Individuals who participate in physical and sports activities could suffer an Achilles tendon tear. Can understanding the symptoms and risks help in treatment and return the individual back to their sports activity sooner?
Achilles Tendon
This is a common injury that occurs when the tendon attaching the calf muscle to the heel gets torn.
About the Tendon
The Achilles tendon is the largest tendon in the body.
In sports and physical activities, intense explosive movements like running, sprinting, quickly shifting positions, and jumping are exerted on the Achilles.
The injury often occurs without any contact or collision but rather the running, starting, stopping, and pulling actions placed on the feet.
Certain antibiotics and cortisone shots can increase the likelihood of Achilles tear injuries.
A specific antibiotic, fluoroquinolones, has been shown to increase the risk of Achilles tendon problems.
Cortisone shots are also associated with Achilles tears, which is why many healthcare providers don’t recommend cortisone for Achilles tendonitis. (Anne L. Stephenson et al., 2013)
Symptoms
A tendon tear or rupture causes sudden pain behind the ankle.
Individuals may hear a pop or a snap and often report the feeling as being kicked in the calf or heel.
Individuals have difficulty pointing their toes downward.
Individuals may have swelling and bruising around the tendon.
A healthcare provider will examine the ankle for continuity of the tendon.
Squeezing the calf muscle is supposed to cause the foot to point downwards, but in individuals with a tear, the foot will not move, resulting in positive results on the Thompson test.
A defect in the tendon can usually be felt after a tear.
X-rays may be used to rule out other conditions, including ankle fracture or ankle arthritis.
Fluoroquinolone antibiotics are commonly used for the treatment of respiratory infections, urinary tract infections, and bacterial infections. These antibiotics are associated with Achilles tendon rupture, but further research is needed to determine how they affect the Achilles tendon. Individuals taking these medications are advised to consider an alternative medication if Achilles tendon problems begin to develop. (Anne L. Stephenson et al., 2013)
Treatment
Depending on the severity of the injury, treatment can consist of non-surgical techniques or surgery.
The benefit of surgery is there is usually less immobilization.
Individuals can often return to sports activities sooner, and there is less chance of re-rupturing the tendon.
Thevendran, G., Sarraf, K. M., Patel, N. K., Sadri, A., & Rosenfeld, P. (2013). The ruptured Achilles tendon: a current overview from biology of rupture to treatment. Musculoskeletal surgery, 97(1), 9–20. https://doi.org/10.1007/s12306-013-0251-6
Stephenson, A. L., Wu, W., Cortes, D., & Rochon, P. A. (2013). Tendon Injury and Fluoroquinolone Use: A Systematic Review. Drug safety, 36(9), 709–721. https://doi.org/10.1007/s40264-013-0089-8
Pedowitz, D., & Kirwan, G. (2013). Achilles tendon ruptures. Current reviews in musculoskeletal medicine, 6(4), 285–293. https://doi.org/10.1007/s12178-013-9185-8
Yasui, Y., Tonogai, I., Rosenbaum, A. J., Shimozono, Y., Kawano, H., & Kennedy, J. G. (2017). The Risk of Achilles Tendon Rupture in the Patients with Achilles Tendinopathy: Healthcare Database Analysis in the United States. BioMed research international, 2017, 7021862. https://doi.org/10.1155/2017/7021862
Athletes and physically active individuals who participate in activities, exercises, and sports that involve kicking, pivoting, and/or shifting directions can develop pelvis overuse injury of the pubic symphysis/joint at the front of the pelvis known as osteitis pubis. Can recognizing the symptoms and causes help in treatment and prevention?
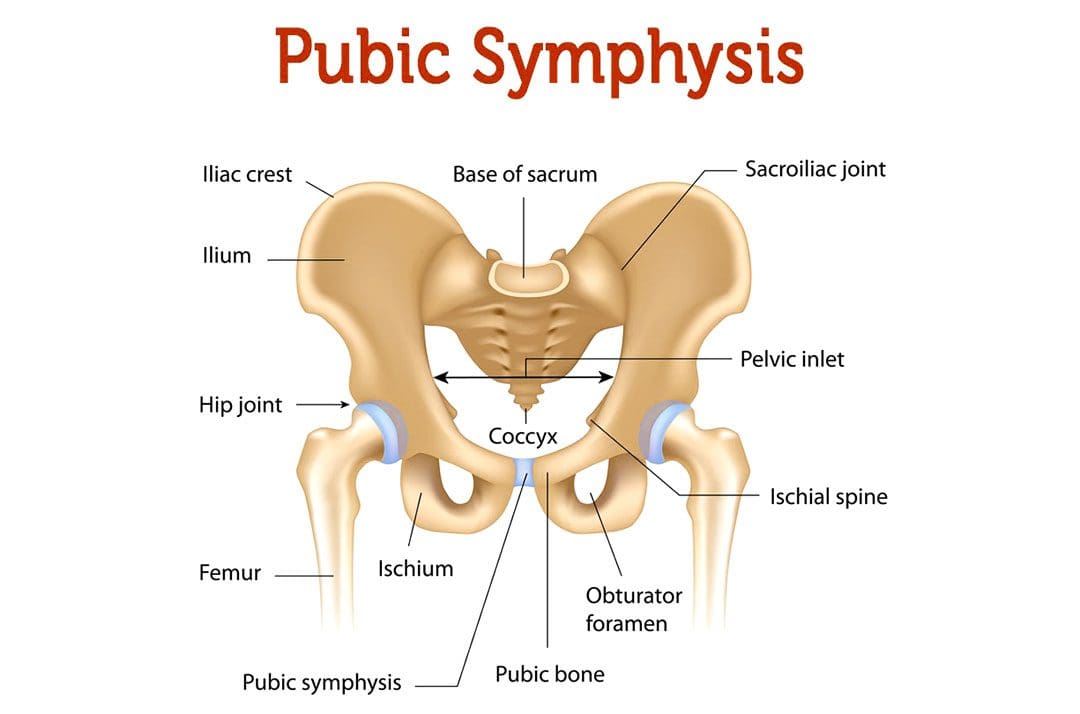
Osteitis Pubis Injury
Osteitis pubis is the inflammation of the joint that connects the pelvic bones, called the pelvic symphysis, and the structures around it. The pubic symphysis is a joint in front of and below the bladder. It holds the two sides of the pelvis together in the front. The pubis symphysis has very little motion, but when abnormal or continued stress is placed on the joint, groin and pelvic pain can present. An osteitis pubis injury is a common overuse injury in physically active individuals and athletes but can also occur as the result of physical trauma, pregnancy, and/or childbirth.
Symptoms
The most common symptom is pain over the front of the pelvis. The pain is most often felt in the center, but one side may be more painful than the other. The pain typically radiates/spreads outward. Other signs and symptoms include: (Patrick Gomella, Patrick Mufarrij. 2017)
Lower abdominal pain in the center of the pelvis
Limping
Hip and/or leg weakness
Difficulty climbing stairs
Pain when walking, running, and/or shifting directions
Clicking or popping sounds with movement or when shifting directions
Pain when lying down on the side
Pain when sneezing or coughing
Osteitis pubis can be confused with other injuries, including a groin strain/groin pull, a direct inguinal hernia, ilioinguinal neuralgia, or a pelvic stress fracture.
Causes
An osteitis pubis injury usually occurs when the symphysis joint is exposed to excessive, continued, directional stress and overuse of the hip and leg muscles. Causes include: (Patrick Gomella, Patrick Mufarrij. 2017)
Sports activities
Exercising
Pregnancy and childbirth
Pelvic injury like a severe fall
Diagnosis
The injury is diagnosed based on a physical examination and imaging tests. Other tests may be used to rule out other possible causes.
The physical exam will involve manipulation of the hip to place tension on the rectus abdominis trunk muscle and adductor thigh muscle groups.
Pain during the manipulation is a common sign of the condition.
Individuals may be asked to walk to look for irregularities in gait patterns or to see if symptoms occur with certain movements.
X-rays will typically reveal joint irregularities as well as sclerosis/thickening of the pubic symphysis.
Magnetic resonance imaging – MRI may reveal joint and surrounding bone inflammation.
Some cases will show no signs of injury on an X-ray or MRI.
Treatment
Effective treatment can take several months or longer. Because inflammation is the underlying cause of symptoms, the treatment will often involve: (Tricia Beatty. 2012)
Rest
Allows the acute inflammation to subside.
During recovery, sleeping flat on the back may be recommended to reduce pain.
Ice and Heat Applications
Ice packs help reduce inflammation.
The heat helps ease pain after the initial swelling has gone down.
Physical Therapy
Physical therapy can be extremely helpful in treating the condition to help regain strength and flexibility. (Alessio Giai Via, et al., 2019)
Anti-inflammatory Medication
Over-the-counter nonsteroidal anti-inflammatory medications – NSAIDs like ibuprofen and naproxen can reduce pain and inflammation.
Assistive Walking Devices
If the symptoms are severe, crutches or a cane may be recommended to reduce stress on the pelvis.
Cortisone
There have been attempts to treat the condition with cortisone injections, but the evidence supporting its use is limited and needs further research. (Alessio Giai Via, et al., 2019)
Prognosis
Once diagnosed, the prognosis for full recovery is optimal but can take time. It can take some individuals six months or more to return to pre-injury level of function, but most return by around three months. If conservative treatment fails to provide relief after six months, surgery could be recommended. (Michael Dirkx, Christopher Vitale. 2023)
Sports Injuries Rehabilitation
References
Gomella, P., & Mufarrij, P. (2017). Osteitis pubis: A rare cause of suprapubic pain. Reviews in urology, 19(3), 156–163. https://doi.org/10.3909/riu0767
Beatty T. (2012). Osteitis pubis in athletes. Current sports medicine reports, 11(2), 96–98. https://doi.org/10.1249/JSR.0b013e318249c32b
Via, A. G., Frizziero, A., Finotti, P., Oliva, F., Randelli, F., & Maffulli, N. (2018). Management of osteitis pubis in athletes: rehabilitation and return to training – a review of the most recent literature. Open access journal of sports medicine, 10, 1–10. https://doi.org/10.2147/OAJSM.S155077
Dirkx M, Vitale C. Osteitis Pubis. [Updated 2022 Dec 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556168/
Individuals suffering from hip, thigh, and/or groin pain could be experiencing iliopsoas syndrome. Could knowing the symptoms and causes help in diagnosis and treatment?
Iliopsoas Syndrome
Iliopsoas syndrome encompasses several conditions that affect the inner hip muscle and can cause hip and thigh pain. The muscle helps to bend the leg toward the body.
The condition is usually caused by overuse injuries and commonly affects individuals who perform repeated hip flexion movements, like cyclists, gymnasts, dancers, runners, and soccer players. (Liran Lifshitz, et al., 2020)
The term is often used interchangeably with psoas syndrome, iliopsoas tendonitis, snapping hip syndrome, and iliopsoas bursitis. However, there are clinical differences.
Hip or groin clicking or snapping that can be heard and/or felt during movement.
Pain and/or stiffness in the hip and thigh area.
Pain that worsens when bending the hip – walking, climbing stairs, squatting, sitting.
Movements that involve bringing the knee toward the chest can worsen the pain.
Causes
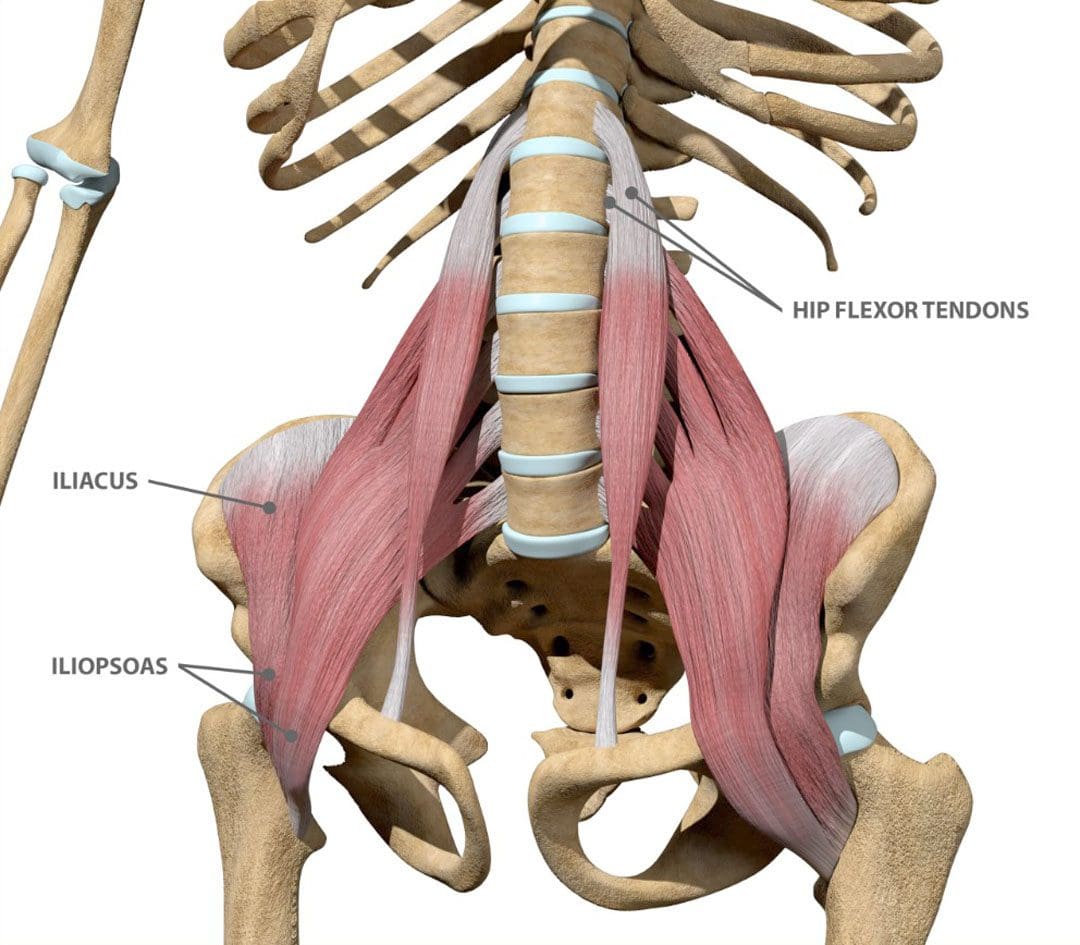
The iliopsoas muscles are hip muscles on the front of the hip. They are made up of the psoas major, the psoas minor, and the iliacus. Small, fluid-filled sacs/bursae are within the hip joint between bones and soft tissues. The bursae reduce friction and provide cushioning to help the tendons, muscles, and other structures move smoothly over the bony prominences.
Iliopsoas bursitis happens when the bursa, which is located between the iliopsoas tendon and the inside of the hip joint, becomes inflamed and irritated.
Iliopsoas tendonitis/hip tendonitis happens when the tendon that attaches the thigh bone to the iliopsoas muscle becomes inflamed and irritated.
Iliopsoas bursitis and tendonitis are commonly caused by overuse injuries and intense activities like cycling, running, rowing, or strength training.
Diagnosis
Healthcare providers can diagnose iliopsoas syndrome based on symptom history and a hip examination.
Imaging tests – MRI and X-rays may be used to rule out other injuries or conditions like muscle tears. (Paul Walker, et al., 2021)
Avoid putting weight on the hip for a few days after the injury.
Ice
Apply ice immediately after the injury to bring the swelling down.
Use a cold pack for 20 minutes at a time, several times a day.
Do not apply ice directly on the skin.
Compression
Wrap the area in a soft bandage or use compression shorts to prevent further swelling.
Elevation
Rest as often as possible with the leg raised higher than the heart.
Medical Treatment
Non-steroidal anti-inflammatory drugs like ibuprofen and naproxen sodium can alleviate pain and reduce inflammation. (Paul Walker, et al., 2021)
Steroid injections can be used if symptoms continue or come back with additional injections administered as necessary. (Paul Walker, et al., 2021)
After pain and swelling subside, physical therapy may be recommended, as well as mild exercises to gradually improve hip strength and flexibility. (Paul Walker, et al., 2021)
A healthcare provider may recommend surgery in severe cases where pain persists, and conservative treatments don’t provide enough relief.
Lifshitz, L., Bar Sela, S., Gal, N., Martin, R., & Fleitman Klar, M. (2020). Iliopsoas the Hidden Muscle: Anatomy, Diagnosis, and Treatment. Current sports medicine reports, 19(6), 235–243. https://doi.org/10.1249/JSR.0000000000000723
Walker, P., Ellis, E., Scofield, J., Kongchum, T., Sherman, W. F., & Kaye, A. D. (2021). Snapping Hip Syndrome: A Comprehensive Update. Orthopedic reviews, 13(2), 25088. https://doi.org/10.52965/001c.25088
American Association of Orthopedic Surgeons. OrthoInfo. Hip strains.
It can be difficult for individuals and athletes to stay motivated, manage stress and prevent becoming overwhelmed. Can mental toughness and a positive attitude help increase potential and performance levels?
Mental Toughness
Athletes and fitness enthusiasts work on conditioning, skills training, and perfecting techniques. Physical training can take individuals far but another necessary part of maximizing athletic potential is building mental toughness and having the right attitude. Like anything, mental training takes time, effort, and regular adjustments to find ways to shift a losing or bad attitude into a positive one that can bring out the best.
Attitude Is Important
If negativity begins to set in like dealing with an injury, getting rid of self-limiting beliefs can be difficult, as well as generate optimism to rise up and succeed. For athletes or individuals who enjoy competitive sports, developing a positive mental attitude will help with:
Emotions that can affect cognitive functioning strategies.
Energy levels.
Other aspects of physical performance.
Mental Strategies
Mood Improvement
Individuals frustrated by a pessimistic perspective tend to dwell on problems or issues. To shift into a positive mood do something to lift your spirits, even if you don’t think it will help.
Listen to your favorite or uplifting music.
Watch an inspirational movie.
Read a sports psychology book.
Get together or call a teammate or friend that are cheerful and upbeat.
Play different games just for fun.
Take a break, go to the park, walk around, and meditate.
Get into hobbies.
Relax with a therapeutic massage.
Positive Self Talk
Continuing sports psychology research shows that practicing positive self-talk can improve athletic performance. (Nadja Walter, et al., 2019) Sports psychologists describe this through the idea that thoughts create beliefs, that drive actions.
Positive self-talk can take different forms.
For some reciting a specific phrase, sentence, or a single word can effectively manage thoughts, push out the negativity, and focus on taking care of business. Anything that inspires can include:
Focus
Remember the fundamentals!
You know what to do!
You can do it!
You got this!
Research shows that positive self-talk reduces anxiety and increases self-confidence, optimization, efficacy, and performance. (Nadja Walter, et al., 2019) However, self-talk needs to be practiced and part of a regular routine to be effective.
Visualization
Another strategy is using visualization exercises.
This could be using all the senses to imagine the venue where the tournament is taking place, the sound of the crowd, the smells, how the ground or court feels, and/or how the ball or specific sports object feels.
The wisdom is if you can think it, you can do it, once that is determined apply strategies to get there.
Sports Injury Rehabilitation
References
Walter, N., Nikoleizig, L., & Alfermann, D. (2019). Effects of Self-Talk Training on Competitive Anxiety, Self-Efficacy, Volitional Skills, and Performance: An Intervention Study with Junior Sub-Elite Athletes. Sports (Basel, Switzerland), 7(6), 148. https://doi.org/10.3390/sports7060148
Reiser, M., Büsch, D., & Munzert, J. (2011). Strength gains by motor imagery with different ratios of physical to mental practice. Frontiers in psychology, 2, 194. https://doi.org/10.3389/fpsyg.2011.00194
Tennis requires strength, power, and endurance. Can combining tennis weight training into a player’s fitness regimen that is broken up into phases achieve optimal results?
Tennis Weight Training
In professional sports that utilize weight lifting, the training is often broken up into seasonal phases. (Daniel S Lorenz, Michael P Reiman, John C Walker. 2010) Each phase consists of specific objectives that contribute to and build upon the previous phase. This is known as periodization. Tennis is played year-round indoors and outdoors. This is an example of a tennis weight training program to build up strength.
Pre-Season
In the early pre-season, players prepare to rebuild their strength after a break.
The emphasis is on building functional strength and some muscle.
Late Pre-Season
In late pre-season, players workout to get ready for the start of the season.
Here, the emphasis is on building maximum power.
In Season
In season, regular practice, play, and competition get underway and players are in top condition.
In this phase, strength and power maintenance is the focus.
Season Break
This is when players need to relax for a while.
However, players need to keep active if they want to maintain some level of fitness.
The emphasis is on rest and recovery with the maintenance of light activity, like cross-training and light gym workouts.
Research has shown that taking a break from serious strength training does help the body recover and rebuild. (Daniel Lorenz, Scot Morrison. 2015)
This is a three-phase all-around program.
The first phase concentrates on building basic strength and muscle
The second phase on power delivery.
Players who play year-round can continue with the power program once they build the basics.
Players who take a break for longer than six weeks should start again with the strength program.
Pre-Season – Phase One
Strength and Muscle
The focus is on lifting heavy weights, but not going full force to begin training the nervous system to work with the muscle fibers.
Some muscle building or hypertrophy/building muscle size will happen during strength development.
Strength is the foundation for the power development phase.
Exercises:
Duration: 6-8 weeks
Workout Days: 2-3, with at least one day, however, two are recommended between sessions.
Reps: 8-10
Sets: 2-4
Rest between sets: 1-2 minutes
Barbell squat, dumbbell squat, or sled hack squat
Romanian deadlift
Dumbbell bent-over row
Dumbbell triceps extension or machine pushdown
Cable wood chop
Lat pulldown to the front with a wide grip
Reverse crunch
Things to Remember
Use the Proper Weight
Adjust the weight so that the last reps are heavy but don’t cause a complete failure.
Balance the Lower Half
The posterior chain of the hips, the gluteals/buttocks, the upper legs, and the abdominals are of equal importance and require equal attention. (Eline Md De Ridder, et al., 2013)
Squats and deadlifts build strength and power in this region.
Follow Proper Form
For upper body exercises like the dumbbell press, lat pulldown, and wood chops the proper form needs to be followed.
Keep the forearms in a vertical plane with the upper arms.
Do not extend excessively at the bottom of the movement.
Remember to protect the vulnerable shoulder joint.
Listen to The Body
Strength training is physically and mentally challenging.
Individuals who are not able to recover from a session with only one rest day are recommended to move the program to two sessions per week.
Muscle soreness or delayed onset muscle soreness – DOMS – is normal, however, joint pain is not.
Monitor arm and shoulder reactions during this phase.
Stop if any joint pain or discomfort is felt.
Late Pre-Season – In-Season – Phase Two
Power
Power is the ability to move the heaviest loads in the shortest time and is the combination of strength and speed. In this phase, the player builds on the strength developed in phase one with tennis weight training that will increase the ability to move a load at high velocity.
Power training requires lifting weights at high velocity and with explosiveness.
The body needs to rest adequately between repetitions and sets so that each movement is done as fast as possible.
The number of sets can be less than phase one because there is no point in training at this level when the body is fatigued.
Exercises
Duration: Ongoing
Days per week: 2
Reps: 8 to 10
Sets: 2-4
Rest between repetitions: 10 to 15 seconds
Rest between sets: at least 1 minute or until recovered
Barbell or dumbbell hang clean
Cable push-pull
Cable wood chop
One arm cable raises
Medicine ball push press
Medicine ball standing twist with a partner or alone – 6×15 repetitions fast and recover between sets.
Reminders When Preparing For the Season
Recovery Time
In power training, it’s important that the body has relatively recovered for each repetition and set so that the individual can maximize the movement.
The weights should not be as heavy and the rest periods sufficient.
Push When Possible
Rest is important, at the same time, the player needs to push through reasonably heavy loads to develop power against significant resistance.
When doing medicine ball twists, do a full set at maximum, then sufficiently rest before the next one.
If doing the medicine ball exercises alone, use a lighter ball and keep the ball in your hands while twisting.
In Season – Phase Three
When the season begins training does not stop in order to help maintain strength and power.
Strength and Power Maintenance
Alternate phase one and phase two for a total of two sessions each week.
Every fifth week, skip weight training to achieve optimal recovery.
Key Points
Things to keep in mind during the season.
Avoid Overscheduling
Avoid strength training on the same day when practicing on the court.
If the weight training has to be both on the same day, try to separate the workouts into morning and afternoon sessions.
Plan Time
Rest completely from strength training one week out of every six.
Light gym work is fine.
During the season, use intuition when it comes to working out at the gym.
Individuals with limited time, stick to court skills training instead of tennis weight training.
Off Season
If there is an off-season, this is the time for emotional and physical decompression and full-body recovery.
For several weeks, forget about weight training and do other things.
Stay fit and active with cross-training or other physical activities but keep it light to prevent injuries.
It is recommended to consult a coach, trainer, sports chiropractor, and/or physical therapist to develop a program specific to an individual’s needs, fitness goals, and access to resources.
Spine Injuries In Sports
References
Lorenz, D. S., Reiman, M. P., & Walker, J. C. (2010). Periodization: current review and suggested implementation for athletic rehabilitation. Sports health, 2(6), 509–518. https://doi.org/10.1177/1941738110375910
Lorenz, D., & Morrison, S. (2015). CURRENT CONCEPTS IN PERIODIZATION OF STRENGTH AND CONDITIONING FOR THE SPORTS PHYSICAL THERAPIST. International journal of sports physical therapy, 10(6), 734–747.
De Ridder, E. M., Van Oosterwijck, J. O., Vleeming, A., Vanderstraeten, G. G., & Danneels, L. A. (2013). Posterior muscle chain activity during various extension exercises: an observational study. BMC musculoskeletal disorders, 14, 204. https://doi.org/10.1186/1471-2474-14-204
The Q or quadriceps angle is a measurement of pelvic width that is believed to contribute to the risk of sports injuries in women athletes. Can non-surgical therapies and exercises help rehabilitate injuries?
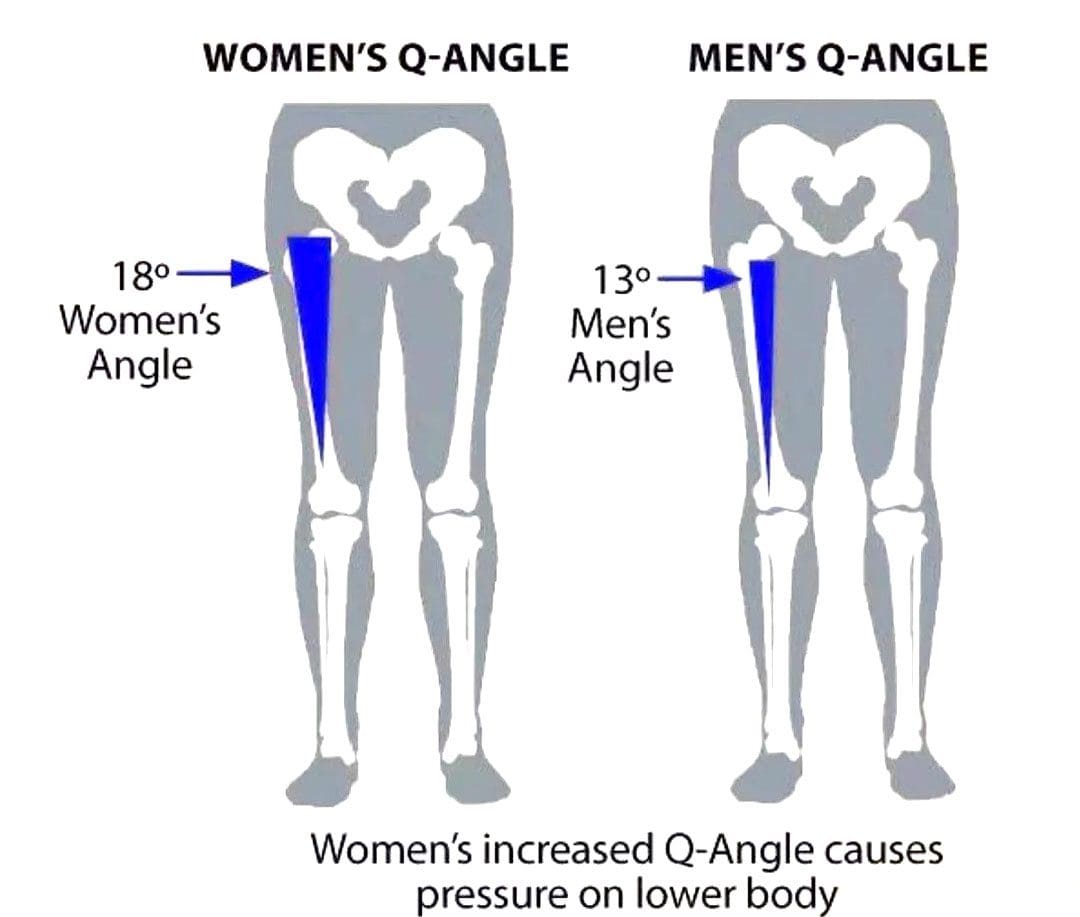
Quadriceps Q – Angle Injuries
The Q angle is the angle where the femur/upper leg bone meets the tibia/lower leg bone. It is measured by two intersecting lines:
One from the center of the patella/kneecap to the anterior superior iliac spine of the pelvis.
The other is from the patella to the tibial tubercle.
On average the angle is three degrees higher in women than men.
Women have biomechanical differences that include a wider pelvis, making it easier to give birth. However, this difference can contribute to knee injuries when playing sports, as an increased Q angle generates more stress on the knee joint, as well as leading to increased foot pronation.
Injuries
Various factors can increase the risk of injury, but a wider Q angle has been linked to the following conditions.
Patellofemoral Pain Syndrome
An increased Q angle can cause the quadriceps to pull on the kneecap, shifting it out of place and causing dysfunctional patellar tracking.
With time, this can cause knee pain (under and around the kneecap), and muscle imbalance.
Foot orthotics and arch supports could be recommended.
Some researchers have found a link, while others have not found the same association. (Wolf Petersen, et al., 2014)
Chondromalacia of the Knee
This is the wearing down of the cartilage on the underside of the kneecap.
An increased Q angle can be a factor that increases stress and causes the knee to lose its stability.
However, this remains controversial, as some studies have found no association between the Q angle and knee injuries.
Chiropractic Treatment
Strengthening Exercises
ACL injury prevention programs designed for women have resulted in reduced injuries. (Trent Nessler, et al., 2017)
The vastus medialis obliquus or VMO is a teardrop-shaped muscle that helps move the knee joint and stabilize the kneecap.
Strengthening the muscle can increase the stability of the knee joint.
Strengthening may require a specific focus on muscle contraction timing.
Closed-chain exercises like wall squats are recommended.
Glute strengthening will improve stability.
Stretching Exercises
Stretching tight muscles will help relax the injured area, increase circulation, and restore range of motion and function.
Muscles commonly found to be tight include the quadriceps, hamstrings, iliotibial band, and gastrocnemius.
Foot Orthotics
Custom-made, flexible orthotics decrease the Q angle and reduce pronation, relieving the added stress on the knee.
A custom orthotic ensures that the foot and leg dynamics are accounted for and corrected.
Motion-control shoes can also help correct overpronation.
Knee Rehabilitation
References
Khasawneh, R. R., Allouh, M. Z., & Abu-El-Rub, E. (2019). Measurement of the quadriceps (Q) angle with respect to various body parameters in young Arab population. PloS one, 14(6), e0218387. https://doi.org/10.1371/journal.pone.0218387
Petersen, W., Ellermann, A., Gösele-Koppenburg, A., Best, R., Rembitzki, I. V., Brüggemann, G. P., & Liebau, C. (2014). Patellofemoral pain syndrome. Knee surgery, sports traumatology, arthroscopy: Official journal of the ESSKA, 22(10), 2264–2274. https://doi.org/10.1007/s00167-013-2759-6
Vaienti, E., Scita, G., Ceccarelli, F., & Pogliacomi, F. (2017). Understanding the human knee and its relationship to total knee replacement. Acta bio-medica : Atenei Parmensis, 88(2S), 6–16. https://doi.org/10.23750/abm.v88i2-S.6507
Mitani Y. (2017). Gender-related differences in lower limb alignment, range of joint motion, and the incidence of sports injuries in Japanese university athletes. Journal of Physical Therapy Science, 29(1), 12–15. https://doi.org/10.1589/jpts.29.12
Nessler, T., Denney, L., & Sampley, J. (2017). ACL Injury Prevention: What Does Research Tell Us? Current reviews in musculoskeletal medicine, 10(3), 281–288. https://doi.org/10.1007/s12178-017-9416-5
Can weight and strength training increase speed and power in athletes that participate in throwing sports?
Throwing Sports
Top-throwing athletes have amazing arm speed. To succeed in throwing sports athletes need to be able to generate quick explosive power. This means the ability to propel the arm forward with substantial velocity for maximum object delivery like a baseball, javelin, hammer throw, shot put, discus, etc. Combined with sports technique training, throwing strength and power can be increased by training with weights. Here is a three-phase training plan to improve throwing performance.
Full Body
The arm provides only one part of the delivery process.
The legs, core, shoulders, and general flexibility need to work cooperatively to exert maximum thrust and achieve maximum object speed.
The natural ability to throw fast with power is largely determined by an individual’s muscle type, joint structure, and biomechanics. (Alexander E Weber, et al., 2014)
Preparation
Preparation should provide all-around muscle and strength conditioning for early pre-season conditioning.
Athletes will be doing throwing training as well, so fieldwork will need to be able to fit in.
It is recommended not to do weight training prior to throwing practice.
This leads to the start of competition and tournament play.
Frequency
2 to 3 sessions per week
Type
Strength and power – 60% to 70% for one-rep max/1RM
The one-repetition maximum test, known as a one-rep max or 1RM, is used to find out the heaviest weight you can lift once.
When designing a resistance training program, individuals use different percentages of their 1RM, depending on whether they’re lifting to improve muscular strength, endurance, hypertrophy, or power. (Dong-Il Seo, et al., 2012)
Throwing practice and competition are the priorities.
Before competition begins, take a 7- to 10-day break from heavyweight sessions while maintaining throwing workouts.
Weight training during competition should provide maintenance.
Frequency
1 to 2 sessions per week
Type
Power – lighter loads and faster execution than in the preparation stage.
Exercises
3 sets of 10
Rapid movement, 40% to 60% of 1RM.
Squats
Power hang clean and press
Romanian deadlift
Lat pulldown
Incline bench press
Crunches
Rest
Between sets 1 to 2 minutes.
Training Tips
Athletes have individual needs, so a general program like this needs modification based on age, sex, goals, skills, competitions, etc.
A certified strength and conditioning coach or trainer could help develop a fitness plan that can be adjusted as the athlete progresses.
Be sure to warm up prior to weight training and cool down afterward.
Don’t try to train through injuries or try to progress too fast – it is recommended not to throw or do weights when treating or recovering from an injury. (Terrance A Sgroi, John M Zajac. 2018)
Focus on the fundamentals and practice proper form.
Take a few weeks off at the end of the season to recover after hard training and competition.
Body Transformation
References
Weber, A. E., Kontaxis, A., O’Brien, S. J., & Bedi, A. (2014). The biomechanics of throwing: simplified and cogent. Sports medicine and arthroscopy review, 22(2), 72–79. https://doi.org/10.1097/JSA.0000000000000019
American College of Sports Medicine (2009). American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Medicine and science in sports and exercise, 41(3), 687–708. https://doi.org/10.1249/MSS.0b013e3181915670
Zaras, N., Spengos, K., Methenitis, S., Papadopoulos, C., Karampatsos, G., Georgiadis, G., Stasinaki, A., Manta, P., & Terzis, G. (2013). Effects of Strength vs. Ballistic-Power Training on Throwing Performance. Journal of sports science & medicine, 12(1), 130–137.
Seo, D. I., Kim, E., Fahs, C. A., Rossow, L., Young, K., Ferguson, S. L., Thiebaud, R., Sherk, V. D., Loenneke, J. P., Kim, D., Lee, M. K., Choi, K. H., Bemben, D. A., Bemben, M. G., & So, W. Y. (2012). Reliability of the one-repetition maximum test based on muscle group and gender. Journal of sports science & medicine, 11(2), 221–225.
Sakamoto, A., Kuroda, A., Sinclair, P. J., Naito, H., & Sakuma, K. (2018). The effectiveness of bench press training with or without throws on strength and shot put distance of competitive university athletes. European journal of applied physiology, 118(9), 1821–1830. https://doi.org/10.1007/s00421-018-3917-9
Sgroi, T. A., & Zajac, J. M. (2018). Return to Throwing after Shoulder or Elbow Injury. Current reviews in musculoskeletal medicine, 11(1), 12–18. https://doi.org/10.1007/s12178-018-9454-7
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine