While some disc herniations don’t cause symptoms, individuals who are overweight with a herniated disc may experience obesity pressure symptoms such as pain, weakness, numbness, or tingling. Can implementing a physical therapy and weight loss treatment program help individuals find relief?
Obesity Pressure
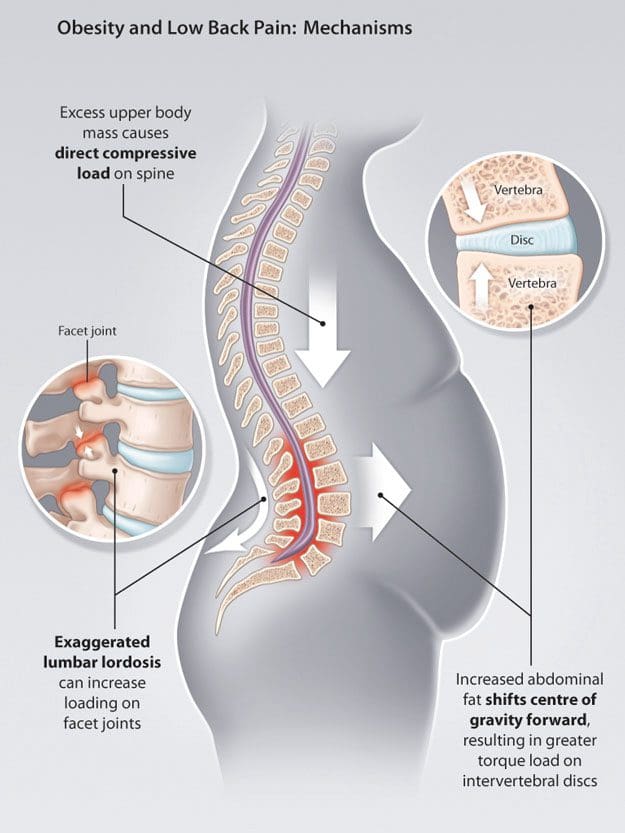
Obesity is one major factor that can contribute to a herniated disc and chronic back pain. When the body has to carry added weight, it can lead to obesity pressure on the intervertebral discs and affect posture and spine position. Researchers have found that other factors, such as inflammation or metabolic changes associated with obesity, can also be involved. (Sheng B. et al., 2017) For individuals who are overweight, weight loss can help resolve a herniated disc combined with physical therapy and can significantly increase herniated disc prevention. (Tokmak M. et al., 2015)
Spine Problems
According to Dr. Alexander Jimenez, owner and head chiropractor at Injury Medical Chiropractic and Functional Medicine Clinic, “When the position of the pelvis and lumbar spine shift out of alignment and become altered, it can profoundly contribute to advanced wearing away of outer fibers in the back region of the discs. These outer fibers house and protect the soft material that cushions and absorbs shock in the spine. Over time, the obesity pressure wear and tear on the fibers can cause chronic pain and microscopic radial tears, leading to a complete rupture.” A rupture causes the soft material to leak, irritate, and inflame surrounding nerve roots. Most herniated discs occur between the sides and back of the vertebra.
Movement Problems
Obesity makes movement difficult, often causing symptoms like shortness of breath and/or early fatigue and exhaustion even with minimal physical activity.
Physical therapy and exercise help relieve obesity and disc herniation.
However, the obesity pressure and herniation pain can make it hard to participate in cardiovascular exercises on a regular basis.
Diagnosis Complications
Obesity can interfere with the diagnosis and treatment of spinal diseases.
This is because weight restrictions and certain imaging tests, like a spinal MRI, can be difficult or impossible to obtain.
A physical examination might not be able to identify signs of nerve compression if an individual is obese. These factors can delay diagnosis.
Disc Position and Posture
Obesity is not the only thing that places pressure on the discs. An individual’s body position significantly influences the health of the shock-absorbing cushions. Sitting generates the most pressure, followed by standing, while lying on your back places the least strain on the discs and, depending on the injury, may help relieve symptoms.
Symptoms depend on the location of the herniation.
The two most common locations are the cervical spine/neck area and the lumbar spine/lower back.
Disc herniations in the neck can affect the arms.
Disc herniations in the lower back affect the buttocks and legs.
Injury Medical Chiropractic and Functional Medicine Clinic
See a healthcare provider if you’re experiencing any of these symptoms. If it is a herniated disc causing symptoms, you might be started on 6 weeks of conservative treatment. This can include physical therapy, rest, health coaching, medication, and surgery, which may be recommended in certain cases. Overcoming these limitations is possible. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Weight Loss Techniques
References
Sheng, B., Feng, C., Zhang, D., Spitler, H., & Shi, L. (2017). Associations between Obesity and Spinal Diseases: A Medical Expenditure Panel Study Analysis. International journal of environmental research and public health, 14(2), 183. https://doi.org/10.3390/ijerph14020183
Tokmak, M., Altiok, I. B., Guven, M., Aras, A. B., & Cosar, M. (2015). Spontaneous Regression of Lumbar Disc Herniation After Weight Loss: Case Report. Turkish neurosurgery, 25(4), 657–661. https://doi.org/10.5137/1019-5149.JTN.9183-13.1
Can individuals have a full night of sleep by making small changes to their sleep posture to reduce general aches and pains?
Introduction
Many individuals know that after a long, hard day of working or running errands, getting much rest is necessary to reduce tension in the body and put it in a relaxed state. Getting a quick nap to a full night of sleep is important not only for the body but also for the posture. However, many people get a bad night’s rest from various environmental factors that can keep them from getting the full benefits of eight hours of sleep. It can range from stressful events impacting a person’s life to overlapping risk profiles correlated with chronic conditions. Today’s article focuses on how poor posture can affect sleep and how there are different ways for a person to get a good night’s rest, improve sleep posture, and find the right mattress and pillows to allow the individual to stay asleep. We discuss with certified medical providers who inform our patients how various environmental factors can cause overlapping risk profiles and not getting a full night of rest. While asking informed questions to our associated medical providers, we advise patients to incorporate various techniques to improve sleep posture when getting a full night of quality sleep. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
Poor Posture Affecting Sleep
Do you feel extremely tired throughout the day, even after a full night? Do you experience stiffness in the morning that gets better throughout the day? Or how often do you wake up constantly at night and have trouble staying asleep? Many individuals who have experienced these scenarios are frequently correlated with bad sleeping habits. Many individuals have dealt with poor sleeping habits throughout the day due to environmental factors that can impact their sleep. Some environmental factors, like poor posture, can affect how people sleep at night. Poor posture has always been associated with musculoskeletal disorders. When musculoskeletal disorders have overlapping risk profiles from physical workload and psychological stress, it can become a predictor or even correlate with sleep disorders. (Hammig, 2020) This is because having habitual in-bed behaviors like movement and posture could cause health complications and prevent people from getting a good night’s rest. (Elnaggar et al., 2023)
This is due to how individuals’ posture can affect their sleep quality and overall health. For instance, individuals dealing with chronic spinal pain will begin to develop poor posture over time. When this happens, it can coexist with other comorbidities like insomnia, which can lead to a larger negative effect on a person’s physical and mental functioning while preventing them from being less productive and having poor quality of sleep. (Bilterys et al., 2021) When people experience spinal pain, causing them to develop poor posture, it can lead to sleep disturbances. The correlation between sleep disturbances and poor posture can cause impairment of the physiological process that can contribute to maintaining chronic pain. (Skillgate et al., 2021) However, there are numerous ways for people to get a good night’s rest while improving their posture.
The Benefits Of Stretching-Video
Ways To Get a Good Night Rest
When it comes to finding ways to get a good night’s rest, many people will try to devise solutions to establish a routine for their bedtime. Some of the ways people can utilize for a good night’s rest include:
Lowering room temperature
Keeping a sleep diary
Limit caffeinated drinks in the evening
Limit electronics before bed
Stick and create a sleep schedule
By creating some of these habits and sticking with them, many people can get much-needed rest and more energy when they wake up. At the same time, proper sleeping habits can help improve sleeping posture.
Improving Sleep Posture
There is no right way to do it regarding proper sleeping habits and improving sleep posture. Everyone has a position they favor more to be comfortable. For instance, a person who sleeps on the back is more relaxed than sleeping on their sides. Since sleep posture is associated with sleep quality, poor posture may provoke increased wake time and affect a person’s ability to maintain an asleep state. (Cary et al., 2021) So, by listening to the body and following its natural sleep flow, a person can stay asleep longer and be comfortable.
Finding The Right Mattress & Pillow
At the same time, improving one’s sleeping posture is not the only way to get a good night’s rest. Finding the right mattress and pillows is important, too. When people seek mattresses and pillows to improve their sleep quality, many often seek out tempur-pedic mattresses to support their body and have the best sleep. Many tempur-pedic mattresses can help reduce pressure from the body, making a person comfortable and minimizing movement. Additionally, new pillows supporting the neck and lower back can reduce somatic symptoms and provide neutral spinal alignment for the body. (Yamada et al., 2023) When it comes to having the best quality of sleep, it can be achievable with proper sleep habits, a new set of pillows and mattresses, and a comfortable position that will allow people to feel refreshed and re-energized.
References
Bilterys, T., Siffain, C., De Maeyer, I., Van Looveren, E., Mairesse, O., Nijs, J., Meeus, M., Ickmans, K., Cagnie, B., Goubert, D., Danneels, L., Moens, M., & Malfliet, A. (2021). Associates of Insomnia in People with Chronic Spinal Pain: A Systematic Review and Meta-Analysis. J Clin Med, 10(14). https://doi.org/10.3390/jcm10143175
Cary, D., Jacques, A., & Briffa, K. (2021). Examining relationships between sleep posture, waking spinal symptoms and quality of sleep: A cross sectional study. PLOS ONE, 16(11), e0260582. https://doi.org/10.1371/journal.pone.0260582
Elnaggar, O., Arelhi, R., Coenen, F., Hopkinson, A., Mason, L., & Paoletti, P. (2023). An interpretable framework for sleep posture change detection and postural inactivity segmentation using wrist kinematics. Sci Rep, 13(1), 18027. https://doi.org/10.1038/s41598-023-44567-9
Hammig, O. (2020). Work- and stress-related musculoskeletal and sleep disorders among health professionals: a cross-sectional study in a hospital setting in Switzerland. BMC Musculoskelet Disord, 21(1), 319. https://doi.org/10.1186/s12891-020-03327-w
Skillgate, E., Isacson Hjortzberg, M., Stromwall, P., Hallqvist, J., Onell, C., Holm, L. W., & Bohman, T. (2021). Non-Preferred Work and the Incidence of Spinal Pain and Psychological Distress-A Prospective Cohort Study. Int J Environ Res Public Health, 18(19). https://doi.org/10.3390/ijerph181910051
Yamada, S., Hoshi, T., Toda, M., Tsuge, T., Matsudaira, K., & Oka, H. (2023). Changes in neck pain and somatic symptoms before and after the adjustment of the pillow height. Journal of Physical Therapy Science, 35(2), 106-113. https://doi.org/10.1589/jpts.35.106
Can cervical retraction be a good addition to a home exercise program for individuals with neck pain, spinal arthritis, or needing to strengthen their neck muscles?
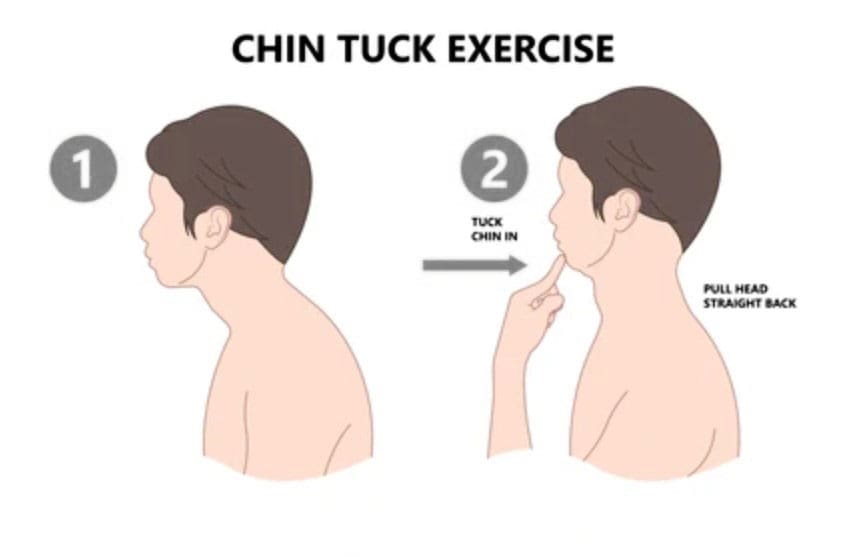
Cervical Retraction
Cervical retraction is a neck exercise that involves gently sliding the head backward while keeping the chin tucked. It can help with:
Neck pain
Stretching and loosening the muscles at the back of the neck.
Headaches
Tightness
Improve posture
Improve flexibility and mobility
Preparation
Basic steps for performing a cervical retraction exercise:
Sit upright with good posture.
Tuck your chin as far as you can comfortably.
Look up while keeping your chin tucked.
Rotate the neck 1-2 inches to each side.
Return to the starting position.
Stop the exercise if you experience pain.
You want to get good at this without loading the joints while learning the movement. Gently and accurately moving your head in alignment with the neck will help you find the correct head action as it moves. Then, it can be performed as a full exercise. Performing the movement correctly requires focus. This is why cervical retraction is done while sitting in a chair with proper posture. Individuals can also stand, but it is more complicated for the body to coordinate than sitting, but it can be done once the individual has practiced.
Sitting or Standing
Gently tuck your chin down toward your neck.
The focus is alignment.
Keeping your chin where it is, press your head back.
There will be soreness, especially for those with pain symptoms, but the neck should feel better.
Be mindful of any intense or severe pain resulting from cervical retraction.
Individuals with cervical spondylosis (neck arthritis) stop if pain presents. (Cleveland Clinic, 2023)
Other Neck Exercises
Another good neck-strengthening exercise is the isometric neck press. In this exercise, you move your head forward, backward, and to each side while your hand provides resistance. This develops flexibility and is recommended for those with arthritis in this area. (Sadeghi, A. et al., 2022) Other exercises include: (Pain Consultants of West Florida, 2019)
Neck extensions: Backward bending can help relieve nerve compression and ease the strain on the cervical spine.
Side rotation: This exercise can improve neck mobility.
Shoulder rolls: This exercise can help keep the neck and shoulder joints fluid.
Injury Medical Chiropractic and Functional Medicine Clinic
If you have a neck condition or radiculopathy that causes pain or other symptoms going down the arm or are unsure how to do it, check with a healthcare provider or physical therapist before trying the exercise. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Neck Injuries
References
North American Spine Society. (2012). Cervical exercise: The Backbone of Spine Treatment. https://www.spine.org/KnowYourBack/Prevention/Exercise/Cervical-Exercise
Cleveland Clinic. (2023). Could your neck pain actually be neck arthritis? https://my.clevelandclinic.org/health/diseases/17685-cervical-spondylosis
Pain Consultants of West Florida. (2019). Chronic Neck Pain: How Core Exercises Can Help. Our Blog. https://pcwfl.com/chronic-neck-pain-how-core-exercises-can-help/
Sadeghi, A., Rostami, M., Ameri, S., Karimi Moghaddam, A., Karimi Moghaddam, Z., & Zeraatchi, A. (2022). Effectiveness of isometric exercises on disability and pain of cervical spondylosis: a randomized controlled trial. BMC sports science, medicine & rehabilitation, 14(1), 108. https://doi.org/10.1186/s13102-022-00500-7
For individuals trying to retrain their body movements for back health improvement, what is the spinal area that helps the body twist, bend, and stand upright?
Lumbosacral Joint L5-S1
The L5-S1, also called the lumbosacral joint, is a term used to describe a part of the spine. It is where the lumbar spine ends and the sacral spine begins, and it connects these bones. The lumbosacral joint is also susceptible to misalignment and injury, such as disc herniation or a spinal disorder called spondylolisthesis.
The spinal column is the structure that allows the body to stand upright and helps you twist, bend, and alter trunk and neck position. Typically, 24 movable bones in the spine connect to the sacrum and the coccyx, or the tailbone. The sacrum and the coccyx each have multiple bones that fuse over time. L5-S1 consists of the last bone in the lumbar spine, called L5, and the triangle-shaped bone under it, known as the sacrum. S1 is at the top of the sacrum and comprises five fused bones.
Risk of Injury
Each area of the spine has a curve that goes in opposite directions. The places where the spinal curve directions change are junctional levels. The risk of injuries may be higher at junctional levels because the body weight shifts direction as the curves shift. The L5-S1 junction is located between the lumbar curve and the sacral curve. The lumbar curve sweeps forward, and the sacral curve goes backward.
The lumbosacral joint L5-S1 junction is highly vulnerable to misalignment, wear and tear, and injury. This is because the top of the sacrum is positioned at an angle for most individuals. Aging and injury increase the vulnerability of the L5-S1 junction even more. Pain coming from L5-S1 is usually treated with:
Heat and/or ice
Over-the-counter anti-inflammatory medications
Prescription pain medications
Muscle relaxers
Physical therapy
Chiropractic adjustments
Epidural steroid injections
If these therapies do not help, surgery may be recommended. L5-S1 is one of the two most common sites for back surgery.
Conditions
Disc herniation at L5-S1 is a common injury and cause of sciatica, which can cause pain and other issues (MedlinePlus, 2024). The L5-S1 junction is often the site of a condition known as spondylolisthesis.
Disc Herniation
Discs separate the vertebrae, cushioning the spinal column and allowing movement between vertebrae. A disc herniation means the disc slips out of place. (MedlinePlus, 2022) A disc herniation at L5-S1 is a common cause of sciatica. Symptoms of sciatica include:
Burning
Numbness
Pain or tingling that radiates from the buttock down the leg to the knee or foot.
Disc herniation can also cause chronic back pain and stiffness and trigger painful muscle spasms. Bowel problems are also possible with disc issues at L5-S1. Research links irritable bowel syndrome to herniated discs in the lower back. (Bertilson BC, Heidermakr A, Stockhaus M. 2015) Additional studies found disc problems at L5-S1 can lead to difficulty with sphincter control. (Akca N. et al., 2014) Initial treatments for disc herniation include rest and pain relievers to reduce inflammation and swelling, then physical therapy. Most recover with conservative interventions, and those who don’t may require a steroid injection or surgery. (MedlinePlus, 2022)
Spondylolisthesis
Spondylolisthesis occurs when a vertebra slips forward relative to the bone below it. The most common form of this condition is degenerative spondylolisthesis, which generally begins when the spine wears down with age. Isthmic spondylolisthesis is another common variation and starts as a tiny fracture in the pars interarticularis, a bone that connects the adjoining parts of the facet joint. (American Academy of Orthopaedic Surgeons, 2020) These fractures often occur before age 15, but symptoms do not develop until adulthood. Degeneration of the spine in later adulthood can further worsen the condition.
The angle of the sacrum can also contribute to spondylolisthesis. This is because the S1 tips down in the front and up in the back rather than being horizontal. Individuals with a greater tilt are usually at a higher risk of spondylolisthesis. (Gong S. et al., 2019) However, individuals with spondylolisthesis may not have any symptoms. Those who do may experience: (American Academy of Orthopaedic Surgeons, 2020)
Back stiffness
Standing difficulties
Walking difficulties
Lower back pain
Hamstring tightness
Spondylolisthesis is typically treated with non-surgical interventions that can include:
Pain medications
Heat and/or ice application
Physical therapy
Epidural steroid injections
Usually, non-surgical care is tried for at least six months. If pain and symptoms persist, surgery may be an option. Spinal fusion surgery can be effective but requires a long recovery time and can have additional risks.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Healing After Trauma
References
MedlinePlus. (2024). Sciatica. Retrieved from https://medlineplus.gov/sciatica.html
MedlinePlus. (2022). Herniated disk. Retrieved from https://medlineplus.gov/ency/article/000442.htm
American Association of Neurological Surgeons. (2024). Herniate disc. https://www.aans.org/patients/conditions-treatments/herniated-disc/
Bertilson, B. C., Heidermark, A., & Stockhaus, M. (2015). Irritable Bowel Syndrome–a Neurological Spine Problem. Journal of Advances in Medicine and Medical Research, 4(24), 4154–4168. https://doi.org/10.9734/BJMMR/2014/9746
Akca, N., Ozdemir, B., Kanat, A., Batcik, O. E., Yazar, U., & Zorba, O. U. (2014). Describing a new syndrome in L5-S1 disc herniation: Sexual and sphincter dysfunction without pain and muscle weakness. Journal of craniovertebral junction & spine, 5(4), 146–150. https://doi.org/10.4103/0974-8237.147076
American Academy of Orthopaedic Surgeons. (2020). Spondylolysis and spondylolisthesis. https://orthoinfo.aaos.org/en/diseases–conditions/spondylolysis-and-spondylolisthesis/
Gong, S., Hou, Q., Chu, Y., Huang, X., Yang, W., & Wang, Z. (2019). Anatomical factors and pathological parts of isthmic fissure and degenerative lumbar spondylolisthesis.
How are MRIs used to help diagnose bulging and herniated discs and help healthcare providers develop effective treatment programs for individuals experiencing back pain symptoms?
Herniated Bulging Disc MRI
A herniated bulging disc is often identified during magnetic resonance imaging (MRI); however, it’s usually an incidental finding that was done for other reasons where spinal problems and/or injuries are found. A bulging disc is relatively common, even in individuals who experience no symptoms. A herniated or bulging disc in the back can be identified with an MRI test, typically recommended when someone experiences back pain symptoms for at least six weeks. (American Academy of Neurological Surgeons, 2024) Normal wear and tear and age cause changes in the spinal disc/s cushion to bulge and become misaligned with the spine. (Brinjikji W. et al., 2015) And with a herniated disc, it can press against the spinal cord and nerves. Repeated heavy lifting, practicing unhealthy postures, a history of back injuries, or underlying health conditions are common causes.
Bulging Disc
Bulging discs are common even in healthy individuals but can be difficult to interpret independently on an MRI, so other symptoms and findings are as important in diagnosis.
Causes
A bulging disc is usually considered age-related degenerative changes that cause the disc to bulge downward with gravity. (Penn Medicine, 2018)
A significant bulge is expected to cause leg pain due to irritation to the nerves going down the legs. (Amin R. M., Andrade N. S., & Neuman B. J. 2017) As the condition progresses, more than one disc can be affected, leading to other spinal conditions, including spinal stenosis.
A Bulging Disc On MRI
A disc bulge will measure over 25% of the total disc circumference. Its displacement is usually 3 millimeters or less from the normal shape and position of the disc. (Radiopaedia, 2024)
Herniated Disc
A herniated disc shifts out of its correct position and compresses nearby spinal nerves, causing pain and mobility issues.
Herniated discs will measure less than 25% of the total disc circumference. However, herniation is based on the type and can include: (Wei B., & Wu H. 2023)
Disc Protrusion – the displacement is limited, and the ligaments are intact.
Disc Extrusion – part of the disc remains connected but has slipped through the annulus or outer covering of the disc.
Disc Sequestration – a free fragment has separated and broken off from the main disc.
Candidates For Spinal MRI
The MRI is generally safe for most, including those with implanted cardiac devices like newer-model pacemakers. (Bhuva A. N. et al., 2020) However, it’s important to ensure that the healthcare team is aware of cochlear implants or other devices so that necessary precautions can be taken. It is recommended for all individuals that symptoms be present for six weeks before an MRI. A specialist may want to see MRI results sooner, especially if symptoms include: (American Academy of Neurological Surgeons, 2024)
A specific injury, like a fall that caused the pain
Recent or current infection or fever with spinal symptoms
Significant weakness in arms or legs
Loss of pelvic sensation.
A history of metastatic cancer.
Loss of bladder or bowel control
An MRI may be needed if symptoms are rapidly worsening. However, many with a disc bulge don’t have symptoms at all. In most cases, an MRI is an outpatient procedure that can be completed in an hour or less but can take longer if contrast dye is used. The healthcare provider will provide specific instructions about MRI preparation.
Treatment
Treatment for a herniated or bulging disc depends on the cause and severity of symptoms.
Over-the-counter pain relief, including nonsteroidal anti-inflammatory drugs (NSAIDs).
Physical therapy
In rare cases that have not resolved with conservative treatment, surgery may be recommended.
Remember that the MRI findings may not identify or rule out all conditions, including muscle strains or ligament injuries, which may require different treatments, such as targeted stretches and exercises. (Brinjikji W. et al., 2015) (Fujii K. et al., 2019)
Herniated Disc
Treatment depends on the cause and severity of symptoms, if any. It can include stand-alone or a combination of physical therapy, medication, and steroid injections. Cases usually resolve in six to 12 weeks (Penn Medicine, 2018). Electrical nerve stimulation may be performed through specialized devices and/or acupuncture to help with nerve compression. (National Institute of Neurological Disorders and Stroke, 2020) Surgery may be recommended if conservative treatments fail to achieve significant pain relief and healing. (Wang S. et al., 2023)
Injury Medical Chiropractic and Functional Medicine Clinic
A healthcare provider can discuss treatment options such as pain medication, physical therapy, and surgery. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Root Causes of Spinal Stenosis
References
American Academy of Neurological Surgeons. (2024). Herniated disc. https://www.aans.org/patients/conditions-treatments/herniated-disc/
Brinjikji, W., Diehn, F. E., Jarvik, J. G., Carr, C. M., Kallmes, D. F., Murad, M. H., & Luetmer, P. H. (2015). MRI Findings of Disc Degeneration are More Prevalent in Adults with Low Back Pain than in Asymptomatic Controls: A Systematic Review and Meta-Analysis. AJNR. American journal of neuroradiology, 36(12), 2394–2399. https://doi.org/10.3174/ajnr.A4498
Penn Medicine. (2018). Bulging Disc vs. Herniated Disc: What’s The Difference? Penn Musculoskeletal and Rheumatology Blog. https://www.pennmedicine.org/updates/blogs/musculoskeletal-and-rheumatology/2018/november/bulging-disc-vs-herniated-disc
Wu, P. H., Kim, H. S., & Jang, I. T. (2020). Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. International journal of molecular sciences, 21(6), 2135. https://doi.org/10.3390/ijms21062135
Amin, R. M., Andrade, N. S., & Neuman, B. J. (2017). Lumbar Disc Herniation. Current reviews in musculoskeletal medicine, 10(4), 507–516. https://doi.org/10.1007/s12178-017-9441-4
American Academy of Orthopaedic Surgeons. (2022). Herniated disk in the lower back. https://orthoinfo.aaos.org/en/diseases–conditions/herniated-disk-in-the-lower-back/
Wei, B., & Wu, H. (2023). Study of the Distribution of Lumbar Modic Changes in Patients with Low Back Pain and Correlation with Lumbar Degeneration Diseases. Journal of pain research, 16, 3725–3733. https://doi.org/10.2147/JPR.S430792
Bhuva, A. N., Moralee, R., Moon, J. C., & Manisty, C. H. (2020). Making MRI available for patients with cardiac implantable electronic devices: growing need and barriers to change. European radiology, 30(3), 1378–1384. https://doi.org/10.1007/s00330-019-06449-5
Brinjikji, W., Luetmer, P. H., Comstock, B., Bresnahan, B. W., Chen, L. E., Deyo, R. A., Halabi, S., Turner, J. A., Avins, A. L., James, K., Wald, J. T., Kallmes, D. F., & Jarvik, J. G. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR. American journal of neuroradiology, 36(4), 811–816. https://doi.org/10.3174/ajnr.A4173
Fujii, K., Yamazaki, M., Kang, J. D., Risbud, M. V., Cho, S. K., Qureshi, S. A., Hecht, A. C., & Iatridis, J. C. (2019). Discogenic Back Pain: Literature Review of Definition, Diagnosis, and Treatment. JBMR plus, 3(5), e10180. https://doi.org/10.1002/jbm4.10180
Wang, S., Zhao, T., Han, D., Zhou, X., Wang, Y., Zhao, F., Shi, J., & Shi, G. (2023). Classification of cervical disc herniation myelopathy or radiculopathy: a magnetic resonance imaging-based analysis. Quantitative imaging in medicine and surgery, 13(8), 4984–4994. https://doi.org/10.21037/qims-22-1387
National Institute of Neurological Disorders and Stroke. (2020). Low back pain fact sheet. Retrieved from https://www.ninds.nih.gov/sites/default/files/migrate-documents/low_back_pain_20-ns-5161_march_2020_508c.pdf
Can correcting body misalignments and the elements of unhealthy posture help achieve a healthy posture?
Healthy Posture
Maintaining a healthy posture is more important than ever, as individuals from all walks of life realize how practicing awkward and unhealthy postures can wreak havoc on their bodies and quality of life. Unhealthy postures include rounding the upper and lower back, slouching, and forward head posture. Over time, these postures make daily activities more difficult or painful. Mobility, stability, and strengthening exercises can address unhealthy posture problems and issues, along with practicing correct sitting, standing, and resting postural habits to reinforce proper alignment daily. A chiropractic and physical therapy team can treat and train individuals to restore correct and healthy posture.
Body Alignment
Ideal posture involves correct body alignment or how the structural parts, such as the head, trunk, hips, knees, etc., relate to an individual’s form. Whether standing, sitting, lying down, or moving, body parts need to be balanced in relationship to each other to avoid unnecessary stress on the spine and musculoskeletal system. (Bone Health & Osteoporosis Foundation, 2024)
Posture Types
Posture is considered static when sitting or standing still and dynamic when moving. Both are categorized as active postures as they require the activation of stabilizing muscles to deal with gravity and maintain alignment. Lying down and remaining still is considered an inactive posture, as muscle involvement is minimal. However, both have the potential to be healthy or unhealthy.
Proper Body Alignment
An easy way to check proper alignment while standing is to stand against a wall with the base of the head, shoulder blades, and buttocks flush against the wall, with enough space for a hand wide enough to slide in between the wall and the small of the back. This exercise correctly lines up the head, shoulders, and hips to reduce or eliminate undue stress on the spine. Body balance is the foundation for active and inactive postures concerning workstations, industrial ergonomics, daily activities, and sports. (Mayo Clinic, 2023) Healthy alignment is a standard position in which all body joints are centered and balanced and the most mechanically efficient position for static or dynamic activities. Biomechanical efficiency (the ability to use the body’s muscles and joints to perform movements while minimizing energy use and maximizing output) enables the muscles surrounding the joints to work in balance and efficiently activate, which, in turn, helps reduce strain, tension, and injury. Balanced muscles also conserve energy, leading to better daily stamina.
Development of Imbalances
Individuals develop position and movement habits in joint positioning that have led to imbalanced muscles. When this is the case, some muscles can be chronically stretched, and others become chronically tight, all to hold the body up or move around, which can lead to postural conditions like upper crossed (Physiopedia, 2024) or lower crossed syndrome (Physiopedia, 2024) which often leads to pain and/or mobility issues.
Posture Assessment
The recommended way to determine if one’s posture is healthy or poor is by conducting a posture assessment. The examination looks at joint positions and gathers visual information about the planes into which parts of each joint move and the axes around which those movements occur (Singla D. and Veqar Z., 2014) (Debra Coglianese et al., 2006). In a posture assessment, body alignment is compared with the ideal standard, a plumb line, usually a string with a small weight attached to the bottom to help maintain straightness. The other end of the string is affixed to the ceiling to be used as an accurate reference for correct alignment. (Singla D. and Veqar Z. 2014) During a posture assessment, the patient stands next to the plumb line while the doctor or therapist compares the relative positions of the following areas:
Ears
Shoulder joint
Spine
Hip joint
Knee joint
Ankle joint
Feet
Any areas that don’t match the reference can indicate misalignments in one or several regions.
Making Corrections
Chiropractic care can help correct unhealthy posture by realigning the spine and strengthening the musculoskeletal system:
Spinal Adjustments
Chiropractors use their hands or instruments to apply controlled force to the spine to realign the vertebrae. This can help relieve pressure on muscles, ligaments, and nerves, which can improve posture.
Corrective Exercises
Chiropractors can create custom exercises to strengthen postural muscles and maintain proper alignment.
Massage Therapy
Chiropractors can use massage therapy to work on strained ligaments and soft tissue.
Guidance and Training
Chiropractors can teach patients how to move to encourage a neutral spine and provide strategies for maintaining healthy posture.
A posture corrector or brace can also help teach and engage the correct muscles to achieve proper alignment. However, it should not be relied on long-term because promoting and activating one’s stabilizing muscles is important rather than relying on a brace for prolonged periods.
Injury Medical Chiropractic and Functional Medicine Clinic
Achieving and maintaining proper posture requires consistent work and development. Retraining the body and maintaining its optimal health requires daily efforts through exercise, conscious position corrections, and ergonomics. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Upper Cross Syndrome
References
Bone Health & Osteoporosis Foundation. (2024). Proper body alignment. https://www.bonehealthandosteoporosis.org/patients/treatment/exercisesafe-movement/proper-body-alignment/
Mayo Clinic. (2023). Mayo Clinic Q and A: Proper posture and body alignment. https://newsnetwork.mayoclinic.org/discussion/mayo-clinic-q-and-a-proper-posture-and-body-alignment/
Singla, D., & Veqar, Z. (2014). Methods of postural assessment used for sports persons. Journal of clinical and diagnostic research: JCDR, 8(4), LE01–LE4. https://doi.org/10.7860/JCDR/2014/6836.4266
Coglianese, D. (2006). Muscles: Testing and Function With Posture and Pain, ed 5 (with Primal Anatomy CD-ROM). Physical Therapy, 86(2), 304-305. https://doi.org/https://doi.org/10.1093/ptj/86.2.304
Individuals experiencing persistent pain, weakness, numbness, and tingling in the back could be suffering from nerve root encroachment. Could surgery ease nerve compression and improve symptoms for persistent and severe cases?
Surgical Decompression
The pain, weakness, numbness, and tingling associated with nerve root encroachment are usually first treated with non-surgical therapies that include:
Anti-inflammatory medications
Physical therapy
This can be enough to address the irritation of the spinal nerve root. But when cases become severe, surgical decompression may be recommended and necessary. It can be done in a couple of different ways.
Causes and Symptoms
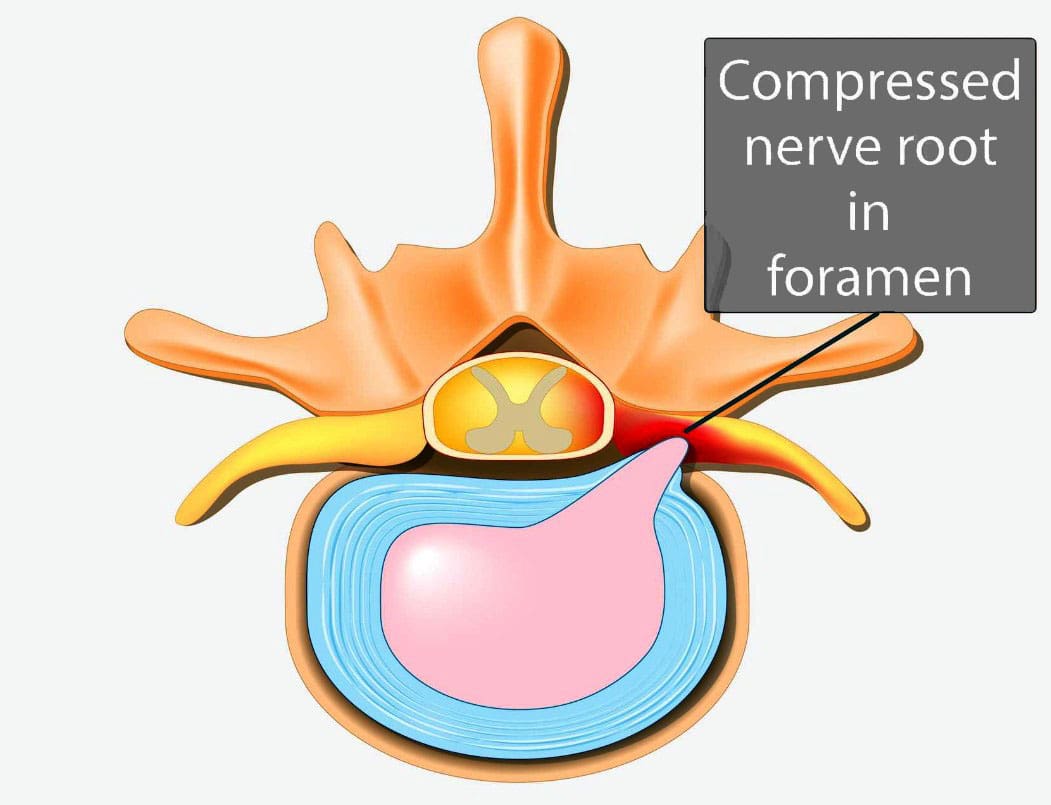
Vertebrae are bones in the spine. Small openings called foramina allow a spinal nerve root to pass through on each side of the vertebra. When nerve root encroachment is present, the spinal nerve root gets compressed, pinched, and trapped, which can cause peripheral symptoms such as numbness, tingling, pain, or weakness to develop. Nerve root encroachment is typically caused by normal aging degenerative wear and tear changes in the vertebrae. (Choi Y. K. 2019) These degenerative changes can include:
Facet joint hypertrophy
Ligament and bone hypertrophy
Disc disorders
Formation of bone spurs or osteophytes.
If these degenerative changes progress, they can encroach and compress a nerve root, leading to peripheral symptoms. (Choi Y. K. 2019)
When Surgery Is Recommended
When symptoms occur, initial treatment will involve:
Physical therapy
Chiropractic realignment
Massage therapies
Rest
Lifestyle adjustments
Nonsteroidal anti-inflammatories – NSAIDs
Corticosteroid injections into the spine
If conservative therapies don’t fully heal or improve symptoms or there are neurological problems like difficulty with balance or walking, then surgery may be recommended. Severe pain that limits normal function is an indication for surgery, and rapidly progressive weakness of the arms and/or legs or signs of cauda equina syndrome are indications for emergency surgery.
Surgery Options
Different types of spinal surgery may be performed. A neurosurgeon will decide the best procedure for each patient based on their case, age, medical conditions, and other factors. Specific spinal surgical decompression depends on what is causing the nerve compression. In most cases, it involves removing bone or tissue to relieve nerve pressure or provide support to stabilize the joint. The most common types of surgical decompression include: (Mayo Clinic Health System, 2022)
Maintain the stability and alignment of the spine.
Improve the stability and alignment of the spine.
Anterior Surgery
The anterior approach to surgery means that the spine is accessed through the anterior/front of the spine. In this surgery, one or more discs and bone spurs may be removed through an incision in the front of the neck. (American Association of Neurological Surgeons, 2024) For example, an anterior cervical discectomy may alleviate pressure on one or more nerve roots in the neck. With an anterior lumbar interbody fusion, a surgeon removes a degenerative disc in the lower spinal area by going through a patient’s lower abdomen. (American Association of Neurological Surgeons, 2024) After the disc is removed, a structural device, usually made of bone, fills the space where it once was. This device encourages bone healing and helps the vertebrae’s bodies fuse.
Posterior Surgery
Posterior surgery means the spine is accessed through the posterior/back of the spine. An example is removing a thickened ligament, bone spur, or disc material in the neck. To do this, a small incision in the back of the neck may be made to remove part of the back of the vertebrae called the lamina. This is called a posterior cervical laminectomy. (American Association of Neurological Surgeons, 2024) A posterior lumbar interbody fusion removes a degenerative disc by going through the back. (American Association of Neurological Surgeons, 2024) Like the anterior approach, a structural device often contains bone to fill the space where the disc once was to fuse the bones.
Potential Risks
As with any surgery, it’s important that the individual and their healthcare provider carefully discuss the benefits and risks. Spinal surgical decompression includes: (Proietti L. et al., 2013)
Bleeding
Blood clots
Surgical site infection
Urinary tract infection
Lung infection
Intestinal blockage
There are also specific risks to the area of the spine being operated on and how it is surgically approached. For example, a cervical anterior procedure may injure the esophagus, trachea, or carotid artery. Likewise, damage to the C5 nerve root/C5 palsy can occur from cervical spinal decompressive surgery. This complication causes weakness, numbness, and pain in the shoulders. (Thompson S. E. et al., 2017) The spinal cord may also be injured during surgery and result in paralysis, although this is rare. (American Association of Neurological Surgeons, 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
The Non-Surgical Solution
References
Choi Y. K. (2019). Lumbar foraminal neuropathy: an update on non-surgical management. The Korean journal of pain, 32(3), 147–159. https://doi.org/10.3344/kjp.2019.32.3.147
Mayo Clinic Health System. (2022). Decompress and stabilize: understanding types of back surgery. Speaking of Health. https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/understanding-types-of-back-surgery
American Association of Neurological Surgeons. (2024). Cervical spine. https://www.aans.org/patients/conditions-treatments/cervical-spine/
American Association of Neurological Surgeons. (2024). Lumbar spinal stenosis. https://www.aans.org/patients/conditions-treatments/lumbar-spinal-stenosis/
Proietti, L., Scaramuzzo, L., Schiro’, G. R., Sessa, S., & Logroscino, C. A. (2013). Complications in lumbar spine surgery: A retrospective analysis. Indian journal of orthopaedics, 47(4), 340–345. https://doi.org/10.4103/0019-5413.114909
Thompson, S. E., Smith, Z. A., Hsu, W. K., Nassr, A., Mroz, T. E., Fish, D. E., Wang, J. C., Fehlings, M. G., Tannoury, C. A., Tannoury, T., Tortolani, P. J., Traynelis, V. C., Gokaslan, Z., Hilibrand, A. S., Isaacs, R. E., Mummaneni, P. V., Chou, D., Qureshi, S. A., Cho, S. K., Baird, E. O., … Riew, K. D. (2017). C5 Palsy After Cervical Spine Surgery: A Multicenter Retrospective Review of 59 Cases. Global spine journal, 7(1 Suppl), 64S–70S. https://doi.org/10.1177/2192568216688189
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine