structures by slip and fall accidents. Shoveling is a frequent cause of back pain and injuries. Injuries are not only limited to the musculoskeletal system but excessive shoveling can also place added stress on the cardiovascular system.� Any hint of shortness of breath or chest pain, stop shoveling immediately but if symptoms continue, seek medical attention.
A study published indicated when handling heavy material with a shovel, the L5-S1 disc has been identified as the weakest link in the body. The most severe injuries along with pain are likely to occur in the back. Here are some tips to prevent injury.
Shoveling Basics
Shoveling can be compared to weight lifting and intense aerobic exercise. To help your body function correctly consider the following tips:
Eat long before shoveling so you have fuel but don’t cramp up.
Avoid caffeinated drinks/beverages. Stimulants can increase heart rate and cause blood vessels to constrict.
If you experience pain, stop immediately and get assistance.
Pace yourself when shoveling.
Take plenty of breaks.
Drink plenty of water to rehydrate your body.
For snow, if the ground is icy or slick, throw sand or salt to help create traction. But still be aware that some areas can still be uneven and cause you to slip, trip, or fall.
Proper Clothing
Consider the weather before beginning the job.
When it’s cold dress in layers, wear gloves, and a hat because a good amount of body heat is lost through the head. If icy cold, use a scarf.
Wear clothing that is easy to move around in.
Proper boots are essential for maintaining balance, traction and keeping feet warm/dry.
Choose specialized work/blister-free gloves or thicker gloves, that allow for a good grip on the handle.
The Shovel That’s Right for You and the Job
Shovels come in different materials, purposes, shapes, and sizes.
Choose an ergonomic shovel with a curved handle. These shovels help keep your back straight and reduce spinal stress.
Hardware stores stock ergonomically designed shovels of all types.
For snow maybe try a shovel with a plastic blade instead of metal as it’s lightweight.
Sometimes a smaller blade is the way to go. You don’t shovel as much per load, but it weighs less and puts less strain on the spine.
Don’t go for a cheap model if the job you are doing is heavy-duty. Your body will thank you.
Once you have your shovel take some time to learn the proper technique.
Technique is Key
Take some time to stretch and prepare your body as warm muscles work better.
Hand placement on the shovel is very important! Don�t grip with the hands close to each other.
Keep some distance between the hands. This will give you more leverage and make it easier to lift.
Think about proper posture and maintaining the natural curve of your spine.
Address the task directly.
Stand with your feet shoulder-width apart to stay balanced.
Try to keep the shovel close to your body. Holding a shovelful with arms outstretched puts added weight on your spine.
Bend at the knees and not the waist or back.
Tighten your stomach muscles as you lift.
Lift with your legs and not your back.
Dump the material in front of you. If you need to move the material to the side, move your feet.
Do not twist your body.
Scoop small amounts into the shovel
Walk to where you want to dump it.
Do not throw over your shoulder.
Go forward with the material.
Pace yourself. Take frequent breaks and stretch your back and body.
Power Equipment
Power equipment is terrific, but if it’s not used correctly, you can still strain or injure your back.
Example: Snowblowers are designed to remove snow at a certain speed but pushing or forcing the equipment to go faster is defeating the purpose of the machine doing the work for you.
You may not realize that you hurt your back. But that little twinge you felt could change your life forever. Getting back to 100% of where you were before the injury could take time and treatment. So, do not take this activity lightly and remember prevention is the best defense.
El Paso, TX Lower Back Pain Chiropractic Care
NCBI Resources
Injuries that are caused by repetitive movements often develop gradually.�It�s not until the symptoms get very painful and debilitating that the individual realizes that something is wrong. Don�t wait, as soon as you feel a tingle, slight pinch, or a little soreness and feel that it’s from your work, get in touch with a doctor or chiropractor.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine