Athletic pubalgia, also known as a hockey hernia,�hockey groin, Gilmore’s Groin,�sports hernia, or groin disruption, is a health issue of the pubic joint. It is a condition characterized by chronic groin pain in athletes and identified by a dilated ring of the inguinal canal. Soccer and ice hockey players are the athletes most commonly affected by athletic pubalgia, and both recreational and professional athletes can be impacted.
Athletic Pubalgia Symptoms
Symptoms of athletic pubalgia�generally manifest as pain following physical activity, most frequently through hip extension, and twisting and turning movements. The painful symptoms usually radiate into the adductor muscle region and the testicles, although it is often difficult for the individual to pinpoint the exact location of the�symptoms. Athletes with athletic pubalgia�experience soreness and stiffness after physical activity.
Any exertion which increases intra-abdominal pressure, such as sneezing or�coughing, as well as physical activity, can lead to pain. While pain in the stomach and pelvis can occur due to a variety of health issues, including injuries to the low back, or lumbar spine, the hip joint, the sacroiliac joint, and the abdomen, along with the genito-urinary system, diagnosis of athletic pubalgia demands skillful differentiation and evaluation.
Clinical Presentation of Athletic Pubalgia
The diagnosis of athletic pubalgia is based on the patient’s history, where healthcare professionals may also depend on the use�of magnetic resonance imaging,�or MRI. Symptoms can frequently be reproduced by certain movements, such as performing crunches or sit-ups. Pain associated with athletic pubalgia may also be elicited with the patient in a “frog posture,” in which the individual is supine with knees bent and heels together.
Many athletes experience concomitant fatigue or tearing of the�adductor muscles or labral tears of the hip. If there is stiffness in the adductor muscles post-injury, painful symptoms can manifest. Alternative treatment options should be to restore normal movement after the adductor has begun to heal, normally 6 to 8 weeks post-injury. Moreover, sleeping in a prone position with the hip on the affected side flexed and externally rotated can offer relief to some athletes with athletic pubalgia.
The precise prevalence of this health issue is unknown. Conservative therapies,�such as gentle stretching, may temporarily alleviate painful symptoms, however, definitive treatment options should be considered for long-term relief.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Sleeping. New parents chase it, Type A personalities fight it, but everyone needs it. The thing is, most people don�t get enough of it. According to the National Sleep Foundation, 45 percent of adults in the United States report that in a seven day period lack of sleep affected their daily activities.
Sleep quantity is not as much of a problem as sleep quality. Around 35 percent of people who said they slept for 7 or 8 hours a night still reported that their sleep quality was �only fair� or �poor� and 20 percent said that they did not feel refreshed upon waking. When a person is dealing with pain, such as lower back pain, it can make it even more difficult to get a good night�s sleep.
The Importance of Sleeping
Sleep is vital for good health. The Centers for Disease Control (CDC) cites insufficient sleep as a contributing factor to a variety of conditions including obesity, diabetes, depression, and cardiovascular disease. It is also a significant contributing factor in many machine related crashed, worksite accidents, and automobile accidents, leading to injury, disability, and even death.
Sleep allows your body to heal and the spine to rejuvenate. It helps you handle stress better and manage pain more effectively. It is an essential part of good health so making sure that you get good quality sleep should be a priority � and it is possible. These are the best sleep positions to get your best sleep when you have lower back pain.
Stomach Position
Sleeping on your stomach is usually the least back friendly sleep position, but some people can�t sleep any other way. Take the strain off of your back by supporting it with a pillow under your lower abdomen and pelvis. Using a pillow may put too much stress on your back, so you might need to try to sleep without one. Another alternative is to use a flatter, less fluffy pillow. Try different positions, such as drawing one leg up or splaying your legs more until you find on that is right for you.
Back Position
If you sleep on your back, you likely won�t be comfortable just lying flat. Try different positions such as placing a rolled towel under your knees or the small of your back to provide added support. Use a good pillow to support your neck. Some pillows are made specifically for people who sleep on their backs; you may want to give it a try.
Side Position
Many people with lower back pain find sleeping on their side to be the most comfortable sleep position. If you sleep on your side, pull your knees up slightly so that they are almost perpendicular from your body. You may have to make some adjustments to how bent your legs are before you find a position that takes the pressure off of your back. Place a pillow between your thighs and knees. You may want to use a body pillow to provide even more support all along your legs.
A Word about Your Pillow and Your Bed
The position that you sleep in can help relieve your back pain, but getting good quality sleep will help you manage your pain much better so it should be your goal to get a�good, restful sleep every night. You should change out your pillow on a regular basis.
Pillows can get worn and no longer deliver the support they once did. If you are waking up with neck or back pain or headaches, it could be your pillow. Additionally, studies show that making your bed every day improves your quality of sleep. Make sure that the temperature is comfortable and avoid electronic devices for about an hour before bedtime. Be kind to your body; make sleep a priority.
The rectus femoris muscle attaches to the pelvis and just below the knee as it is one of four muscles found at the front part of the thigh. It functions by extending the knee and flexing the hip. The rectus femoris muscle is made up of�fibers which adapt to quick action. Rectus femoris muscle strain is caused by forceful movements, such as kicking a ball or when beginning to sprint, and it is particularly vulnerable to stress and pressure.
Painful symptoms generally manifest at the top of the thigh after the rectus femoris muscle suffers a strain or tear. In severe cases, the health issue may even become noticeable if the tissue is completely ruptured. Fortunately, complete tears are rare. Healthcare professionals will commonly use an MRI scan to diagnose the extent of the sports injury. Proper diagnosis and treatment�are�essential. A rectus femoris muscle strain should not be rushed, as individuals who return-to-sport too soon may suffer re-injury.
Treatment for Rectus Femoris Strain
According to many healthcare professionals, when it comes to sports injuries to the rectus femoris muscle, it’s crucial to immediately apply the RICE principle (Rest, Ice, Compression, and Elevation) to the affected thigh. This treatment aims to decrease bleeding and inflammation to the muscle. Also, it will help reduce painful symptoms after the injury. Based on how much pain has been experienced, simple painkillers might be utilized, although it’s best to attempt to prevent the use of these.
Once movement is restored enough to allow the individual to walk using their regular range of motion, and once the swelling has gone down, then you will have recovered from the acute phase of the injury. It would then be an excellent time to engage in physical activity, without inflicting damage or stress to the quadriceps muscles. This can be performed on an exercise bicycle or through swimming, where the weight is kept�off the limb. Stretches and gentle resistance exercises are crucial, as this will help to align the scar tissue that has formed during the healing process.
Recovery must be monitored so that improvements can be noted and the treatment shifted to help the rehabilitation process. It is hard to measure the length of time to complete recovery. It can take from six to eight weeks or even longer, although some people will commonly recover within one to four weeks.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Metastatic Bone Disease (aka Mets) or “Secondaries.” Are the most common malignant bone neoplasms affecting the spine, aka spinal neoplasms (>70%) and the rest of the skeleton in adults.
5-Primaries are m/c involved:
Breast (16-37%)
Lung (12-15%)
Thyroid (4%)
Renal (3-6%)
Prostate (9-15%)
Spine, pelvis, proximal femurs & proximal humeri are m/c affected in that particular order of frequency
Thoracic & upper Lumbar spine considered the m/c site of spinal Mets
Pathophysiology & Etiology of Metastasis
Malignant cells a very good at evading immune detection and elimination
They gain�access to circulation expressing Vascular Endothelial Adhesion Molecules (e.g., integrines & selectins)
Once reaching their target organs, malignant cells stimulate the production of various vasogenic growth factors and by exiting blood vessels invade their target tissues
Lung, Liver, and Bone are particularly at risk due to the character of their blood supply
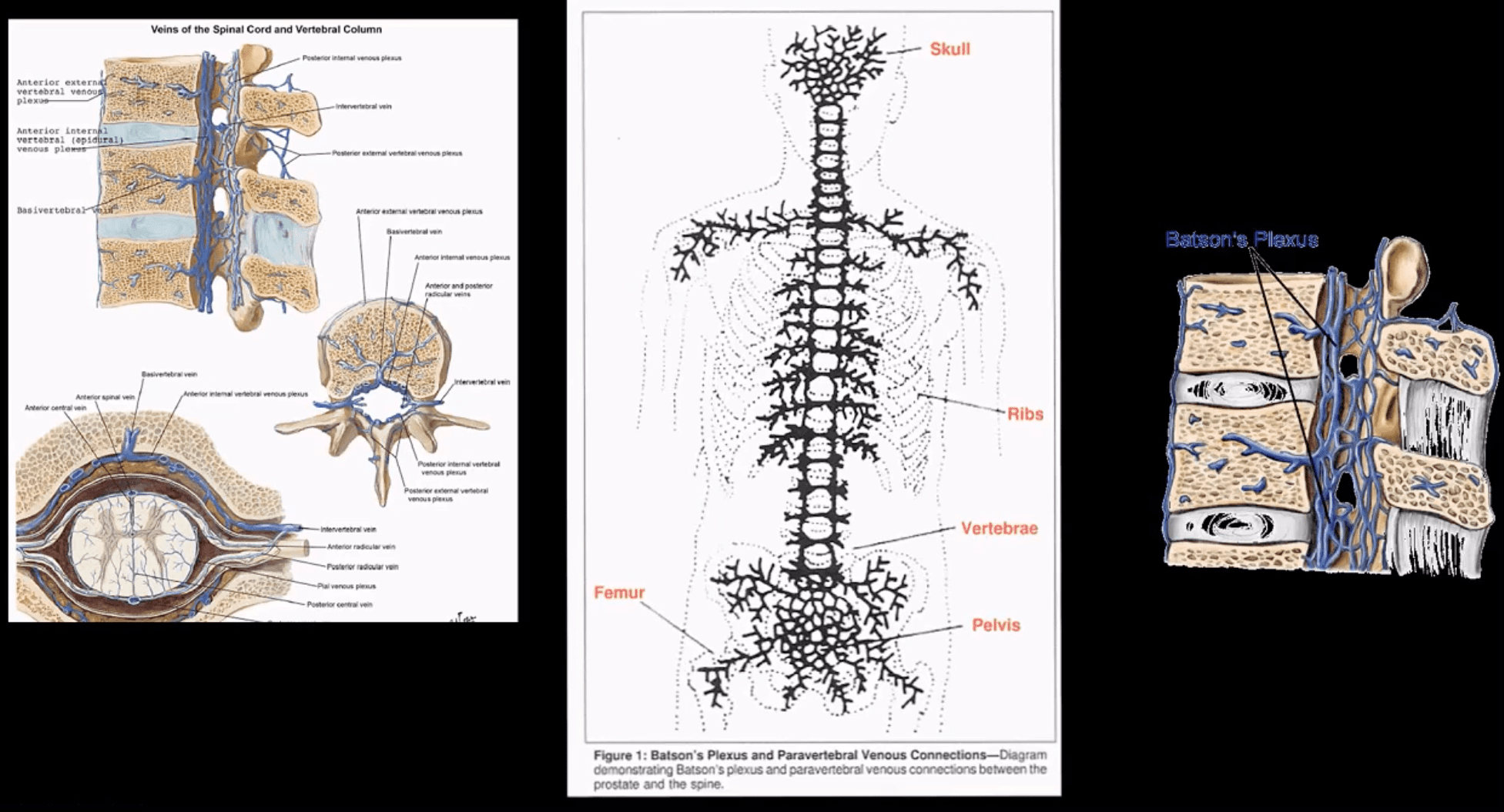
Baston venous plexus-is a network of valveless freely communicating� veins connecting axial skeleton/meninges and proximal femurs/humeri with abdomino-pelvic and thoracic cavities
The risk of Mets is increased during daily variations in the intra-abdominal and intra-thoracic pressure
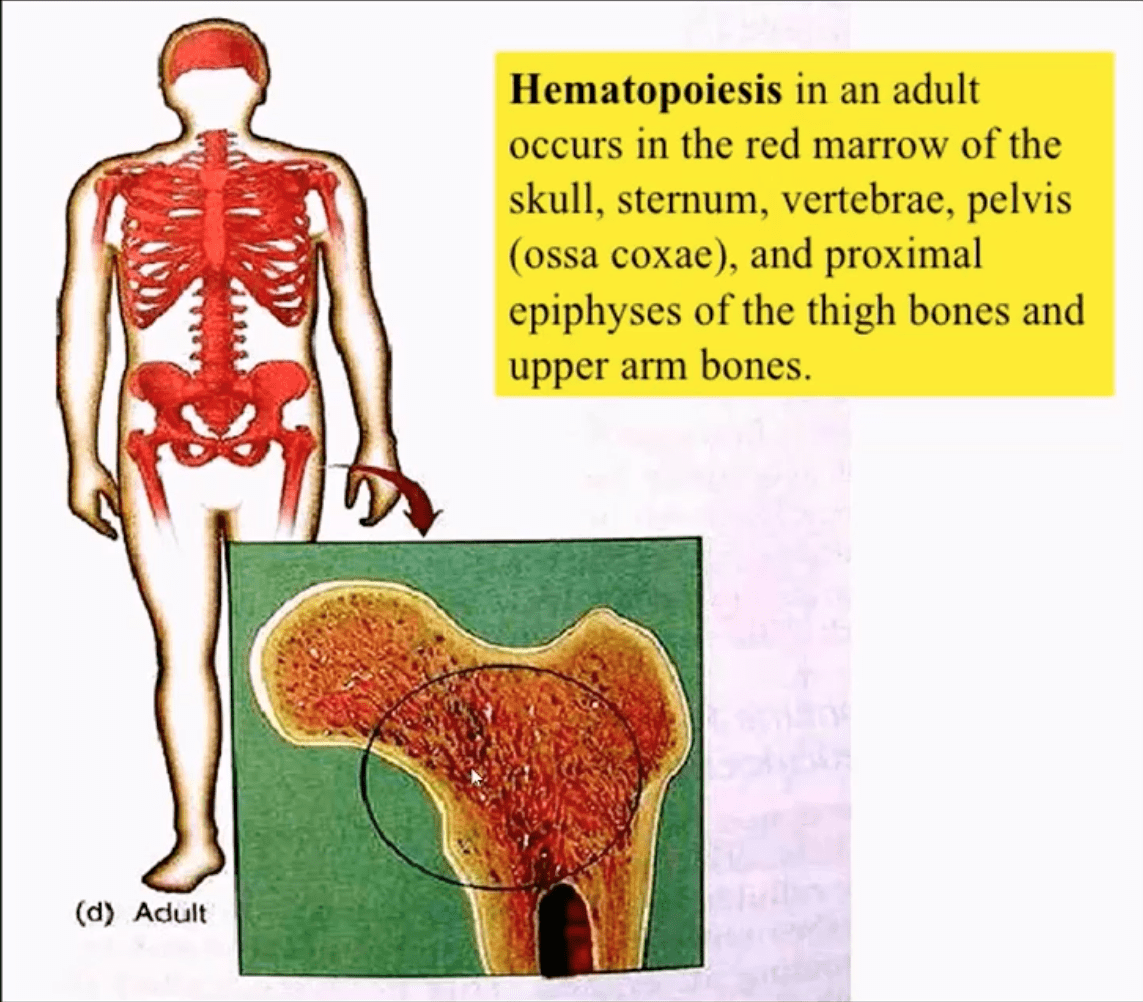
In adults, the axial skeleton is involved in hematopoiesis, and it is particularly vulnerable to metastatic deposits via an abundant network of sinusoids within a spongy bone
The vast majority of bone Mets will be detected in the axial skeleton
Clinical Presentation
Back pain often mimicking “mechanical back pain” is the m/c and often misleading symptom
Chiropractors and other manipulators should be particularly aware of this dangerous pitfall.
Nocturnal pain or pain unresponsive to NSAID may be reported in more advanced cases
Advanced cases may also present with a neurological deficit due to pathologic vertebral fractures and spinal cord/nerves compression
Metastatic hypercalcemia may occasionally develop in severe cases and considered a medical emergency that potentially presents with confusion, muscle weakness, and renal signs
Imaging plays a significant role in the Dx and management of bone metastasis
Lab tests are of limited value, but hypercalcemia and alkaline phosphatase (Alk Phos) may be elevated
In some cases, a bone biopsy may be used to confirm bone Mets
When Bone Mets are Detected, Patients Prognosis is Significantly Worsened
Median survival:
Thyroid – 48 – months
Prostate – 40 – months
Breast – 24 – months
Renal Cell – may vary, can be as low as 6 – months
Lung – 6 – months
Imaging Diagnosis
Begins with radiography investigating a clinical complaint of back/bone pain
If radiographs are unrewarding or equivocal, unique imaging modalities are required
MRI may help to show marrow replacement by Mets foci but limited to specific regions
Tc99 radionuclide bone scan (scintigraphy) is considered one of the most sensitive and reliable imaging steps in evaluating bone Mets
Bone scintigraphy is good at detecting both lytic and blastic Mets
However, very aggressive/vascular osteolytic Mets and Multiple Myeloma often appear “cold” or photopenic on bone scan due to greater stimulation/activation of osteoclasts which “outpace” osteoblasts ability to uptake the radiopharmaceutical
CT scanning is an excellent modality to show bone destruction, but it is not widely used during bone Mets Dx especially if radiography, bone scintigraphy, and MRI provide adequate information about the process
CT scanning may be particularly helpful with delineation of pathological fractures
General Radiographic Features of Bone Mets
Osteolytic (lytic), osteoblastic (blastic) aka sclerotic Mets or misec Mets can be identified radiographically
However, it takes between 30-50% of lamella (cortical) bone and 50-75% of trabecular (cancellous) or spongy bone to be destroyed before it can be detected on plain film radiographs
This can make early radiographic detection of bone Mets very difficult, requiring particular imaging modalities (e.g., MRI)
Also, bowel gas/fecal matter and numerous soft tissue densities in the abdomino-pelvic and thoracic cavities may pose challenges of bone Mets detection
Different tumors often manifest with different metastatic appearance, depending on tumor activity and release of cytokines (IL6, IL11), endothelin 1 or other growth factors that will be responsible for either osteolytic, osteoblastic or mixed Mets
For example: purely lytic bone Mets are noted in Lung, Thyroid, and Renal cell CA (very vascular)
Breast CA may present with 60% of blastic Mets
Prostate CA presents with 90% of blastic Mets
Other blastic Mets may derive from urinary bladder, melanoma and GI adenocarcinomas
Sclerotic foci may also represent as previously treated primaries
Very vascular� Mets like Renal cell and Thyroid may present with markedly� lytic and expansile foci often called “blow out Mets.”
Mets found distal to elbows and knees (acro-metastasis) are commonly associated with Lung CA
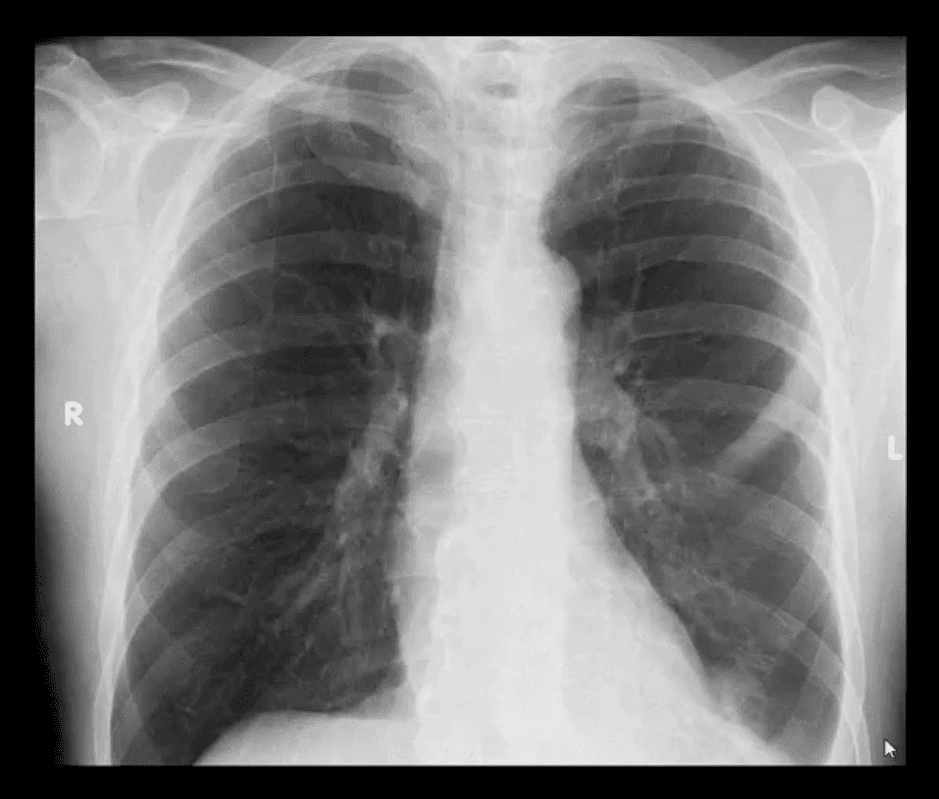
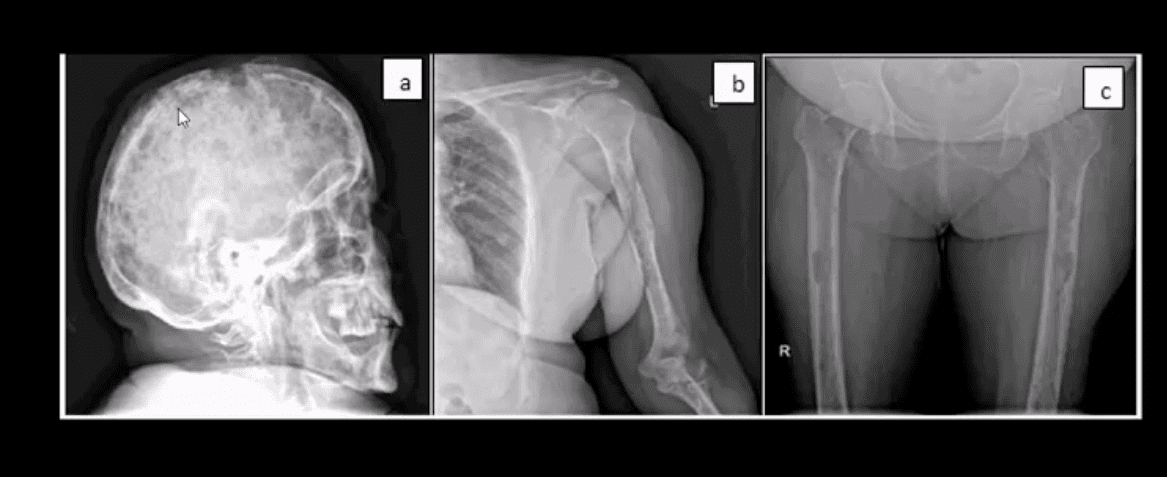
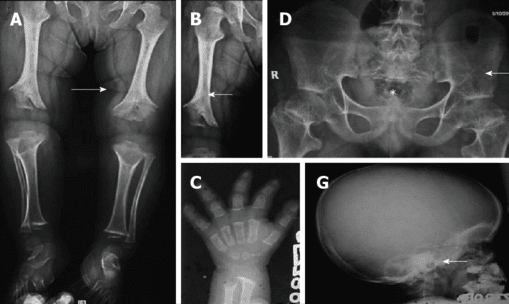
PA chest view of a routinely screened patient with a known Hx of Prostatic adenocarcinoma
Note sclerotic lesion identified in the left posterior Rib 5
What imaging modality is required next?
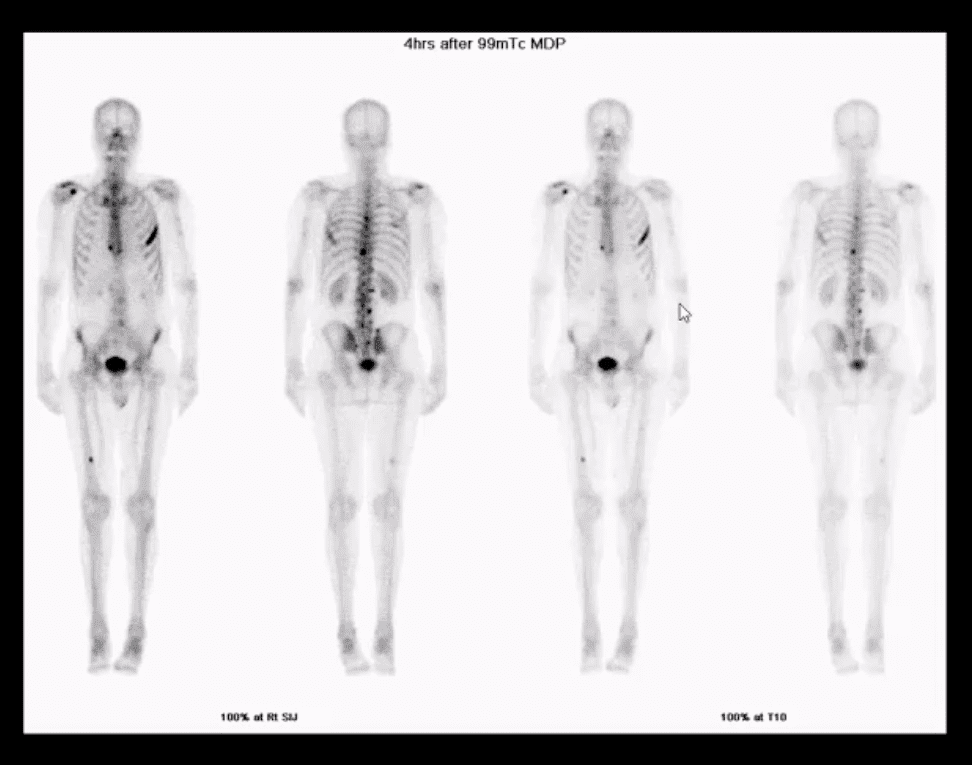
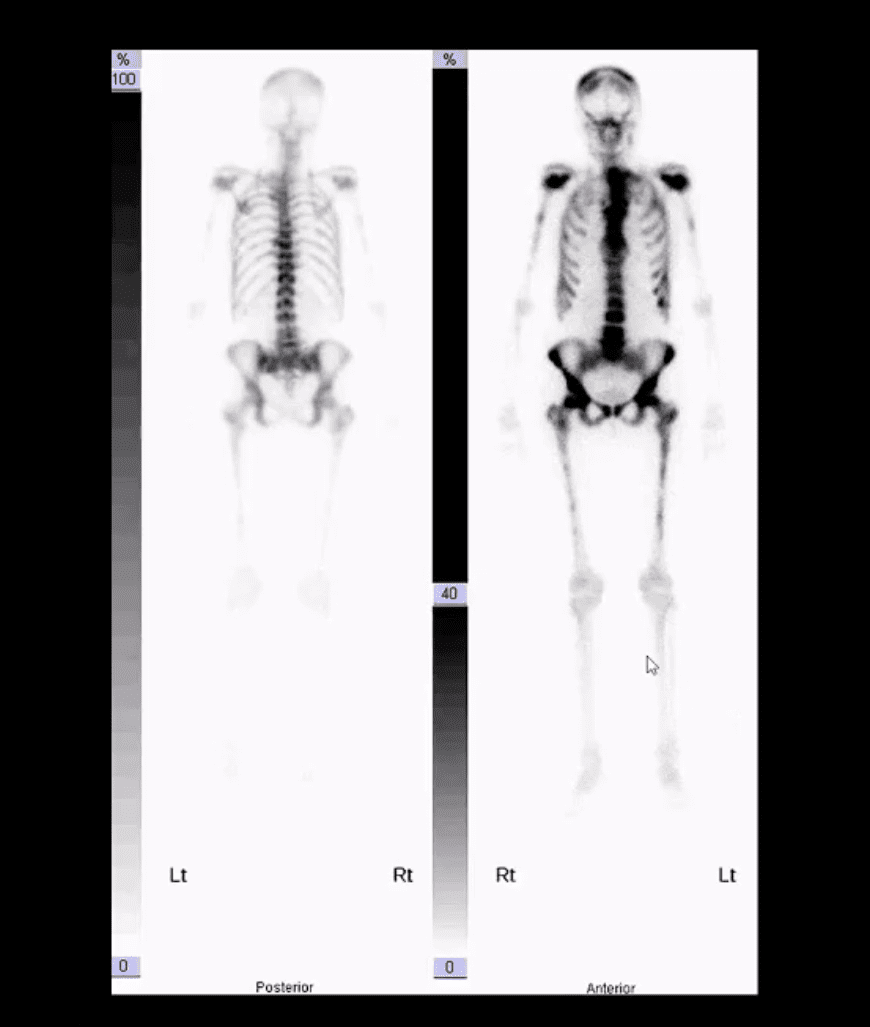
Radionuclide bone scan should be suggested
Multiple foci of high uptake of the Tc99 radiopharmaceutical
This is due to Mets and increased osteoblastic activity in the thoracic and lumbar spine, ribs and other sites of the skeleton
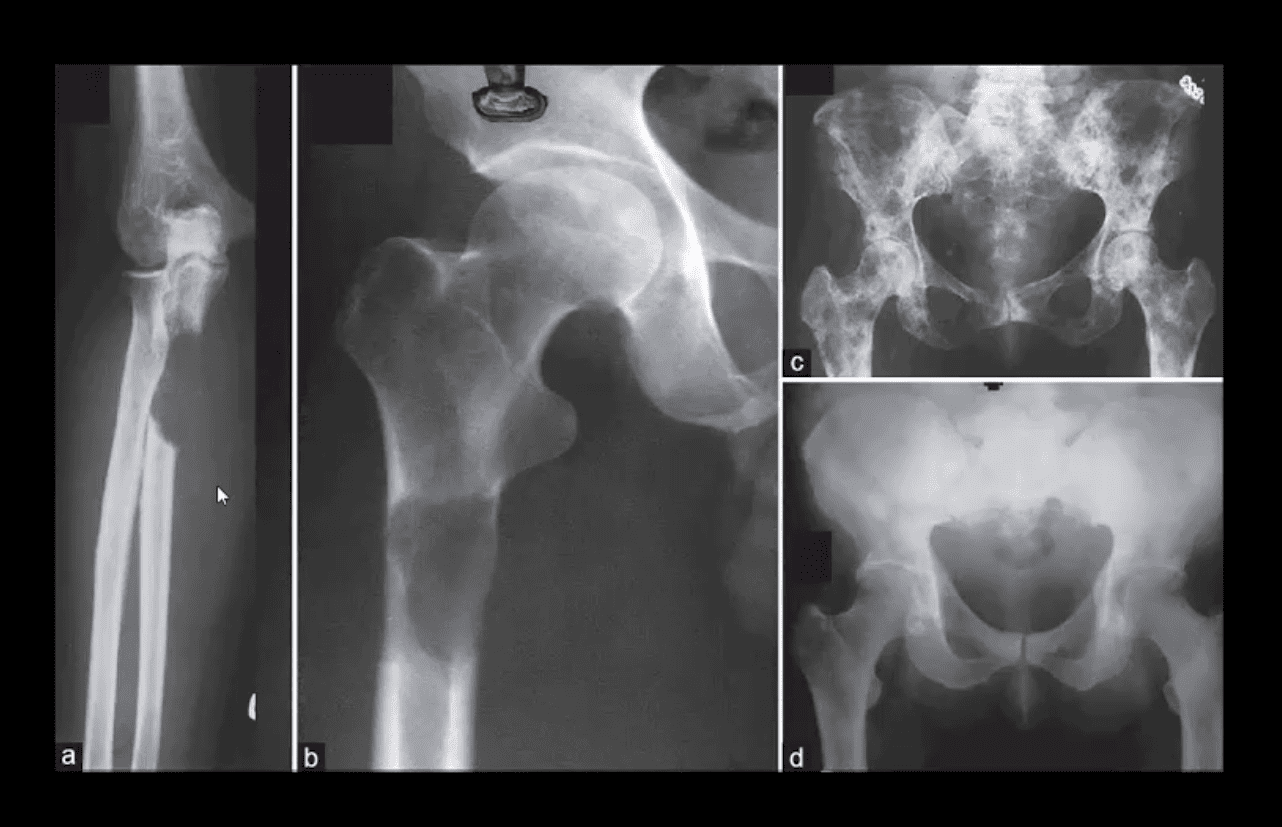
Comparison of purely lytic (a and b) versus blastic (d) and mixed (c) Mets
What primaries to consider?
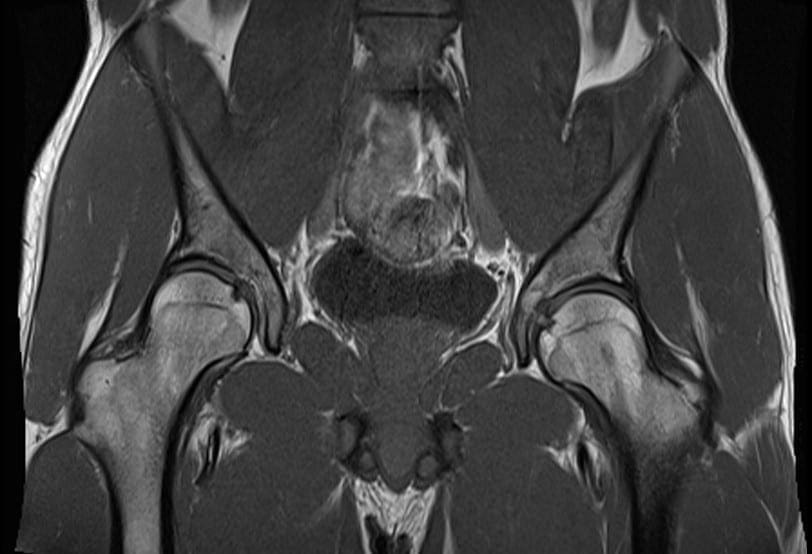
Frog leg view of the hip
Clinical Dx: Prostatic adenocarcinoma
Note diffuse blastic Mets in the proximal femur
Hx: severe shoulder and arm pain unrelieved by rest
Rad DDx: Mets, Myeloma or less frequently Lymphoma
This classic DDx is used by the majority of Radiologists when aggressive osteolytic bone lesions are noted
The patient had a known Hx of Breast CA
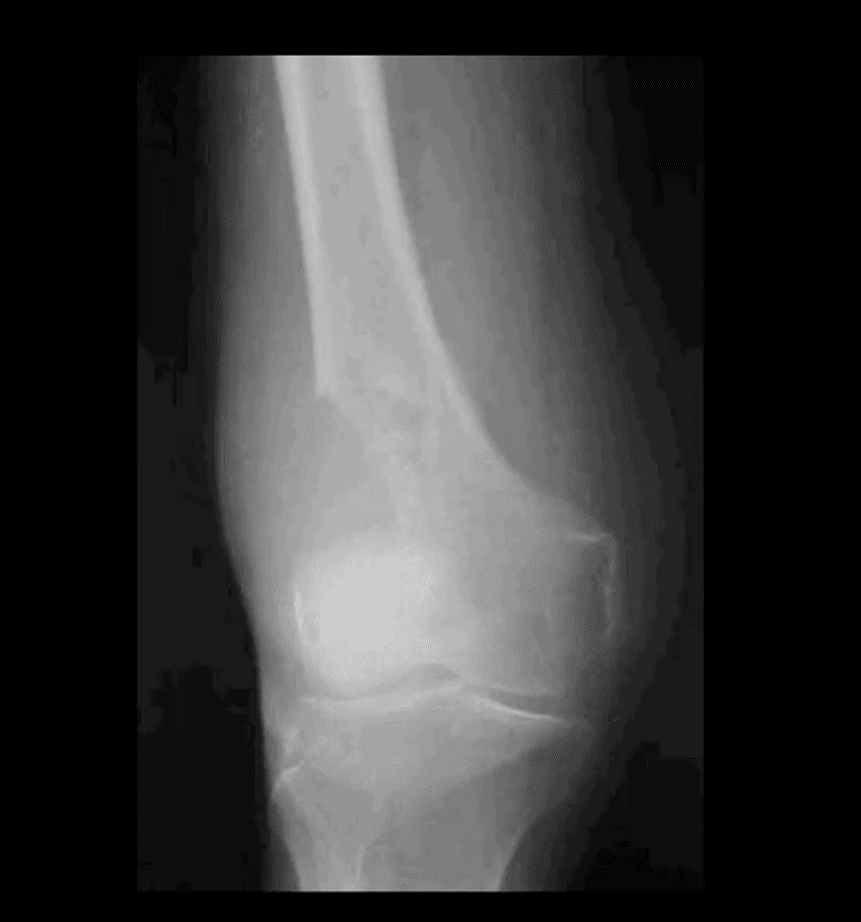
A 51-year-old female with Breast CA
Large lytic destructive lesion in the distal femoral metaphysis characteristic of aggressive osteolytic Mets
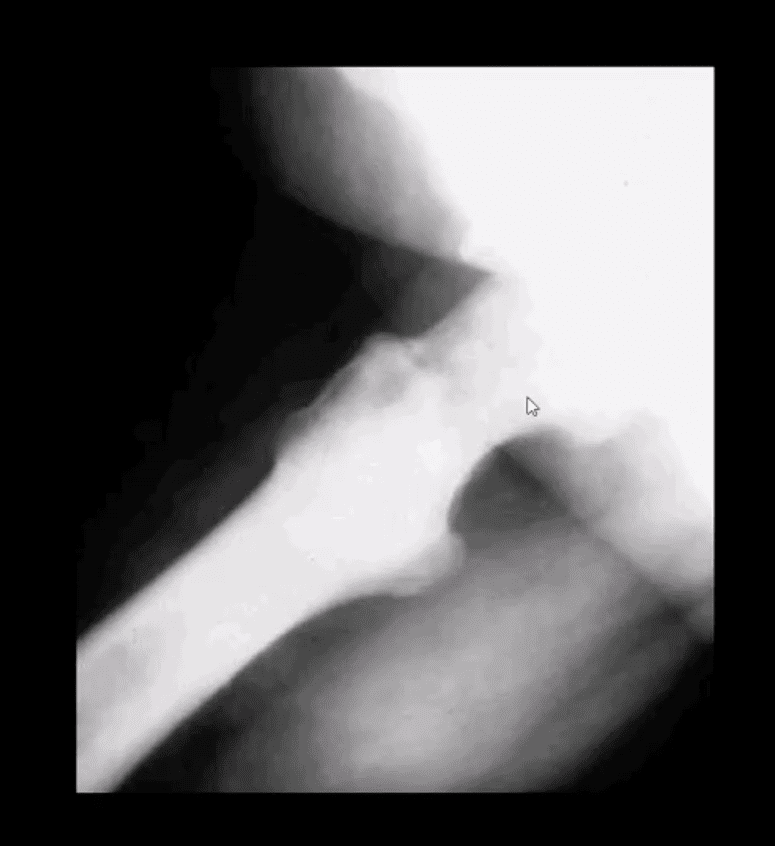
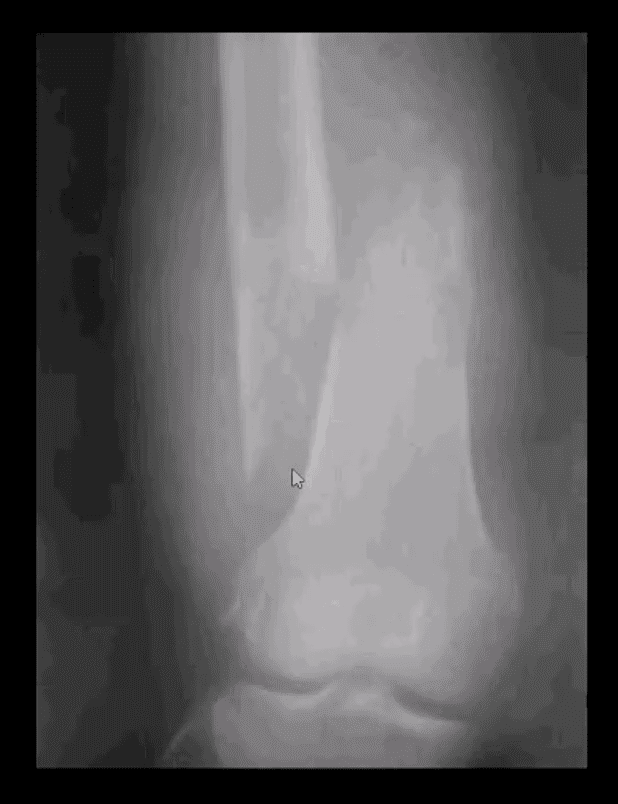
Sudden onset of severe leg pain and inability to stand in a 53-year-old female with Breast CA
Dx: Pathological fracture through the distal femoral shaft
Pathological Mets fractures in the spine and extremities are dreaded by most Oncologists due to higher association with severe complications and poor clinical prognosis
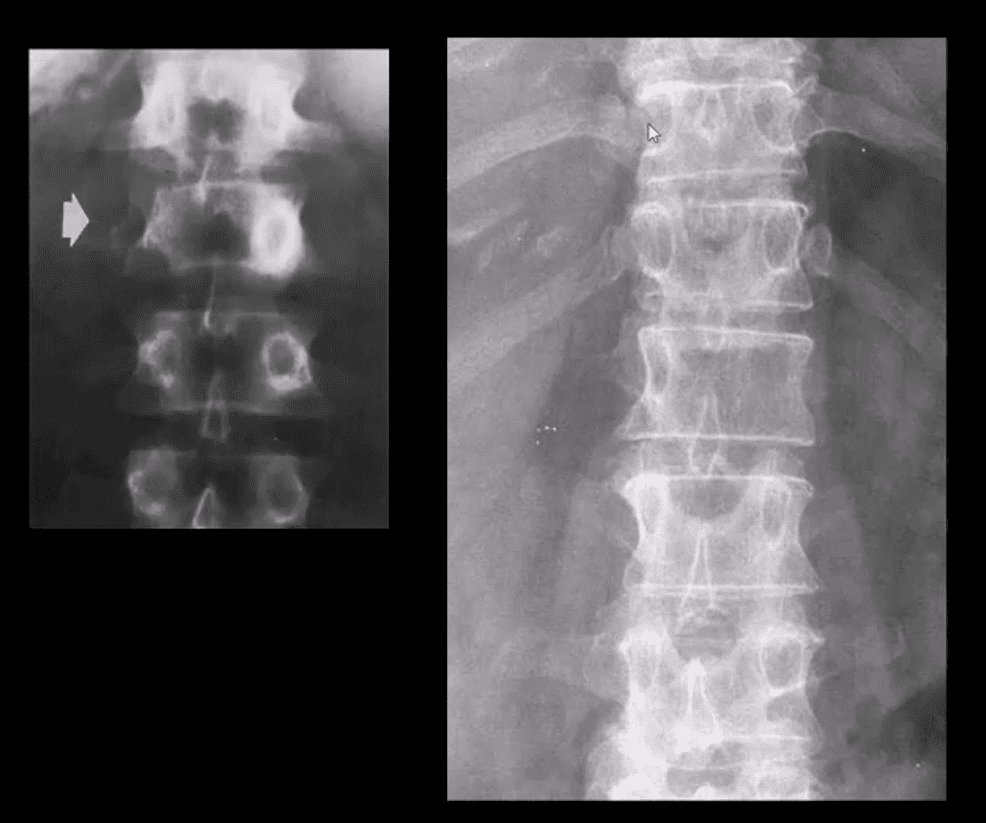
Radiographic Dx of vertebral Mets should be suspected if a “missing pedicle sign” aka “winking owl sign” is noted
DDx: pedicle agenesis (above left) shows hypertrophy and sclerosis of a contralateral pedicle d/t increased mechanical stress
Pedicle Mets are often thought of as the m/c initial site of spinal Mets
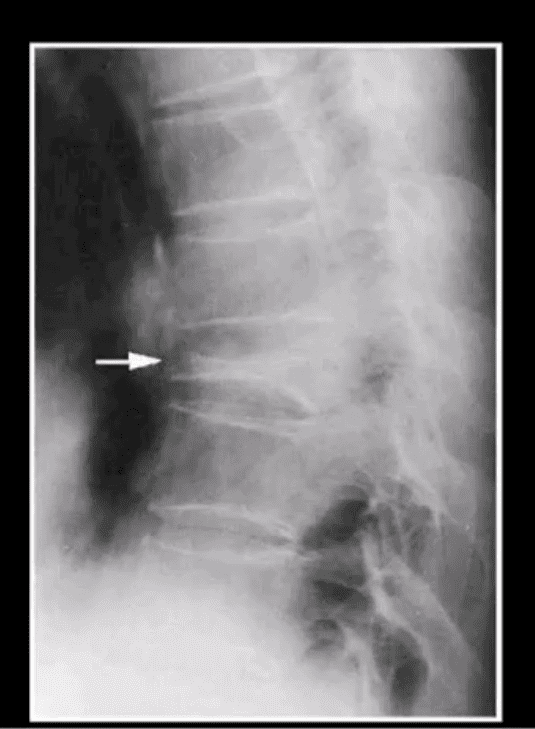
Vertebral Body Pathologic Fracture (VERTEBRA PLANA)
Isolated compression fracture at the T8 segment noted (above arrow)
The loss of the posterior and anterior height suggest an underlying pathologic condition for which the differential diagnosis includes:
Differentiating Pathological Fx of the vertebral body from an osteoporotic insufficiency Fx can be a significant challenge
Close inspection of the posterior body height is helpful but often not reliable
In metastasis, the posterior body is collapsed
In OSP, the posterior body may be maintained appearing more as anteriorly wedge fracture
MR imaging and/or radionuclide bone scan need to be performed
A skeletal radiographic survey may be used occasionally for the evaluation of bone Mets especially in well-established cases
It includes bilateral AP & lateral Thoracic and Lumbar views, AP pelvis, humeri, femurs, and the skull
Availability of special imaging has supplanted the use of skeletal radiographic survey
However, in a clinical practice skeletal radiographic study of Multiple Myeloma may still be used primarily if the diagnosis was previously established
Technetium-99 (99mTc) bone scintigraphy is very sensitive and cost-effective study:
For the detection/localization of Mets and often an assessment of their biologic activity and response to treatment
This modality is a well-established part of the workup for known as well as unknown primaries
It may also help with determination of lesions that will be most accessible and easy to biopsy
When the burden of Mets is significantly high as shown in the case above
The radiotracer uptake is being almost entirely taken in by metastatic lesions
No material is left for the kidneys to excrete
This is known as a “super scan”
Sagittal Lumbar and Lower Thoracic MRI. Multiple metastasis are noted on T1 (above right) and T2 (above left)� WI as hypointense foci of marrow replacement of the vertebral bodies in a patient with Hx of Prostate CA
MR imaging protocol with T1, T2, and T1+C gad can be used in many cases if x-radiography is unrewarding or questionable
�MRI can reveal bone marrow changes due to bone marrow replacement by Mets and surrounding edema
Typically blastic Mets appear as abnormally decreased signal intensity (hypointense) lesions on T1 and T2 pulse sequences
Purely lytic Mets often appear as hypo-intense on T1 and hype-intense on T2
Increased gadolinium uptake may also be evident on T1+C fat suppressed sequence d/t increased vascularity of malignant foci especially in very aggressive vascular neoplasms
The hip is commonly described as a “ball-and-socket” type joint. In a healthy hip, the ball at the top end of the thighbone, or femur, should fit firmly into the socket, which is part of the large pelvis bone. In babies and children with developmental dysplasia, or dislocation, of the hip, abbreviated as DDH, the hip joint may not have formed normally. As a result, the ball of the femur might easily dislocate and become loose from the socket.
Although DDH is often present from birth, it could also develop during a child’s first year of life. Recent research studies have demonstrated that infants whose thighs are swaddled closely with the hips and knees straight are at a higher risk for developing DDH. Because swaddling has become�increasingly popular, it is essential for parents to understand how to swaddle their babies safely, and they should realize that when done improperly, swaddling may cause health issues such as DDH.
Diagnosis for�Developmental Dysplasia of the Hip
In addition to visual cues, when�diagnosing for DDH, the healthcare professional will perform a careful evaluation, such as listening and feeling for “clunks” which indicates that the hip is placed in different positions. The doctor will also utilize other methods and techniques to determine if the hip is dislocated. Newborns recognized to be at higher risk for DDH are often tested using ultrasound. For babies and children, x-rays of the hip might be taken to provide further detailed images of the hip joint.
Treatment for�Developmental Dysplasia of the Hip
If DDH is discovered at birth, it can usually be treated with the use of a harness or brace. If the hip isn’t dislocated at birth, the condition might not be diagnosed until the child starts walking. At that point, treatment for DDH is much more complex, with less predictable results. If diagnosed and treated accordingly, children ought to have no restriction in function and develop the standard hip joint. DDH may result in atherosclerosis and other problems. It may produce a difference in agility or leg length.
In spite of proper treatment, hip deformity and osteoarthritis may develop later in life. This is particularly true when treatment starts after the age of 2 years. Therefore, diagnosis and treatment are essential in newborns and children with DDH. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
�
�
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
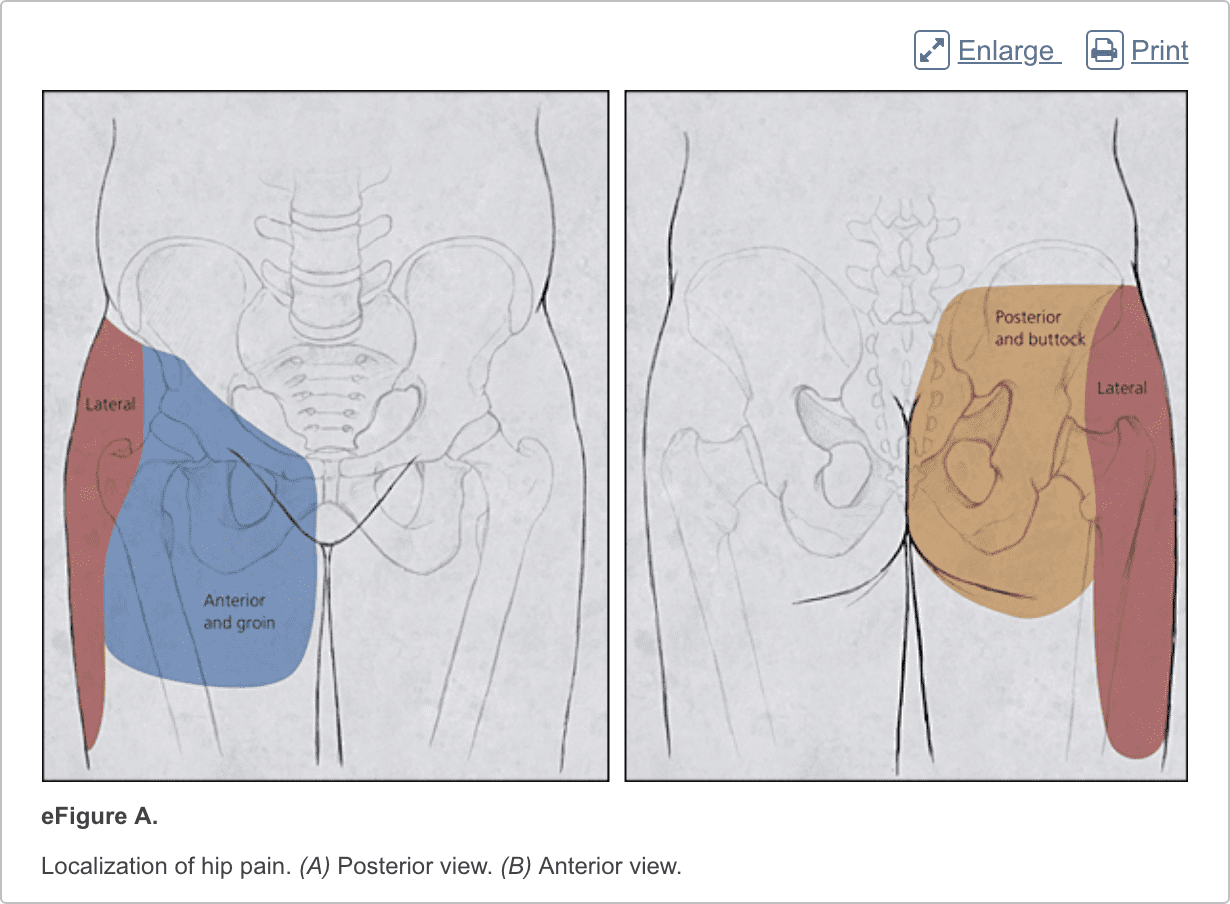
Hip pain is a well-known health issue which can be caused by a wide array of problems, however, the site of the patient’s hip pain can provide valuable information regarding the underlying cause of this common health issue. Pain on the inside of the hip or groin can be due to problems within the hip joint itself while pain on the outside of the hip, upper thigh and outer buttocks may be due to problems with the ligaments, tendons and muscles, among other soft tissues, surrounding the hip joint. Furthermore, hip pain can be due to other injuries and conditions, including back pain.
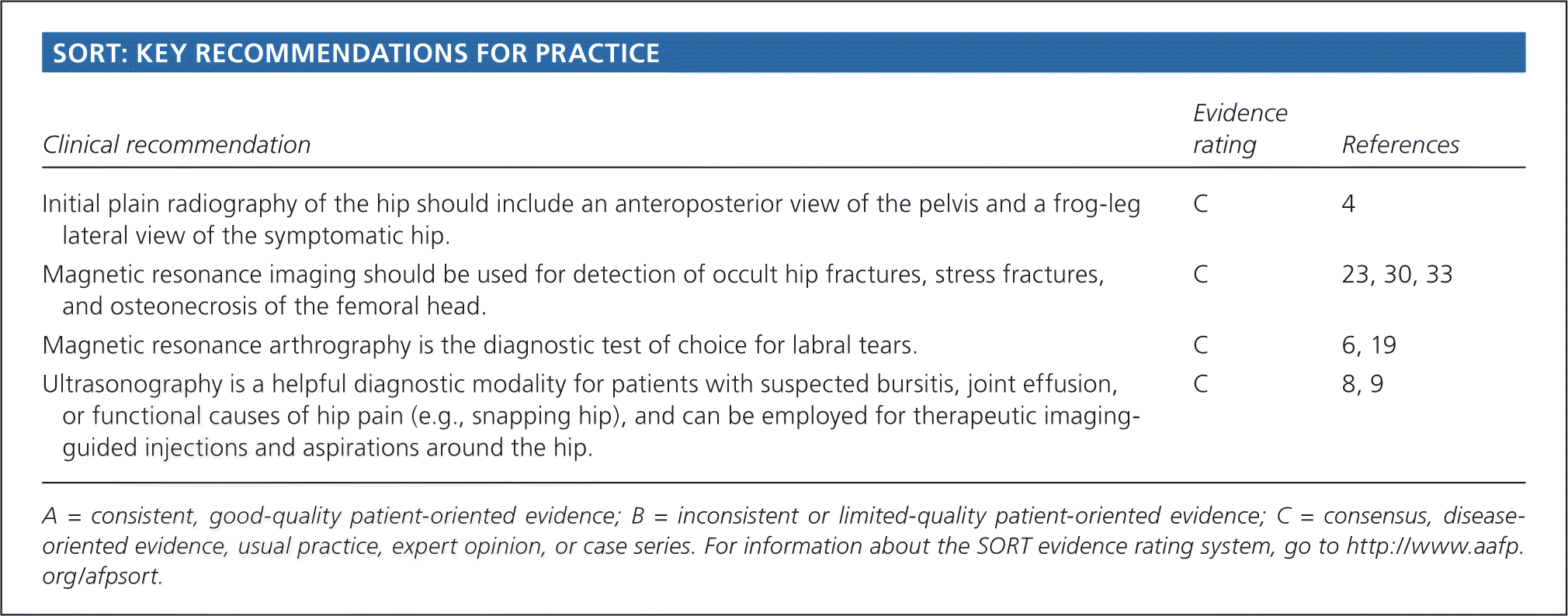
Abstract
Hip pain is a common and disabling condition that affects patients of all ages. The differential diagnosis of hip pain is broad, presenting a diagnostic challenge. Patients often express that their hip pain is localized to one of three anatomic regions: the anterior hip and groin, the posterior hip and buttock, or the lateral hip. Anterior hip and groin pain is commonly associated with intra-articular pathology, such as osteoarthritis and hip labral tears. Posterior hip pain is associated with piriformis syndrome, sacroiliac joint dysfunction, lumbar radiculopathy, and less commonly ischiofemoral impingement and vascular claudication. Lateral hip pain occurs with greater trochanteric pain syndrome. Clinical examination tests, although helpful, are not highly sensitive or specific for most diagnoses; however, a rational approach to the hip examination can be used. Radiography should be performed if acute fracture, dislocations, or stress fractures are suspected. Initial plain radiography of the hip should include an anteroposterior view of the pelvis and frog-leg lateral view of the symptomatic hip. Magnetic resonance imaging should be performed if the history and plain radiograph results are not diagnostic. Magnetic resonance imaging is valuable for the detection of occult traumatic fractures, stress fractures, and osteonecrosis of the femoral head. Magnetic resonance arthrography is the diagnostic test of choice for labral tears.
Introduction
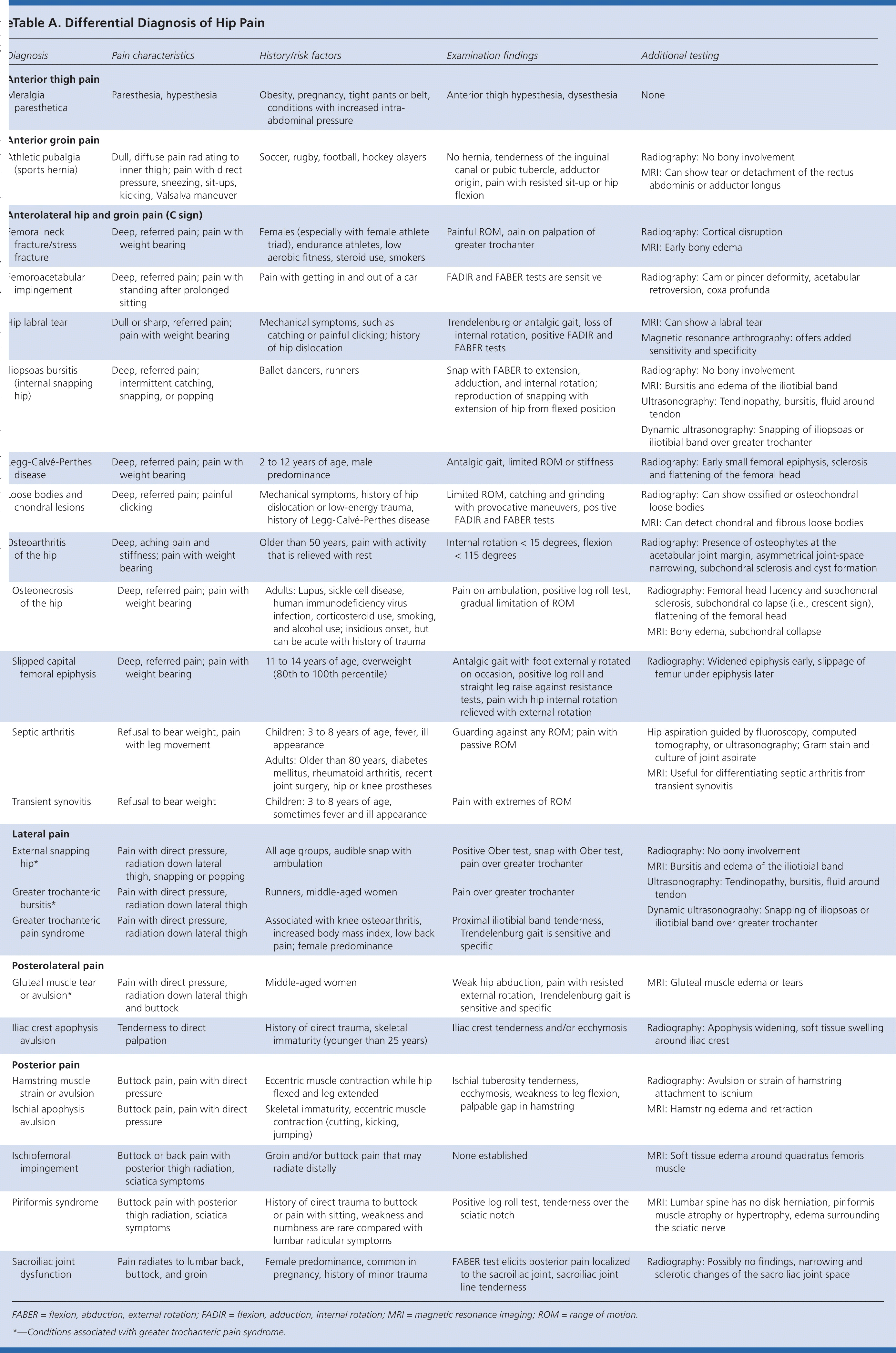
Hip pain is a common presentation in primary care and can affect patients of all ages. In one study, 14.3% of adults 60 years and older reported significant hip pain on most days over the previous six weeks.1 Hip pain often presents a diagnostic and therapeutic challenge. The differential diagnosis of hip pain (eTable A) is broad, including both intra-articular and extra-articular pathology, and varies by age. A history and physical examination are essential to accurately diagnose the cause of hip pain.
Anatomy
The hip joint is a ball-and-socket synovial joint designed to allow multiaxial motion while transferring loads between the upper and lower body. The acetabular rim is lined by fibrocartilage (labrum), which adds depth and stability to the femoroacetabular joint. The articular surfaces are covered by hyaline cartilage that dissipates shear and compressive forces during load bearing and hip motion. The hip’s major innervating nerves originate in the lumbosacral region, which can make it difficult to distinguish between primary hip pain and radicular lumbar pain.
The hip joint’s wide range of motion is second only to that of the glenohumeral joint and is enabled by the large number of muscle groups that surround the hip. The flexor muscles include the iliopsoas, rectus femoris, pectineus, and sartorius muscles. The gluteus maximus and hamstring muscle groups allow for hip extension. Smaller muscles, such as gluteus medius and minimus, piriformis, obturator externus and internus, and quadratus femoris muscles, insert around the greater trochanter, allowing for abduction, adduction, and internal and external rotation.
In persons who are skeletally immature, there are several growth centers of the pelvis and femur where injuries can occur. Potential sites of apophyseal injury in the hip region include the ischium, anterior superior iliac spine, anterior inferior iliac spine, iliac crest, lesser trochanter, and greater trochanter. The apophysis of the superior iliac spine matures last and is susceptible to injury up to 25 years of age.2
The hip joint is one of the larger joints found in the human body and it serves in locomotion as the thigh moves forward and backward. The hip joint also rotates when sitting and with changes of direction while walking. A variety of complex structures surround the hip joint. When an injury or condition affects these, it can ultimately lead to hip pain.
Dr. Alex Jimenez D.C., C.C.S.T.
Evaluation of Hip Pain
History
Age alone can narrow the differential diagnosis of hip pain. In prepubescent and adolescent patients, congenital malformations of the femoroacetabular joint, avulsion fractures, and apophyseal or epiphyseal injuries should be considered. In those who are skeletally mature, hip pain is often a result of musculotendinous strain, ligamentous sprain, contusion, or bursitis. In older adults, degenerative osteoarthritis and fractures should be considered first.
Patients with hip pain should be asked about antecedent trauma or inciting activity, factors that increase or decrease the pain, mechanism of injury, and time of onset. Questions related to hip function, such as the ease of getting in and out of a car, putting on shoes, running, walking, and going up and down stairs, can be helpful.3 Location of the pain is informative because hip pain often localizes to one of three basic anatomic regions: the anterior hip and groin, posterior hip and buttock, and lateral hip (eFigure A).
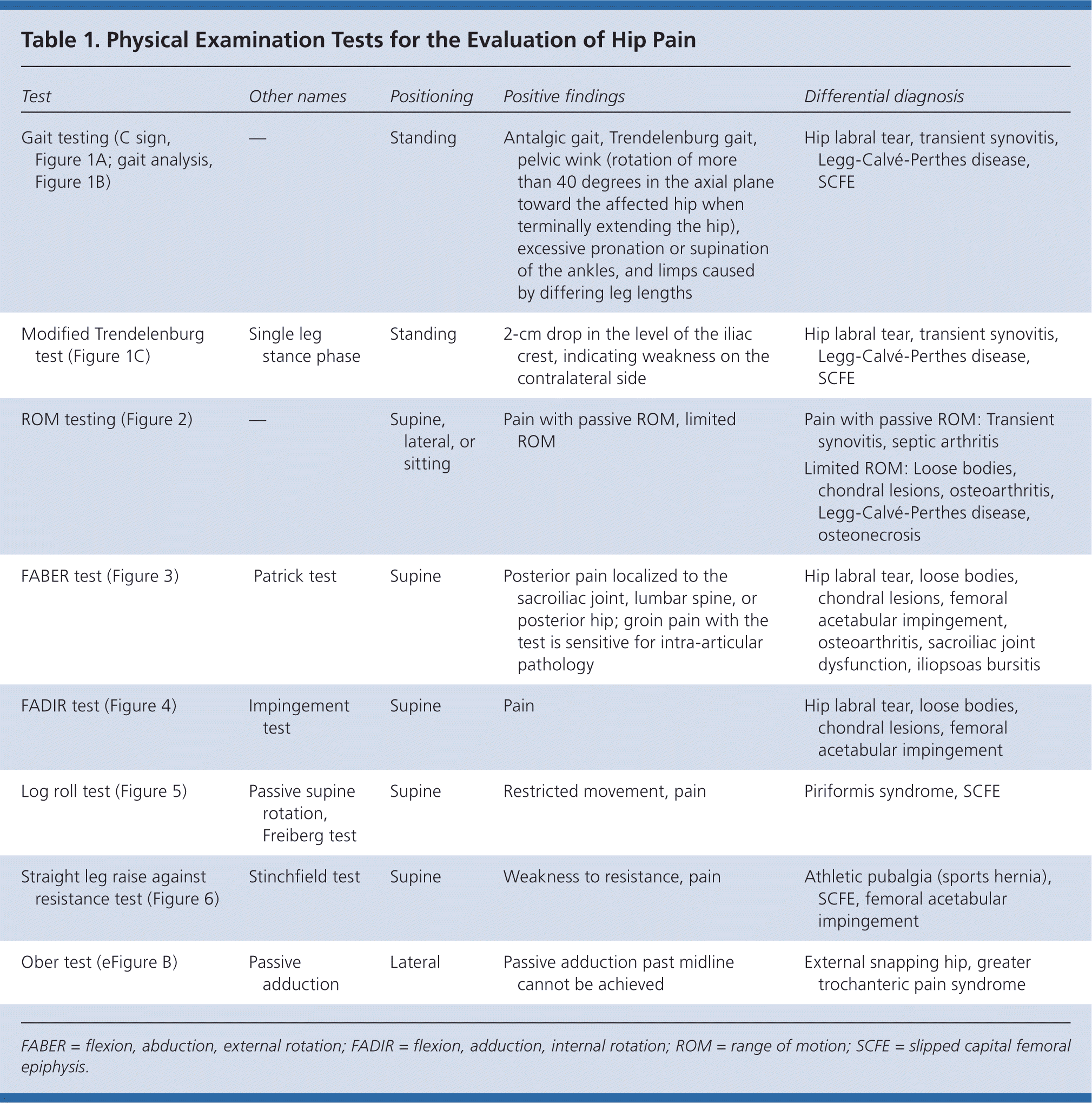
Physical Examination
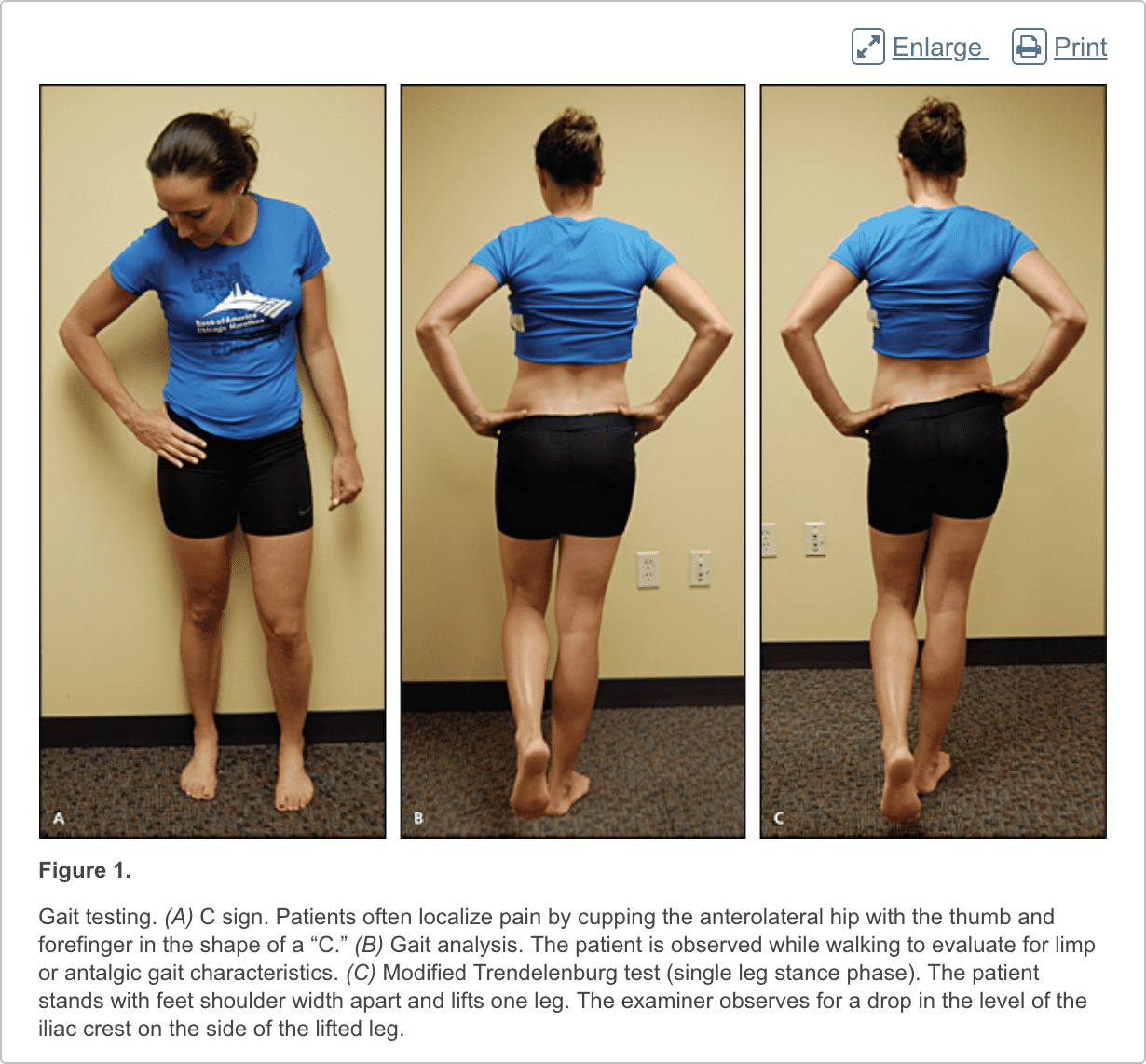
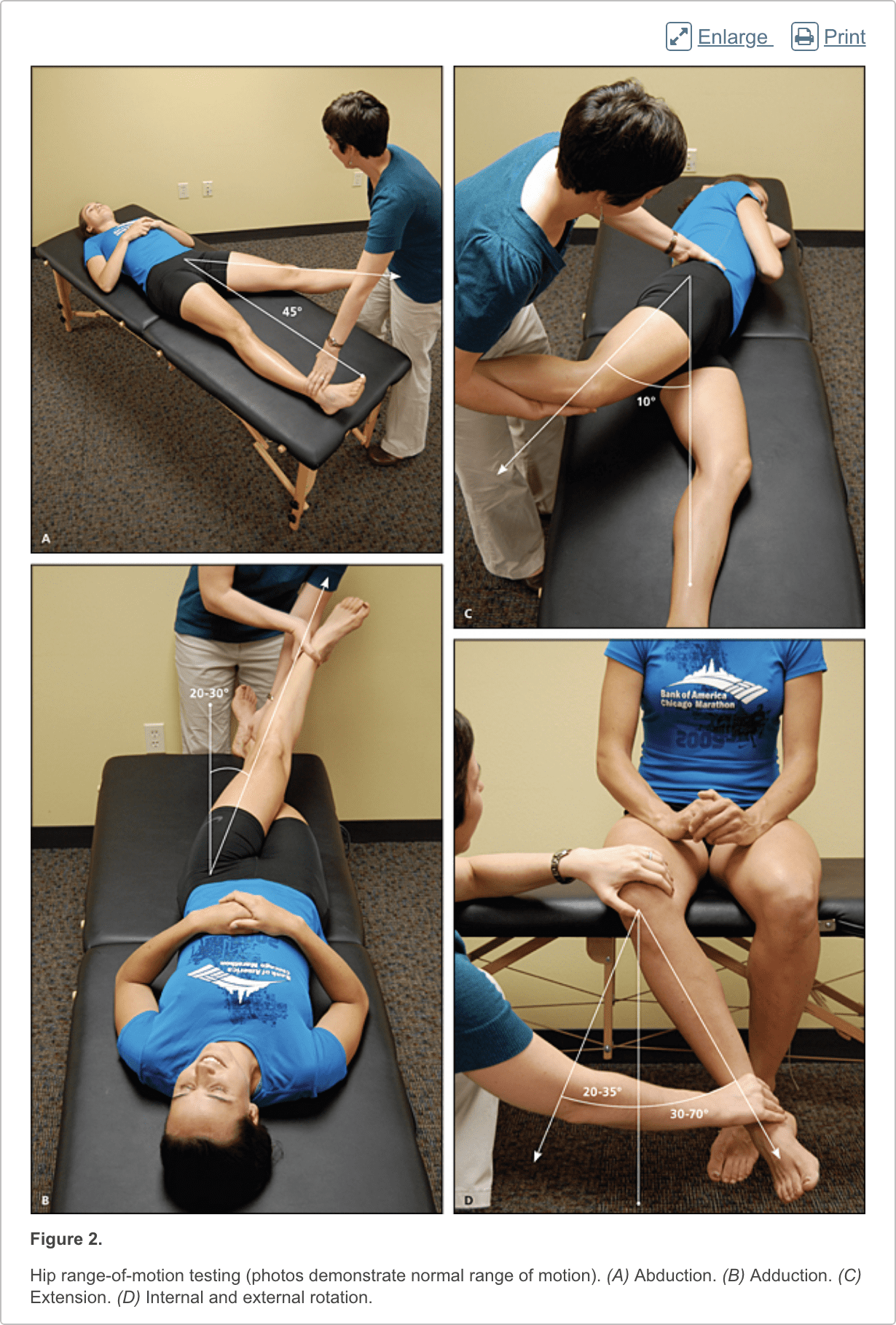
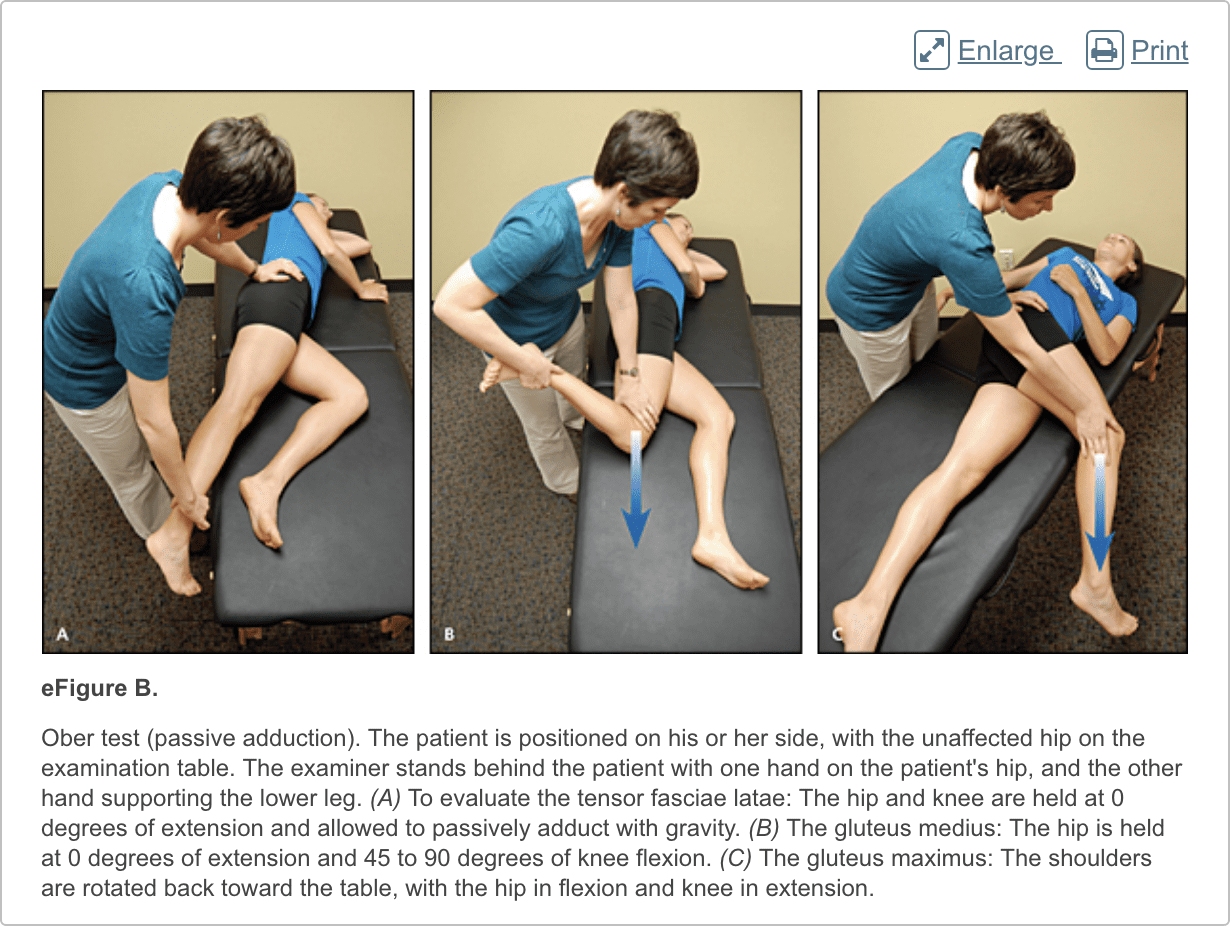
The hip examination should evaluate the hip, back, abdomen, and vascular and neurologic systems. It should start with a gait analysis and stance assessment (Figure 1), followed by evaluation of the patient in seated, supine, lateral, and prone positions (Figures 2 through 6, and eFigure B). Physical examination tests for the evaluation of hip pain are summarized in Table 1.
Imaging
Radiography. Radiography of the hip should be performed if there is any suspicion of acute fracture, dislocation, or stress fracture. Initial plain radiography of the hip should include an anteroposterior view of the pelvis and a frog-leg lateral view of the symptomatic hip.4
Magnetic Resonance Imaging and Arthrography. Conventional magnetic resonance imaging (MRI) of the hip can detect many soft tissue abnormalities, and is the preferred imaging modality if plain radiography does not identify specific pathology in a patient with persistent pain.5 Conventional MRI has a sensitivity of 30% and an accuracy of 36% for diagnosing hip labral tears, whereas magnetic resonance arthrography provides added sensitivity of 90% and accuracy of 91% for the detection of labral tears.6,7
Ultrasonography. Ultrasonography is a useful technique for evaluating individual tendons, confirming suspected bursitis, and identifying joint effusions and functional causes of hip pain.8 Ultrasonography is especially useful for safely and accurately performing imaging-guided injections and aspirations around the hip.9 It is ideal for an experienced ultrasonographer to perform the diagnostic study; however, emerging evidence suggests that less experienced clinicians with appropriate training can make diagnoses with reliability similar to that of an experienced musculoskeletal ultrasonographer.10,11
These are numerous causes for hip pain. Although some hip pain may only be temporary, other forms of hip pain can become chronic if left untreated for an extended period of time. Several common causes of hip pain include, arthritis, fracture, sprain, avascular necrosis, Gaucher’s disease, sciatica, muscle strain, iliotibial band syndrome or IT band syndrome and hematoma, among others described below.
Dr. Alex Jimenez D.C., C.C.S.T.
Differential Diagnosis of Anterior Hip Pain
Anterior hip or groin pain suggests involvement of the hip joint itself. Patients often localize pain by cupping the anterolateral hip with the thumb and forefinger in the shape of a �C.� This is known as the C sign (Figure 1A).
Osteoarthritis
Osteoarthritis is the most likely diagnosis in older adults with limited motion and gradual onset of symptoms. Patients have a constant, deep, aching pain and stiffness that are worse with prolonged standing and weight bearing. Examination reveals decreased range of motion, and extremes of hip motion often cause pain. Plain radiographs demonstrate the presence of asymmetrical joint-space narrowing, osteophytosis, and subchondral sclerosis and cyst formation.12
Femoroacetabular Impingement
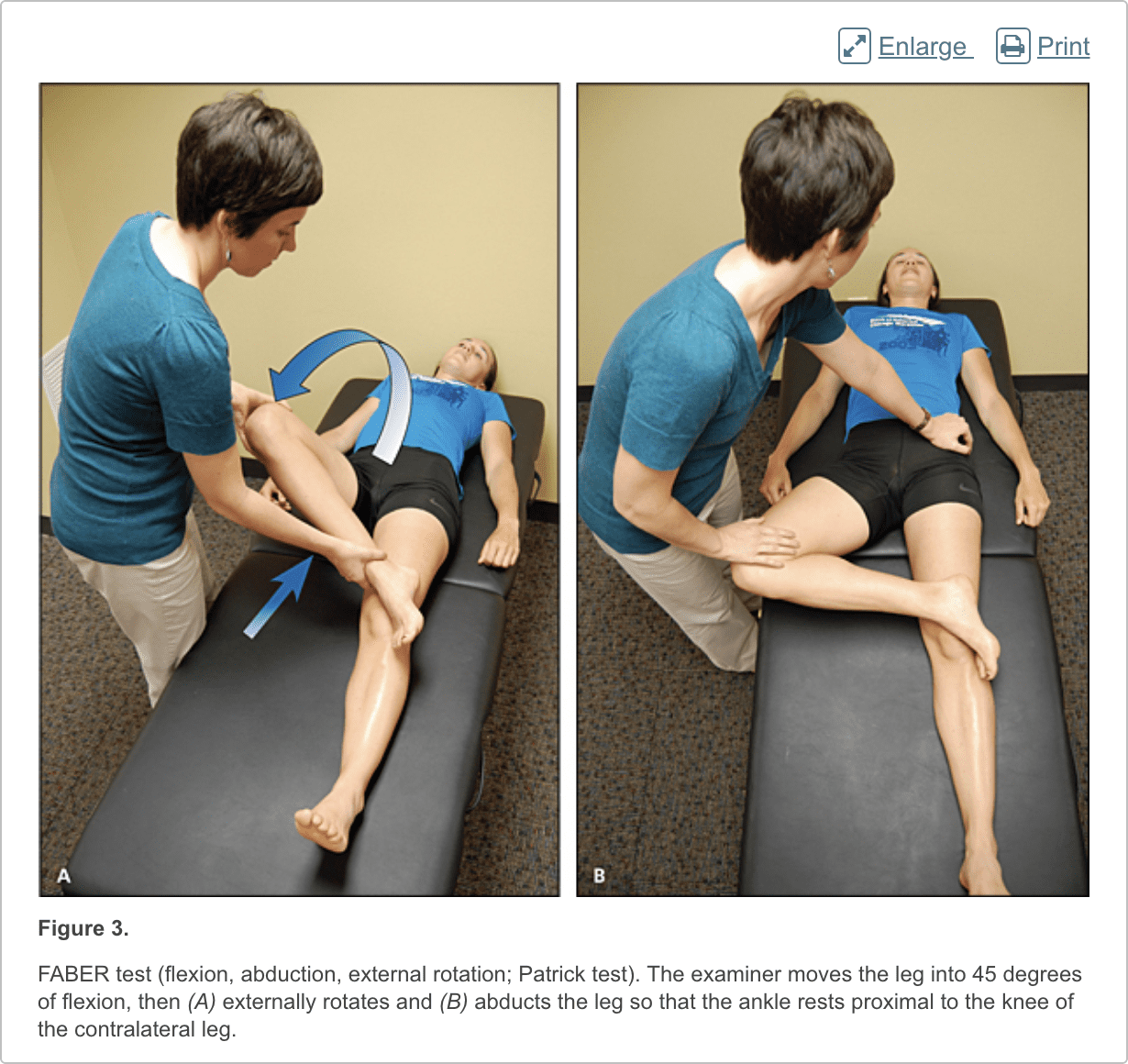
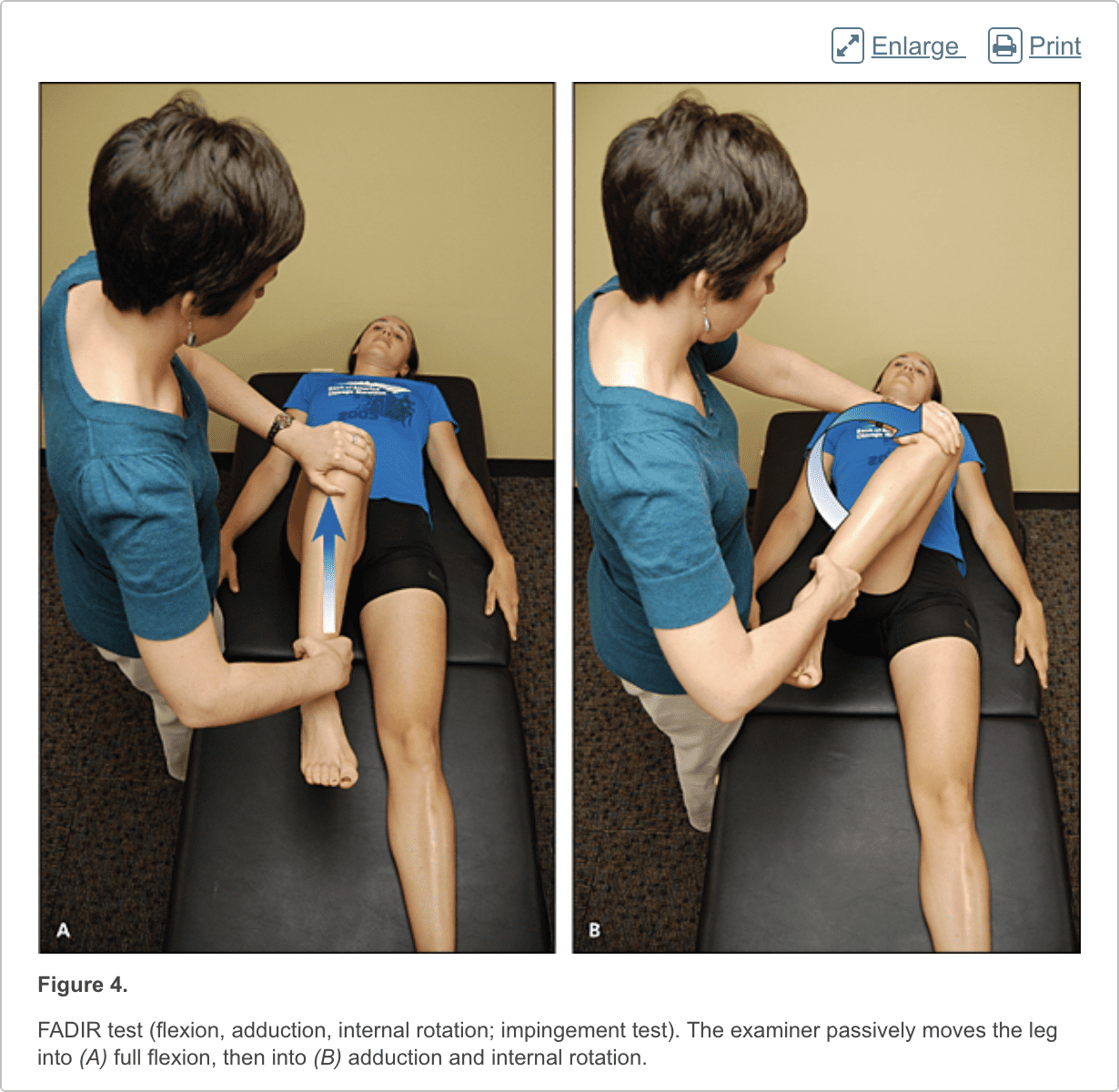
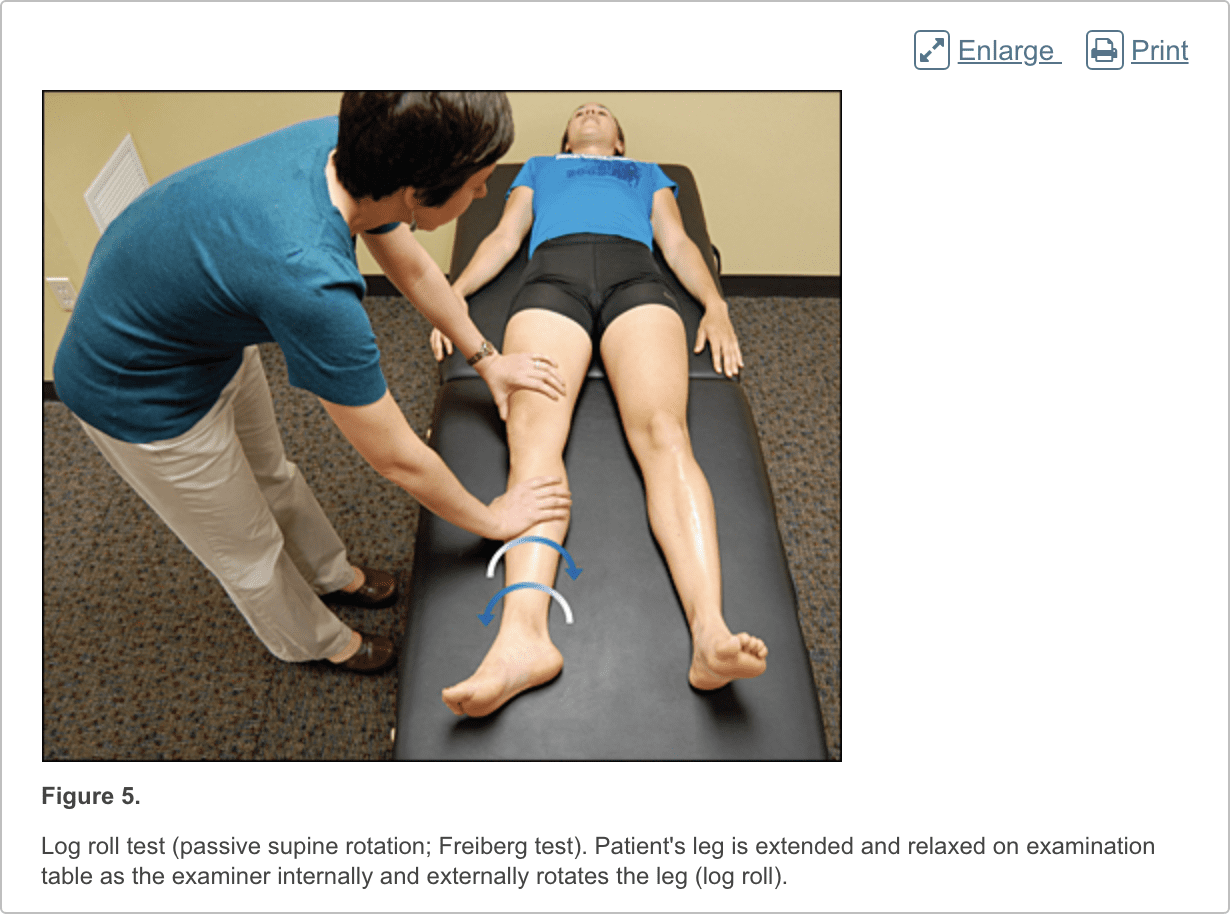
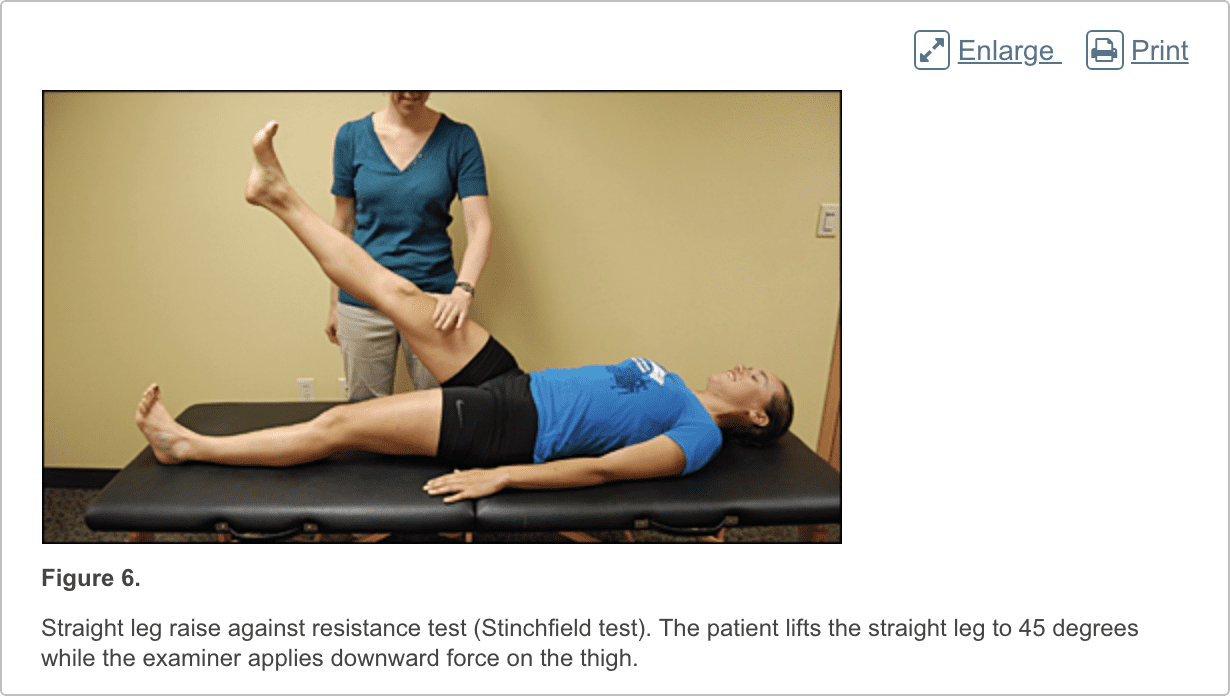
Patients with femoroacetabular impingement are often young and physically active. They describe insidious onset of pain that is worse with sitting, rising from a seat, getting in or out of a car, or leaning forward.13 The pain is located primarily in the groin with occasional radiation to the lateral hip and anterior thigh.14 The FABER test (flexion, abduction, external rotation; Figure 3) has a sensitivity of 96% to 99%. The FADIR test (flexion, adduction, internal rotation; Figure 4), log roll test (Figure 5), and straight leg raise against resistance test (Figure 6) are also effective, with sensitivities of 88%, 56%, and 30%, respectively.14,15 In addition to the anteroposterior and lateral radiograph views, a Dunn view should be obtained to help detect subtle lesions.16
Hip Labral Tear
Hip labral tears cause dull or sharp groin pain, and one-half of patients with a labral tear have pain that radiates to the lateral hip, anterior thigh, and buttock. The pain usually has an insidious onset, but occasionally begins acutely after a traumatic event. About one-half of patients with this injury also have mechanical symptoms, such as catching or painful clicking with activity.17 The FADIR and FABER tests are effective for detecting intra-articular pathology (the sensitivity is 96% to 75% for the FADIR test and is 88% for the FABER test), although neither test has high specificity.14,15,18 Magnetic resonance arthrography is considered the diagnostic test of choice for labral tears.6,19 However, if a labral tear is not suspected, other less invasive imaging modalities, such as plain radiography and conventional MRI, should be used first to rule out other causes of hip and groin pain.
Iliopsoas Bursitis (Internal Snapping Hip)
Patients with this condition have anterior hip pain when extending the hip from a flexed position, often associated with intermittent catching, snapping, or popping of the hip.20 Dynamic real-time ultrasonography is particularly useful in evaluating the various forms of snapping hip.8
Occult or Stress Fracture
Occult or stress fracture of the hip should be considered if trauma or repetitive weight-bearing exercise is involved, even if plain radiograph results are negative.21 Clinically, these injuries cause anterior hip or groin pain that is worse with activity.21 Pain may be present with extremes of motion, active straight leg raise, the log roll test, or hopping.22 MRI is useful for the detection of occult traumatic fractures and stress fractures not seen on plain radiographs.23
Transient Synovitis and Septic Arthritis
Acute onset of atraumatic anterior hip pain that results in impaired weight bearing should raise suspicion for transient synovitis and septic arthritis. Risk factors for septic arthritis in adults include age older than 80 years, diabetes mellitus, rheumatoid arthritis, recent joint surgery, and hip or knee prostheses.24 Fever, complete blood count, erythrocyte sedimentation rate, and C-reactive protein level should be used to evaluate the risk of septic arthritis.25,26 MRI is useful for differentiating septic arthritis from transient synovitis.27,28 However, hip aspiration using guided imaging such as fluoroscopy, computed tomography, or ultrasonography is recommended if a septic joint is suspected.29
Osteonecrosis
Legg-Calv�-Perthes disease is an idiopathic osteonecrosis of the femoral head in children two to 12 years of age, with a male-to-female ratio of 4:1.4 In adults, risk factors for osteonecrosis include systemic lupus erythematosus, sickle cell disease, human immunodeficiency virus infection, smoking, alcoholism, and corticosteroid use.30,31 Pain is the presenting symptom and is usually insidious. Range of motion is initially preserved but can become limited and painful as the disease progresses.32 MRI is valuable in the diagnosis and prognostication of osteonecrosis of the femoral head.30,33
Differential Diagnosis of Posterior Hip and Buttock Pain
Piriformis Syndrome and Ischiofemoral Impingement
Piriformis syndrome causes buttock pain that is aggravated by sitting or walking, with or without ipsilateral radiation down the posterior thigh from sciatic nerve compression.34,35 Pain with the log roll test is the most sensitive test, but tenderness with palpation of the sciatic notch can help with the diagnosis.35
Ischiofemoral impingement is a less well-understood condition that can lead to nonspecific buttock pain with radiation to the posterior thigh.36,37 This condition is thought to be a result of impingement of the quadratus femoris muscle between the lesser trochanter and the ischium.
Unlike sciatica from disc herniation, piriformis syndrome and ischiofemoral impingement are exacerbated by active external hip rotation. MRI is useful for diagnosing these conditions.38
Other
Other causes of posterior hip pain include sacroiliac joint dysfunction,39 lumbar radiculopathy,40 and vascular claudication.41 The presence of a limp, groin pain, and limited internal rotation of the hip is more predictive of hip disorders than disorders originating from the low back.42
Differential Diagnosis of Lateral Hip Pain
Greater Trochanteric Pain Syndrome
Lateral hip pain affects 10% to 25% of the general population.43 Greater trochanteric pain syndrome refers to pain over the greater trochanter. Several disorders of the lateral hip can lead to this type of pain, including iliotibial band thickening, bursitis, and tears of the gluteus medius and minimus muscle attachment.43�45 Patients may have mild morning stiffness and may be unable to sleep on the affected side. Gluteus minimus and medius injuries present with pain in the posterior lateral aspect of the hip as a result of partial or full-thickness tearing at the gluteal insertion. Most patients have an atraumatic, insidious onset of symptoms from repetitive use.43,45,46
In conclusion, hip pain is a common complaint which may occur due to a wide variety of health issues. Moreover, the precise location of the patient’s hip pain can provide valuable information to healthcare professionals regarding the underlying cause of the problem. The purpose of the article above was to demonstrate and discuss the evaluation of the patient with hip pain. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Data Sources: We searched articles on hip pathology in American Family Physician, along with their references. We also searched the Agency for Healthcare Research and Quality Evidence Reports, Clinical Evidence, Institute for Clinical Systems Improvement, the U.S. Preventive Services Task Force guidelines, the National Guideline Clearinghouse, and UpToDate. We performed a PubMed search using the keywords greater trochanteric pain syndrome, hip pain physical examination, imaging femoral hip stress fractures, imaging hip labral tear, imaging osteomyelitis, ischiofemoral impingement syndrome, meralgia paresthetica review, MRI arthrogram hip labrum, septic arthritis systematic review, and ultrasound hip pain. Search dates: March and April 2011, and August 15, 2013.
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
1.�Christmas C, Crespo CJ, Franckowiak SC, et al. How common is hip pain among older adults? Results from the Third National Health and Nutrition Examination Survey.�J Fam Pract. 2002;51(4):345�348.
2.�Rossi F, Dragoni S. Acute avulsion fractures of the pelvis in adolescent competitive athletes.�Skeletal Radiol. 2001;30(3):127�131.
3.�Martin HD, Shears SA, Palmer IJ. Evaluation of the hip.�Sports Med Arthrosc. 2010;18(2):63�75.
4.�Gough-Palmer A, McHugh K. Investigating hip pain in a well child.�BMJ. 2007;334(7605):1216�1217.
5.�Bencardino JT, Palmer WE. Imaging of hip disorders in athletes.�Radiol Clin North Am. 2002;40(2):267�287.
6.�Czerny C, Hofmann S, Neuhold A, et al. Lesions of the acetabular labrum: accuracy of MR imaging and MR arthrography in detection and staging.�Radiology. 1996;200(1):225�230.
7.�Czerny C, Hofmann S, Urban M, et al. MR arthrography of the adult acetabular capsular-labral complex.�AJR Am J Roentgenol. 1999;173(2):345�349.
8.�Deslandes M, Guillin R, Cardinal E, et al. The snapping iliopsoas tendon: new mechanisms using dynamic sonography.�AJR Am J Roentgenol. 2008;190(3):576�581.
9.�Blankenbaker DG, De Smet AA. Hip injuries in athletes.�Radiol Clin North Am. 2010;48(6):1155�1178.
10.�Balint PV, Sturrock RD. Intraobserver repeatability and interobserver reproducibility in musculoskeletal ultrasound imaging measurements.�Clin Exp Rheumatol. 2001;19(1):89�92.
11.�Ramwadhdoebe S, Sakkers RJ, Uiterwaal CS, et al. Evaluation of a training program for general ultrasound screening for developmental dysplasia of the hip in preventive child health care.�Pediatr Radiol. 2010;40(10):1634�1639.
12.�Altman R, Alarc�n G, Appelrouth D, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip.�Arthritis Rheum. 1991;34(5):505�514.
14.�Clohisy JC, Knaus ER, Hunt DM, et al. Clinical presentation of patients with symptomatic anterior hip impingement.�Clin Orthop Relat Res. 2009;467(3):638�644.
15.�Ito K, Leunig M, Ganz R. Histopathologic features of the acetabular labrum in femoroacetabular impingement.�Clin Orthop Relat Res. 2004;(429):262�271.
16.�Beall DP, Sweet CF, Martin HD, et al. Imaging findings of femoroacetabular impingement syndrome.�Skeletal Radiol. 2005;34(11):691�701.
17.�Burnett RS, Della Rocca GJ, Prather H, et al. Clinical presentation of patients with tears of the acetabular labrum.�J Bone Joint Surg Am. 2006;88(7):1448�1457.
18.�Leunig M, Werlen S, Ungersb�ck A, et al. Evaluation of the acetabular labrum by MR arthrography [published correction appears in�J Bone Joint Surg Br. 1997;79(4):693].�J Bone Joint Surg Br. 1997;79(2):230�234.
19.�Groh MM, Herrera J. A comprehensive review of hip labral tears.�Curr Rev Musculoskelet Med. 2009;2(2):105�117.
20.�Blankenbaker DG, De Smet AA, Keene JS. Sonography of the iliopsoas tendon and injection of the iliopsoas bursa for diagnosis and management of the painful snapping hip.�Skeletal Radiol. 2006;35(8):565�571.
21.�Egol KA, Koval KJ, Kummer F, et al. Stress fractures of the femoral neck.�Clin Orthop Relat Res. 1998;(348):72�78.
22.�Fullerton LR Jr, Snowdy HA. Femoral neck stress fractures.�Am J Sports Med. 1988;16(4):365�377.
24.�Margaretten ME, Kohlwes J, Moore D, et al. Does this adult patient have septic arthritis?�JAMA. 2007;297(13):1478�1488.
25.�Eich GF, Superti-Furga A, Umbricht FS, et al. The painful hip: evaluation of criteria for clinical decision-making.�Eur J Pediatr. 1999;158(11):923�928.
26.�Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children.�J Bone Joint Surg Am. 1999;81(12):1662�1670.
27.�Learch TJ, Farooki S. Magnetic resonance imaging of septic arthritis.�Clin Imaging. 2000;24(4):236�242.
28.�Lee SK, Suh KJ, Kim YW, et al. Septic arthritis versus transient synovitis at MR imaging.�Radiology. 1999;211(2):459�465.
29.�Leopold SS, Battista V, Oliverio JA. Safety and efficacy of intraarticular hip injection using anatomic landmarks.�Clin Orthop Relat Res. 2001; (391):192�197.
30.�Mitchell DG, Rao VM, Dalinka MK, et al. Femoral head avascular necrosis: correlation of MR imaging, radiographic staging, radionuclide imaging, and clinical findings.�Radiology. 1987;162(3):709�715.
31.�Mont MA, Zywiel MG, Marker DR, et al. The natural history of untreated asymptomatic osteonecrosis of the femoral head.�J Bone Joint Surg Am. 2010;92(12):2165�2170.
32.�Assouline-Dayan Y, Chang C, Greenspan A, et al. Pathogenesis and natural history of osteonecrosis.�Semin Arthritis Rheum. 2002;32(2):94�124.
33.�Totty WG, Murphy WA, Ganz WI, et al. Magnetic resonance imaging of the normal and ischemic femoral head.�AJR Am J Roentgenol. 1984;143(6):1273�1280.
35.�Hopayian K, Song F, Riera R, et al. The clinical features of the piriformis syndrome.�Eur Spine J. 2010;19(12):2095�2109.
36.�Torriani M, Souto SC, Thomas BJ, et al. Ischiofemoral impingement syndrome.�AJR Am J Roentgenol. 2009;193(1):186�190.
37.�Ali AM, Whitwell D, Ostlere SJ. Case report: imaging and surgical treatment of a snapping hip due to ischiofemoral impingement.�Skeletal Radiol. 2011;40(5):653�656.
38.�Lee EY, Margherita AJ, Gierada DS, et al. MRI of piriformis syndrome.�AJR Am J Roentgenol. 2004;183(1):63�64.
39.�Slipman CW, Jackson HB, Lipetz JS, et al. Sacroiliac joint pain referral zones.�Arch Phys Med Rehabil. 2000;81(3):334�338.
40.�Moore KL, Dalley AF, Agur AM.�Clinically Oriented Anatomy. 6th ed. Philadelphia, Pa.: Lippincott Williams & Wilkins; 2010.
41.�Adlakha S, Burket M, Cooper C. Percutaneous intervention for chronic total occlusion of the internal iliac artery for unrelenting buttock claudication.�Catheter Cardiovasc Interv. 2009;74(2):257�259.
42.�Brown MD, Gomez-Marin O, Brookfield KF, et al. Differential diagnosis of hip disease versus spine disease.�Clin Orthop Relat Res. 2004; (419):280�284.
43.�Segal NA, Felson DT, Torner JC, et al.; Multicenter Osteoarthritis Study Group. Greater trochanteric pain syndrome.�Arch Phys Med Rehabil. 2007;88(8):988�992.
44.�Strauss EJ, Nho SJ, Kelly BT. Greater trochanteric pain syndrome.�Sports Med Arthrosc. 2010;18(2):113�119.
The workstation is one of the most damaging places you can spend your day when it comes to your spine. Office chairs are not designed to promote good posture or spinal health while desks and computer monitors are notorious for being too low or too high. The result can cause pain in your neck and back, headaches, and a variety of other conditions.� A stability ball could be the answer.
However, if you have a job that requires you to sit at a desk for an extended period, what can you do? Are you stuck with an achy, stiff neck and back because your workstation doesn�t promote a healthy posture? You don�t have to suffer; you can work healthier and smarter. Using an exercise ball as your chair is a great way to combat the painful and even detrimental effects of the traditional desk and chair.
Stability Ball as an Office Chair
A stability ball, also known as a Swiss ball, exercise ball, or physioball, is a large, inflatable ball used for training. A stability ball helps to increase pillar strength, improve stability and have better balance. It is large, making it high enough that it can easily be used as a desk chair.
At least one company has combined the fitness benefits of a stability ball with some of the convenient features of an office chair (wheels, lumbar support, etc.). Gaiam Balance Ball Chairs are stability balls that are intended to be used as chairs. The ball needs to be inflated before use and may need to be reinflated from time to time. It also has a 300-pound weight capacity. It is a somewhat pricier alternative to the plain stability ball.
How Sitting on a Stability Ball Benefits your Spine
There are at least three outstanding benefits you can enjoy by using a stability ball as your chair. Try it for just 30 days and see the difference for yourself. In that time you will see:
Your core muscles are toned. As you balance on the stability ball, it forces you to engage your core muscles including those in your low back, abdominal, and pelvic floor. It will keep your muscles engaged for extended periods of time but also encourage you to move for little extra core work. This, in turn, will help to keep your spine correctly aligned and stabilized.
Your back pain is relieved. Sitting on your stability ball improves your circulation, encouraging blood flow throughout your body. An office chair, on the other hand, does just the opposite. This is helpful in relieving pain. It keeps your spine aligned which also helps with any back pain you may experience. This is in part to the core strength you develop, but also because you are less likely to slouch or sit in a position that puts a strain on your back.
You have better posture.�A better-aligned spine naturally leads to better posture. Sitting on the ball works your core, strengthening those muscles so that your spine is supported, resulting in better posture. You will find that you sit up straighter and over time you will walk taller. Better posture is perfect for your spine, making it more flexible and stronger.
It should be noted that it isn�t healthy to sit in any position for too long. Stand up and move about every hour or so. While the stability ball causes you to change positions throughout the day, you also need full body movement, which includes standing, stretching and walking.
Every new parent has experienced a fussy baby with colic � some more often than others. It is always the same, though, an inconsolable baby and frustrated, frazzled parents who only want to comfort their child but can�t. It hurts to know that your baby is uncomfortable, or worse, in pain, and there is nothing you can do about it.
Colic can leave parents feeling helpless. There is a treatment, though, that has given many parents hope and brought relief to their little ones. Chiropractic is an effective treatment for colic that is drug-free and gentle. Both infants and their parents reap the benefits because when a baby is happy, mom and dad are happy.
What is Colic?
Colic is a condition that occurs in healthy, well-fed infants, beginning when the baby is a few weeks old. By the time the baby is three months old, the condition usually improves, and by five months it is often no longer occurring. It is marked by inconsolable crying that meets three criteria regarding length:
More than three hours a day
Three days a week or more
For three weeks or longer
During these episodes, it seems as if there is nothing that can be done for the baby. The good news is, it is relatively short-lived, but while it is happening it can cause a great deal of distress to the baby and the parents.
Symptoms of Colic
All babies cry and even get fussy from time to time. That is just normal baby behavior; it does not necessarily point to colic as the culprit. When a baby that is well fed and otherwise healthy, symptoms of colic may include:
Episodes of crying that are often predictable. Colic usually occurs in the latter part of the day � late afternoon or evening � and at around the same time each day. So a baby with colic will usually get fussy at the same time and the period of distress can last a few minutes to several hours.
Baby is inconsolable with intense crying. The baby with colic will seem very distressed. The cry is very high pitched and no response to attempts to comfort. The baby�s face may become flushed, and near the end of the episode they may pass gas or have a bowel movement.
The crying does not seem to have a source or reason. Babies cry, all babies � but they are usually crying because they need something. They may cry because they are hungry, need a diaper change, or want to be held by mom or dad. A colicky baby will cry for no apparent reason.
There are Changes in posture. Several posture changes are relatively consistent with colic. The baby will often clench their fists, curl their legs, and tense the abdominal muscles.
Chiropractic for Colic
Childbirth is not easy, and it isn�t gentle. As the baby passes through the birth canal and emerges, it�s little body is stretched and compressed which can cause misalignment of the back and neck. If the labor was extensive, there was prolonged pushing, or if a device like forceps or vacuum extraction is used, the chances of misalignment are very likely. These misalignments can lead to difficulty nursing and even impede normal organ function. This can lead to digestive issues which may lead to colic.
Some parents may be uncomfortable at first when they consider getting chiropractic care for their infant, but it is safe and gentle. The popping and cracking that is associated with chiropractic is not a part of infant and child chiropractic. The doctor applies gentle pressure to areas on the neck and back, using his fingers. Many times the baby will completely relax during these adjustments.
Chiropractic for colic is very useful. Parents considering this type of treatment for their baby should look for a chiropractor who has experience providing treatment for babies. It can make a world of difference for a colicky, distressed baby.
There is no denying that water is an integral part of good health. Dehydration can cause problems with skin, digestion, and organ function. It can cause leg and foot cramps and impair cognitive processes. Staying well hydrated is vital to overall wellness. Because water is part of every cell in the body, and when we don�t drink enough water, the body suffers.
Good spinal health begins with proper hydration. The spine is constructed in such a way that dehydration can cause limited mobility, decreased flexibility, and pain. It can make the backbone to age faster than it should which impacts the entire body. As the natural functions begin to break down the body suffers, and it isn�t long and depression and anxiety often set in. The spine depends heavily on hydration.
Overview of the Spine
The spine of made up of vertebrae, a row of bones that sit on top of each other, connected by small joints. A disc sits between each vertebra, cushioning it and acting as a shock absorber. It allows the spine to flex, bend, and move about without the bones rubbing together.
Each disc has a fluid center (nucleus pulposis) that is surrounded by a flexible, sturdy ring. The ring contains a gel-like substance while the center of the disc is comprised of water. The outer ring protects the center, and the center protects the vertebrae, acting as a cushion for the bones.
If the fluid center does not have adequate water, it cannot do its job, and the spine begins to experience problems. Aging makes it more difficult for the discs to rehydrate and a sedentary lifestyle also complicates the process. It just cannot work without proper hydration. A healthy spine starts with adequate hydration.
The Benefits of Water for the Spine
From the time you get up in the morning, you are putting pressure on your spine and subsequently, the discs that lie between each vertebra. As you move the discs are compressed by the spine, and the water that is inside is squeezed out.
Even upright activities like standing, sitting, or walking can cause pressure on the discs as gravity causes compression in the spine. When the discs do not have enough water, it results in limited mobility, pain, and an increased risk of back injury.
If you don�t drink enough water, your body becomes dehydrated and is unable to replenish the water that the discs so desperately need. You may not even notice the typical signs of dehydration such as a headache and lethargy, but also lower levels of dehydration can cause severe problems in the body, especially if it is prolonged. Soda and similar beverages do not provide adequate water to the body.
How to Properly Hydrate the Body
Water is the best way to hydrate the body, but it isn�t the only way. Foods like watermelon, lettuce, spinach, and soups are excellent sources of hydration. H2O, of course, is the best way, but herbal teas are also good.
Drinks with caffeine are not as effective since the caffeine can have a diuretic effect. Traditionally, people have been told to drink eight glasses of water a day, and that is good advice. However, studies indicate that proper hydration can occur with an intake of just 30 to 50 ounces of water a day.
If you have constant or frequent back pain, the answer could be as close as your kitchen faucet. Dehydration could be the source of your back pain and immobility.
Water also affects the way the cerebrospinal fluid works and moves in the body. When the body is dehydrated, it doesn�t move as it should, and brain function, reflexes, and cognitive processing could be impacted. Don�t chance it. If your problems are caused by something as simple as not drinking enough water, that is something you can change today. Drink up! Your body will thank you.
Achondroplasia is a genetic disorder that leads to dwarfism. In those with the condition, the legs and arms are short, while the chest is generally of regular length. Those affected have an average adult height of 131 centimetres (4 ft 4 in) for males and 123 centimetres (4 feet ) for females. Other features include a prominent forehead and an enlarged head. Intelligence is typically considered normal in people with achondroplasia. The condition affects approximately 1 in 27,500 individuals.
Diagnosis for Achondroplasia
Achondroplasia is the result of a mutation in the fibroblast growth factor receptor 3 (FGFR3) gene. This occurs during early development as a new mutation. It is also inherited from the parents in an autosomal dominant way. Those with two affected genes do not survive. Testing if uncertain of diagnosis based on symptoms is often strongly encouraged.
Achondroplasia can be detected before birth�through the use of prenatal ultrasound. Moreover, a DNA test can also be performed to identify homozygosity, where two copies of the gene are inherited causing the deadly condition resulting in stillbirths. Clinical features include megalocephaly, short limbs, prominent forehead, thoracolumbar kyphosis and mid-face hypoplasia. Complications such as dental malocclusion, hydrocephalus and replicated otitis media may also develop. The risk of death in infancy may be increased as a result of the probability of compression of the spinal cord with or without upper airway obstruction.
Achondroplasia and Sciatica
Individuals with achondroplasia commonly experience back pain, which may often progress to sciatica symptoms, such as pain and discomfort, tingling and burning sensations in the lower extremities, and numbness, among other consequences. Both children and adults with achondroplasia have hip flexion contractures which have been found to be a contributing factor for sciatica and muscle fatigue reported by individuals with achondroplasia. Individuals with achondroplasia also typically demonstrate a mixed pattern of joint mobility, including joint contracture and joint hypermobility at characteristic joints.�
Achondroplasia Management
There is no known cure for achondroplasia even though the cause of the mutation has been found. Management for the condition might include support groups and growth hormone treatment. Efforts to treat or prevent complications like obesity, hydrocephalus, obstructive sleep apnea, middle ear infections, or spinal stenosis may be required for the management�of achondroplasia. Life expectancy of those affected is approximately 10 years less than ordinary.�The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Alternative treatment options, such as chiropractic care, can help ease back pain through spinal adjustments and manual manipulations, ultimately improving pain relief.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine