Skeletal muscles attached to the arms, legs, neck, back, and trunk bones are voluntary and consciously controlled. Weakness or inability to control these muscles can signal a health issue like a neuromuscular disorder or electrolyte imbalance. Can recognizing the symptoms can help healthcare providers develop effective treatment programs?
Voluntary Muscles
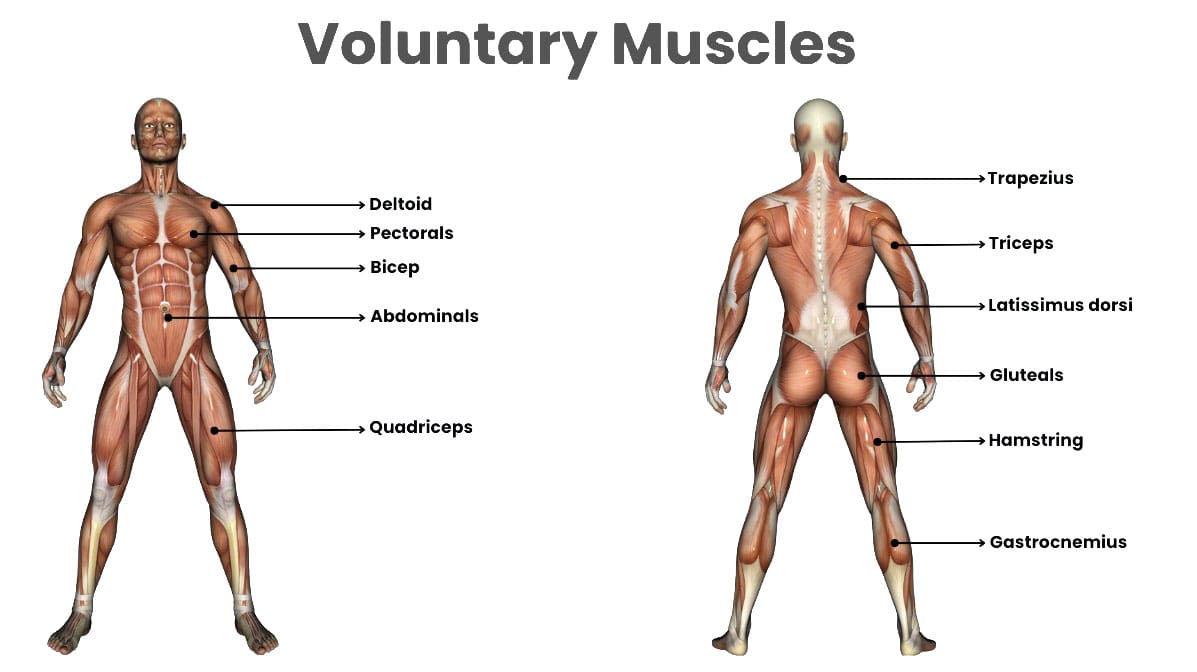
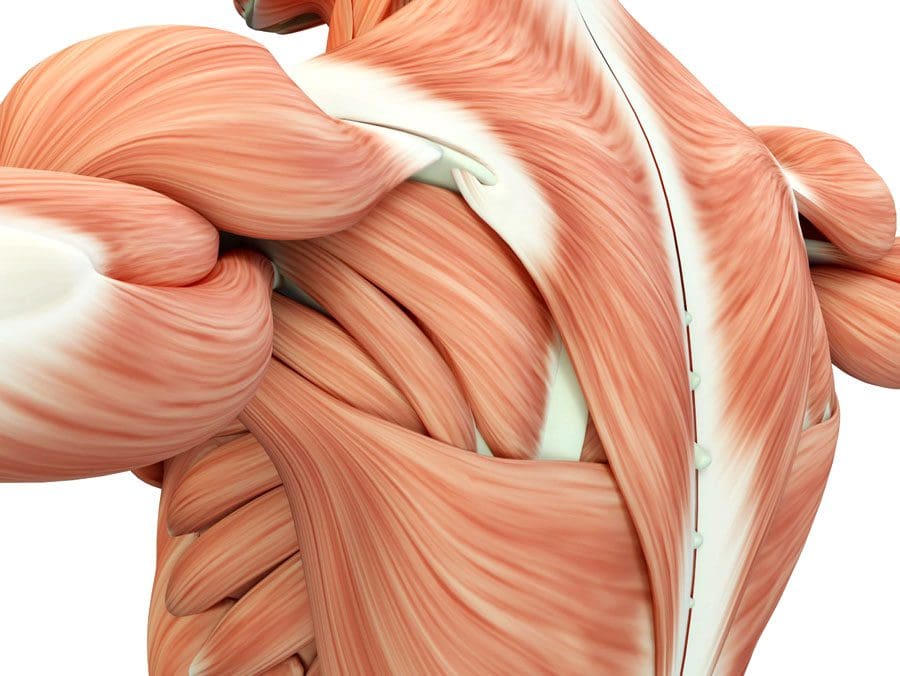
Voluntary muscles are the skeletal muscles that attach to bones and control movement of the limbs, head, neck, and body under an individual’s conscious control. Skeletal muscles are controlled by neuromuscular signals from the brain that communicate with individual muscle fibers and cause them to contract.
Difference
Voluntary muscles are skeletal muscles that contract and relax under conscious control.
These muscles attach to bones and regulate movement of the body.
Involuntary muscles are not under conscious control.
Involuntary muscles involve automatic internal processes needed for survival, like controlling blood vessels and organs like the heart, lungs, and digestive system.
They contract and relax automatically and receive signals from the autonomic nervous system, which regulates internal bodily functions.
Voluntary
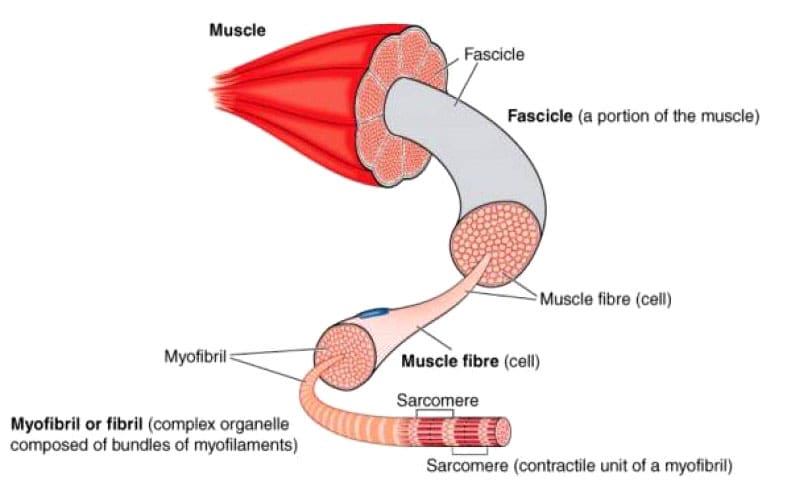
Voluntary muscles are skeletal muscles that comprise 40% of the body’s weight and 50% to 75% of the body’s proteins. These muscles can convert chemical and mechanical energy to cause voluntary muscle contraction and movement. (Trovato F.M. et al., 2016) Skeletal muscle comprises fascicles or bundled units of multiple muscle fibers or muscle cells. Each muscle fiber consists of a cross-banded structure further divided into myofibrils containing thick myosin and thin actin myofilaments, which give the muscle its stripe appearance, and the structure gives the characteristic striated structure. (Trovato F.M. et al., 2016) Muscle contraction occurs when these myofilaments move closer together, stimulated by the release of the neurotransmitter acetylcholine from nerve cells that communicate with the muscle fiber.
Involuntary
The autonomic nervous system controls involuntary muscles, regulating their contraction and relaxation. This system also controls the activity of organs and blood vessels for essential daily functions, including breathing, circulation, digestion, heartbeat regulation, and urination. Most involuntary muscles are composed of smooth muscles. Smooth muscles do not have the striated structure of skeletal muscles and consist of sheets or layers of smooth muscle cells. When the autonomic nervous system stimulates these muscle cells to contract by releasing hormones or other chemical signals, smooth muscle cells shorten through the movement of actin and myosin myofilaments. Involuntary smooth muscles include the blood vessel walls, diaphragm, intestines, and bladder. (Webb R. C. 2003) One exception of an involuntary muscle is the myocardium, or heart muscle. The myocardium comprises a specialized cardiac muscle cell found only in the heart. Cardiac muscle is striated like skeletal muscle but is controlled by the autonomic nervous system and pacemaker cells, causing it to contract automatically and rhythmically.
Weakened Voluntary Muscles
Skeletal muscle diseases, neuromuscular disorders, and other causes can weaken muscles. Neuromuscular or skeletal muscle disorders affect the nerves that send electrical signals to voluntary skeletal muscles to control movement. When the nerves are damaged, communication between the nerves and muscles becomes disrupted. This can result in significant muscle weakness, atrophy, and loss of function. Most neuromuscular disorders are genetic or caused by issues with the immune system. Nerves communicate with muscles through the release of neurotransmitters at the neuromuscular junction, which is the space between a nerve cell and muscle fiber. Neuromuscular disorders can damage the nerve or the neuromuscular junction. Neuromuscular disorder symptoms can include: (Cleveland Clinic, 2023)
Numbness and tingling
Muscle weakness
Muscle twitches, cramps, or spasms
Muscle pain
Muscle atrophy
Decreased coordination
Balance problems
Drooping eyelids and double vision from eye muscle weakness.
Difficulty swallowing due to weakness of the pharynx.
Difficulty breathing due to weakness of the diaphragm.
Common Neuromuscular Disorders
Amyotrophic Lateral Sclerosis – ALS
More commonly known as Lou Gehrig’s disease, it is a genetic disorder that results from hardening of the spinal cord.
It causes damage to the nerves that control muscles and voluntary movement.
Charcot-Marie-Tooth Disease
This is a class of peripheral nerve disorders that cause muscle weakness, atrophy, and loss of sensation, most commonly in the legs and feet.
It is a genetic disorder caused by a gene mutation that damages myelin, or the insulating sheath that surrounds all nerves and supports the conduction of electrical signals.
Multiple Sclerosis – MS
MS causes degeneration of the myelin sheath surrounding nerves, decreasing the impulses along the nerves to muscles.
It can result in muscle weakness, which is often more severe on the dominant side of the body.
There are different forms of MS, but the condition is often progressive and gets worse over time if left untreated.
Muscular Dystrophies
These are genetic diseases characterized by gradual loss of motor function, muscle weakness and atrophy, walking gait problems, progressive respiratory failure, and cardiomyopathy.
There are nine types of muscular dystrophy, all caused by genetic mutations.
Myasthenia Gravis
This is an autoimmune disease that causes inflammation throughout the body.
An autoimmune disease occurs when the immune system attacks healthy cells by mistake.
With myasthenia gravis, the body produces antibodies that attack the receptors for acetylcholine, reducing the body’s ability to contract muscles.
This leads to muscle weakness, atrophy, and fatigue.
Myopathies
These are diseases of muscles that cause muscle weakness and atrophy.
Depending on the type, they may progress and get worse over time.
Electrolyte Imbalances
Muscle weakness can result from altered sodium, potassium, calcium, or magnesium levels.
Always seek immediate medical attention for any sudden, unexplained muscle weakness. Individuals who experience skeletal muscle weakness should discuss the type and duration of symptoms with their doctor, specialist, physical therapist, or chiropractor, as this might be a sign of a medical condition such as a neuromuscular disorder. Working with a chiropractic team can help expedite healing. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized treatment program through an integrated approach to treat injuries and chronic pain syndromes, improving flexibility, mobility, and agility, relieving pain, and helping individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Chiropractic Massage Therapy
References
Trovato FM, I. M., Conway N, Castrogiovanni P. (2016). Morphological and functional aspects of human skeletal muscle. J Funct Morphol Kinesiol., 1(3), 289-302. doi.org/https://doi.org/10.3390/jfmk1030289
Webb R. C. (2003). Smooth muscle contraction and relaxation. Advances in physiology education, 27(1-4), 201–206. doi.org/10.1152/advan.00025.2003
Can physical therapies help relieve muscle contractures in individuals who have endured prolonged bed rest, inactivity, or lack of use of certain muscle groups?
Muscle Contracture
A muscle contracture, or contracture deformity, is caused when a muscle loses elasticity. This causes permanent shortening and tightening of muscle fibers, which reduces flexibility and makes movement difficult. Muscles that cannot move and stretch cause the surrounding joints to lose mobility and develop pain symptoms. When trying to stretch the contracted muscle, the individual will feel the muscle become very rigid, which can increase pain. (Lieber, R. L., and Fridén, J. 2019) Delaying treatment can potentially cause irreversible and chronic symptoms.
Commonly Affected Muscles
Flexor muscles bend the joints and are those most affected by contractures. The stiffening and tightening prevent the body parts from moving out and away. The most common include:
Wrist and Finger Flexors
Muscle groups that bend the wrist and fingers.
Biceps
The primary elbow flexor that bends the arm.
Gastrocnemius and Soleus
The calf muscles which allow the ankle to point the foot/plantarflexion.
Hamstrings
A group of three muscles behind the thigh that bend the knee.
Causes
The permanent shortening of muscle fibers and changes in muscle structure cause muscle contractures or stiffer-than-normal tissue that is difficult to stretch. Sarcomeres are structural units of muscles that cause fibers to contract.
With contractures, the sarcomeres overly lengthen when the muscle fibers tighten. This increase in sarcomere length prevents the muscle from contracting normally, resulting in weakness. Muscle fibers are encased in an extracellular matrix, a mesh composed of collagen and other proteins that help transmit force and provide muscle contraction. Muscle contractures cause the amount of collagen within the extracellular matrix to increase, causing a stiffening of fibers that restricts movement. (Lieber, R. L., and Fridén, J. 2019)
Muscle contractures also form from decreased satellite cells. Satellite cells are specialized stem cells that can rebuild muscle and are necessary for muscle regeneration and repair. Without the proper amount of satellite cells, other cells like fibroblasts significantly increase in the muscle tissue, causing the fibers to become stiff and fibrotic or more fibrous. These changes to the sarcomeres, collagen within the extracellular matrix, and decreased satellite cells all result from conditions in which neurological input to the brain and spinal cord muscles becomes reduced. This is caused by lack of use, injury, or neurological and neuromuscular conditions. (Lieber, R. L., and Fridén, J. 2019)
Cerebral Palsy
Contractures often occur from upper motor neuron lesions, which prevent signals from the brain and spinal cord from reaching the motor neurons that control muscle contraction. When these signals are weakened or blocked, muscles become stiff and weak from lack of stimulation. (Lieber, R. L., and Fridén, J. 2019)
Cerebral palsy is a group of disorders affecting mobility caused by an upper motor neuron lesion that is present at birth and is the most common motor disability in children. It causes:
Cognitive impairment
Decreased muscle strength
Problems with movement, coordination, and functional motions.
Because cerebral palsy prevents the muscles of the legs from being sufficiently stimulated, contractures commonly develop in the hips, knees, and ankles. Individuals can have a 75% decrease in satellite cells to repair muscle tissue and prevent muscle fibrosis or stiffening. Specific genes linked to collagen production are also altered, causing irregular changes to the extracellular matrix of muscles. (Lieber, R. L., and Fridén, J. 2019)
Muscular Dystrophy
Muscular dystrophy is a group of inherited neuromuscular disorders characterized by muscle weakness and wasting. Deficient nerve supply to muscles causes them to become stiff and tight, inhibiting the functional range of motion needed to move joints and activate muscles to move. Clinical research suggests that individuals with muscular dystrophy have decreased levels of satellite cells to repair, increasing the risk of developing muscle contracture. (Lieber, R. L., and Fridén, J. 2019)
Disuse-induced Muscle Wasting or Disuse Atrophy
When muscles are not used for some time because of hospitalization, prolonged bed rest, or immobilization from wearing braces, splints, or casts after injuries, the blood circulation and electrical signaling from nerves to muscles decreases. This results in weakness, increased muscle tightness and stiffness, and muscle wasting/atrophy. Over time, stiff and tight muscles can progress to contractures that become extremely difficult to stretch.
Trauma or Injury
Muscle or tendon injuries can cause contractures as scar tissue develops, joining muscle fibers and joints together. This can significantly restrict movement. Large burns can also cause skin, muscles, and joint contractures. The range of motion can become significantly limited, and the changes can become irreversible if not aggressively treated.
Other Causes
Other forms of upper motor neuron lesions that can cause contractures because of weak or blocked electrical input to muscles as a result of brain or spinal cord damage include:
Neuromuscular disorders like spinal muscular atrophy – SMA.
Conditions that cause inflammation and joint stiffening, like juvenile rheumatoid arthritis.
A history of diabetes also increases the risk of developing contractures affecting finger flexors, like Dupuytren’s contractures and stenosing tenosynovitis
or trigger finger. (Lieber, R. L., and Fridén, J. 2019)
Symptoms
Symptoms include:
Extremely stiff and tight muscles resistant to stretching.
Pain from the inability to stretch.
Loss of range of motion.
Impaired joint mobility.
Severe contractures can interfere with the functional range of motion needed to move joints to complete normal tasks and movements, such as standing up from a chair and walking.
Treatment
Physical Therapy
Physical therapies can help reduce the severity through stretching and soft tissue mobilization to decrease tightness. (Lieber, R. L., and Fridén, J. 2019)
Specialized braces or splints can be custom-made to fit different body parts.
These provide a prolonged low-intensity stretch over a period of time to increase muscle length.
Once the muscle has stretched, a new brace or splint may be needed to adjust to the increased range of motion. (Lieber, R. L., and Fridén, J. 2019)
Surgery
In severe cases where muscle contractures limit the functional range of motion needed for activities of daily living or ADLs, surgical release of the contracted tissue may be recommended. This surgery can improve functional movements like walking, getting in and out of bed, and standing up from chairs. The tight muscles can be surgically cut, and the tendons can be lengthened to allow more mobility. (Lieber, R. L., and Fridén, J. 2019)
The causes of muscle contracture are not always avoidable, but various treatment options are available to help loosen up tight muscles and preserve or restore the range of motion. It’s important to move daily and stretch common areas like the fingers, arms, and legs to reduce the risk of muscle tightness and prevent contractures from developing. It is imperative to seek medical treatment for severe contractures resulting from neuromuscular disorders, including physical and occupational therapy, to prevent contractures from worsening and regaining as much functional range as possible.
Injury Medical Chiropractic and Functional Medicine Clinic uses an integrated approach personalized to the individual that focuses on what works for them and treats injuries and chronic pain syndromes through personalized care plans that improve ability through flexibility, mobility, and agility programs to relieve pain. Our providers use an integrated approach to create personalized care plans for each patient, including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Our goal is to relieve pain naturally by restoring health and function to the body. If other treatment is needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Chiropractic Treatment for Cerebral Palsy
References
Lieber, R. L., & Fridén, J. (2019). Muscle contracture and passive mechanics in cerebral palsy. Journal of applied physiology (Bethesda, Md. : 1985), 126(5), 1492–1501. doi.org/10.1152/japplphysiol.00278.2018
For individuals who have exhausted all other treatment options for low back pain and nerve root compression, can laser spine surgery help alleviate nerve compression and provide long-lasting pain relief?
Laser Spine Surgery
Laser spine surgery is a minimally invasive surgical procedure that uses a laser to cut through and remove spinal structures that are compressing nerves and causing intense pain. The minimally invasive procedure often results in less pain, tissue damage, and faster recovery than more extensive surgeries.
How It Works
Minimally invasive procedures result in less scarring and damage to surrounding structures, often reducing pain symptoms and a shorter recovery time. (Stern, J. 2009) Small incisions are made to access spinal column structures. With open-back surgery, a large incision is made down the back to access the spine. The surgery differs from other surgeries in that a laser beam, rather than other surgical instruments, is used to cut structures in the spine. However, the initial incision through the skin is made with a surgical scalpel. Laser is an acronym for Light Amplification Stimulated by Emission of Radiation. A laser can generate intense heat to cut through soft tissues, especially those with a high water content, like spinal column discs. (Stern, J. 2009) For many spine surgeries, the laser cannot be used to cut through bone as it generates instant sparks that can damage surrounding structures. Rather, laser spine surgery is primarily used to perform a discectomy, which is a surgical technique that removes a portion of a bulging or herniated disc that is pushing against the surrounding nerve roots, causing nerve compression and sciatic pain. (Stern, J. 2009)
Surgical Risks
Laser spine surgery may help resolve the cause of nerve root compression, but there is an increased risk of damage to nearby structures. Associated risks include: (Brouwer, P. A. et al., 2015)
Infection
Bleeding
Blood clots
Remaining symptoms
Returning symptoms
Further nerve damage
Damage to the membrane around the spinal cord.
Need for additional surgery
A laser beam is not precise like other surgical tools and requires practiced mastery and control to avoid damage to the spinal cord and nerve roots. (Stern, J. 2009) Because lasers cannot cut through bone, other surgical instruments are often used around corners and at different angles because they are more efficient and allow greater accuracy. (Atlantic Brain and Spine, 2022)
Purpose
Laser spine surgery is performed to remove structures that are causing nerve root compression. Nerve root compression is associated with the following conditions (Cleveland Clinic. 2018)
Bulging discs
Herniated discs
Sciatica
Spinal stenosis
Spinal cord tumors
Nerve roots that are injured or damaged and constantly send chronic pain signals can be ablated with laser surgery, known as nerve ablation. The laser burns and destroys the nerve fibers. (Stern, J. 2009) Because laser spine surgery is limited in treating certain spinal disorders, most minimally invasive spine procedures do not use a laser. (Atlantic Brain and Spine. 2022)
Preparation
The surgical team will provide more detailed instructions on what to do in the days and hours before surgery. To promote optimal healing and a smooth recovery, it is recommended that the patient stay active, eat a healthy diet, and stop smoking prior to the operation. Individuals may need to stop taking certain medications to prevent excess bleeding or interaction with anesthesia during the operation. Inform the healthcare provider about all prescriptions, over-the-counter drugs, and supplements being taken.
Laser spine surgery is an outpatient procedure at a hospital or outpatient surgical center. The patient will likely go home on the same day of the operation. (Cleveland Clinic. 2018) Patients cannot drive to or from the hospital before or after their surgery, so arrange for family or friends to provide transportation. Minimizing stress and prioritizing healthy mental and emotional well-being is important to lowering inflammation and aiding recovery. The healthier the patient goes into surgery, the easier the recovery and rehabilitation will be.
Expectations
The surgery will be decided by the patient and healthcare provider and scheduled at a hospital or outpatient surgical center. Arrange for a friend or family member to drive to the surgery and home.
Before Surgery
The patient will be taken to a pre-operative room and asked to change into a gown.
The patient will undergo a brief physical examination and answer questions about medical history.
The patient lies on a hospital bed, and a nurse inserts an IV to deliver medication and fluids.
The surgical team will use the hospital bed to transport the patient in and out of the operating room.
The surgical team will assist the patient in getting onto the operating table, and the patient will be administered anesthesia.
The patient may receive general anesthesia, which will cause the patient to sleep for the surgery, or regional anesthesia, injected into the spine to numb the affected area. (Cleveland Clinic. 2018)
The surgical team will sterilize the skin where the incision will be made.
An antiseptic solution will be used to kill bacteria and prevent the risk of infection.
Once sanitized, the body will be covered with sterilized linens to keep the surgical site clean.
During Surgery
For a discectomy, the surgeon will make a small incision less than one inch in length with a scalpel along the spine to access the nerve roots.
A surgical tool called an endoscope is a camera inserted into the incision to view the spine. (Brouwer, P. A. et al., 2015)
Once the problematic disc portion causing the compression is located, the laser is inserted to cut through it.
The cut disc portion is removed, and the incision site is sutured.
After Surgery
After surgery, the patient is brought to a recovery room, where vital signs are monitored as the effects of the anesthesia wear off.
Once stabilized, the patient can usually go home one or two hours after the operation.
The surgeon will determine when the individual is clear to resume driving.
Recovery
Following a discectomy, the individual can return to work within a few days to a few weeks, depending on the severity, but it can take up to three months to return to normal activities. Length of recovery can range from two to four weeks or less to resume a sedentary job or eight to 12 weeks for a more physically demanding job that requires heavy lifting. (University of Wisconsin School of Medicine and Public Health, 2021) During the first two weeks, the patient will be given restrictions to facilitate the spine’s healing until it becomes more stable. Restrictions can include: (University of Wisconsin School of Medicine and Public Health, 2021)
No bending, twisting, or lifting.
No strenuous physical activity, including exercise, housework, yard work, and sex.
No alcohol in the initial stage of recovery or while taking narcotic pain medications.
No driving or operating a motor vehicle until discussed with the surgeon.
The healthcare provider may recommend physical therapy to relax, strengthen, and maintain musculoskeletal health. Physical therapy may be two to three times weekly for four to six weeks.
Process
Optimal recovery recommendations include:
Getting enough sleep, at least seven to eight hours.
Maintaining a positive attitude and learning how to cope and manage stress.
Maintaining body hydration.
Following the exercise program as prescribed by the physical therapist.
Practicing healthy posture with sitting, standing, walking, and sleeping.
Staying active and limiting the amount of time spent sitting. Try to get up and walk every one to two hours during the day to stay active and prevent blood clots. Gradually increase the amount of time or distance as recovery progresses.
Do not push to do too much too soon. Overexertion can increase pain and delay recovery.
Learning correct lifting techniques to utilize the core and leg muscles to prevent increased pressure on the spine.
Discuss treatment options for managing symptoms with a healthcare provider or specialist to determine if laser spine surgery is appropriate. Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers. We focus on restoring normal body functions after trauma and soft tissue injuries using Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Brouwer, P. A., Brand, R., van den Akker-van Marle, M. E., Jacobs, W. C., Schenk, B., van den Berg-Huijsmans, A. A., Koes, B. W., van Buchem, M. A., Arts, M. P., & Peul, W. C. (2015). Percutaneous laser disc decompression versus conventional microdiscectomy in sciatica: a randomized controlled trial. The spine journal : official journal of the North American Spine Society, 15(5), 857–865. doi.org/10.1016/j.spinee.2015.01.020
University of Wisconsin School of Medicine and Public Health. (2021). Home Care Instructions after Lumbar Laminectomy, Decompression or Discectomy Surgery. patient.uwhealth.org/healthfacts/4466
For individuals starting to lift weights, motor units are important for muscle movement. Can building more motor units help build strength and maintain muscle mass?
Motor Units
Motor units control the skeletal muscles and are the force behind every body movement. (C J. Heckman, Roger M. Enoka 2012)
This includes voluntary movements like lifting weights and involuntary movements like breathing. When lifting objects and weights, the body adapts to motor unit needs, meaning that individuals must consistently increase the weight to progress.
Lifting weights regularly trains the body to generate more motor units and force.
General guidelines recommend lifting weights for all muscle groups two to three non-consecutive days a week.
Consistency helps maintain muscle mass.
Regular progression increases the risk of plateauing.
What They Are
Exercise increases the body’s muscle strength, while sedentariness and inactivity weaken them. A motor unit is a single nerve cell/neuron that supplies the nerves to innervate a group of skeletal muscles. The neuron receives signals from the brain that stimulate all the muscle fibers in that particular motor unit to generate movement.
Muscles comprise different fiber types.
They are attached to the bones with connective tissue, which is stronger than the muscle.
Multiple motor units are dispersed throughout the muscle.
The motor units help ensure muscle contraction force is evenly spread throughout the muscle.
Motor units are different sizes and operate differently depending on where and what they do.
Small motor units might only innervate five or ten fibers. For example, to blink or sniff.
Large motor units can comprise hundreds of muscle fibers for swinging or jumping movements.
How They Work
The number of units activated depends on the task. Stronger muscle contractions require more. However, fewer units are needed to accomplish the movement for individuals expending less effort.
Contraction
Once a unit receives a signal from the brain, the muscle fibers contract simultaneously.
The force generated depends on how many units are required to accomplish the task. (Purves D. et al., 2001)
For example, picking up small objects like a pen and paper requires only a few units to generate the force needed.
If picking up a heavy barbell, the body needs more units because more force is needed to lift the heavier load.
The body can generate more force with stronger muscles.
This happens when lifting weights on a regular basis and overloading the muscles with more weight than they can handle.
This process is known as adaptation.
Adaptation
The purpose of lifting weights is to challenge the muscles so they adapt to the new challenge and grow in strength and mass. Motor units are a major part of the adaptation process. (Dr. Erin Nitschke. American Council on Exercise. 2017)
As individuals continue working out, their ability to generate more force increases and units activate more rapidly.
This makes movements more efficient.
Individuals can increase motor unit recruitment by consistently increasing the weight challenge to their muscles.
The development creates movement memory.
A relationship between the brain, muscles, and motor units is established even if the individual stops working out. The pathways are still there no matter how long the individual takes off.
When returning to training, the body will remember how to ride a bike, do a bicep curl, or squat.
However, the muscles will not have the same strength as the strength needs to be built back along with endurance that may have been lost.
It is the movement memory that remains.
Military Training and Chiropractic Care: Maximizing Performance
References
Heckman, C. J., & Enoka, R. M. (2012). Motor unit. Comprehensive Physiology, 2(4), 2629–2682. doi.org/10.1002/cphy.c100087
Purves D, Augustine GJ, Fitzpatrick D, et al., editors. (2001). Neuroscience. 2nd edition. Sunderland (MA): Sinauer Associates; 2001. The Motor Unit. Available from: www.ncbi.nlm.nih.gov/books/NBK10874/
Nerves control muscle fibers. Muscle twitching is an involuntary contraction of the muscle fibers. When individuals play sports/work out vigorously or for a long time, they may experience muscle twitching and can often see and/or feel the twitches happening. The most worked-out muscles are likely to twitch, which includes the biceps, thighs, and calves, but twitches can occur in any muscle. Chiropractic care, massage therapy, and functional medicine can help relax the muscles, improve circulation, restore function, and train individuals to prevent future episodes.
Muscle Twitching
A muscle twitch often occurs after intense physical activity or a hard workout because the muscle or muscles have been overworked, and there is hyper-excitability of the nerve/s that makes the muscle/s continue to contract.
A muscle twitch that can be seen is called fasciculation.
A muscle twitch that cannot be seen is called fibrillation.
If there is pain or the twitching is prolonged, it is a muscle spasm.
Causes
The most common causes include the following:
Intense exercise and rigorous physical activity build up lactic acid in the muscles.
Dehydration is a very common factor for shaky muscles.
Vitamin D and calcium deficiencies could cause muscle spasms in the hand, calves, and eyelids.
Using caffeinated products to increase physical performance.
Not enough or a lack of healthy sleep.
Anxiety or stress.
Certain medications like estrogen and corticosteroids.
Nicotine and tobacco use.
Physical Activity/Exercise
Intense exercise and physical activity can cause muscle fatigue.
Muscle fatigue triggers twitching and cramping in overworked muscle fibers.
Electrolytes play a role in muscle contraction.
Electrolyte loss and imbalances within muscle fibers through sweating can lead to twitching.
Dehydration
Muscle mass comprises 75% water.
Water carries nutrients and minerals to muscles to support function.
Not being properly hydrated can cause twitching and cramping.
Vitamin D Deficiency
Nerves need vitamin D to relay messages to and from the brain to the body’s muscles.
A vitamin D deficiency can cause muscle weakness and twitching.
Lack of sleep can affect neurotransmitter function.
A common site of fasciculation tiredness occurs in the eyelids.
Anxiety and Stress
Experiencing psychological stress or high anxiety levels can cause excess muscle tension.
This can lead to muscle twitching.
Muscle fasciculation caused by stress can occur anywhere in the body.
Certain Medications
Certain medications can lead to involuntary muscle twitching.
The reaction can be a side effect due to interactions with other medications.
Individuals should discuss side effects and medication interactions with their doctor when taking a new medication.
Chiropractic Care
Chiropractors are experts on the musculoskeletal system and have many techniques to treat muscle fasciculation and spasms. It often depends on the cause/s, and specific treatment varies on a case-by-case basis. Common chiropractic treatments include:
Massage therapy
Heat and ice therapy
Manual manipulation
Joint adjustments
Ultrasound
Stretches to keep the muscles flexible
Exercises to strengthen the muscles
Nutritional recommendations
Fasciculation
References
Bergeron, Michael F.. Muscle Cramps during Exercise-Is It Fatigue or Electrolyte Deficit?. Current Sports Medicine Reports July 2008 – Volume 7 – Issue 4 – p S50-S55 doi: 10.1249/JSR.0b013e31817f476a
Gragossian A, Bashir K, Friede R. Hypomagnesemia. [Updated 2022 May 15]. In: StatPearls [Internet]. Treasure Island (F.L.): StatPearls Publishing; 2022 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK500003/
Küçükali, Cem Ismail, et al. “Peripheral nerve hyperexcitability syndromes.” Reviews in the neurosciences vol. 26,2 (2015): 239-51. doi:10.1515/revneuro-2014-0066
Maughan, Ronald J, and Susan M Shirreffs. “Muscle Cramping During Exercise: Causes, Solutions, and Questions Remaining.” Sports medicine (Auckland, N.Z.) vol. 49, Suppl 2 (2019): 115-124. doi:10.1007/s40279-019-01162-1
Miller, Kevin C et al. “Exercise-associated muscle cramps: causes, treatment, and prevention.” Sports health vol. 2,4 (2010): 279-83. doi:10.1177/1941738109357299
Riebl, Shaun K, and Brenda M Davy. “The Hydration Equation: Update on Water Balance and Cognitive Performance.” ACSM’s health & fitness journal vol. 17,6 (2013): 21-28. doi:10.1249/FIT.0b013e3182a9570f
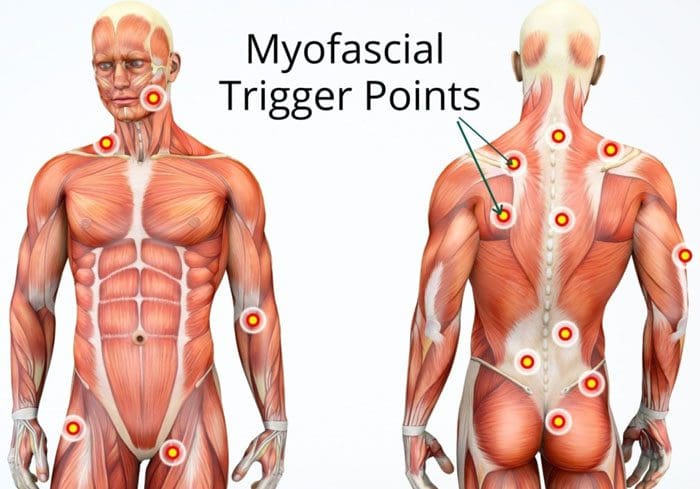
Muscle knots are common and can occur anywhere on the body. They can cause aching and pain in the muscles and joints. When examining a muscle knot also known as myofascial trigger points, it can feel swollen, tense, or like a bump. A particular area where these knots present is in the low back. This happens from excessive wear-and-tear on the lower spine from work, school, daily tasks, and chores. This causes the muscle fibers to tear, and with restricted or no time to rest the area and let it heal properly leads to the fibers bunching/clumping together forming a painful knot.
Muscle Knots In The Lower Back
A muscle knot in the lower back causes aching, soreness, and full-on pain. They tighten and contract even when the muscle is resting. The affected area often becomes inflamed or swollen causing pain and aches to radiate/spread to the gluteal muscles, as well.
Development
These knots develop when the tissue fibers pull apart and bunch up together. They start to stick together and with time the area becomes thicker. This results in the muscle knot. They can be caused by:
Stress
Tension
Poor posture
Muscle overuse
Muscle strain
Sedentary habits
Body dehydration and an unhealthy diet can also contribute to muscle knots. They look like a small bump under the skin. The bump can be red and is usually tender/sore when touched. However, not all muscle knots are visible, but when touched there is soreness and/or pain.
Do They Go Away?
They can go away on their own, but this comes from proper rest and recovery time. However, muscle knots should not be ignored, as even the smallest knot can compress surrounding nerves and muscle tissues. This can cause irritation and weakness. Larger muscle knots could cause movement/mobility issues.
Therapies
Stretching
Stretching will help stretch out and release tight muscle knots. Stretching loosens the muscle fibers and prevents them from becoming attached. Stretches to release a muscle knot include:
Start with these simple stretches/exercises and slowly work up to more vigorous ones.
Chiropractic Care
Chiropractic care can break down muscle knots through various adjustments. They are experts on the musculoskeletal system and understand where the problem is occurring along with the connected muscles.
A chiropractor will palpate the spot where the most pain presents and the surrounding area.
They will begin with a soft massage. This warms up the area getting the blood circulating. The blood circulation helps prevent pain making the adjustment/s far more effective.
Then pressing on nearby joints that the muscle knot is connected to breaks up the tight fibers.
Then the section/area is stretched out. This extends the fibers and prevents them from winding back into a knot.
They will recommend stretches and exercises
Therapeutic Massage
A massage helps to release tension and encourages muscle knots to loosen up and break down. A massage therapist will perform a deep tissue massage or a Swedish massage. Massage helps to release endorphins, which are the body’s natural painkiller. These calm the body and reduce pain. They will also recommend simple massages at home. These can include:
Rolling a massage ball/roller on the muscle knot
Self-massage using the fingers in circular motions on the affected area
Heat and Ice
Hot and cold therapy can calm and prevent inflammation. Heating pads are best if the area has stiffness or is painful. The heat relaxes tight muscles and increases blood flow. Cold therapy stops the swelling. If the muscle knot gets bigger or begins turning red, icing the area is recommended. Alternating between the two can eliminate symptoms and assist with quicker healing.
Body Composition
Building Functional Strength
There are exercises to improve functional strength. Functional training targets specific areas:
Then lift the outside leg up as high as possible and hold for 10 seconds
Repeat on the other side
Do 6-10 repetitions on each side
This exercise builds shoulder, arm, and hip strength. It engages the core and abdominal muscles and improves flexibility in the shoulders, back, and hips.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: coach@elpasofunctionalmedicine.com
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Cramer, Holger et al. “Postural awareness and its relation to pain: validation of an innovative instrument measuring awareness of body posture in patients with chronic pain.” BMC musculoskeletal disorders vol. 19,1 109. 6 Apr. 2018, doi:10.1186/s12891-018-2031-9
Malanga, Gerard A et al. “Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury.” Postgraduate medicine vol. 127,1 (2015): 57-65. doi:10.1080/00325481.2015.992719
El Paso, TX. Chiropractor, Dr. Alexander Jimenez continues the discussion on the anatomy of nerve fibers, receptors, spinal tracts and brain pathway/s. As the spinal nerve nears the spinal cord, it splits into the dorsal and ventral roots. The dorsal root only contains the axons of sensory neurons. While the ventral roots contain only the axons of motor neurons. Some of the branches synapse with local neurons in the dorsal root ganglion, posterior (dorsal) horn, and even the anterior (ventral) horn, at the spine where they enter.
Other branches travel short distances up or down the spine to interact with neurons at other levels of the spinal cord. A branch can also turn into the posterior (dorsal) column white matter to connect with the brain. Spinal nerve systems that connect to the brain are contralateral, in that the right side of the body is connected to the left side of the brain and the left side of the body is connected to the right side of the brain.
Cranial nerves convey specific sense information from the head and neck directly to the brain. Whereas spinal information is contralateral, cranial nerve systems are for the most part�ipsilateral, meaning that a cranial nerve on the right side of the head is connected to the right side of the brain. Some cranial nerves contain only sensory axons. Other cranial nerves have both sensory and motor axons, including the trigeminal, facial and glossopharyngeal. General senses of somatosensation for the face travel through the trigeminal system.
PATHWAYS
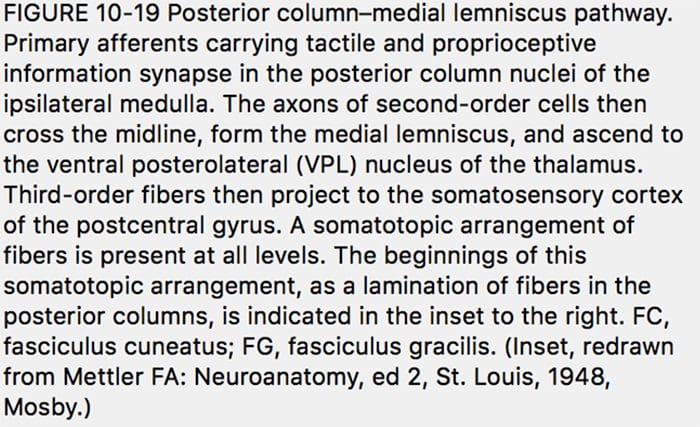
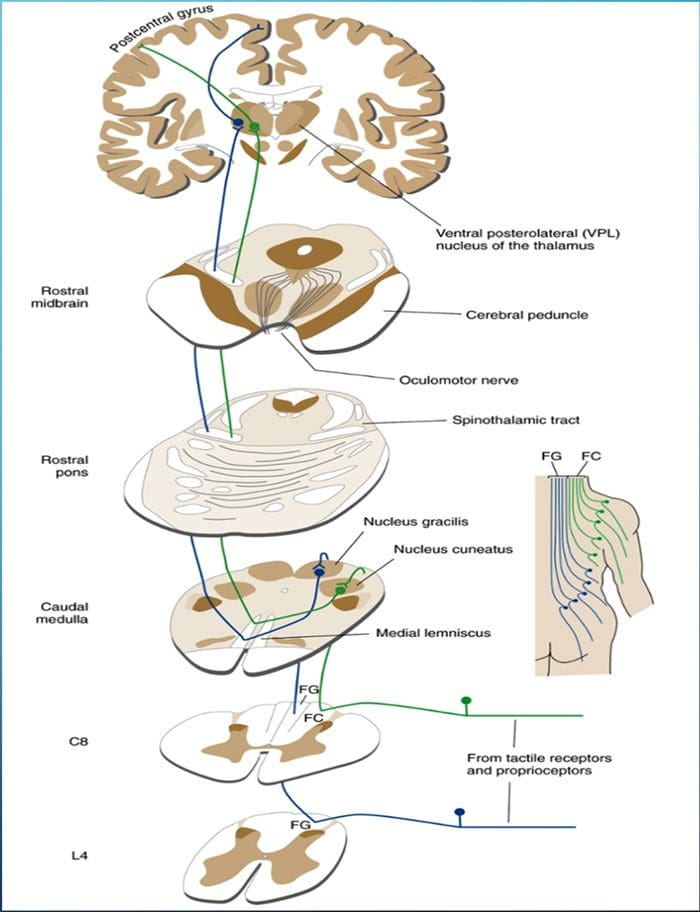
THE POSTERIOR COLUMN� MEDIAL LEMNISCUS SYSTEM CONVEYS INFORMATION ABOUT TOUCH AND LIMB POSITION
POSTERIOR COLUMN MEDIAL LEMNISCAL PATHWAY
The term posterior column refers to the entire contents of a posterior funiculus, exclusive of its share of the propriospinal tract. The posterior columns consist mainly of ascending collaterals of large myelinated primary afferents carrying impulses from various kinds of mechanoreceptors (although substantial numbers of second-order fibers and unmyelinated fibers are also included). This has traditionally been considered the major pathway by which information from low-threshold cutaneous, joint, and muscle receptors reaches the cerebral cortex.
2-Minute Neuroscience: Touch & The Dorsal Columns-Medial Lemniscus
DAMAGE TO THE POSTERIOR COLUMN�MEDIAL LEMNISCUS SYSTEM CAUSES IMPAIRMENT OF PROPRIOCEPTION AND DISCRIMINATIVE TACTILE FUNCTIONS
�As might be expected from the types of afferents contained in the posterior columns, this pathway carries information important for the conscious appreciation of touch, pressure, and vibration and of joint position and movement. However, because input from cutaneous receptors also reaches the cortex by other routes, damage to the posterior columns causes impairment, but not abolition, of tactile perception. Complex discrimination tasks are more severely affected than is the simple detection of stimuli. Other functions, such as proprioception and kinesthesia, are classically considered to be totally lost after posterior column destruction. The result is a distinctive type of ataxia (incoordination of movement); the brain is unable to direct motor activity properly without sensory feedback about the current position of parts of the body. This ataxia is particularly pronounced when the patient�s eyes are closed, preventing visual compensation.�
Given the role of the posterior column, the patient should be screened for any abnormalities regarding their sense of fine touch, vibration, barognosis, graphesthesia, stereognosis, kinaesthesia, two-point discrimination and conscious proprioception:
A common way of testing for fine touch is to ask the patient to recognize common objects placed within a cloth using their touch.
Vibration sense can be tested using a low pitched C128 tuning fork placed along a bony prominence of the desired corresponding spinal level(s) to be tested.
Barognosis refers to the ability to determine the approximate weight of an object.
Graphesthesia refers to the ability to recognize writing on the skin by touch. The practitioner can draw out a letter on the patients skin as a way of testing.
Kinaesthesia refers to ones own sense of body motion (excluding equilibrium which is controlled in part by the inner ear) and is commonly tested using the subject�s ability to detect an externally imposed passive movement, or the ability to reposition a joint to a predetermined position.
Proprioception is often assessed using the Rombergs test. This examination is based on the notion that a person requires at least two of the three following senses to maintain balance while standing: proprioception; vestibular function and vision. A patient who has a defect within their proprioceptive mechanism can still maintain balance by using vestibular function and vision. In the Romberg test, the patient is stood up and asked to close their eyes. A loss of balance is interpreted as a positive Romberg sign.
THE SPINOTHALAMIC TRACT CONVEYS INFORMATION ABOUT PAIN AND TEMPERATURE
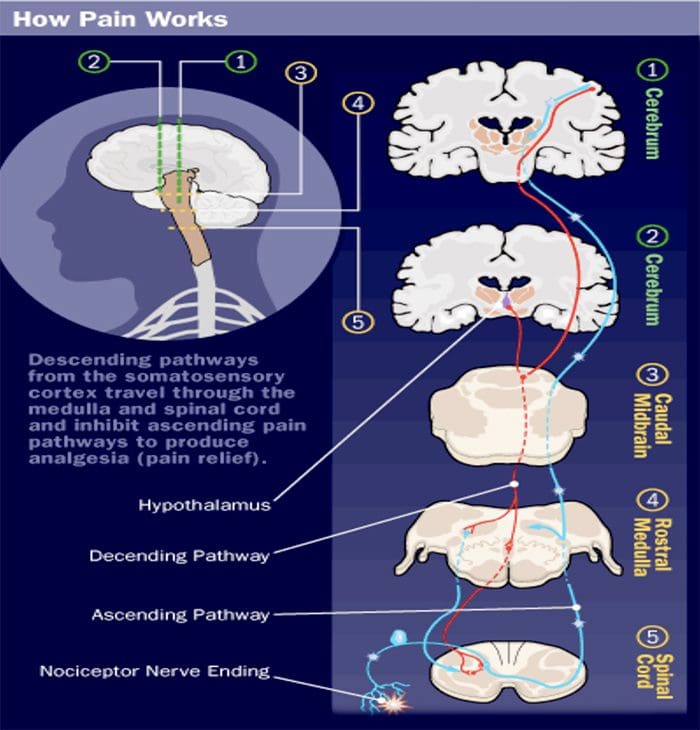
A GOOD BRAIN CAN MODULATE PAIN
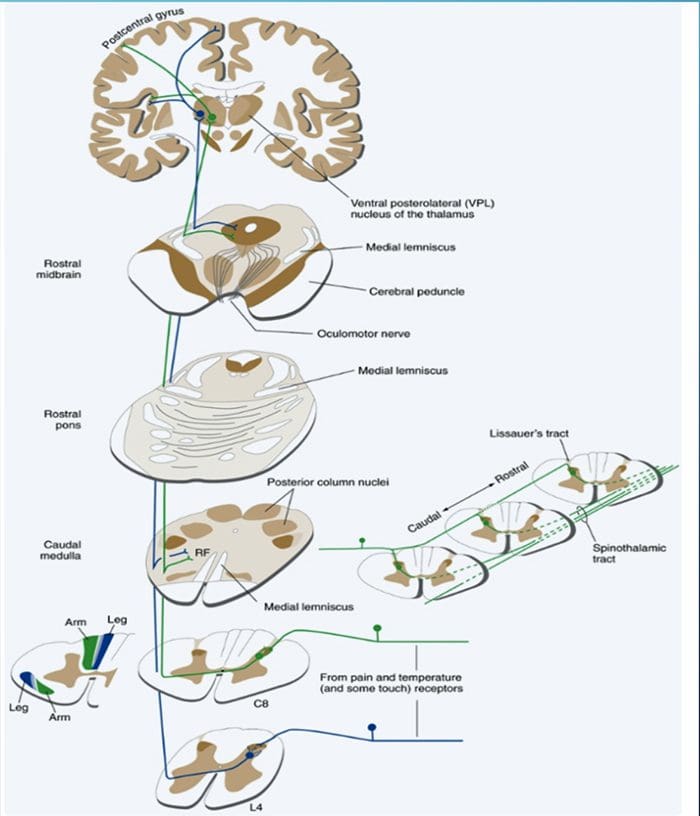
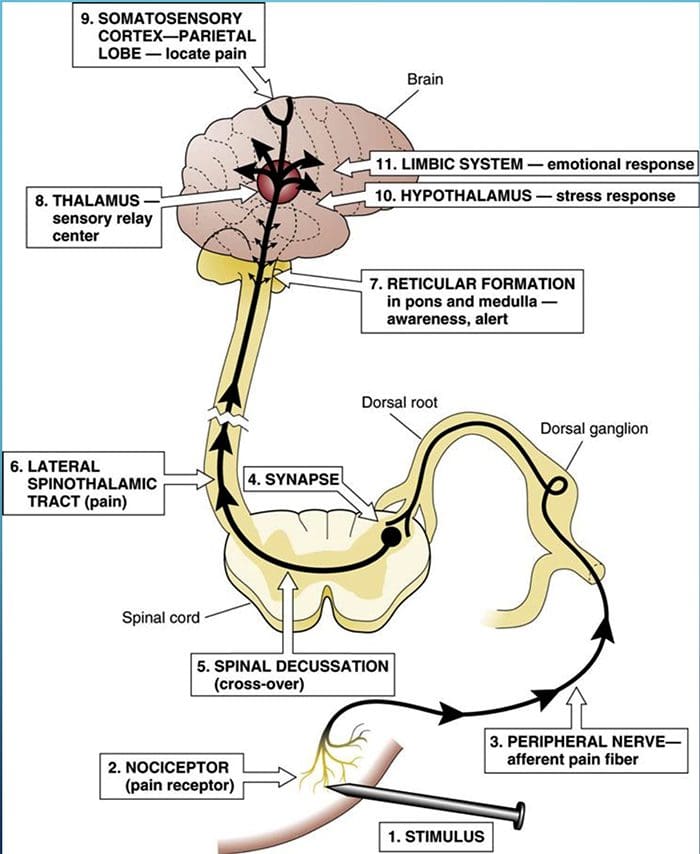
SPINOTHALAMIC TRACT
Pain is a complex sensation, in that a noxious stimulus leads not only to the perception of where it occurred but also to things such as a rapid increase in level of attention, emotional reactions, autonomic responses, and a greater likelihood that the event and its circumstances will be remembered. Corresponding to this complexity, multiple pathways convey nociceptive information rostrally from the spinal cord. One of them (the spinothalamic tract) is analogous to the posterior column�medial lemniscus pathway.
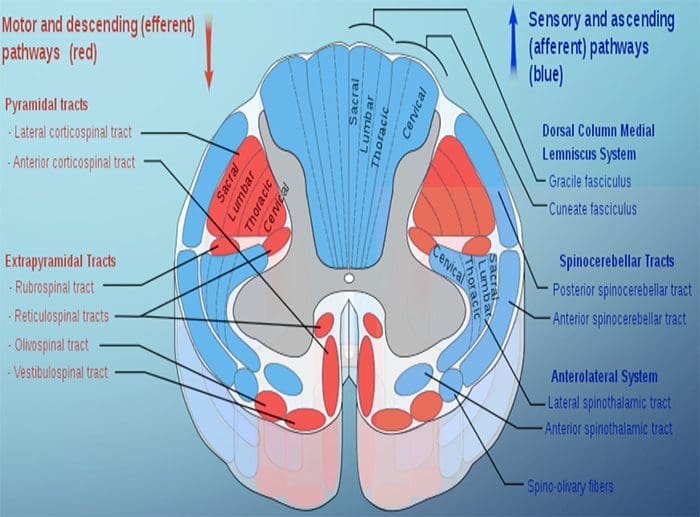
SPINOTHALAMIC TRACTS
Two main parts of the Spinothalamic Tract (STT)
Lateral Spinothalamic Tract
Transmission of pain and temperature
Anterior Spinothalamic Tract
Transmission of crude touch and firm pressure
DAMAGE TO THE ANTEROLATERAL SYSTEM CAUSES DIMINUTION OF PAIN AND TEMPERATURE SENSATIONS
Examination:
Given the role of the spinothalamic tract, the patient should be screened for any abnormalities regarding their sense of touch, pain, temperature, and pressure sensation.
Screening for such abnormalities is commonly done using gentle pin pricks and cotton wool, to contrast between sharp and soft, following cutaneous sensory nerve root distributions. Hot and cold discrimination can be ascertained using the cold metal arm of a tuning fork, and a warm palm or heated object.
2 Minute Neuroscience: Pain & The Anterolateral System
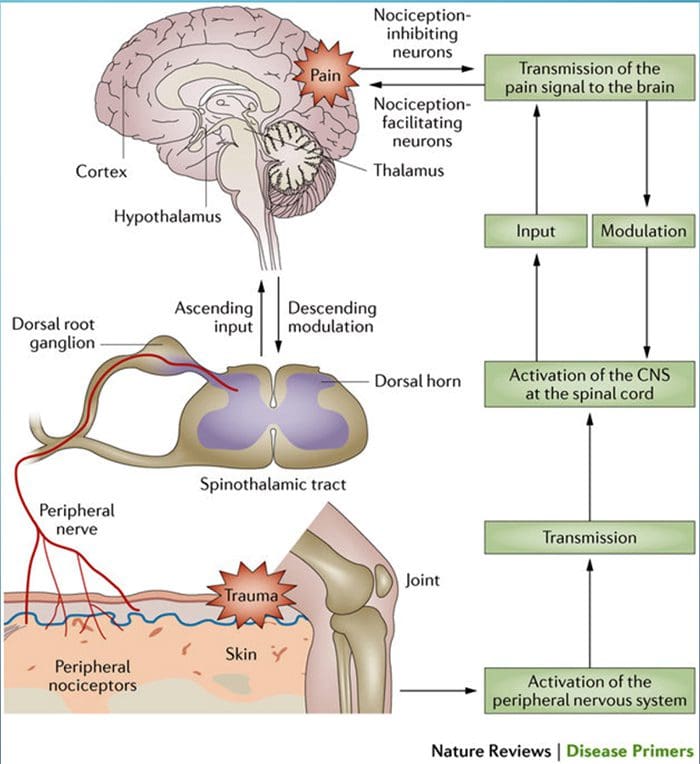
HAUSER ET AL. FIBROMYALGIA, 2015
�Pain processing and its modulation: Activation of peripheral pain receptors (also called nociceptors) by noxious stimuli generates signals that travel to the dorsal horn of the spinal cord via the dorsal root ganglion. From the dorsal horn, the signals are carried along the ascending pain pathway or the spinothalamic tract to the thalamus and the cortex. Pain can be controlled by nociception- inhibiting and nociception-facilitating neurons. Descending signals originating in the supraspinal centers can modulate activity in the dorsal horn by controlling spinal pain transmission. CNS, central nervous system.�
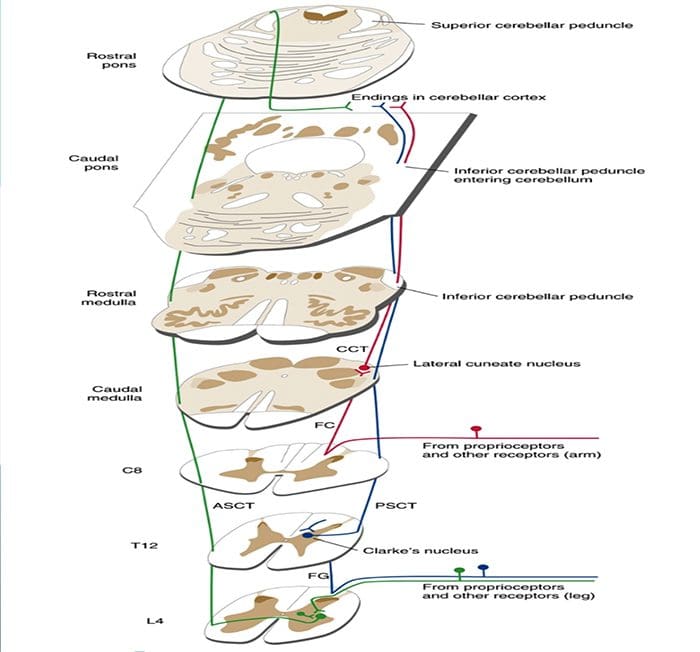
SPINAL INFORMATION REACHES THE CEREBELLUM BOTH DIRECTLY AND INDIRECTLY
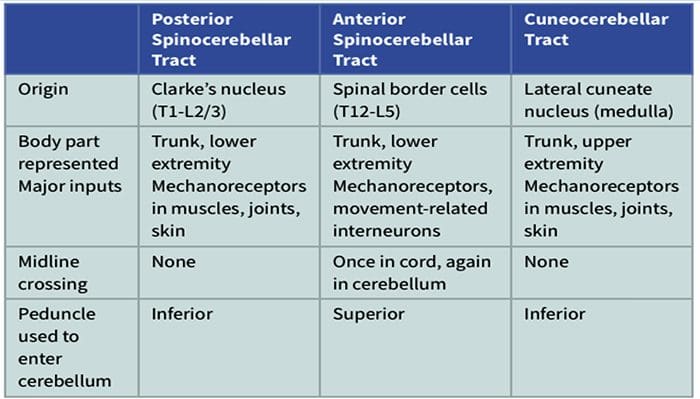
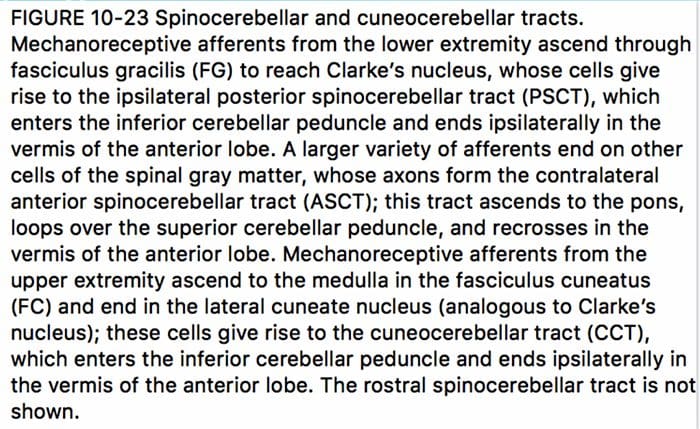
The spinal cord is an important source of information used by the cerebellum in the coordination of movement. This information reaches the cerebellar cortex and nuclei both directly, by way of spinocerebellar tracts, and indirectly, by way of relays in brainstem nuclei. A number of spinocerebellar tracts have been described, some representing the upper extremity and others the lower extremity. Only three have been well characterized.
Ascending Tracts | Spinocerebellar Tract
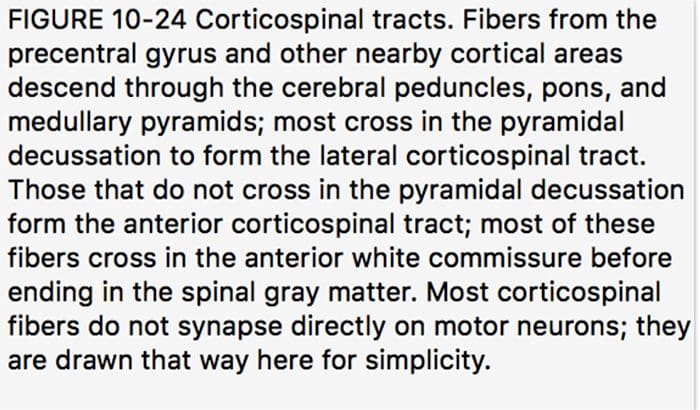
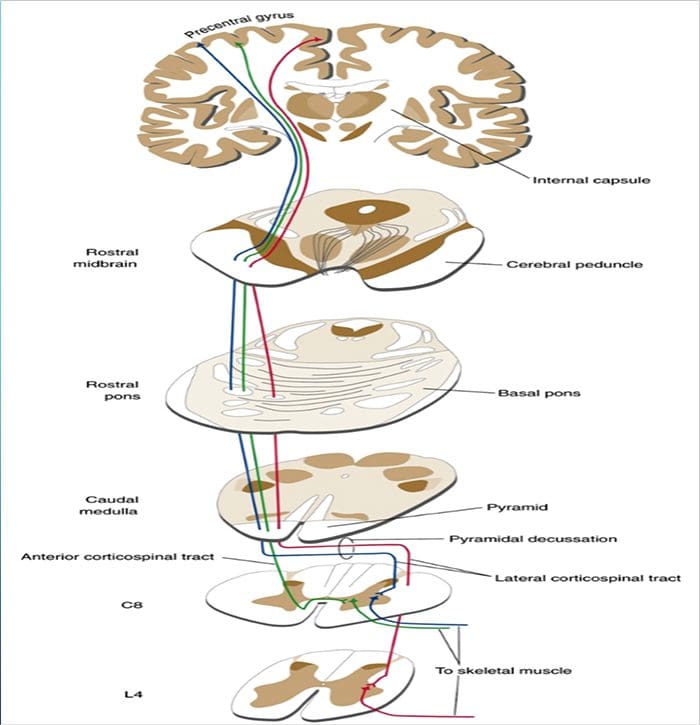
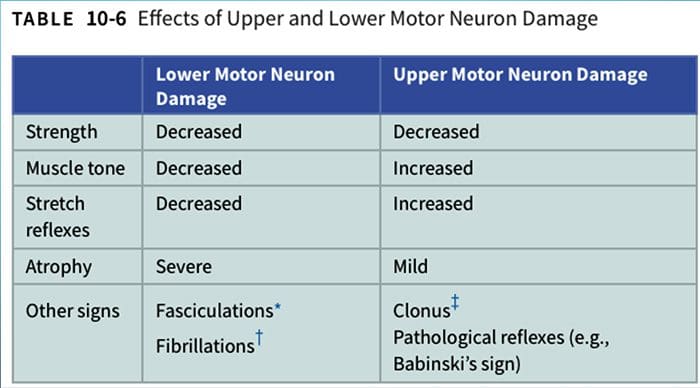
DESCENDING PATHWAYS INFLUENCE THE ACTIVITY OF LOWER MOTOR NEURONS
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


 With contractures, the sarcomeres overly lengthen when the muscle fibers tighten. This increase in sarcomere length prevents the muscle from contracting normally, resulting in weakness. Muscle fibers are encased in an extracellular matrix, a mesh composed of collagen and other proteins that help transmit force and provide muscle contraction. Muscle contractures cause the amount of collagen within the extracellular matrix to increase, causing a stiffening of fibers that restricts movement. (
With contractures, the sarcomeres overly lengthen when the muscle fibers tighten. This increase in sarcomere length prevents the muscle from contracting normally, resulting in weakness. Muscle fibers are encased in an extracellular matrix, a mesh composed of collagen and other proteins that help transmit force and provide muscle contraction. Muscle contractures cause the amount of collagen within the extracellular matrix to increase, causing a stiffening of fibers that restricts movement. (





 The term posterior column refers to the entire contents of a posterior funiculus, exclusive of its share of the propriospinal tract. The posterior columns consist mainly of ascending collaterals of large myelinated primary afferents carrying impulses from various kinds of mechanoreceptors (although substantial numbers of second-order fibers and unmyelinated fibers are also included). This has traditionally been considered the major pathway by which information from low-threshold cutaneous, joint, and muscle receptors reaches the cerebral cortex.
The term posterior column refers to the entire contents of a posterior funiculus, exclusive of its share of the propriospinal tract. The posterior columns consist mainly of ascending collaterals of large myelinated primary afferents carrying impulses from various kinds of mechanoreceptors (although substantial numbers of second-order fibers and unmyelinated fibers are also included). This has traditionally been considered the major pathway by which information from low-threshold cutaneous, joint, and muscle receptors reaches the cerebral cortex.