The body’s lower extremities have various muscles that allow the legs and feet to move around from one location to another. The different muscles that make up the lower extremities of the body help stabilize the hips and allow mobility to the legs. The legs and hip muscles have a mutual relationship with one body muscle that helps the lower body, and it’s the glutes, specifically the gluteus maximus. Many individuals must realize that the glutes must be activated when working out. When the glutes are not activated, it can lead to the rest of the lower extremities, like the lower back, hips, and knees, taking most of the loaded weight on the body. This leads to the development of trigger points associated with butt pain along the gluteus maximus, causing referred pain down the legs. Today’s article looks at the gluteus maximus muscles, how trigger points are associated with butt pain, and relieving pain is associated with trigger points along the gluteus maximus. We refer patients to certified providers who incorporate multiple techniques in the lower body extremities, like butt pain treatments related to trigger points, to aid individuals dealing with pain symptoms along the gluteus maximus muscles near and surrounding the body’s lower extremities. We encourage and appreciate patients by referring them to our associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Gluteus Maximus?
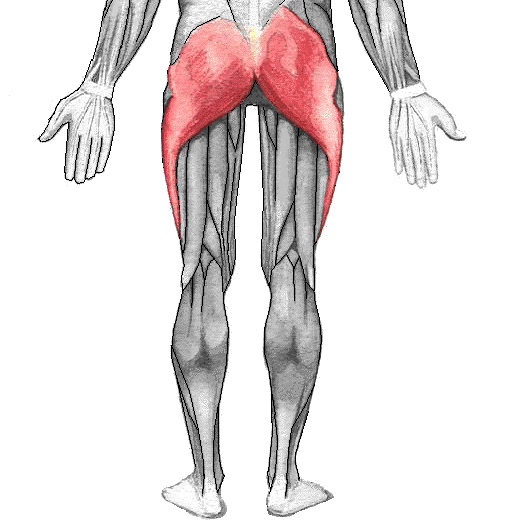
Have you been experiencing pain in your hips, low back, and knees? Are you uncomfortable when you are trying to sit down? Or are you experiencing sciatic pain-like symptoms running from your buttock to your leg? These issues affecting the body’s lower extremities may correlate with trigger points along the gluteus maximus in the buttock. The gluteus maximus is the largest gluteus muscle that makes up the shape and form of the buttock and hip areas of the body. The gluteus maximus can come in different sizes depending on the individual’s body type. This large muscle plays a prominent role in the body as it helps maintain an erect posture for the upper body. Studies reveal that the gluteus maximus is one of the primary hip extensors, and some of its functions include extending and externally rotating the thighs. The gluteus maximus, when trained properly through exercise, can increase in size and strength while supporting the upper body. However, only a few people realize that when their gluteus maximus muscles are not properly trained, it can lead to various issues that can cause trigger points to form along the gluteus maximus.
Trigger Points Associated With Butt Pain
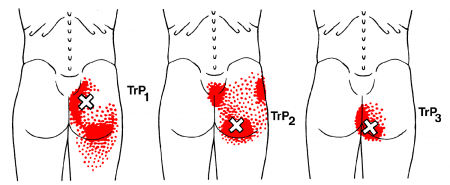
As mentioned earlier, when individuals don’t properly strengthen their gluteus maximus through exercises, it can lead to unwanted pain symptoms affecting the lower back, hips, and knees in the lower body. When the gluteus maximus muscles are not fully activated to their full potential, they can develop into trigger points associated with butt pain. Studies reveal that trigger points or myofascial pain syndrome associated with the gluteus maximus can affect the entry point of the inferior gluteal nerve, causing pain and a limited range of motion to the joints. Dr. Janet G. Travell, M.D., who wrote “Myofascial Pain and Dysfunction,” mentioned that the symptoms caused by active trigger points could make the individual uncomfortable and cause a cramping sensation to the gluteus maximus. At the same time, trigger points along the gluteus maximus can correlate with referred pain that can entrap the sciatic nerve causing sciatica to affect the legs. When this happens, many other issues can pop up and affect the lower extremities, mimicking low back pain.
How To Release Trigger Points On The Gluteus Maximus-Video
Are you experiencing a cramping sensation in your buttock? What about feeling an electric sense running down your leg? Or are you dealing with low back pain? Many of these issues are associated with trigger points affecting the gluteus maximus, causing butt pain. The gluteus maximus is a large, superficial muscle that helps support the hips and ensures that the upper body has an erect posture. When issues affect the gluteus maximus, it can lead to unwanted pain in the lower back, hips, and knees, causing the individual to be in constant pain. This leads to the development of trigger points along the gluteus maximus, thus mimicking sciatica. The video above demonstrates where the trigger points are located in the gluteus maximus and how they can potentially overlap to cause sciatica nerve pain. The video also shows how to use various techniques to relieve the pain from the trigger points and help release the trapped muscle from causing additional pain in the lower body.
Relieving Pain Associated With Trigger Points Along The Gluteus Maximus
Since the gluteus maximus is a large important muscle, it is important to strengthen the glutes to prevent low back pain. When it comes to relieving pain associated with trigger points along the gluteus maximus, there are various techniques that many people can utilize to release the tension from the gluteus maximus and the rest of the lower body. Various glute stretches can help elongate the gluteus maximus muscle after a workout and reduce the chances of triggering points and referred pain re-occurring. Another technique that many people should do is to bend at the knees when lifting heavy objects to reduce overload on the lower back and cause more issues on the gluteus maximus.
Conclusion
The gluteus maximus is a large superficial muscle with a very important function in the body. This muscle helps with extending and externally rotating the thighs and helps keep the posture erect for the upper back. However, the gluteus maximus muscles are not properly trained and can lead to unwanted issues that cause referred pain to the hips, low back, and knees that correlate with triggering points. Luckily though, through proper training and stretching, the lower body can prevent the gluteus maximus from developing trigger points and help improve a person’s posture.
References
Akamatsu, Flavia Emi, et al. “Anatomical Basis of the Myofascial Trigger Points of the Gluteus Maximus Muscle.” BioMed Research International, Hindawi, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5733974/.
Elzanie, Adel, and Judith Borger. “Anatomy, Bony Pelvis and Lower Limb, Gluteus Maximus Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 28 Mar. 2022, https://www.ncbi.nlm.nih.gov/books/NBK538193/.
Neto, Walter Krause, et al. “Gluteus Maximus Activation during Common Strength and Hypertrophy Exercises: A Systematic Review.” Journal of Sports Science & Medicine, Uludag University, 24 Feb. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7039033/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
The body’s pelvic region has many functions crucial for functionality with the host. The various muscles surrounding the pelvis help provide stability to the body’s core, allow circulation to the heart in the cardiovascular system, support the reproductive and abdominal organs, and much more the body requires. The pelvic joints’ various muscles also allow hip mobility and function for the lower body extremities. When traumatic injuries or abnormal activities start to affect the pelvic floor muscles, the various issues can affect the functionality of the pelvic region and cause problems in bladder control for both the male and female bodies. Many of these issues correlate with trigger points surrounding or on the pelvic floor muscles that can affect how the vital organs operate in the body. Today’s article examines the pelvic floor muscles, how trigger points correlate with pelvic pain, and managing pelvic pain is associated with trigger points. We refer patients to certified providers who incorporate multiple techniques in the lower body extremities, like pelvic pain treatments related to trigger points, to aid individuals dealing with pain symptoms along the pelvic floor muscles near and surrounding the pelvis. We encourage and appreciate patients by referring them to our associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Are The Pelvic Floor Muscles?
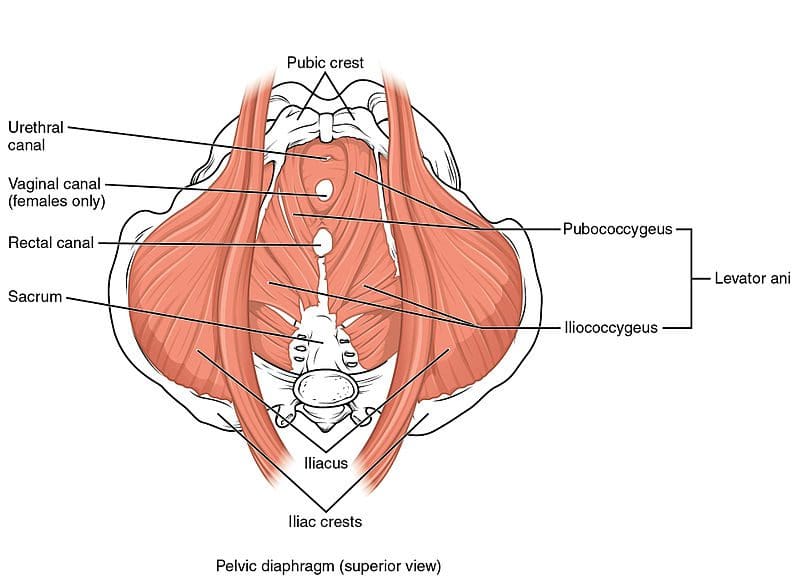
Have you been experiencing bladder issues that constantly make you go to the bathroom? Have you been dealing with severe cramps that mimic sciatica pain? Or does it hurt when you are sitting down? Many of these issues correlate with muscle pain associated with trigger point pain along the pelvic floor muscles. The pelvic floor muscles are a unique anatomical body location with a balance of different pressures (visceral, muscular, or liquid) that play a fundamental role in the body’s lower extremities. The pelvic floor muscles have four divided compartments but have different parts and functions to allow optimal bodily function. The four pelvic floor compartments include:
Anterior or urinary (bladder)
Medium or genital (uterus in women, prostate in men)
Posterior or anterior (anus, anal cavity, and rectum)
Peritoneal (endopelvic fascia and perineal membrane)
Some of the functions that the pelvic floor muscles allow the body to perform properly include proper contraction for sexual function, allowing respiration in the abdominal organs, maintaining bodily fluid actions like going to the restroom, and maintaining good posture by working together with the thoracolumbar and lumbosacral columns of the spine. Studies reveal that the spine’s autonomic nerves, which include the sympathetic and parasympathetic, help supply the posterior and anterior compartments in the pelvic floor. When traumatic factors affect the pelvic floor muscles, it can lead to correlating issues regarding trigger points in the pelvic muscles.
How Do Trigger Points Correlate With Pelvic Pain?
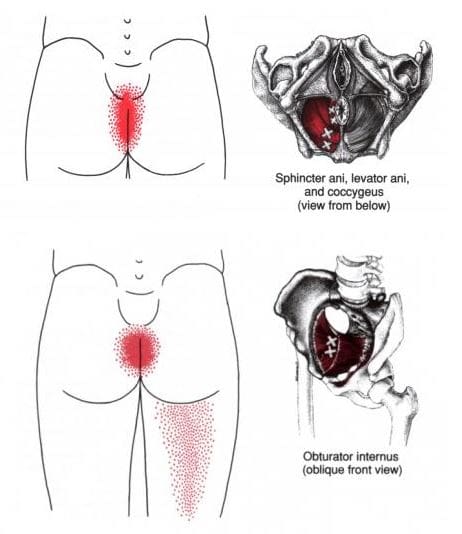
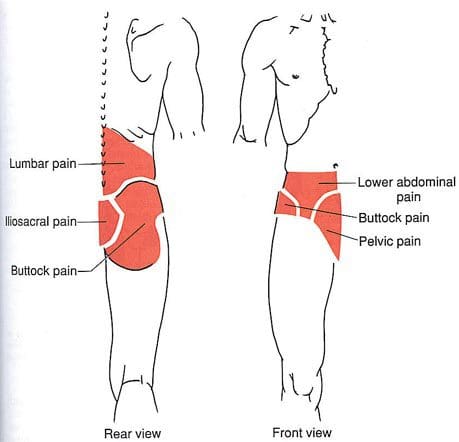
The pelvic floor has four different components to allow the muscles to function properly when traumatic factors start to invoke pain-like symptoms that can affect pelvic functionality in both the male and female body, thus developing trigger point pain associated with pelvic pain. For the female body, trigger points along the bulbospongiosus muscle (part of the pelvic floor muscles) may cause aching pain in the perineal region. In contrast, in the male body, trigger points along the retroscrotal area may cause discomfort while sitting erect. According to the book, “Myofascial Pain and Dysfunction,” written by Dr. Janet G. Travell, M.D., stated that many individuals that are dealing with trigger point pain along their pelvic floor muscles would often complain about feeling localized aching pain in their anal region and may experience painful bowel movements when going to the bathroom.
Studies reveal that myofascial trigger points develop “muscle contraction knots” of the pelvic floor muscles, may be identified in many patients suffering from pelvic pain syndrome (urological, colorectal, and gynecological), and are associated with trigger points. Trigger points are tricky when diagnosing where the pain is located since myofascial pain syndrome mimics other chronic conditions of the surrounding muscles, causing referred pain. Additional studies reveal that the location and severity of pelvic floor myofascial pain was significantly correlated with various pelvic pain symptoms that can affect both males and females with different conditions. When doctors recognize that their patients are dealing with trigger points associated with pelvic pain after an examination, they devise a treatment plan and work with other specialists to manage trigger points and reduce pain in the pelvic region.
Top 3 Pelvic Floor Exercises- Video
Have you been dealing with urinary issues that make it tricky to go to the bathroom? Do you have trouble finding a comfortable position when you are sitting down? Or do you feel pain radiating down your buttock and leg? Pelvic pain is a common issue that can affect both men and women that can cause various pain symptoms that correlate with trigger points along the pelvic floor muscles. When trigger points affect the pelvic floor muscles, it can lead to referred pain that connects with pelvic pain in the body’s lower extremities. Many factors can affect the pelvis, like issues affecting the digestive, reproductive, or urinary systems, a trauma in the surrounding pelvic muscles that causes them to be weak or corresponding issues on the hips and lower back. Trigger points associated with pelvic pain may be tricky. Still, they can be treatable with different therapies that can reduce the pain and help strengthen those weak muscles in the pelvic region. The video above demonstrates three other pelvic floor exercises that can help support the pelvic muscles and reduce the trigger points from reoccurring in the pelvic area of the lower body.
Managing Pelvic Pain Associated With Trigger Points
Various treatments can manage pain associated with trigger points through multiple therapies that can reduce pain-like symptoms along the pelvic floor muscles. Many therapies, like trigger point therapy and muscle training, can help reduce the pain along the pelvic floor muscles and bring back bowel function to the pelvic region. Studies reveal that doctors provide a range of protocols designed to strengthen the pelvic floor muscles and the different muscle groups around the pelvic area while improving function. However, treatment alone can only go so far, as people must take corrective actions to ensure that the trigger points do not return in the future. Movements like corrective posture exercises focusing on the lower back, hips, and pelvis and eating a fiber-rich diet can reduce pelvic pain. This allows the individual to get their lower half mobility back.
Conclusion
The pelvic floor muscle has four divided components that will enable optimal bodily function that has different jobs in the male and female bodies. The pelvic floor muscles have many crucial functions that provide the host stability in the body’s core, allow circulation to the cardiovascular system, and, most importantly, support the reproductive and abdominal organs. When issues affect the pelvic floor muscles, it can lead to pelvic pain associated with trigger points that can disrupt many from going to the bathroom or disrupting sexual functionality. All is not lost, as various therapies can reduce the pain and strengthen the pelvic muscles in the lower body. This allows lower body mobility back to the host and prevents unnecessary issues from reoccurring.
References
Bordoni, Bruno, et al. “Anatomy, Abdomen and Pelvis, Pelvic Floor.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 18 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK482200/.
Marques, Andrea, et al. “The Status of Pelvic Floor Muscle Training for Women.” Canadian Urological Association Journal = Journal De L’Association Des Urologues Du Canada, Canadian Medical Association, Dec. 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2997838/.
Meister, Melanie R, et al. “Pelvic Floor Myofascial Pain Severity and Pelvic Floor Disorder Symptom Bother: Is There a Correlation?” American Journal of Obstetrics and Gynecology, U.S. National Library of Medicine, Sept. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6732028/.
Moldwin, Robert M, and Jennifer Yonaitis Fariello. “Myofascial Trigger Points of the Pelvic Floor: Associations with Urological Pain Syndromes and Treatment Strategies Including Injection Therapy.” Current Urology Reports, U.S. National Library of Medicine, Oct. 2013, https://pubmed.ncbi.nlm.nih.gov/23943509/.
Raizada, Varuna, and Ravinder K Mittal. “Pelvic Floor Anatomy and Applied Physiology.” Gastroenterology Clinics of North America, U.S. National Library of Medicine, Sept. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2617789/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
The posterior section of the lower half of the body consists of the hips, low back, pelvis, legs, and feet, which provide stability to the body while supporting the upper body’s weight. The various muscles surround the lower extremities and make different motions for mobility and functionality by contracting and retracting when the legs and hips are in motion. The various muscles that provide stability to the hips and the legs are the iliopsoas muscles. When normal age or incidents affect the lower body extremities, it can correlate to the development of trigger point pain. Today’s article examines the iliopsoas muscles, how referred trigger pain affects the thighs and low back, and treating trigger point pain on the thighs and low back. We refer patients to certified providers who incorporate multiple techniques in the low back and thigh pain therapies related to trigger points to aid individuals dealing with pain symptoms along the iliopsoas muscle in the lower back, thigh, and near the pelvis. We encourage and appreciate patients by referring them to our associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Iliopsoas Muscle?
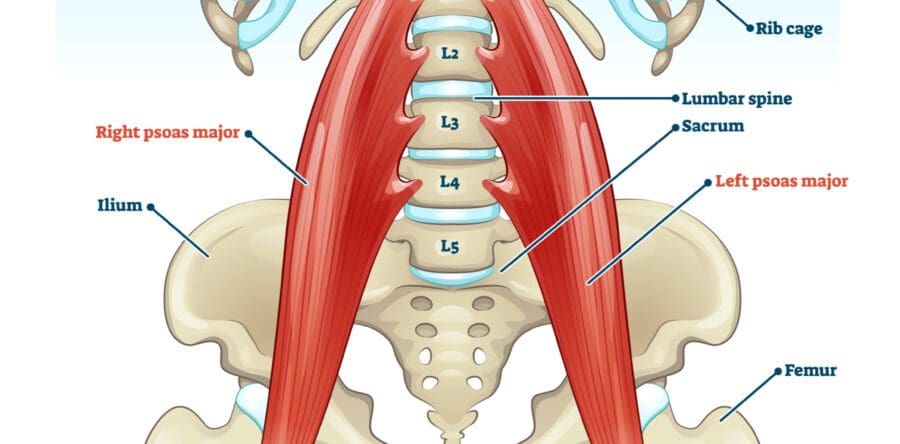
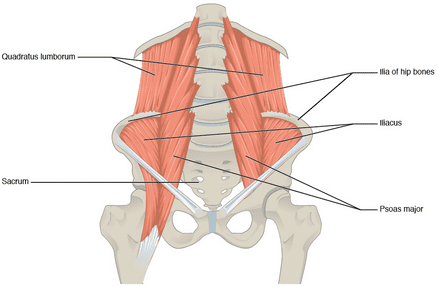
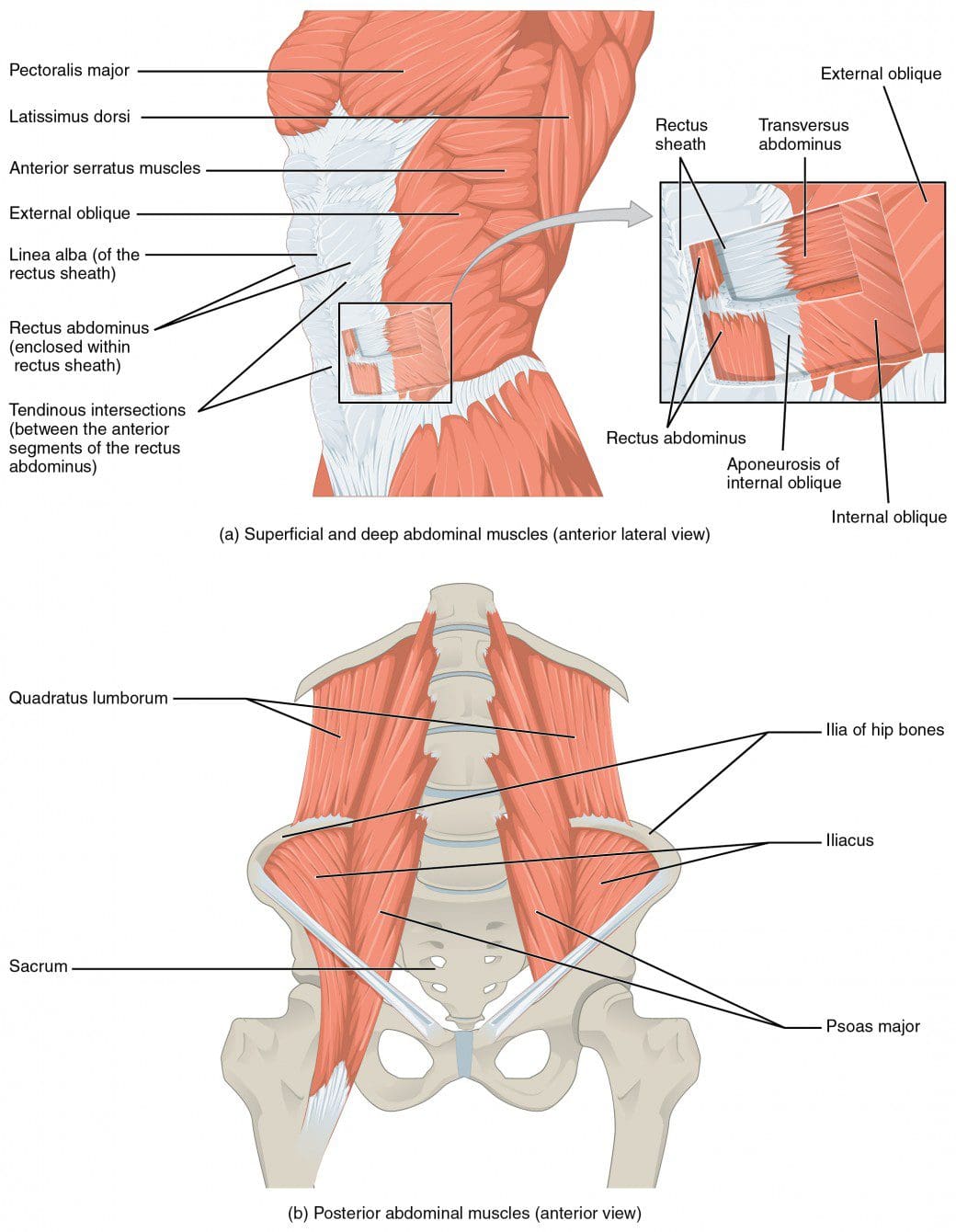
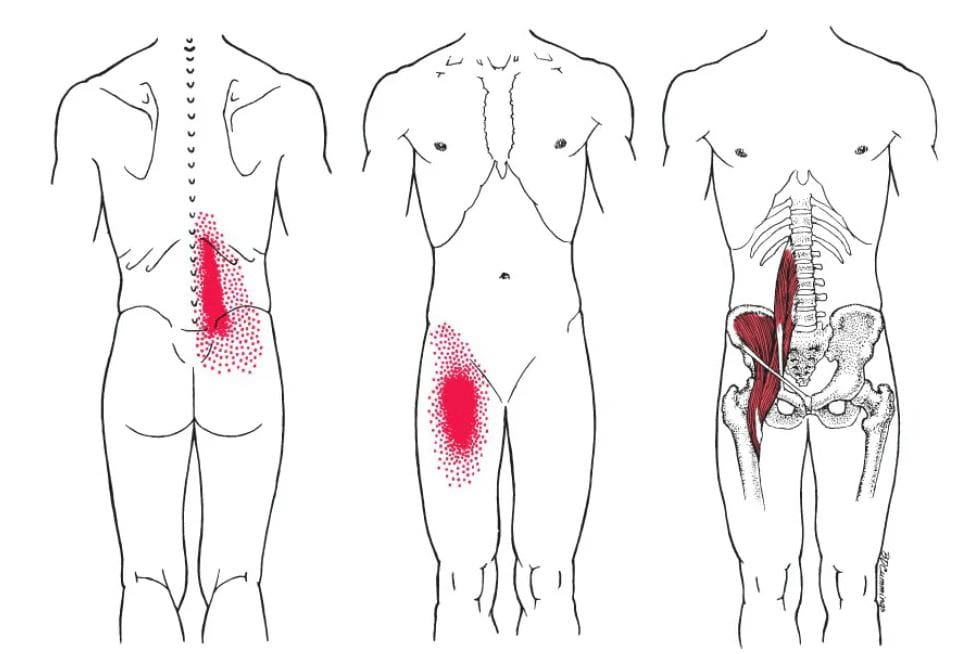
Have you been dealing with muscle cramps in your thighs? What about feeling muscle stiffness in your lower back when you are stretching? Or do you feel your thigh muscles become heavy after a workout? Many of these issues correlate with the iliopsoas muscle becoming overused and developing trigger points, thus affecting the thighs and lower back. In the lower body extremities, the muscles that help provide stability to the hips are the iliopsoas muscles. The iliopsoas muscles consist of three muscles: iliacus, psoas major, and psoas minor, which can work individually or as a unit. When working individually, the iliacus muscle provides stability to the pelvis, the psoas major muscle helps stabilize the lumbar spine when a person is sitting, and the psoas minor helps with flexion of the trunk and stretch the iliac fascia. As a unit, however, these muscles work together to become the primary flexors of the thighs and allow hip flexion.
Studies reveal that the iliopsoas is a deep muscle group that anatomically connects the spine to the body’s lower limbs. The iliopsoas muscles have an important function in the body’s lower limbs as primary hip flexors for daily activities, especially for those in sports. However, many impairments and pathologies affect the iliopsoas, which causes significant limitations and challenges since the symptoms mask the pain, causing individuals to think they are dealing with low back and hip pain.
Referred Trigger Pain On The Thighs & Low Back
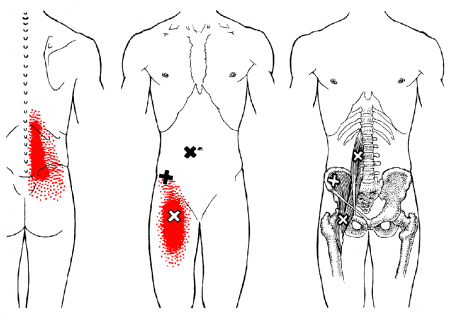
Since the iliopsoas muscles provide hip and thigh flexion to the lower body, many impairments and pathologies can affect this muscle group, causing issues in the hips, thighs, and even the lower back. These impairments can cause the iliopsoas muscles to be overused and overstretched, thus potentially developing trigger points along the iliopsoas muscles, causing referred pain on the thighs and low back. Studies reveal that when the iliopsoas muscle becomes overused or traumatic issues affect it, it can lead to problems in hip flexion and impairment in the lower extremities. In “Myofascial Pain and Disorders: The Trigger Point Manual,” written by Dr. Janet G. Travell, M.D., when trigger points begin to affect the iliopsoas muscles, it is known as the “Hidden Prankster” as normal factors like poor posture can overload the back causing trigger points to form not only on the iliopsoas muscles but the hamstrings, gluteal, thoracolumbar paraspinal, and posterior cervical muscles. Trigger points can mimic other chronic conditions that cause referred pain in different body areas. Trigger point pain in the iliopsoas muscle can lead to back pain, groin pain, snapping hips, and standing up difficult for the individual if it is not treated immediately.
Trigger Point Therapy: Iliopsoas Muscle- Video
Since the iliopsoas muscles provide hip and thigh flexion to the lower body, many impairments and pathologies can affect this muscle group, causing issues in the hips, thighs, and even the lower back. These impairments can cause the iliopsoas muscles to be overused and overstretched, thus potentially developing trigger points along the iliopsoas muscles, causing referred pain in the thighs and low back. Studies reveal that when the iliopsoas muscle becomes overused or traumatic issues affect it, it can lead to problems in hip flexion and impairment in the lower extremities. In “Myofascial Pain and Disorders: The Trigger Point Manual,” written by Dr. Janet G. Travell, M.D., when trigger points begin to affect the iliopsoas muscles, it is known as the “Hidden Prankster” as normal factors like poor posture can overload the back causing trigger points to form not only on the iliopsoas muscles but the hamstrings, gluteal, thoracolumbar paraspinal, and posterior cervical muscles. Trigger points can mimic other chronic conditions that cause referred pain in different body areas. Trigger point pain in the iliopsoas muscle can lead to back pain, groin pain, snapping hips, and standing up difficult for the individual if it is not treated immediately.
Treating Trigger Point Pain On The Thighs & Low Back
When trigger point pain begins to cause issues in the thighs and low back, the iliopsoas muscles will suffer from muscle spasms, stiffness, and difficulty standing. This is due to nerve entrapment from aggravated iliopsoas muscles caused by trigger points. However, various treatments can manage trigger point pain in the thighs, and low back through multiple techniques that pain specialists utilize can help relieve the pain symptoms from the iliopsoas muscle and manage trigger point pain. Studies reveal that combination treatments like soft tissue manipulation and trigger point therapy can help release the tiny nodules from the affected muscle and reduce the symptoms from re-occurring in the body. Other treatments, like correcting one’s posture, strength exercising, and even stretching, can help lengthen the iliopsoas muscles, stretch and strengthen the surrounding muscles, and prevent pain-like symptoms from affecting the thigh and low back muscles again. These various treatments can even improve hip mobility in the lower body extremities.
Conclusion
In the lower body extremities, an iliopsoas is a group of deep muscles that provide stability to the lumbar spine and allow hip and thigh flexion. These groups of deep muscles can work individually or together to enable the individual to sit, stand and move around through physical activities; however, when the iliopsoas muscles become overused or suffer from a traumatic event, they can develop trigger points that can cause mobility issues on the thighs, hips, and lower back. Even though trigger points are difficult to diagnose, they are treatable through various treatments. Various treatments, like soft tissue massages, trigger point therapy, strength exercising, or stretching the iliopsoas muscles, can release trigger points from the affected body part and help bring back mobility function to the hips, thighs, and low back.
References
Bordoni, Bruno, and Matthew Varacallo. “Anatomy, Bony Pelvis and Lower Limb, Iliopsoas Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 2 Apr. 2022, https://www.ncbi.nlm.nih.gov/books/NBK531508/.
Dydyk, Alexander M, and Amit Sapra. “Psoas Syndrome.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 12 June 2022, https://www.ncbi.nlm.nih.gov/books/NBK551701/.
Kameda, Masahiro, and Hideyuki Tanimae. “Effectiveness of Active Soft Tissue Release and Trigger Point Block for the Diagnosis and Treatment of Low Back and Leg Pain of Predominantly Gluteus Medius Origin: A Report of 115 Cases.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6382483/.
Lifshitz, Liran, et al. “Iliopsoas the Hidden Muscle: Anatomy, Diagnosis, and Treatment.” Current Sports Medicine Reports, U.S. National Library of Medicine, June 2020, https://pubmed.ncbi.nlm.nih.gov/32516195/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
The lower back works with the body’s lower extremities by stabilizing the hips and helping support the upper body’s weight. The lower back also has many functions when it comes to mobility. The lower back allows the person to bend, twist, and rotate the torso without any pain inflicted on the body. When normal factors or traumatic issues start to cause low back pain in the individual, the pain-like symptoms can correlate to the development of trigger points in the lower back muscles. Today’s article examines the quadratus lumborum, how myofascial trigger pain affects the low back, and how to manage myofascial trigger pain through various treatments. We refer patients to certified providers who incorporate multiple techniques in low back pain therapies related to trigger points to aid individuals dealing with pain symptoms along the quadratus lumborum in the lower back. We encourage and appreciate patients by referring them to our associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Quadratus Lumborum?
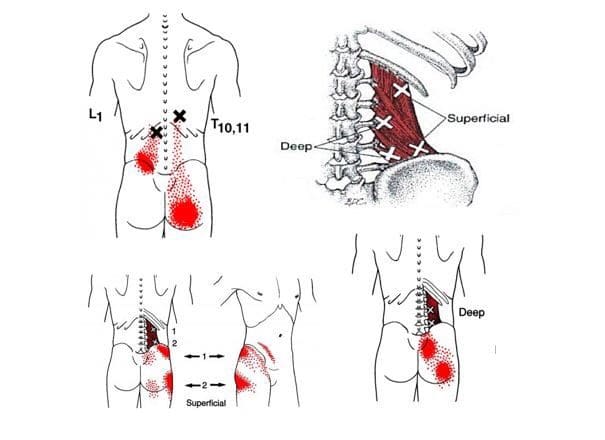
Have you been experiencing low back pain? Do you feel relief when you stretch your lower back, only to have the pain return later? Do you feel tenderness or soreness on the sides? Many of these complaints are correlated with low back pain associated with trigger points along the quadratus lumborum. The quadratus lumborum is a flat, quadrangular-shaped muscle in the iliac crest and deep back. This muscle plays an important part in the thoracolumbar fascia that covers the posterior body area while involving the lower and upper parts of the limbs. According to “Myofascial Pain and Dysfunction: The Trigger Point Manual,” written by Dr. Janet G. Travell, M.D., mentioned that the quadratus lumborum functions to control the side bending to the opposite side by lengthening contraction. Other studies reveal that various actions on the lumbar spine have been attributed to the quadratus lumborum. When the quadratus lumborum goes through these different actions, it can cause the muscles to become overused, or when injuries occur in the lower back, it can lead to various issues that can develop into overlapping conditions in the lower back.
Myofascial Trigger Pain Affecting The Low Back
When it comes to the lower back, many individuals worldwide experience some pain in their backs, and low back pain is common. Various factors cause low back pain from lifting heavy objects, over-exerting the sides with rapid turning, or even normal wear and tear of the body, which can cause lower back pain. When low back pain affects the quadratus lumborum, it can develop trigger points or myofascial trigger pain. Studies reveal that low back pain from the quadratus lumborum can present myofascial pain, causing the individual to have an acute pain episode in their lower back. Myofascial trigger pain is developed when the affected muscle has been overused and causes tiny knots to form along the muscle fibers. When myofascial trigger pain is in the quadratus lumborum, it becomes activated acutely through awkward movements or sudden trauma in the lower back, affecting the mobility of the lower back and the hips. Additional studies reveal that the prevalence of myofascial trigger pain in the quadratus lumborum, when being diagnosed, can display significantly less hip abduction strength. Low back pain associated with myofascial trigger pain can correlate with other chronic issues affecting the body’s lower extremities.
Trigger Point Release: Quadratus Lumborum- Video
Are you experiencing mobility issues in your hips? Do you feel symptoms of tenderness or stiffness in your lower back? Does it hurt when you are bending down to pick up an item? Most of these symptoms correlate with low back pain, potentially involving trigger points along the quadratus lumborum. Trigger points are formed when the muscle has been overused or been through a traumatic event like an auto accident, and since low back pain is common worldwide, it can mask other chronic conditions that overlap the pain. The video explains where the quadratus lumborum is located in the back, where the trigger points are marked, and how to manage the trigger points through manual manipulation while reducing pain away from the lower body. When myofascial trigger pain begins to wreak havoc on the affected muscles in the lower back. Various treatments applied to the lower back can help alleviate the symptoms caused by trigger points associated with the lower back along the quadratus lumborum.
Managing Myofascial Trigger Pain Through Various Treatments
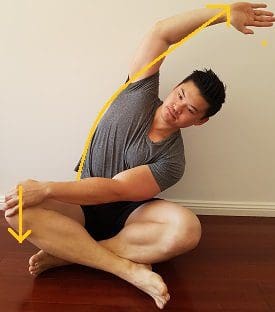
Since low back pain is common worldwide and can potentially lead to the development of trigger points along the various lower back muscles, especially the quadratus lumborum, many individuals would utilize medication specifically for low back pain to reduce the pain symptoms; however, it only masks the pain caused by myofascial trigger pain. Studies reveal manual trigger-point therapy techniques that healthcare providers use to assess patients who are in pain from myofascial trigger pain. Many will go to a pain specialist to manage trigger points when the pain becomes too much for the individual. Another method that many people should utilize as part of their daily practice is doing gentle side stretching on the quadratus lumborum to loosen up the stiff muscles and reduce the chances of trigger points forming in the affected muscle in the future.
Conclusion
The quadratus lumborum is a flat, quadrangular-shaped muscle in the iliac crest and deep back. This muscle helps with posterior mobility of the lower extremities and, when overused, can develop myofascial trigger pain associated with the low back. This can lead to various common back pain issues that affect how a person moves and become unstable when in motion. Fortunately, low back pain associated with myofascial trigger pain is treatable through various treatments that can reduce the pain and manage trigger points located in the low back. When people incorporate treatments to alleviate pain in their lower back, they will begin to experience relief and have their sense of purpose back in their lives.
References
Bordoni, Bruno, and Matthew Varacallo. “Anatomy, Abdomen and Pelvis, Quadratus Lumborum.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 18 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK535407/.
de Franca, G G, and L J Levine. “The Quadratus Lumborum and Low Back Pain.” Journal of Manipulative and Physiological Therapeutics, U.S. National Library of Medicine, Feb. 11AD, https://pubmed.ncbi.nlm.nih.gov/1826922/.
Grover, Casey, et al. “Atraumatic Back Pain Due to Quadratus Lumborum Spasm Treated by Physical Therapy with Manual Trigger Point Therapy in the Emergency Department.” Clinical Practice and Cases in Emergency Medicine, University of California Irvine, Department of Emergency Medicine Publishing Western Journal of Emergency Medicine, 29 May 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6682240/.
Phillips, S, et al. “Anatomy and Biomechanics of Quadratus Lumborum.” Proceedings of the Institution of Mechanical Engineers. Part H, Journal of Engineering in Medicine, U.S. National Library of Medicine, Feb. 2008, https://pubmed.ncbi.nlm.nih.gov/18441751/.
Roach, Sean, et al. “Prevalence of Myofascial Trigger Points in the Hip in Patellofemoral Pain.” Archives of Physical Medicine and Rehabilitation, U.S. National Library of Medicine, Mar. 2013, https://pubmed.ncbi.nlm.nih.gov/23127304/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
The body’s lower extremities have a very important role as it helps support the upper body’s weight and provide stability to the lower body. The lower half of the body consists of the lower abdominals, hips, pelvic, and buttock regions, which have various muscles surrounding the lumbar and pelvic areas of the spine. These muscles help protect the lower vital organs and work with the central nervous system to utilize the sensory-motor function of the legs and feet. When normal factors like prolonged sitting or standing begin to affect the lower body, it can cause referred pain to travel down to the legs and push the lower extremities to develop symptoms associated with trigger points on the lower torso. Today’s article looks at the lower torso, how trigger points affect the lower torso, and therapeutic ways to manage trigger points in the lower torso. We refer patients to certified providers who incorporate various techniques in more inadequate body pain treatments related to trigger points to aid people suffering from pain-like symptoms along the lower torso muscles along the body’s lower extremities. We encourage and appreciate patients by referring them to our associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Lower Torso?
Have you been feeling stiffness around your hips lately? Have you noticed that you are leaning forward constantly, causing strain on your lower back? Or have you been experiencing pain in one location in your lower half? When dealing with these issues in the lower half of the body, it could correlate with somato-visceral symptoms associated with trigger points in the lower torso. The lower torso of the human body, or the lower abdominals, is defined as the anterior region of the trunk between the thoracic diaphragm and serves as the cavity to house the digestive, urinary, endocrine, and parts of the reproductive system. The lower torso has various muscles and nerves that surround the lower back, the hips, the pelvis, and the buttock region of the body that stabilizes the legs when in motion and supports the upper body. The muscles in the lower torso also surround the lumbar and pelvic areas of the spine to protect the joints and vertebrae from becoming dysfunctional. When issues begin to rise and affect the lower torso, it can lead to overlapping problems affecting the body’s lower extremities.
How Do Trigger Points Affect The Lower Torso?
Some of the issues affecting the lower torso that most people don’t realize are that prolonged sitting or standing can cause problems to the legs, hips, pelvis, and feet. This causes the blood supply to pool into the legs and feet, thus causing swelling and muscle weakness in the lower torso muscles. Another issue is when the lower torso has been through a traumatic event that can cause the affected muscles to develop tiny nodules known as trigger points to cause problems in the lower back, hips, pelvis, and buttock region of the body. Studies reveal that trigger points are often characterized by pain causing a limited range of motion in the joints while causing muscular contracture and mimicking other chronic conditions affecting the muscles. When trigger points affect the muscles in the lower torso, “Myofascial Pain and Dysfunction,” written by Dr. Janet Travell, M.D., pain associated with movement can cause tingling or electric sensations down to the lower extremities causing somato-visceral referred pain to the lower torso. Since the nerve roots from the spinal cord branch out to the various muscles and become irritated, causing referred pain to different areas of the lower extremities.
Trigger Point Therapy For The Abs- Video
Have you been dealing with hip mobility issues? What about experiencing low back pain after being in a hunch position for an extended period? Or have you been experiencing problems in your pelvic region? Many of these issues are correlated with trigger points associated with the lower torso. Trigger points or myofascial pain syndrome are caused when the affected muscles have been overused or been through a traumatic event that causes referred pain to different body locations. The video explains where trigger points are located in the lower torso, especially in the abdomen and how to release them through palpations and massage. These techniques can help reduce the pain symptoms that affect the lower torso and manage myofascial pain from developing in the future.
Therapeutic Ways To Manage Trigger Points In The Lower Torso
Pain specialists like chiropractors and massage therapists will use various techniques to reduce the pain and alleviate the trigger points from the affected muscles. Many often go to a pain specialist who deals with trigger points through recommendations by their primary doctor. They will go through an examination process and explain to the pain specialist where the pain is located. Afterward, they will devise a treatment plan with the patient’s primary doctor, allowing them to follow a routine to prevent the pain from returning. Various techniques like stretching the abdominals, exercising, and resting can manage trigger points from returning to the affected muscles and even help bring muscle strength back to the body.
Conclusion
The lower torso consists of the hips, lower back, pelvis, and buttock region while protecting the body’s vital organs. The lower torso helps stabilize, the lower body extremities and supports the upper body’s weight. When normal issues like prolonged sitting or standing start to cause muscle strain to the lower torso region, it can develop trigger points to cause various problems to that region and cause mobility issues in the lower abdominal area. When the pain becomes unbearable, many individuals go to a pain specialist to help manage the trigger points from affecting the lower torso region and bring back mobility function to the lower extremities.
References
Akamatsu, Flavia Emi, et al. “Anatomical Basis of the Myofascial Trigger Points of the Gluteus Maximus Muscle.” BioMed Research International, Hindawi, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5733974/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Wade, Christian I, and Matthew J Streitz. “Anatomy, Abdomen and Pelvis, Abdomen – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK553104/.
When it comes to the torso is surrounded by various muscles that help protect the vital organs known as the gut system and help with stabilizing the spinal column in the body. The abdominal muscles are essential to maintaining good posture and core support for many individuals. When normal activities or chronic issues begin to affect the body, the abdominal muscles can also be affected and can cause referred pain all around the torso area. When the abdominal muscles are dealing with referred pain, it can develop into trigger points that mask other chronic conditions affecting the torso and the thoracolumbar region. Today’s article looks at the abdominal muscles and their function, how trigger points are affecting the abdomen, and how various treatments help manage trigger points associated with abdominal pain. We refer patients to certified providers who provide different techniques in abdominal pain therapies related to trigger points to aid many suffering from pain-like symptoms along the abdominal muscles along the torso. We encourage patients by referring them to our associated medical providers based on their examination when it is appropriate. We designate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
The Abdominal Muscles & Their Function
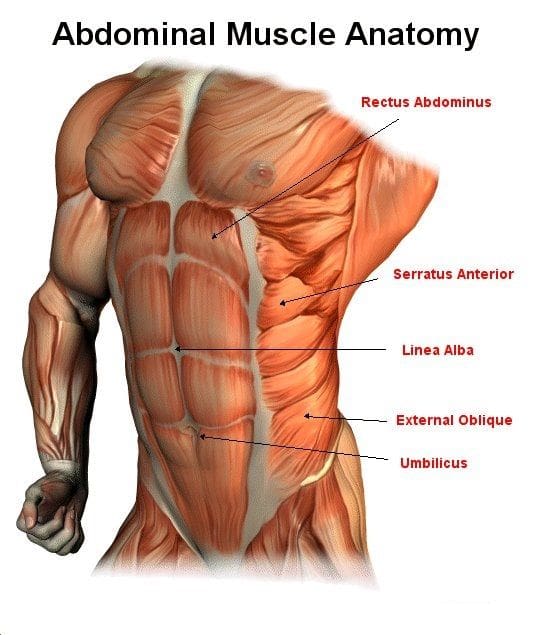
Do you have trouble moving around? Have you been dealing with muscle spasms along your abdomen? Does it hurt when you are sneezing, laughing, or coughing constantly? All these actions affecting your abdominal muscles might correlate with trigger points along the muscles and disrupt the torso area. The abdomen in the body has various muscles, a complex organ with many functions that contribute to a person’s quality of life. The abdominal muscles have many important parts, from supporting the trunk, allowing movement like twisting and turning, and holding the organs in the gut system in place through internal abdominal pressure regulation. The abdominal muscles have five main muscles that work together with the back muscles to keep body stability. They are:
Pyramidalis
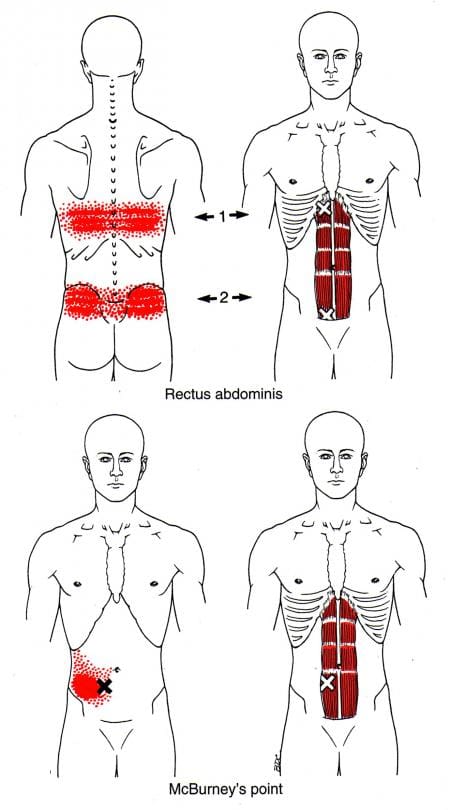
Rectus Abdominus
External Obliques
Internal Obliques
Transversus Abdominis
Studies reveal that the abdominal muscles can help increase the stability of the lumbar region of the body from the vertebral columns by tending the thoracolumbar fascia and raising the intra-abdominal pressure. This allows the abdominal muscle to bend and flex in different positions without feeling pain. However, overusing the abdominal muscles can lead to unnecessary issues that can affect not only the torso but the surrounding muscles around the torso.
How Trigger Points Are Affecting The Abdomen
The book “Myofascial Pain and Dysfunction,” by Dr. Janet Travell, M.D., mentioned that abdominal symptoms are common and can cause diagnostic confusion for many people. Since the abdominal muscles can provide stability to the body’s trunk when a person overuses the abdominal muscles through various activities like quick and violent twisting of the mid-section, lifting heavy objects with the core instead of the legs, overdoing exercise regimes, or having a persistent cough, these various activities could potentially lead to the development of trigger points in the abdominal muscles causing pain in the abdomen and causing referred pain to the lower back. Studies reveal that trigger points along the abdominal muscles are developed through aggravating factors like prolonged sitting or standing can cause the abdominal muscles to become extremely tender and hyperirritable along the taut muscle bands. When trigger points affect the abdominal muscles, they can produce referred abdominal pain and visceral disorders (somato-visceral effects) that work closely together to mimic visceral diseases. This pertains to many individuals thinking something is wrong in their gut system, but their abdominal muscles are causing issues in their bodies.
Releasing Trigger Points In The Abdominal Muscles-Video
Have you been experiencing abdominal issues around your torso? Does it hurt when you laugh, cough, or sneeze? Do you feel muscle stiffness or tenderness along your abdominals? If you have been dealing with these symptoms throughout your life, you could be experiencing abdominal pain associated with trigger points in your torso. Abdominal pain is common for many individuals and can vary from gut issues or muscle issues that various factors can cause in the torso. Abdominal issues can even cause confusion to doctors when they are diagnosing the issues that are affecting their patients. When various actions cause pain to the abdominals, it can develop referred pain associated with trigger points. Trigger points develop when the muscle has been overused, creating tiny nodules in the taut band. Trigger points can be tricky to pinpoint but are treatable. The video above shows where the trigger points are located in the abdominal muscles and how to release them from the affected abdominal muscles to provide relief and reduce the mimic effects of visceral-somatic pain.
Managing Trigger Points Associated With Abdominal Pain Through Various Treatments
When abdominal pain affects the muscles, the symptoms can develop trigger points. When this happens, it can lead to confusion and often misdiagnosed. All is not lost; there are ways to manage trigger points associated with abdominal pain through various treatments. Studies reveal that various therapies like dry needling combined with palpations can reduce trigger points from causing more referred pain issues in the abdomen. Other ways to prevent trigger points from developing in the future are through exercises that can help strengthen the abdominal muscles. Exercises like abdominal breathing, pelvic tilts, sit-ups, and even laughter can help strengthen weak abdominal muscles and positively affect the body.
Conclusion
The torso has various muscles, known as abdominal muscles, that help protect the vital organs in the gut system, help stabilize the spinal column, and maintain good posture for many individuals. Various factors affecting the abdominal muscles can lead to a confusing diagnosis, as it could be an internal or external issue. When the abdominal muscles are affected by being overused through various activities, it can develop into trigger points in the muscles, causing visceral referred pain to the torso and cause muscle weakness. Luckily multiple treatments can help reduce the effects of trigger points associated with abdominal pain and can help strengthen the core of the body. This allows the individual to feel better and consider what not to do to their abdominals.
References
Balyan, Rohit, et al. “Abdominal Wall Myofascial Pain: Still an Unrecognized Clinical Entity.” The Korean Journal of Pain, The Korean Pain Society, Oct. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5665744/.
Rajkannan, Pandurangan, and Rajagopalan Vijayaraghavan. “Dry Needling in Chronic Abdominal Wall Pain of Uncertain Origin.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, Jan. 2019, https://pubmed.ncbi.nlm.nih.gov/30691770/.
Seeras, Kevin, et al. “Anatomy, Abdomen and Pelvis, Anterolateral Abdominal Wall.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK525975/.
Tesh, K M, et al. “The Abdominal Muscles and Vertebral Stability.” Spine, U.S. National Library of Medicine, June 1987, https://pubmed.ncbi.nlm.nih.gov/2957802/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
Many individuals don’t realize that the various muscles in their back help provide functionality to the body. The back muscles help move, bend, rotate, and help the individual stand up straight when they are out and about. The back muscles also help protect the cervical, thoracic, and lumbar sections of the spine and work together with the head, neck, shoulders, arms, and legs to provide mobility. When the body begins to wear down with age naturally, it can lead to back issues that can limit a person’s mobility, or normal activities can cause the back muscles to be overused and develop trigger points to invoke back pain or lumbago. Today’s article looks at the thoracolumbar paraspinal muscles in the back, how the lumbago is associated with trigger points, and treatments to relieve the lumbago in the thoracolumbar muscles. We refer patients to certified providers who provide different techniques in thoracic lumbar back pain therapies associated with trigger points to aid many suffering from pain-like symptoms along the thoracolumbar paraspinal muscles along the back, causing lumbago. We encourage patients by referring them to our associated medical providers based on their examination when it is appropriate. We designate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
The Thoracolumbar Paraspinal Muscles In The Back
Have you been finding it difficult to walk even for a short period? Do you feel aches and soreness when getting out of bed? Are you constantly in pain when bending over to pick up items from the ground? These various actions that you are doing incorporate the thoracolumbar paraspinal muscle in the back, and when issues affect these muscles, it can lead to lumbago associated with trigger points. The thoracolumbar paraspinal in the back is a group of muscles closely surrounded by the thoracolumbar spine, where the thoracic region ends, and the lumbar region begins. The thoracolumbar paraspinal muscles in the back have a casual relationship with the body as it requires contribution from the systems requiring movement. Studies reveal that the thoracolumbar paraspinal muscles are modulated through communication with the three sub-systems, which include:
The passive system: vertebrae, discs, and ligaments
The active system: muscles and tendons
The control system: central nervous system and nerves
Each system provides muscular activities when a person is bending down to pick up an object or doing simple movements. However, when the muscles become overused, it can lead to various issues affecting the back and surrounding muscles.
Lumbago Associated With Trigger Points
Studies reveal that paraspinal muscle integrity plays a very critical role when it comes to the maintenance of spinal alignment in the back. When the thoracolumbar paraspinal muscles become overused from normal activities, it can affect the back by causing back pain symptoms or lumbago associated with trigger points. In Dr. Travell, M.D.’s book “Myofascial Pain and Dysfunction,” trigger points may be activated due to sudden movements or sustained muscular contraction over time that leads to the development of lumbago. Atrophy issues in the paraspinal muscles can contribute to lumbago associated with trigger points that cause deep referred pain in the thoracolumbar regions of the back. Active trigger points in the deep muscle group of the thoracolumbar paraspinal can impair movement between the vertebrae during flexion or side bending.
An Overview Of Lumbago- Video
Lumbago or back pain is one of the most common issues that many individuals, from acute to chronic, depending on how severe the pain is inflicted on the back. Have you been feeling pain in your mid-lower back? Do you feel an electric shock when you run down your leg in a weird position? Or have you felt tenderness in the middle of your back? Experiencing these symptoms could indicate that the thoracolumbar paraspinal muscles are affected by trigger points associated with lumbago. The video explains what lumbago is, the symptoms, and various treatment options to relieve the pain and manage trigger points that are causing the thoracolumbar muscles issues in the back. Many individuals who suffer from lumbago don’t often realize that various factors can affect the surrounding muscles in the thoracolumbar region and mask other previous conditions from which they could suffer. Regarding managing lumbago associated with trigger points, various treatment options can help reduce the pain affecting the thoracolumbar paraspinal muscles while managing trigger points for progressing further in the back.
Treatments To Relieve Lumbago In The Thoracolumbar Muscles
Since lumbago or back pain is a common issue for many people, various treatments can reduce the pain-like symptoms in the thoracolumbar muscles and manage the associated trigger points. Some of the simplest treatments that many individuals can use are to correct how they are standing. Many individuals often lean on one side of their bodies which causes the thoracolumbar paraspinal muscles on the opposite sides to be overloaded. This causes spinal subluxation or misalignment to the thoracolumbar region. Another treatment that many people can incorporate into their daily lives is by going to a chiropractor for a spinal adjustment for the thoracolumbar spine. Studies reveal that chiropractic care combined with physical therapy can relieve the thoracolumbar back while reducing the pain symptoms associated with trigger points by loosening the stiff muscles and causing relief to the back.
Conclusion
The back has various muscles known as the thoracolumbar paraspinal muscles that allow movement and mobility to the body. The back muscles help protect the cervical, thoracic, and lumbar sections of the spine while working with the rest of the body’s components to keep the body stable. When natural aging or actions affect the back muscles, it can lead to various pain issues that can activate trigger points causing lumbago or back pain. Fortunately, some treatments can help alleviate back pain in the thoracolumbar paraspinal muscles while managing trigger points to bring back mobility to the back.
References
Bell, Daniel J. “Paraspinal Muscles: Radiology Reference Article.” Radiopaedia Blog RSS, Radiopaedia.org, 10 July 2021, https://radiopaedia.org/articles/paraspinal-muscles?lang=us.
du Rose, Alister, and Alan Breen. “Relationships between Paraspinal Muscle Activity and Lumbar Inter-Vertebral Range of Motion.” Healthcare (Basel, Switzerland), MDPI, 5 Jan. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4934538/.
He, Kevin, et al. “The Implications of Paraspinal Muscle Atrophy in Low Back Pain, Thoracolumbar Pathology, and Clinical Outcomes after Spine Surgery: A Review of the Literature.” Global Spine Journal, SAGE Publications, Aug. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7359686/.
Khodakarami, Nima. “Treatment of Patients with Low Back Pain: A Comparison of Physical Therapy and Chiropractic Manipulation.” Healthcare (Basel, Switzerland), MDPI, 24 Feb. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7151187/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine