Best Foods and Hydration Tips to Heal Spinal Disc Herniations Naturally
A chiropractor gives a thumbs-up to promote spine health.
Spinal disc herniations happen when the soft center of a disc pushes out through a crack in the tough outer layer. This can press on nerves, causing pain, numbness, or weakness. Good news: the right foods and plenty of water can help the body heal tissue, cut swelling, and keep the spine strong. Protein builds new tissue. Omega-3 fatty acids calm swelling. Vitamins and minerals protect cells and support bones. Water keeps discs plump and flexible. Adding these to daily meals, along with gentle care like chiropractic adjustments, can ease pressure on discs, improve nerve signals, and speed recovery without surgery.
Why Nutrition Matters for Disc Herniations
Discs act as cushions between the vertebrae. They are mostly water and collagen, a type of protein. When a disc herniates, the body needs extra building blocks to fix the damage. Poor nutrition can slow healing and worsen swelling. A diet rich in healthy nutrients does the opposite—it speeds repair and reduces pain (The Pain Relief Doctor, n.d.).
Protein is the star for repair. It produces collagen, which holds discs together. Without enough, cracks stay open longer. Studies show people who eat more protein heal connective tissue faster (Frisco Spine, n.d.). Omega-3 fatty acids fight swelling around the herniated area. Less swelling means less nerve pain. Vitamins like C and D help make collagen and keep bones dense. Minerals such as magnesium relax tight muscles that pull on the spine.
Dr. Alexander Jimenez, a chiropractor and nurse practitioner, sees this in his clinic every day. Patients who add anti-inflammatory foods notice less back stiffness in weeks. He tells them, “Feed the spine like you feed a muscle after a workout” (Jimenez, n.d.; Jimenez, LinkedIn profile).
Top Foods Rich in Protein for Tissue Repair
Lean meats, fish, eggs, and plant sources provide the body with amino acids to rebuild collagen. Chicken breast, turkey, salmon, and tuna top the list. A 4-ounce piece of salmon has about 25 grams of protein plus omega-3s. Eggs supply complete protein and vitamin D for bone support. For plant eaters, lentils, chickpeas, Greek yogurt, and quinoa are excellent options. One cup of cooked lentils offers 18 grams of protein and fiber to keep weight down—extra pounds stress discs (Bonati Spine Institute, n.d.; Texas Back Institute, n.d.).
Dr. Jimenez advises patients to aim for 20–30 grams of protein at each meal. In his El Paso clinic, people who follow this plan report stronger cores and fewer flare-ups. He pairs food advice with light core exercises to lock in the gains.
Omega-3 Fatty Acids to Lower Inflammation
Swelling makes herniated discs hurt more. Omega-3s act like natural pain relievers. Fatty fish—salmon, mackerel, sardines, and anchovies—lead the pack. Two servings a week can drop inflammation markers by 20% (Healthline, 2023). Plant sources include chia seeds, flaxseeds, and walnuts. A handful of walnuts delivers 2.5 grams of omega-3s plus magnesium.
Clinical notes from Dr. Jimenez indicate that patients who switch from red meat to salmon experience relief within 10–14 days. He often hands out a simple meal card: grilled salmon, steamed broccoli, and brown rice. The combination promotes healing and simultaneously soothes nerves.
Berries and Leafy Greens for Vitamins and Antioxidants
Bright berries and dark greens fight cell damage. Blueberries, strawberries, and raspberries pack vitamin C and antioxidants. Vitamin C is key for collagen cross-links that make discs tough. One cup of strawberries gives 98 mg of vitamin C—more than an orange (Spine Orthopedic Center, n.d.). Spinach, kale, and Swiss chard provide vitamins A and K, as well as folate. They also carry potassium to balance fluids inside discs.
Antioxidants in berries mop up free radicals that weaken tissue. People who eat 2 cups of mixed berries daily show lower oxidative stress on blood tests (Illinois Back Institute, n.d.). Dr. Jimenez tells patients to toss berries into oatmeal or blend spinach into smoothies. The habit builds spine armor over the course of months.
Nuts and Seeds for Magnesium and Healthy Fats
Almonds, walnuts, pumpkin seeds, and chia seeds bring magnesium, zinc, and beneficial fats. Magnesium relaxes back muscles and stops spasms that pinch herniated discs. One ounce of almonds has 80 mg of magnesium—20% of the daily goal. Seeds add fiber to help control weight and stabilize blood sugar, both of which are helpful for spine loads (417 Spine, n.d.; Spine Health, n.d.).
Dr. Jimenez keeps pumpkin seeds in his office for quick snacks. Patients who grab a handful between adjustments say cramps fade faster. He warns against salted versions; plain or lightly roasted keep sodium low to avoid water retention.
The Power of Hydration for Disc Health
Discs are 70–80% water. Dehydration shrinks them, making herniations worse. Drinking eight to ten glasses of plain water daily keeps the jelly-like center plump. It also flushes toxins that cause swelling. Caffeine and alcohol pull water out, so balance them with extra glasses (Anssi Wellness, n.d.).
Dr. Jimenez starts every visit by asking about water intake. He finds that patients who carry a 32-ounce bottle and sip throughout the day cut morning stiffness in half. A simple trick: add lemon or cucumber for taste without sugar.
Sample Daily Meal Plan
Breakfast: Greek yogurt with blueberries, chia seeds, and a boiled egg.
Lunch: Grilled chicken salad with spinach, strawberries, walnuts, and olive oil dressing.
Snack: Apple slices with almond butter.
Dinner: Baked salmon, quinoa, steamed broccoli.
Drinks: 80–100 ounces of water, and herbal tea is okay.
This plan hits 80–100 grams of protein, 2 grams of omega-3s, and plenty of vitamins in under 2,000 calories.
Integrative Care Beyond the Plate
Chiropractic adjustments take pressure off herniated discs. When combined with nutrition, results add up. Gentle spinal decompression opens space for discs to rehydrate. Soft tissue work relaxes tight muscles. Dr. Jimenez uses both in his protocols. Patients who pair weekly adjustments with the meal plan above return to light activity in 4–6 weeks (Park Slope Chiropractor, n.d.).
Other non-invasive helpers include walking 20 minutes daily, yoga for core strength, and magnesium oil rubs at night. Sleep on a medium-firm mattress to keep the spine neutral.
Foods to Limit
Cut processed snacks, sugary drinks, and trans fats. They spike swelling and weight. Fried foods and excess salt pull water from discs. One study linked high-sugar diets to faster disc wear (Elite Spine FL, n.d.).
Putting It All Together
Start small: add one protein source, one colorful fruit or veggie, and one extra glass of water today. Track pain in a notebook. Most people notice less ache in 7–10 days. Work with a chiropractor or doctor to tweak the plan. Dr. Jimenez says, “Consistency beats perfection. Feed the spine daily, and it rewards you with movement.”
Healing a herniated disc takes teamwork between smart eating, hydration, and gentle care. The body has built-in repair tools—give it the right fuel, and recovery follows.
Your Spine, Your Life: An El Paso-Ready Guide to Strong, Flexible, Pain-Resistant Backs
A young woman is performing a spine checkup at a vertebra clinic.
What “spinal health” means (and why it matters here in El Paso)
Spinal health refers to the proper structure, alignment, and function of the spine, enabling it to support the body, facilitate movement, and protect the spinal cord—the pathway for nerve signals between the brain and the body. Good spinal health comes from regular exercise, posture awareness, a nutrient-dense diet, steady hydration, and a healthy weight. Poor spinal health can lead to chronic pain, nerve irritation or damage, and a lower quality of life (Raleigh Orthopaedics, 2024; Orthopedic Specialists of Southwest Florida [OSSWF], 2024; National Spine Health Foundation, 2024).
How a healthy spine supports your whole body
Support & alignment: Your spine acts like a central pillar that shares load with the hips and legs and keeps you upright (Premier Spine & Sports Medicine, n.d.).
Movement & shock absorption: Curves, discs, and joints allow for safe bending and twisting, enabling you to lift, reach, and play (Raleigh Orthopaedics, 2024).
Nerve protection: The spinal column shields the spinal cord and nerve roots, so signals move clearly. Irritation can cause pain, tingling, or weakness (Cary Orthopaedics, 2023).
Quality of life: Ongoing spine issues can lead to fatigue, poor sleep, headaches, and reduced participation in work or sports (Raleigh Orthopaedics, 2024).
Common problems we see—and why early action helps
Strains/sprains and facet irritation from long sitting, poor lifting form, or sudden loads
Disc problems that can press on nearby nerves and create radiating symptoms
Spinal stenosis (narrowing) that pinches nerves
Degenerative changes related to age, low activity, smoking, or extra weight
Most cases respond to conservative care when initiated early, including movement, postural changes, targeted exercises, and load management (OSSWF, 2024).
Red flags—don’t wait: radiating pain, numbness, weakness, headaches, or loss of function. Seek a prompt exam (Cary Orthopaedics, 2023; Suarez Physical Therapy, n.d.).
An El Paso Back Clinic–style plan: simple steps that fit your day
1) Movement you can keep
20–30 minutes of low-impact cardio most days (e.g., walking, cycling, swimming).
Core & hip strength 2–3 days/week: planks, side planks, glute bridges, and bird-dogs.
Mobility after warm-ups: thoracic open-books, hip-flexor, and hamstring stretches (National Spine Health Foundation, 2024; Mobility Project PT, 2024).
2) Posture that holds up at work and home
Sit: feet flat, hips back in the chair, lumbar support, screen at eye level.
Stand: weight balanced, knees soft, ears over shoulders.
Micro-breaks: move every 30–45 minutes (National Spine Health Foundation, 2024).
3) Ergonomics you actually feel
The chair is high enough so the hips are level with or slightly above the knees.
Keyboard and mouse close; forearms supported; shoulders relaxed.
Lift with a hip hinge, keep the load close, and exhale as you stand.
4) Sleep & stress recovery
Neutral neck/back with a supportive mattress and the right pillow height.
Side sleepers: pillow between knees. Back sleepers: pillow under knees.
Use breathing drills, short walks, and stretch breaks to lower tension (Raleigh Orthopaedics, 2024).
5) Hydration & healthy weight
Steady water intake supports disc hydration and tissue recovery (Centeno-Schultz Clinic, n.d.).
A healthy body weight lowers compressive load on joints and discs (Raleigh Orthopaedics, 2024).
Nutrition for a stronger spine (simple and local-friendly)
Protein for muscle and connective-tissue repair
Omega-3s (salmon, trout, walnuts) to help regulate inflammation
Calcium & vitamin D for bone strength
Magnesium for nerve and muscle function
Colorful fruits/vegetables for antioxidants that support recovery
Water for disc hydration and nutrient transport These habits reduce inflammation and support healing (Watkins Family Chiropractic, 2023; OSSWF, 2024).
Four-week “Borderland Back Reset” (minimal gear, steady progress)
Week 1 — Start easy
Daily: 10-minute walk + 5 minutes mobility (open-books, hip-flexor, hamstrings).
Core set (3x/week): plank 20 s, side plank 15 s/side, glute bridge 10 reps.
Posture: Raise the screen and add a small lumbar roll.
Week 2 — Build consistency
Daily: 15–20 minutes walk/cycle + mobility.
Core set (3x/week): plank 25–30 s, side plank 20 s/side, bridge 12 reps; add bird-dog 6/side.
Nutrition: add one serving of leafy greens and one serving of lean protein to each meal (Watkins Family Chiropractic, 2023).
Week 3 — Strength + recovery
Cardio most days: 20–25 minutes.
Light hinge pattern (backpack or kettlebell) 1–2 days/week; focus on form.
Before bed, do slow breathing for 5 minutes.
Week 4 — Re-test & adjust
Compare flexibility, pain, and energy levels with those of Week 1.
Keep what helps; trim what doesn’t.
If numbness, weakness, or radiating pain persists, book an exam (Cary Orthopaedics, 2023; Suarez Physical Therapy, n.d.).
Real-world injuries: work, sports, and motor-vehicle accidents (MVAs)
Work: Desk roles need posture breaks and lumbar support; physical jobs need task rotation, hip-hinge training, and planned recovery.
Sports: Combine mobility, core/hip strength, and gradual return to play.
MVAs: Even “minor” collisions can cause whiplash or soft-tissue injury. A stepwise evaluation, along with imaging when necessary, guides safe return and documentation (OSSWF, 2024).
Inside our integrative approach in El Paso
(Clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC, Nurse Practitioner and Chiropractor)
Dual-scope diagnosis: We blend chiropractic and medical perspectives. Your exam includes a detailed history, movement, and neurological screens, as well as, when necessary, advanced imaging to clarify the problem and rule out potential red flags (Jimenez, n.d.; see Imaging/Diagnostics and Personal-Injury topics).
Evidence-based conservative care:
Chiropractic adjustments to restore motion and reduce joint irritation
Therapeutic exercise to build core/hip strength and mobility
Manual therapy/massage for tight or sensitive tissues
Acupuncture as part of an integrative plan when appropriate
Lifestyle coaching on posture, lifting, sleep, and stress (Prestige Health & Wellness, n.d.; Mobility Project PT, 2024; Raleigh Orthopaedics, 2024)
Documentation & advocacy: For work, sports, personal, and MVA cases, we document the mechanism of injury, exam findings, functional limits, and response to care. When claims or legal issues arise, clear records and appropriate imaging support decision-making (Jimenez, n.d.; Rangeline Chiropractic, n.d.).
Myths vs. facts (short and clear)
Myth: “If my back hurts, I should rest all day.” Fact: Gentle movement and short walks often speed recovery; long bed rest adds stiffness (National Spine Health Foundation, 2024).
Myth: “Only heavy lifting causes back pain.” Fact: Prolonged sitting, poor ergonomics, stress, and sleep problems also drive pain (National Spine Health Foundation, 2024; Raleigh Orthopaedics, 2024).
The El Paso Back Clinic checklist
☐ Break up sitting every 30–45 minutes
☐ Screen at eye level; use lumbar support
☐ 10–15 minutes daily core + mobility
☐ 20–30 minutes low-impact cardio most days
☐ Hydrate across the day
☐ Build meals around protein + produce + healthy fats
☐ Sleep with neutral neck/back alignment
☐ Seek care quickly for red flags or lasting symptoms
Uncover important information on sciatica correlated with a herniated disc resulting from an auto accident and how to manage your symptoms.
Managing Sciatica Pain from Herniated Discs After Auto Accidents: A Comprehensive Guide to Chiropractic and Holistic Care
Sciatica pain resulting from herniated discs, particularly following an auto accident, can profoundly impact daily life, causing discomfort and limiting mobility. This condition, marked by radiating pain, numbness, or weakness along the sciatic nerve, is a frequent consequence of spinal injuries sustained in motor vehicle accidents (MVAs). Nonsurgical treatments such as chiropractic care, targeted exercises, massage therapy, acupuncture, and integrative medicine offer effective solutions to alleviate pain, promote healing, and prevent long-term complications. Drawing on clinical expertise and supported by peer-reviewed research, this comprehensive guide explores the causes, risk factors, and treatment options for sciatica associated with herniated discs. It emphasizes the role of patient-centered care, clear communication, and holistic approaches in supporting the body’s natural recovery processes.
Understanding Herniated Discs and Sciatica
What Is a Herniated Disc?
The spine is a complex structure composed of vertebrae, muscles, ligaments, and intervertebral discs that act as cushions between the vertebrae. Each disc consists of a tough outer layer, the annulus fibrosus, and a gel-like inner core, the nucleus pulposus (Nedresky et al., 2025). A herniated disc occurs when the nucleus pulposus protrudes through a tear in the annulus fibrosus, often due to trauma such as an MVA. This protrusion can compress nearby nerves, leading to pain, numbness, or weakness in the back, legs, or arms, depending on the herniation’s location (Stretanski et al., 2025).
MVAs are a leading cause of spinal injuries, contributing to over 40% of spinal complications annually (El Paso Back Clinic, 2016). The sudden, high-impact forces from a collision can strain or rupture the spinal discs, resulting in herniation and nerve irritation.
What Is Sciatica?
Sciatica is not a standalone condition but a set of symptoms caused by irritation or compression of the sciatic nerve, the body’s largest nerve, formed by nerve roots from L4 to S3 (Davis et al., 2025). It is characterized by radiating pain that travels from the lower back through the buttocks and down one or both legs, often accompanied by numbness, tingling, or weakness in the affected areas. Symptoms can range from mild to severe and are often exacerbated by movements such as bending, twisting, or coughing.
A common cause of sciatica is a herniated disc in the lumbar spine, particularly at the L4-L5 or L5-S1 levels, where the disc material compresses the sciatic nerve roots (Blamoutier, 2019). MVAs can trigger this condition by causing acute trauma to the spine, leading to disc herniation and subsequent nerve irritation.
Causes of Herniated Discs and Sciatica in Motor Vehicle Accidents
How MVAs Lead to Herniated Discs
The spine is designed to support the body’s weight and facilitate movement, but it is not built to withstand the intense forces of an MVA. The sudden jolt from a collision can cause various injuries to the spine, including:
Whiplash: The rapid back-and-forth motion of the neck and upper spine during a crash can strain the cervical and thoracic discs, potentially leading to herniation.
Direct Trauma: The force of impact can rupture the annulus fibrosus, allowing the nucleus pulposus to protrude and compress nearby nerves.
Facet Joint Damage: The facet joints, which connect the vertebrae, can be injured, contributing to spinal instability and increasing the risk of disc herniation (El Paso Back Clinic, 2016).
These injuries disrupt the spine’s structural integrity, making herniated discs a common outcome of MVAs, particularly in rear-end or high-speed collisions.
Factors Contributing to Herniated Discs and Sciatica
Several factors increase the likelihood of developing herniated discs and sciatica following an MVA:
Age: As individuals age, intervertebral discs lose water content, becoming less flexible and more prone to rupture. This risk increases significantly after age 30, as disc degeneration accelerates (Nosikova et al., 2012).
Obesity: Excess body weight places additional stress on the spine, increasing the risk of disc herniation, particularly in women with higher body mass indices (Sonntag, 2010).
Sedentary Lifestyle: Weak core and back muscles from lack of physical activity reduce spinal support, making discs more susceptible to injury during trauma.
Poor Posture: Chronic poor posture, such as slouching while driving, can exacerbate spinal stress during an accident.
Pre-existing Spinal Conditions: Conditions like degenerative disc disease or scoliosis heighten the risk of herniation following trauma (Hincapié et al., 2025).
Accident Severity: The intensity of the collision, including speed and angle, directly correlates with the likelihood and severity of spinal injuries.
Overlapping Risk Profiles of Herniated Discs and Sciatica
Herniated discs and sciatica share interconnected risk profiles due to their closely related pathophysiology. A herniated disc can directly cause sciatica by compressing the sciatic nerve roots, but additional factors amplify the risks and complications for both conditions:
Inflammatory Response: When a disc herniates, the nucleus pulposus releases proinflammatory cytokines, such as interleukin-1, interleukin-6, interleukin-8, and tumor necrosis factor-alpha, which irritate the surrounding nerves and exacerbate sciatica symptoms (Cosamalón-Gan et al., 2021). This inflammation can prolong pain and delay recovery.
Autoimmune Reaction: The nucleus pulposus is immunologically privileged, meaning it is typically shielded from the immune system. When exposed due to a herniation, it can trigger an autoimmune response, further increasing inflammation and nerve irritation (Cosamalón-Gan et al., 2021).
Neurological Complications: Severe disc herniation can lead to serious conditions like cauda equina syndrome, characterized by bowel or bladder dysfunction, requiring immediate surgical intervention (Tang et al., 2019).
Motor Dysfunction: Compression of the sciatic nerve or its roots can cause weakness in the hamstrings, calf muscles, or foot muscles, impairing mobility and increasing the risk of falls (Davis et al., 2025).
Chronic Pain Development: Untreated sciatica or herniated discs can contribute to chronic pain syndromes, such as fibromyalgia, due to prolonged nerve irritation and central sensitization (El Paso Back Clinic, 2016).
These overlapping risks underscore the need for early intervention to address both the mechanical and inflammatory components of sciatica and herniated discs, preventing long-term complications.
Clinical Rationale for Chiropractic Care in Managing Sciatica
Chiropractic care is a cornerstone of nonsurgical treatment for sciatica caused by herniated discs, offering a safe, effective, and evidence-based approach to pain relief and functional restoration. Experts in musculoskeletal health emphasize the importance of personalized, patient-centered care to address the root causes of sciatica and promote long-term healing. Below is the clinical rationale for why chiropractic care is effective for sciatica associated with herniated discs:
1. Restoring Spinal Alignment and Reducing Nerve Compression
Chiropractic adjustments, or spinal manipulations, aim to realign the spine, reducing pressure on compressed nerve roots. By correcting vertebral subluxations (misalignments), chiropractors alleviate nerve irritation and improve spinal mobility. For sciatica caused by herniated discs, techniques such as the flexion-distraction technique utilize specialized tables to gently stretch the spine, thereby moving the disc material away from the nerve root and reducing inflammation and pain (El Paso Back Clinic, 2016).
Clinical Evidence: A randomized controlled trial demonstrated that nonsurgical spinal decompression therapy, similar to flexion-distraction, significantly reduced leg pain and disability in patients with subacute lumbar disc herniation, with a 26.9% reduction in herniation volume compared to controls (Choi et al., 2022).
2. Mitigating Inflammation
The inflammatory response triggered by a herniated disc is a major contributor to sciatica pain. Chiropractic adjustments improve blood flow and stimulate the release of anti-inflammatory mediators, helping to reduce inflammation around the affected nerve. Manual therapies also disrupt the cycle of inflammation caused by proinflammatory cytokines (Cosamalón-Gan et al., 2021).
Expert Insight: Chiropractic care addresses both the mechanical and chemical aspects of sciatica, supporting the body’s natural anti-inflammatory processes to alleviate pain and promote healing.
3. Enhancing Spinal Mobility and Function
Herniated discs and sciatica often restrict spinal mobility, exacerbating pain and dysfunction. Chiropractic adjustments restore range of motion by mobilizing stiff joints and relaxing tense muscles, which is particularly beneficial after an MVA, where muscle spasms and joint stiffness can worsen symptoms.
Clinical Evidence: A systematic review found that spinal manipulative therapy significantly reduced pain and improved function in patients with low back pain and radiculopathy, supporting its use in sciatica management (Alrwaily et al., 2018).
4. Drug-Free Pain Management
Chiropractic care provides a non-pharmacological approach to pain relief, avoiding the risks associated with long-term medication use, such as opioid dependency or gastrointestinal side effects from nonsteroidal anti-inflammatory drugs (NSAIDs). By targeting the underlying cause of sciatica, chiropractic care offers sustainable pain relief.
Expert Approach: Chiropractic care combines spinal adjustments with patient education to empower individuals to manage their pain through lifestyle modifications, thereby reducing their reliance on medications.
5. Preventing Chronic Conditions
Untreated sciatica or herniated discs can lead to chronic pain, neurological deficits, or permanent nerve damage. Chiropractic care focuses on early intervention to prevent these complications by addressing the root cause and promoting natural healing processes.
Clinical Evidence: A meta-analysis revealed that discectomy offers short-term relief for sciatica but yields negligible long-term benefits compared to nonsurgical treatments, such as chiropractic care, which can be equally effective with fewer risks (Liu et al., 2023).
Holistic Approaches to Managing Sciatica Pain
In addition to chiropractic care, holistic approaches enhance recovery, reduce pain, and support the body’s natural healing processes. These methods address physical, emotional, and lifestyle factors to provide comprehensive care for sciatica and herniated discs.
1. Targeted Exercises and Physical Therapy
Therapeutic exercises strengthen the muscles supporting the spine, improve flexibility, and reduce pressure on the sciatic nerve. Programs combining strength training, agility exercises, and biomechanical assessments create personalized rehabilitation plans that optimize recovery (El Paso Back Clinic, 2016).
Recommended Exercises:
Piriformis Stretch: Targets the piriformis muscle, which can compress the sciatic nerve when tight (Hicks et al., 2023).
Cat-Cow Stretch: Enhances spinal flexibility and reduces lower back stiffness.
Core Strengthening: Exercises such as planks and bridges strengthen the abdominal and back muscles, providing better spinal support.
Hamstring Stretches: Reduces tension in the posterior chain, alleviating sciatic nerve irritation.
Clinical Evidence: A systematic review confirmed that targeted exercises and physical therapy significantly reduced pain and disability in patients with lumbar radiculopathy (Vanti et al., 2021).
2. Massage Therapy
Massage therapy relieves muscle tension, improves circulation, and reduces inflammation, all of which contribute to sciatica pain relief. Techniques like deep tissue massage and myofascial release target tight muscles and fascia that may compress the sciatic nerve (El Paso Back Clinic, n.d.).
Expert Insight: Massage therapy complements chiropractic adjustments by enhancing muscle relaxation and the effectiveness of spinal manipulations.
3. Acupuncture
Acupuncture involves inserting thin needles into specific points on the body to stimulate healing and reduce pain. It modulates pain signals and reduces inflammation, making it an effective adjunctive therapy for sciatica.
Clinical Evidence: A network meta-analysis found that acupuncture provided significant pain relief for lumbar disc herniation, comparable to other nonsurgical treatments (Huang et al., 2019).
4. Integrative Medicine
Integrative medicine combines conventional and alternative therapies to address the root causes of sciatica and promote overall wellness. Key components include:
Nutrition: An anti-inflammatory diet rich in omega-3 fatty acids, antioxidants, and whole foods can reduce systemic inflammation and support disc healing (Cosamalón-Gan et al., 2021).
Stress Management: Techniques such as mindfulness meditation and yoga help reduce muscle tension and improve pain tolerance, addressing the emotional aspects of chronic pain.
Weight Management: Maintaining a healthy weight helps reduce spinal stress, thereby lowering the risk of recurrent disc herniation.
Expert Approach: Integrative care combines chiropractic adjustments with nutritional counseling and stress reduction techniques to create a comprehensive treatment plan.
5. Postural Correction and Ergonomics
Poor posture and improper ergonomics can exacerbate sciatica symptoms, particularly after an MVA. Educating patients on proper posture and ergonomic adjustments reduces spinal stress (El Paso Back Clinic, 2016).
Practical Tips:
Use a chair with lumbar support to maintain the spine’s natural curve.
Take breaks every 30 minutes to stand and stretch, avoiding prolonged sitting.
Sleep on a medium-firm mattress with a pillow under the knees to reduce lower back strain.
Feeling Better Than Ever After a Semi-Truck Accident- Video Testimonial
The Importance of Clear Communication in Treatment Success
Clear communication between healthcare providers and patients is critical for successful outcomes in managing sciatica and herniated discs. Patient education empowers individuals to take an active role in their recovery (El Paso Back Clinic, n.d.).
Key Communication Strategies
Explaining the Diagnosis: Patients should understand that sciatica is a symptom of an underlying issue, such as a herniated disc, and that treatment targets the root cause.
Setting Realistic Expectations: Chiropractic care and holistic treatments require time and consistency. Patients should be informed about the expected timeline for pain relief and functional improvement.
Encouraging Active Participation: Patients who engage in prescribed exercises and lifestyle changes tend to have better outcomes.
Addressing Concerns: Open dialogue about risks, benefits, and alternative treatments builds trust and ensures patients feel confident in their care.
Clinical Evidence: Studies show that patient-centered communication improves adherence to treatment plans and enhances outcomes in musculoskeletal conditions (Alrwaily et al., 2018).
Preventing Long-Term Complications
Untreated sciatica or herniated discs can lead to chronic pain, neurological deficits, or permanent disability. Nonsurgical treatments like chiropractic care, targeted exercises, and holistic therapies help prevent these complications by:
Reducing Nerve Compression: Early intervention prevents prolonged nerve irritation, which could lead to permanent damage.
Promoting Tissue Healing: Therapies like spinal decompression and acupuncture enhance blood flow and nutrient delivery to the injured disc (Choi et al., 2022).
Strengthening Supporting Structures: Exercises strengthen muscles and ligaments around the spine, reducing the risk of recurrent injuries.
Addressing Inflammation: Integrative approaches, such as anti-inflammatory diets and acupuncture, help manage the inflammatory response, thereby preventing chronic pain syndromes (Cosamalón-Gan et al., 2021).
Expert Insight: Proactive, nonsurgical interventions are crucial in preventing long-term complications, allowing patients to return to normal activities more quickly and with greater resilience.
Case Study: A Patient’s Journey to Recovery
A patient involved in an MVA experienced sciatica symptoms due to a herniated disc. Initially struggling with pain and limited mobility, they underwent a comprehensive treatment plan including chiropractic adjustments, targeted exercises, and nutritional guidance. This integrative approach, combining spinal decompression, core strengthening, and an anti-inflammatory diet, resulted in significant pain relief and restored function, demonstrating the effectiveness of nonsurgical, patient-centered care (El Paso Back Clinic, 2016).
Conclusion
Sciatica pain caused by herniated discs from MVAs is a complex condition driven by mechanical, inflammatory, and neurological factors. Chiropractic care offers a clinically supported, nonsurgical solution to alleviate pain, restore function, and prevent long-term complications. By integrating targeted exercises, massage therapy, acupuncture, and holistic approaches like nutrition and stress management, patients can achieve lasting relief and support their body’s natural healing processes. Clear communication and patient education are crucial for ensuring adherence and achieving optimal outcomes. For those experiencing sciatica after an MVA, seeking nonsurgical care from qualified professionals can be a critical step toward recovery and improved quality of life.
References
Alrwaily, M., Almutiri, M., & Schneider, M. (2018). Assessment of variability in traction interventions for patients with low back pain: A systematic review. Chiropractic & Manual Therapies, 26(35). https://pubmed.ncbi.nlm.nih.gov/30237870/
Blamoutier, A. (2019). Nerve root compression by lumbar disc herniation: A French discovery? Orthopaedics & Traumatology: Surgery & Research, 105(2), 335–338. https://pubmed.ncbi.nlm.nih.gov/30799172/
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P.-B. (2022). Effect of nonsurgical spinal decompression on intensity of pain and herniated disc volume in subacute lumbar herniated disc. International Journal of Clinical Practice, 2022, 6343837. https://pubmed.ncbi.nlm.nih.gov/36263240/
Cosamalón-Gan, I., Cosamalón-Gan, T., Mattos-Piaggio, G., Villar-Suárez, V., García-Cosamalón, J., & Vega-Álvarez, J. A. (2021). Inflammation in the intervertebral disc herniation. Neurocirugia (English Edition), 32(1), 21–35. https://pubmed.ncbi.nlm.nih.gov/32169419/
Hincapié, C. A., Kroismayr, D., Hofstetter, L., Kurmann, A., Cancelliere, C., Raja Rampersaud, Y., Boyle, E., Tomlinson, G. A., Jadad, A. R., Hartvigsen, J., Côté, P., & Cassidy, J. D. (2025). Incidence of and risk factors for lumbar disc herniation with radiculopathy in adults: A systematic review. European Spine Journal, 34(1), 263–294. https://pubmed.ncbi.nlm.nih.gov/39453541/
Huang, R., Meng, Z., Cao, Y., Yu, J., Wang, S., Luo, C., Yu, L., Xu, Y., Sun, Y., & Jiang, L. (2019). Nonsurgical medical treatment in the management of pain due to lumbar disc prolapse: A network meta-analysis. Seminars in Arthritis and Rheumatism, 49(2), 303–313. https://pubmed.ncbi.nlm.nih.gov/30940466/
Liu, C., Ferreira, G. E., Abdel Shaheed, C., Chen, Q., Harris, I. A., Bailey, C. S., Peul, W. C., Koes, B., & Lin, C.-W. C. (2023). Surgical versus non-surgical treatment for sciatica: Systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://pubmed.ncbi.nlm.nih.gov/37076169/
Nosikova, Y. S., Santerre, J. P., Grynpas, M., Gibson, G., & Kandel, R. A. (2012). Characterization of the annulus fibrosus-vertebral body interface: Identification of new structural features. Journal of Anatomy, 221(6), 577–589. https://pubmed.ncbi.nlm.nih.gov/22747710/
Understanding Nerve Conditions of the Spine: Causes, Symptoms, and Treatments
The spine is a critical part of the body, serving as a highway for nerves that transmit signals between the brain and the rest of the body. When something goes wrong with these nerves—whether they’re compressed, irritated, or damaged—it can lead to a range of uncomfortable symptoms like pain, numbness, tingling, or weakness. These issues, known as nerve-related spine conditions, can affect the back, arms, or legs and stem from various causes, including injuries, degenerative conditions, or infections. In this article, we’ll explore these conditions, their symptoms, causes, and how they’re diagnosed and treated, with a special focus on integrative approaches like those used by Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas. We’ll also look at how chiropractic care, targeted exercises, massage therapy, acupuncture, and integrative medicine can promote healing and prevent long-term problems.
What Are Nerve-Related Spine Conditions?
Nerve-related spine conditions happen when the spinal nerves or spinal cord are compressed, irritated, or damaged. The spine is made up of bones called vertebrae, which protect the spinal cord—a bundle of nerves that carries messages to and from the brain. Between the vertebrae are intervertebral discs, which act as cushions, and small openings called foramina, where nerve roots exit the spinal cord to connect to other parts of the body. When these nerves or the spinal cord itself are affected, it can disrupt the signals, leading to symptoms like pain, numbness, tingling, or weakness (Mayo Clinic Health System, n.d.).
Some of the most common nerve-related spine conditions include:
Radiculopathy: Often referred to as a “pinched nerve,” this condition occurs when a nerve root is compressed or irritated as it exits the spine. It can cause pain, numbness, or weakness that radiates along the nerve’s path. For example, lumbar radiculopathy can lead to sciatica, a condition characterized by pain that shoots from the lower back down the leg (Cleveland Clinic, n.d.).
Spinal stenosis refers to the narrowing of the spinal canal, which puts pressure on the spinal cord or nerve roots. It’s often caused by aging or degenerative changes and can lead to symptoms like back pain, numbness, or difficulty walking (HSS Education, n.d.).
Herniated or Bulging Discs: Discs can bulge or herniate (when the inner gel-like material pushes out), pressing on nearby nerves. This can cause pain, tingling, or weakness in the arms or legs, depending on where the disc is located (Penn Medicine, n.d.).
Degenerative Conditions: Conditions like arthritis or bone spurs can narrow the spaces where nerves travel, causing compression and symptoms like pain or stiffness (Health Central, n.d.).
Trauma or Injury: Accidents, such as car crashes or falls, can damage the spine and compress nerves, leading to immediate or delayed symptoms (Verywell Health, n.d.).
Infections or Structural Abnormalities: Infections, tumors, or abnormal spine alignment (like scoliosis) can also press on nerves, causing similar symptoms (MSD Manuals, n.d.).
These conditions can range from mild annoyances to serious issues requiring immediate medical attention, especially if they cause severe symptoms like loss of bladder or bowel control, which may indicate cauda equina syndrome, a medical emergency (Verywell Health, n.d.).
Symptoms of Nerve-Related Spine Conditions
The symptoms of nerve-related spine conditions depend on where the nerve compression or damage occurs and the severity of the condition. Common symptoms include:
Pain: This can be sharp, burning, or aching and may stay in one spot (like the neck or lower back) or radiate to other areas, such as the arms, buttocks, or legs. For example, sciatica often causes burning pain that travels from the lower back to the legs (Penn Medicine, n.d.).
Numbness or Tingling: These sensations, often described as “pins and needles,” can occur in the hands, arms, feet, or legs, depending on the affected nerve (Cleveland Clinic, n.d.).
Weakness: Muscle weakness in the arms, hands, or legs can make it hard to lift objects, walk, or maintain balance. In severe cases, it can cause issues like foot drop, where a person struggles to lift their foot while walking (Johns Hopkins Medicine, n.d.).
Loss of Coordination: Compression of the spinal cord (myelopathy) can affect fine motor skills, making tasks like buttoning a shirt or writing difficult (Verywell Health, n.d.).
Balance Issues: Spinal stenosis or myelopathy can cause trouble walking or maintaining balance, sometimes described as feeling like “walking through mud” (Spine-health, n.d.).
Loss of Bladder or Bowel Control: This is a rare but serious symptom that requires immediate medical attention, as it may signal cauda equina syndrome (HSS Education, n.d.).
Symptoms can develop suddenly, like after an injury, or gradually, as with degenerative conditions like arthritis. If you experience severe or worsening symptoms, especially loss of bladder or bowel control, seek medical care right away.
Causes of Nerve-Related Spine Conditions
Nerve-related spine conditions can have many causes, ranging from natural aging to sudden injuries. Here are some of the main culprits:
Degenerative Changes: As people age, the spine can undergo wear and tear. Osteoarthritis can cause bone spurs, and degenerative disc disease can lead to bulging or herniated discs, both of which can press on nerves (Mayo Clinic Health System, n.d.).
Herniated or Bulging Discs: When a disc’s inner material bulges or herniates, it can push against nearby nerves, causing pain or numbness. This is a common cause of radiculopathy, including sciatica (Penn Medicine, n.d.).
Spinal Stenosis: The spinal canal can narrow due to thickened ligaments, bone spurs, or other changes, putting pressure on the spinal cord or nerve roots (Cleveland Clinic, n.d.).
Trauma: Car accidents, sports injuries, or falls can fracture vertebrae, dislocate joints, or cause swelling that compresses nerves, leading to severe consequences. For example, a car crash can lead to whiplash, which may cause nerve damage in the neck (Solomon Law, n.d.).
Infections: Spinal infections, like abscesses, can press on the spinal cord or nerves, causing pain and neurological symptoms (MSD Manuals, n.d.).
Structural Abnormalities: Conditions like scoliosis (abnormal spine curvature) or tumors can compress nerves, leading to symptoms like pain or weakness (Johns Hopkins Medicine, n.d.).
Inflammatory or Autoimmune Conditions: Diseases like rheumatoid arthritis can cause inflammation that compresses nerves, contributing to symptoms (OrthoTOC, n.d.).
Each cause can lead to different symptoms and requires specific diagnostic and treatment approaches to address the root issue.
Diagnosing Nerve-Related Spine Conditions
Diagnosing nerve-related spine conditions starts with a doctor asking about your symptoms and medical history, followed by a physical exam to check for numbness, weakness, reflexes, and posture. Depending on the findings, additional tests may be needed to pinpoint the cause (Penn Medicine, n.d.). Common diagnostic tools include:
Imaging tests, such as X-rays, CT scans, or MRIs, can reveal the spine’s structure, including bones, discs, and nerves, to identify compression or damage (Spine Info, n.d.).
Nerve Conduction Studies (NCS) and Electromyography (EMG): These tests assess the function of nerves and muscles, and can help confirm nerve damage (Spine Info, n.d.).
Myelogram: A special X-ray or CT scan with contrast dye can highlight pressure on the spinal cord or nerves (Spine Info, n.d.).
Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, uses a dual-scope approach to diagnosis, combining his expertise in chiropractic care and advanced nursing. His clinic utilizes advanced neuromusculoskeletal imaging techniques, such as MRIs and CT scans, to obtain a clear picture of the spine’s condition. Dr. Jimenez correlates patient injuries—whether from work, sports, car accidents, or personal incidents—with clinical findings to create a precise diagnosis. This approach ensures that the treatment plan targets the specific cause of the nerve issue, whether it’s a herniated disc, spinal stenosis, or trauma-related damage (Jimenez, n.d.).
Treatment Options for Nerve-Related Spine Conditions
Treatment for nerve-related spine conditions depends on the cause, severity, and symptoms. Most doctors start with conservative (non-surgical) treatments, moving to surgery only if needed. Here’s an overview of common treatments:
Non-Surgical Treatments
Medications: Over-the-counter pain relievers, such as ibuprofen, or prescription medications, like gabapentin, can help manage pain and inflammation (Spine Info, n.d.).
Physical Therapy: Targeted exercises can strengthen muscles, improve posture, and reduce pressure on nerves. Physical therapy is often effective for radiculopathy and spinal stenosis (Cleveland Clinic, n.d.).
Epidural Steroid Injections: These deliver anti-inflammatory medication directly to the affected nerve root, reducing pain and swelling (Penn Medicine, n.d.).
Chiropractic Care: Adjustments and manipulations can realign the spine, relieving pressure on nerves. Dr. Jimenez’s clinic utilizes chiropractic techniques to treat conditions such as sciatica and herniated discs, with a focus on restoring spinal alignment (Jimenez, n.d.).
Massage Therapy: This can relax tight muscles, improve blood flow, and reduce nerve irritation, especially for conditions caused by muscle tension or spasms (Inova, n.d.).
Acupuncture: By stimulating specific points, acupuncture can reduce pain and promote natural healing, often used alongside other treatments (Total Spine Ortho, n.d.).
Activity Modification: Avoiding activities that worsen symptoms, like heavy lifting, can help the spine heal (Penn Medicine, n.d.).
Surgical Treatments
If conservative treatments are not effective, surgery may be necessary. Common procedures include:
Laminectomy: Removes part of a vertebra to create more space for nerves, often used for spinal stenosis (Spine Info, n.d.).
Microdiscectomy: Removes part of a herniated disc that’s pressing on a nerve, commonly used for radiculopathy (Spine Info, n.d.).
Spinal Fusion: Fuses vertebrae together to stabilize the spine, used for severe degenerative conditions or trauma (Inova, n.d.).
Dr. Jimenez’s clinic takes an integrative approach, combining chiropractic care with targeted exercises, massage therapy, and acupuncture to treat nerve-related spine conditions. For example, a patient with sciatica resulting from a herniated disc may receive spinal adjustments to realign the spine, exercises to strengthen core muscles, and acupuncture to alleviate pain. This holistic approach addresses the root cause while promoting long-term healing and preventing future problems (Jimenez, n.d.).
Dr. Alexander Jimenez’s Integrative Approach in El Paso
Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, has extensive experience treating nerve-related spine conditions caused by work, sports, personal, or motor vehicle accident injuries. His clinic uses a dual-scope approach, blending chiropractic expertise with advanced medical knowledge to provide comprehensive care. Here’s how his clinic handles these cases:
Treating Different Types of Injuries
Work Injuries: Repetitive motions or heavy lifting at work can lead to conditions like herniated discs or radiculopathy. Dr. Jimenez uses spinal adjustments, targeted exercises, and ergonomic advice to relieve nerve compression and prevent recurrence (Jimenez, n.d.).
Sports Injuries: Athletes may suffer nerve compression from trauma or overuse. The clinic employs chiropractic care, physical therapy, and massage to restore function and reduce pain, helping athletes return to their activities (Jimenez, n.d.).
Personal Injuries: Falls or other accidents can cause nerve damage. Dr. Jimenez’s team uses advanced imaging to assess the injury and creates personalized treatment plans, often including acupuncture and exercise (Jimenez, n.d.).
Motor Vehicle Accident (MVA) Injuries: Car crashes can cause whiplash or other trauma that compresses nerves. The clinic provides detailed diagnostic assessments, including MRIs, to identify nerve damage and offers treatments like spinal adjustments and massage to promote healing (Solomon Law, n.d.; Jimenez, n.d.).
Medical Care and Legal Documentation
Dr. Jimenez’s clinic is skilled in handling the medical and legal aspects of injury cases, especially for MVAs. They provide thorough documentation of injuries, diagnoses, and treatments, which is critical for insurance claims or legal cases. For example, if a patient has radiculopathy from a car accident, the clinic documents the injury’s impact on their daily life, the diagnostic findings (like MRI results), and the treatment plan. This detailed paperwork supports patients in legal proceedings while ensuring they receive proper medical care (Jimenez, n.d.).
Integrative Medicine for Healing and Prevention
Dr. Jimenez’s approach emphasizes integrative medicine, combining chiropractic care with other therapies to address the cause of nerve issues and enhance overall health. For instance:
Chiropractic Adjustments: Realign the spine to relieve nerve pressure, effective for conditions like sciatica or herniated discs.
Targeted Exercises: Strengthen muscles around the spine to improve stability and prevent future injuries.
Massage Therapy: Reduces muscle tension and improves circulation, aiding in nerve healing.
Acupuncture: Stimulates natural pain relief and promotes recovery, especially for chronic pain.
Lifestyle Changes: Advice on posture, ergonomics, and nutrition helps prevent long-term problems (Jimenez, n.d.).
This integrative approach not only treats the immediate symptoms but also focuses on long-term health, reducing the risk of chronic pain or recurring issues.
How Integrative Medicine Promotes Healing
Integrative medicine, as practiced by Dr. Jimenez, combines conventional medical treatments with complementary therapies to address the whole person, not just the symptoms. For nerve-related spine conditions, this approach offers several benefits:
Natural Healing: Chiropractic care and acupuncture stimulate the body’s natural healing processes, reducing reliance on medications (Total Spine Ortho, n.d.).
Pain Reduction: Therapies such as massage and acupuncture can help reduce pain levels, thereby improving quality of life (Inova, n.d.).
Improved Function: Exercises and adjustments restore mobility and strength, helping patients return to normal activities (Cleveland Clinic, n.d.).
Prevention: By addressing underlying causes, like poor posture or weak muscles, integrative medicine reduces the risk of future nerve problems (Jimenez, n.d.).
For example, a patient with spinal stenosis might receive adjustments to improve spinal alignment, exercises to strengthen their core, and massage to relax tight muscles. Over time, these treatments can reduce nerve compression, improve mobility, and prevent the condition from worsening.
Preventing Long-Term Problems
Preventing long-term nerve-related spine issues involves addressing the root causes and maintaining spinal health. Here are some strategies:
Maintain Good Posture: Proper posture reduces strain on the spine and nerves (Mayo Clinic Health System, n.d.).
Stay Active: Regular exercise, especially core-strengthening workouts, supports the spine and prevents injuries (Cleveland Clinic, n.d.).
Utilize ergonomics: Adjust workstations or lifting techniques to prevent repetitive strain (Jimenez, n.d.).
Manage Weight: Excess weight can put pressure on the spine, worsening nerve conditions (Health Central, n.d.).
Seek Early Treatment: Addressing symptoms early with chiropractic care or physical therapy can prevent conditions like radiculopathy from becoming chronic (Spine Info, n.d.).
Dr. Jimenez’s clinic emphasizes these preventive measures, educating patients on lifestyle changes to keep their spines healthy and reduce the risk of future nerve issues.
Conclusion
Nerve-related spine conditions, like radiculopathy, spinal stenosis, and herniated discs, can cause significant discomfort and disrupt daily life. These conditions stem from various causes, including degenerative changes, trauma, infections, or structural issues, and lead to symptoms like pain, numbness, tingling, and weakness. Through proper diagnosis using imaging and clinical assessments, doctors can pinpoint the cause and recommend treatments, ranging from medications and physical therapy to surgery in severe cases. Integrative approaches, like those used by Dr. Alexander Jimenez in El Paso, combine chiropractic care, targeted exercises, massage therapy, and acupuncture to treat injuries from work, sports, or accidents while promoting natural healing. By addressing the root cause and focusing on prevention, these methods can help patients recover and avoid long-term problems. If you’re experiencing symptoms of a nerve-related spine condition, consult a healthcare provider to explore your treatment options and start your journey to recovery.
Understand the role of chiropractic care for herniated discs in relieving pain and restoring function for a healthier spine.
Chiropractic Care for Low Back Pain: A Deep Dive into Herniated Discs, Spinal Decompression, and Recovery with Dr. Alex Jimenez
Mon cher, picture this: your spine, that elegant column of bones, is like a grand chandelier in the Addams Family mansion—beautiful, complex, but oh so prone to a flicker or two when things go awry! When a herniated disc sneaks into the lumbar spine, it’s like Gomez Addams tripping over a loose floorboard, sending chaos through the household. But fear not, for chiropractic care, led by the masterful Dr. Alexander Jimenez in El Paso, Texas, is here to restore harmony with a twirl and a flourish!
Low back pain is a common complaint, affecting millions worldwide, with herniated discs often playing the villain in this spine-tingling drama. This blog post explores the clinical rationale behind chiropractic care and spinal decompression as effective treatments for low back pain caused by herniated discs. We’ll dive into the anatomy of the lumbar spine, how herniated discs disrupt daily life, and why Dr. Alex Jimenez, DC, APRN, FNP-BC, stands out as a beacon of hope for personal injury victims in El Paso. With advanced imaging, diagnostic evaluations, and his unique dual-scope approach, Dr. Jimenez bridges the gap between medical care and legal documentation, ensuring patients recover while navigating the complexities of personal injury cases. So, grab a seat—preferably not on a wobbly one—and let’s unravel this tale of spinal recovery with a dash of Gomez Addams’ charm!
The Lumbar Spine: The Backbone of Your Daily Grind
The lumbar spine, or lower back, is the unsung hero of your body, supporting the weight of your upper torso while allowing you to bend, twist, and tango like Gomez with Morticia. It consists of five vertebrae (L1-L5), sturdy bones stacked like a tower of Gothic bricks, connected by intervertebral discs that act as shock-absorbing cushions. These discs, with their tough outer layer (annulus fibrosus) and jelly-like center (nucleus pulposus), are designed to handle pressure, much like a well-crafted torture device from the Addams Family—resilient but not invincible.
When a disc herniates, the nucleus pulposus bulges or ruptures through the annulus fibrosus, often pressing on nearby spinal nerves. This can happen due to aging, wear and tear, or sudden trauma, like lifting a heavy coffin or surviving a fender-bender in El Paso’s bustling streets. The result? Pain, numbness, or weakness that can radiate from the lower back into the buttocks, thighs, or calves, often mimicking the electric jolt Gomez feels when Morticia speaks French.
How Herniated Discs Affect Daily Life
A herniated disc in the lumbar spine, particularly at the L4-L5 or L5-S1 levels, can turn everyday activities into a comedy of errors—minus the laughs. Imagine trying to tie your shoes but feeling like Lurch is sitting on your back. Common symptoms include:
Low Back Pain: A dull ache or sharp, stabbing pain that worsens with movement, making bending or lifting as daunting as facing Uncle Fester’s experiments.
Sciatica: Pain radiating down the leg, caused by nerve root compression, often described as a burning or electric sensation. It’s like Gomez’s fencing foil zapping you unexpectedly.
Numbness or Tingling: A pins-and-needles feeling in the legs or feet, disrupting your ability to walk or stand without feeling like you’re on a bed of nails.
Weakness: Muscles served by affected nerves may weaken, causing stumbling or difficulty lifting objects, as if Pugsley swapped your weights for marshmallows.
These symptoms can severely limit daily routines. Sitting at a desk, driving to work, or even sleeping can become painful, leading to missed workdays, reduced productivity, and a dampened zest for life. For El Paso residents, who often lead active lifestyles and demanding jobs, a herniated disc can feel like a betrayal by their spine.
Chiropractic care, much like Gomez’s passionate dance moves, is all about restoring balance and flow. It focuses on the musculoskeletal system, particularly the spine, to correct misalignments (subluxations) that disrupt nerve function and cause discomfort. For herniated discs, chiropractic care offers a non-surgical, evidence-based approach to relieve pain, reduce nerve compression, and restore mobility. Here’s why it works:
Spinal Manipulation: The Chiropractic Tango
Spinal manipulation, also known as adjustments, involves the precise and controlled application of force to the spine to correct misalignments. Think of it as Gomez gently nudging Morticia back into step during a waltz. By realigning the vertebrae, chiropractors reduce pressure on the herniated disc and compressed nerves, alleviating pain and improving function. A 2020 study in the Spine Journal found that spinal manipulative therapy significantly reduces pain and disability in patients with chronic low back pain (Rubinstein et al., 2020, as cited in).
For patients with MRI-confirmed lumbar disc herniation and sacroiliac joint hypomobility, spinal manipulation has shown promising results. A quasi-experimental study in Chiropractic & Manual Therapies demonstrated that patients receiving spinal manipulation experienced significant pain reduction and improved mobility compared to the control group (Shokri et al., 2018). This is because adjustments restore joint function, reduce inflammation, and enhance blood flow, helping the body heal naturally.
Spinal Decompression: Stretching the Spine with Flair
Non-surgical spinal decompression is like stretching out a tightly wound Addams Family tapestry. This therapy uses a motorized table to gently elongate the spine, creating negative pressure within the disc. This negative pressure can help retract the herniated nucleus pulposus, reducing nerve compression and promoting disc healing. A 2017 study in the Journal of Physical Therapy Science found that spinal decompression significantly reduced pain and disability in patients with lumbar disc herniation (Choi et al., 2017, as cited in).
Dr. Alex Jimenez, a leading chiropractor in El Paso, emphasizes that spinal decompression not only alleviates pain but also rehydrates the disc by improving nutrient delivery. “It’s like giving your spine a refreshing sip of water after a long, dry day,” he notes on his website (El Paso Back Clinic, n.d.). By increasing disc height and reducing herniation volume, decompression therapy restores spinal flexibility, allowing patients to move without wincing.
Functional Medicine: A Holistic Twist
Dr. Jimenez’s practice extends beyond adjustments, incorporating functional medicine to address underlying issues such as inflammation and nutritional deficiencies. For instance, dietary changes can reduce systemic inflammation, accelerating recovery from disc injuries. A 2019 meta-analysis in Pain Physician confirmed that regenerative therapies, like platelet-rich plasma (PRP), can complement chiropractic care by reducing lumbar pain (Sanapati et al., 2019, as cited in). This holistic approach ensures that the body heals from the inside out, much like Gomez nurturing his beloved carnivorous plants.
Shokri, M., et al. (2018). Spinal manipulation in the treatment of patients with MRI-confirmed lumbar disc herniation and sacroiliac joint hypomobility: A quasi-experimental study. Chiropractic & Manual Therapies, 26, 16. https://chiromt.biomedcentral.com/articles/10.1186/s12998-018-0185-z
Rubinstein, S. M., et al. (2020). Spinal manipulative therapy for chronic low-back pain. Spine Journal, 20(4), 489–502.
Dr. Alex Jimenez: El Paso’s Chiropractic Maestro
In El Paso, Texas, Dr. Alexander Jimenez is the Gomez Addams of chiropractic care—passionate, skilled, and dedicated to his craft. With over 25 years of experience as a Doctor of Chiropractic (DC) and a board-certified Family Nurse Practitioner (APRN, FNP-BC), Dr. Jimenez brings a dual-scope approach to treating herniated discs and personal injury cases. His practice at El Paso Back Clinic (https://elpasobackclinic.com/) is a haven for those seeking relief from low back pain, sciatica, and other musculoskeletal woes.
Advanced Imaging and Diagnostics
Dr. Jimenez utilizes state-of-the-art imaging techniques, including MRI and CT scans, to precisely identify the location and severity of a herniated disc. These tools provide a clear picture of soft tissues, revealing disc bulges or nerve compression that X-rays might miss (Personal Injury Doctor Group, 2017). By combining imaging with physical exams, such as the straight leg raise test, he confirms diagnoses with precision, ensuring treatments are tailored to each patient’s individual needs.
Dual-Scope Procedures
What sets Dr. Jimenez apart is his ability to blend chiropractic and medical expertise. His dual-scope approach involves:
Chiropractic Assessments: Identifying spinal misalignments and nerve compression through hands-on evaluations.
Medical Evaluations: Assessing systemic factors, like inflammation or hormonal imbalances, that may hinder healing (Jimenez, 2023, as cited in).
This comprehensive method enables him to create personalized treatment plans that address both the biomechanical and physiological aspects of a herniated disc. For example, he might use spinal adjustments to relieve nerve pressure while recommending nutritional changes to reduce inflammation, ensuring a holistic recovery.
Bridging Medical and Legal Needs
In personal injury cases, such as those from auto accidents, Dr. Jimenez shines as a liaison between medical care and legal documentation. His detailed reports, backed by advanced diagnostics, provide critical evidence for insurance claims or court cases, ensuring patients receive fair compensation. “My goal is to help patients heal while protecting their rights,” Dr. Jimenez shares on his LinkedIn profile (Jimenez, n.d., https://www.linkedin.com/in/dralexjimenez/). His expertise in documenting injuries, from whiplash to complex herniated discs, makes him a trusted practitioner for El Paso’s personal injury victims.
Personal Injury in El Paso: Why Chiropractic Care Matters
El Paso, a vibrant city with a bustling economy, sees its fair share of personal injuries, particularly from motor vehicle accidents (MVAs). These incidents often result in herniated discs, whiplash, or nerve compression, leaving victims in pain and struggling to navigate insurance claims or legal battles. Chiropractic care, especially under Dr. Jimenez’s guidance, is a cornerstone of recovery for these individuals.
The Impact of MVAs
MVAs can cause sudden trauma to the lumbar spine, leading to disc herniation or nerve injuries. For instance, a rear-end collision might whip the spine, causing the nucleus pulposus to bulge and compress the sciatic nerve, resulting in debilitating pain. Dr. Jimenez’s clinic specializes in these cases, using non-invasive techniques like spinal decompression and adjustments to restore function without surgery.
Legal Documentation and Medical Care
Personal injury cases require meticulous documentation to prove the extent of injuries. Dr. Jimenez’s dual licensure as a chiropractor and nurse practitioner enables him to provide comprehensive medical reports that meet legal standards. His use of advanced imaging ensures that injuries are documented, strengthening patients’ cases while guiding their recovery. This dual role is particularly valuable in El Paso, where personal injury claims are common due to the high volume of traffic and industrial activity.
References
El Paso Back Clinic. (2016, September 29). El Paso, TX: Wellness Chiropractic Care Clinic. https://elpasobackclinic.com/
Spinal decompression is a star player in the chiropractic playbook, especially for herniated discs. By gently stretching the spine, this therapy creates a vacuum effect that pulls the herniated disc material back into its proper position, thereby reducing pressure on the nerves. It’s like coaxing a wayward bat back into the Addams Family attic—gentle but effective.
How It Works
During a decompression session, patients lie on a specialized table that alternates between traction and relaxation. This process:
Reduces Disc Pressure: Negative pressure within the disc helps retract the herniated material, relieving nerve compression.
Promotes Healing: Increased blood flow delivers oxygen and nutrients to the disc, aiding rehydration and repair.
Restores Mobility: By alleviating pain and stiffness, decompression allows patients to move freely again.
A 2022 study on PubMed found that non-surgical spinal decompression reduced pain and herniated disc volume in patients with subacute lumbar disc herniation, supporting its efficacy (Choi et al., 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9473337/). Dr. Jimenez’s clinic leverages this therapy to help patients avoid surgery, with many reporting significant relief after a six-week course (El Paso Back Clinic, 2022).
Rehydration: The Disc’s Fountain of Youth
As we age, spinal discs lose water content, becoming less flexible and more prone to herniation. Spinal decompression counteracts this by improving nutrient exchange, effectively “rehydrating” the disc. Dr. Jimenez likens it to “watering a parched plant, bringing it back to life” (El Paso Back Clinic, n.d.). This process not only reduces pain but also enhances disc resilience, preventing future injuries.
References
Choi, J., et al. (2022). Effect of nonsurgical spinal decompression on intensity of pain and herniated disc volume in subacute lumbar herniated disc. International Journal of Clinical and Experimental Medicine, 15(4), 159–167. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9473337/
The effectiveness of chiropractic care for herniated discs is grounded in science, not just Gomez’s theatrical flair. Here’s a closer look at the mechanisms:
Nerve Root Compression Relief
Herniated discs often compress nerve roots, causing radiculopathy—pain, numbness, or weakness radiating along the nerve’s path. Chiropractic adjustments and decompression reduce this compression by realigning the spine and retracting disc material. A French study highlighted that nerve root compression due to lumbar disc herniation is a significant cause of sciatica, and non-surgical interventions, such as chiropractic care, can effectively address it (Valat et al., 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912793/).
Reducing Inflammation
Inflammation exacerbates disc-related pain. Chiropractic care, when combined with functional medicine, helps reduce inflammation through adjustments, targeted nutrition, and lifestyle modifications. Dr. Jimenez’s approach includes dietary plans to reduce systemic inflammation, which supports disc healing (Jimenez, 2023).
Enhancing Biomechanics
Misaligned vertebrae or sacroiliac joint hypomobility can worsen disc issues. Spinal manipulation corrects these misalignments, improving biomechanics and reducing stress on the disc. This is particularly effective for patients with both disc herniation and joint dysfunction (Shokri et al., 2018).
Shokri, M., et al. (2018). Spinal manipulation in the treatment of patients with MRI-confirmed lumbar disc herniation and sacroiliac joint hypomobility: A quasi-experimental study. Chiropractic & Manual Therapies, 26, 16. https://chiromt.biomedcentral.com/articles/10.1186/s12998-018-0185-z
Practical Tips for Managing Herniated Disc Pain
While chiropractic care is a powerful tool, patients can support their recovery with these practical tips, sprinkled with a touch of Addams Family mischief:
Stay Active (Carefully): Gentle movements, such as walking or stretching, keep the spine limber. Avoid heavy lifting—leave that to Lurch!
Mind Your Posture: Sit and stand like Gomez, proud and upright, to reduce spinal stress.
Apply Heat or Ice: Ice reduces inflammation, while heat soothes muscle spasms. Alternate them like Morticia’s mood swings.
Follow Dr. Jimenez’s Nutrition Advice: Anti-inflammatory foods, like berries or fatty fish, support healing. Avoid processed foods—they’re as harmful as Pugsley’s pranks.
Dr. Jimenez’s practice is a beacon for El Paso’s injury victims, offering a blend of compassion and expertise. His clinic, El Paso Back Clinic, provides:
Personalized Care: Tailored treatment plans based on advanced diagnostics.
Holistic Approach: Combining chiropractic, functional medicine, and rehabilitation.
Legal Support: Detailed documentation for personal injury claims, ensuring fair compensation.
Community Trust: Patient testimonials highlight his transformative impact (Jimenez, 2023).
His dual licensure and certifications (IFMCP, CFMP) make him uniquely qualified to address complex cases, from sciatica to chronic pain, with a focus on restoring function and quality of life.
My dear reader, we’ve danced through the shadowy halls of herniated discs and chiropractic care with the grace of Gomez Addams, but now it’s time to dim the candelabra and speak plainly. Low back pain from herniated discs is a serious condition that can disrupt daily life, but chiropractic care, including spinal manipulation and decompression, offers a proven, non-surgical solution. Dr. Alexander Jimenez, with his dual expertise and advanced diagnostic tools, stands out as a trusted practitioner in El Paso, particularly for personal injury cases. His ability to bridge medical care and legal documentation ensures patients recover physically and financially.
Disclaimer: This blog post is for informational purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider, such as Dr. Alex Jimenez, DC, APRN, FNP-BC, before starting any treatment. Individual results may vary, and chiropractic care may not be suitable for all conditions. For personalized guidance, contact El Paso Back Clinic at 915-850-0900 or visit https://elpasobackclinic.com/.
Choi, J., et al. (2022). Effect of nonsurgical spinal decompression on intensity of pain and herniated disc volume in subacute lumbar herniated disc. International Journal of Clinical and Experimental Medicine, 15(4), 159–167. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9473337/
Shokri, M., et al. (2018). Spinal manipulation in the treatment of patients with MRI-confirmed lumbar disc herniation and sacroiliac joint hypomobility: A quasi-experimental study. Chiropractic & Manual Therapies, 26, 16. https://chiromt.biomedcentral.com/articles/10.1186/s12998-018-0185-z
While some disc herniations don’t cause symptoms, individuals who are overweight with a herniated disc may experience obesity pressure symptoms such as pain, weakness, numbness, or tingling. Can implementing a physical therapy and weight loss treatment program help individuals find relief?
Obesity Pressure
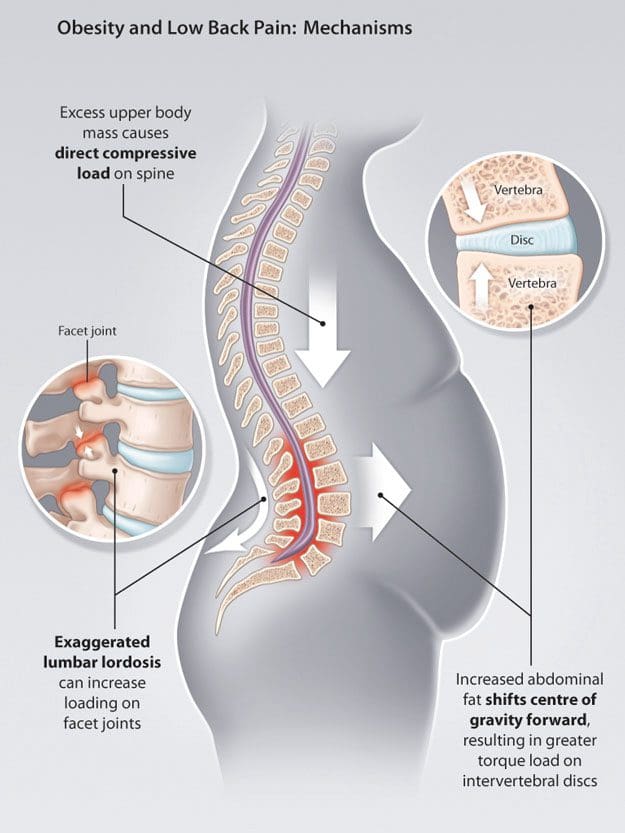
Obesity is one major factor that can contribute to a herniated disc and chronic back pain. When the body has to carry added weight, it can lead to obesity pressure on the intervertebral discs and affect posture and spine position. Researchers have found that other factors, such as inflammation or metabolic changes associated with obesity, can also be involved. (Sheng B. et al., 2017) For individuals who are overweight, weight loss can help resolve a herniated disc combined with physical therapy and can significantly increase herniated disc prevention. (Tokmak M. et al., 2015)
Spine Problems
According to Dr. Alexander Jimenez, owner and head chiropractor at Injury Medical Chiropractic and Functional Medicine Clinic, “When the position of the pelvis and lumbar spine shift out of alignment and become altered, it can profoundly contribute to advanced wearing away of outer fibers in the back region of the discs. These outer fibers house and protect the soft material that cushions and absorbs shock in the spine. Over time, the obesity pressure wear and tear on the fibers can cause chronic pain and microscopic radial tears, leading to a complete rupture.” A rupture causes the soft material to leak, irritate, and inflame surrounding nerve roots. Most herniated discs occur between the sides and back of the vertebra.
Movement Problems
Obesity makes movement difficult, often causing symptoms like shortness of breath and/or early fatigue and exhaustion even with minimal physical activity.
Physical therapy and exercise help relieve obesity and disc herniation.
However, the obesity pressure and herniation pain can make it hard to participate in cardiovascular exercises on a regular basis.
Diagnosis Complications
Obesity can interfere with the diagnosis and treatment of spinal diseases.
This is because weight restrictions and certain imaging tests, like a spinal MRI, can be difficult or impossible to obtain.
A physical examination might not be able to identify signs of nerve compression if an individual is obese. These factors can delay diagnosis.
Disc Position and Posture
Obesity is not the only thing that places pressure on the discs. An individual’s body position significantly influences the health of the shock-absorbing cushions. Sitting generates the most pressure, followed by standing, while lying on your back places the least strain on the discs and, depending on the injury, may help relieve symptoms.
Symptoms depend on the location of the herniation.
The two most common locations are the cervical spine/neck area and the lumbar spine/lower back.
Disc herniations in the neck can affect the arms.
Disc herniations in the lower back affect the buttocks and legs.
Injury Medical Chiropractic and Functional Medicine Clinic
See a healthcare provider if you’re experiencing any of these symptoms. If it is a herniated disc causing symptoms, you might be started on 6 weeks of conservative treatment. This can include physical therapy, rest, health coaching, medication, and surgery, which may be recommended in certain cases. Overcoming these limitations is possible. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Weight Loss Techniques
References
Sheng, B., Feng, C., Zhang, D., Spitler, H., & Shi, L. (2017). Associations between Obesity and Spinal Diseases: A Medical Expenditure Panel Study Analysis. International journal of environmental research and public health, 14(2), 183. https://doi.org/10.3390/ijerph14020183
Tokmak, M., Altiok, I. B., Guven, M., Aras, A. B., & Cosar, M. (2015). Spontaneous Regression of Lumbar Disc Herniation After Weight Loss: Case Report. Turkish neurosurgery, 25(4), 657–661. https://doi.org/10.5137/1019-5149.JTN.9183-13.1
Lower back leg pain depends on specific symptoms and their duration. Can having a better idea of symptoms help individuals inform their medical providers to develop an effective treatment plan?
Low Back Leg Pain
Lower back leg pain, sciatica, and weakness of the lower-extremity muscles are often diagnosed as a herniated (compressed or ruptured) disc. Nerves surrounding the spine are sensitive to irritation and pressure caused by a disc shifting out of position or physical damage to the disc and surrounding area, ranging from mild to severe. This is why it is important to be evaluated by a healthcare provider. Treatment depends on the type of spinal disc herniation and the severity, but getting an early medical evaluation helps ensure optimal outcomes. Non-surgical conservative treatments are often effective, but some cases may require more aggressive treatment, especially if the pain persists.
Spine and Nerves
Spinal discs are the shock absorbers between vertebrae. They consist of a tough outer layer, annulus fibrosis, covering a soft gel core, nucleus pulposus. When a disc is damaged, it can bulge and irritate surrounding nerves. In more severe cases, the annulus fibrosis can weaken and tear, allowing the material to leak and compress the spinal cord or nerves. As the nerves are not functioning properly, abnormal signals may be sent to and from the brain. The most common lower back herniations occur in the lumbar region, where five vertebrae near the base of the spine are classified from top to bottom as L1 through L5. (Dydyk A.M. et al., 2023) Pain resulting from an injury to this part of the spine can be debilitating because it may involve sciatic nerve irritation. Herniated disc causes are generally a combination of age-related degeneration, being overweight/obese, trauma, a sedentary lifestyle, and overloading of the spine. (Cleveland Clinic, 2021)
Symptoms
The most common symptoms include:
Back Pain
Caused by nerve irritation, muscle spasms, and inflammation.
Radiculopathy
Abnormal signaling of the nerves.
Electrical Shooting Pain
Nerve pressure can cause abnormal sensations, commonly experienced as electric shooting pains.
For low back herniations, the shocks go down one or both legs.
Tingling – Numbness
There are often abnormal sensations such as tingling, numbness, or pins and needles down one or both legs.
Muscle Weakness
Nerve signals may be interrupted, causing lower-body muscle weakness. (Dydyk A.M. et al., 2023)
Bowel – Bladder Symptoms
These symptoms may signal cauda equina syndrome, a rare condition resulting from a herniated disc between the L5 vertebrae and the first vertebrae of the sacrum.
Diagnosis
Diagnosing a herniated disc as the cause of low back leg pain involves testing sensation, muscle strength, and reflexes. MRI also aids this process (American Association of Neurological Surgeons, 2024). MRIs can often show herniated discs and other abnormalities, especially in older patients.
Treatment
A herniated disc treatment plan is based on patient symptoms, physical examination findings, and imaging results. Most herniated disc symptoms resolve themselves in four to six weeks. Lower back pain is generally treated conservatively through:
Topical pain ointments or creams for muscle spasms.
Non-surgical decompression relieves pressure, activates healing, and restores circulation and nutrients.
Chiropractic adjustments realign the spine and musculoskeletal system.
Massage loosens the muscles and maintains their relaxation.
Total rest is never recommended, even if movement is challenging,
Exercise and stretching help avoid muscle degeneration and strengthen the muscles.
Relaxation techniques and other natural pain therapies can help manage symptoms and restore overall health.
Pain-blocking injections which can include anesthetics or corticosteroids at the source (Cleveland Clinic, 2021)
Surgery is recommended only when conservative treatments are ineffective after six weeks, if there is significant muscle weakness from nerve damage, or if motor functions are compromised. (American Association of Neurological Surgeons, 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
Chiropractic therapy is among the more conservative treatment options and may be tried first before proceeding with surgery. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other associated medical professionals to integrate a treatment plan to improve the body’s flexibility and mobility and resolve musculoskeletal issues.
Disc Herniation
References
Dydyk AM, Ngnitewe Massa R, Mesfin FB. Disc Herniation. [Updated 2023 Jan 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441822/
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine