T-bone accidents/collisions, also known as side-impact or broadside collisions where the front end of one car slams into the side of another, can result in severe injuries and tend to have a more devastating effect on the body. Side impact collisions account for 24% of driver or passenger deaths; even at 30 mph, side-impacts regularly cause injuries to the occupants of the struck car. Modern vehicles have many safety features, including safety belt features, airbags, and collision avoidance systems that protect drivers and passengers from front and rear collisions; however, when it comes to side-impact, occupants tend to remain unprotected.
T-Bone Side Collision Causes
T-bone accidents usually happen at intersections. Usual Causes of T-bone accidents involve someone failing to yield the right of way. The most common causes include:
A driver makes a risky left turn at an intersection, believing the other car/s will stop.
A driver decides to run a red light crashing into a vehicle making a left turn.
A driver runs through a stop sign, slams into a vehicle, or gets slammed.
Back injuries can damage the spinal cord causing herniated discs, sciatica, and chronic pain that can radiate to the rest of the body.
Treatment and Recovery
Individuals have different recovery times and depend on the severity of the injury and on any pre-existing conditions. Brain injuries and spinal issues can take months to recover fully. Fractures placed in a hard or soft cast to heal for weeks or months can lead to muscle atrophy. Chiropractic therapeutic massage and decompression strengthens muscle weakness, resets and realigns the spinal column, improves range of motion/movement, strengthens grip, and relieves pain.
Neurosurgeon Explains DRX9000
References
Gierczycka, Donata, and Duane Cronin. “Importance of impact boundary conditions and pre-crash arm position for the prediction of thoracic response to pendulum, side sled, and near side vehicle impacts.” Computer methods in biomechanics and biomedical engineering vol. 24,14 (2021): 1531-1544. doi:10.1080/10255842.2021.1900132
Hu, JunMei, et al. “Chronic widespread pain after motor vehicle collision typically occurs through immediate development and nonrecovery: results of an emergency department-based cohort study.” Pain vol. 157,2 (2016): 438-444. doi:10.1097/j.pain.0000000000000388
Lidbe, Abhay, et al. “Do NHTSA vehicle safety ratings affect side impact crash outcomes?.” Journal of safety research vol. 73 (2020): 1-7. doi:10.1016/j.jsr.2020.02.001
Mikhail, J N. “Side impact motor vehicular crashes: patterns of injury.” International journal of trauma nursing vol. 1,3 (1995): 64-9. doi:10.1016/s1075-4210(05)80041-0
Shaw, Greg et al. “Side impact PMHS thoracic response with a large-volume airbag.” Traffic injury prevention vol. 15,1 (2014): 40-7. doi:10.1080/15389588.2013.792109
Stretching Fundamentals: Stretching benefits the body by keeping the muscles flexible, strong, healthy, and able to maintain optimal physical performance. As with any other discipline stretching correctly requires using the proper form, correct technique, and practicing regularly. The angles need to be accurate; the body has to move at the right speed and maintain correct posture. The focus should be moving the joint as little as possible as the muscle/s stretch and elongate.
Stretching Fundamentals
Stretching should become a daily activity that turns into a healthy habit. The muscles need frequent maintenance from daily/nightly bending, twisting, reaching, carrying, and lifting work. This is especially true for individuals dealing with constant soreness, aches, pains, and problems with tight, tense, and stressed-out muscles. When the body is stressed, heart rate increases, and individuals tend to tighten up. Stretching benefits include:
Stress relief.
Increased muscle blood flow.
Increased body flexibility.
Helps joints move through their full range of motion.
Improves performance in physical activities.
Decreases soreness, aches, and pains.
Injury prevention.
Improves posture.
Improves sleep.
Preps the body for exercise and activities.
Improves mental health.
Human nature is to take the path of least resistance, which makes the body feel flexible and comfortable. This is a common reason individuals consider stretching unnecessary or too painful to engage in. However,stretching fundamentals need to be maintained as stretching carelessly or poorly can negatively affect other muscles and joints and worsen injuries/conditions.
Guidelines
To stretch safely, it is recommended to do a proper warm-up, stretch slowly, working the right muscles and joints. The guidelines make stretching safer, more effective, and increase body awareness.
Warm-Up
Warming the muscles increases blood flow.
Warming up muscles before physical activity/workout is crucial for preventing injuries and maximizing effectiveness.
Dynamic stretching involves moving into and out of positions through a full range of motion rather than holding a stretch for a prolonged period.
Dynamic stretches are recommended to be held for 2-3 seconds for 4-6 repetitions.
Take It Slow
Stretching out too fast can make the body think that the muscle is about to get torn or injured.
To protect the muscle, it contracts, preventing it from reaching the full stretch.
This is why the correct technique needs to be observed.
A couple of degrees in the wrong direction can mean the difference between a healthy stretch and pulling a joint capsule causing injury.
Body Composition
Muscle Recovery
When engaged in physical activity, exercise, or working, microscopic tears are happening to muscle cells. Because of the body’s stress and fatigue, hormone and enzyme levels fluctuate, and inflammation increases. This helps in fat loss, increases metabolism, increases strength and muscle growth. However, these benefits only happen with proper recovery. Different types of recovery include:
Immediate Recovery
These are the quick moments’ in-between physical movements.
For example, the time between each stride when jogging.
Short-Term Recovery
This is the time between activities or sets of exercises.
For example, the rest periods between doing a heavy job or sprint intervals.
Training Recovery
This is the time between when one workout or job ends, and the next begins.
There is no one size fits all, as everyone’s body is different; it is recommended to consult with a trainer or fitness expert and experiment with what feels right.
For some individuals, 24 hours is enough.
For others, it can take 48 or 72 hours to feel fully recovered.
Other factors that affect recovery are:
Age
Fitness level
Work/exercise intensity
Diet
Sleep
References
Behm, David G, and Anis Chaouachi. “A review of the acute effects of static and dynamic stretching on performance.” European Journal of applied physiology vol. 111,11 (2011): 2633-51. doi:10.1007/s00421-011-1879-2
Freitas, S R et al. “Stretching Effects: High-intensity & Moderate-duration vs. Low-intensity & Long-duration.” International journal of sports medicine vol. 37,3 (2016): 239-44. doi:10.1055/s-0035-1548946
Hotta, Kazuki et al. “Daily muscle stretching enhances blood flow, endothelial function, capillarity, vascular volume and connectivity in aged skeletal muscle.” The Journal of physiology vol. 596,10 (2018): 1903-1917. doi:10.1113/JP275459
Kataura, Satoshi et al. “Acute Effects of the Different Intensity of Static Stretching on Flexibility and Isometric Muscle Force.” Journal of strength and conditioning research vol. 31,12 (2017): 3403-3410. doi:10.1519/JSC.0000000000001752
Sciatic nerve injury happens from trauma to the nerve and can cause numbness, tingling, loss of muscle power, and pain. The traumatic experience can be a muscle spasm that pulls and/or pinches the sciatic nerve, force/pressure impact injury, over-stretching injury, or a laceration/cutting injury. A slipped disk, or herniated disk, is the most common cause of irritation on the sciatic nerve. A slipped disk occurs when one becomes slightly dislodged, pushing out from the spine. This places pressure/compression on the sciatic nerve.
Trauma to the lower back, buttocks, or leg from an automobile accident, sports injury, work injury.
Medical treatment causes:
Direct surgical trauma.
Total hip replacement surgery can cause nerve compression and stretch during the procedure, causing damage to the sciatic nerve resulting in dysfunction.
Injection injuries via intramuscular injection in the gluteal region. This is a situation where there is a loss of movement and or lack of sensation at the affected lower extremity with or without pain.
Injection palsy can begin suddenly or hours following damage to the sciatic nerve.
A misplaced intramuscular injection at the gluteal region is the most common cause of injury. It is attributed to frequent injections or poor techniques resulting from inadequately trained or unqualified staff.
Complaints of radiating pain in the leg, which follows a sensory nerve pattern.
Pain radiates below the knee, into the foot.
Complaints of low back pain, which is often less severe than leg pain.
Report of electrical, burning, numbing sensations.
Diagnosis
A detailed subjective and objective physical examination is necessary to figure out the severity of the sciatic nerve injury. Diagnostic studies include:
Chiropractic and physical therapy exercises and stretches improve nerve regeneration after nerve damage.
Electrical Muscle Stimulation
TENS and Electroacupuncture have been shown to help enhance nerve regrowth.
Bio-laser stimulation can help with nerve nutrition and regeneration.
Joint or Soft Tissue mobilization
Helps to retain muscle, nerve, and soft tissue flexibility and prevent deformity.
Balance Training
Coordination, strength, and flexibility exercises help to restore balance.
Splinting
In the early stages after a sciatic nerve injury, bracing may be needed to prevent deformity and new injury or re-injury risks.
Ankle Foot Orthosis – AFO can help prevent foot drop, muscle damage, and falls risk.
Body Composition
Optimize Diet for Fat Loss
Individuals that want to lose fat need to create a calorie deficit. Individuals need to consistently eat less than they need for Total Daily Energy Expenditure – TDEE. The safest way to handle a caloric reduction is to reduce calorie intake in small doses like 200-300 calories, for example. After a week or two, perform a body composition analysis. If Fat Mass numbers begin to drop or not, adjust calorie needs accordingly. Restricting calories is the most common way, a deficit can also be created by increasing calorie needs through exercise.
References
Kline, D G et al. “Management and results of sciatic nerve injuries: a 24-year experience.” Journal of neurosurgery vol. 89,1 (1998): 13-23. doi:10.3171/jns.1998.89.1.0013
Schmalzried, TP et al. “Update on nerve palsy associated with total hip replacement.” Clinical Orthopedics and related research,344 (1997): 188-206.
Shim, Ho Yong et al. “Sciatic nerve injury caused by a stretching exercise in a trained dancer.” Annals of rehabilitation medicine vol. 37,6 (2013): 886-90. doi:10.5535/arm.2013.37.6.886
Suszyński, Krzysztof et al. “Physiotherapeutic techniques used in the management of patients with peripheral nerve injuries.” Neural regeneration research vol. 10,11 (2015): 1770-2. doi:10.4103/1673-5374.170299
There are many different treatments for cerebral palsy available today, however each case of cerebral palsy is as unique as the individual it affects. Because cerebral palsy can ultimately affect the normal functioning of the brain, treatment approaches which enhance the connection between the brain and the body are essential. Various treatments will work for different patients. A treatment known as physical therapy, or physiotherapy, is categorized as a non-medicinal treatment of cerebral palsy with the usage of massage, exercise, heat, and other external means of treatment.
Physiotherapy can be used to help cerebral palsy patients improve motion and motor abilities. Since cerebral palsy is a physical and movement disorder that disrupts the brain’s ability to correctly control muscle movement, physiotherapy can work wonders in helping cerebral palsy patients achieve mobility. Cerebral palsy physical therapy techniques are dependent on the degree of physical limitations of the person, and what’s going to be most beneficial to the cerebral palsy patient. Chiropractic care, can also include physical therapy techniques. Because the brain is believed to be lacking proper stimulation for functioning through cerebral palsy, chiropractic care can offer proprioception of touch for the assistance of mobility for the increased sensory stimulation of the brain through spinal adjustments and manipulations.
Physiotherapy for Cerebral Palsy
Cerebral palsy is the most common physical disability in children and it also represents the most frequent diagnosis in children who receive physical therapy. The harshness of limitations in gross motor function among children with cerebral palsy varies greatly, as some can walk without helping devices while some must use battery-powered wheelchairs. Physical therapists help children discover better ways to balance and move, as well as learn to walk, use their wheelchair, stand up with help, or go up and down stairs safely. The physical therapists engaged in physiotherapy reduce further growth of musculoskeletal problems by preventing muscle weakening, deterioration, and contracture during the suitable physiotherapy methods.
Physiotherapy usually consists of a couple kinds of treatment and helps a cerebral palsy patient to improve their gross motor abilities. Motor abilities that utilize the big muscles in the body, such as those in the arms and legs, are called gross motor abilities. This kind of physical therapy can help improve a cerebral palsy patient’s balance and motion.
Physical therapy for cerebral palsy patients consists of activities and education to enhance flexibility, strength, mobility, and function. A physical therapist also designs, modifies, and orders elastic gear to be used in the rehabilitation. Physical therapy can take place in clinics, hospitals, schools, and ought to continue in the home through a workout program. Physical treatment for cerebral palsy patients won’t be effective without an ongoing daily home program.
Physical Therapy Methods for Cerebral Palsy
A physical therapy program must include lots of exercises that include stretching, strengthening, and positioning. To elongate the muscles, the arms and legs must be transferred in ways that produce a slow, steady pull on the muscles to keep them loose. Because of the greater muscle tone of the cerebral palsy patient, they tend to have tight muscles. Therefore, it’s extremely important to perform daily stretches to maintain the arms and legs limber, allowing the child to continue to move and function. Strengthening exercises work specific muscle groups to enable them to encourage your system better and increase function. Positioning requires your system to be set in a particular position to achieve long stretches. Some places help minimize unwanted tone. Positioning can be achieved in many different ways. Bracing, abduction pillows, knee immobilizers, wheelchair inserts, sitting recommendations, and handling techniques are a part of placement techniques utilized in physical therapy for cerebral palsy patients.
New methods of physical therapy for cerebral palsy patients have taken into the water. Aquatic-based rehabilitation employs the physical properties of water to either resist or help in the operation of exercises. Cerebral palsy patients undergo muscle shortening in the majority of their involved extremities and it becomes a difficult job to lengthen the affected musculature with regular stretching while needing to manage the effects that gravity has on the spastic leg or arm. In earlier times there was clinical bias against strengthening activities for this population. But, recent study findings are revealing that kids with cerebral palsy may gain from strengthening applications and that strength is directly associated with motor function. Some of the recorded advantages are optimization of neuromuscular responses, improved motor unit contraction synchrony and facilitation of maximal muscle contraction combined with a wide available selection of motion.
Physical treatment for cerebral palsy patients does not heal spasticity but can improve impairments and limitations. Physical treatment for cerebral palsy patients is an important step towards an independent lifestyle. If these changes happen only in the therapy gym, the disability remains unchanged. Therapy must improve skills to carry out meaningful tasks in everyday life. Changing the level of handicap is the ultimate aim of physical therapy for cerebral palsy.
Occupational therapy is another element of physiotherapy used for cerebral palsy patients, and it’s used for aiding in the development of fine motor skills. Fine motor skills focus on the use of smaller muscles, such as those from the face, fingers, toes, palms, and feet. Fine motor skills have been used during daily living skills such as eating, dressing, writing, etc., and are fine tuned by occupational physiotherapy.
Physiotherapy also entails picking the right sort of adaptive equipment that could enhance a cerebral palsy patient’s motor abilities. Wheelchairs, walkers, special eating utensils and other adaptive equipment supply a patient with the liberty to accomplish some tasks on their own.
Additional types of physiotherapy like language and speech therapy might also be incorporated into a cerebral palsy patient’s program. Physiotherapy in the form of language and speech therapy that enables a cerebral palsy patient to communicate more easily with other people by developing the facial and jaw muscles, enhancing speech or sign language messages, and introducing communication resources such as computers and other visual aids.
Dr. Alex Jimenez’s Insight
Cerebral palsy is a lifelong group of movement disorders with no cure. However, several treatment options can help improve the quality of life of a patient with cerebral palsy. Chiropractic care and physical therapy, or physiotherapy, are some of the most common treatment approaches utilized to help restore strength, flexibility and mobility for individuals and children with cerebral palsy, without the need for drugs/medications and surgery. Chiropractic care can help improve many aspects associated with cerebral palsy due to the stimulation of the brain through touch, using spinal adjustment and manual manipulations to enhance sensory receptors in patients with this movement disorder. A physical therapist, as well as a chiropractor, may generally recommend a series of stretches and exercises which can improve range of motion in patients with cerebral palsy. Chiropractic care and physical therapy have the ability to develop self-sufficiency in cerebral palsy patients where it was previously absent.
Chiropractic Care for Cerebral Palsy
Several other physical therapy options can also help provide some form of relief from painful symptoms for cerebral palsy patients. Chiropractic care has become a popular, alternative treatment approach which focuses on maintaining as well as improving the overall health of the body through the use of spinal adjustments and manual manipulations. Because different areas of the body can be affected in individuals and children with cerebral palsy, chiropractic care can be beneficial towards helping those limbs regains some strength, flexibility and mobility. A chiropractor who specializes in patients with cerebral palsy can also offer several rehabilitation and physical therapy stretches and exercises to achieve the desired semblance of activity from the cerebral palsy patient. Because chiropractic care utilizes touch through spinal adjustments and manual manipulations to enhance the structure and function of the brain and the body, the sensory stimulation provided by a chiropractor can promote the migration of the brain in order to help change the receptors of the brain.
Furthermore, chiropractic care can help treat other, less noticeable aspects of the motor disorder. When used as a part of a rehabilitation and physical therapy program, chiropractic care can help improve some of the more problematic symptoms associated with cerebral palsy, including muscle spasms, seizures, and leg and arm issues through touch mobility protocols. The connection between the body and the brain has long been the center focus of chiropractic care, which is why spinal adjustments and manual manipulations are commonly utilized to enhance the stimulation of the brain, the spine, the nerves and the remaining structures of the body, especially in the case of patients with cerebral palsy, where the proper stimulation of the brain is necessary in order to restore function and improve quality of life. By carefully working to restore the natural alignment of the spine, a doctor of chiropractic, or chiropractor, can improve symptoms of back pain which may often be caused by the stress being placed on the spine�in patients with cerebral palsy. The purpose of chiropractic care and physical therapy is to improve physical movement and coordination, speech, vision and intellectual development�for patients with cerebral palsy.
Physiotherapy is an integral part in the vast majority of many cerebral palsy patients’ lives. Physiotherapy has the ability to develop self-sufficiency in cerebral palsy patients in which it was previously absent. A kid with cerebral palsy can start physiotherapy in just about any age. Speak with your child’s doctor about setting up physiotherapy program today. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
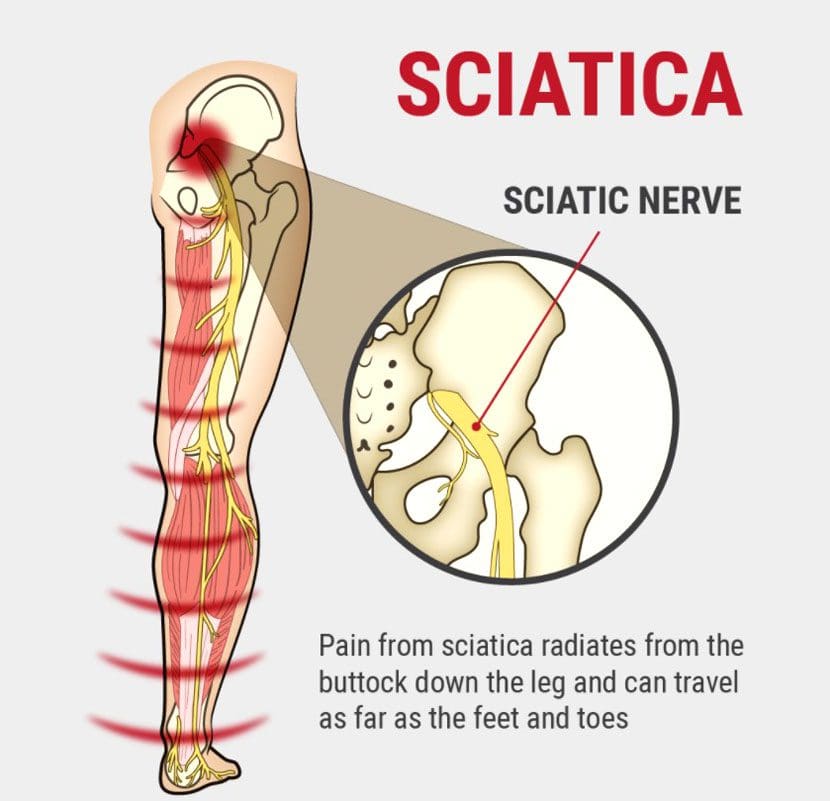
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Children with cerebral palsy have various needs. Some children have problems with motor skills and spasticity, but normally pick up things pretty fast. Others have a full range of issues from motor skills to esophageal and respiratory problems. Since so many kids with cerebral palsy have an array of different medical needs, there isn’t one particular type of treatment which may help each and every child. Luckily, there are a number of different therapeutic remedies to select from, which range from holistic care, water therapy, and much more.
Acupuncture
Whilst generally not adopted in Western Medicine, acupuncture has been used for centuries by Asian countries and is viewed as a medicinal art. Some families with children who have cerebral palsy take their kids to an acupuncturist to try and relieve the frequent pain related to the disorder. Other kids find relief in acupuncture for painful birth injuries such as spina bifida, Erb’s palsy, and brain damage. Acupuncture uses needles to ease pain, often instead of medication.
Aquatherapy
Aquatherapy is among the most popular and beneficials form of treatment for children with cerebral palsy, as they suffer from limb maladiess, but this might also be advantageous for children who suffer with Erb’s palsy and are trying to regain movement in their arm.
Under the supervision of a trained and experienced professional therapist, kids may gain from the strength exercise and training afforded by the anti-gravity character of a pool. In this soothing environment, a child can have a respite from some of the pain which comes with the disability (occasionally cerebral palsy causes stress on the musculoskeletal frame by simply gravity and body weight), and they can still work through the natural curative and restorative nature of water.
Behavioral Therapy (Psychotherapy)
Some birth injuries involve an intellectual disability that impacts how kids interact in social scenarios. Other children might have had physical constraints that included them being house-bound for a long time, causing them to have a deficiency in social skills or cues. Behavioral therapy, also known as psychotherapy, allows patients to work through problems they may have within their social and mental health with a behavioral health professional.
Chiropractic Care and Massage Therapy
Children with cerebral palsy may benefit from chiropractic care and massage therapy for a few different reasons. Because some children with cerebral palsy may have experienced lots of strain or stress on their musculoskeletal system as a result of the disorder, requiring chiropractic care may ultimately be fundamental towards their proper spinal alignment as well as for their overall health and wellness.
Chiropractic care is a well-known alternative treatment option which utilizes spinal adjustments and manual manipulations to treat a variety of injuries and/or conditions associated with the musculoskeletal and nervous system, including back pain.
Another reason that a patient with cerebral palsy might need chiropractic care or massage treatment is for the basic goal of extending and stretching muscles. When muscles relax as they perform through such therapies, they are more inclined to become stronger and healthier which is needed if they are going to correctly learn how to walk. This kind of treatment isn’t generally suggested for kids suffering from spina bifida because the raw exposed nerves could be inadvertently mishandled, causing more problems.
Furthermore, chiropractic care can be used to help treat other, less noticeable aspects of cerebral palsy. The theory of chiropractic care is that by healing the central area around the spine, the extremities and other parts of the body affected by the disorder can become more normalized, allowing for improved function and quality of life. Chiropractic care can also help improve strength, mobility and flexibility in children with cerebral palsy and its associated symptoms.
Conductive Education
Some children with neurological or mobility impairment found in almost any brain-related birth trauma need help performing activities that regular people learn through daily exercise, learning, and experience. Since these children don’t often have the same sorts of experiences that non-disabled people have, conductive education is a form of special education that functions as a kind of study group for life.
Conductive education provides opportunities of every day learning experiences so that kids can have the exact same general education that non-disabled individuals do.
Hippotherapy
Using equine motion and connections with horses, children with all kinds of birth injuries could learn basic occupational and speech therapy. Hippotherapy is not therapeutic horseback riding, but rather a trained practitioner introduces the child to the horse and uses the horse to access the child in ways which were previously thought of as unconventional.
Hyperbaric Oxygen Therapy
Normally short-term treatment and frequently only experienced once or twice, Hyperbaric Oxygen Therapy is a method of fast-healing for some kids that have suffered oxygen deprivation (anoxic, hypoxic, HIE, birth asphyxia, and perinatal asphyxia). If an infant is delivered and does not breathe for the upcoming instant minutes, hyperbaric oxygen treatment is a great way to introduce a lot of oxygen into the blood stream preventing or lessening the seriousness of birth injuries such as cerebral palsy.
Occupational Therapy
Occupational therapy’s main objective is to work on creating balance, strength, and gait. An occupational therapist might consult with an orthopedic surgeon to operate on strengthening and firming muscles, in which following the occupational therapist can delegate casts and orthopedic devices which also help strengthen and form muscles. These methods are to help patients learn how to walk, and also to create control and strength to stop spasticity.
The occupational therapist also trains patients to function on decision-making, abstract reasoning, problem-solving, perception, memory, sequencing, and much more.
Play Therapy
Utilizing play with a variety of different toys in various public places, kids with all kinds of birth injuries can learn to appreciate themselves. Often children with birth injuries can feel that they’re different or that they have health issues and end up stressing about their difficulties more than having fun.
While they’re having fun in play therapy, they can learn the way to interact with other kids, learn about themselves, and to construct self-confidence.
Physiotherapy and Physical Therapy
Physiotherapy and physical therapy both operate on the rehabilitation of muscle groups. This is extremely important for children with shoulder dystocia, Erb’s palsy, Klumpke’s palsy, or Brachial Plexus palsy, and, in fact, kids suffering from these birth injuries won’t regain use of their hand or arm without physical and physiotherapy. Through this type of treatment, therapists strive to receive the perfect movement from their patients through an assortment of different challenges and exercises.
This can be like occupational therapy, though the focus is mainly on what the muscle groups are doing, and not on so many different targets like occupational therapy. A physical therapist is often like a personal trainer in a gym, training, cheering, and challenging.
Respiratory, Digestive, and Dietician Therapy
Some kids with cerebral palsy encounter respiration and esophageal problems. Consequently they can experience issues with eating, breathing, and drinking, which divides into digestive and dietician treatment, addressing what foods and drinks should be consumed. Respiratory treatment may primarily tackle breathing exercises to strengthen and optimize lung development, but may also address these other concerns.
Speech and Language Therapy
Speech and language therapy can be very important for kids with cerebral palsy and other forms of brain-related birth harm. Approximately, 1 out of every 4 patients with cerebral palsy don’t have the capability to speak. Speech and language therapy helps them to work on exercises which progress the learning of speech and get kids closer to communicating effectively.
Some speech and language therapists utilize programs that help patients understand the operation of language inside individuals, and these programs also provide communication boards using pre-formed responses so that children can get in the habit of responding with particular answers until they consider trying to verbalize these answers.
Vocational Counseling
This has many different sorts of therapists, a few children could be confused or jeopardized by visiting a lot of individuals, or, worse, by having so many people invade their home. One way of approaching treatment is by using a vocational counselor, one individual who can master several distinct types of treatment.
As vocational counselors might not have exactly the exact same depth in all of these subjects as one therapist would have regarding one subject, this might be a great first step for treatment with your little one. By getting your child to adjust to only one person interacting within their lifetime, they’re more inclined to concentrate on the subjects at hand.
Afterwards, if more obstacles and more depth is required, your kid may have more assurance in different areas (and with a few social abilities from connecting with this particular counselor) and may be able to handle other therapists more efficiently.
Yoga Therapy
Normally prescribed under the direction of an occupational or physical therapist, yoga therapy is a fantastic alternative for kids whose muscles need to be loosened or lengthened. Children with cerebral palsy suffer from particularly tight muscles, so yoga therapy helps them to work on extending and on making the muscles more limb. This type of treatment might be incorporated to other sorts of therapy, and it might also be delegated as “homework” to kids with cerebral palsy for optimal flexibility and, ultimately, optimal freedom.
Dr. Alex Jimenez’s Insight
Cerebral palsy is a lifelong set of movement disorders with no cure. However, various types of treatment options can help provide some forms of relief for individuals and children with cerebral palsy as well as help restore some function and quality of life. Because cerebral palsy can affect patients differently, people with the disorder can benefit from many different therapies, including chiropractic care and physical therapy. Chiropractic care is a popular, alternative treatment option which focuses on the diagnosis and treatment of several kinds of injuries and/or conditions, including cerebral palsy. Through the use of spinal adjustments and manual manipulations, a chiropractor can help improve strength, mobility and flexibility in people with cerebral palsy.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Herniated discs are a debilitating condition characterized by pain, numbness and weakness in one or more limbs. While some people may experience no pain at all, those that do may often wish for fast pain relief to avoid long periods of sick leave from their jobs. Many healthcare professionals recommend surgery for patients with persistent and/or worsening herniated disc symptoms but other non-operative treatment options can help treat disc herniations. The purpose of the following article is to demonstrate how a�structured physiotherapy treatment model can provide rapid relief to patients who qualify for lumbar disc surgery.
A Structured Physiotherapy Treatment Model Can Provide Rapid Relief to Patients Who Qualify for Lumbar Disc Surgery: A Prospective Cohort Study
Abstract
Objective: To evaluate a structured physiotherapy treatment model in patients who qualify for lumbar disc surgery.
Design: A prospective cohort study.
Patients: Forty-one patients with lumbar disc herniation, diagnosed by clinical assessments and magnetic resonance imaging.
Methods: Patients followed a structured physiotherapy treatment model, including Mechanical Diagnosis and Therapy (MDT), together with graded trunk stabilization training. Study outcome measures were the Oswestry Disability Index, a visual analogue scale for leg and back pain, the Tampa Scale for Kinesiophobia, the European Quality of Life in 5 Dimensions Questionnaires, the Zung Self-Rating Depression Scale, the Self-Efficacy Scale, work status, and patient satisfaction with treatment. Questionnaires were distributed before treatment and at 3-, 12- and 24-month follow-ups.
Results: The patients had already improved significantly (p<0.001) 3 months after the structured physiotherapy treatment model in all assessments: disability, leg and back pain, kinesiophobia, health-related quality of life, depression and self-efficacy. The improvement could still be seen at the 2-year follow-up.
Conclusion: This study recommends adopting the structured physiotherapy treatment model before considering surgery for patients with symptoms such as pain and disability due to lumbar disc herniation.
Symptoms of lumbar disc herniation are relatively common in the general population, although the prevalence rates vary widely between different studies (1). Symptom severity also varies and, in many patients, pain and loss of function may lead to disability and long periods of sick leave (2). Spontaneous resolution of symptoms after a lumbar disc herniation is regarded as common, which makes it difficult to evaluate the effects of treatment. Furthermore, in studies evaluating spontaneous healing, different physiotherapy treatments are often included, together with pain medication (3�5), which makes it difficult to determine the extent of natural healing. On the other hand, in patients with sciatica, but without confirmed disc herniation on magnetic resonance imaging (MRI), approximately one-third of subjects recover 2 weeks after the onset of sciatica and approximately three-quarters recover after 3 months (6).
In contrast to evaluating spontaneous healing, surgery for lumbar disc herniation has been investigated in numerous studies. Surgery has been compared with a variety of treatments, such as education, chiropractic, unspecified physiotherapy, acupuncture, injections and medication (7�10). The non-surgical treatments have, however, been described only in vague terms, and variations in treatments have been used. Previous studies have reported favourable short-term (after 1 year) outcomes for surgery, but no major differences between surgical and other treatments have been demonstrated in the long term (over 2 years) (7, 10, 11). The conclusions that are drawn from the comparison between surgery and non-systematic non-surgical treatments may thus be misleading. This has been confirmed in a systematic review, which concluded that there is conflicting evidence as to whether surgery is more beneficial than nonsurgical care for both short- and long-term follow-up (12).
Kinesiophobia has been evaluated in patients after lumbar disc surgery, and almost 50% of patients were classified as having kinesiophobia (13). To our knowledge kinesiophobia has not been evaluated in patients with lumbar disc herniation treated with a structured physiotherapy treatment.
There are many different non-surgical treatment methods for patients with low-back pain and sciatica. One common management method is Mechanical Diagnosis and Therapy (MDT), also known as the McKenzie method, which aims to eliminate or minimize pain (14). A systematic review from 2004 of the efficacy of MDT showed that patients with low-back pain treated�with MDT reported a greater, more rapid reduction in pain and disability compared with non-steroidal anti-inflammatory drugs (NSAIDs), educational booklets, back massage and back care advice, strength training, spinal mobilization and general exercises (15). In a randomized controlled trial with a 1-year follow-up from 2008, Paatelma and co-workers (16) found that the McKenzie method was only marginally more effective compared with only giving advice to patients with low-back pain. For patients with low-back pain, sciatica and a verified lumbar disc herniation, it has, however, been shown that a selected group of patients who responded to MDT after 5 days of treatment also reported that they were satisfied after 55 weeks (17). The patients started treatment just 12 days after the onset of symptoms and the effects of spontaneous healing cannot therefore be excluded. Taken together, the treatment effects of MDT for patients with a verified lumbar disc herniation appear to require further evaluation.
Trunk stabilization exercises, which aim to restore deep trunk muscle control, have been used for the prevention and rehabilitation of low-back pain (18). A randomized controlled trial revealed a reduction in the recurrence of low-back pain episodes after specific trunk stabilization exercises compared with a control group receiving advice and the use of medication (19). Dynamic lumbar stabilization exercises have been found to relieve pain and improve function in patients who have undergone microdiscectomy (20). The effects of trunk stabilization exercises combined with MDT have, however, not been studied in patients with non-operated lumbar disc herniation. MDT is seldom recommended for patients with MRI verified lumbar disc herniation with a broken outer annulus. At our hospital, however, we have several years of good clinical experience of a combination of MDT and trunk stabilization exercises for this category of patients. To our knowledge, no previous study has investigated whether patients with a lumbar disc herniation verified by MRI, symptoms for at least 6 weeks (minimizing effects of spontaneous healing) and who qualified for disc surgery could improve with a structured physiotherapy treatment model including MDT and gradually progressive trunk stabilization exercises. The aim of this study was therefore to�evaluate a structured physiotherapy treatment model in patients who qualified for lumbar disc surgery.
Material and Methods
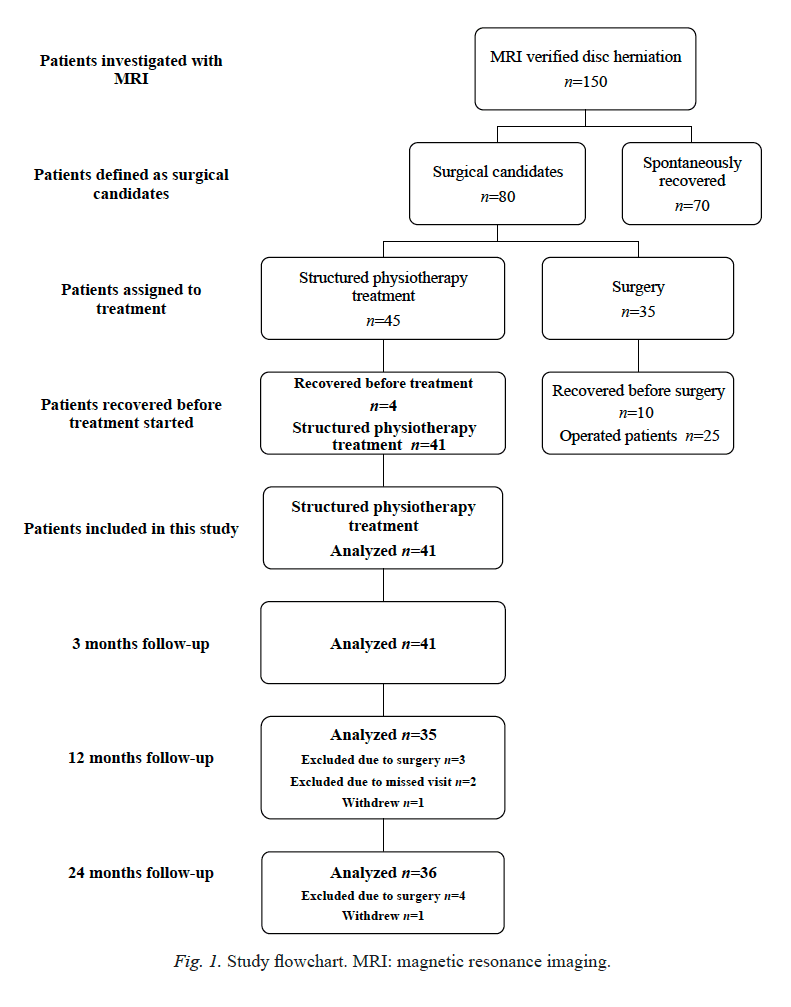
During the study inclusion period, 150 patients, who were referred to the orthopaedic clinic at Sahlgrenska University Hospital, Gothenburg, from November 2003 to January 2008, were identified as potential participants since disc herniation was confirmed with MRI. Inclusion criteria were: 18�65 years of age; MRI confirming disc herniation explaining the clinical findings; symptoms for at least 6 weeks (minimizing the effects of spontaneous healing) and pain distribution with concomitant neurological disturbances correlated to the affected nerve root. Exclusion criteria were: cauda equina syndrome, previous spinal surgery, other spinal diseases, such as spinal stenosis and spondylolisthesis, and inadequate command of Swedish. However, 70 patients were excluded because of spontaneous resolution of pain and symptoms. The remaining 80 patients met the inclusion criteria and qualified for surgery. Orthopaedic surgeons determined whether the patients qualified for lumbar disc surgery after MRI and physical examination according to the recommendations of the American Academy of Orthopaedic Surgeons for patients with lumbar disc herniation (21).
Initially, the study was planned as a randomized controlled trial (RCT) between a structured physiotherapy treatment model and surgery, but the number of patients was not sufficient to obtain acceptable power. Eighteen of the 80 patients were initially randomized to physiotherapy, 17 patients were randomized to surgery and 45 patients did not agree to undergo randomization. Twenty-seven of the 45 patients who did not agree to randomization agreed to take part in the structured physiotherapy treatment and 18 patients agreed to undergo surgery. A decision was therefore made solely to present a cohort of 45 patients treated according to the structured physiotherapytreatment protocol (Fig. 1). Patients were given verbal and written information and informed consent was obtained. The study was approved by the Regional Ethical Review Board.
Before structured physiotherapy treatment began, 4 patients recovered to the extent that they could no longer be accepted as surgical candidates and they were therefore excluded from the study. The remaining 41 patients treated according to the structured physiotherapy model are presented in this paper.
A Structured Physiotherapy Treatment Model
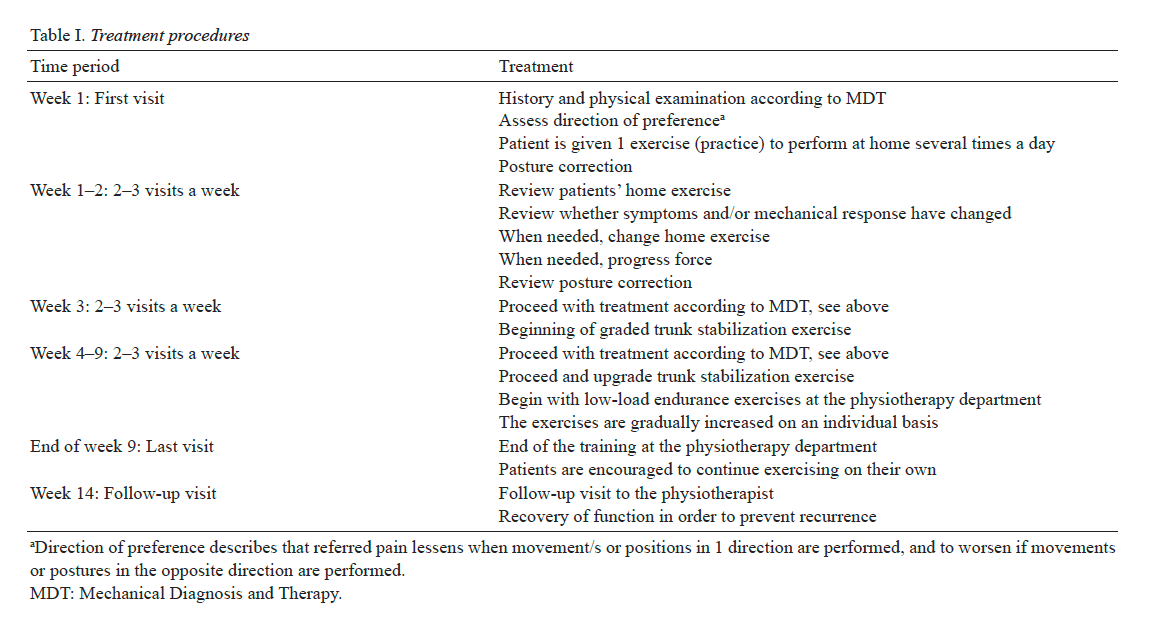
Six physiotherapists with credentialed examinations in MDT, which is an examination within the MDT concept after completing 4 courses of 4 days each for evaluating and treating patients with spinal problems. Following completion of these courses, an extensive literature study and practice in evaluating and treating patients is required before the examination can be completed. The physiotherapists involved in the study had 5�20 years of clinical experience of treating patients with back problems and herniated lumbar disc. The inter-examiner reliability of the MDT assessment has been shown to be good if the examiner is trained in the MDT method (22). The physiotherapists examined and treated the patients during a 9-week period (Table I). For the first 2 weeks of treatment, an MDT protocol was followed, based on clinical examinations of individual mechanical and symptomatic responses to positions and movements, with the aim of minimizing pain and with the emphasis on self-management (14). During the third week of treatment, graded trunk stabilization exercises were added to the MDT protocol. The purpose of graded trunk stabilization exercises was to improve muscle control (23). The low-load muscular endurance exercises were gradually increased in intensity on an individual�basis with respect to the patients� reported leg pain and the observed movement control and quality. During treatment, the patients were encouraged to continue exercising on their own at a gym, or to perform some other type of physical training of their own choice after the structured physiotherapy treatment was concluded. Four weeks after the completion of the 9-week physiotherapy treatment period, the patients attended a follow-up visit with the physiotherapist who had treated them. The aim of this visit was to encourage a high level of compliance with respect to continued trunk stabilization exercises and MDT practice (Table I).
Study Outcome Measures
The patients were given a battery of questionnaires to complete. Independent examiners, who were not involved in the treatment, distributed the questionnaires before treatment (baseline) and at the 3-, 12- and 24-month follow-ups.
The primary outcome measures were pain intensity in the leg, rated using a visual analogue scale (VAS) 0�100 mm (24) and the Oswestry Disability Index (ODI) 0�100 % (25). A score of 0�10 mm on the VAS was defined as no pain according to �berg et al. (26). An ODI score of 0�20% was defined as minimal or no disability, and a score of over 40% was defined as severe disability (25). These primary outcome measures are commonly used in evaluations after surgery for lowback pain and for assessing patients with lumbar disc herniation (27).
Secondary outcome measures included pain intensity in the back rated using a VAS and the degree of kinesiophobia using the Tampa Scale for Kinesiophobia (TSK). The TSK score varies between 17 and 68 and a cut-off more than 37 was defined as a high degree of kinesiophobia (28). Health-Related Quality of Life (HRQoL) in the European Quality of Life in 5 Dimensions Questionnaires (EQ-5D) was used. The EQ-5D includes 2 parts, EQ-5Dindex ranges from 0 to 1.0, where 1.0 is optimal health and EQ-5DVAS is a vertical visual analogue scale ranging from 0 (worst possible health state) to 100 (best possible health state) (29). The Zung Self-Rating Depression Scale (ZDS) ranges from 20�80 and the more depressed the patient is, the higher score (30). The Self-Efficacy Scale (SES) ranges from 8 to 64, with higher scores indicating more positive beliefs (31) was also used. Work status was measured using a 3-grade Likert scale: working full time, full-time sick leave and part-time sick leave. Likewise, patient�satisfaction with treatment was measured on a 3-grade Likert scale; satisfied, less satisfied and dissatisfied (32). These secondary outcome measures evaluate bio-psychosocial factors described as important in connection with lumbar disc surgery (33).
Statistical Analyses
The results are presented as median values and interquartile range (IQR), except for age, which is presented as the mean and standard deviation (SD). Changes over time within the group were analysed with the Wilcoxon signed-rank test. Statistical significance was set at an alpha level of 0.05.
Results
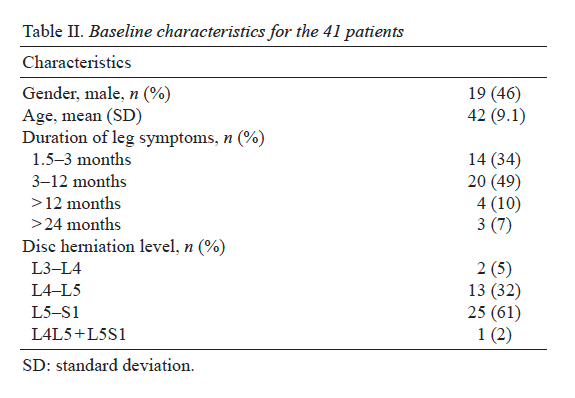
The baseline characteristics are shown in Table II. No patient had undergone surgery at the 3-month follow-up. At the 12-month follow-up, 3 patients had undergone surgery and, at the 24-month follow-up, 1 additional patient had been operated on. After surgery, these 4 patients were excluded from further follow-ups (Fig. 1).
Change Over Time in Primary Outcome Measures
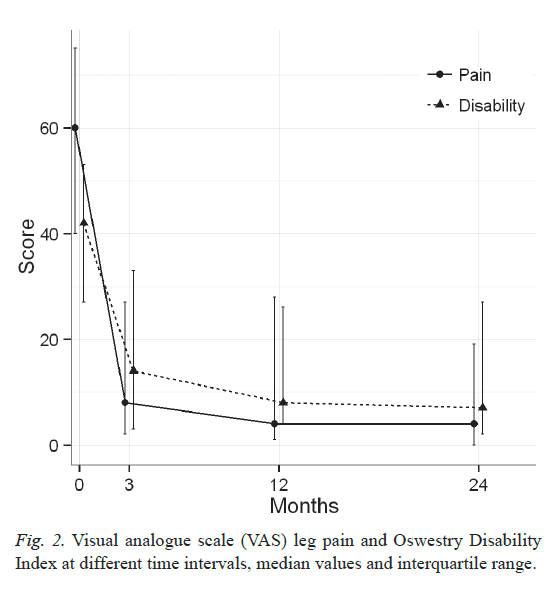
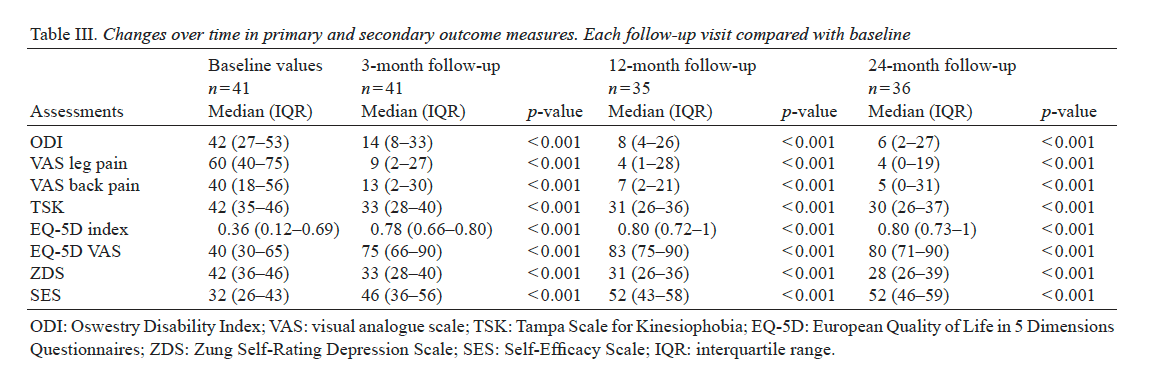
Disability. The patients showed significant improvements (p < 0.001) in ODI at the 3-month follow-up compared with baseline. The median (IQR) score decreased from 42 (27�53) to 14 (8�33). This improvement could still be seen at 12 and 24 months (Table III and Fig. 2). At baseline, 22 patients reported�severe disability (54%) and 3 patients reported no disability. The degree of disability decreased at the 3-month follow-up, as only 9 patients (22%) reported severe disability and 26 (64%) reported no disability. At 12- and 24-month follow-ups only 2 patients (5%) reported severe disability. At 12-month followup 26 patients still reported no disability, and at 24-month follow-up 27 patients reported no disability.
Leg pain. A significant reduction in patients� leg pain was found at the 3-month follow-up (p < 0.001) on the VAS compared with baseline. The median (IQR) on the VAS decreased from 60 (40�75) to 9 (2�27). This improvement could still be seen at the 12- and 24-month follow-ups (Table III and Fig. 2). Before treatment, all patients reported leg pain. Three months after treatment, the median on the VAS was 9 mm, i.e. classified as no leg pain (26). Twenty-three patients (56%) reported no leg pain at the 3-month follow-up. At the 12-month follow-up 22 patients reported no leg pain, and after 24 months 24 patients reported no leg pain.
Change in Secondary Outcome Measures Over Time
Back pain. A significant improvement in back pain was found at the 3-month follow-up (p < 0.001) on the VAS compared with baseline. This improvement could still be seen at 12 and 24 months (Table III). At baseline, 6 patients (15%) reported no back pain. Three months after treatment began, 20 patients (49%) reported no back pain.
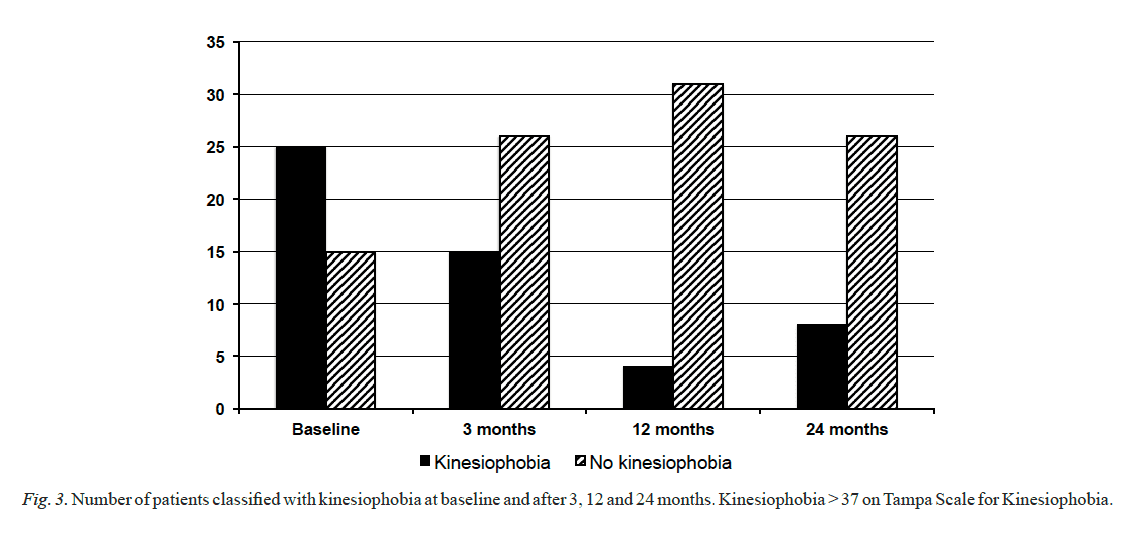
Kinesiophobia. The degree of kinesiophobia showed a significant improvement at the 3-month follow-up (p < 0.001) and the improvement could be seen throughout the follow-up period (Table III). Before treatment, 25 patients (61%) were classified as having kinesiophobia and 15 patients (37%) had no kinesiophobia, while data for 1 patient was missing. After 3 months, 15 patients (37%) had kinesiophobia and 26 (63%) had no kinesiophobia. At the 12-month follow-up, the number of patients with kinesiophobia had reduced to 4 (11%) (Fig. 3).
Health-related quality of life, depression and self-efficacy. All 4 assessments (EQ-5Dindex, EQ-5DVAS, ZDS and SES) showed significant improvements at the 3-month follow-up (p < 0.001). This improvement could still be seen at 12 and 24 months (Table III).
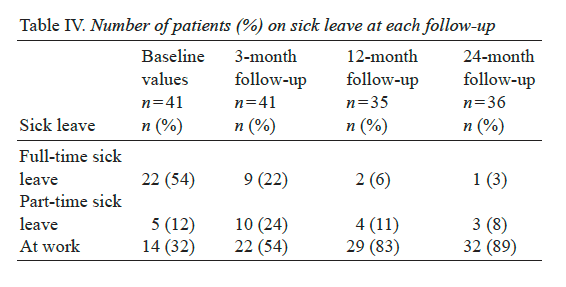
Sick leave. At baseline, 22 patients (54%) were on full-time sick leave (Table IV), compared with 9 (22%) patients at�the 3-month follow-up. At baseline, 14 patients (34%) were working full time, compared with 22 (54%) at the 3-month follow-up.
Satisfaction with Treatment
At the 3-month follow-up, 32 (78%) of 41 patients were satisfied with the structured physiotherapy treatment. Seven patients were less satisfied and 2 patients were dissatisfied. Both of the dissatisfied patients were later operated. At the 2-year follow-up, the number of satisfied patients was 29 (80%) of 36. Seven patients were less satisfied, but none dissatisfied after structured physiotherapy treatment.
Dr. Alex Jimenez’s Insight
A disc herniation in the lumbar spine can cause pain, numbness and weakness in the lower back. Because of the severity of the symptoms, many patients seeking fast pain relief consider surgery. However, many non-operative treatment options can help improve as well as manage lumbar herniated disc symptoms.�A structured physiotherapy treatment model can provide rapid pain relief to patients who would otherwise qualify for lumbar disc surgery, according to the following article. Patients looking to avoid taking long periods of sick leave from work due to their symptoms may benefit from a structured physiotherapy treatment model. As with any type of injury and/or condition, the use of other treatment options should be properly considered before turning to surgical interventions for fast pain relief.
Discussion
The principal finding of this study was that patients who qualified for lumbar disc surgery improved to a statistically significant and clinically substantial degree just 3 months after the start of the structured physiotherapy treatment in all assessments: disability, leg and back pain, kinesiophobia, health-related quality of life, depression and self-efficacy. The improvements could still be seen at the 2-year follow-up.
The natural course of healing must be considered carefully, especially when evaluating treatment effects in patients with disc herniation. The symptoms often vary over time and many discs heal spontaneously and the symptoms cease. Approximately 75% of patients with sciatica, without an MRI-verified disc herniation, recover within 3 months, and approximately one-third of patients recover within 2 weeks after the onset of sciatica (6). The natural course of sciatica was evaluated in a randomized controlled trial (34), which compared NSAIDs with placebo. The patients were, however, examined within 14 days after the onset of radiating leg pain. After 3 months, 60% of the patients had recovered and, after 12 months, 70% had recovered. In order to minimize the influence of spontaneous healing in the present study, the patients were therefore included only if they had had persistent pain and disability for more than 6 weeks. In fact, the majority of the patients had had pain and disability for more than 3 months. It is therefore most likely that the effects of treatment seen in the present study are, in the majority of patients, an effect of the structured physiotherapy treatment model and not a result of spontaneous healing.
In the study by Weber et al. (34), the VAS leg pain mean score was reduced from 54 mm at baseline to 19 mm within 4 weeks for all 183 patients, regardless of treatment. After 1 year, the VAS leg pain mean score was 17 mm. The patients in the present study who were a little worse at baseline (60 mm) reported 9 mm on the VAS leg pain just 3 months after treatment. Consequently, in the present study, the median VAS level had already been reduced to under the no-pain score, defined as 0�10 on the VAS (26), at the 3-month follow-up and this was maintained to the 12- and 24-month follow-ups.
Physiotherapy treatment for patients with lumbar disc herniation can lead to improvements. Br�tz et al. (17) included a selected group of patients who responded with the centralization of pain after the first 5 daily sessions of treatment according to the MDT method. Centralization of pain is defined as a clinically induced change in the location of pain referred from the spine, that moves from the most distal position toward the lumbar midline (35). However, the patients� medium duration of symptoms before treatment was only 12 days and the possibility that patients recovered naturally cannot therefore be excluded (17).
In a retrospective study, 95 patients were treated with a functional restoration programme (36). The patients achieved significant improvements after a mean treatment period of 8.7 months. The evaluation was performed at discharge only. With a treatment period of this length, it is, however, difficult to differentiate between the effects of treatment and the natural healing process. In the present study, a shorter treatment period was adopted, and large and significant improvements were found after just 3 months and were still present at the 24-month follow-up. It is therefore not likely that the natural healing process was responsible for the positive results in the present study.
In a prospective study of 82 consecutive patients with acute severe sciatica, included for conservative management, only a minority of the patients had made a full recovery after 12 months (37). Twenty-five percent of the patients underwent surgery within 4 months and one-third had surgery within 1 year. In spite of the fact that the inclusion criteria in the present study followed the recommendations for surgery (21, 38), no patient required surgery at the 3-month follow-up and, after 12 months, only 3 patients (7%) had undergone surgery. The interpretation of the divergence could be that the structured physiotherapy treatment model used in the present study appeared to influence patients with lumbar disc herniation in a very positive direction. One recommendation is therefore to follow the structured physiotherapy treatment model before considering surgery.
In this study, MRI verification of disc herniation was an inclusion criterion. In clinical practice, MRI verification is not mandatory, as it is in surgical treatment, before introducing structured physiotherapy treatment to patients with symptoms from a disc herniation. Consequently, treatment according to the structured physiotherapy treatment model can start early after the commencement of symptoms, as it is not necessary to wait for an MRI. It is possible to speculate that, if treatment with a structured physiotherapy model starts earlier than in the present study, the improvements would be even better, further reducing the risk of persistent pain and accompanying problems. Moreover, the need for MRI is likely to diminish; this, however, should be further evaluated in future studies.
One explanation for the good results of this study could be that the patients followed a structured physiotherapy treatment model, comprising MDT and trunk stabilization exercises, allowing for an individual design and progression of the treatment. Similar results were described in a retrospective cohort study (39) using several treatment methods for pain control as well as for exercise training for patients with lumbar disc herniation. The evaluation was not carried out until approximately 31 months after treatment. The results of Saal et al. (39) and of the present study are in agreement, in that structured physiotherapy treatment can reduce symptoms, but symptoms were relieved much more rapidly in the present study.
In a multicentre study comprising 501 patients, randomized to surgery or non-operative care, 18% of the patients assigned to non-operative treatment underwent surgery within 6 weeks and 30% had surgery at approximately 3 months (7). The nonoperative treatment group received non-specified �usual care�, which could include a variety of different treatment methods. In contrast, the patients in the present study were offered a structured physiotherapy treatment model that included both bio-psychological and social components, as described in the International Classification of Functioning, Disability and Health (40).
There are many possible explanations for the positive effects seen in this present study, and 5 of these will now be discussed. Firstly, the patients were well informed about the design of the structured physiotherapy treatment model, including the timetable for different phases of the treatment and when the treatment was planned to end. This information enhanced the patients� opportunity for self-management and gave them an active role in treatment decision-making.
Secondly, the patients acquired strategies to deal with their pain by using the different activities and movements in order to reduce pain according to the MDT method (14). The MDT method aims to enhance the patients� ability to cope with the symptoms, motivate the patient to comply with the treatment and empower them to achieve independence. Leijon et al. (41) have shown that low levels of motivation plus pain are important factors that enhance non-adherence to physical activity. It therefore appears important to reduce pain and increase motivation as early as possible. It is reasonable to believe that, when the patients participated in the evaluation of different activities and exercises, this augmented their opportunity to discover the connection between activities and the following reduction or increase in symptoms. This could have led to the increased self-efficacy and empowerment of the patients. The use of empowerment in physiotherapy has been recommended in a review by Perrault (42), who argues that empowerment improves the intervention.
Thirdly, the intensity of exercises was gradually increased on an individual basis with respect to the patients� reported pain. The objective was to strengthen the patients� self-efficacy, which also improved significantly in the present study. Fourthly, the trunk stabilization exercises were conducted with the aim of increasing deep trunk muscle control (23). It can be speculated that the physiological effects of training may also have led to reduced pain through increased blood circulation, muscle relaxation and the release of pain-reducing substances, such as endorphins.
Finally, one reason for the improvements could be that the physiotherapists were experienced and well educated in the MDT method. Subsequently, the physiotherapists were able to guide the patients during the rehabilitation process. It is, however, not possible to determine whether and how much each of the reasons discussed above contributed to the improvements. It seems reasonable to assume that all 5 factors were operating.
In this study, the majority of patients experienced kinesiophobia before treatment started. As early as 3 months after the structured physiotherapy treatment started, the number of patients with kinesiophobia fell dramatically and the majority of patients no longer experienced kinesiophobia. These results are in agreement with those of a study of patients with chronic pain and high kinesiophobia who increased their physical activity level after a pain management programme designed to enable the patients to regain overall function (43).
There are some limitations to this study. It is not possible to exclude the possibility that some patients may have improved spontaneously without treatment. Measures were taken to limit this risk by using symptoms for at least 6 weeks as an inclusion criterion. Again, the majority of patients had symptoms for more than 3 months. Another limitation might relate to whether the patients were selected accurately for the study. Clinically experienced orthopaedic surgeons evaluated the clinical findings and the MRI scans and classified the patients as surgical candidates based on recommendations from the American Academy of Orthopaedic Surgeons for intervention for disc herniation published in 1993 (21). The patients included in the present study also fulfilled the recommendations as presented by Bono and co-workers in 2006 (38). The patients can therefore be regarded as serving as their own controls, and comparisons can be made with baseline symptoms and with patients from other studies. An RCT would have been the best way to explore different treatment options; however, we did not reach the number of patients required for an RCT. As the treatment model used in the present study has not been evaluated previously in a group of patients with long-standing pain, with the majority of the patients having pain for more than 3 months due to disc herniation, and, as the results are clinically interesting, it was decided to present the results as a cohort study.
In conclusion, this study shows that patients eligible for lumbar disc surgery improved significantly after treatment with the structured physiotherapy model, as early as 3 months after treatment, and the results could still be seen at the 24-month follow-up. Consequently, these patients did not qualify for lumbar disc surgery 3 months after the physiotherapy treatment started. Moreover, the majority of patients had symptoms for more than 3 months at the start of treatment and, for this reason, most of the spontaneous healing ought to have occurred before this study started. This study therefore recommends adoption of the structured physiotherapy treatment model before considering surgery when patients report symptoms such as pain and disability due to lumbar disc herniation.
Acknowledgements
The authors would like to thank physiotherapists Patrik Drevander, Christina Grund�n, Sofia Frid�n and Eva Fahlgren for treating the patients and Valter Sundh for statistical support. This study was supported by grants from the Health & Medical Care Committee of the V�stra G�taland Region, Ren�e Eander�s Foundation and Wilhelm & Martina Lundgren�s Foundation of Science.
Herniated discs can cause pain, numbness and weakness, a variety of symptoms which may often become so severe, that surgery might seem like the only option for fast relief. However, a�structured physiotherapy treatment model can provide rapid relief to patients who qualify for lumbar disc surgery, according to the results of the research study. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Konstantinou K, Dunn KM. Sciatica: review of epidemiological
studies and prevalence estimates. Spine (Phila Pa 1976) 2008;
33: 2464�2472.
2. Nygaard OP, Kloster R, Solberg T. Duration of leg pain as a
predictor of outcome after surgery for lumbar disc herniation:
a prospective cohort study with 1-year follow up. J Neurosurg
2000; 92: 131�134.
3. Orief T, Orz Y, Attia W, Almusrea K. Spontaneous resorption
of sequestrated intervertebral disc herniation. World Neurosurg
2012; 77: 146�152.
4. Maigne JY, Rime B, Deligne B. Computed tomographic follow-up
study of forty-eight cases of nonoperatively treated lumbar intervertebral
disc herniation. Spine (Phila Pa 1976) 1992; 17: 1071�1074.
5. Takada E, Takahashi M, Shimada K. Natural history of lumbar disc
hernia with radicular leg pain: spontaneous MRI changes of the
herniated mass and correlation with clinical outcome. J Orthopaed
Surg (Hong Kong) 2001; 9: 1�7.
6. Vroomen PC, de Krom MC, Knottnerus JA. Predicting the outcome
of sciatica at short-term follow-up. Br J Gen Pract 2002;
52: 119�123.
7. Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Hanscom
B, Skinner JS, et al. Surgical vs nonoperative treatment for lumbar
disk herniation: the Spine Patient Outcomes Research Trial
(SPORT): a randomized trial. JAMA 2006; 296: 2441�2450.
8. Peul WC, van den Hout WB, Brand R, Thomeer RT, Koes BW.
Prolonged conservative care versus early surgery in patients with
sciatica caused by lumbar disc herniation: two year results of a
randomised controlled trial. BMJ 2008; 336: 1355�1358.
9. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-term
outcomes of surgical and nonsurgical management of sciatica secondary
to a lumbar disc herniation: 10 year results from the maine
lumbar spine study. Spine (Phila Pa 1976) 2005; 30: 927�935.
10. Weber H. Lumbar disc herniation. A controlled, prospective
study with ten years of observation. Spine (Phila Pa 1976) 1983;
8: 131�140.
11. Osterman H, Seitsalo S, Karppinen J, Malmivaara A. Effectiveness of microdiscectomy for lumbar disc herniation: a randomized
controlled trial with 2 years of follow-up. Spine (Phila Pa 1976)
2006; 31: 2409�2414.
12. Jacobs WC , van Tulder M, Arts M, Rubinstein SM, van Middelkoop
M, Ostelo R, et al. Surgery versus conservative management of
sciatica due to a lumbar herniated disc: a systematic review. Eur
Spine J 2011; 20: 513�522.
13. Svensson GL, Lundberg M, �stgaard HC, Wendt GK. High degree
of kinesiophobia after lumbar disc herniation surgery: a crosssectional
study of 84 patients. Acta Orthop 2011; 82: 732�736.
14. McKenzie R, May S. The lumbar spine: mechanical diagnosis
& therapy. 2nd ed. Spinal Publications New Zealand Limited:
Wellington; 2003.
15. Clare HA, Adams R, Maher CG. A systematic review of efficacy
of McKenzie therapy for spinal pain. Aust J Physiother 2004;
50: 209�216.
16. Paatelma M, Kilpikoski S, Simonen R, Heinonen A, Alen M, Videman
T. Orthopaedic manual therapy, McKenzie method or advice
only for low back pain in working adults: a randomized controlled
trial with one year follow-up. J Rehabil Med 2008; 40: 858�863.
17. Br�tz D, Kuker W, Maschke E, Wick W, Dichgans J, Weller M.
A prospective trial of mechanical physiotherapy for lumbar disk
prolapse. J Neurol 2003; 250: 746�749.
18. Hodges PW, Moseley GL. Pain and motor control of the lumbopelvic
region: effect and possible mechanisms. J Electromyogr
Kinesiol 2003; 13: 361�370.
19. Hides JA, Jull GA, Richardson CA. Long-term effects of specific
stabilizing exercises for first-episode low back pain. Spine (Phila
Pa 1976) 2001; 26: E243�E248.
20. Yilmaz F, Yilmaz A, Merdol F, Parlar D, Sahin F, Kuran B. Efficacy
of dynamic lumbar stabilization exercise in lumbar microdiscectomy.
J Rehabil Med 2003; 35: 163�167.
21. Nachemson AL. Lumbar disc herniation � conclusions. Acta Orthop
Scand Suppl 1993; 251: 49�50.
22. Kilpikoski S, Airaksinen O, Kankaanpaa M, Leminen P, Videman
T, Alen M. Interexaminer reliability of low back pain assessment
using the McKenzie method. Spine (Phila Pa 1976) 2002; 27:
E207�E214.
23. Richardson CA, Jull GA. Muscle control-pain control. What exercises
would you prescribe? Man Ther 1995; 1: 2�10.
24. Scott J, Huskisson EC. Graphic representation of pain. Pain 1976;
2: 175�184.
25. Fairbank JC, Couper J, Davies JB, O�Brien JP. The Oswestry
low back pain disability questionnaire. Physiotherapy 1980; 66:
271�273.
26. �berg B, Enthoven P, Kjellman G, Skargren E. Back pain in
primary care: a prospective cohort study of clinical outcome and
healthcare consumption. Adv Physiother 2003; 5: 98.
27. Bombardier C. Outcome assessments in the evaluation of treatment
of spinal disorders: summary and general recommendations. Spine
2000; 25: 3100�3103.
28. Vlaeyen JW, Kole-Snijders AM, Boeren RG, van Eek H. Fear of
movement/(re)injury in chronic low back pain and its relation to
behavioral performance. Pain 1995; 62: 363�372.
29. EuroQol � a new facility for the measurement of health-related quality
of life. The EuroQol Group. Health Policy 1990; 16: 199�208.
30. Zung WW. A self-rating depression scale. Arch Gen Psychiatry
1965; 12: 63�70.
31. Estlander AM, Vanharanta H, Moneta GB, Kaivanto K. Anthropometric
variables, self-efficacy beliefs, and pain and disability
ratings on the isokinetic performance of low back pain patients.
Spine 1994; 19: 941�947.
32. Str�mqvist B, J�nsson B, Fritzell P, H�gg O, Larsson BE, Lind B.
The Swedish National Register for lumbar spine surgery: Swedish
Society for Spinal Surgery. Acta Orthop Scand 2001; 72: 99�106.
33. den Boer JJ, Oostendorp RA, Beems T, Munneke M, Oerlemans
M, Evers AW. A systematic review of bio-psychosocial risk factors
for an unfavourable outcome after lumbar disc surgery. Eur Spine
J 2006; 15: 527�536.
34. Weber H, Holme I, Amlie E. The natural course of acute sciatica
with nerve root symptoms in a double-blind placebo-controlled
trial evaluating the effect of piroxicam. Spine (Phila Pa 1976)
1993; 18: 1433�1438.
35. Werneke M, Hart DL, Cook D. A descriptive study of the centralization
phenomenon. A prospective analysis. Spine (Phila Pa
1976) 1999; 24: 676�683.
36. Hahne AJ, Ford JJ, Hinman RS, Taylor NF, Surkitt LD, Walters
AG, et al. Outcomes and adverse events from physiotherapy
functional restoration for lumbar disc herniation with associated
radiculopathy. Disabil Rehabil 2011; 33: 1537�1547.
37. Balague F, Nordin M, Sheikhzadeh A, Echegoyen AC, Brisby H,
Hoogewoud HM, et al. Recovery of severe sciatica. Spine (Phila
Pa 1976) 1999; 24: 2516�2524.
38. Bono CM, Wisneski R, Garfin SR. Lumbar disc herniations. In:
Herkowitz HN, Garfin SR, Eismont FJ, Bell GR, Balderston RA,
editors. Rothman-Simeone the spine. 5th ed. Saunders Elsevier:
Philadelphia; 2006: p. 979�980.
39. Saal JA, Saal JS. Nonoperative treatment of herniated lumbar
intervertebral disc with radiculopathy. An outcome study. Spine
(Phila Pa 1976) 1989; 14: 431�437.
40. World Health Organisation. International Classification of Functioning,
Disability and Health (ICF). 2001 [cited 2012 Oct 9].
Available from: www.who.int/classifications/icf/en/.
41. Leijon ME, Faskunger J, Bendtsen P, Festin K, Nilsen P. Who is
not adhering to physical activity referrals, and why? Scand J Prim
Health Care 2011; 29: 234�240.
42. Perreault K. Linking health promotion with physiotherapy for low
back pain: a review. J Rehabil Med 2008; 40: 401�409.
43. Koho P, Orenius T, Kautiainen H, Haanpaa M, Pohjolainen T, Hurri
H. Association of fear of movement and leisure-time physical
activity among patients with chronic pain. J Rehabil Med 2011;
43: 794�799.
Recognizing clinical and experimental evidence, physiotherapy is a healthcare profession that helps restore and maintain function to individuals affected by injury, disease or disability by using mechanical force and movements, manual therapy, exercise and electrotherapy, as well as through patient education and advice. The terms physiotherapy and physical therapy are used interchangeably to describe the same healthcare profession. Physiotherapy is recommended for a variety of injuries and conditions, and it can help support overall health and wellness for people of all ages.
For further notice,�physiotherapy services may be offered alongside chiropractic care, to provide a cautious and gentle manipulation and/or mobilization of the cervical and thoracic spine in the instance of a large cervical disc herniation. Cervical disc herniations can cause pain and discomfort, numbness and weakness in the neck, shoulders, chest, arms and hands.
Abstract
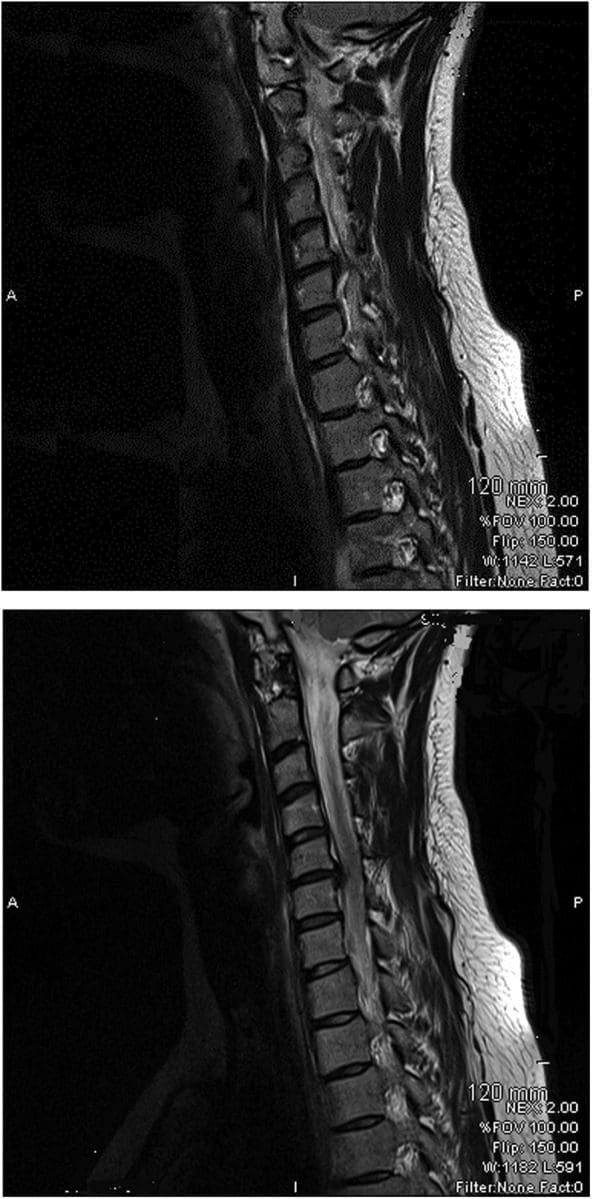
A 34-year-old woman was seen in a physiotherapy department with signs and symptoms of cervical radiculopathy. Loss of cervical lordosis and a large paracentral to intraforaminal disc prolapse (8?mm) at C5�C6 level was reported on MRI. She was taking diclofenac sodium, tramadol HCl, diazepam and pregabalin for the preceding 2?months and no significant improvement, except temporary relief, was reported. She was referred to physiotherapy while awaiting a surgical opinion from a neurosurgeon. In physiotherapy she was treated with mobilisation of the upper thoracic spine from C7 to T6 level. A cervical extension exercise was performed with prior voluntary extension of the thoracic spine and elevated shoulders. She was advised to continue the same at home. General posture advice was given. Signs and symptoms resolved within the following four sessions of treatment over 3?weeks. Surgical intervention was subsequently deemed unnecessary.
Background
Surgical interventions are commonly recommended in large cervical prolapsed discs and the importance of non-aggressive physiotherapy interventions is less recognised and poorly understood. We present interventions that were associated with resolution of symptoms of radiculopathy resulting from a larger cervical herniated disc. These interventions, if applied correctly, may help to reduce the number of surgeries required for cervical prolapsed discs.
Case Presentation
The patient was a 34-year-old woman. She was seen in the physiotherapy department with a complaint of left-sided neck and shoulder pain. The pain was radiating to her left arm and there was associated numbness. The duration of symptoms was more than 2?months with no history of trauma. The pain was present on waking in the morning and gradually increased during the day. She was otherwise a healthy woman. Neck movements were aggravating the symptoms. She was seen in the acute hospital accident and emergency department (A&E) twice since onset and had been taking diclofenac sodium, tramadol HCl, diazepam and pregabalin. An MRI was planned and a request was sent for physiotherapy during the MRI waiting period. A neurosurgical review was requested by the A&E consultant upon receipt of the MRI report 7?weeks later.
Patient examination in the physiotherapy department revealed a normal gait pattern, her left arm held in front of her chest with the left shoulder slightly elevated. Her active range of neck motion was restricted and was painful on the left side. Flexion and rotation to the left were aggravating her arm and shoulder pain. Strength deficits were noted in the left elbow flexors and wrist extensors (4/5) when compared with the right side. There was paraesthesia along the radial border of the forearm and thumb regions. The brachioradialis reflex was diminished and biceps reflex was sluggish. Triceps and plantar reflexes were normal. Passive intervertebral movements were tender at C5�C6 level and were reproducing the pain. Sustained pressure at C7 and below was easing the pain and also improving the neck range of motion. The patient was deemed to have C6 radiculopathy. The MRI report, available 2?weeks after the commencement of physiotherapy, confirmed the diagnosis.
Investigations
The findings from the plain cervical x-ray were unremarkable. MRI showed (Figure 1) loss of cervical spine lordosis, a left paracentral to intraforaminal lesion with 8?mm hernia, which indented the cord and obstructed the left paracentral recess and neural foramen.
Figure 1: Loss of cervical spine lordosis and large disc herniation at C5 and C6 on MRI.
Differential Diagnosis
Cervical myelopathy.
Treatment
The patient received pharmacological treatment for the initial two symptomatic months, which included diclofenic sodium, tramadol, diazepam and pregabalin (lyrica) tablet. Physiotherapy was started after 2?months. Physiotherapy intervention consisted of mobilisation of the thoracic spine, resisted cervical extension exercises, a home programme of exercises and advice regarding the posture.
Mobilisation of the thoracic spine was administered in the prone lying position from C7 toT6 level. Mild intensity oscillations (15?reps) in an anterosuperior direction were directly applied to each of the spinal segments, through the thumb over the spinous processes, during the first visit. The applied force was enough to appreciate intervertebral movement in each segment and without significant pain. High-intensity oscillations (10�20) were applied during the subsequent treatment sessions. The patient was asked for symptom feedback during treatment.
Cervical spine extension exercises were carried out in a sitting position. The patient was asked to extend her thoracic spine with lungs fully inflated and shoulders elevated followed by extension of her cervical spine. Head extension was moderately resisted by the therapist near the end range of extension for 5�10?s and brought back to neutral after each resisted movement. The resisted movement was repeated at least three times with intervals of 30?s. The patient was asked to perform the same exercise at home every hour during the day.
The patient was educated regarding the rationale of extension exercises, sitting and lying posture and their effects on the spine. The duration of each session was approximately 20�25?min.
Dr. Alex Jimenez’s Insight
Surgical interventions are generally recommended and widely considered for large cervical disc herniations. Although less recognized and often misunderstood, however, physiotherapy can be just as effective towards improving herniated discs in the cervical spine, excluding the need for surgery, according to the research study. Pharmacological treatments are also commonly used to help temporarily reduce symptoms alongside physiotherapy interventions. Cautious and gentle, spinal manipulation and mobilization of the cervical spine should be performed in the case of large cervical disc herniations to avoid aggravating the injury and/or condition. As recommended by a physiotherapist, or other healthcare professional experienced in physiotherapy, proper exercise can restore the function of the cervical spine and prevent regression of large prolapsed discs along the spine. Through appropriate physiotherapy intervention as well as through patient safety and compliance, the retraction of the cervical herniated discs is possible.
Outcome and Follow-Up
Pharmacological interventions were helpful to reduce the patient’s pain on a temporary basis. Symptoms were recurring and resolution was not sustainable. The symptoms started improving after the first physiotherapy session and continued to improve during the subsequent sessions. It fully resolved in four sessions extended over 3?weeks. The patient was reviewed 4?months after the resolution of symptoms and there was no recurrence of symptoms. She was reviewed by a neurosurgeon and the surgical option was withdrawn.
Discussion
Stiffness of the thoracic spine has been linked to the painful pathologies of the cervical spine, and manipulation of the thoracic spine has been shown to improve painful symptoms and mobility of the cervical spine. However, cervical disc herniations of greater than 4?mm are considered inappropriate for physiotherapy interventions such as traction and manipulation. Spinal manipulation refers to a passive movement thrust of high velocity and low amplitude, usually applied at the end range of movement and is beyond the patient’s control. Manipulation of the cervical spine is an aggressive procedure, which carries various risks and is often associated with worsening of symptoms. Manipulation was not considered in the treatment options for this patient because of the risks associated with it, and also because of patient’s anxiety and lack of MRI-confirmed diagnosis.
Active extension of the thoracic spine increases the range of motion of the cervical spine and, in these authors� clinical experience, relieves minor neck symptoms. Conversely, thoracic spine kyphosis, such as slouch sitting, restricts the mobility of the cervical spine and aggravates the painful symptoms. A good sitting posture is constituted by a slightly extended thoracic spine. Therefore, active extension of the thoracic spine prior to cervical extension may improve cervical movements and restore cervical curvature.
It is believed that excessive pressure during flexion on the anterior aspect of the intervertebral discs pushes the nucleus pulposus posteriorly and causes herniations. Conversely, cervical lordosis might have the reverse effect�that is, decreases pressure on the anterior aspect of the discs and may create a suction effect which retracts the herniated contents. Therefore, a combination of short duration and repeated movements at the end of extension may serve as a suction pump and possibly retract the extruded content of the disc. Active cervical extension exercises, with an extended thoracic spine posture, may have been the key element in a home exercise programme to restore lordosis of the cervical spine and relieve radiculopathy symptoms in the current case. This may possibly have been due to the retraction of the herniated discs.
Spinal mobilisation refers to a gentle, oscillatory, passive movement of a spinal segment. These are applied to a spinal segment to gently increase the passive range of motion. It allows the patient to report aggravation of pain and to resist any unwanted movements. No mobilisation treatment was administered at C5�C6 level as palpation at this level was aggravating the symptoms. Segments below this level were mobilised with emphasis at C7�T1 level. Any treatment at the affected segment was likely to irritate the nerve root and thereby increase the inflammatory process.
Various interventions are reported for the treatment of prolapsed discs. Saal et al reported the use of traction, specific physical therapy exercise, oral anti-inflammatory medication and patient education in the treatment of 26 patients with herniated cervical discs (<4?mm) and reported significant improvement in outcomes for 24 patients. They observed that surgery for disc herniations occurs when a patient has significant myotomal weakness, severe pain or pain that persists beyond an arbitrary conservative treatment period of 2�8?weeks.
Spontaneous regressions of cervical disc protrusions are reported in the literature. However, spontaneous regressions of herniated cervical discs are speculated to be rare. Various factors related to regression are hypothesised and theorised. Pan et al summarised the factors related to the resorption of herniated disc as: the age of the patients; dehydration of the expanded nucleus pulposus; resorption of haematoma; revascularisation; penetration of herniated cervical disc fragments through the posterior longitudinal ligament; size of disc herniations; and existence of cartilage and annulus fibrosus tissue in the herniated material. Some studies on spontaneous regressions of discs reported that the patients were receiving physiotherapy. Physiotherapy interventions are not defined in any of these studies, however. Therefore, it is possible that disc regressions in these studies may be due to similar physiotherapy interventions as described here, or the patients were practising techniques and adopting postures as reported in the current case.
Learning Points
Thoracic spine mobilisation improves cervical spine biomechanics and can be considered in conjunction with other interventions in all painful conditions of the cervical spine.
Active extension of the thoracic spine facilitates movements of the cervical spine and may help regression of large prolapsed discs.
There is a possibility of retraction of herniated cervical discs through appropriate physiotherapy intervention.
Patient education ensures safety and compliance to therapist advice.
Meticulous assessment and patient feedback guides the therapist in selection of intensity of mobilisation.
Footnotes
Competing interests: None.
Patient consent: Obtained.
In conclusion,�physiotherapy, or physical therapy, is used to treat various injuries, diseases and disabilities, through the use of mechanical force and movements, manual therapy, exercise, electrotherapy, and through patient education and advice to restore and maintain function. As in the case above, physiotherapy can be recommended and considered as treatment before referring to surgical interventions of large cervical disc herniations. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1.�Norlander S, Gustavsson BA, Lindell J, et al.�Reduced mobility in the cervico-thoracic motion segment�a risk factor for musculoskeletal neck-shoulder pain: a two-year prospective follow-up study.�Scand J Rehabil Med�1997;29:167�74.�[PubMed]
2.�Walser RF, Meserve BB, Boucher TR.�The effectiveness of thoracic spine manipulation for the management of musculoskeletal conditions: a systematic review and meta-analysis of randomized clinical trials.�J Man Manipulative Ther�2009;17:237�46.�[PMC free article]�[PubMed]
3.�Krauss J, Creighton D, Ely JD, et al.�The immediate effects of upper thoracic translatoric spinal manipulation on cervical pain and range of motion: a randomized clinical trial.�J Man Manipulative Ther2008;16:93�9.�[PMC free article]�[PubMed]
4.�Saal JS, Saal JA, Yurth EF.�Nonoperative management of herniated cervical intervertebral disc with radiculopathy.�Spine (Phila Pa 1976)�1996;21:1877�83.�[PubMed]
5.�Murphy DR, Beres JL.�Cervical myelopathy: a case report of a �near-miss� complication to cervical manipulation.�J Manipulative Physiol Ther�2008;31:553�7.�[PubMed]
6.�Leon-Sanchez A, Cuetter A, Ferrer G.�Cervical spine manipulation: an alternative medical procedure with potentially fatal complications.�South Med J�2007;100:201�3.�[PubMed]
7.�Scannell JP, McGill SM.�Disc prolapse: evidence of reversal with repeated extension.�Spine (Phila Pa 1976)�2009;34:344�50.�[PubMed]
8.�Gurkanlar D, Yucel E, Er U, et al.�Spontaneous regression of cervical disc herniations.�Minim Invasive Neurosurg�2006;49:179�83.�[PubMed]
9.�Mochida K, Komori H, Okawa A, et al.�Regression of cervical disc herniation observed on magnetic resonance images.�Spine (Phila Pa 1976)�1998;23:990�5; discussion 6�7.�[PubMed]
10.�Song JH, Park HK, Shin KM.�Spontaneous regression of a herniated cervical disc in a patient with myelopathy. Case report.�J Neurosurg�1999;90(1 Suppl):138�40.�[PubMed]
12.�Pan H, Xiao LW, Hu QF.�Spontaneous regression of herniated cervical disc fragments and its clinical significance.�Orthop Surg�2010;2:77�9.�[PubMed]
13.�Teplick JG, Haskin ME.�Spontaneous regression of herniated nucleus pulposus.�AJR Am J Roentgenol1985;145:371�5.�[PubMed]
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine