Yoga has long been touted as a healing activity that extends beyond its known fitness benefits. It can help alleviate depression, relieve stress, and decrease anxiety as well as tighten and tone the body.
A 2016 study by Yoga Alliance and Yoga Journal shows that the more than 20 million people who practice yoga spend more than $10 billion on related classes and products. Chiropractors have picked up on the benefits of yoga and are recommending it to their patients. Why, because it helps to improve flexibility as well as spinal health.
Chiropractic and the spine�s role in the body.
Chiropractic is primarily intended to align the spine and balance the body. The spine is the primary support for the body. It houses most of the central nervous system and provides pathways for neural impulses to move throughout the body.
When the spine is out of alignment, it can affect how the central nervous system functions. It can also affect flexibility and even overall mobility as well as cause pain and stiffness.
Chiropractic treatment brings the spine back into alignment. It helps to balance the body and treat injuries as well as help with the changes the aging body experiences.
One of the best-known uses for chiropractic is to treat pain. It is a medication free, non-invasive treatment for chronic pain, sports-related injuries, and even automobile accidents. Many patients had reported finding relief with chiropractic when nothing else worked.
Combining yoga with chiropractic increases the effectiveness of the treatment while strengthening the body and making it better able to respond to it. It is the perfect complement to chiropractic care, and many patients are discovering tremendous health benefits from this winning, healthy combination.
What is Yoga?
In its purest form, it is an ascetic and spiritual discipline that comes from Hindu culture. It involves simple meditation, conscious breathing or breath control, and performing certain body postures.
While an ancient practice long used for spiritual and emotional healing as well as physical wellness, yoga has been adopted in western culture and widely accepted as a form of fitness as well as a therapeutic practice used for relaxation and overall good health. It focuses on inward healing for outward results.
People who regularly practice find they are more centered, handle stress better, and aren�t as likely to experience depression and anxiety. They also are more flexible, have better mobility, and have stronger leaner bodies.
What happens when you combine yoga and chiropractic care?
Because yoga helps to lower blood pressure, decrease stress, and strengthen the body�s core, it is perfect therapy for the chiropractic patient. While chiropractic care is working to align the spine and balance the body, yoga is helping to strengthen the muscles surrounding the spine, providing better support. The numerous health benefits, particularly regarding blood flow and relaxation help to increase chiropractic�s effectiveness as a pain management tool.
Patients who combine yoga and chiropractic will also often find that they see the effects of both treatments much faster than they would if they were only doing one or the other. Both chiropractic and yoga help with balance, flexibility, and mobility, but they come at it from somewhat different approaches. The benefit of this is that it provides a more balanced, well-rounded treatment in these areas as one supports the other.
Yoga also tones and tightens the body, preparing it for much more profound levels of healing, cleansing and releasing the body of tensions that may have been held�in for years. It also works to stretch muscles that have been restricted for years, or even for the patient�s entire life. It prepares the body to accept the full benefits of chiropractic and respond faster and more thoroughly.
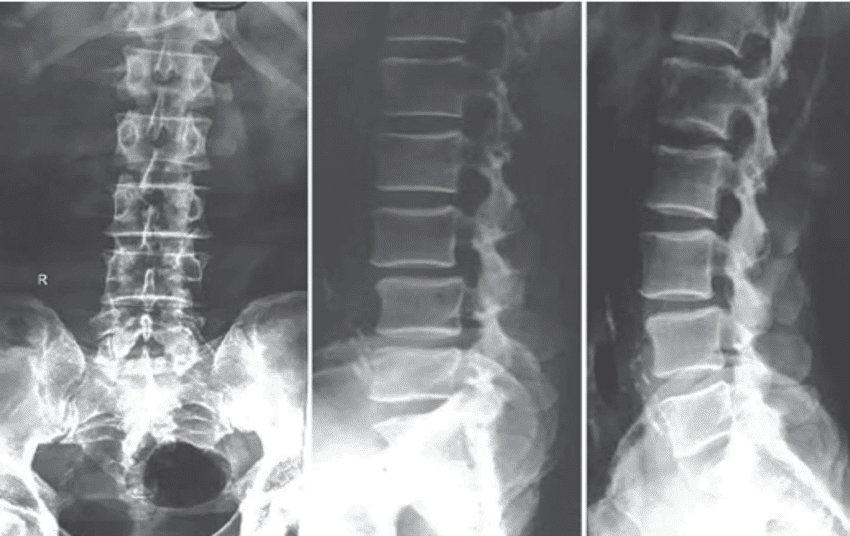
Spondylolisthesis occurs when a�vertebra of the spine slips forward over the vertebra below it. Spondylolisthesis can be categorized as: congenital spondylolisthesis, which means the disorder is present at birth; isthmic spondylolisthesis, which occurs when a defect occurs in a supportive vertebral structure of the spine; and degenerative spondylolisthesis, which is more common and is frequently associated with degenerative disc disease, or DDD, where the intervertebral discs lose hydration with age.
Development of Spondylolisthesis
The spinal column is exposed to directional pressures while it carries, absorbs, and also distributes most of the fat of the body throughout physical activities and during rest. To put it differently, while the spine is consuming and carrying body fat, additionally, it moves in different directions (e.g., rotate, bend forwards ). This mixture of functions causes unnecessary stress to be placed onto the vertebra and the supportive vertebral�structures of the spine, and it might result in one of these slipping forwards over the ones beneath it, ultimately developing into spondylolisthesis.
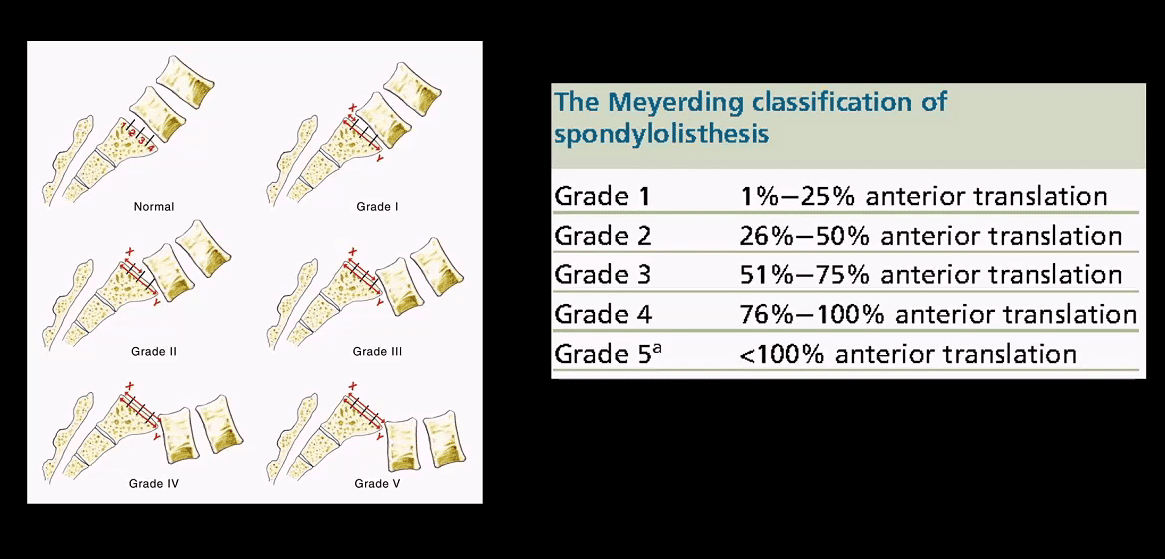
Grading spondylolisthesis
Doctors “grade” the severity of spondylolisthesis utilizing five descriptive categories. Even though there are several factors your physician notes when evaluating your spondylolisthesis, the grading scale (below) relies on how far forward a vertebral body has slid over the vertebra beneath it. Often, the doctor uses a lateral (side view) x-ray to examine and grade�spondylolisthesis. Grade I is a smaller slide than Grade IV or V.
Grade I: Less than 25% slip
Grade II: 25% to 49% slip.
Grade III: 50% to 74% slip.
Grade IV: 75% to 99% slip.
Grade V: The vertebra has fallen forward off the vertebra below it. This�grade is the most severe type of spondylolisthesis and is medically referred to as�spondyloptosis.
Who Might be at Risk
If a family member has spondylolisthesis, your risk for developing the disorder may be higher. Also, some physical activities can make you more vulnerable to developing spondylolisthesis. Gymnasts, linemen in football, and weightlifters, all put pressure and stress on their spine. Picture the movements gymnasts perform on a regular basis: they bend backward and twist through the air, landing quickly and absorbing the impact through their legs and back. Those motions can place strain on the spine, potentially causing spondylolisthesis.�The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Scoliosis Pain and Chiropractic
The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, other aggravated conditions can also cause back pain.�Scoliosis�is a well-known, health issue characterized by an abnormal curvature of the spine and it is subcategorized by cause as a secondary condition, idiopathic, or of unknown cause, or congenital. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain associated with scoliosis through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. Chiropractic care can help restore the normal curvature of the spine.
Everyone knows that exercise is great for overall wellness, better health, and a healthy body. Many chiropractors will often recommend regular exercise to their patients who need to lose weight, want better mobility, or are seeking relief from depression. Some chiropractors are turning to Pilates to help their patients get stronger, more flexible, and more mobile.
What is Pilates?
In the early 20th century Joseph Pilates developed the exercise program to help World War I soldiers improve their physical fitness. It was used to rehabilitate patients who had been injured. By incorporating resistance, stretching, and target strengthening exercise, Pilates uses resistance bands, individual machines, and floor work to reshape and rehabilitate the body. Dancers, gymnasts, athletes, and celebrities use Pilates to stay in shape. However, anyone can do it for a healthier, more supple spine.
Care of the spine is at the core of Pilates. By keeping it in a neutral, or natural, position, this exercise can prevent back pain as well as help ease it. When done correctly, Pilates can:
Improve muscle control and movement efficiency through mental focus.
Make you more mindful of your body�s position, specifically, remaining aware of the spine�s position and keeping it neutral
Improve centering and mental focus through special, breathing techniques
Support and improve posture by strengthening the abdominal and back muscles.
Benefits of Pilates for Chiropractic Patients
The benefits of Pilates tremendous, but for chiropractic patients, it is even more so. By regularly incorporating Pilates into your exercise routine, you can enjoy these incredible benefits.
You can adapt Pilates to your fitness level and needs. Whether you are just starting a fitness program or you�ve been working out for years, Pilates can be tailored to your fitness needs and level.
It helps you strengthen your core. The deep muscles of your abdomen, back, and pelvic floor make up the core muscles of your body. Many of the movements focus on these muscles, making a body that is strong and the frame is supported.
Allows you to strengthen your muscles without bulking up. With Pilates your muscles get strong, but it also stretches the muscles so that they are lean and long. You will look toned and tight but not bulky and muscular.
It focuses on whole body fitness. Many types of exercise only work certain parts of the body, but this focuses on entire body fitness. It works every part of the body so that the muscle development is balanced.
It helps to improve your posture. It strengthens your body and helps to keep your spine in proper alignment due to a strong core. As a result, your posture naturally improves. By incorporating it into your exercise routine, you will find yourself standing taller, stronger, and more graceful.
You can become more connected through your mind and body by increased awareness. Pilates engages your mind and increases body awareness. It unites the mind, body, and spirit for complete coordination. Each movement is done with full attention.
It improves your flexibility. Pilates is a gentle but powerful exercise that works to safely stretch the muscles, making them longer, and increasing the range of motion in the joints.
It can protect you from injuries. By strengthening your body, Pilates can help protect you against injury. It conditions your whole body so that your muscles and strength are balanced. This reduces your risk of injury.
You get a natural energy boost. Just like with any exercise, it will give you an energy boost. However, it is increased even more thanks to the focused breathing and increase in circulation stimulating the muscles and spine.
It can help you lose weight and attain a lean, long, healthy body. It tones and strengthens the body, and if you do it regularly, it will reshape you. The body is more muscular and more balanced. It also helps you move with more grace and ease.
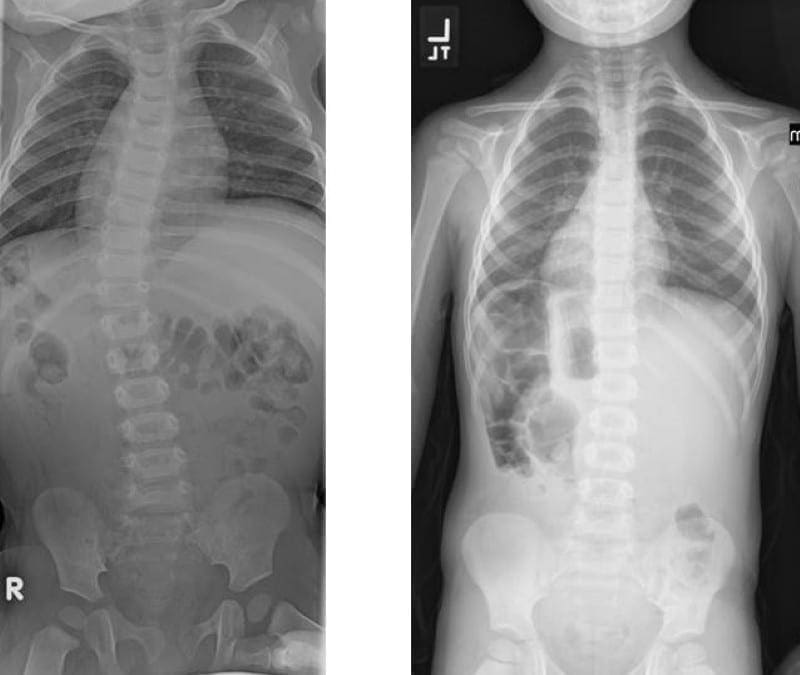
Scoliosis is a medical condition where an individual’s spine is diagnosed with an abnormal curve. The natural curvature of the spine is generally “S” shaped when viewed laterally, or from the side, and it should appear straight when viewed from the front or back. In many instances, the abnormal curvature of the spine with scoliosis increases over time, while in others, it remains the same. Scoliosis can cause a variety of symptoms.
Scoliosis affects approximately 3 percent of the population. The cause of most instances is unknown, however, it is believed to involve a mixture of environmental and genetic variables. Risk factors include having relatives with the same problem. It may also develop due to other health issues, such as Marfan syndrome, cerebral palsy, muscle spasms, and tumors like neurofibromatosis.� Scoliosis commonly develops between the ages of 10 and 20 and it commonly affects girls more than boys. Diagnosis is supported with X-rays. Scoliosis is classified as structural, in which the curve is fixed, or functional, in which the underlying spine is normal.
Treatment is based upon the level of curve, place, and trigger. Curves can be viewed periodically to record the progression of scoliosis. Bracing is frequently utilized to treat scoliosis. The brace must be fitted into the individual and used until the progression of scoliosis stops. Exercise is advocated towards the improvement of scoliosis. Other alternative treatment options, such as chiropractic care, can restore the natural curvature of the spine. The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Scoliosis Pain and Chiropractic
The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, other aggravated conditions can also cause back pain. Scoliosis is a well-known, health issue characterized by an abnormal curvature of the spine and it is subcategorized by cause as a secondary condition, idiopathic, or of unknown cause, or congenital. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain associated with scoliosis through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. Chiropractic care can help restore the normal curvature of the spine.
New Year�s Resolutions made by well-meaning but, unfortunately, less than 10 percent of people who make resolutions feel that they successfully achieve them and only 45 percent last past six months. Self-improvement goals like lose weight, eat healthier, quit smoking, and life improvement rank in the top five more popular resolutions. So, what is that 10 percent doing that makes them successful at achieving their goals? What sets them apart?
SMART Approach to Successful Goals
The SMART approach is a guide for setting realistic goals and attaining them. It is an acronym that outlines a success-focused strategy for goal setting:
Specific
Measurable
Accountable
Realistic
Timeframe
Each step will bring you closer to achieving your goals and improve your health.
Be SPECIFIC about your goals
Vague, ambiguous goals can�t stand up to time and temptation. Get specific.
Say you want to lose weight. How much do you want to lose? How do you plan to accomplish it? What are your reasons for setting this goal? Whatever goal you are setting, ask why and get specific about the details.
Set Goals that are MEASURABLE
If you set a goal that you can�t measure, how will you know when you reach it?
Any goal that you have can be measured in some way. Weight loss is measured in pounds, how your clothes fit, or how many inches you�ve lost. Eating healthy can be measured by what foods you incorporate into your diet, getting the junk food out of your pantry, and finding healthy recipes.
It helps to break your main goal into several smaller, attainable ones. It lets you see success very early, and you keep seeing success which spurs your motivation, making you less likely to abandon your efforts.
Hold Yourself ACCOUNTABLE
Accountability is a great motivator for helping you stick to your goals. Keeping a journal has long been a great way to keep yourself accountable, but there are many website and software programs that you can use to track your efforts that may prove to be even more effective.
Partnering up with a buddy is also a great strategy. Choosing someone who has a goal similar to yours allows you to hold each other accountable. Plus, success is always better when you can share it with a friend.
Keep Your Goals REALISTIC
Unrealistic or unattainable goals are motivation killers. Even goals that are too difficult or require high-pressure effort over a long period can be challenging to�see all the way through.
As you sit down, think about not only what you want to achieve, but what that looks like in your life. In other words, consider your personality and lifestyle, structuring your goals to accommodate those factors.
If your goal is to lose weight, setting a goal of 30 pounds in 30 days is not only unrealistic but unhealthy. On the other hand, setting a 2 pound per week loss is a goal that you will likely find to be much easier.
Set a TIME-FRAME, but Keep it Flexible
Creating a timeframe for meeting your goals gives your efforts structure which helps to keep you motivated. Make sure your timelines are realistic; give yourself enough time.
If the constraints are too tight, you could find that you veer off the path and even lose sight. Stay flexible, though. If you don�t reach a target within a given timeframe, don�t be afraid to move it a little.
As long as you are moving forward, toward your goal you don�t need to limit yourself just because you didn�t complete it within the time you allotted initially. It�s about meeting your goals�and making lasting changes that will affect your overall health for the better. Cut yourself some slack.
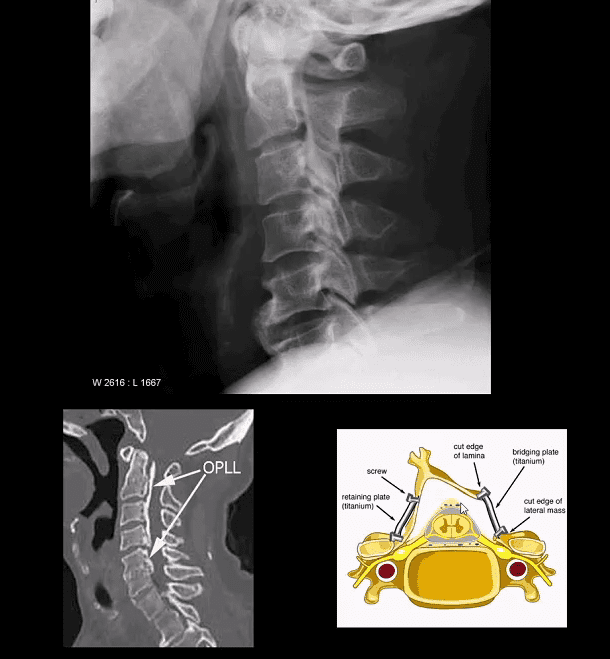
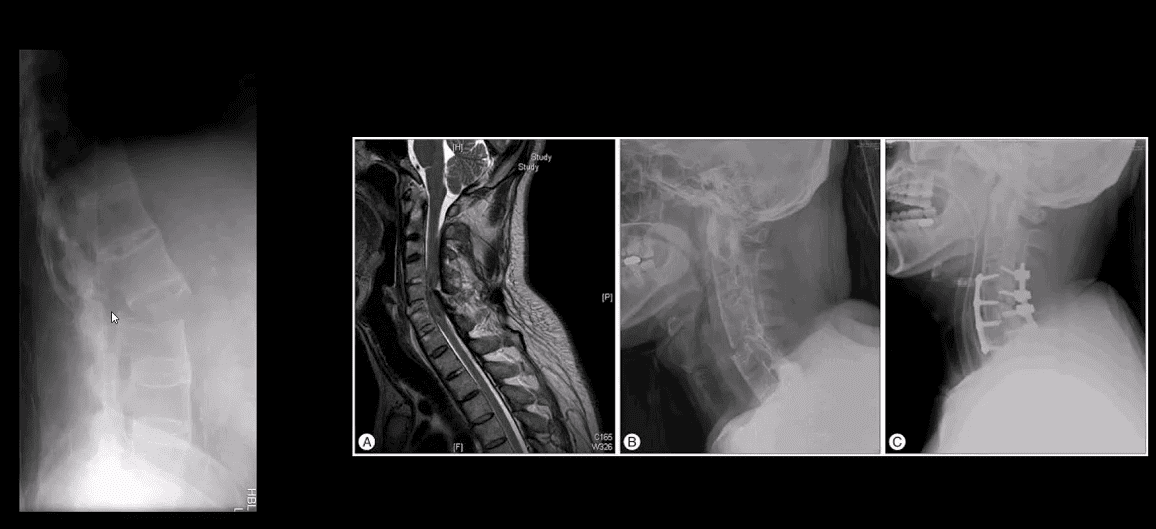
Ossification of Posterior Longitudinal Ligament (OPLL). Less frequent than DISH.
Greater clinical importance d/t spinal canal stenosis and cervical myelopathy
Asian patients are at higher risk
Both OPLL & DISH may co-exist and increase the risk of Fx
Imaging: x-rad: linear radioopacity consistent with OPLL
Imaging modality of choice: CT scanning w/o contrast
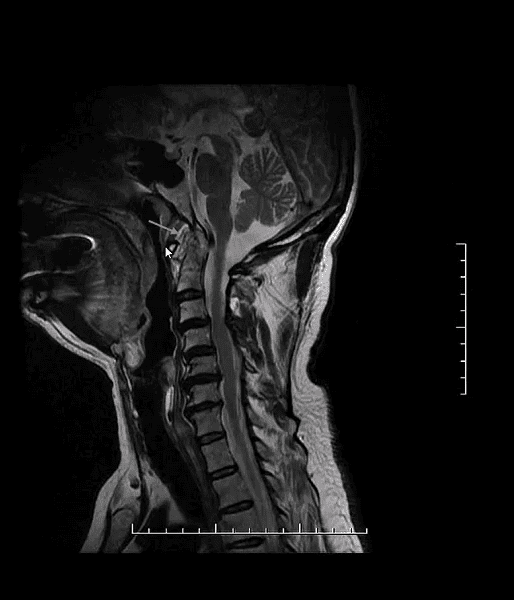
MRI may help� to evaluate myelopathy
Care: surgical with laminoplasty (above right image) that has been pioneered and advanced in the Far East
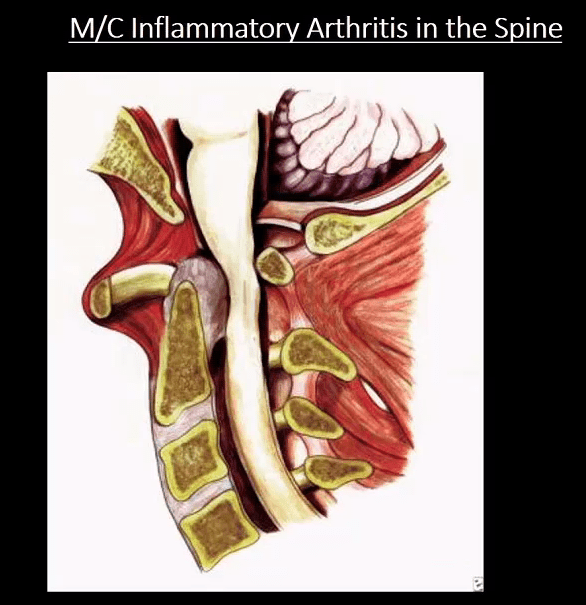
M/C Inflammatory Arthritis In Spine
Rheumatoid spondylitis (Rheumatoid arthritis) d/t inflammatory synovial proliferation pannus rich in lymphocytes, macrophages, and plasma cells
C/S RA may affect 70-90% of patients
Variable severity from mild to destructive disabling arthropathy
RA IN C/S m/c affects C1-C2 due to an abundance of rich synovial tissue
Typically infrequent in the thoracic/lumbar region
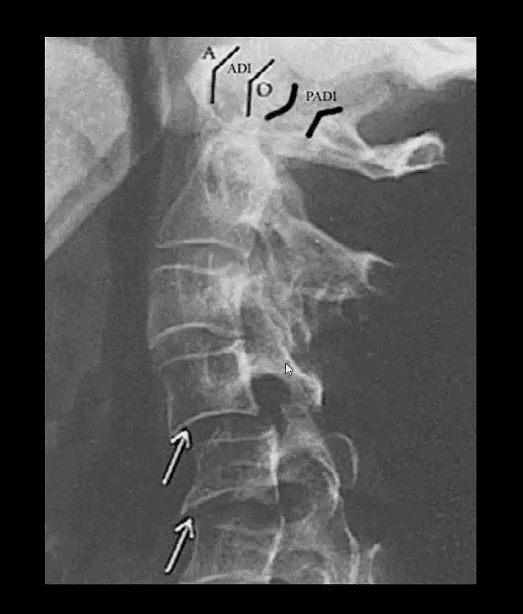
Sub-axial C/spine may be affected later due to facets, erosions, ligament laxity and instability showing “Stepladder” appearance
Clinically: HA, neck pain, myelopathy, etc. inc. Risk of Fx/subluxation. Any spinal manipulation HVLT ARE STRICTLY CONTRAINDICATED.
Rx: DMARD, anti-TNF-alfa, operative for subluxations, etc.
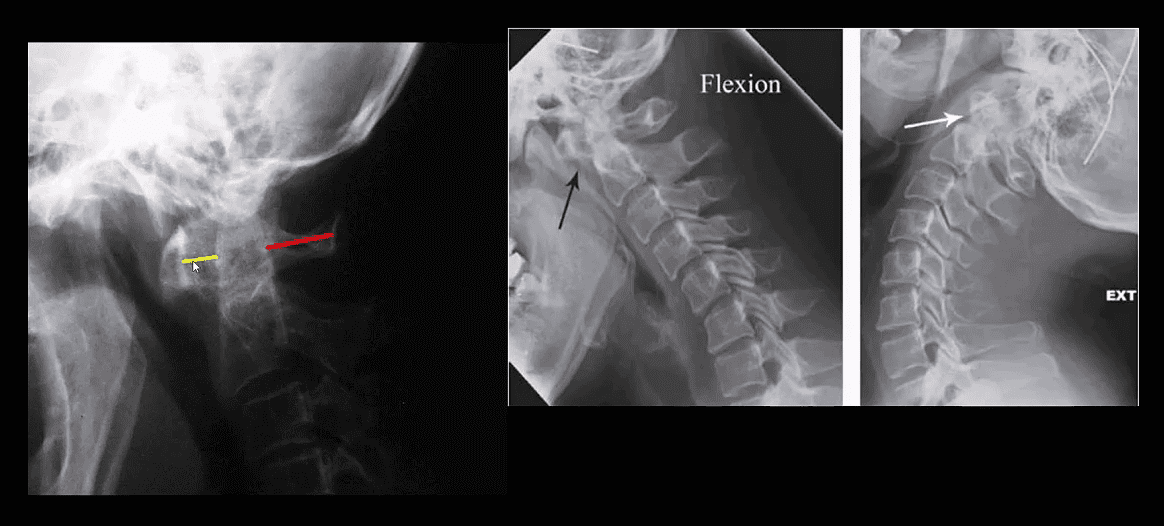
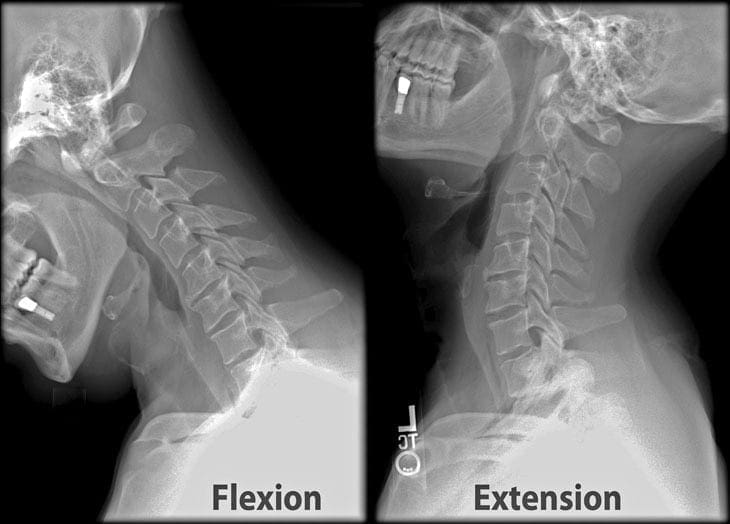
Rheumatoid Spondylitis C1-C2. Perform X-radiography initially with flexed-extended views. Note Dens erosion, C1-2 subluxation (2.5 mm) that changes on mobility
RA spondylitis: an erosion of the odontoid with the destruction of C1-C2 ligaments and instability
M:F 4:1, age: 20-40 m/c. Clinic LBP/stiffness, reduced rib expansion <2 cm is > specific than HLA-B27, progressive kyphosis, risk of Fx’s.
Imaging steps: 1st step-x-rays to id. Sacroiliitis/spondylitis.�MRI & CT may help if x-rays are unrewarding.
Labs: HLA-B27, CRP/ESR, RF-
Dx: clinical+labs+imaging.
Rx: NSAID, DMARD, anti-TNF factor therapy
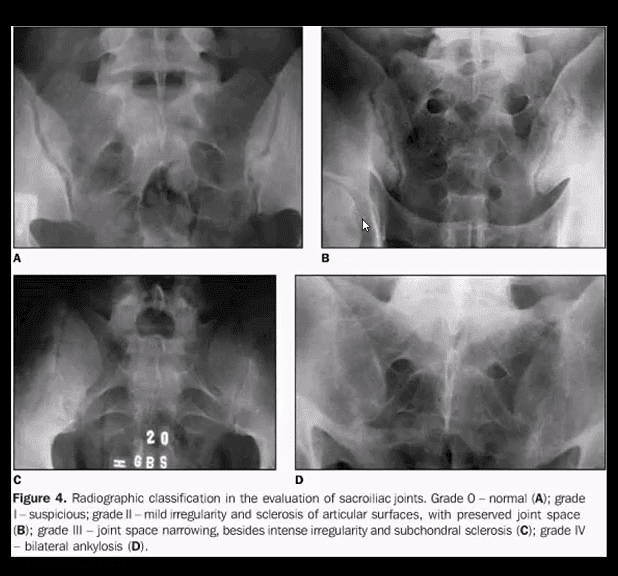
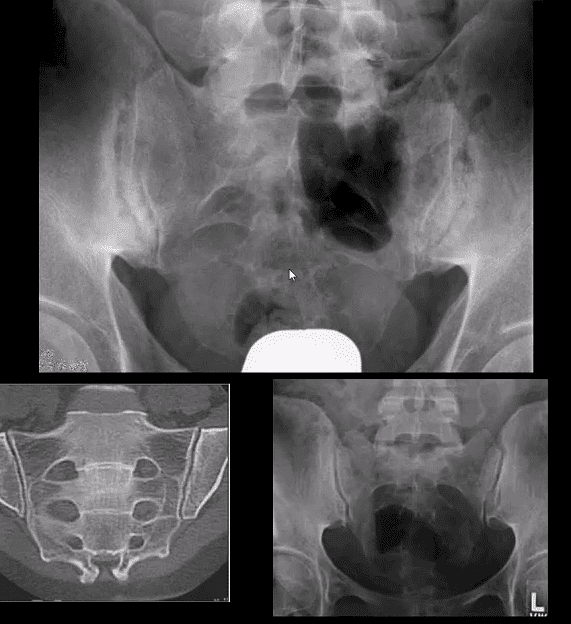
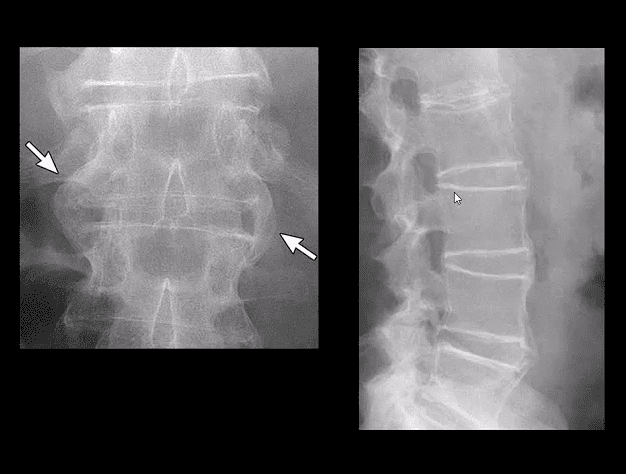
Key Imaging Dx: always presents initially as b/l symmetrical sacroiliitis that will progress to complete ankylosis. Spondylitis presents with continuous ascending discovertebral osteitis (i.e., marginal syndesmophytes, Romanus lesion, Anderson lesion), facets and all spinal ligament inflammation and fusion with a late feature of “bamboo spine, trolley track, dagger sign,” all indicating complete spinal ossification/fusion. Increasing risk of Fx’s.
Key Dx of Sacroiliitis
Blurring, cortical indistinctness/irregularity with adjacent reactive subchondral sclerosis initially identified primarily on the iliac side of� SIJs.
Normal SIJ should maintain a well defined white cortical line. Dimension 2-4 mm. May look incongruous d/t 3D anatomy masked by 2D x-rays.
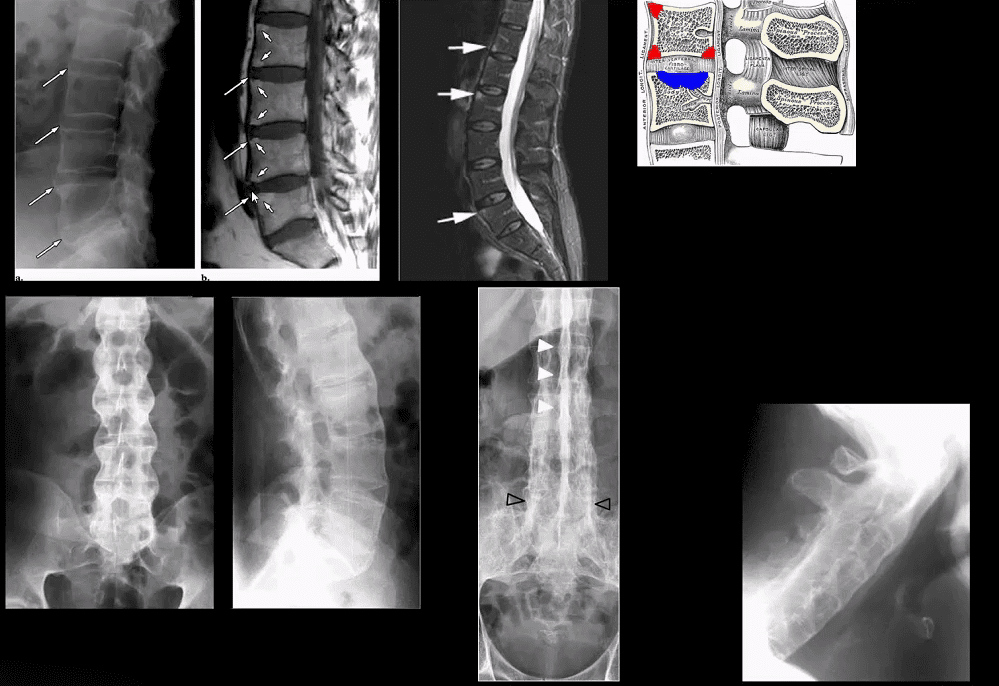
Key Imaging Dx In Spine
Marginal syndesmophytes and inflammation at the annulus-disc (above arrows) at the earliest dx; by MRI as marrow signal changes on T1 and fluid sensitive imaging (above top images).
These represent enthesitis-inflammation that will ossify into bamboo spine.
Lig ossification: trolley track/dagger sign
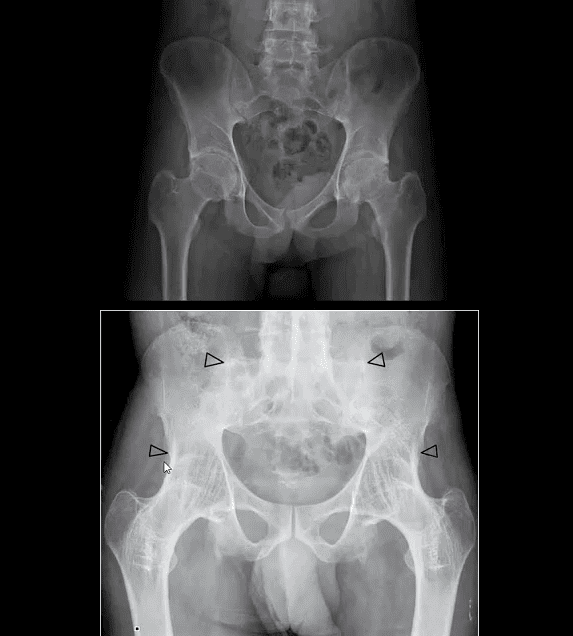
AS in extraspinal joints: root joints, hips, and shoulders
Symphysis pubis
Less frequent in peripheral joints (hands/feet)
All seronegatives may present with heel pain d/t enthesitis
Complication: Above Carrot-stick/chaulk-stick Fx
PsA & ReA (formerly Reiter’s) present with b/l sacroiliitis that virtually identical to AS
In the spine PsA & ReA DDx from AS by the formation of non-marginal syndesmophytes aka bulky paravertebral ossifications (indicate vertebral enthesitis)
For a clinical discussion of Spondyloarthropathies refer to:
Rheumatoid arthritis, or RA, is a chronic health issue which affects approximately 1 percent of the population in the United States. RA is an autoimmune disorder that causes the inflammation and degeneration of the synovial tissue, specific cells and tissue which form the lining of the joints within the human body. Rheumatoid arthritis may and generally does affect every joint in the body, especially as people get older. RA commonly develops in the joints of the hands and feet, severely restricting an individual’s ability to move, however, those with significant disease in the spine are at risk of damage like paraplegia. Rheumatoid arthritis of the spine is frequent in three areas, causing different clinical problems.
The first is basilar invagination, also referred to as cranial settling or superior migration of the odontoid, a health issue where degeneration from rheumatoid arthritis at the base of the skull causes the it to “settle” into the spinal column, causing the compression or impingement of the spinal cord between the skull and the 1st cervical nerves. The second health issue, and also the most frequent, is atlanto-axial instability. A synovitis and erosion of the ligaments and joints connecting the 1st (atlas) and the 2nd (axis) cervical vertebrae causes instability of the joint, which may ultimately result in dislocation and spinal cord compression. In addition, a pannus, or localized mass/swelling of rheumatoid synovial tissue, can also form in this region, causing further spinal cord compression. The third health issues is a subaxial subluxation which causes the degeneration of the cervical vertebrae (C3-C7) and often results in other problems like spinal stenosis.
Imaging studies are crucial to properly diagnose patients with rheumatoid arthritis of the cervical spine. X-rays will demonstrate the alignment of the spine, and if there is obvious cranial settling or instability. It can also be difficult to demonstrate the anatomy at the bottom of the skull, therefore, computed tomography scanning, or CT scan, with an injection of dye within the thecal sac is arranged. Magnetic resonance imaging, or MRI, is beneficial to assess the severity of nerve compression or spinal cord injury, and allows visualization of structures, including the nerves, muscles, and soft tissues. Flexion/extension x-rays of the cervical spine are usually obtained to evaluate for signs of ligamentous instability. These imaging studies entails a plain lateral x-ray being taken with the patient bending forward and the other lateral x-ray being taken with the individual extending the neck backwards.�The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain and Auto Injury
Whiplash is one of the most common causes of neck pain after an automobile accident. A whiplash-associated disorder occurs when a person’s head and neck moves abruptly back-and-forth, in any direction, due to the force of an impact. Although whiplash most commonly occurs following a rear-end car crash, it can also result from sports injuries. During an auto accident, the sudden motion of the human body can cause the muscles, ligaments, and other soft tissues of the neck to extend beyond their natural range of motion, causing damage or injury to the complex structures surrounding the cervical spine. While whiplash-associated disorders are considered to be relatively mild health issues, these can cause long-term pain and discomfort if left untreated. Diagnosis is essential.
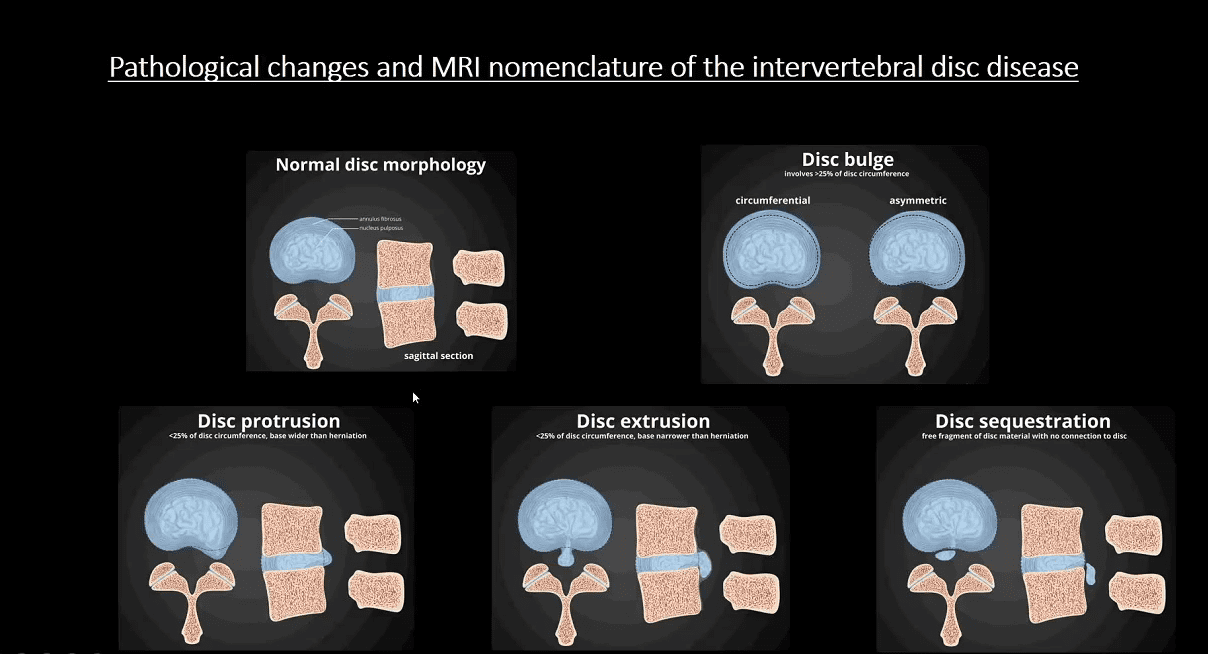
Spondylosis aka Degenerative disease of the spine represents an evolution of changes affecting most mobile spinal segments beginning with:
Intervertebral disc (IVD) dehydration (desiccation) and degeneration aka Degenerative Disc Disease (DDD) with an abnormal increase in mechanical stress and degeneration of posterior elements affecting 4-mobile synovial articulations ( true osteoarthritis)
2-Facets in the L/S & 2-Facets & 2-Uncovertebral joints in the C/S
Imaging plays a significant role in the diagnosis, grading, and evaluation of neurological complications (e.g., spondylotic myelopathy/radiculopathy)
X-radiography with AP, Lateral & Oblique spinal views provides Dx and classification of Spondylosis
MR imaging may help to evaluate the degree of neurological changes associated with degenerative spinal canal and neural foraminal stenosis
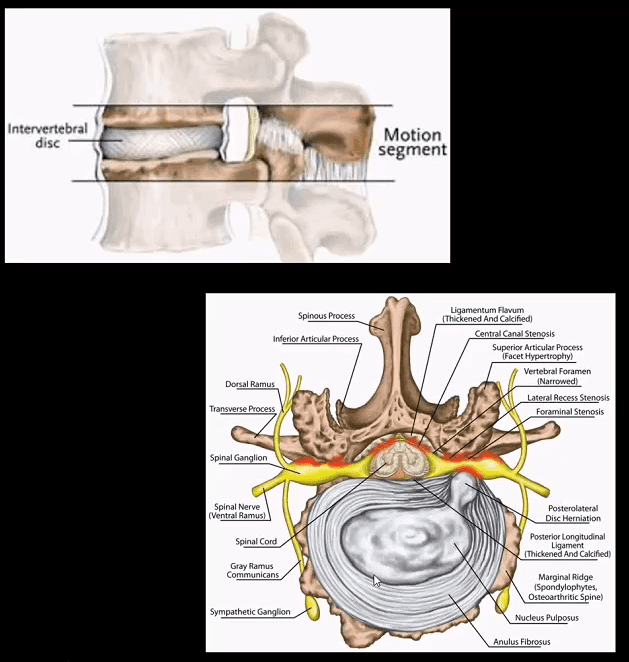
Spinal motion segment:
2-adjacent vertebrae
IVD (fibrocartilage)
2-facets (synovial)
Pathology: loss of disc height increases mechanical stress on mobile elements
Ligamentum flavum “hypertrophy” or thickening due to buckling
Loss of normal lordosis with or w/o reversal or kyphosis
Vertebral canal & neural foraminal stenosis
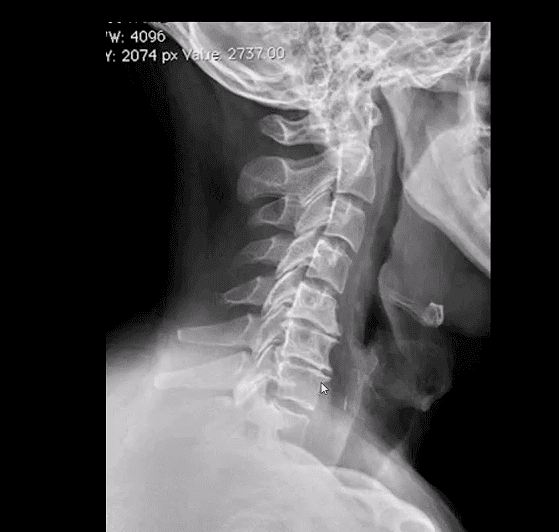
Neutral lateral cervical radiograph: note mild to moderate disc narrowing and spondylophyte formation at C5-6 & C6-C7 (most common levels affected by cervical spondylosis). Straightening or flattening with mild reversal of cervical lordosis. Some mild facet proliferation is noted at the above levels
On radiographs: evaluate for disc height (mild, moderate or severe) loss
End-plate sclerosis & spondylophytes; mild, moderate or severe
Facet and uncinate irregularity, hypertrophy/degeneration; mild, moderate or severe
Key Dx: correlate with a clinical presentation: neck/back pain with or w/o neurological disturbance ( myelopathy vs. radiculopathy or both)
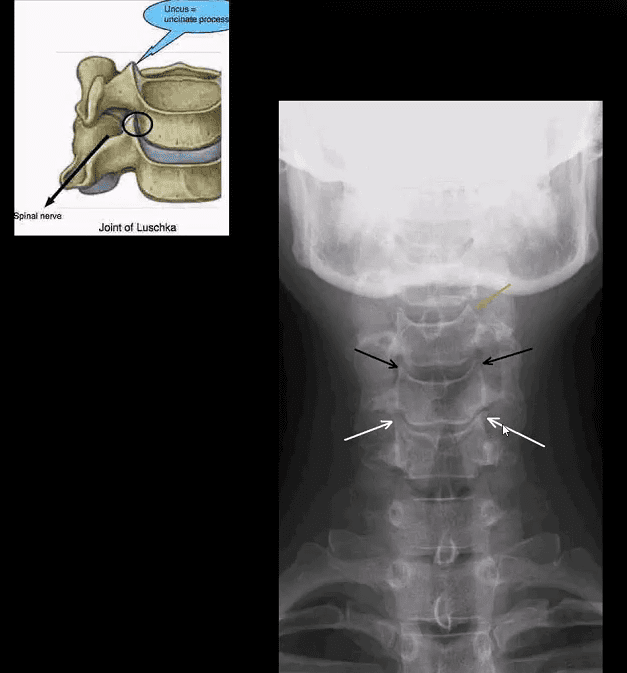
Uncinate processes undergo degeneration/proliferation resulting in uncovertebral arthrosis
Early findings present with mild bone proliferation along the cortical margin (white and black arrows) if compared to normal uncinate (orange arrow)
Later, more extensive bone proliferation extending into and narrowing vertebral canal and neural osseous foramina (IVF’s) may be noted. The latter may contribute to spinal/IVF stenosis and potential neurological changes
Posterior oblique views may help further
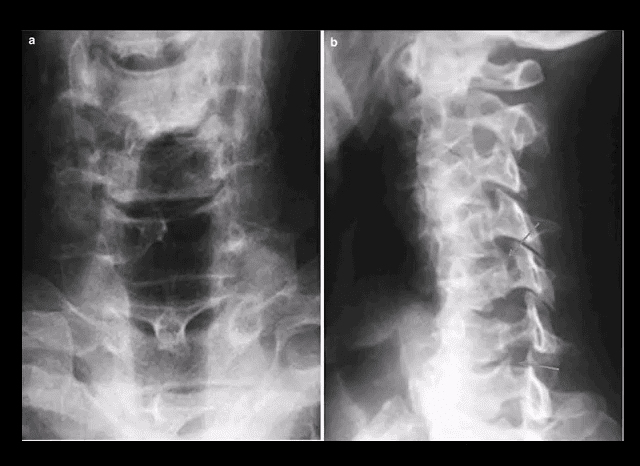
AP lower cervical (a) and posterior oblique (b) views
Note mild uncinated process proliferation with neural foraminal narrowing (arrows)
Typically if less than a third of IVF becomes narrowed, patients may present w/o significant neurological signs
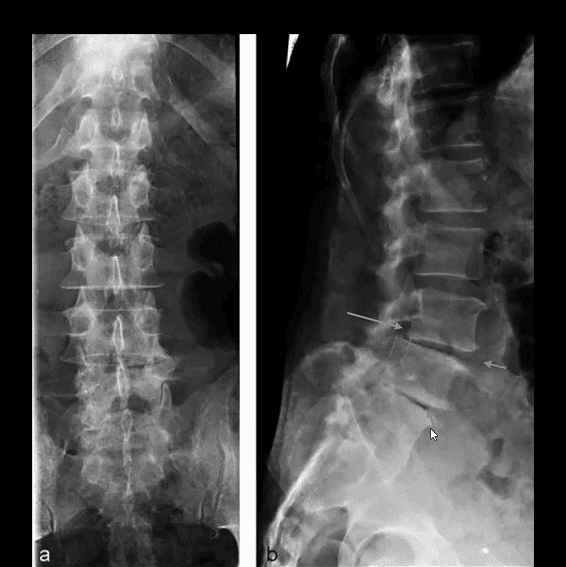
Lumbar spondylosis is evaluated with AP and lateral views with additional AP L5-S1 spot view to examine lumbosacral junction
Typical features include disc height loss/degeneration
Intra-discal gas (vacuum) phenomenon (blue arrow) along with spondylophytes
Degenerative spondylolisthesis and/or retrolisthesis (green arrow) may follow disc and facet degeneration and can be graded by the Meyerding classification
In most cases, degenerative spondylolisthesis rarely progresses beyond Grade 2
Lumbar facet degeneration seen as bone proliferation/sclerosis and IVF narrowing
MR imaging w/o gad C is an effective modality to evaluate clinical signs of spondylosis & associated neurological complications with pre-surgical evaluation
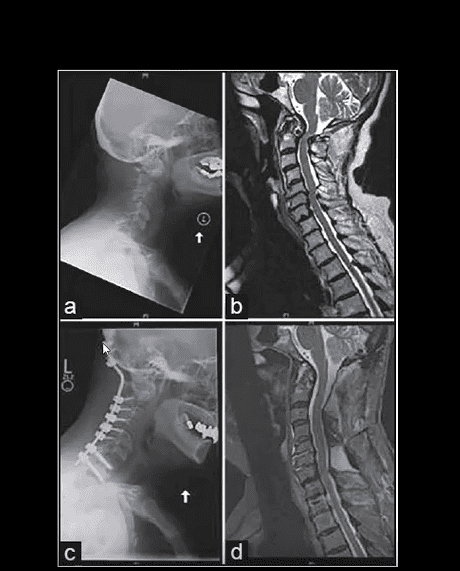
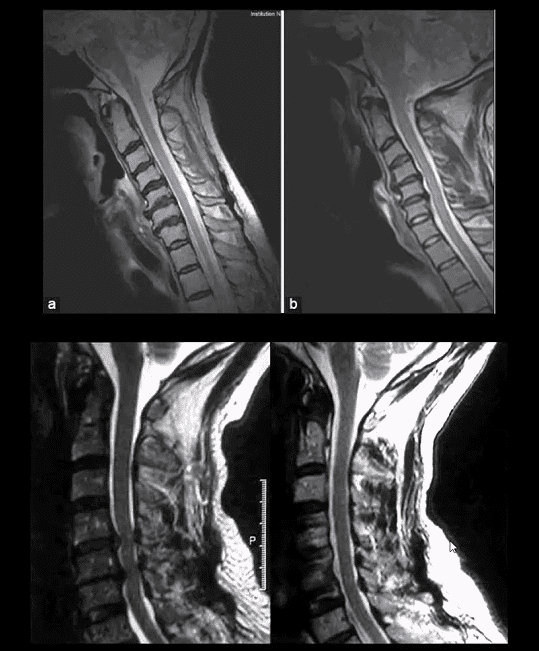
Case: 50-y.o Fe with neck pain. Case b-45-y.o.M (top a b images). MRI reveals: loss of disc hydration or desiccation, spondylophytes and disc herniation w/o neurological changes
(Bottom images) Left: preoperative and right postoperative MRI slices of the patient presented with clinical signs of cervical spondylotic myelopathy. Note disc herniation, ligam flavum hypertrophy and canal stenosis (left)
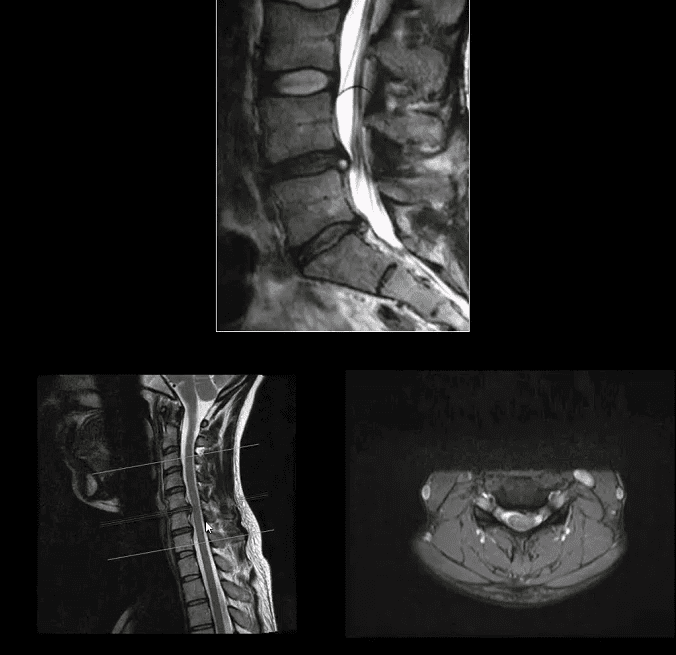
Sagittal MRI slice of lumbar DDD manifested with disc desiccation and posterior herniation effacing thecal sac
Correlating sagittal and axial slices will be more informative to evaluate canal stenosis and potential degree of neurological involvement (above-bottom images)
Use the following resources to learn more on MRI evaluation and diagnosis of Degenerative Disc Disease:
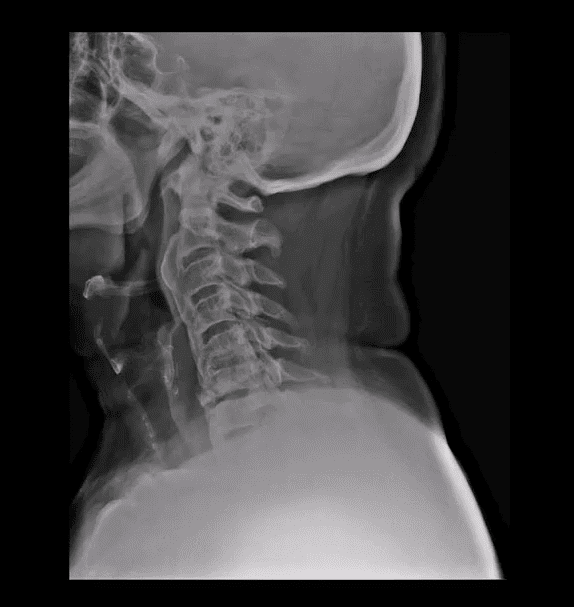
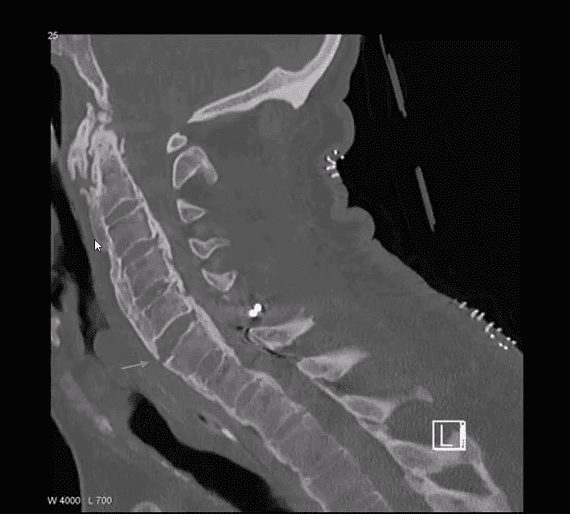
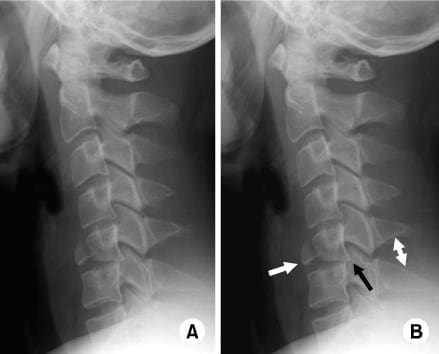
A teardrop fracture is caused when the anteroinferior aspect of a cervical vertebral body is damaged due to flexion of the spine together with vertical compression. The fracture throughout the body is also associated with deformity of the human body and subluxation or dislocation of the facet joints. A teardrop fracture is generally associated with a spinal cord injury due to the displacement of the anterior portion of the body into the spine.
The flexion teardrop fracture shouldn’t be confused with a similar-looking vertebral fracture called “expansion teardrop fracture”. Both usually happen in the cervical spine, but as their names indicate, they result from other mechanisms (flexion-compression vs. hyperextension). Both are linked to a small fragment being broken apart from the anteroinferior corner of the affected vertebra. Flexion teardrop fractures normally involve instability in most elements of the backbone, commonly occur at the C4-C7 vertebra, and have a higher association with spinal cord injury (specifically anterior cord syndrome). In contrast, the extension-type fracture happens more commonly in C2 or C3, causes significantly less if any disturbance to the middle and posterior elements, and does not normally result in spinal cord injury (but it may co-occur with more harmful spinal injuries).
A flexion teardrop fracture is a common injury of the cervical spine,�or neck, which can be severe in nature. Its name�is characterized by the triangle-shaped fragment which typically fractures from the anteroinferior corner of�the vertebral body and that resembles a drop of water dripping from the vertebral body. The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work. Back pain attributes to the most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Chiropractic care is a respected, effective treatment for a variety of conditions as well as for promoting overall wellness. Every day patients seek it out to manage their pain, find relief from health issues, and recover from injuries. But did you know that pro athletes also utilize chiropractic for injuries, soreness, and to keep them playing at optimal levels?
What many may not realize is that an estimated 90 percent of top athletes use chiropractic to step up their game. You don�t have to be an athlete to step up your own game with chiropractic care. Here are three benefits that the pros enjoy � and so can you!
Chiropractic is an effective treatment for pain management.
Chiropractic has long been regarded as a natural, non-invasive, drug-free approach to pain management. Numerous studies have proven its effectiveness in treating pain for some conditions and injuries. Many pro athletes utilize this option to manage their pain from overtaxed muscles and ligaments to activity related injuries.
When the spine not correctly aligned it can put pressure or stress on other areas of the body. Spinal adjustments can help relieve pain in ligaments, joints, discs, and muscles. However, chiropractic techniques can be used for all parts of the body, including arms, hands, fingers, feet, hips, and knees.
Chiropractic helps in preventing injury and enhancing performance.
Doctors of Chiropractic understand that when it comes to treatment, there is not a one size fits all option. Every patient is different, and they will tailor a custom plan that benefits the entire body based on lifestyle, activity level, age, health conditions, and other factors.
The first appointment will include a variety of evaluations that help the doctor determine the best course of treatment for you, including the activities you engage in and the frequency. This way he or she can get an idea of your risk of injury and the areas to concentrate on in your treatment. So, whether you are a pro football player or a weekend warrior, chiropractic can improve your performance and help protect you from injury.
Chiropractic helps in treating many types of injuries.
For pro athletes, injuries are just part of the game. High impact sports like hockey, football, and wrestling tend to result in injuries, but even non-contact sports like baseball, cycling, and golf can lead to injuries as well.
Low impact, as well as low impact athletes, find great value in routine adjustments and spinal alignments. This alone helps to lower their risk of injury as well as improve flexibility and enhance performance. It can help reduce the stress and strain that all types of physical activity place on the body, whether you are a pro golfer or football player, or if you enjoy working in your garden or are a stay at home mom running after kids all day.
Sports equipment with a football, basketball, baseball, soccer, tennis and golf ball and badminton hockey puck as recreation and leisure fun activities for team and individual playing.
Some of the top names in pro sports rely on chiropractic to treat injuries, manage pain, and enhance athletic performance. You might recognize some of the names: Barry Bonds, Arnold Schwarzenegger, Lance Armstrong, Evander Holyfield, Tiger Woods, Joe Montana, and Martina Navratilova are just a few. You don�t have to be an athlete, though, to reap the same benefits that the pros do. You can get them by scheduling an appointment with a chiropractor.
Chiropractic care is a safe, useful healthcare option that is appropriate for all ages and activity levels. Your Doctor of Chiropractic will sit down with you and work with you to create a treatment plan that is tailored to meet your unique needs.
Because this type of treatment focuses on the root of the problem instead of just managing symptoms, your treatment plan will usually involve not only adjustments and chiropractic techniques, but dietary recommendations, exercises, and lifestyle modifications as well so that you enjoy whole body wellness.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine