For individuals dealing with stress, back and neck pain, and wanting to improve overall health, can trying a Hatha yoga class help?
Hatha Yoga Class
A yoga class is great for moms, athletes, or anyone interested in low-impact exercise. Today, many practice yoga for its mind and body, health and wellness benefits. Research shows that hatha yoga helps to reduce stress, relieve back and arthritis pain, support healthy habits, and improve emotional health. (National Center for Complementary and Integrative Health, 2023) Hatha classes stretch, unwind, and release tension, providing a healthy outlet for hectic lifestyles.
What Is It?
In Sanskrit, Hatha translates to force. Hatha yoga focuses on posture and breathing techniques to channel energy. Classes last 45 to 90 minutes and consist of breathing, poses, and meditation.
Yoga can help relieve everyday anxiety and depressive symptoms.
However, it may not be effective for clinically diagnosed mental health conditions.
The reviews and published studies on yoga did not find conclusive evidence to support its effectiveness in managing anxiety disorder, depression, or PTSD.
Arthritis and Fibromyalgia
According to the NCCIH, there is limited evidence to support yoga’s benefits for osteoarthritis, rheumatoid arthritis, and fibromyalgia.
Back Pain
The American College of Physicians recommends yoga as a non-pharmacological back pain treatment. (Qaseem A. et al., 2017)
A review of studies found that yoga improves low-back pain and function with both short-term and intermediate-term benefits, and its effects are similar to those of other types of exercise. (Skelly A. C. et al., 2020)
Balance
According to 11 out of 15 reviewed studies, yoga helps to improve balance in generally healthy individuals.
Emotional Health
Yoga has a positive impact on mental health. Ten out of 14 studies reviewed showed benefits in improving resilience or general mental well-being.
Menopause
Yoga can relieve physical and psychological symptoms of menopause, including hot flashes, according to the review of 1,300 study participants.
Mindfulness
In a survey of 1,820 young adults, participants attributed increased mindfulness, motivation to participate in other forms of activity, and eating healthier. (Watts A. W. et al., 2018)
Multiple Sclerosis
The NCCIH reports showed that yoga had short-term benefits on mood and fatigue in individuals with multiple sclerosis.
However, it did not affect muscle function, cognitive function, or quality of life.
Neck Pain
A 2019 meta-analysis, including ten studies and a total of 686 subjects, found that yoga can reduce neck pain intensity and disability pain while also improving the range of motion. (Li Y. et al., 2019)
Sleep
Several studies have found yoga can improve sleep quality and duration.
Populations found to experience sleep benefits include cancer patients, older adults, individuals with arthritis, pregnant women, and women experiencing menopause symptoms.
Stress Management
Yoga improved physical or psychological stress-related measures in 12 of 17 studies reviewed.
What to Expect
There are several different styles of yoga to choose from. Classes labeled yoga are likely the Hatha variety. Hatha is a gentle style that focuses on static poses and is great for beginners. However, it can still be physically and mentally challenging. Practitioners should wear athletic clothes and sports bras for maximum comfort and ease of movement. Each class varies depending on the instructor, but most last between 45 and 90 minutes.
Class Breakdown
Classes typically start with a gentle warm-up, advance to more physical poses, and end with a short meditation.
Breathing
Most Hatha classes start with a period of focus on breathing.
As you perform the poses, the instructor will continue to remind everyone to focus on breathing and may suggest different breathing exercises.
Poses
Yoga poses, also called postures or asanas, are a series of movements that help improve balance, flexibility, and strength.
Poses range in difficulty from laying flat on the floor to physically challenging positions.
If, during a class, a pose is too difficult, the instructor can provide a modified posture.
Meditation
Most classes end with a short period of meditation.
If you go into a Hatha class and it feels too slow or inactive, there are faster-paced, more athletic yoga classes, including flow, vinyasa, or power yoga classes. See if it’s more your speed.
Injury Medical Chiropractic Clinic
At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you and strive to create fitness and better the body through research methods and total wellness programs. These programs use the body’s ability to achieve health and fitness goals, and athletes can condition themselves to excel in their sport through proper fitness and nutrition. Our providers use an integrated approach to create personalized programs, often including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles.
Home Exercises for Pain Relief
References
National Center for Complementary and Integrative Health. (2023). Yoga: What you need to know. Retrieved from https://www.nccih.nih.gov/health/yoga-what-you-need-to-know#hed11
Qaseem, A., Wilt, T. J., McLean, R. M., Forciea, M. A., Clinical Guidelines Committee of the American College of Physicians, Denberg, T. D., Barry, M. J., Boyd, C., Chow, R. D., Fitterman, N., Harris, R. P., Humphrey, L. L., & Vijan, S. (2017). Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Annals of internal medicine, 166(7), 514–530. https://doi.org/10.7326/M16-2367
Skelly, A. C., Chou, R., Dettori, J. R., Turner, J. A., Friedly, J. L., Rundell, S. D., Fu, R., Brodt, E. D., Wasson, N., Kantner, S., & Ferguson, A. J. R. (2020). Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review Update. Agency for Healthcare Research and Quality (US).
Watts, A. W., Rydell, S. A., Eisenberg, M. E., Laska, M. N., & Neumark-Sztainer, D. (2018). Yoga’s potential for promoting healthy eating and physical activity behaviors among young adults: a mixed-methods study. The international journal of behavioral nutrition and physical activity, 15(1), 42. https://doi.org/10.1186/s12966-018-0674-4
Li, Y., Li, S., Jiang, J., & Yuan, S. (2019). Effects of yoga on patients with chronic nonspecific neck pain: A PRISMA systematic review and meta-analysis. Medicine, 98(8), e14649. https://doi.org/10.1097/MD.0000000000014649
Can chiropractic treatment alleviate pain and correct swayback posture, a postural deformity that can cause lower back pain and mobility issues, for individuals experiencing it?
Swayback Posture
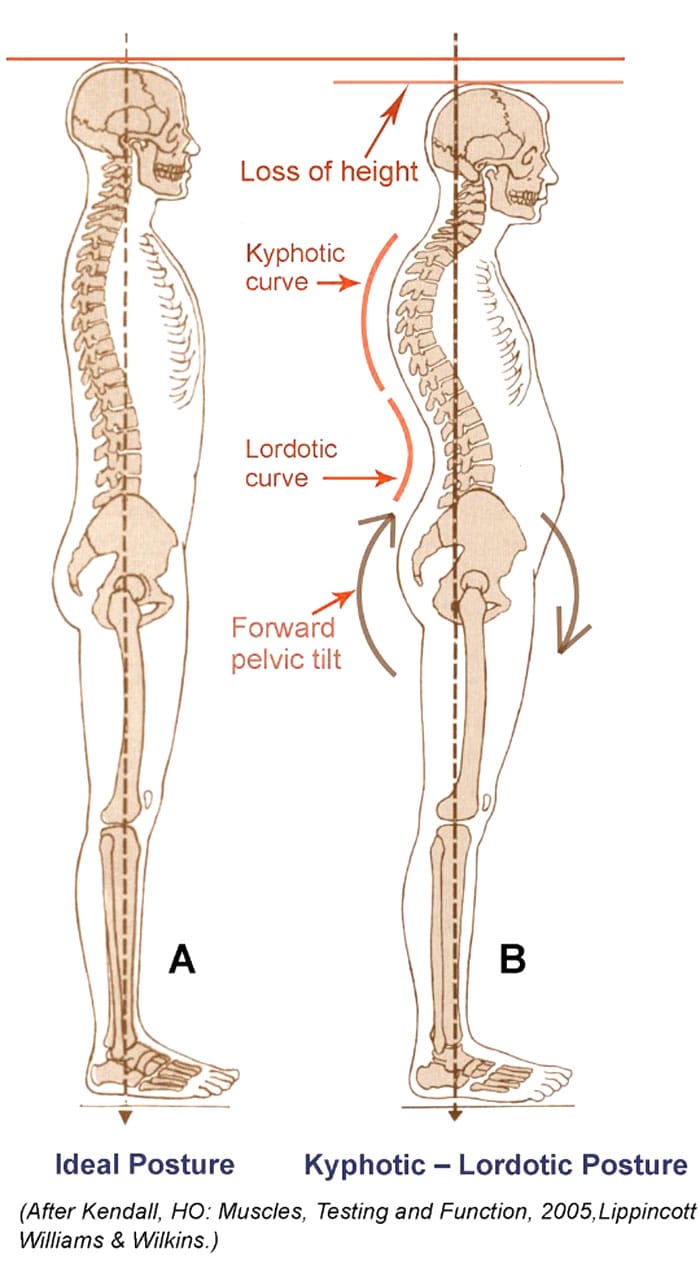
Swayback posture is a common dysfunction involving the pelvis and hip joints tilted forward in front. This causes the pelvis to shift forward, which exaggerates the curves in the lower and upper back, known as lordosis and kyphosis. The pelvis may tilt backward relative to the upper half, causing the buttocks to tuck under. The pelvis coordinates the movements of the head, shoulders, and trunk with those of the feet, legs, and thighs. A neutral pelvis, the ideal position, generally supports a mild curve/normal lordosis in the lower back. The small arch helps the body balance the skeletal parts as they work together to support and move the body’s weight. When a postural deformity occurs, one or more bones may shift from their ideal position to compensate for any pain or loss of balance caused by the original deviation. This deviation can lead to muscle strain, ligament sprain, and/or pain. (Czaprowski, D. et al., 2018)
Postural Deviations
Swayback posture causes the thoracic spine to move backward and round over into kyphosis. At the same time, the pelvis is tilted forward, resulting in an exaggeration of the normal lumbar lordosis. (Czaprowski, D. et al., 2018)
Healthcare providers, chiropractors, and physical therapists use exact measurements to define and treat postural deformities.
A neutral pelvis is a position of balance the entire body uses to help it stay upright, move, and be pain-free.
The ideal or neutral pelvic tilt is a 30-degree angle between the vertical and the plane that passes through the top of the sacrum and the axis of the hip joint socket in the front.
Swayback posture causes the pelvis to tilt forward another 10 degrees.
As a result, the spine compensates, exaggerating the curves in the lower back/lordotic curve and in the mid and upper back/kyphotic curve.
When viewed from the side, individuals can see a backward movement of the thoracic spine.
In front, the chest tends to sink in.
Muscle Group Imbalances
Healthcare providers look at different contributors or causes of postural deviations. Swayback can sometimes be associated with strength imbalances between muscle groups that move the hips, spine, and pelvis and hold the body upright. This includes:
Weakened hip flexors and overly strong or tense hip extensors/the hamstrings.
Tight upper abdominals, weak lower abdominals, and weak mid-back muscles may also contribute.
A corrective exercise program after seeing a physical therapist will help address some or all underlying muscle imbalances.
Risk Factors
Because weight in the abdominal region pulls the pelvis forward, pregnant women and obese individuals can have an increased risk of developing a swayback posture. (Vismara, L. et al., 2010)
Symptoms
The symptoms of swayback posture often include:
Severe lower back pain
Difficulty sitting or standing for long periods
Difficulty performing certain physical activities.
Tightness in the hamstrings and hip flexors
Tightness in the upper back muscles
Headaches or migraines
Chiropractic Treatment
Chiropractic adjustments are a common treatment used to correct swayback posture and can be corrected through various treatments. These include:
Spinal adjustments: The doctor applies pressure to specific spine areas to realign them and help restore proper spinal function.
Non-surgical decompression
Massage therapies
Muscle Energy Technique, or MET, improves muscle strength, flexibility, and function.
Acupuncture
Exercises to strengthen and stabilize the core muscles
Lifestyle adjustments to help reduce stress on the spine
Posture exercises
Biomechanics training
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized care plan for each patient through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility programs to relieve pain and help individuals return to optimal function. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
How I Gained My Mobility Back With Chiropractic Care
References
Czaprowski, D., Stoliński, Ł., Tyrakowski, M., Kozinoga, M., & Kotwicki, T. (2018). Non-structural misalignments of body posture in the sagittal plane. Scoliosis and spinal disorders, 13, 6. https://doi.org/10.1186/s13013-018-0151-5
Vismara, L., Menegoni, F., Zaina, F., Galli, M., Negrini, S., & Capodaglio, P. (2010). Effect of obesity and low back pain on spinal mobility: a cross sectional study in women. Journal of neuroengineering and rehabilitation, 7, 3. https://doi.org/10.1186/1743-0003-7-3
For individuals living with chronic pain and various diseases like Parkinson’s, arthritis, and diabetes, can water aerobics be beneficial?
Water Aerobics
Water aerobics are low-impact exercises performed commonly in swimming pools. It is a great way to exercise for a full-body, low-impact workout without overworking the body’s joints and muscles. Other names used include:
Aquafitness
Aqua aerobics
Aquarobics
Many types can be tailored to individual needs, injuries, and/or conditions. The exercises have various health benefits, especially for those who cannot perform higher-impact movements.
Individuals participating in water aerobics will need a bathing suit, towel, goggles, and a swim cap to protect their eyes or hair from chlorinated water. Individuals do not need other special equipment while exercising as the water acts as extra resistance. Foam dumbbells or paddles can be used to increase resistance. Other optional equipment includes: (Plunge San Diego, 2024) (Harvard Health Publishing Harvard Medical School, 2023)
Kickboards
Wrist and ankle weights
Water-jogging belts
Swim bar
Pool Exercises
There are many types of pool exercises to help reach health and fitness goals. They include:
Water Walking
The basic act of walking in water is a great way to get a full-body workout.
Start by standing in waist-deep water with the feet planted on the bottom of the pool.
Lengthen the spine by bringing the shoulders up and back and aligning the shoulders with the hips and knees.
Once in a good starting position, walk through the water, putting pressure on the heel first and then the toes, just like walking out of the water, while swinging the arms back and forth through the water.
This exercise can be done for five to 10 minutes.
The muscles that will get the most attention are the arms, core, and the lower body.
Arm Lifts
Stand up to the shoulders in water.
With the palms facing up, draw the elbows into the torso while lifting the forearms in front of the body up to the water’s surface.
Once at the surface, rotate the palms to face down and slowly move the forearms back down to the sides.
For more resistance, this exercise can also be done using foam dumbbells.
Repeat the action 10–15 times for one to three sets.
The muscles targeted are the core and the arm muscles.
Jumping Jacks
Water resistance makes jumping jacks in the water much more difficult than on land.
To perform, start by standing in chest-level water with your feet together and your arms straight down the sides.
Once in position, begin by simultaneously swinging the legs out to the side and arms over the head before returning to the starting position.
Muscles targeted include the entire body and cardiovascular system.
Add wrist or ankle weights for more resistance and to make the exercise more challenging.
High-Knee-Lift Extensions
High-knee-lift extensions are performed while standing in water that is waist deep.
To do the exercise, engage the core and lift one leg in a bent position until it is level with the water’s surface.
Hold the position for a few seconds, then extend the leg out in front and hold again.
After the hold period, move the leg back down through the water to the starting position while keeping it straight and flexing the foot.
Repeat on both legs for two to three sets of 15 reps per leg.
Use weights on the ankles to increase resistance.
The muscles targeted include the core, glutes, and lower body.
Risks
While exercising in water, individuals may not notice how much they sweat. This can make it seem like the workout is not as hard and can lead to dehydration. Individuals should always hydrate before and after a pool workout. Individuals who cannot swim well should avoid exercises that do not require a flotation device. Sometimes pools are heated, so choosing one 90 degrees F or below is recommended so the body doesn’t get overheated while exercising.
Stop Pool Exercises Immediately
Performing pool exercises can often seem easier than they are, leading to overworking. Stop exercising immediately if you feel:
Pain in any area of the body
Shortness of breath
Nauseated
Faint
Dizzy
Pressure in the upper body or chest
Other Health Conditions That Benefit
Water aerobics is recommended for most individuals, completely healthy or with a chronic disease. Those with chronic disease have been shown to benefit from the low-impact exercise. (Faíl, L. B. et al., 2022) One study looked at individuals with various health conditions, with the results showing that the following conditions saw improvements after 12 weeks of regular water exercise (Faíl, L. B. et al., 2022)
Diabetes
Arthritis
Fibromyalgia
Bone diseases
High blood pressure
Coronary artery disease
Stroke
Multiple sclerosis (MS)
Parkinson’s disease
While the benefits of water aerobics have been studied and proven effective, individuals should be cleared by a medical professional before starting any new exercise regimen. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility programs to relieve pain and help individuals return to normal. Our providers create personalized care plans for each patient. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Chiropractic and Integrative Healthcare
References
Harvard Health Publishing Harvard Medical School. (2023). Basic types of water-based exercises. HealthBeat. https://www.health.harvard.edu/healthbeat/basic-types-of-water-based-exercise
Pereira Neiva, H., Brandão Faíl, L., Izquierdo, M., Marques, M. C., & Marinho, D. A. (2018). The effect of 12 weeks of water-aerobics on health status and physical fitness: An ecological approach. PloS one, 13(5), e0198319. https://doi.org/10.1371/journal.pone.0198319
Harvard Health Publishing Harvard Medical School. (2024). Advantages of water-based exercise. HealthBeat. https://www.health.harvard.edu/healthbeat/advantages-of-water-based-exercise
Plunge San Diego. (2024). 5 must-have pieces of aquatic exercise equipment for water aerobics. Plunge San Diego. https://plungesandiego.com/what-equipment-needed-water-aerobics-shoes/
Faíl, L. B., Marinho, D. A., Marques, E. A., Costa, M. J., Santos, C. C., Marques, M. C., Izquierdo, M., & Neiva, H. P. (2022). Benefits of aquatic exercise in adults with and without chronic disease-A systematic review with meta-analysis. Scandinavian journal of medicine & science in sports, 32(3), 465–486. https://doi.org/10.1111/sms.14112
For individuals who sit at work for long hours, can years of practicing unhealthy posture be corrected through a step-by-step approach to ensure optimal body position while sitting?
Sitting Posture
Sitting up straight with a healthy posture requires the conscious alignment of the hips, pelvis, lower back, upper back, shoulders, neck, and head. Learning or retraining oneself to maintain correct sitting posture can relieve lower back pain, improve respiration and digestion, and reduce tension in the neck and shoulders. (Albarrati, A. et al., 2018) It starts by paying attention to posture throughout the day and correcting it whenever forward head posture, leaning, or slouching develops. Targeted exercises can also help build upper-body strength, and stretching can stabilize and strengthen the core muscles, lower back, and pelvic joints. (Albarrati, A. et al., 2018)
Sit Up Straight Guide
Sitting up straight can be uncomfortable because it is not a natural position for the body to be in for an extended time. Nowadays, work, school, appointments, and other activities require us to sit much longer than intended. The muscles also have to work against gravity, leading to muscle exhaustion, slouching, and slumping, which can cause chronic back, leg, neck, and/or shoulder pain. (Jung, K. S. et al., 2020)
Sitting up straight may seem simple, but the focus tends to be on straightening just the lower/lumbar spine. This posture is unsustainable and exhausts and stresses the upper and lower back. (Jung, K. S. et al., 2020) The whole body needs to be considered when protecting the stability and balance of the spine. Learning and maintaining the ability to sit up straight is a process that requires practice. Find a comfortable chair to sit in, and follow these steps to achieve the optimal postural alignment (Canadian Centre for Occupational Health and Safety, 2022)
Knee Spacing
The hips should be at a roughly 90-degree angle.
Knee Position
The knees should be at a 90-degree angle level with the hips.
Use a pillow to achieve the right knee position if the seat is too low.
Keep the Feet Flat on the Floor
If feet don’t reach the floor, place a footstool, box, book, or other flat object underneath them.
Sitting Bones
Also known as the ischial tuberosities, these are two knobby bones on the underside of the pelvis.
Feel around to find them.
Pelvis Adjustment
Shift the body so that the sitting bones are directly under the pelvis rather than situated too far back, stressing the lower back or too far forward, leading to slumping.
Spine Check
There should be a slight spinal curve, and one should be able to slip a hand between the lower back and the back of the chair.
Shoulder Check
The shoulders should be level and vertically aligned with the hips.
If the shoulder blades are pulled back or the shoulders are lifted or curled forward, relax them into a neutral position.
Head Positioning
The head tends to tilt too far forward while sitting as work and the day progresses.
Adjust the head position to align the neck with the upper spine.
The head should be slightly tilted forward, with the ears aligned with the shoulders.
Check for Pain and Discomfort
Pain may be due to structural imbalances of the spine, pelvis, or hips.
Use a lumbar chair support or place a rolled-up towel or cushion at the lower back to keep the back straight.
Added Tips
Tools and tricks to help prevent and avoid back, hip, and neck pain.
Chairs
All the bells and whistles for an ergonomic desk chair are unnecessary.
Focus on features like adjustable seat height and lumbar support. The correct seat depth recommendations are deeper if tall and shallower if short. (van Niekerk, S. M. et al., 2012)
Cushions
If sitting on a cushion or using one to bolster the back or hips, recommendations are not to go too soft.
Cushions that are too soft allow the ability to shift from one hip to the next, often without realizing it.
They usually eventually flatten and lose support.
Monitor Position
There is no point in sitting straight if the monitor is too high or too low.
The monitor should be at eye level to maintain the proper head and shoulder alignment.
If the monitor is too low, place a box or book underneath it.
If it is too high, raise the chair’s height and place a footrest under the feet to keep them flat.
Avoid Crossing Legs or Feet
Crossing the legs or feet places stress on the opposite hip, thigh, and knee and wears the body out faster.
If the hips or legs are tiring prematurely, the individual is not sitting correctly or in the wrong chair.
Use Comfortable Footwear
Maintaining flat feet on the floor while sitting is imperative.
This is not possible in high heels or platform shoes.
Change into a comfortable pair of flat shoes while sitting.
Take Regular breaks
Even with an ergonomic desk chair, the body is not meant to be sitting for hours and hours.
Get up at least every hour, walking and stretching to reactivate the muscles and circulation.
Sitting up straight requires body alignment awareness, stable core muscles, and balanced pelvis, hips, spine, shoulders, neck, and head positioning. It may take some time before these steps become normal, but they will become second nature with perseverance and practice. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution that fully benefits the individual to get back to normal. Using an integrated approach to treat injuries and chronic pain syndromes to improve ability through flexibility, mobility, and agility programs to relieve pain. Our providers create personalized care plans for each patient, including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. If other treatment is needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Posture and Mobility
References
Albarrati, A., Zafar, H., Alghadir, A. H., & Anwer, S. (2018). Effect of Upright and Slouched Sitting Postures on the Respiratory Muscle Strength in Healthy Young Males. BioMed research international, 2018, 3058970. https://doi.org/10.1155/2018/3058970
Jung, K. S., Jung, J. H., In, T. S., & Cho, H. Y. (2020). Effects of Prolonged Sitting with Slumped Posture on Trunk Muscular Fatigue in Adolescents with and without Chronic Lower Back Pain. Medicina (Kaunas, Lithuania), 57(1), 3. https://doi.org/10.3390/medicina57010003
Canadian Centre for Occupational Health and Safety. (2022). Working in a sitting position – good body position. Retrieved from https://www.ccohs.ca/oshanswers/ergonomics/sitting/sitting_position.html
van Niekerk, S. M., Louw, Q. A., & Hillier, S. (2012). The effectiveness of a chair intervention in the workplace to reduce musculoskeletal symptoms. A systematic review. BMC musculoskeletal disorders, 13, 145. https://doi.org/10.1186/1471-2474-13-145
Can the thoracolumbar fascia cause or contribute to lower back pain and inflammation?
Thoracolumbar Fascia
Tissue behind the spinal column, positioned at both the lower back and mid-back levels, is connected to the thoracolumbar fascia, also called the lumbodorsal fascia or LF. The fascia is a thick connective tissue that covers and supports all the body’s muscles, bones, tendons, ligaments, and organs. The fascia also contains nociceptive nerve endings, also known as free nerve endings, that arise from the central nervous system, i.e., the brain and spinal cord, which may be responsible for some forms of back pain and stiffness caused by injury or inflammation.
Anatomy
The thoracolumbar fascia is divided into three layers:
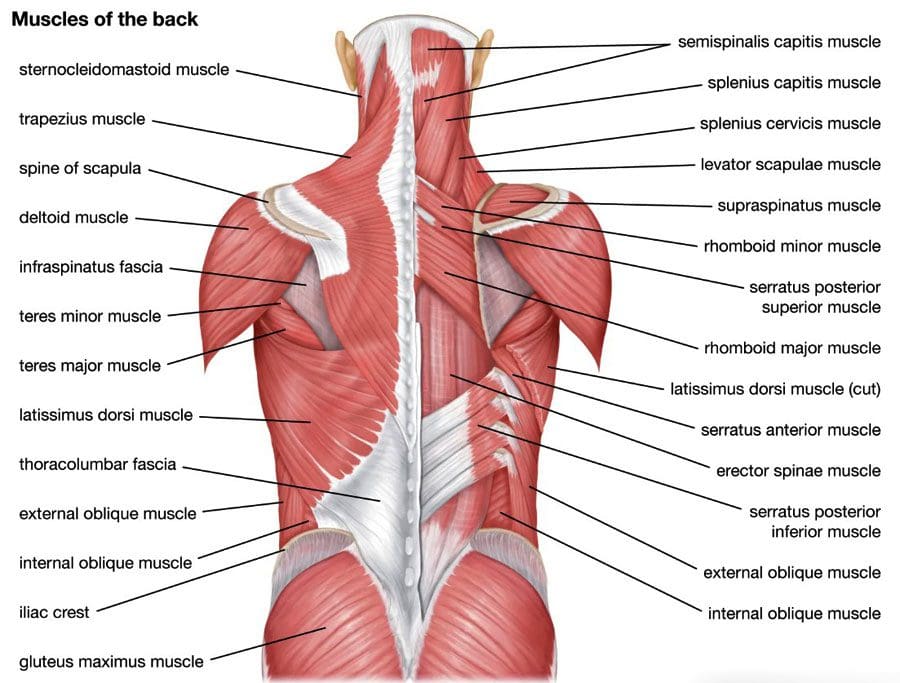
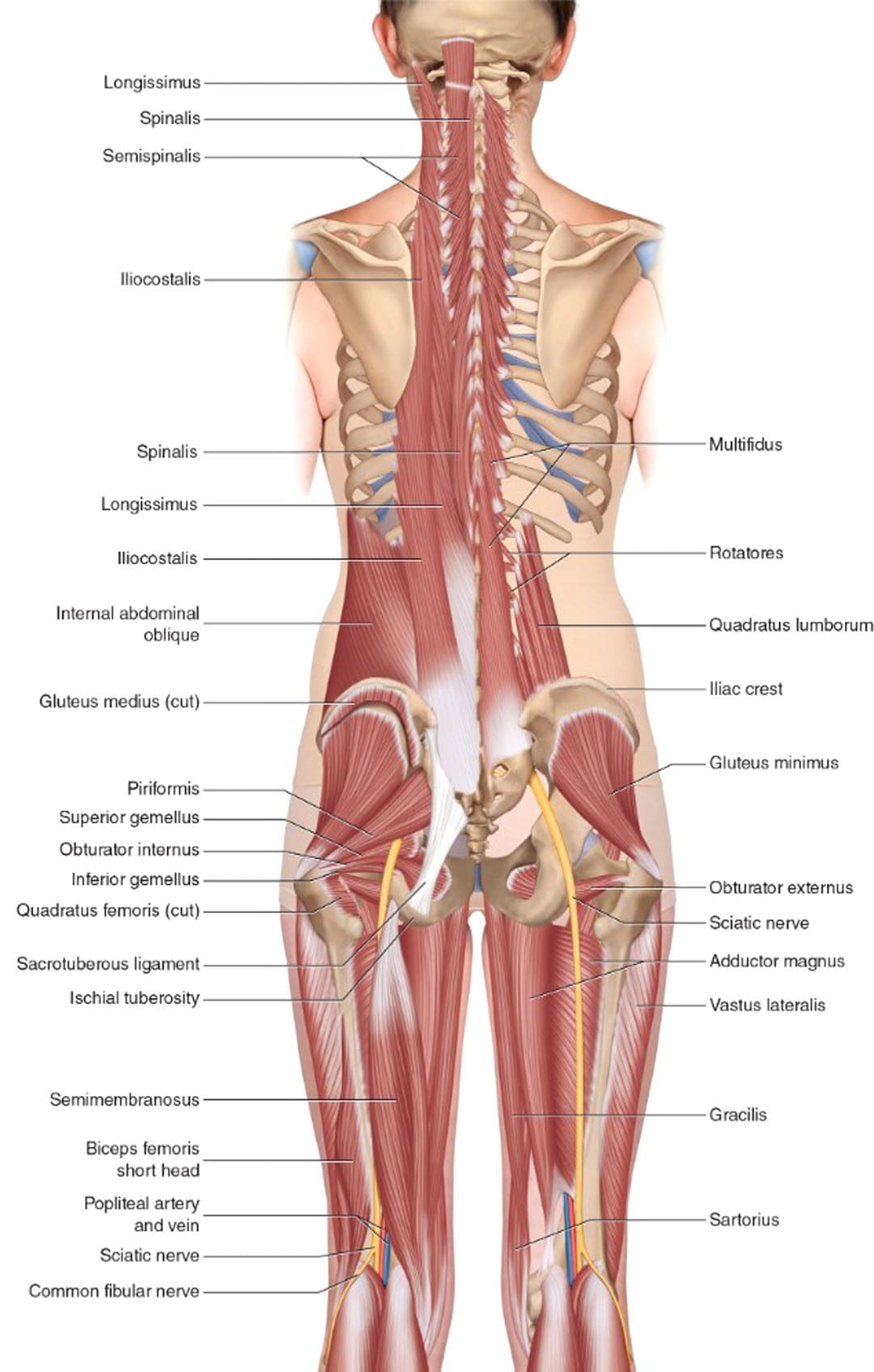
Many of the back muscles attach to the thoracolumbar fascia. The erector spinae muscle group, known as the paraspinals, runs longitudinally down the spine. They are attached to the thoracolumbar fascia and the bony spine. The lumbar part of the posterior layer of the thoracolumbar fascia extends from the lowest rib to the top of the hip bone or the iliac crest. On the same path, it connects with the transverse abdominal muscle. The thoracolumbar fascia connections help bridge the back muscles to the abdominal wall muscles. The latissimus dorsi, a large back muscle that bears and moves the body’s weight with the arms and shoulders, is also connected to the thoracolumbar fascia, with the fibers extending outward from the fascia. The front part of the thoracolumbar fascia, or anterior layer, covers a muscle called the quadratus lumborum. This muscle bends the trunk to the side, helps maintain a healthy posture, and is often focused on muscle-related lower back pain.
What the Fascia Does
The thoracolumbar fascia, examined from the back of an anatomical drawing or diagram, is diamond-shaped. Its shape, large size, and central location uniquely position it to unify and synchronize the upper body’s movements with the lower body’s. The fascia’s fibers are very strong, enabling the tissue sheath to lend support (Willard, F. H. et al., 2012) . The tissue is also flexible, enabling it to help circulate forces of movement and contralateral movements as the back muscles contract and relax. An example is walking.
Back Pain
Scientists and doctors don’t know for sure, but it’s possible that the thoracolumbar fascia may contribute to lower back pain. A study found that the fascia may generate back pain based on: (Wilke, J. et al., 2017)
Sustaining micro-injuries and/or inflammation, which are often related, may cause signal changes in the free nerve endings in the fascia. Nerve endings acquire information from the outer areas of the body, like skin and other fascia, and relay it back to the central nervous system. The theory is that when the fascia close to the skin becomes injured, damaged, and/or backed up with inflammatory chemicals and substances, it is communicated as pain and other sensations back to the brain and spinal cord.
After a back injury, tissues tighten and stiffen. Some studies of patients with back pain noted alterations in their thoracolumbar fascia.
Injuries tend to stimulate nerves, which can lead to increased sensitivity.
Injury Medical Chiropractic and Functional Medicine Clinic focuses on and treats injuries and chronic pain syndromes through personalized care plans that improve ability through flexibility, mobility, and agility programs to relieve pain. Our providers use an integrated approach to create personalized care plans for each patient, including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Our goal is to relieve pain naturally by restoring health and function to the body. If other treatment is needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Sciatica, Causes, Symptoms, and Tips
References
Willard, F. H., Vleeming, A., Schuenke, M. D., Danneels, L., & Schleip, R. (2012). The thoracolumbar fascia: anatomy, function and clinical considerations. Journal of anatomy, 221(6), 507–536. https://doi.org/10.1111/j.1469-7580.2012.01511.x
Wilke, J., Schleip, R., Klingler, W., & Stecco, C. (2017). The Lumbodorsal Fascia as a Potential Source of Low Back Pain: A Narrative Review. BioMed research international, 2017, 5349620. https://doi.org/10.1155/2017/5349620
Can incorporating electrical muscle stimulation help control pain, strengthen muscles, increase physical function, retrain lost movements, and/or manage inflammation for individuals experiencing neck and back pain?
Female doctor placing myostimulation physical therapy equipment on patient’s back
Electric Muscle Stimulation
Electrical muscle stimulation or E-stim is a physical therapy used to reactivate the muscles’ ability to contract. E-stim uses devices that transmit electrical impulses through the skin to target nerves and/or muscles. The most common forms include
Transcutaneous electric nerve stimulation, or TENS, is the most well-known type of electrical stimulation that offers devices that can be used at home or on the go.
Electrical muscle stimulation or EMS.
In physical therapy, E-stim stimulates muscles to contract, strengthening them and encouraging blood circulation.
Blood circulation can directly affect the condition of muscle tissue.
Electrical muscle stimulation is also used in spinal cord injury and other neuromuscular conditions. (Ho, C. H. et al., 2014)
E-stim
During treatment, electrodes are hooked to an electric stimulation machine and placed around the affected neck or back area.
The electrodes will be placed on the skin for most neck or back injuries.
The placement of the electrodes depends on the reason for treatment and the depth or superficiality of the electrical stimulation.
The electrodes are often placed near a motor point of a muscle to ensure the correct contraction.
The therapist will adjust the controls of the stimulation machine to achieve thorough muscle contraction with minimal discomfort.
Stimulation can last 5 – 15 minutes, depending on the treatment plan and injury severity.
Spinal Joint Stabilization
Activation of the muscles may help increase spinal joint stability, improving problems with spinal instability. (Ho, C. H. et al., 2014) Electric muscle stimulation is thought to enhance the exercise program a therapist prescribes to help maintain joint stability. Electrical stimulation may also help build muscle strength and endurance. (Veldman, M. P. et al., 2016) Muscle endurance is the repetitions a muscle can contract before it fatigues.
Healing and Pain Management
Electric muscle stimulation therapy can enhance tissue healing and help manage inflammation by reducing swelling and increasing circulation. It can reduce pain sensations by blocking nerve transmission at the spinal cord. (Johnson, M. I. et al., 2019) A healthcare professional may suggest a TENS or take-home electric stimulation unit to manage symptoms. (Johnson, M. I. et al., 2019)
Treatment
Interdisciplinary therapies tailored to an individual’s specific back or neck pain have been found to provide positive results. Exercise, yoga, short-term cognitive behavioral therapy, biofeedback, progressive relaxation, massage, manual therapy, and acupuncture are recommended for neck or back pain. (Chou, R. et al., 2018) Taking non-steroidal anti-inflammatory medications may also help. Electrical muscle stimulation could be an effective neck or back treatment.
Individuals unsure whether they need or would benefit from electrical should discuss symptoms and conditions with a primary physician, healthcare provider, or specialist to guide them in the right direction and determine the best treatment. Injury Medical Chiropractic and Functional Medicine Clinic focuses on what works for the patient and strives to better the body through researched methods and total wellness programs. Using an integrated approach, we treat injuries and chronic pain syndromes through personalized care plans that improve ability through flexibility, mobility, and agility programs personalized to the individual to relieve pain. If other treatment is needed, Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective treatments.
Thoracic Spine Pain
References
Ho, C. H., Triolo, R. J., Elias, A. L., Kilgore, K. L., DiMarco, A. F., Bogie, K., Vette, A. H., Audu, M. L., Kobetic, R., Chang, S. R., Chan, K. M., Dukelow, S., Bourbeau, D. J., Brose, S. W., Gustafson, K. J., Kiss, Z. H., & Mushahwar, V. K. (2014). Functional electrical stimulation and spinal cord injury. Physical medicine and rehabilitation clinics of North America, 25(3), 631–ix. https://doi.org/10.1016/j.pmr.2014.05.001
Veldman, M. P., Gondin, J., Place, N., & Maffiuletti, N. A. (2016). Effects of Neuromuscular Electrical Stimulation Training on Endurance Performance. Frontiers in physiology, 7, 544. https://doi.org/10.3389/fphys.2016.00544
Johnson, M. I., Jones, G., Paley, C. A., & Wittkopf, P. G. (2019). The clinical efficacy of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain: a protocol for a meta-analysis of randomised controlled trials (RCTs). BMJ open, 9(10), e029999. https://doi.org/10.1136/bmjopen-2019-029999
Chou, R., Côté, P., Randhawa, K., Torres, P., Yu, H., Nordin, M., Hurwitz, E. L., Haldeman, S., & Cedraschi, C. (2018). The Global Spine Care Initiative: applying evidence-based guidelines on the non-invasive management of back and neck pain to low- and middle-income communities. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 27(Suppl 6), 851–860. https://doi.org/10.1007/s00586-017-5433-8
Can a rowing machine provide a full-body workout for individuals looking to improve fitness?
A group of people exercise in the gym using a rowing machine together. A side view of a sportswoman exercising on a rowing machine in a CrossFit center. A muscular girl and a sporty man are working out on a training simulator at a CrossFit gym.
Rowing Machine
Today, rowing machines are widely recognized as effective fitness tools. They can be found in gyms, fitness centers, physical therapy, and sports rehabilitation clinics. Rowing is low-impact, allowing control of movement and pace, and is recommended for active recovery. It’s sometimes recommended as an exercise for individuals with early stages of osteoarthritis.
Benefits
The benefits include:
Rowing is a total-body workout that strengthens major muscle groups in the arms, legs, and core and increases cardiovascular endurance.
The upper and lower body are used on every stroke.
Strengthens and tones the muscles.
Rowing burns significant calories without placing added stress on the joints.
Improves endurance and heart and lung health.
Cardiovascular Fitness
Rowing is a rare exercise that involves power and endurance. It is an aerobic exercise that increases the body’s heart rate and oxygen, improving cardiovascular fitness. (Hansen RK, et al. 2023) Through continuous, rhythmic movement, which increases oxygen utilization, rowing enhances the heart and lungs’ ability to supply oxygen to the body and works on muscular endurance.
Full-Body Workout
A rowing workout is a comprehensive full-body workout that simultaneously works multiple body areas and muscle groups, specifically the arms, back, core, and legs. The motion moves major muscle groups through the full range of motion, promoting flexibility and muscle tone improvements that are great for individuals with trouble with weight-bearing exercises like running. Rowing can also improve physiological markers, depending on the intensity of the workout and the heart rate zone maintained.
Joint-Friendly
Rowing is a low-impact exercise, making it easier on joints and suitable for individuals with joint concerns or those looking for a joint-friendly workout. The workout engages the largest muscles in a low-impact way with no pounding on the joints or excessive rotation.
Burns Calories
Rowing can be an efficient way to burn calories. Its cardiovascular and resistance training combination makes it an effective tool for weight management and weight loss. Alternating between higher and lower intensities can enhance calorie burning during and after the exercise session from excess post-exercise oxygen consumption (EPOC),also known as the afterburn effect. (Sindorf, M. A. G. et al., 2021)
Improves Posture
Maintaining a healthy posture offers numerous benefits, such as improving breathing ability, aiding in digestion, and preventing injuries. (Kim D, 2015) Rowing can be an effective workout that enhances postural strength and awareness and reduces back pain risks. Proper spine activation is necessary for efficient rowing, which also helps to pull the shoulders back. The hip flexors help to lengthen during the drive phase while the shoulders open. Proper rowing technique involves:
Dorsiflexion of the foot.
Stretching of the Achilles tendon.
Engaging the tibialis.
Getting Started
Rowing is not too difficult to get started. Following techniques shared by experts will help improve the experience and reduce the risk of injury.
Maintaining Upright Posture
The back should be straight throughout the movement.
Brace the core muscles to keep the back from rounding while bending at the knees and hips during the movement.
This keeps the body aligned, prevents injuries, and makes the exercise more effective.
Maintain Stroke Sequences
There are four parts to the sequence:
The catch – is when you sit at the front of the machine with your knees bent and arms reaching out to hold the handle.
The drive – is the next step, which involves pushing into the platform with your heels and driving through your legs while engaging your legs, glutes, and core. During the drive, you want to lean back slightly as you push with your legs while pulling the handle to the bottom of the rib cage.
The finish – lean back a little more while pulling the handle to the lower chest level.
The recovery – extend your arms forward while bending the hips to bring the torso forward, using your legs to pull back to the starting position.
Adjust Resistance Accordingly
Most rowing machines have adjustable resistance settings. Beginners should start with a lower resistance level to focus on proper technique and gradually increase as they become more comfortable so that the resistance provides a challenge without compromising form. On a rowing machine, the individual should feel like they are gliding efficiently over water with strong, powerful strokes repeated for however many reps depending on the workout.
Breathing
Aerobic workouts require proper breathing. It is recommended to inhale during the recovery phase as you slide the seat forward and exhale during the drive phase when pushing through the legs. Breathing in sync with the rowing motion keeps the oxygen flow going, so the body maintains energy and smooth strokes.
Injury Medical Chiropractic and Functional Medicine Clinic
As with any fitness program, individuals should consult a healthcare professional or fitness expert, especially if pre-existing health conditions or concerns exist. At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you and strive to better the body through researched methods and total wellness programs. We focus on treating patients’ injuries and chronic pain syndromes to create personalized care plans that improve ability through flexibility, mobility, and agility programs personalized to the individual. Using an integrated approach, our goal is to relieve pain naturally by restoring health and function to the body through Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine protocols. If other treatment is needed, Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective treatments available.
Core Exercises and Back Pain
References
Hansen, R. K., Samani, A., Laessoe, U., Handberg, A., Mellergaard, M., Figlewski, K., Thijssen, D. H. J., Gliemann, L., & Larsen, R. G. (2023). Rowing exercise increases cardiorespiratory fitness and brachial artery diameter but not traditional cardiometabolic risk factors in spinal cord-injured humans. European journal of applied physiology, 123(6), 1241–1255. https://doi.org/10.1007/s00421-023-05146-y
Sindorf, M. A. G., Germano, M. D., Dias, W. G., Batista, D. R., Braz, T. V., Moreno, M. A., & Lopes, C. R. (2021). Excess Post-Exercise Oxygen Consumption and Substrate Oxidation Following High-Intensity Interval Training: Effects of Recovery Manipulation. International journal of exercise science, 14(2), 1151–1165.
Kim, D., Cho, M., Park, Y., & Yang, Y. (2015). Effect of an exercise program for posture correction on musculoskeletal pain. Journal of physical therapy science, 27(6), 1791–1794. https://doi.org/10.1589/jpts.27.1791
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine








 What the Fascia Does
What the Fascia Does










