Postural orthostatic tachycardia syndrome is a medical condition that causes lightheadedness and palpitations after standing. Can lifestyle adjustments and multidisciplinary strategies help reduce and manage symptoms?
Postural Orthostatic Tachycardia Syndrome – POTS
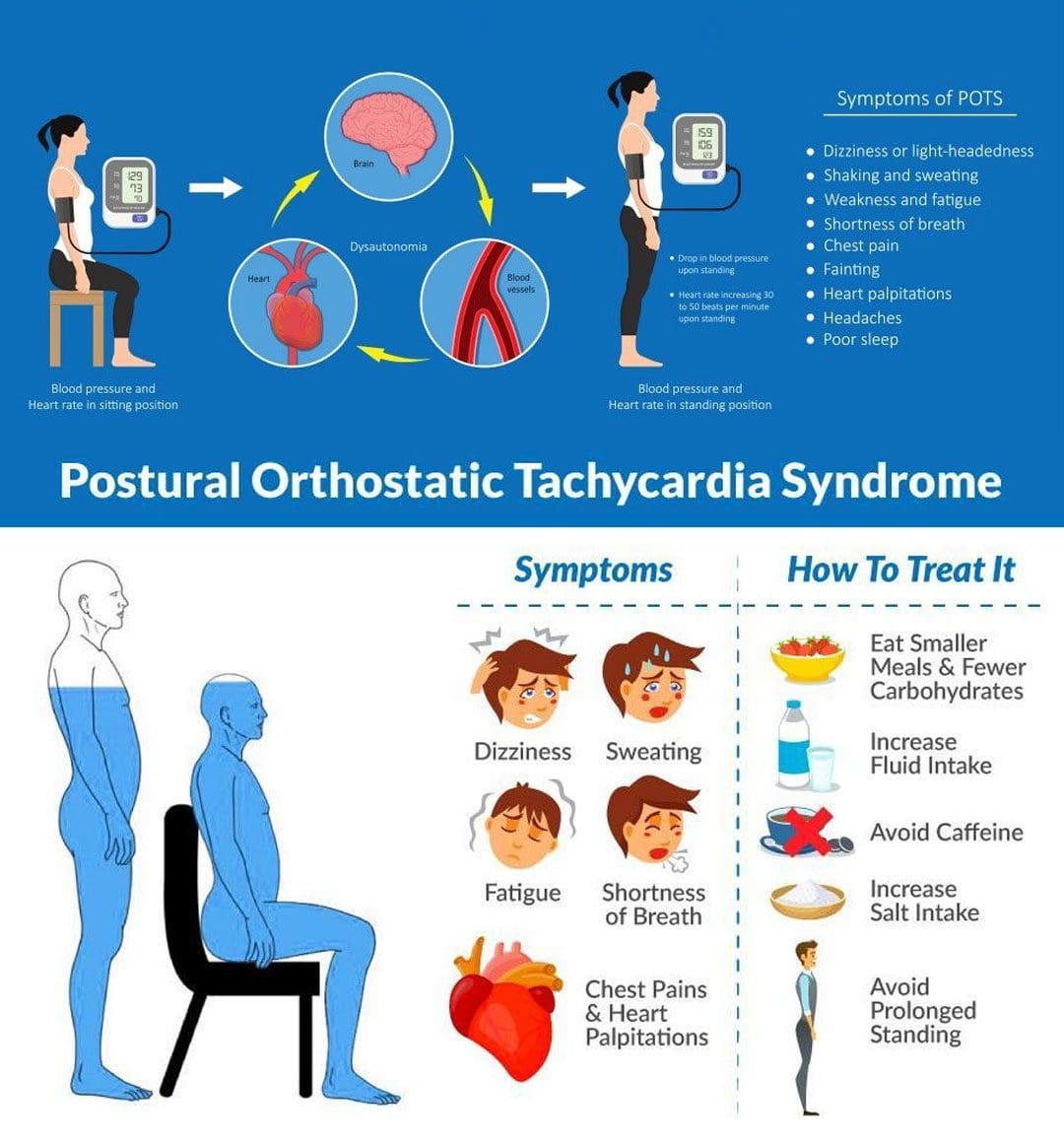
Postural orthostatic tachycardia syndrome, or POTS, is a condition that varies in severity from relatively mild to incapacitating. With POTS:
The heart rate increases dramatically with body position.
This condition often affects young individuals.
Most individuals with postural orthostatic tachycardia syndrome are women between the ages of 13 and 50.
Some individuals have a family history of POTS; some individuals report POTS began after an illness or stressor, and others report it began gradually.
It usually resolves over time.
Treatment can be beneficial.
Diagnosis is based on assessing blood pressure and pulse/heart rate.
Symptoms
Postural orthostatic tachycardia syndrome can affect young individuals who are otherwise healthy and can begin suddenly. It usually happens between the ages of 15 and 50, and women are more likely to develop it than men. Individuals can experience various symptoms within a few minutes of standing up from a lying or seated position. The symptoms can occur regularly and daily. The most common symptoms include: (National Institutes of Health. National Center for Advancing Translational Sciences. Genetic and Rare Diseases Information Center. 2023)
Anxiety
Lightheadedness
A feeling like you’re about to pass out.
Palpitations – sensing rapid or irregular heart rate.
Dizziness
Headaches
Blurred vision
Legs turn to reddish-purple.
Weakness
Tremors
Fatigue
Sleep problems
Trouble concentrating/brain fog.
Individuals may also experience recurrent episodes of fainting, usually without any trigger/s other than standing up.
Individuals can experience any combination of these symptoms.
Sometimes, individuals cannot handle sports or exercise and may feel light-headed and dizzy in response to mild or moderate physical activity, which can be described as exercise intolerance.
Associated Effects
Postural orthostatic tachycardia syndrome can be associated with other dysautonomia or nervous system syndromes, like neurocardiogenic syncope.
Individuals are often co-diagnosed with other conditions like:
Chronic fatigue syndrome
Ehlers-Danlos syndrome
Fibromyalgia
Migraines
Other autoimmune conditions.
Bowel conditions.
Causes
Usually, standing up causes blood to rush from the torso to the legs. The sudden change means less blood is available for the heart to pump. To compensate, the autonomic nervous system sends signals to the blood vessels to constrict to push more blood to the heart and maintain blood pressure and a normal heart rate. Most individuals do not experience significant changes in blood pressure or pulse when standing up. Sometimes, the body is unable to perform this function correctly.
If blood pressure drops from standing and causes symptoms like lightheadness, it is known as orthostatic hypotension.
If the blood pressure remains normal, but the heart rate gets faster, it is POTS.
The exact factors that cause postural orthostatic tachycardia syndrome are different in individuals but are related to changes in:
The autonomic nervous system, adrenal hormone levels, total blood volume, and poor exercise tolerance. (Robert S. Sheldon et al., 2015)
Autonomic Nervous System
The autonomic nervous system controls blood pressure and heart rate, which are the areas of the nervous system that manage internal bodily functions like digestion, respiration, and heart rate. It is normal for blood pressure to drop slightly and the heart rate to speed up a little when standing. With POTS, these changes are more pronounced.
POTS is considered a type of dysautonomia, which is diminished regulation of the autonomic nervous system.
Several other syndromes are also thought to be related to dysautonomia, like fibromyalgia, irritable bowel syndrome, and chronic fatigue syndrome.
It isn’t clear why the syndrome or any of the other types of dysautonomia develop, but there seems to be a familial predisposition.
Sometimes the first episode of POTS manifests after a health event like:
Pregnancy
Acute infectious illness, for example, a severe case of influenza.
An episode of trauma or concussion.
Major surgery
Diagnosis
A diagnostic evaluation will include a medical history, a physical examination, and diagnostic tests.
The healthcare provider will take blood pressure and pulse at least twice. Once while lying down and once while standing.
Blood pressure measurements and pulse rate lying down, sitting, and standing are orthostatic vitals.
Typically, standing up increases the heart rate by 10 beats per minute or less.
With POTS, heart rate increases by 30 beats per minute while blood pressure remains unchanged. (Dysautonomia International. 2019)
The heart rate stays elevated for over a few seconds upon standing/usually 10 minutes or more.
Symptoms happen frequently.
Lasts more than a few days.
Positional pulse changes are not the only diagnostic consideration for postural orthostatic tachycardia syndrome, as individuals can experience this change with other conditions.
During this test, blood pressure and pulse are measured several times when lying on a table and when the table is moved to an upright position.
Differential Diagnosis
There are various causes of dysautonomia, syncope, and orthostatic hypotension.
Throughout the evaluation, the healthcare provider may look at other conditions, like dehydration, deconditioning from prolonged bed rest, and diabetic neuropathy.
Medications like diuretics or blood pressure medication can cause similar effects.
Treatment
Several approaches are used in managing POTS, and individuals may require a multidisciplinary approach. The healthcare provider will advise regularly checking blood pressure and pulse at home to discuss the results when going in for medical checkups.
Fluids and Diet
Drinking non-caffeinated fluids can keep the body hydrated.
A healthcare provider can calculate the right amount of fluids that are needed each day.
Overnight dehydration is common, so it is especially important to drink fluids first thing in the morning, preferably before getting out of bed and standing.
Exercise and physical therapy can help the body learn to adjust to an upright position.
Because it can be challenging to exercise when dealing with POTS, a targeted exercise program under supervision may be required.
An exercise program may begin with swimming or using rowing machines, which do not require upright posture. (Dysautonomia International. 2019)
After a month or two, walking, running, or cycling may be added.
Studies have shown that individuals with POTS, on average, have smaller cardiac chambers than individuals who don’t have the condition.
Regular aerobic exercise has been shown to increase cardiac chamber size, slow heart rate, and improve symptoms. (Qi Fu, Benjamin D. Levine. 2018)
Individuals must continue an exercise program for the long term to keep symptoms from returning.
Medication
Prescription medications to manage POTS include midodrine, beta-blockers, pyridostigmine – Mestinon, and fludrocortisone. (Dysautonomia International. 2019)
Ivabradine, used for the heart condition of sinus tachycardia, has also been used effectively in some individuals.
Conservative Interventions
Other ways to help prevent symptoms include:
Sleeping in the head-up position by elevating the head of the bed off the ground 4 to 6 inches utilizing an adjustable bed, blocks of wood, or risers.
This increases the blood volume in circulation.
Performing countermeasure maneuvers like squatting, squeezing a ball, or crossing the legs. (Qi Fu, Benjamin D. Levine. 2018)
Wearing compression stockings to prevent too much blood from flowing into the legs when standing can help avoid orthostatic hypotension. (Dysautonomia International. 2019)
Conquering Congestive Heart Failure
References
National Institutes of Health. National Center for Advancing Translational Sciences. Genetic and Rare Diseases Information Center (GARD). (2023). Postural orthostatic tachycardia syndrome.
Sheldon, R. S., Grubb, B. P., 2nd, Olshansky, B., Shen, W. K., Calkins, H., Brignole, M., Raj, S. R., Krahn, A. D., Morillo, C. A., Stewart, J. M., Sutton, R., Sandroni, P., Friday, K. J., Hachul, D. T., Cohen, M. I., Lau, D. H., Mayuga, K. A., Moak, J. P., Sandhu, R. K., & Kanjwal, K. (2015). 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart rhythm, 12(6), e41–e63. https://doi.org/10.1016/j.hrthm.2015.03.029
For individuals working at a desk or work station where the majority of the work is done in a sitting position and increases the risk for a variety of health problems, can using a standing desk help prevent musculoskeletal problems and improve short and long-term wellness?
Stand Desks
More than 80% of jobs are done in a seated position. Stand desks have proven to help. (Allene L. Gremaud et al., 2018) An adjustable stand desk is intended to be the standing height of an individual. Some desks can be lowered to use while sitting. These desks can improve:
Blood circulation
Back pain
Energy
Focus
Individuals who are less sedentary may experience decreased depression, anxiety, and risk of chronic disease.
Improve Posture and Decrease Back Pain
Sitting for prolonged periods can cause fatigue and physical discomfort. Back pain symptoms and sensations are common, especially when practicing unhealthy postures, already dealing with existing back problems, or using a non-ergonomic desk set-up. Instead of only sitting or standing for the whole workday, alternating between sitting and standing is far healthier. Practicing sitting and standing regularly reduces body fatigue and lower back discomfort. (Alicia A. Thorp et al., 2014) (Grant T. Ognibene et al., 2016)
Increases Energy Levels
Prolonged sitting correlates with fatigue, reduced energy, and productivity. A sit-stand desk can provide benefits like increased productivity levels. Researchers discovered that sit-stand desks could improve the general health and productivity of office workers. Individuals in the study reported:
According to the CDC, six in 10 individuals in the U.S. have at least one chronic disease, like diabetes, heart disease, stroke, or cancer. Chronic disease is the leading cause of death and disability, as well as a leading force of healthcare costs. (Centers for Disease Control and Prevention. 2023) While further research is needed to see if standing desks can reduce the risk of chronic disease, one study looked to quantify the association between sedentary time and the risk of chronic disease or death. Researchers reported that sedentariness for prolonged periods was independently associated with negative health outcomes regardless of physical activity. (Aviroop Biswas et al., 2015)
Improved Mental Focus
Sitting for extended periods slows down blood circulation. This decreased blood flow to the brain lowers cognitive function and increases the risk of neurodegenerative conditions. One study confirmed that healthy individuals who worked in a prolonged sitting position had reduced brain blood flow. The study found that frequent, short walks could help prevent this. (Sophie E. Carter et al., 2018) Standing increases blood and oxygen circulation. This improves cognitive function, which also helps improve focus and concentration.
Depression and Anxiety Reduction
Modern lifestyles typically contain large amounts of sedentary behavior.
However, there is a small amount about the mental health risks of prolonged sedentary behavior. There have been a few studies aimed at improving public understanding. One study focused on a group of older adults, having them self-report sedentary habits that included television, internet, and reading time. This information was compared to their individual scoring on the Centre of Epidemiological Studies Depression scale. (Mark Hamer, Emmanuel Stamatakis. 2014)
The researchers found that certain sedentary behaviors are more harmful to mental health than others.
Television watching, for example, resulted in increased depressive symptoms and decreased cognitive function. (Mark Hamer, Emmanuel Stamatakis. 2014)
Internet use had the opposite effect, decreasing depressive symptoms and increasing cognitive function.
Researchers theorize that the results come from the contrasting environmental and social contexts in which they are happening. (Mark Hamer, Emmanuel Stamatakis. 2014)
Another study looked at the possible correlation between sedentary behavior and anxiety.
Incorporating a standing desk into the workspace can help to reduce the negative effects of sedentary behaviors, leading to improved productivity, improved mental and physical health, and a healthy work environment for individuals who work long hours at a desk or workstation.
Understanding Academic Low Back Pain: Impact and Chiropractic Solutions
References
Gremaud, A. L., Carr, L. J., Simmering, J. E., Evans, N. J., Cremer, J. F., Segre, A. M., Polgreen, L. A., & Polgreen, P. M. (2018). Gamifying Accelerometer Use Increases Physical Activity Levels of Sedentary Office Workers. Journal of the American Heart Association, 7(13), e007735. https://doi.org/10.1161/JAHA.117.007735
Thorp, A. A., Kingwell, B. A., Owen, N., & Dunstan, D. W. (2014). Breaking up workplace sitting time with intermittent standing bouts improves fatigue and musculoskeletal discomfort in overweight/obese office workers. Occupational and environmental medicine, 71(11), 765–771. https://doi.org/10.1136/oemed-2014-102348
Ognibene, G. T., Torres, W., von Eyben, R., & Horst, K. C. (2016). Impact of a Sit-Stand Workstation on Chronic Low Back Pain: Results of a Randomized Trial. Journal of occupational and environmental medicine, 58(3), 287–293. https://doi.org/10.1097/JOM.0000000000000615
Ma, J., Ma, D., Li, Z., & Kim, H. (2021). Effects of a Workplace Sit-Stand Desk Intervention on Health and Productivity. International journal of environmental research and public health, 18(21), 11604. https://doi.org/10.3390/ijerph182111604
Centers for Disease Control and Prevention. Chronic disease.
Biswas, A., Oh, P. I., Faulkner, G. E., Bajaj, R. R., Silver, M. A., Mitchell, M. S., & Alter, D. A. (2015). Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Annals of internal medicine, 162(2), 123–132. https://doi.org/10.7326/M14-1651
Carter, S. E., Draijer, R., Holder, S. M., Brown, L., Thijssen, D. H. J., & Hopkins, N. D. (2018). Regular walking breaks prevent the decline in cerebral blood flow associated with prolonged sitting. Journal of applied physiology (Bethesda, Md. : 1985), 125(3), 790–798. https://doi.org/10.1152/japplphysiol.00310.2018
Hamer, M., & Stamatakis, E. (2014). Prospective study of sedentary behavior, risk of depression, and cognitive impairment. Medicine and science in sports and exercise, 46(4), 718–723. https://doi.org/10.1249/MSS.0000000000000156
Teychenne, M., Costigan, S. A., & Parker, K. (2015). The association between sedentary behaviour and risk of anxiety: a systematic review. BMC public health, 15, 513. https://doi.org/10.1186/s12889-015-1843-x
For individuals experiencing a turf toe injury, can knowing the symptoms help athletes and non-athletes with treatment, recovery time, and returning to activities?
Turf Toe Injury
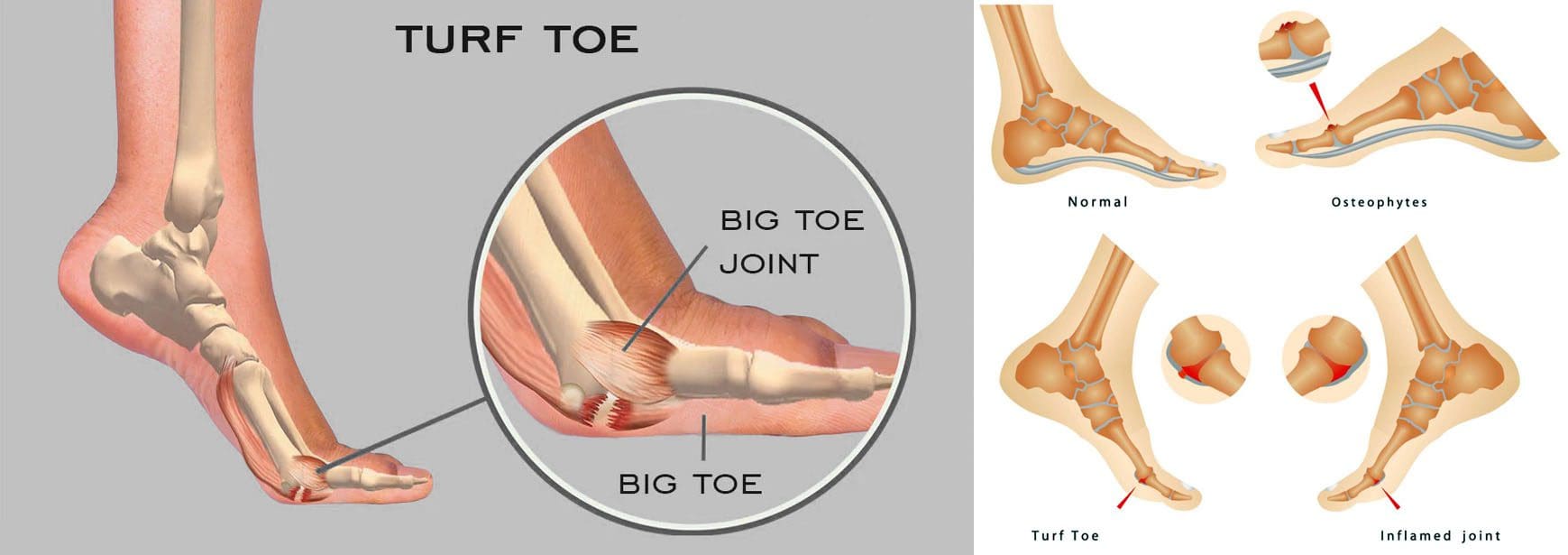
A turf toe injury affects the soft tissue ligaments and tendons at the base of the big toe under the foot. This condition usually occurs when the toe is hyperextended/forced upward, such as when the ball of the foot is on the ground and the heel is lifted. (American Academy of Orthopaedic Surgeons. 2021) The injury is common among athletes who play sports on artificial turf, which is how the injury got its name. However, it can also affect non-athletes, like individuals working on their feet all day.
Recovery time after turf toe injury depends on the severity and the type of activities the individual plans to return to.
Returning to high-level sports activities after a severe injury can take six months.
These injuries vary in severity but usually improve with conservative treatment. In severe cases, surgery could be required.
Pain is the primary issue that stops physical activities after a grade 1 injury, while grades 2 and 3 can take weeks to months to heal completely.
Meaning
A turf toe injury refers to a metatarsophalangeal joint strain. This joint comprises ligaments that connect the bone on the sole of the foot, below the big toe/proximal phalanx, to the bones that connect the toes to the larger bones in the feet/metatarsals. The injury is usually caused by hyperextension that often results from a pushing-off motion, like running or jumping.
If experiencing turf toe symptoms, see a healthcare provider for a proper diagnosis so they can develop a personalized treatment plan. They will perform a physical exam to assess pain, swelling, and range of motion. (American Academy of Orthopaedic Surgeons. 2021) If the healthcare provider suspects tissue damage, they may recommend imaging with X-rays and (MRI) to grade the injury and determine the proper course of action.
Grades 2 and 3 come with partial or complete tissue tearing, severe pain, and swelling. Treatments for more severe turf toe can include: (Ali-Asgar Najefi et al., 2018)
Limited weight bearing
Using assistive devices like crutches, a walking boot, or a cast.
Physical therapy also includes proprioception and agility training exercises, orthotics, and wearing recommended shoes for specific physical activities. (Lisa Chinn, Jay Hertel. 2010)
A physical therapist can also help ensure that the individual does not return to physical activities before the injury is fully healed and prevent the risk of re-injury.
Grade 1 – Subjective as it varies depending on the individual’s pain tolerance.
Grade 2 – Four to six weeks of immobilization.
Grade 3 – Eight weeks minimum of immobilization.
It can take up to six months to return to normal function.
Returning To Normal Activities
After a grade 1 turf toe injury, individuals can return to normal activities once the pain is under control. Grades 2 and 3 take longer to heal. Returning to sports activities after a grade 2 injury can take around two or three months, while grade 3 injuries and cases that require surgery can take up to six months. (Ali-Asgar Najefi et al., 2018)
Sports Chiropractic Treatment
References
American Academy of Orthopaedic Surgeons. (2021). Turf toe.
American College of Foot and Ankle Surgeons. Foot Health Facts. (2023). RICE protocol.
Najefi, A. A., Jeyaseelan, L., & Welck, M. (2018). Turf toe: A clinical update. EFORT open reviews, 3(9), 501–506. https://doi.org/10.1302/2058-5241.3.180012
Pinter, Z. W., Farnell, C. G., Huntley, S., Patel, H. A., Peng, J., McMurtrie, J., Ray, J. L., Naranje, S., & Shah, A. B. (2020). Outcomes of Chronic Turf Toe Repair in Non-athlete Population: A Retrospective Study. Indian journal of orthopaedics, 54(1), 43–48. https://doi.org/10.1007/s43465-019-00010-8
Chinn, L., & Hertel, J. (2010). Rehabilitation of ankle and foot injuries in athletes. Clinics in sports medicine, 29(1), 157–167. https://doi.org/10.1016/j.csm.2009.09.006
Individuals in post-surgery recovery or dealing with illness or an injury can experience weakened muscles and endurance that can cause temporary loss of sleeping mobility and not being able to move around normally because of weakness, decreased range of motion, or pain. Can they benefit from physical therapy to help get back to normal functional mobility?
Sleeping Mobility
For individuals who are hospitalized or homebound from injury, illness, or surgical recovery, a physical therapist will assess various areas of functional mobility. These include transfers – from sitting to standing positions, walking, and sleeping mobility. Sleeping mobility is the ability to perform specific motions while in bed. A therapist can assess sleeping or bed mobility and recommend strategies and exercises to improve movements. (O’Sullivan, S. B., Schmitz, T. J. 2016) A therapist may have the individual use specific devices, like an over-the-bed trapeze or a sliding board, to help move around.
All of these movements require strength in different muscle groups. By checking out individual motions in sleeping mobility, a therapist can work out specific muscle groups that may be weak and require targeted exercises and stretches to restore mobility to normal. (O’Sullivan, S. B., Schmitz, T. J. 2016) Individuals visiting a therapist in an outpatient clinic or rehabilitation area may have the individual work on sleeping mobility on a treatment table. The same motions on the treatment table can be done in the bed.
Importance
The body is meant to move.
For individuals who cannot move comfortably on their bed, the body may suffer disuse atrophy or the wasting away of muscular strength, which can lead to increased difficulties. Not being able to move can also lead to pressure ulcers, especially for individuals who are severely deconditioned and/or remain in one position for a long period. Skin health may start to break down, leading to painful wounds that require specialized care. Being able to move around in bed can help prevent pressure ulcers. (Surajit Bhattacharya, R. K. Mishra. 2015)
Improvement
A physical therapist can prescribe specific exercises to strengthen muscle groups and improve sleeping mobility. The muscles include:
Shoulder and rotator cuff muscles.
Triceps and biceps in the arms.
Gluteus muscles of the hips.
Hamstrings
Quadriceps
Calf muscles
The shoulders, arms, hips, and legs work together when moving the body around the bed.
Various Exercises
To improve bed movement, physical therapy exercises can include:
Physical therapists are trained to assess these motions and functions and prescribe treatments to improve body movement. (O’Sullivan, S. B., Schmitz, T. J. 2016) Maintaining appropriate physical fitness can help the body stay active and mobile. Performing mobility exercises prescribed by a physical therapist can keep the right muscle groups working properly, and working with a physical therapist can ensure the exercises are correct for the condition and are performed properly.
Bhattacharya, S., & Mishra, R. K. (2015). Pressure ulcers: Current understanding and newer modalities of treatment. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India, 48(1), 4–16. https://doi.org/10.4103/0970-0358.155260
For individuals wanting to improve their fitness routine can incorporating wearable weights and knowing how to use them effectively help achieve health goals?
Wearable Weights
Adding wearable weights allows individuals to use their body weight with added resistance. This can add strength training to a routine but can also be used during walks or runs to increase cardiovascular health and aid in weight loss. Research studies have found that wearing a weighted vest reduces body weight and fat mass. This is because heavier loads increase energy expenditure for the increase in physical workload. (Claes Ohlsson, et al., 2020)
Benefits
Wearable weights are easy to use.
Depending on the type, they are compact and can be taken on the go.
Wearing weights is an option for individuals with injuries or degenerative joint disease like arthritis that makes it difficult to hold or move weights.
Because many are only a few pounds, they are available to anyone from adolescents to the elderly.
Anyone can benefit from the different types of wearable weights.
Types
Three main types of wearable weights include wrist weights, ankle weights, and weighted vests.
Wrist weights can replace dumbbells in some cases.
They are typically between 1 to 10 pounds.
Ankle weights can provide extra resistance to leg motions.
They can be found from 1 pound up to 20 pounds.
Weighted vests provide a full-body challenge.
The weight choices for them vary, as most contain pockets where weight can be increased or decreased.
Using The Weights
Individuals can use wearable weights as a complement to strength and cardiovascular regimens. Beginners will want to start with lighter weights worn for less time. As the body becomes stronger, it’s important to increase the weight to see results.
Ankle Weights
Ankle weights can be used during a strength training workout to add resistance to lower body exercises.
As the body ages, it becomes more important to decrease the risk of falls by increasing lower limb and trunk strength.
Wearing weights on the wrists generates a higher energy expenditure, which allows one to add intensity to a walk or run without having to increase speed. (Catherine T. Campaña, Pablo B Costa. 2017)
Weighted Vests
Wearing a weighted vest during workouts will create a full-body challenge.
They can be used while walking or running and automatically add more difficulty.
Another way to utilize a weighted vest is to wear it while completing a regular workout.
Whether doing HITT, strength training, etc, individuals can wear a weighted vest.
The weight should be evenly distributed to prevent any injuries or functional disorders to the lower body.
Individuals want to talk to a healthcare provider before beginning a new fitness program, and adding weights is no different, especially if there are any current or past injuries.
Is Motion Key To Healing?
References
Ohlsson, C., Gidestrand, E., Bellman, J., Larsson, C., Palsdottir, V., Hägg, D., Jansson, P. A., & Jansson, J. O. (2020). Increased weight loading reduces body weight and body fat in obese subjects – A proof of concept randomized clinical trial. EClinicalMedicine, 22, 100338. https://doi.org/10.1016/j.eclinm.2020.100338
Chen, L., & Yu, Y. (2020). Exercise and Osteoarthritis. Advances in experimental medicine and biology, 1228, 219–231. https://doi.org/10.1007/978-981-15-1792-1_15
Akatsu, H., Manabe, T., Kawade, Y., Masaki, Y., Hoshino, S., Jo, T., Kobayashi, S., Hayakawa, T., & Ohara, H. (2022). Effect of Ankle Weights as a Frailty Prevention Strategy in the Community-Dwelling Elderly: A Preliminary Report. International journal of environmental research and public health, 19(12), 7350. https://doi.org/10.3390/ijerph19127350
Yang, H. S., James, C. R., Atkins, L. T., Sawyer, S. F., Sizer, P. S., Jr, Kumar, N. A., & Kim, J. (2018). Effects of arm weight on gait performance in healthy subjects. Human movement science, 60, 40–47. https://doi.org/10.1016/j.humov.2018.05.003
Campaña, C. T., & Costa, P. B. (2017). Effects of walking with hand-held weights on energy expenditure and excess postexercise oxygen consumption. Journal of exercise rehabilitation, 13(6), 641–646. https://doi.org/10.12965/jer.1735100.550
Gaffney, C. J., Cunnington, J., Rattley, K., Wrench, E., Dyche, C., & Bampouras, T. M. (2022). Weighted vests in CrossFit increase physiological stress during walking and running without changes in spatiotemporal gait parameters. Ergonomics, 65(1), 147–158. https://doi.org/10.1080/00140139.2021.1961876
For individuals having difficulty moving or functioning normally due to injury, surgery, or illness, can a chiropractic and physical therapy team help expedite recovery?
Friction Massage
Individuals may develop scar tissue or tissue adhesions that limit normal motion after injury or surgery. A pain management team may use various treatments and modalities and may incorporate friction massage as part of a rehabilitation treatment plan. Friction massage, also known as transverse friction or cross friction massage, is a technique used to help improve scar tissue and adhesion mobility to move better and decrease the negative effects. The therapist uses their fingers to massage the scar in a direction that is at right angles to the scar line. It is a specialized technique that breaks up tissue adhesions that are limiting normal movement in the skin and underlying tissues. (Haris Begovic, et al., 2016)
Scar Tissue and Adhesions
For individuals who require surgery due to an injury or an orthopedic condition, their doctor will cut into the skin, tendons, and muscle tissue during the operation. Once sutured and healing has begun, scar tissue forms. Healthy tissue is made up of collagen that is comprised of cells that are arranged in a regular pattern. Healthy collagen is strong and can resist forces when tissues are pulled and stretched. (Paula Chaves, et al., 2017)
During the healing process after an injury, the collagen cells are laid down in a haphazard pattern and form scar tissue. The random accumulation of cells becomes tight and does not react well to tension and stretching forces. (Qing Chun, et al., 2016) The body can form scar tissue after a soft tissue injury, like a muscle or tendon strain. (Qing Chun, et al., 2016)
If a muscle or tendon gets strained the body will generate new collagen during the healing. The new collagen is laid down in a random fashion, and scar tissue or tissue adhesions can form that can limit the normal range of motion. Healthy tissue stretches and glides as the body moves. Scar tissue is rigid. At the site of the scar tissue, there can be some movement, but it is tight, less pliable, and can be painful. If scar tissue or adhesions are limiting motion, cross-friction massage can improve tissue gliding and sliding. This process is referred to as remodeling.
Massage Objectives
The objectives and goals of friction massage to adhesions or scar tissue may include:
Stimulation of nerve fibers to decrease and relieve pain.
The entire area of scar tissue or adhesion should be treated.
If the scar tissue is in a muscle, it should be relaxed.
If the scar tissue is in a tendon sheath, that tendon should be slightly stretched during the procedure.
The therapist places two or three fingers over the scar or adhesion and moves their fingers perpendicular to the scar to smooth the collagen fibers down.
The fingers and underlying tissues move together.
The massage should feel deep and uncomfortable but not painful.
There may be some pain, but should remain within the individual’s tolerance.
If the massage is too painful, less pressure may be used.
After several minutes the therapist will assess the tissue mobility.
Specific stretches may be done to elongate the scar tissue or adhesions.
At-home exercises and stretches may be prescribed to maintain flexibility.
Contraindications
There are situations where friction massage should not be used and can include: (Paula Chaves, et al., 2017)
Around an active open wound.
If there is a bacterial infection.
Areas with decreased sensation.
If calcification is present in the muscle or tendon tissue.
The therapist will explain the procedure and inform of the goals and risks associated with it.
Adhesive capsulitis in the shoulder/frozen shoulder.
Joint contracture.
Ligament tears.
Scar tissue buildup after surgery or trauma.
Friction massage is a popular technique used in physical therapy, but some research suggests it is not any more effective than other rehabilitation techniques. One study found that static stretches and exercises were more effective than massage in improving tissue length and strength in uninjured soccer players. Other studies have supported this, but individuals may find that the massage helps improve injured tissues’ movement as well. (Mohammed Ali Fakhro, et al. 2020)
The main goal of any treatment in physical therapy is to help the individual regain movement and flexibility. Friction massage, combined with targeted stretches and exercises, can help individuals expedite recovery and get back to normal.
Chiropractic Care After Accidents and Injuries
References
Begovic, H., Zhou, G. Q., Schuster, S., & Zheng, Y. P. (2016). The neuromotor effects of transverse friction massage. Manual therapy, 26, 70–76. https://doi.org/10.1016/j.math.2016.07.007
Chaves, P., Simões, D., Paço, M., Pinho, F., Duarte, J. A., & Ribeiro, F. (2017). Cyriax’s deep friction massage application parameters: Evidence from a cross-sectional study with physiotherapists. Musculoskeletal science & practice, 32, 92–97. https://doi.org/10.1016/j.msksp.2017.09.005
Chun, Q., ZhiYong, W., Fei, S., & XiQiao, W. (2016). Dynamic biological changes in fibroblasts during hypertrophic scar formation and regression. International wound journal, 13(2), 257–262. https://doi.org/10.1111/iwj.12283
Fakhro, M. A., Chahine, H., Srour, H., & Hijazi, K. (2020). Effect of deep transverse friction massage vs stretching on football players’ performance. World journal of orthopedics, 11(1), 47–56. https://doi.org/10.5312/wjo.v11.i1.47
Facet hypertrophy is an incurable, chronic disease that affects the facet joints in the spine. Can recognizing symptoms, help in diagnosis, and treatment?
Facet Hypertrophy
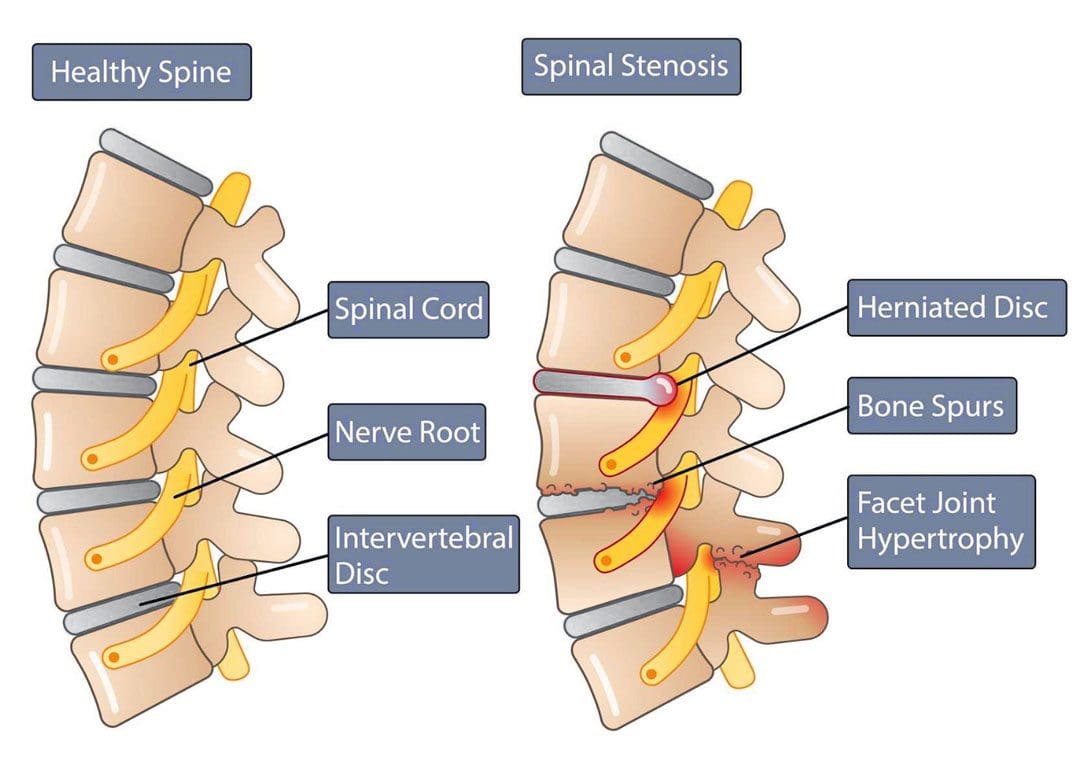
Facet hypertrophy causes the facet joints in the spine to enlarge. They are found where the vertebrae come into contact on the back of the vertebrae that form the backbone. These joints stabilize the spine when twisting and bending. Hypertrophy results when damage wears down the cartilage that cushions the bones that meet in the joint. This can include:
Aging
Wear and tear
Arthritis
Other joint diseases can damage facet joints.
Swelling, new bone growth, and bone spurs can occur as the joint tries to repair the damaged cartilage. The swelling and new bone growth can narrow the spinal canal and compress surrounding nerves, causing pain and other sensation symptoms. This ailment does not have a cure and worsens over time. The objective of treatment is to manage the pain symptoms and slow down the disease’s progress.
Types
Facet hypertrophy can be described as unilateral or bilateral.
Symptoms can have a wide range of intensity, from a dull ache to chronic, disabling pain. The location of symptoms depends on the affected joint and the nerves involved, Pain manifests when the enlarged joints and new bone growth compresses the nearby nerves. The result leads to nerve damage and the following symptoms: (Weill Cornell Medicine Brain & Spine Center. 2023) (Cedars Sinai. 2022)
Stiffness, especially when standing up or getting out of a chair.
Inability to stand straight when walking.
Inability to look up to the left or right without turning the whole body.
Reduced range of motion and mobility.
Numbness or a tingling sensation of pins and needles.
Radiating pain from the affected joint into the buttocks, hips, and upper thigh when the affected joint/s are in the lower back.
Radiating pain from the affected joint into the shoulder, neck, and back of the head when the affected joint/s are in the upper back.
Headaches when the affected joint is in the neck.
Causes
A common cause is the age-related degeneration of the joints, called spondylosis. Research indicates that more than 80% of individuals who are 40 or older have radiologic evidence of spondylosis, even though they may not have symptoms. (The University of Toledo Medical Center. N.D.) The following conditions can also increase the risk of facet hypertrophy (Weill Cornell Medicine Brain & Spine Center. 2023)
Unhealthy posture
Being overweight or obese
Sedentary lifestyle
Injury or trauma to the spine
Inflammatory conditions like rheumatoid arthritis or ankylosing spondylitis
Osteoarthritis
Genetic predisposition to the condition
Diagnosis
Diagnosis can be challenging when neck or back pain is the main complaint, as symptoms can mimic conditions such as sciatica from a herniated disc or hip arthritis. (Weill Cornell Medicine Brain & Spine Center. 2023)
A healthcare provider will conduct a complete physical examination, medical history, and discussion of symptoms.
CT scans with or without myelogram – the use of contrast dye in the space around the spinal cord.
MRI
X-rays with or without a myelogram
A diagnosis is confirmed by injecting a diagnostic block that involves administering an anesthetic injection, sometimes with an anti-inflammatory like cortisone, into the joint or nerves near the affected joint. Two injections are given at different times to confirm the effect. (Romain Perolat et al., 2018)
If immediate relief improves after each injection, the facet joint is confirmed as the source of the pain symptoms.
If the block does not decrease the pain, the facet joint is probably not the source of the pain symptoms. (Brigham and Women’s Hospital. 2023)
Treatment
There is no cure for facet hypertrophy.
The goal of treatment is to make the pain more manageable.
Conservative treatment is usually successful in making a difference.
Nonsteroidal anti-inflammatory – aspirin, ibuprofen, and naproxen.
Muscle relaxers – cyclobenzaprine or metaxalone.
Steroid injection into the facet joints.
Injection of platelet-rich plasma/PRP into the joints.
Medial Branch or Facet Block
A medial branch block injects local anesthetic near the medial nerves that connect to an inflamed joint.
Medial nerves are small nerves outside the joint space near the nerve that transmit signals and other impulses to the brain.
A facet block injects the medication outside the joint space near the nerve that supplies the joint called the medial branch.
Neurolysis
Neurolysis, also known as rhizotomy or neurotomy, is a procedure that destroys affected nerve fibers to relieve pain, reduce disability, and reduce the need for analgesics. This treatment can relieve pain for six to 12 months until the nerve regenerates, where further treatments may be necessary. (Matthew Smuck et al., 2012) Neurolysis can be performed using one of the following techniques (Romain Perolat et al., 2018)
Radiofrequency ablation RFA – the application of heat through radiofrequency.
Cryoneurolysis – the application of cold temperatures to the targeted nerve.
Chemical neurolysis – applying chemical agents, like a combination of phenol and alcohol.
Severing the nerves with surgical instrumentation.
Surgery
When one or more facet joints are severely damaged, they can become nonfunctional and painful. Surgery may be recommended when symptoms are not relieved by other therapies. (Ali Fahir Ozer, et al., 2015)
Prognosis
Facet hypertrophy is a chronic condition that progresses with age and does not affect life expectancy. (Weill Cornell Medicine Brain & Spine Center. 2023) The disorder is incurable, but symptoms can be managed with conservative therapies
A healthcare provider can help develop a treatment plan based on the extent and location of the joint affected.
Early diagnosis and treatment can help individuals achieve the best results.
Maintaining an active lifestyle and healthy weight can help prevent further joint stress. Individuals may be recommended to do regular stretching and strengthening exercises to lower inflammation, reduce stress, and improve overall health.
Facet Syndrome Treatment
References
Perolat, R., Kastler, A., Nicot, B., Pellat, J. M., Tahon, F., Attye, A., Heck, O., Boubagra, K., Grand, S., & Krainik, A. (2018). Facet joint syndrome: from diagnosis to interventional management. Insights into imaging, 9(5), 773–789. https://doi.org/10.1007/s13244-018-0638-x
Smuck, M., Crisostomo, R. A., Trivedi, K., & Agrawal, D. (2012). Success of initial and repeated medial branch neurotomy for zygapophysial joint pain: a systematic review. PM & R : the journal of injury, function, and rehabilitation, 4(9), 686–692. https://doi.org/10.1016/j.pmrj.2012.06.007
Ozer, A. F., Suzer, T., Sasani, M., Oktenoglu, T., Cezayirli, P., Marandi, H. J., & Erbulut, D. U. (2015). Simple facet joint repair with dynamic pedicular system: Technical note and case series. Journal of craniovertebral junction & spine, 6(2), 65–68. https://doi.org/10.4103/0974-8237.156049
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine