Ankylosing Spondylitis is a type of arthritis that typically begins during adolescence or in a person�s early twenties and occurs more often in men than in women. However, once experiences onset, they are affected for the rest of their lives. It is estimated that between 0.2% and 0.5% of individuals in the United States suffers from ankylosing spondylitis. �It can cause significant pain, discomfort, and immobility. While there is no cure for the condition, the symptoms can be treated, bringing some degree of comfort and mobility.
What is Ankylosing Spondylitis?
Ankylosing Spondylitis, or AS, is a type of arthritis that causes inflammation in the spine. While the vertebrae are primarily involved, it can also affect other joints as well, including the hips, shoulders, heels, ribs, and the small joints of the feet and hands.
In some cases, the heart, lungs, and even eyes can be involved. If left untreated, the condition can progress, causing chronic pain that can be severe as the spinal inflammation increases. More advanced cases can cause the spine to grow new bone formations so that it is immobile, or fixed, sometimes resulting in kyphosis, which is a bowed or forward-stooped posture.
What Causes Ankylosing Spondylitis?
While genetics is believed to be a key player in the development of Ankylosing Spondylitis, the exact cause has not yet been determined. The majority of people who have AS also carry a specific gene that has been linked to the condition.
This gene produces HLA-B27, a protein or genetic marker, that more than 95% of Caucasians with ankylosing spondylitis have. However, some people don�t have this protein who develop AS and many people do carry this marker yet never develop the condition.
Researchers theorize that there may be other genes that may be involved, as well as environmental factors that trigger the gene activation, such as a bacterial infection, causing people who are susceptible to AS to activate it. Scientists have identified more than 60 genes that are believed to be associated with AS with only about 30% that are linked to HLA-B27 regarding overall risk. Other genes that have been identified as key to AS include IL-23, IL-17, IL-12, and ERAP.
It is also believed that AS can be triggered when the intestinal defenses break down, allowing certain bacteria into the bloodstream. This can, in turn, cause an immune response.
How is Ankylosing Spondylitis Treated?
AS cannot be cured, but the symptoms can be treated to relieve stiffness and pain as well as delay or prevent spinal deformity and other complications. The damage that it does to the joints is irreversible, so it is best if treatment is started before that occurs. There are several ways that AS is treated:
Medication � Nonsteroidal anti-inflammatory drugs (NSAIDs) like indomethacin (Indocin) and naproxen (Naprosyn) are commonly used to treat the symptoms of AS. They can be useful in relieving pain, inflammation, and stiffness but may cause some side effects, including gastrointestinal bleeding. This makes long-term use impractical and even unsafe. If NSAIDs do not help, other medications may be prescribed, including:
Golimumab (Simponi; Simponi Aria)
Certolizumab pegol (Cimzia)
Adalimumab (Humira)
Etanercept (Enbrel)
Infliximab (Remicade)
Physical therapy – PT is often recommended to help with flexibility, strength, and pain relief. It can help with posture and prevent some of the more debilitating symptoms.
Surgery � Most people with AS do not require surgery, but it may be recommended if there is severe joint damage or pain. In some cases, it can cause significant damage to hip joints, and they will need to be replaced.
Chiropractic � Many patients with AS have with outstanding results with chiropractic treatment. It is non-invasive and does not have the unpleasant side effects that many medications have.
Chiropractic Treatment for Ankylosing Spondylitis
Chiropractors strongly recommend chiropractic treatment for the non-acute inflammatory stage of AS. Once the condition has progressed to acute joint disease, there is a very high risk of injury or damage to the connective tissue. Adjustments and exercise are used to relieve symptoms, but some of the traditional spinal manipulation treatments are not performed.
A chiropractor will also make recommendations to the patient regarding lifestyle changes that can help with symptoms, such as stopping smoking. Tobacco use can increase inflammation and damage connective tissue. They may also advise increasing their intake of omega three fatty acids in their diet. Regular chiropractic care can help patients manage symptoms and prevent disease progression, improving their quality of life.
Sciatica is a collection of symptoms in the low back, which radiate down one or both legs. Sciatica is generally caused by the compression or irritation of the sciatic nerve, the largest nerve in the human body. One of the most common health issues that cause sciatic nerve pain is called piriformis syndrome. The piriformis muscle stretches from the front of the sacrum, the triangle-shaped bone between the hipbones on the pelvis.
The piriformis muscle extends to the top of the femur around the sciatic nerve. The femur, as previously mentioned, is the large bone in the upper leg. The piriformis muscle functions by helping the thigh move from side to side. A piriformis muscle spasm, or any other type of injury and/or condition along the piriformis muscle, can place pressure on the sciatic nerve and cause pain and discomfort. The result is piriformis�syndrome.
Piriformis Syndrome Causes and Symptoms
Sciatic nerve pain,�or sciatica, is one of the most prevalent�symptoms of piriformis syndrome. The pain and discomfort, however, may be felt in another part of the body. This is known as referred pain. Other common symptoms of piriformis syndrome include tingling sensations and numbness; tenderness;�difficulty sitting along with�pain while sitting and pain in the buttocks and thighs with physical activities.
The piriformis muscle can easily become damaged or injured from periods of inactivity or an excessive amount of exercise. Some common causes of piriformis syndrome include overuse; repetitive movements involving the legs; sitting for lengthy periods of time; lifting heavy objects; and extensive stair climbing. Sports injuries or automobile accident injuries can also harm the piriformis muscle and cause it to compress the sciatic nerve.�
�
Piriformis Syndrome Diagnosis
A doctor appointment for diagnosis of piriformis syndrome may include a review of the patient’s health history, their symptoms, and other probable causes of their pain and discomfort. If you recall straining a muscle during physical activity, be sure to share that information with your doctor. The�doctor may also perform a physical exam. The patient will participate in a series of range of movements to determine the cause of symptoms.
Some imaging tests may also be essential to help rule out other causes of piriformis syndrome. A CT scan or an MRI scan may help the healthcare professional determine whether even a herniated disc or arthritis is causing the patient’s pain and discomfort. An ultrasound of the piriformis muscle may also be helpful in diagnosing the problem if it seems that piriformis syndrome is causing the patient’s overall symptoms.
�
Piriformis syndrome is a health issue associated with the compression or impingement of the sciatic nerve around the piriformis muscle. Symptoms may include pain and discomfort, tingling sensations and numbness along the low back, or sciatica. Chiropractic care is a well-known alternative treatment option which can help reduce the compression of the sciatic nerve and improve piriformis syndrome.
Dr. Alex Jimenez D.C., C.C.S.T.
Piriformis Syndrome Treatment
Piriformis syndrome may often not need any treatment to�relieve its symptoms. Just avoiding the physical activities which caused the pain and discomfort to manifest and rest can help improve the health issue. If symptoms do persist, however, alternating between ice and heat can help decrease pain. Apply ice for 15 to 20 minutes then use a heating pad on the affected area. Try that every couple of hours to help relieve symptoms.
Over-the-counter painkillers�may also help decrease pain and discomfort. The symptoms associated with piriformis syndrome can go away with no additional treatment, however, if it doesn’t, the patient might benefit from alternative treatment options, such as chiropractic care or physical therapy. Chiropractic care is a treatment approach which utilizes spinal adjustments and manual manipulations to treat a variety of injuries and/or conditions.
A chiropractor,�or doctor of chiropractic, may also provide piriformis syndrome relief through the use of transcutaneous electrical nerve stimulator, or TENS, treatment. A TENS device is a handheld unit which sends electrical charges directly to the affected region of the piriformis muscle. The nerves are then stimulated by the electric energy, which interferes with pain signals being transmitted to the brain.
The chiropractor or physical therapist may also recommend a series of lifestyle modifications, including physical activity guidance and nutritional advice. Various stretches and exercises can help improve the strength, flexibility, and mobility of the�piriformis muscle. In severe cases of piriformis syndrome, corticosteroid injections or even surgical interventions may be required to help alleviate the symptoms.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Chiropractic for Athletes with Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain is the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
The hips are some of the most flexible structures in the human body, providing the necessary amount of strength and stability needed to support the human body when walking, running or jumping. However, the hip joint can also be vulnerable to damage or injury, resulting in debilitating hip pain. Trochanteric bursitis is hip pain brought on by the inflammation of the fluid-filled sac, or bursa, found on the outer border of the hip.
Trochanteric Bursitis Overview
There are about 160 bursae located around the entire body. Bursae act as a sort of “cushion” between soft tissues and bones, preventing bones from rubbing against tendons, ligaments, and muscles. Trochanteric bursitis can affect any of the bursae inside the human body. Trochanteric bursitis affects the outer part of the thighbone, or the femur, at the edge of the hip. This bony point is best known as the greater trochanter.
Another bursa, called the iliopsoas bursa, can be found on the inside of the hip. Inflammation of the iliopsoas bursa also triggers pain in the groin. Bursitis is considered to be one of the top causes of hip pain. Repetitive physical activities, such as climbing stairs, or even surgical interventions to the hip may cause inflammation in the bursa. Many doctors commonly refer to trochanteric�bursitis as greater trochanteric pain syndrome.
Signs and Symptoms of Trochanteric Bursitis
The main characteristic of trochanteric bursitis involves pain in the outer area of the hip or pain when laying on the affected side of the hip. The painful signs and symptoms will also generally become worse through certain physical activities, such as walking or climbing stairs. Pain may also�radiate down the�thigh and into the feet, or it may disperse. Pain can be sharp and fade into an ache, accompanied by swelling in the legs.
Causes of Trochanteric Bursitis
Common causes of trochanteric bursitis include�slip-and-fall accidents, strong blows to the hip, or lying on one side of the body for an extended period of time. Sports injuries involving�overuse from repetitive physical activities like running, bicycling, or climbing stairs, a ripped tendon or even standing may cause trochanteric�bursitis. Health issues, such as�bone spurs in the hip or thighbone, may consequently cause trochanteric bursitis.�
A variety of conditions and disorders may also lead to trochanteric bursitis, including spine problems, such as scoliosis or arthritis of the lumbar spine, even rheumatoid arthritis, and gout as well as thyroid disease. Moreover, legs of two different lengths,�hip surgery or prosthetic implants can create problems in the hips. Trochanteric bursitis is most common in middle-aged or elderly people and it is most prevalent in women than men.
�
Trochanteric Bursitis Treatment and Chiropractic Care
Avoiding the physical activities which caused trochanteric bursitis will allow time for the body to heal. After seeing a healthcare professional for diagnosis, the doctor may often recommend nonsteroidal anti-inflammatory drugs, or NSAIDs to help control pain and inflammation. The recommended amount should be used to avoid side effects. Some doctors may also use steroid injections to control pain and inflammation.
Many healthcare professionals may also recommend alternative treatment options,�such as chiropractic care and physical therapy to help improve trochanteric bursitis signs and symptoms. A chiropractor may utilize spinal adjustments�and manual manipulations to reduce pressure from the spine while a physical therapist may teach the patient exercises to maintain strength. A cane or crutches can also take the weight off a patient’s hip.
If pain relievers or alternative treatment options, such as chiropractic care or physical therapy, do not work for the patient, the healthcare professional might recommend surgery to remove the bursa. This procedure can be accomplished through very small incisions with a camera. Other treatment approaches should be considered before following through with surgery.� The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
�
�
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain is the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Athletic pubalgia is a debilitating health issue which affects the groin. The injury commonly happens through sports that use sudden changes of direction or intense twisting motions. Also referred to as a sports hernia, athletic pubalgia is characterized as a tear or strain in any soft tissue (muscle, tendon, ligament) of the abdominal or lower abdomen region.
Physiology of Athletic Pubalgia
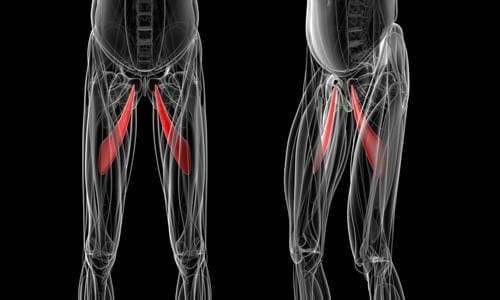
The soft tissues most often affected by athletic pubalgia are the oblique muscles found in the lower abdomen, especially in the tendons that attach the oblique muscles to the pubic bone. In many instances, the joints that connect the thigh muscles to the pubic bone,�known as the adductor muscles, are also stretched or torn as a result of athletic pubalgia.
Physical activities which involve planting the feet and twisting with maximum exertion can cause athletic pubalgia. A sports hernia is most prevalent in vigorous sports, such as hockey, soccer, wrestling, and football. Athletic pubalgia�causes pain and discomfort in the groin region which typically gets better with rest but comes back with physical activity.
A sports�hernia does not result in a visible bulge in the groin, such as the well-known inguinal hernia does. As time passes, athletic pubalgia can lead to an inguinal hernia, and abdominal organs can push against the diminished cells to form a visible bulge. Without treatment, this sports injury could lead to chronic, disabling pain and other symptoms.
Healthcare Professional Diagnosis
During the first consultation, a doctor will discuss the individual’s symptoms and how the injury happened. To�diagnose athletic pubalgia, the healthcare professional will look for tenderness in the groin or above the pubis. Although a sports hernia may be related to an inguinal hernia, the doctor may not find any hernias during a physical examination.
Furthermore, to help determine the presence of athletic pubalgia, the healthcare professional will probably ask the patient to perform a sit-up or to�bend the trunk against resistance. If you have a sports hernia, these tests will be painful. The doctor may also require�x-rays or magnetic resonance imaging (MRI) to help determine whether you have athletic pubalgia.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Athletic pubalgia, also known as a hockey hernia,�hockey groin, Gilmore’s Groin,�sports hernia, or groin disruption, is a health issue of the pubic joint. It is a condition characterized by chronic groin pain in athletes and identified by a dilated ring of the inguinal canal. Soccer and ice hockey players are the athletes most commonly affected by athletic pubalgia, and both recreational and professional athletes can be impacted.
Athletic Pubalgia Symptoms
Symptoms of athletic pubalgia�generally manifest as pain following physical activity, most frequently through hip extension, and twisting and turning movements. The painful symptoms usually radiate into the adductor muscle region and the testicles, although it is often difficult for the individual to pinpoint the exact location of the�symptoms. Athletes with athletic pubalgia�experience soreness and stiffness after physical activity.
Any exertion which increases intra-abdominal pressure, such as sneezing or�coughing, as well as physical activity, can lead to pain. While pain in the stomach and pelvis can occur due to a variety of health issues, including injuries to the low back, or lumbar spine, the hip joint, the sacroiliac joint, and the abdomen, along with the genito-urinary system, diagnosis of athletic pubalgia demands skillful differentiation and evaluation.
Clinical Presentation of Athletic Pubalgia
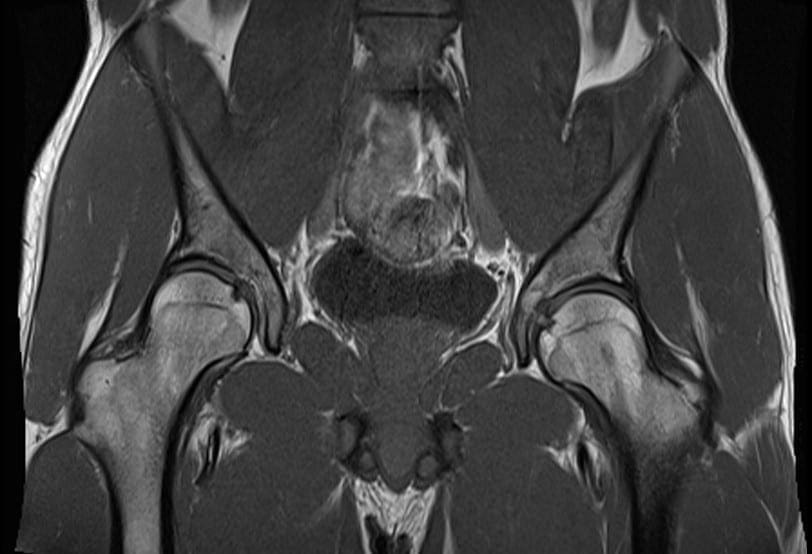
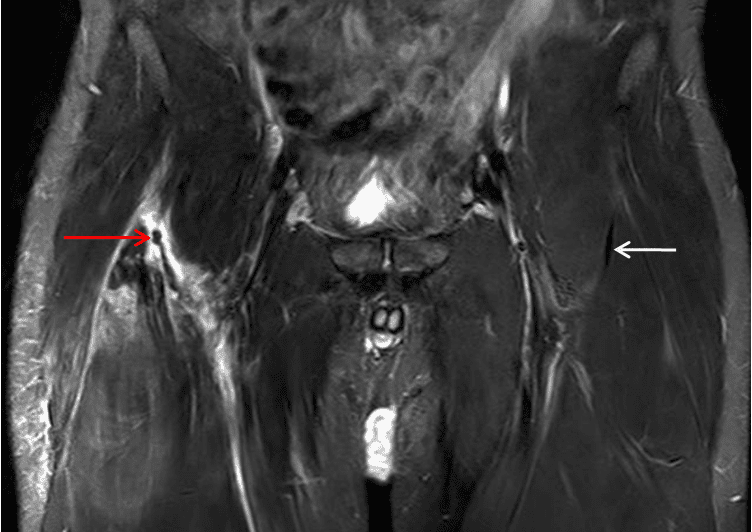
The diagnosis of athletic pubalgia is based on the patient’s history, where healthcare professionals may also depend on the use�of magnetic resonance imaging,�or MRI. Symptoms can frequently be reproduced by certain movements, such as performing crunches or sit-ups. Pain associated with athletic pubalgia may also be elicited with the patient in a “frog posture,” in which the individual is supine with knees bent and heels together.
Many athletes experience concomitant fatigue or tearing of the�adductor muscles or labral tears of the hip. If there is stiffness in the adductor muscles post-injury, painful symptoms can manifest. Alternative treatment options should be to restore normal movement after the adductor has begun to heal, normally 6 to 8 weeks post-injury. Moreover, sleeping in a prone position with the hip on the affected side flexed and externally rotated can offer relief to some athletes with athletic pubalgia.
The precise prevalence of this health issue is unknown. Conservative therapies,�such as gentle stretching, may temporarily alleviate painful symptoms, however, definitive treatment options should be considered for long-term relief.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
The rectus femoris muscle attaches to the pelvis and just below the knee as it is one of four muscles found at the front part of the thigh. It functions by extending the knee and flexing the hip. The rectus femoris muscle is made up of�fibers which adapt to quick action. Rectus femoris muscle strain is caused by forceful movements, such as kicking a ball or when beginning to sprint, and it is particularly vulnerable to stress and pressure.
Painful symptoms generally manifest at the top of the thigh after the rectus femoris muscle suffers a strain or tear. In severe cases, the health issue may even become noticeable if the tissue is completely ruptured. Fortunately, complete tears are rare. Healthcare professionals will commonly use an MRI scan to diagnose the extent of the sports injury. Proper diagnosis and treatment�are�essential. A rectus femoris muscle strain should not be rushed, as individuals who return-to-sport too soon may suffer re-injury.
Treatment for Rectus Femoris Strain
According to many healthcare professionals, when it comes to sports injuries to the rectus femoris muscle, it’s crucial to immediately apply the RICE principle (Rest, Ice, Compression, and Elevation) to the affected thigh. This treatment aims to decrease bleeding and inflammation to the muscle. Also, it will help reduce painful symptoms after the injury. Based on how much pain has been experienced, simple painkillers might be utilized, although it’s best to attempt to prevent the use of these.
Once movement is restored enough to allow the individual to walk using their regular range of motion, and once the swelling has gone down, then you will have recovered from the acute phase of the injury. It would then be an excellent time to engage in physical activity, without inflicting damage or stress to the quadriceps muscles. This can be performed on an exercise bicycle or through swimming, where the weight is kept�off the limb. Stretches and gentle resistance exercises are crucial, as this will help to align the scar tissue that has formed during the healing process.
Recovery must be monitored so that improvements can be noted and the treatment shifted to help the rehabilitation process. It is hard to measure the length of time to complete recovery. It can take from six to eight weeks or even longer, although some people will commonly recover within one to four weeks.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
The hip is commonly described as a “ball-and-socket” type joint. In a healthy hip, the ball at the top end of the thighbone, or femur, should fit firmly into the socket, which is part of the large pelvis bone. In babies and children with developmental dysplasia, or dislocation, of the hip, abbreviated as DDH, the hip joint may not have formed normally. As a result, the ball of the femur might easily dislocate and become loose from the socket.
Although DDH is often present from birth, it could also develop during a child’s first year of life. Recent research studies have demonstrated that infants whose thighs are swaddled closely with the hips and knees straight are at a higher risk for developing DDH. Because swaddling has become�increasingly popular, it is essential for parents to understand how to swaddle their babies safely, and they should realize that when done improperly, swaddling may cause health issues such as DDH.
Diagnosis for�Developmental Dysplasia of the Hip
In addition to visual cues, when�diagnosing for DDH, the healthcare professional will perform a careful evaluation, such as listening and feeling for “clunks” which indicates that the hip is placed in different positions. The doctor will also utilize other methods and techniques to determine if the hip is dislocated. Newborns recognized to be at higher risk for DDH are often tested using ultrasound. For babies and children, x-rays of the hip might be taken to provide further detailed images of the hip joint.
Treatment for�Developmental Dysplasia of the Hip
If DDH is discovered at birth, it can usually be treated with the use of a harness or brace. If the hip isn’t dislocated at birth, the condition might not be diagnosed until the child starts walking. At that point, treatment for DDH is much more complex, with less predictable results. If diagnosed and treated accordingly, children ought to have no restriction in function and develop the standard hip joint. DDH may result in atherosclerosis and other problems. It may produce a difference in agility or leg length.
In spite of proper treatment, hip deformity and osteoarthritis may develop later in life. This is particularly true when treatment starts after the age of 2 years. Therefore, diagnosis and treatment are essential in newborns and children with DDH. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
�
�
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine