For individuals dealing with lower back pain, it could be quadricep muscle tightness causing the symptoms and posture problems. Can knowing the signs of quadricep tightness help prevent pain and avoid injury?
Quadriceps Tightness
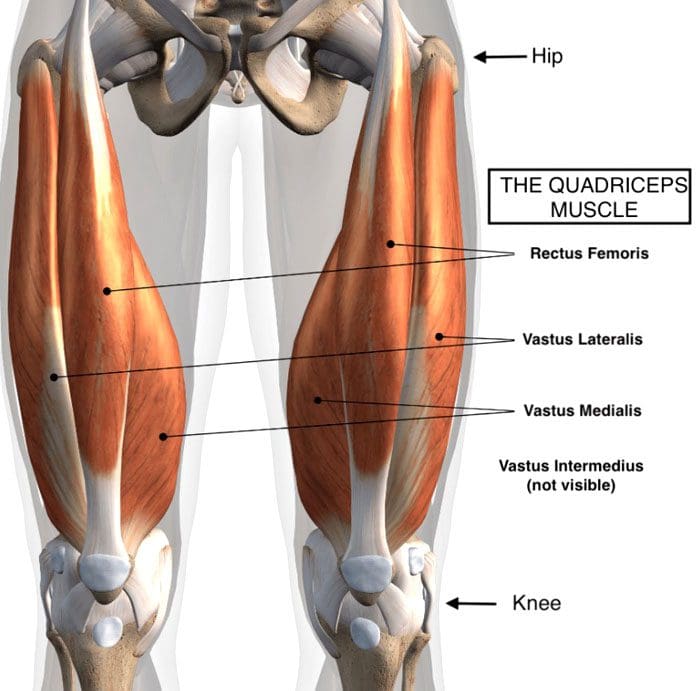
Quadriceps muscles are in the front of the thigh. Forces that could be creating chronic pain and posture problems could be happening at the same time are:
Quadricep tightness causes lower back pain as the pelvis gets pulled down.
Tight quadriceps lead to weakened hamstring muscles.
These are the opposing muscles behind the thigh.
Stress and pressure on the hamstrings can cause back pain and problems.
The rectus femoris attaches to the pelvis at the anterior superior iliac spine, which is the front part of the hip bone.
The rectus femoris is the only muscle in the group that crosses over the hip joint, which also affects movement.
When the quadriceps, especially the rectus femoris, become tight, they pull down on the hips.
The pelvis tilts downward or forward, technically referred to as the anterior tilt of the pelvis. (Anita Król et al., 2017)
The spine is between the pelvis, and if the pelvis tilts forward, the lumbar spine compensates by arching.
A larger arch in the lower back is referred to as excessive lordosis and often causes tightness and pain in the back muscles. (Sean G. Sadler et al., 2017)
Hamstring Compensation
When the quadriceps tighten and the pelvis gets pulled down, the back has an abnormal lift. This puts the hamstring on a consistent stretch that can cause pain symptoms.
Healthy posture and hamstring muscle tone help maintain correct pelvic positioning in the back.
This is correct because it helps maintain a comfortable position.
Quadricep tightness can set off a reaction as the pelvis tilts down in front and up in the back while overly stretching the hamstrings.
Pain and soreness are the usual result
Lack of hamstring strength and quadriceps stretching can cause the hamstrings to lose their ability to support correct pelvic and spinal positions. (American Council on Exercise. 2015)
Knowing When Quads Are Tightening
Individuals often don’t realize their quadriceps are tight, especially those who spend most of the day sitting.
The more time spent in a chair can cause the quadriceps and lower back muscles to tighten steadily.
Individuals can try a few tests at home:
Standing Up
Push the hips forward.
Push from the sitting bones so you’re at the correct level.
How far forward do the hips go?
What is felt?
Pain could indicate tight quadriceps.
In A Lunge Position
With one leg forward and bent in front of the other.
The back leg is straight.
How far forward does the leg go?
What is felt?
How does the front of the hip on the back leg feel?
Standing Bent Leg
Stand with the front leg bent and the back leg straight.
Discomfort in the back leg could mean tight quadriceps.
In A Kneeling Position
Arch the back
Grab the ankles
Modify the position to adjust for any pain or joint issues.
If you have to prop yourself up or modify the pose to reduce pain, it could be tight quadriceps.
Helping to understand the condition can help in communication with a healthcare provider.
A healthcare provider and/or physical therapist can conduct a posture evaluation examination to test the quadriceps.
Understanding Academic Low Back Pain: Impact and Chiropractic Solutions
References
Kripa, S., Kaur, H. (2021). Identifying relations between posture and pain in lower back pain patients: a narrative review. Bulletin of Faculty of Physical Therapy, 26(34). https://doi.org/doi: 10.1186/s43161-021-00052-w
Król, A., Polak, M., Szczygieł, E., Wójcik, P., & Gleb, K. (2017). Relationship between mechanical factors and pelvic tilt in adults with and without low back pain. Journal of back and musculoskeletal rehabilitation, 30(4), 699–705. https://doi.org/10.3233/BMR-140177
Sadler, S. G., Spink, M. J., Ho, A., De Jonge, X. J., & Chuter, V. H. (2017). Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: a systematic review of prospective cohort studies. BMC musculoskeletal disorders, 18(1), 179. https://doi.org/10.1186/s12891-017-1534-0
American Council on Exercise. (2015). 3 Stretches for Opening Up Tight Hips (Fitness, Issue. https://www.acefitness.org/resources/everyone/blog/5681/3-stretches-for-opening-up-tight-hips/
For individuals with arthritis, can incorporating acupuncture with other therapies help manage pain and other symptoms?
Acupuncture For Arthritis
Acupuncture has been around for thousands of years and is a form of traditional Chinese medicine that utilizes needles inserted into various parts of the body to relieve pain and inflammation. The practice is based on the concept of life energy that flows throughout the body along pathways called meridians. When the energy flow becomes disrupted, blocked, or injured, pain or illness can present. (Arthritis Foundation. N.D.) Further research is needed to determine how the acupuncture therapeutic mechanisms work and the overall effectiveness. However, there is emerging evidence suggesting that acupuncture can provide symptom relief for individuals with joint pain, especially those with osteoarthritis and rheumatoid arthritis. (Pei-Chi Chou, Heng-Yi Chu. 2018)
Benefits
The actual method that reduces the pain and inflammation is still unclear. Theories include that the needles suppress inflammatory responses, improve blood flow, and relax muscles. Although acupuncture cannot cure or reverse arthritis, it may be useful for managing pain and decreasing associated symptoms, especially in combination with other therapies. (Pei-Chi Chou, Heng-Yi Chu. 2018)
Rheumatoid Arthritis
A systematic review of 43 studies, including humans and animals with rheumatoid arthritis, demonstrated varied results. Several studies showed improvement in symptoms and decreased biological markers of rheumatoid arthritis following one to three sessions of acupuncture for four weeks or more. (Sharon L. Kolasinski et al., 2020) Beneficial outcomes following acupuncture treatment for rheumatoid arthritis include:
Reduced pain
Reduced joint stiffness
Improved physical function
The results of the human and animal studies suggested that acupuncture has the potential to down-regulate:
Levels of interleukins
Levels of tumor necrosis factor
Specific cell signaling proteins/cytokines involved in the inflammatory response, which become elevated in autoimmune conditions like rheumatoid arthritis. (Pei-Chi Chou, Heng-Yi Chu. 2018)
Most of the study subjects were also receiving other forms of treatment, especially medication. Therefore, it is difficult to conclude how beneficial acupuncture is alone or as a supplemental addition to other medical treatments. (Pei-Chi Chou, Heng-Yi Chu. 2018)
Osteoarthritis
Acupuncture for osteoarthritis of the hand, hip, and knee is recommended, according to the American College of Rheumatology and Arthritis Foundation, meaning that it may be worth trying, although more research is needed to confirm its effectiveness. However, since the risk is relatively minor, acupuncture is generally considered a safe alternative treatment option for managing the symptoms. (Sharon L. Kolasinski et al., 2020)
Chronic Pain
As clinical trials suggest that acupuncture may be effective in providing pain relief, it may be a recommended option for individuals suffering from chronic pain. A recent systematic review of 20,827 patients and 39 trials concluded that acupuncture is effective for the treatment of chronic musculoskeletal pain, headache, and osteoarthritis pain. (Andrew J. Vickers et al., 2018)
Triggering the release of endorphins/hormones that help reduce pain.
Safety
Acupuncture is considered a safe procedure by a licensed and certified professional.
To practice acupuncture in the United States, an acupuncturist needs a minimum of a master’s degree from a program accredited by the American Academy of Acupuncture and Oriental Medicine and a license in the state where they received their acupuncture treatment.
Doctors with an MD or DO degree licensed in the United States to practice medicine can also be licensed by the American Academy of Medical Acupuncture after additional training.
Risks
Risks associated with acupuncture are bleeding and bruising, especially for individuals who have a bleeding disorder like hemophilia or take a blood thinning medication. Individuals are recommended to talk to their healthcare provider to determine if acupuncture is a safe option.
Side Effects
Most individuals do not experience any side effects, although possible reactions can include: (Shifen Xu et al., 2013)
Soreness
Bruising
Scarring
Needle shock: a vasovagal response that presents as feeling faint, clammy hands, chills, and slight nausea.
Acupuncture Session
During the initial treatment, individuals will discuss their medical history and what joints and areas of their bodies are presenting with symptoms.
After a physical exam, the individual will lie on a treatment table.
Individuals may be face up or down depending on what areas of the body the acupuncturist needs to access.
It is recommended to wear loose clothing that can be rolled up or moved out of the way to access different areas easily.
Depending on what areas need to be accessed, individuals may be asked to change into a medical gown.
The acupuncturist will use alcohol swabs to disinfect the area before inserting the needles.
The needles are made of stainless steel and are extremely thin.
Individuals may feel a slight pinch in sensitive areas like the hands and feet, but needle insertion should be comfortable and well-tolerated without significant discomfort.
For electroacupuncture, the acupuncturist will pass a mild electric current through the needles, typically 40 to 80 volts.
The needles stay in place for 20 to 30 minutes.
After the treatment is finished, the acupuncturist will remove the needles and dispose of them.
Frequency
The frequency of acupuncture sessions will vary depending on the severity of the symptoms and whether the visits are approved and reimbursed by the health insurance company.
Cost and Insurance
Costs for acupuncture can vary from $75 to $200 per session.
The first session, which involves an initial assessment and evaluation, usually costs more than follow-up visits.
Whether the health insurance will cover some or all of the costs of acupuncture sessions depends on the individual insurance company and the condition being treated.
Medicare currently covers acupuncture services up to 12 visits within a 90-day period for chronic low back pain only.
Medicare will not cover acupuncture for other conditions. (Medicare.gov. N.D.)
Acupuncture is not a cure for arthritis, but it may be a useful tool to help manage pain and other symptoms. Make sure to consult a healthcare provider if acupuncture is safe to try based on medical history.
Chou, P. C., & Chu, H. Y. (2018). Clinical Efficacy of Acupuncture on Rheumatoid Arthritis and Associated Mechanisms: A Systemic Review. Evidence-based complementary and alternative medicine : eCAM, 2018, 8596918. https://doi.org/10.1155/2018/8596918
Kolasinski, S. L., Neogi, T., Hochberg, M. C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W. F., Hawker, G., Herzig, E., Kwoh, C. K., Nelson, A. E., Samuels, J., Scanzello, C., White, D., Wise, B., … Reston, J. (2020). 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis care & research, 72(2), 149–162. https://doi.org/10.1002/acr.24131
Vickers, A. J., Vertosick, E. A., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., Irnich, D., Witt, C. M., Linde, K., & Acupuncture Trialists’ Collaboration (2018). Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis. The journal of pain, 19(5), 455–474. https://doi.org/10.1016/j.jpain.2017.11.005
Xu, S., Wang, L., Cooper, E., Zhang, M., Manheimer, E., Berman, B., Shen, X., & Lao, L. (2013). Adverse events of acupuncture: a systematic review of case reports. Evidence-based complementary and alternative medicine : eCAM, 2013, 581203. https://doi.org/10.1155/2013/581203
Medicare.gov. (N.D.). Acupuncture. Retrieved from https://www.medicare.gov/coverage/acupuncture
Individuals may not realize they have a cracked rib until symptoms like pain when taking in a deep breath begin to present. Can knowing the symptoms and causes of cracked or broken ribs help in diagnosis and treatment?
Cracked Rib
A broken/fractured rib describes any break in the bone. A cracked rib is a type of rib fracture and is more a description than a medical diagnosis of a rib that has been partially fractured. Any blunt impact to the chest or back can cause a cracked rib, including:
Falling
Vehicle collision
Sports injury
Violent coughing
The main symptom is pain when inhaling.
The injury typically heals within six weeks.
Symptoms
Cracked ribs are usually caused by a fall, trauma to the chest, or intense violent coughing. Symptoms include:
Swelling or tenderness around the injured area.
Chest pain when breathing/inhaling, sneezing, laughing, or coughing.
Chest pain with movement or when lying down in certain positions.
Possible bruising.
Although rare, a cracked rib can cause complications like pneumonia.
See a healthcare provider immediately if experiencing difficulty breathing, severe chest pain, or a persistent cough with mucus, high fever, and/or chills.
Types
In most cases, a rib usually gets broken in one area, causing an incomplete fracture, which means a crack or break that does not go through the bone. Other types of rib fractures include:
Displaced and Nondisplaced Fractures
Completely broken ribs may or may not shift out of place.
If the rib does move, this is known as a displaced rib fracture and is more likely to puncture lungs or damage other tissues and organs. (Yale Medicine. 2024)
A rib that stays in place usually means the rib is not completely broken in half and is known as a nondisplaced rib fracture.
Flail Chest
A section of the ribcage can break away from the surrounding bone and muscle, although this is rare.
If this happens, the ribcage will lose stability, and the bone will move freely as the individual inhales or exhales.
This broken ribcage section is called a flail segment.
This is dangerous as it can puncture the lungs and cause other serious complications, like pneumonia.
Causes
Common causes of cracked ribs include:
Vehicle collisions
Pedestrian accidents
Falls
Impact injuries from sports
Overuse/Repetitive stress brought on by work or sports
Severe coughing
Older individuals can experience a fracture from a minor injury due to the progressive loss of bone minerals. (Christian Liebsch et al., 2019)
The Commonality of Rib Fractures
Rib fractures are the most common type of bone fracture.
They account for 10% to 20% of all blunt trauma injuries seen in emergency rooms.
In cases where an individual seeks care for a blunt injury to the chest, 60% to 80% involve a broken rib. (Christian Liebsch et al., 2019)
Diagnosis
A cracked rib is diagnosed with a physical exam and imaging tests. During the examination, a healthcare provider will listen to the lungs, press gently on the ribs, and watch as the rib cage moves. The imaging test options include: (Sarah Majercik, Fredric M. Pieracci 2017)
X-rays – These are for detecting recently cracked or broken ribs.
CT Scan – This imaging test comprises multiple X-rays and can detect smaller cracks.
MRI – This imaging test is for soft tissues and can often detect smaller breaks or cartilage damage.
Bone Scan – This imaging test uses a radioactive tracer to visualize the structure of bones and can show smaller stress fractures.
Treatment
In the past, treatment used to involve wrapping the chest with a band known as a rib belt. These are rarely used today as they can restrict breathing, increasing the risk of pneumonia or even a partial lung collapse. (L. May, C. Hillermann, S. Patil 2016). A cracked rib is a simple fracture that requires the following:
Rest
Over-the-counter or prescription medications can help manage pain symptoms.
Nonsteroidal anti-inflammatory drugs – NSAIDs like ibuprofen or naproxen are recommended.
If the break is extensive, individuals may be prescribed stronger pain medication depending on the severity and underlying conditions.
Physical therapy can expedite the healing process and help maintain the range of motion of the chest wall.
For patients who are frail and elderly individuals, physical therapy can help the patient walk and normalize certain functions.
A physical therapist can train the individual to transfer between bed and chairs safely while maintaining awareness of any movements or positioning that make the pain worse.
A physical therapist will prescribe exercises to keep the body as strong and limber as possible.
For example, lateral twists can help improve the range of motion in the thoracic spine.
During the early stages of recovery, it is recommended to sleep in an upright position.
Lying down can add pressure, causing pain and possibly worsen the injury.
Use pillows and bolsters to help support sitting up in bed.
What may feel like a cracked rib may be a similar condition, which is why it’s important to get checked out. Other possible symptom causes can include:
Bruised ribs – This occurs when the ribs are not cracked, but the smaller blood vessels around the region burst and leak into surrounding tissues. (Sarah Majercik, Fredric M. Pieracci 2017)
Pulled muscle – A muscle strain, or pulled muscle, occurs when the muscle gets overstretched, which can lead to a tear. The ribs are not affected, but it can feel like they are. (Sarah Majercik, Fredric M. Pieracci 2017)
Emergency
The most common complication is being unable to take a deep breath because of the pain. When the lungs cannot breathe deeply enough, mucous and moisture can build up and lead to an infection like pneumonia. (L. May, C. Hillermann, S. Patil 2016). Displaced rib fractures can also damage other tissues or organs, increasing the risk of a collapsed lung/pneumothorax or internal bleeding. It is recommended to seek immediate medical attention if symptoms develop like:
Shortness of breath
Difficulty breathing
A bluish color of the skin caused by lack of oxygen
A persistent cough with mucus
Chest pain when breathing in and out
Fever, sweating, and chills
Rapid heart rate
The Power of Chiropractic Care In Injury Rehabilitation
Liebsch, C., Seiffert, T., Vlcek, M., Beer, M., Huber-Lang, M., & Wilke, H. J. (2019). Patterns of serial rib fractures after blunt chest trauma: An analysis of 380 cases. PloS one, 14(12), e0224105. https://doi.org/10.1371/journal.pone.0224105
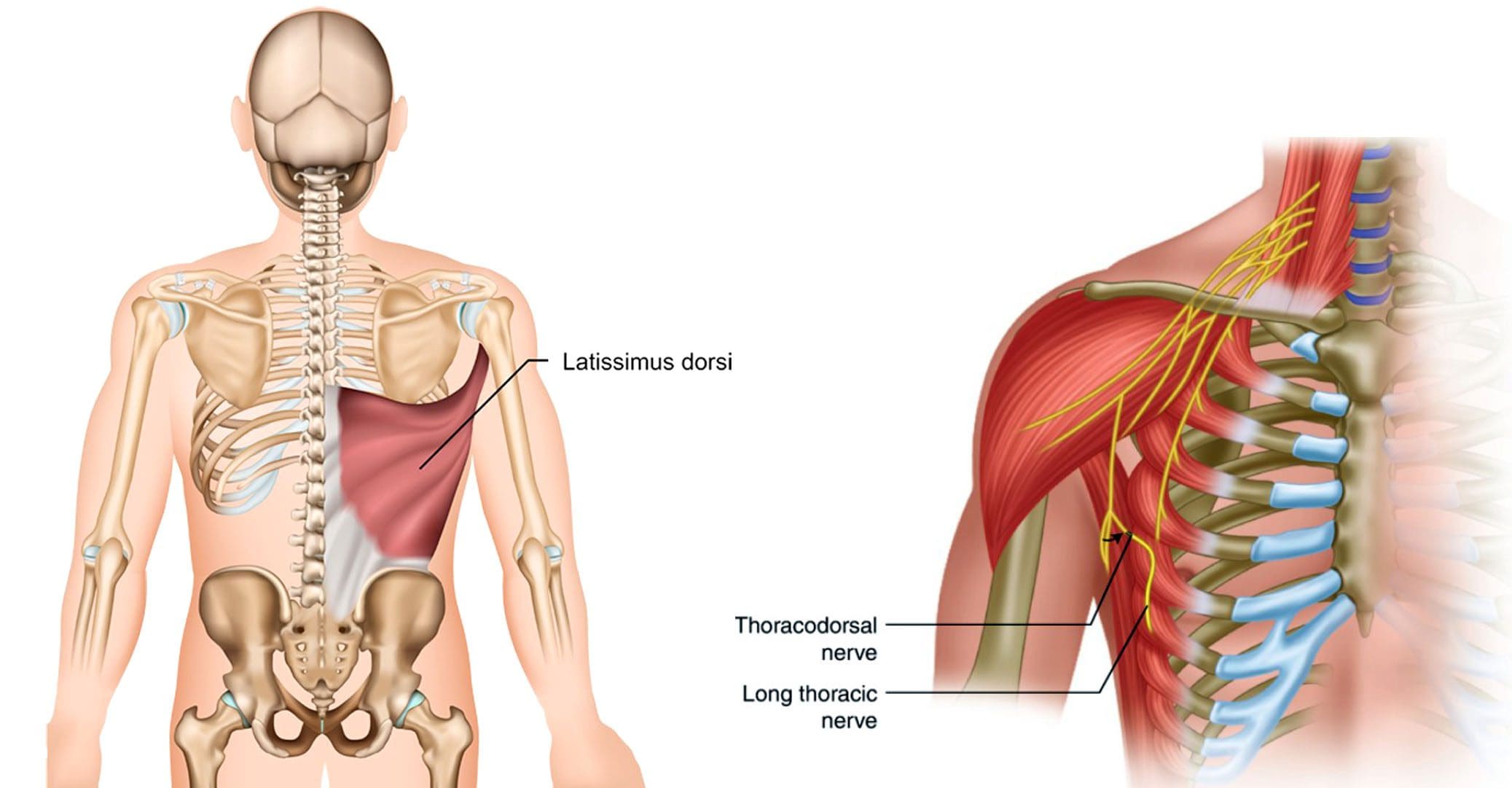
Individuals experiencing pain symptoms like shooting, stabbing, or electrical sensations to the latissimus dorsi of the upper back could be caused by a nerve injury to the thoracodorsal nerve. Can knowing the anatomy and symptoms help healthcare providers develop an effective treatment plan?
Thoracodorsal Nerve
Also known as the middle subscapular nerve or the long subscapular nerve, it branches out from a part of the brachial plexus and provides motor innervation/function to the latissimus dorsi muscle.
Anatomy
The brachial plexus is a network of nerves that stem from the spinal cord in the neck. The nerves supply most of the sensation and movement of the arms and hands, with one on each side. Its five roots come from the spaces between the fifth through eighth cervical vertebrae and the first thoracic vertebra. From there, they form a larger structure, then divide, re-combine, and divide again to form smaller nerves and nerve structures as they travel down the armpit. Through the neck and chest, the nerves eventually join and form three cords that include:
Lateral cord
Medial cord
Posterior cord
The posterior cord produces major and minor branches that include:
Axillary nerve
Radial nerve
The minor branches include:
Superior subscapular nerve
Inferior subscapular nerve
Thoracodorsal nerve
Structure and Position
The thoracodorsal nerve branches off the posterior cord in the armpit and travels down, following the subscapular artery, to the latissimus dorsi muscle.
It connects to the upper arm, stretches across the back of the armpit, forming the axillary arch, and then expands into a large triangle that wraps around the ribs and the back.
The thoracodorsal nerve lies deep in the latissimus dorsi, and the lower edge typically reaches close to the waist.
Variations
There is a standard location and course of the thoracodorsal nerve, but individual nerves are not the same in everyone.
The nerve typically branches off the posterior cord of the brachial plexus from three different points.
The lats can have a rare anatomical variation known as a Langer’s arch, which is an extra part that connects to muscles or connective tissue of the upper arm beneath the common connecting point.
In individuals with this abnormality, the thoracodorsal nerve supplies function/innervation) to the arch. (Ahmed M. Al Maksoud et al., 2015)
Function
The latissimus dorsi muscle cannot function without the thoracodorsal nerve. The muscle and nerve help:
Stabilize the back.
Pull the body weight up when climbing, swimming, or doing pull-ups.
Assist with breathing by expanding the rib cage during inhalation and contracting when exhaling. (Encyclopaedia Britannica. 2023)
Rotate the arm inward.
Pull the arm toward the center of the body.
Extend the shoulders by working with the teres major, teres minor, and posterior deltoid muscles.
Bring down the shoulder girdle by arching the spine.
Pain that can be shooting, stabbing, or electrical sensations.
Numbness, tingling.
Weakness and loss of function in the associated muscles and body parts, including wrist and finger drop.
Because of the nerve’s path through the armpit, doctors have to be cautious of the anatomical variants so they don’t inadvertently damage a nerve during breast cancer procedures, including axillary dissection.
The procedure is performed to examine or remove lymph nodes and is used in staging breast cancer and in treatment.
According to a study, 11% of individuals with axillary lymph node dissection suffered damage to the nerve. (Roser Belmonte et al., 2015)
Breast Reconstruction
In breast reconstruction surgery, the lats can be used as a flap over the implant.
Depending on the circumstances, the thoracodorsal nerve can be left intact or severed.
There is some evidence that leaving the nerve intact can cause the muscle to contract and dislocate the implant.
An intact thoracodorsal nerve may also cause atrophy of the muscle, which can lead to shoulder and arm weakness.
Graft Uses
A portion of the thoracodorsal nerve is commonly used in nerve graft reconstruction to restore function after injury, which includes the following:
Musculocutaneous nerve
Accessory nerve
Axillary nerve
The nerve can also be used to restore nerve function to the triceps muscle in the arm.
Rehabilitation
If the thoracodorsal nerve is injured or damaged, treatments can include:
Braces or splints.
Physical therapy to improve range of motion, flexibility, and muscle strength.
If there is compression, surgery may be required to alleviate the pressure.
Exploring Integrative Medicine
References
Chu B, Bordoni B. Anatomy, Thorax, Thoracodorsal Nerves. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539761/
Al Maksoud, A. M., Barsoum, A. K., & Moneer, M. M. (2015). Langer’s arch: a rare anomaly affects axillary lymphadenectomy. Journal of surgical case reports, 2015(12), rjv159. https://doi.org/10.1093/jscr/rjv159
Britannica, The Editors of Encyclopaedia. “latissimus dorsi“. Encyclopedia Britannica, 30 Nov. 2023, https://www.britannica.com/science/latissimus-dorsi. Accessed 2 January 2024.
Belmonte, R., Monleon, S., Bofill, N., Alvarado, M. L., Espadaler, J., & Royo, I. (2015). Long thoracic nerve injury in breast cancer patients treated with axillary lymph node dissection. Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer, 23(1), 169–175. https://doi.org/10.1007/s00520-014-2338-5
Kwon, S. T., Chang, H., & Oh, M. (2011). Anatomic basis of interfascicular nerve splitting of innervated partial latissimus dorsi muscle flap. Journal of plastic, reconstructive & aesthetic surgery : JPRAS, 64(5), e109–e114. https://doi.org/10.1016/j.bjps.2010.12.008
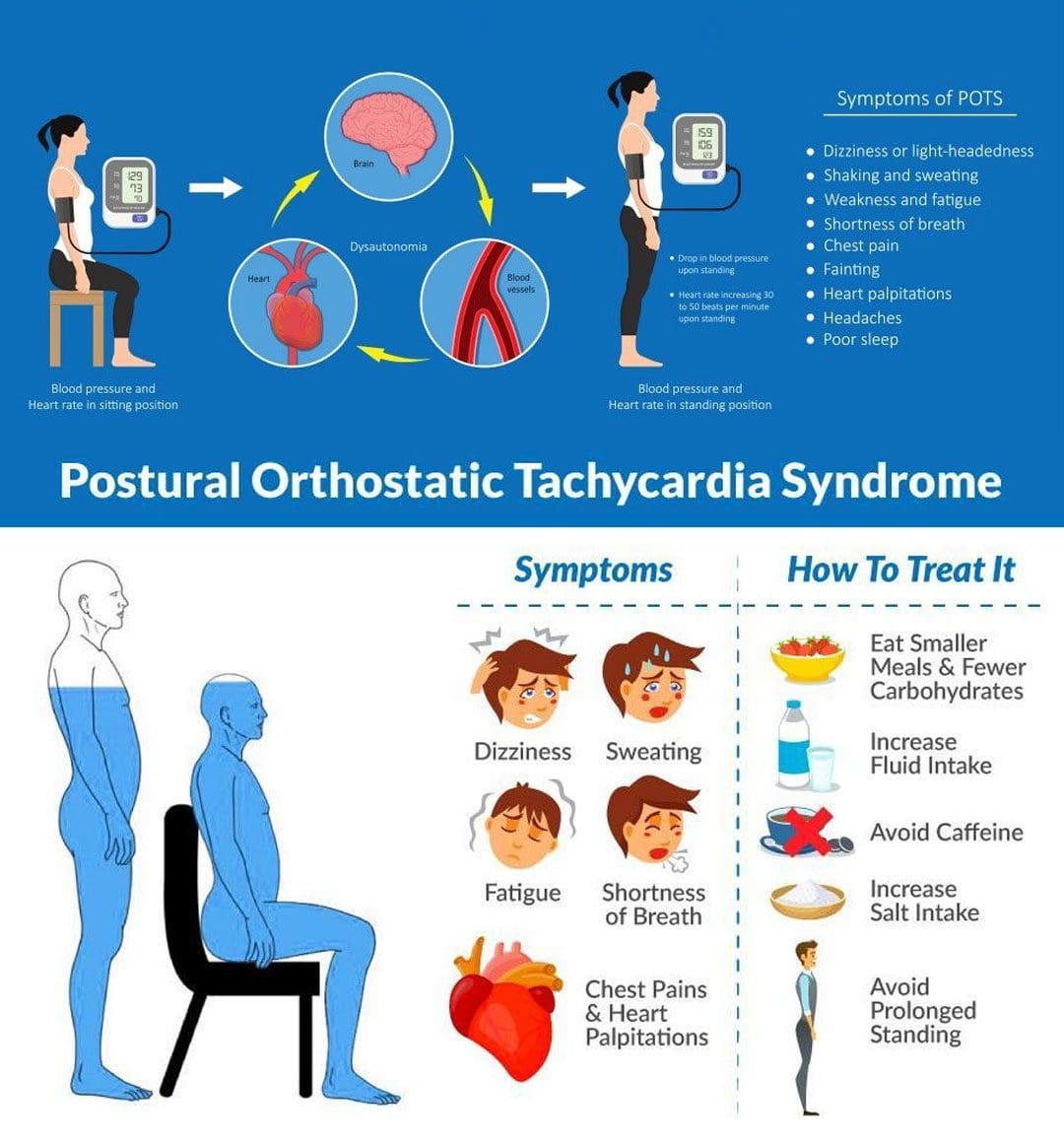
Postural orthostatic tachycardia syndrome is a medical condition that causes lightheadedness and palpitations after standing. Can lifestyle adjustments and multidisciplinary strategies help reduce and manage symptoms?
Postural Orthostatic Tachycardia Syndrome – POTS
Postural orthostatic tachycardia syndrome, or POTS, is a condition that varies in severity from relatively mild to incapacitating. With POTS:
The heart rate increases dramatically with body position.
This condition often affects young individuals.
Most individuals with postural orthostatic tachycardia syndrome are women between the ages of 13 and 50.
Some individuals have a family history of POTS; some individuals report POTS began after an illness or stressor, and others report it began gradually.
It usually resolves over time.
Treatment can be beneficial.
Diagnosis is based on assessing blood pressure and pulse/heart rate.
Symptoms
Postural orthostatic tachycardia syndrome can affect young individuals who are otherwise healthy and can begin suddenly. It usually happens between the ages of 15 and 50, and women are more likely to develop it than men. Individuals can experience various symptoms within a few minutes of standing up from a lying or seated position. The symptoms can occur regularly and daily. The most common symptoms include: (National Institutes of Health. National Center for Advancing Translational Sciences. Genetic and Rare Diseases Information Center. 2023)
Anxiety
Lightheadedness
A feeling like you’re about to pass out.
Palpitations – sensing rapid or irregular heart rate.
Dizziness
Headaches
Blurred vision
Legs turn to reddish-purple.
Weakness
Tremors
Fatigue
Sleep problems
Trouble concentrating/brain fog.
Individuals may also experience recurrent episodes of fainting, usually without any trigger/s other than standing up.
Individuals can experience any combination of these symptoms.
Sometimes, individuals cannot handle sports or exercise and may feel light-headed and dizzy in response to mild or moderate physical activity, which can be described as exercise intolerance.
Associated Effects
Postural orthostatic tachycardia syndrome can be associated with other dysautonomia or nervous system syndromes, like neurocardiogenic syncope.
Individuals are often co-diagnosed with other conditions like:
Chronic fatigue syndrome
Ehlers-Danlos syndrome
Fibromyalgia
Migraines
Other autoimmune conditions.
Bowel conditions.
Causes
Usually, standing up causes blood to rush from the torso to the legs. The sudden change means less blood is available for the heart to pump. To compensate, the autonomic nervous system sends signals to the blood vessels to constrict to push more blood to the heart and maintain blood pressure and a normal heart rate. Most individuals do not experience significant changes in blood pressure or pulse when standing up. Sometimes, the body is unable to perform this function correctly.
If blood pressure drops from standing and causes symptoms like lightheadness, it is known as orthostatic hypotension.
If the blood pressure remains normal, but the heart rate gets faster, it is POTS.
The exact factors that cause postural orthostatic tachycardia syndrome are different in individuals but are related to changes in:
The autonomic nervous system, adrenal hormone levels, total blood volume, and poor exercise tolerance. (Robert S. Sheldon et al., 2015)
Autonomic Nervous System
The autonomic nervous system controls blood pressure and heart rate, which are the areas of the nervous system that manage internal bodily functions like digestion, respiration, and heart rate. It is normal for blood pressure to drop slightly and the heart rate to speed up a little when standing. With POTS, these changes are more pronounced.
POTS is considered a type of dysautonomia, which is diminished regulation of the autonomic nervous system.
Several other syndromes are also thought to be related to dysautonomia, like fibromyalgia, irritable bowel syndrome, and chronic fatigue syndrome.
It isn’t clear why the syndrome or any of the other types of dysautonomia develop, but there seems to be a familial predisposition.
Sometimes the first episode of POTS manifests after a health event like:
Pregnancy
Acute infectious illness, for example, a severe case of influenza.
An episode of trauma or concussion.
Major surgery
Diagnosis
A diagnostic evaluation will include a medical history, a physical examination, and diagnostic tests.
The healthcare provider will take blood pressure and pulse at least twice. Once while lying down and once while standing.
Blood pressure measurements and pulse rate lying down, sitting, and standing are orthostatic vitals.
Typically, standing up increases the heart rate by 10 beats per minute or less.
With POTS, heart rate increases by 30 beats per minute while blood pressure remains unchanged. (Dysautonomia International. 2019)
The heart rate stays elevated for over a few seconds upon standing/usually 10 minutes or more.
Symptoms happen frequently.
Lasts more than a few days.
Positional pulse changes are not the only diagnostic consideration for postural orthostatic tachycardia syndrome, as individuals can experience this change with other conditions.
During this test, blood pressure and pulse are measured several times when lying on a table and when the table is moved to an upright position.
Differential Diagnosis
There are various causes of dysautonomia, syncope, and orthostatic hypotension.
Throughout the evaluation, the healthcare provider may look at other conditions, like dehydration, deconditioning from prolonged bed rest, and diabetic neuropathy.
Medications like diuretics or blood pressure medication can cause similar effects.
Treatment
Several approaches are used in managing POTS, and individuals may require a multidisciplinary approach. The healthcare provider will advise regularly checking blood pressure and pulse at home to discuss the results when going in for medical checkups.
Fluids and Diet
Drinking non-caffeinated fluids can keep the body hydrated.
A healthcare provider can calculate the right amount of fluids that are needed each day.
Overnight dehydration is common, so it is especially important to drink fluids first thing in the morning, preferably before getting out of bed and standing.
Exercise and physical therapy can help the body learn to adjust to an upright position.
Because it can be challenging to exercise when dealing with POTS, a targeted exercise program under supervision may be required.
An exercise program may begin with swimming or using rowing machines, which do not require upright posture. (Dysautonomia International. 2019)
After a month or two, walking, running, or cycling may be added.
Studies have shown that individuals with POTS, on average, have smaller cardiac chambers than individuals who don’t have the condition.
Regular aerobic exercise has been shown to increase cardiac chamber size, slow heart rate, and improve symptoms. (Qi Fu, Benjamin D. Levine. 2018)
Individuals must continue an exercise program for the long term to keep symptoms from returning.
Medication
Prescription medications to manage POTS include midodrine, beta-blockers, pyridostigmine – Mestinon, and fludrocortisone. (Dysautonomia International. 2019)
Ivabradine, used for the heart condition of sinus tachycardia, has also been used effectively in some individuals.
Conservative Interventions
Other ways to help prevent symptoms include:
Sleeping in the head-up position by elevating the head of the bed off the ground 4 to 6 inches utilizing an adjustable bed, blocks of wood, or risers.
This increases the blood volume in circulation.
Performing countermeasure maneuvers like squatting, squeezing a ball, or crossing the legs. (Qi Fu, Benjamin D. Levine. 2018)
Wearing compression stockings to prevent too much blood from flowing into the legs when standing can help avoid orthostatic hypotension. (Dysautonomia International. 2019)
Conquering Congestive Heart Failure
References
National Institutes of Health. National Center for Advancing Translational Sciences. Genetic and Rare Diseases Information Center (GARD). (2023). Postural orthostatic tachycardia syndrome.
Sheldon, R. S., Grubb, B. P., 2nd, Olshansky, B., Shen, W. K., Calkins, H., Brignole, M., Raj, S. R., Krahn, A. D., Morillo, C. A., Stewart, J. M., Sutton, R., Sandroni, P., Friday, K. J., Hachul, D. T., Cohen, M. I., Lau, D. H., Mayuga, K. A., Moak, J. P., Sandhu, R. K., & Kanjwal, K. (2015). 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart rhythm, 12(6), e41–e63. https://doi.org/10.1016/j.hrthm.2015.03.029
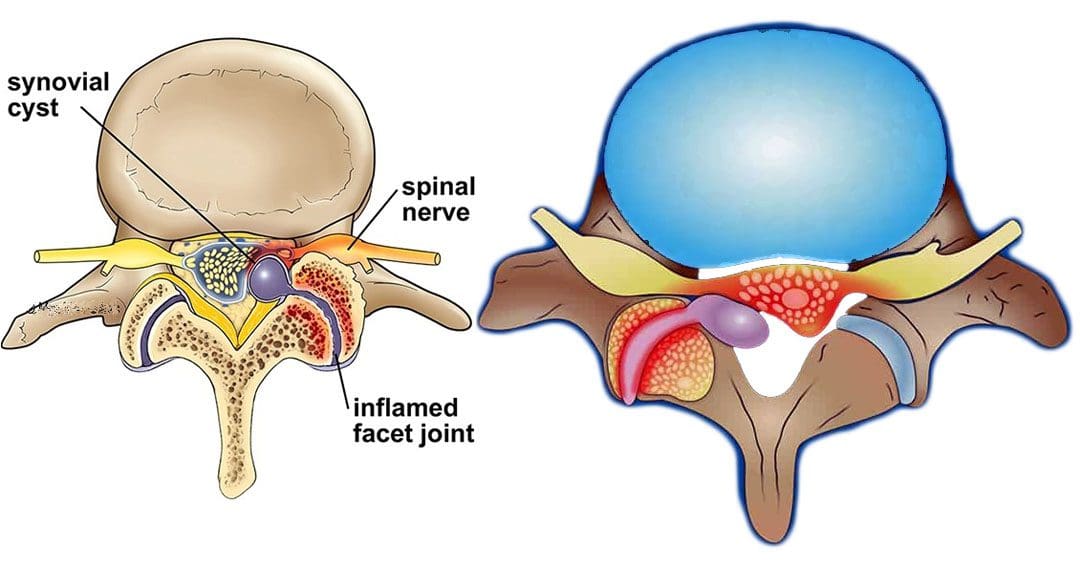
Individuals that have gone through a back injury may develop a synovial spinal cyst as a way to protect the spine that could cause pain symptoms and sensations. Can knowing the signs help healthcare providers develop a thorough treatment plan to relieve pain, prevent worsening of the condition and other spinal conditions?
Spinal Synovial Cysts
Spinal synovial cysts are benign fluid-filled sacs that develop in the spine’s joints. They form because of spinal degeneration or injury. The cysts can form anywhere in the spine, but most occur in the lumbar region/lower back. They typically develop in the facet joints or junctions that keep the vertebrae/spinal bones interlocked.
Symptoms
In most cases, synovial cysts don’t cause symptoms. However, the doctor or specialist will want to monitor for signs of degenerative disc disease, spinal stenosis, or cauda equina syndrome. When symptoms do present, they typically cause radiculopathy or nerve compression, which can cause back pain, weakness, numbness, and radiating pain caused by the irritation. The severity of symptoms depends on the size and location of the cyst. Synovial cysts can affect one side of the spine or both and can form at one spinal segment or at multiple levels.
Effects Can Include
Radiculopathy symptoms can develop if the cyst or inflammation caused by the cyst comes into contact with a spinal nerve root. This can cause sciatica, weakness, numbness, or difficulty controlling certain muscles.
Neurogenic claudication/impingement and inflammation of spinal nerves can cause cramping, pain, and/or tingling in the lower back, legs, hips, and buttocks. (Martin J. Wilby et al., 2009)
If the spinal cord is involved, it may cause myelopathy/severe spinal cord compression that can cause numbness, weakness, and balance problems. (Dong Shin Kim et al., 2014)
Symptoms related to cauda equina, including bowel and/or bladder problems, leg weakness, and saddle anesthesia/loss of sensation in the thighs, buttocks, and perineum, can present but are rare, as are synovial cysts in the middle back and neck. If thoracic and cervical synovial cysts develop, they can cause symptoms like numbness, tingling, pain, or weakness in the affected area.
Causes
Spinal synovial cysts are generally caused by degenerative changes like osteoarthritis that develop in a joint over time. With regular wear and tear, facet joint cartilage/the material in a joint that provides protection, a smooth surface, friction reduction, and shock absorption begins to waste away. As the process continues, the synovium can form a cyst.
Traumas, large and small, have inflammatory and degenerative effects on joints that can result in the formation of a cyst.
Around a third of individuals who have a spinal synovial cyst also have spondylolisthesis.
This condition is when a vertebrae slips out of place or out of alignment onto the vertebra underneath.
It is a sign of spinal instability.
Instability can occur in any spine area, but L4-5 are the most common levels.
This segment of the spine takes most of the upper body weight.
Epidural corticosteroid injections can reduce inflammation and could be an option to relieve pain.
Patients are recommended to receive no more than three injections per year.
Surgical Options
For severe or persistent cases, a doctor may recommend decompression surgery to remove the cyst and surrounding bone to relieve pressure on the nerve root. Surgical options range from minimally invasive endoscopic procedures to larger, open surgeries. The best surgical option varies based on the severity of the situation and whether associated disorders are present. Surgical options include:
Laminectomy – Removal of the bony structure that protects and covers the spinal canal/lamina.
Hemilaminectomy – A modified laminectomy where a smaller portion of the lamina is removed.
Facetectomy – The removal of part of the affected facet joint where the synovial cyst is located, usually following a laminectomy or hemilaminectomy.
Fusionof the facet joints and vertebra – Decreases vertebral mobility in the injured area.
Most individuals experience immediate pain relief following a laminectomy or hemilaminectomy.
Fusion can take six to nine months to heal completely.
If surgery is performed without fusion where the cyst originated, the pain could return, and another cyst could form within two years.
Surgery Complications include infection, bleeding, and injury to the spinal cord or nerve root.
How I Gained My Mobility Back With Chiropractic
References
Wilby, M. J., Fraser, R. D., Vernon-Roberts, B., & Moore, R. J. (2009). The prevalence and pathogenesis of synovial cysts within the ligamentum flavum in patients with lumbar spinal stenosis and radiculopathy. Spine, 34(23), 2518–2524. https://doi.org/10.1097/BRS.0b013e3181b22bd0
Kim, D. S., Yang, J. S., Cho, Y. J., & Kang, S. H. (2014). Acute myelopathy caused by a cervical synovial cyst. Journal of Korean Neurosurgical Society, 56(1), 55–57. https://doi.org/10.3340/jkns.2014.56.1.55
Epstein, N. E., & Baisden, J. (2012). The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surgical neurology international, 3(Suppl 3), S157–S166. https://doi.org/10.4103/2152-7806.98576
For individuals working at a desk or work station where the majority of the work is done in a sitting position and increases the risk for a variety of health problems, can using a standing desk help prevent musculoskeletal problems and improve short and long-term wellness?
Stand Desks
More than 80% of jobs are done in a seated position. Stand desks have proven to help. (Allene L. Gremaud et al., 2018) An adjustable stand desk is intended to be the standing height of an individual. Some desks can be lowered to use while sitting. These desks can improve:
Blood circulation
Back pain
Energy
Focus
Individuals who are less sedentary may experience decreased depression, anxiety, and risk of chronic disease.
Improve Posture and Decrease Back Pain
Sitting for prolonged periods can cause fatigue and physical discomfort. Back pain symptoms and sensations are common, especially when practicing unhealthy postures, already dealing with existing back problems, or using a non-ergonomic desk set-up. Instead of only sitting or standing for the whole workday, alternating between sitting and standing is far healthier. Practicing sitting and standing regularly reduces body fatigue and lower back discomfort. (Alicia A. Thorp et al., 2014) (Grant T. Ognibene et al., 2016)
Increases Energy Levels
Prolonged sitting correlates with fatigue, reduced energy, and productivity. A sit-stand desk can provide benefits like increased productivity levels. Researchers discovered that sit-stand desks could improve the general health and productivity of office workers. Individuals in the study reported:
According to the CDC, six in 10 individuals in the U.S. have at least one chronic disease, like diabetes, heart disease, stroke, or cancer. Chronic disease is the leading cause of death and disability, as well as a leading force of healthcare costs. (Centers for Disease Control and Prevention. 2023) While further research is needed to see if standing desks can reduce the risk of chronic disease, one study looked to quantify the association between sedentary time and the risk of chronic disease or death. Researchers reported that sedentariness for prolonged periods was independently associated with negative health outcomes regardless of physical activity. (Aviroop Biswas et al., 2015)
Improved Mental Focus
Sitting for extended periods slows down blood circulation. This decreased blood flow to the brain lowers cognitive function and increases the risk of neurodegenerative conditions. One study confirmed that healthy individuals who worked in a prolonged sitting position had reduced brain blood flow. The study found that frequent, short walks could help prevent this. (Sophie E. Carter et al., 2018) Standing increases blood and oxygen circulation. This improves cognitive function, which also helps improve focus and concentration.
Depression and Anxiety Reduction
Modern lifestyles typically contain large amounts of sedentary behavior.
However, there is a small amount about the mental health risks of prolonged sedentary behavior. There have been a few studies aimed at improving public understanding. One study focused on a group of older adults, having them self-report sedentary habits that included television, internet, and reading time. This information was compared to their individual scoring on the Centre of Epidemiological Studies Depression scale. (Mark Hamer, Emmanuel Stamatakis. 2014)
The researchers found that certain sedentary behaviors are more harmful to mental health than others.
Television watching, for example, resulted in increased depressive symptoms and decreased cognitive function. (Mark Hamer, Emmanuel Stamatakis. 2014)
Internet use had the opposite effect, decreasing depressive symptoms and increasing cognitive function.
Researchers theorize that the results come from the contrasting environmental and social contexts in which they are happening. (Mark Hamer, Emmanuel Stamatakis. 2014)
Another study looked at the possible correlation between sedentary behavior and anxiety.
Incorporating a standing desk into the workspace can help to reduce the negative effects of sedentary behaviors, leading to improved productivity, improved mental and physical health, and a healthy work environment for individuals who work long hours at a desk or workstation.
Understanding Academic Low Back Pain: Impact and Chiropractic Solutions
References
Gremaud, A. L., Carr, L. J., Simmering, J. E., Evans, N. J., Cremer, J. F., Segre, A. M., Polgreen, L. A., & Polgreen, P. M. (2018). Gamifying Accelerometer Use Increases Physical Activity Levels of Sedentary Office Workers. Journal of the American Heart Association, 7(13), e007735. https://doi.org/10.1161/JAHA.117.007735
Thorp, A. A., Kingwell, B. A., Owen, N., & Dunstan, D. W. (2014). Breaking up workplace sitting time with intermittent standing bouts improves fatigue and musculoskeletal discomfort in overweight/obese office workers. Occupational and environmental medicine, 71(11), 765–771. https://doi.org/10.1136/oemed-2014-102348
Ognibene, G. T., Torres, W., von Eyben, R., & Horst, K. C. (2016). Impact of a Sit-Stand Workstation on Chronic Low Back Pain: Results of a Randomized Trial. Journal of occupational and environmental medicine, 58(3), 287–293. https://doi.org/10.1097/JOM.0000000000000615
Ma, J., Ma, D., Li, Z., & Kim, H. (2021). Effects of a Workplace Sit-Stand Desk Intervention on Health and Productivity. International journal of environmental research and public health, 18(21), 11604. https://doi.org/10.3390/ijerph182111604
Centers for Disease Control and Prevention. Chronic disease.
Biswas, A., Oh, P. I., Faulkner, G. E., Bajaj, R. R., Silver, M. A., Mitchell, M. S., & Alter, D. A. (2015). Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Annals of internal medicine, 162(2), 123–132. https://doi.org/10.7326/M14-1651
Carter, S. E., Draijer, R., Holder, S. M., Brown, L., Thijssen, D. H. J., & Hopkins, N. D. (2018). Regular walking breaks prevent the decline in cerebral blood flow associated with prolonged sitting. Journal of applied physiology (Bethesda, Md. : 1985), 125(3), 790–798. https://doi.org/10.1152/japplphysiol.00310.2018
Hamer, M., & Stamatakis, E. (2014). Prospective study of sedentary behavior, risk of depression, and cognitive impairment. Medicine and science in sports and exercise, 46(4), 718–723. https://doi.org/10.1249/MSS.0000000000000156
Teychenne, M., Costigan, S. A., & Parker, K. (2015). The association between sedentary behaviour and risk of anxiety: a systematic review. BMC public health, 15, 513. https://doi.org/10.1186/s12889-015-1843-x
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine