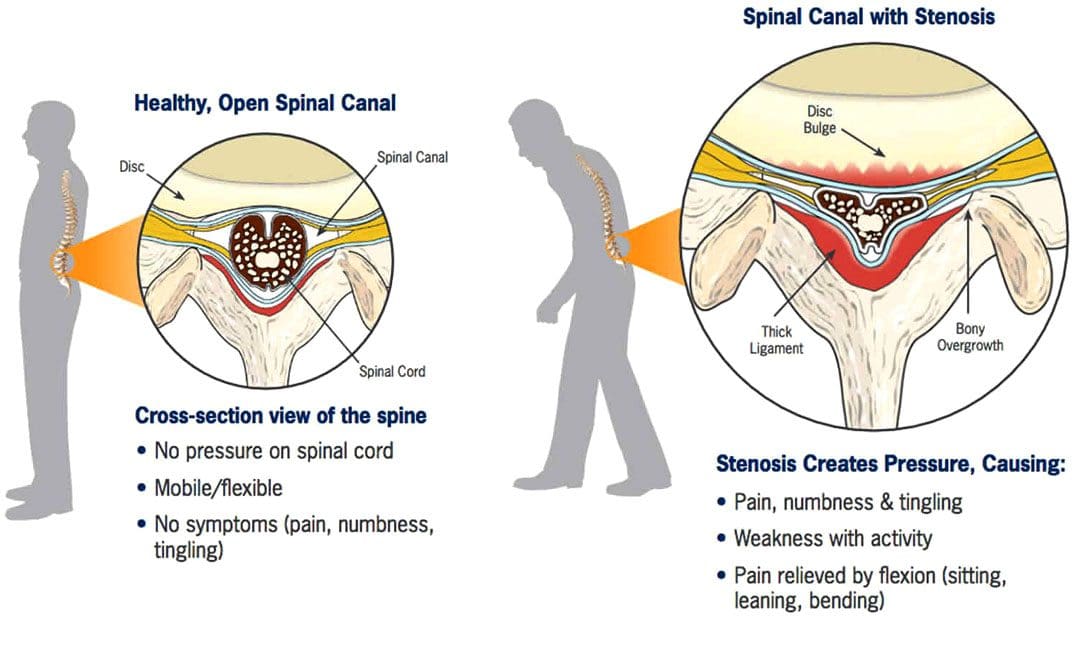
The discs between the spine’s vertebrae provide cushioning and shock absorption in the spine and the rest of the body. Degenerative changes to the discs are believed to be the start of spinal stenosis. When the discs lack sufficient hydration/water and disc height decreases over time, the cushioning and shock absorption becomes less and less effective. The vertebrae can then become compressed, causing friction. Degenerative spinal stenosis can also develop from excess scar tissue and bone spurs (growth that develops on the edge of a bone) that can form after injury or spinal surgery.
Assessment
A physician will make a diagnosis of spinal stenosis. The doctor will take an imaging scan of the spine to determine the exact location of the degeneration and to measure how narrow the openings have become. Pain, stiffness, limited mobility, and loss of range of motion are often present. If spinal stenosis has caused nerve compression, there may also be pain, numbness, tingling, or weakness in the buttocks (sciatica), thighs, and lower legs. A physical therapist will determine the degree by assessing the following:
Vertebrae mobility – how the spine bends and twists in different directions.
Ability to change positions.
The strength of the core, back, and hip muscles.
Balance
Posture
Gait pattern
Nerve compression to determine if there are any symptoms in the legs.
Milder cases usually do not involve nerve compression, as back stiffness is more common.
In more severe cases, there may be significant pain, limited mobility, and nerve compression, causing leg weakness.
The most common symptom of spinal stenosis is increased pain with backward bending or extension of the lumbar spine. This includes positions that extend the spine, such as standing, walking, and lying on the stomach. Symptoms usually improve when bending forward and when the spine is positioned more into a flexed or bent position, like when sitting and reclining. These body positions open up the spaces in the central spinal canal.
Surgery
Spinal stenosis is the most common reason for undergoing surgery in adults 65 and older. However, surgery is almost always performed as a last resort if pain, symptoms, and disability persist after trying conservative therapies, including chiropractic, non-surgical decompression, and physical therapy, for months or years. The severity of symptoms and current state of health will determine whether a doctor will recommend surgery. (Zhuomao Mo, et al., 2018). Conservative measures can be safer and just as effective. A systematic review or study based on all available primary research found that physical therapy and exercise resulted in similar outcomes to surgery for improving pain and disability. (Zhuomao Mo, et al., 2018). Except for severe cases, surgery is often not necessary.
Physical Therapy for Spinal Stenosis
The objective of physical therapy includes:
Decreasing pain and joint stiffness.
Relieving nerve compression.
Reducing tightness in the surrounding muscles.
Improving the range of motion.
Improving postural alignment.
Strengthening the core muscles.
Improving leg strength to help with balance and overall function.
Stretching of the back muscles, including those running vertically along the spine and those running diagonally from the pelvis to the lumbar spine, helps relieve muscle tightness and pain and can improve overall mobility and range of motion of the lumbar spine.
Stretching the hip muscles, including the hip flexors in the front, the piriformis in the back, and the hamstrings that run from the back of the hip down the leg to the knee, is also important as these muscles are attached to the pelvis, which directly connects to the spine.
Exercises for strengthening the abdominal core muscles, including the muscles in the trunk, pelvis, lower back, hips, and abdomen, help stabilize the spine and protect it from excessive movement and compressive forces.
With spinal stenosis, the core muscles often become weak and inactive and unable to do their job to support the spine. Core exercises often begin by activating the deep abdominal muscles while lying flat on the back with the knees bent.
Exercises will progress as the individual gains more strength and control as the spine stabilizes.
Spinal stenosis physical therapy will also involve balance training and glute exercises for strengthening the leg muscles.
Prevention
Working with a physical therapist can help prevent future problems by maintaining spinal mobility, keeping the individual active, and exercising to maintain strength and stability to provide a solid foundation to support the lower back and prevent symptoms from worsening.
Severe Spinal Stenosis Physical Therapy
Physical therapy usually involves performing stretches for the lower back, hips, and legs, mobility exercises, and core strengthening exercises to improve spinal support and decrease pain. Treatments like heat or electrical stimulation may also be used on a case-by-case basis if there is significant pain or tightness in the back muscles. However, there is not enough clinical evidence to support that there are additional benefits. (Luciana Gazzi Macedo, et al., 2013) The effectiveness of physical therapy is high because surgery alone cannot strengthen the muscles that stabilize the spine, increase the mobility or flexibility of the surrounding muscles, and improve postural alignment.
The Root Causes of Spinal Stenosis
References
Lurie, J., & Tomkins-Lane, C. (2016). Management of lumbar spinal stenosis. BMJ (Clinical research ed.), 352, h6234. https://doi.org/10.1136/bmj.h6234
Mo, Z., Zhang, R., Chang, M., & Tang, S. (2018). Exercise therapy versus surgery for lumbar spinal stenosis: A systematic review and meta-analysis. Pakistan journal of medical sciences, 34(4), 879–885. https://doi.org/10.12669/pjms.344.14349
Macedo, L. G., Hum, A., Kuleba, L., Mo, J., Truong, L., Yeung, M., & Battié, M. C. (2013). Physical therapy interventions for degenerative lumbar spinal stenosis: a systematic review. Physical therapy, 93(12), 1646–1660. https://doi.org/10.2522/ptj.20120379
For individuals trying to maintain a healthy spine, can understanding the causes and prevention of rotated vertebrae help protect the spine from harmful rotation of vertebrae?
Spinal Rotation
Healthy spine rotation is an important aspect of injury prevention, and rotated vertebrae or a twisted spine can result from spine, nerve, or muscle disease or certain movements.
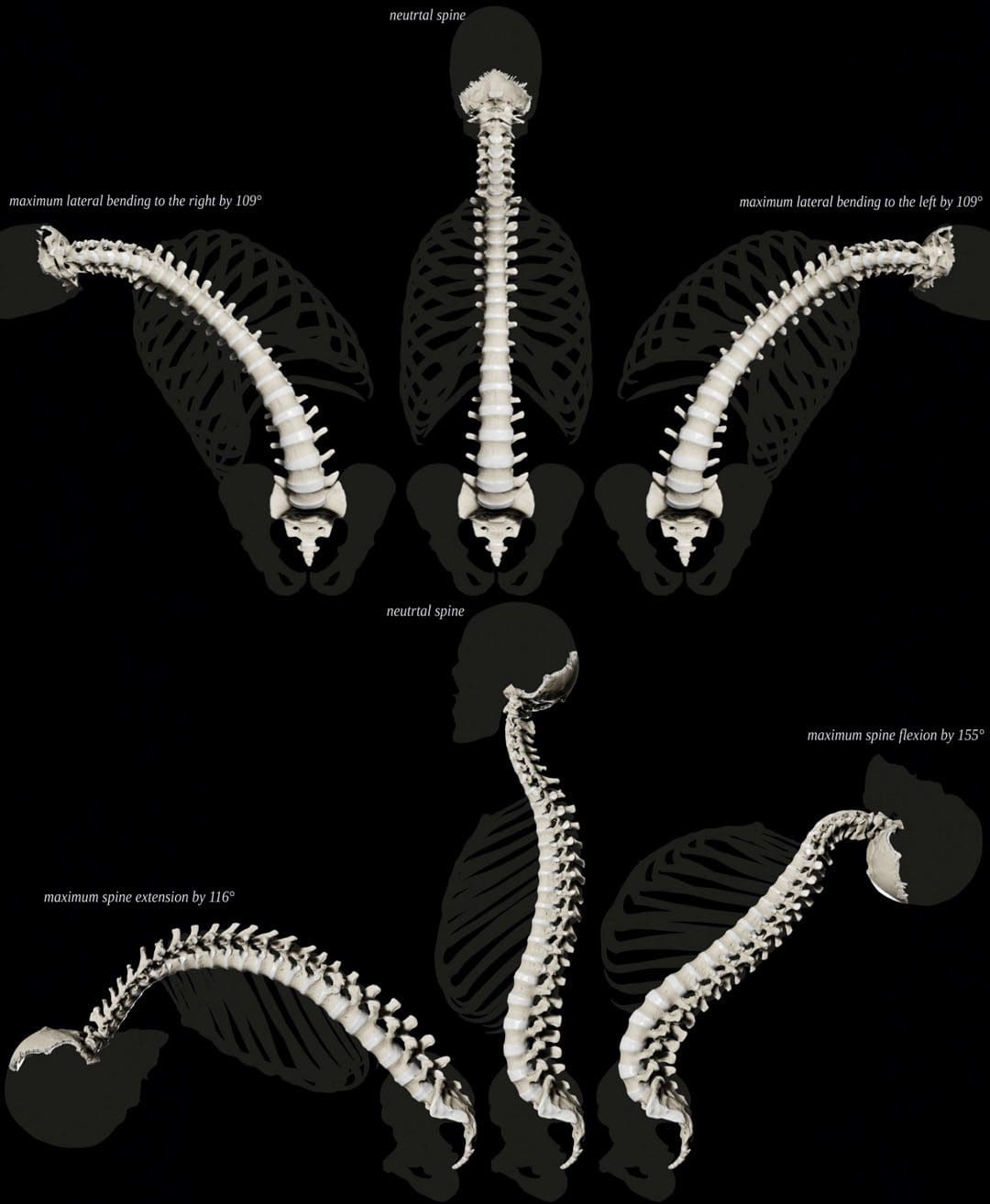
Normal Spine Twisting Capability
The spine can move in several ways. Spine movements include:
Bending – Rounding forward
Extending – Arching backward
Tilting sideways is powered by muscles that aid in twisting.
Although the spine can move in many directions, there are limits to how far it can and should go. (Xinhai Shan et al., 2013). This is especially true with twisting. The spinal column is made of 26 interconnected bones called vertebrae. When moving, each vertebrae bone moves accordingly. Rotated or twisted vertebrae, especially when bending forward like lifting heavy objects, are associated with a risk of back injuries like strain and herniated discs.
How Rotation Works
Rotation is a basic movement in which individuals can turn their spinal column. When twisting, the spine also bends to the side. The muscles involved in spine rotation include:
The internal oblique abdominals and the external oblique abdominals don’t directly attach to the spine but are the primary muscles responsible for powering spinal rotation in the lower back.
Intrinsic muscles, including the multifidus and longissimus, contribute to twisting movement as well.
The multifidus helps the spine twist when one side is contracted/activated and extends the lumbar spine when both sides contract.
The multifidus helps control the movement, and the longissimus provides the movement with some extension.
Age and The Spine
As individuals age, the body accumulates tension and/or weakness in the oblique abdominal and other trunk muscles. Sedentary habits primarily bring on these changes. (Pooriput Waongenngarm et al., 2016)
Chronically tight back and abdominal muscles impair the range of motion of the trunk, as well as twisting ability.
Muscle weakness and tightness affect spinal movements.
Weakened muscles can decrease support for spinal movement and decrease overall trunk stability.
Spinal Rotation and Scoliosis
Scoliosis is a common condition that causes a lateral curve of the spine. Some of the vertebrae become displaced to the side. Often, abnormal vertebral rotation underlies this displacement. Treatment often focuses on controlling vertebral rotation with medical guidance and physical therapy. (John P. Horne et al., 2014)
Over-Rotating The Spine
Many individuals over-rotate their spines with manual work, which can increase the risk of back injuries. (National Institutes of Health. 2020). Over-rotation can happen with activities like digging or shoveling.
Exercise For A Healthy Spine
A recommended way to achieve optimal rotation of the spine is with daily back exercises. (National Spine Health Foundation. 2015). An effective back exercise program will consist of movements in every direction.
Yoga is recommended because it places emphasis on developing flexibility and strength in all directions.
Pilates does the same.
An injury prevention exercise program will work the hip and pelvic muscles as well.
Individuals with a spine condition should consult their healthcare provider or physical therapist about how to exercise the spine safely, as rotation exercises could worsen back problems like bulging or herniated discs.
Core Strength For A Pain-Free Back
References
Shan, X., Ning, X., Chen, Z., Ding, M., Shi, W., & Yang, S. (2013). Low back pain development response to sustained trunk axial twisting. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 22(9), 1972–1978. https://doi.org/10.1007/s00586-013-2784-7
Waongenngarm, P., Rajaratnam, B. S., & Janwantanakul, P. (2016). Internal Oblique and Transversus Abdominis Muscle Fatigue Induced by Slumped Sitting Posture after 1 Hour of Sitting in Office Workers. Safety and health at work, 7(1), 49–54. https://doi.org/10.1016/j.shaw.2015.08.001
For individuals into sports, fitness enthusiasts, and those that engage in physical activities, musculoskeletal injuries are common. Can using ice tape help during the initial or acute phase of injury decrease inflammation and swelling to expedite recovery and return to activities sooner?
Ice Tape
After a musculoskeletal injury, individuals are recommended to follow the R.I.C.E. method to help reduce swelling and inflammation. R.I.C.E. is the acronym for Rest, Ice, Compression, and Elevation. (Michigan Medicine. University of Michigan. 2023) The cold helps to decrease pain, lower tissue temperature, and decrease swelling around the site of the injury. By controlling the inflammation with ice and compression early after injury, individuals can maintain the appropriate range of motion and mobility around the injured body part. (Jon E. Block. 2010) There are different ways to apply ice to an injury.
Store-bought ice bags and cold packs.
Soaking the injured body part in a cold whirlpool or tub.
Making reusable ice packs.
A compression bandage can be used together with the ice.
Ice Tape is a compression bandage that provides cold therapy all at once. After an injury, applying it can help decrease the pain and swelling during the acute inflammatory phase of healing. (Matthew J. Kraeutler et al., 2015)
How The Tape Works
The tape is a flexible bandage that is infused with therapeutic cooling gel. When applied to an injured body part and exposed to air, the gel activates, generating a cold sensation around the area. The therapeutic medicinal effect can last five to six hours. Combined with a flexible bandage, it provides ice therapy and compression. The ice tape can be used straight out of the package but can also be stored in the refrigerator to increase the cold effect. Depending on the maker’s instructions, the tape should not be stored in the freezer as this can make it too hard to wrap around the injured area.
Advantages
The benefits include the following:
Easy to Use
The product is easy to use.
Take out the tape, and start wrapping it around the injured body part.
Fasteners Not Required
The wrap sticks to itself, so the tape stays in place without using clips or fasteners.
Easy to Cut
The standard roll is 48 inches long by 2 inches wide.
Most injuries require enough to wrap around the injured area.
Scissors cut the exact amount needed, and store the rest in the resealable bag.
Reusable
After 15 to 20 minutes of application, the product can be easily removed, rolled up, stored in the bag, and used again.
The tape can be used multiple times.
The tape begins to lose its cooling quality after several uses.
Portable
The tape does not need to be placed in a cooler when traveling.
It is easily portable and perfect for a quick ice and compression application immediately after an injury.
It can decrease pain and inflammation and kept at the workplace.
Disadvantages
A few disadvantages include the following:
Chemical Odor
The gel on the flexible wrap can have a medicine odor.
It is not quite as powerful smelling as pain creams, but the chemical odor could bother some individuals.
Might Not Be Cold Enough
The tape works for immediate pain relief and inflammation, but it may not get cold enough for the user when applied right from the package at room temperature.
However, it can be placed in a refrigerator to increase the coldness and may provide a more therapeutic cooling effect, especially for those dealing with tendinitis or bursitis.
Stickiness Could Be Distracting
The tape could be a bit sticky for some.
This sticky factor can be a minor annoyance.
However, it just feels sticky when being applied.
A couple of flecks of the gel may get left behind when removed.
The ice tape can also stick to clothing.
For individuals looking for a quick, on-the-go cooling therapy for injured or aching body parts, ice tape may be an option. It could be good to have on hand to provide cooling compression if a minor injury occurs while participating in athletics or physical activities and relief for overuse or repetitive strain injuries.
Block J. E. (2010). Cold and compression in the management of musculoskeletal injuries and orthopedic operative procedures: a narrative review. Open access journal of sports medicine, 1, 105–113. https://doi.org/10.2147/oajsm.s11102
Kraeutler, M. J., Reynolds, K. A., Long, C., & McCarty, E. C. (2015). Compressive cryotherapy versus ice-a prospective, randomized study on postoperative pain in patients undergoing arthroscopic rotator cuff repair or subacromial decompression. Journal of shoulder and elbow surgery, 24(6), 854–859. https://doi.org/10.1016/j.jse.2015.02.004
For individuals experiencing tightness in the lower back and hamstrings, can utilizing the sit and reach test help determine an individual’s risk for future pain and injury?
Sit and Reach Test
Lower back and hamstring tightness and pain symptoms are usually brought on by muscle stiffness. The sit-and-reach test is one of the most common ways to measure lower back and hamstring flexibility. Exercise physiologists, physical therapists, chiropractors, and fitness trainers use the sit-and-reach test to measure lower back and hamstring flexibility to assess baseline flexibility. The test has been around since 1952 (Katharine F. Wells & Evelyn K. Dillon 2013) and has an extensive database of results across all age groups and genders.
Individuals can use the sit-and-reach test to compare flexibility to the average result for individuals of the same gender and age.
For healthcare providers, the test may be repeated after several weeks to determine flexibility progress.
Measurement
The test can be a valuable measurement of functional flexibility to sit with the legs straight in front and reach the toes. Jobs, sports, and everyday tasks regularly require bending over, reaching, and lifting objects. These are real-life examples of how having a healthy back and hamstring flexibility is vital in preventing pain symptoms and injuries. New flexibility assessments are currently being developed, and many trainers and therapists use their own versions with patients and clients. But even with more advanced specialized flexibility tests, the sit and reach test can be a functional testing tool for tracking general flexibility changes over time. (Daniel Mayorga-Vega et al., 2014)
Performing The Test
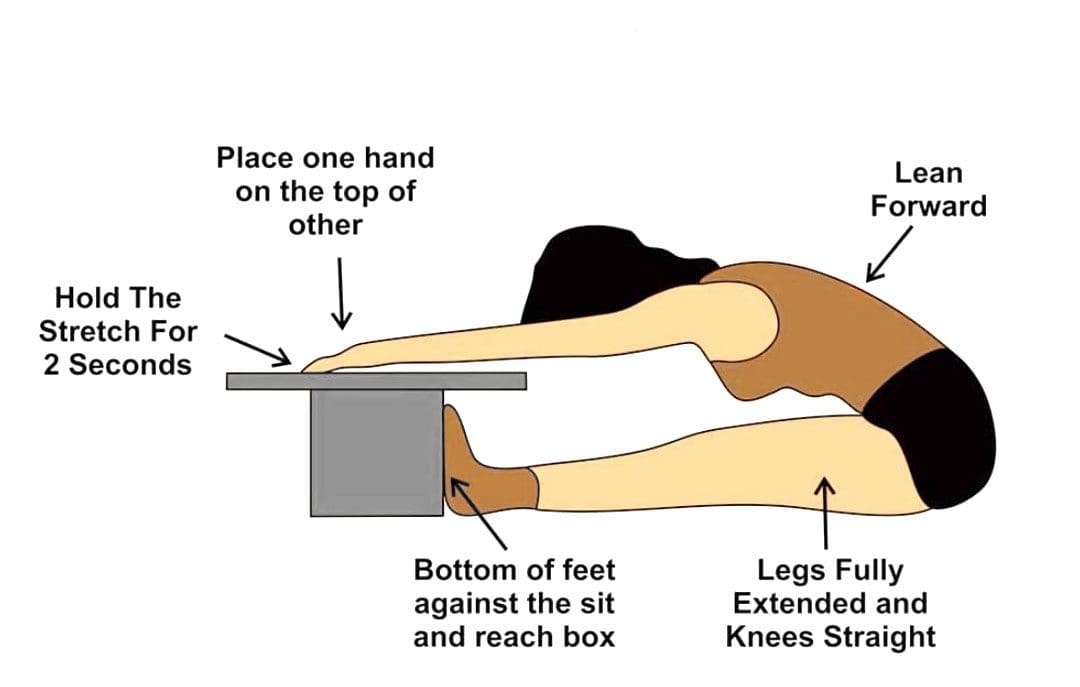
A special sit-and-reach testing box is used; however, individuals can make their own testing box by finding a heavy-duty box around 30cm or 11.811 inches tall. Set a measurement ruler/stick on top of the box so that 26 cm or 10.2362 inches of the ruler extends over the front edge toward the individual being tested. The 26cm mark should be at the edge of the box.
Get into position – Remove shoes and sit on the floor with legs stretched out in front with the knees straight and feet flat against the front end of the test box.
Start the movement – In a slow, steady motion, lean forward, keeping the knees straight, and slide the hands up the ruler as far as possible.
Stretch and repeat – Extend as far as possible, record the results, rest, and repeat three times.
Calculate the results – Average the results.
Results
Results compare flexibility over time to norms, or averages, for gender and age. Adequate flexibility is reaching the toes – the 26-cm mark on the ruler while keeping the legs straight.
Adult Women
37cm or 14.5669 inches or above: Excellent
33 to 36cm or 12.9921 inches: Above average
29 to 32cm or 11.4173 inches: Average
23 to 28cm or 9.05512 inches: Below average
Below 23cm or 8.66142 inches: Poor
Adult Men
34cm or 13.3858 inches or above: Excellent
28 to 33cm or 11.0236 inches: Above average
23 to 27cm or 9.05512 inches: Average
16 to 22cm or 6.29921 inches: Below average
Below 16cm or 5.90551 inches: Poor
Alternatives
Individuals can test their own hamstring and lower back flexibility with some easy at-home tests. Use these methods while working on flexibility, and keep a record to see improvements. (Brittany L. Hansberger et al., 2019) One alternative is the V-sit reach test.
To perform this, make a line on the floor with tape, then place a measuring tape perpendicular to the tape, making a cross.
Sit with the feet in a V shape, touching the tape, feet about a foot apart, with the measuring tape between the legs; the 0 end starts where the legs part.
Overlap hands with arms outstretched in front.
Repeat three times, leaning forward and reaching with hands out.
Then, repeat and take note of how far the hands could reach.
Individuals will need someone to measure the distance between their fingertips and the floor.
Warm up with a few practice stretches of standing and bending toward the floor.
Then, measure how far from the floor the fingertips are.
The ability to touch the floor is a good sign.
Improving Flexibility
Individuals with less than adequate flexibility are recommended to work on stretching the major muscle groups in both the upper and lower body on a regular basis to improve and maintain body flexibility.
Individuals can incorporate dynamic stretching, which consists of active movements utilizing a full range of motion as part of warming up for workouts, sports, or other activities.
Static stretching is recommended when cooling down after the muscles are warmed up and joints are lubricated.
The American College of Sports Medicine recommends 2 to 3 sessions a week of flexibility training and learning to stretch daily.
Stretches should be held for 15 to 30 seconds, then released and repeated 2 to 4 times. (Phil Page 2012)
This will take time and dedication, but with the help of trained specialists, regaining flexibility and full range of motion can be accomplished.
Benefits of Stretching
References
Katharine F. Wells & Evelyn K. Dillon (1952) The Sit and Reach—A Test of Back and Leg Flexibility, Research Quarterly. American Association for Health, Physical Education and Recreation, 23:1, 115-118, DOI: 10.1080/10671188.1952.10761965
Mayorga-Vega, D., Merino-Marban, R., & Viciana, J. (2014). Criterion-Related Validity of Sit-and-Reach Tests for Estimating Hamstring and Lumbar Extensibility: a Meta-Analysis. Journal of sports science & medicine, 13(1), 1–14.
Hansberger, B. L., Loutsch, R., Hancock, C., Bonser, R., Zeigel, A., & Baker, R. T. (2019). EVALUATING THE RELATIONSHIP BETWEEN CLINICAL ASSESSMENTS OF APPARENT HAMSTRING TIGHTNESS: A CORRELATIONAL ANALYSIS. International journal of sports physical therapy, 14(2), 253–263.
Page P. (2012). Current concepts in muscle stretching for exercise and rehabilitation. International journal of sports physical therapy, 7(1), 109–119.
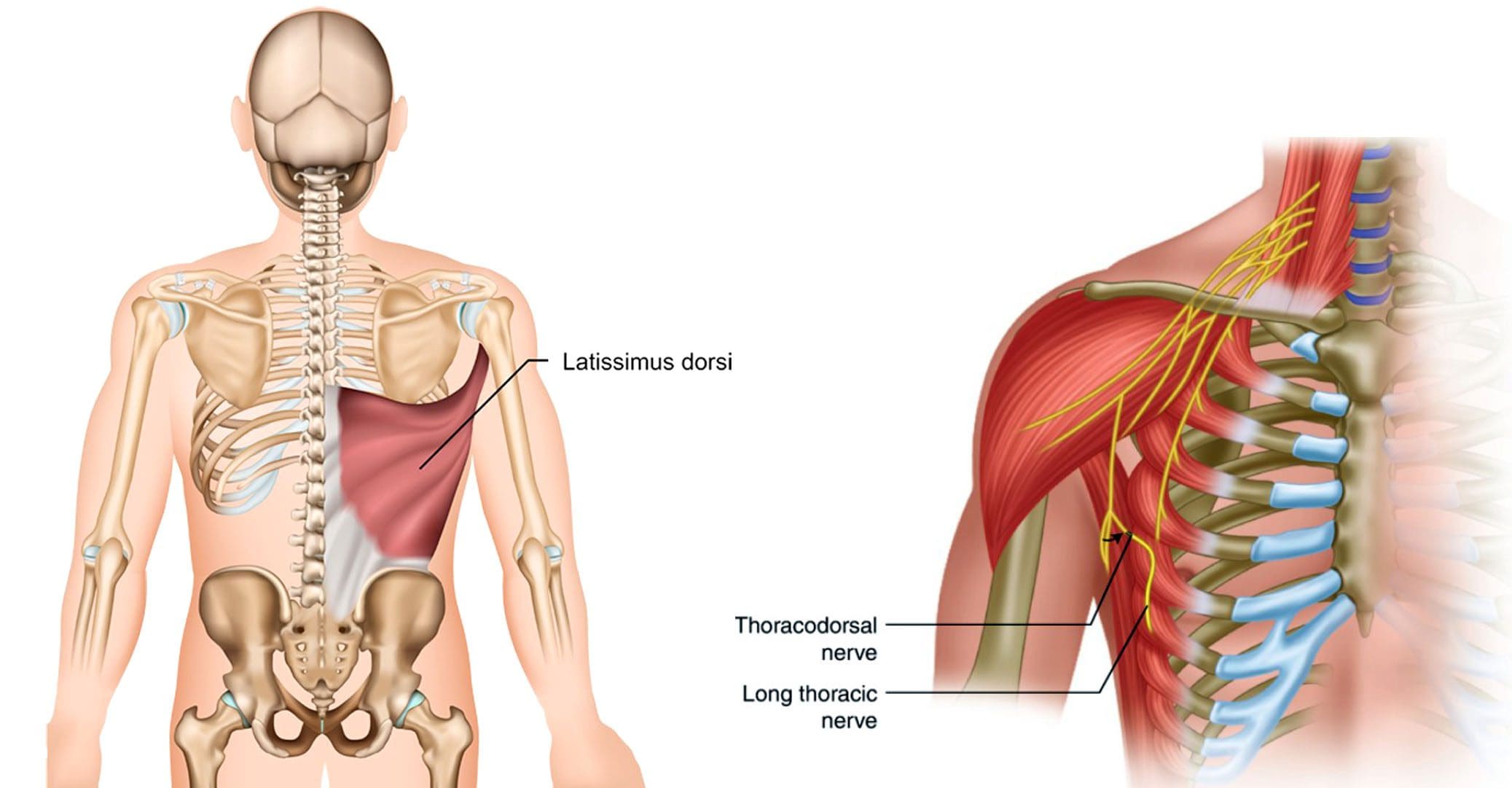
Individuals experiencing pain symptoms like shooting, stabbing, or electrical sensations to the latissimus dorsi of the upper back could be caused by a nerve injury to the thoracodorsal nerve. Can knowing the anatomy and symptoms help healthcare providers develop an effective treatment plan?
Thoracodorsal Nerve
Also known as the middle subscapular nerve or the long subscapular nerve, it branches out from a part of the brachial plexus and provides motor innervation/function to the latissimus dorsi muscle.
Anatomy
The brachial plexus is a network of nerves that stem from the spinal cord in the neck. The nerves supply most of the sensation and movement of the arms and hands, with one on each side. Its five roots come from the spaces between the fifth through eighth cervical vertebrae and the first thoracic vertebra. From there, they form a larger structure, then divide, re-combine, and divide again to form smaller nerves and nerve structures as they travel down the armpit. Through the neck and chest, the nerves eventually join and form three cords that include:
Lateral cord
Medial cord
Posterior cord
The posterior cord produces major and minor branches that include:
Axillary nerve
Radial nerve
The minor branches include:
Superior subscapular nerve
Inferior subscapular nerve
Thoracodorsal nerve
Structure and Position
The thoracodorsal nerve branches off the posterior cord in the armpit and travels down, following the subscapular artery, to the latissimus dorsi muscle.
It connects to the upper arm, stretches across the back of the armpit, forming the axillary arch, and then expands into a large triangle that wraps around the ribs and the back.
The thoracodorsal nerve lies deep in the latissimus dorsi, and the lower edge typically reaches close to the waist.
Variations
There is a standard location and course of the thoracodorsal nerve, but individual nerves are not the same in everyone.
The nerve typically branches off the posterior cord of the brachial plexus from three different points.
The lats can have a rare anatomical variation known as a Langer’s arch, which is an extra part that connects to muscles or connective tissue of the upper arm beneath the common connecting point.
In individuals with this abnormality, the thoracodorsal nerve supplies function/innervation) to the arch. (Ahmed M. Al Maksoud et al., 2015)
Function
The latissimus dorsi muscle cannot function without the thoracodorsal nerve. The muscle and nerve help:
Stabilize the back.
Pull the body weight up when climbing, swimming, or doing pull-ups.
Assist with breathing by expanding the rib cage during inhalation and contracting when exhaling. (Encyclopaedia Britannica. 2023)
Rotate the arm inward.
Pull the arm toward the center of the body.
Extend the shoulders by working with the teres major, teres minor, and posterior deltoid muscles.
Bring down the shoulder girdle by arching the spine.
Pain that can be shooting, stabbing, or electrical sensations.
Numbness, tingling.
Weakness and loss of function in the associated muscles and body parts, including wrist and finger drop.
Because of the nerve’s path through the armpit, doctors have to be cautious of the anatomical variants so they don’t inadvertently damage a nerve during breast cancer procedures, including axillary dissection.
The procedure is performed to examine or remove lymph nodes and is used in staging breast cancer and in treatment.
According to a study, 11% of individuals with axillary lymph node dissection suffered damage to the nerve. (Roser Belmonte et al., 2015)
Breast Reconstruction
In breast reconstruction surgery, the lats can be used as a flap over the implant.
Depending on the circumstances, the thoracodorsal nerve can be left intact or severed.
There is some evidence that leaving the nerve intact can cause the muscle to contract and dislocate the implant.
An intact thoracodorsal nerve may also cause atrophy of the muscle, which can lead to shoulder and arm weakness.
Graft Uses
A portion of the thoracodorsal nerve is commonly used in nerve graft reconstruction to restore function after injury, which includes the following:
Musculocutaneous nerve
Accessory nerve
Axillary nerve
The nerve can also be used to restore nerve function to the triceps muscle in the arm.
Rehabilitation
If the thoracodorsal nerve is injured or damaged, treatments can include:
Braces or splints.
Physical therapy to improve range of motion, flexibility, and muscle strength.
If there is compression, surgery may be required to alleviate the pressure.
Exploring Integrative Medicine
References
Chu B, Bordoni B. Anatomy, Thorax, Thoracodorsal Nerves. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539761/
Al Maksoud, A. M., Barsoum, A. K., & Moneer, M. M. (2015). Langer’s arch: a rare anomaly affects axillary lymphadenectomy. Journal of surgical case reports, 2015(12), rjv159. https://doi.org/10.1093/jscr/rjv159
Britannica, The Editors of Encyclopaedia. “latissimus dorsi“. Encyclopedia Britannica, 30 Nov. 2023, https://www.britannica.com/science/latissimus-dorsi. Accessed 2 January 2024.
Belmonte, R., Monleon, S., Bofill, N., Alvarado, M. L., Espadaler, J., & Royo, I. (2015). Long thoracic nerve injury in breast cancer patients treated with axillary lymph node dissection. Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer, 23(1), 169–175. https://doi.org/10.1007/s00520-014-2338-5
Kwon, S. T., Chang, H., & Oh, M. (2011). Anatomic basis of interfascicular nerve splitting of innervated partial latissimus dorsi muscle flap. Journal of plastic, reconstructive & aesthetic surgery : JPRAS, 64(5), e109–e114. https://doi.org/10.1016/j.bjps.2010.12.008
A dislocated elbow is a common injury in adults and children and often happens in tandem with bone fractures and nerve and tissue damage. Can physical therapy help to support recovery and ensure range of motion?
Dislocated Elbow Injury
Elbow dislocations are generally caused by trauma when the elbow bones no longer connect. Individuals falling onto an outstretched hand is the most common cause of the injury. (James Layson, Ben J. Best 2023) Healthcare providers will try to relocate the elbow using a closed reduction. Individuals may require surgery if they cannot relocate the elbow using closed reduction.
The hinge function allows the bending and straightening of the arm.
Ball-and-socket joint
The ball-and-socket function allows you to rotate the palm of your hand to face up or face down.
A dislocated elbow injury can damage bones, muscles, ligaments, and tissues. (American Academy of Orthopaedic Surgeons. 2021) The longer the elbow remains out of the joint, the more damage can occur. Elbow dislocations rarely reset into their joints on their own and are recommended to be evaluated by a qualified healthcare provider to prevent permanent damage to nerves or function.
It is not recommended to try to reset the elbow on your own.
A healthcare provider will work to restore the joint and ensure proper alignment.
Before the reset, they will perform a physical examination to assess blood circulation and any nerve damage.
A closed reduction means that the elbow can be relocated without surgery.
Before the closed reduction, a healthcare provider will administer medications to help relax the individual and address the pain. (Medline Plus. 2022)
Once relocated into the correct position, a healthcare provider applies a splint (usually at a 90-degree angle of flexion) to keep the elbow in place. (James Layson, Ben J. Best 2023)
The objective is to prevent elbow extension, which can cause re-dislocation.
Progress can be challenging for individuals in post total ankle replacement surgery. How can physical therapy help in recovery and restoring leg function?
Total Ankle Replacement Post Surgery Physical Therapy
Total ankle replacement surgery is a major procedure that takes time to recover. A total ankle replacement surgery or arthroplasty can benefit individuals with chronic ankle pain or disability. This procedure can significantly improve an individual’s overall pain and function with time. Physical therapy is essential to regaining movement in the ankle and restoring full mobility. A physical therapist will work with the individual to control pain and swelling, restore the ankle’s range of motion, train on walking gait and balance, and rebuild strength in the leg. This will help maximize the chances of a successful outcome after surgery.
Total Ankle Replacement
The ankle joint is the section of the lower leg where the shinbone/tibia meets the talus bone on the top of the foot. What can happen is the slippery surface/articular cartilage that coats the ends of these bones begins to thin or deteriorate. As the deterioration progresses, it can lead to significant pain, disability, and difficulty walking. (Cleveland Clinic. 2021) This is where a specialist may recommend total ankle replacement for the best results. Various conditions can be helped by this procedure, including:
During an ankle replacement procedure, an orthopedic surgeon removes the damaged ends of the tibia and talus bones and replaces them with an artificial covering. A polyethylene component is also secured between the two structures to support the smooth movement of the new joint endings. (Massachusetts General Hospital. N.D.) Following the procedure, individuals are typically placed in a protective boot or splint. The healthcare provider will recommend staying off the leg for 4 to 8 weeks to allow healing.
Physical Therapy
Outpatient physical therapy is usually initiated several weeks after the ankle operation. (UW Health Orthopedics and Rehabilitation. 2018) Physical therapy can last for five months or more, depending on the severity of the condition and injury. The physical therapist will focus on different areas to get the best results. (Cort D. Lawton et al., 2017)
Pain and Swelling Control
Post-operative pain and swelling are normal after a total ankle replacement. It is not unusual for an ankle to be swollen for even six to 12 months after the operation. (UW Health Orthopedics and Rehabilitation. 2018) The surgeon will normally prescribe medication to help manage discomfort early on, and physical therapy also plays an important role in addressing the symptoms. Treatments used can include:
Electrical stimulation – mild electrical pulses applied to the muscles.
Ice
Vasopneumatic compression, where an inflatable sleeve is used to create pressure around the area, is commonly utilized at the beginning of physical therapy to reduce pain or swelling.
Other modalities, such as stretching and targeted exercises, are combined with other treatments.
Range of Motion
Early after the procedure, the ankle will be very stiff and tight. This is due to several factors, including the inflammation and swelling after surgery and the time spent immobilized in a boot.
The physical therapist will employ various techniques to improve the ankle joint’s range of motion to rotate and flex.
The physical therapist may employ passive stretching induced by an outside force such as the therapist or a resistance band) to help improve mobility.
After multiple weeks of reduced movement and lack of bearing any weight on the ankle, the muscles that surround the ankle have often atrophied/weakened, which can impact balance.
When the individual can begin placing weight on the leg, the therapist will apply proprioceptive/sense of body position training to improve overall stability. (UW Health Orthopedics and Rehabilitation. 2018)
Balance exercises will be added to the home program and will progress from week to week.
Strength
The muscles in the leg, ankle, and foot become weak from the surgery and the time spent in a splint or boot. These structures have a significant role in balance, the ability to stand, walk, and go up or down the stairs.
Regaining the strength and power of these muscles is a critical goal of rehabilitation.
In the first weeks, the physical therapist will focus on gentle strengthening exercises.
Isometrics lightly activate the muscles but avoid irritating the surgical site.
As time passes and weight-bearing is allowed, these gentle moves are replaced with more challenging ones, like resistance bands and standing exercises, to accelerate strength gains.
Lawton, C. D., Butler, B. A., Dekker, R. G., 2nd, Prescott, A., & Kadakia, A. R. (2017). Total ankle arthroplasty versus ankle arthrodesis-a comparison of outcomes over the last decade. Journal of orthopaedic surgery and research, 12(1), 76. https://doi.org/10.1186/s13018-017-0576-1
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine