Speeding and Aggressive Driving Motor Vehicle Accidents: Causes, Dangers, and How Integrative Care Supports Recovery
Speeding and aggressive driving cause thousands of serious crashes every year. These collisions occur when drivers ignore traffic laws, putting other people’s safety at risk. The results often include painful injuries to the neck, back, and spine that can last for months or years if not treated properly.
This article explains what these dangerous behaviors are, why they happen, and the real risks they create. It also shows how integrative chiropractic clinics use a team approach to help people heal from the physical damage these crashes cause. Understanding the problem is the first step. Knowing your recovery options is next.
What Are Speeding and Aggressive Driving?
These terms describe different but related problems on the road.
Speeding means driving faster than the posted speed limit or faster than conditions safely allow. This includes going too fast in heavy rain, at night, or on wet roads. Nearly one in three traffic deaths across the country involves speeding. It remains one of the most common and deadly driving mistakes.
Aggressive driving is a pattern of moving violations that endanger other drivers or property. The National Highway Traffic Safety Administration describes it as a combination of two or more risky actions, such as tailgating, improper passing, running red lights, or weaving through traffic. These behaviors show a clear disregard for the rules and for other people’s safety.
Road rage is different. While aggressive driving is a traffic violation, road rage involves intentional violent acts with a vehicle or weapon. It often starts from a traffic dispute but turns into a criminal assault. Examples include ramming another car or forcing someone off the road.
Why Do These Crashes Happen?
Most people do not plan to drive dangerously. Several common factors push drivers into these behaviors:
Feeling rushed or late for work, appointments, or family obligations
Frustration from sitting in traffic congestion
The feeling of being anonymous inside a vehicle, which can lower normal social inhibitions
Stress from daily life that spills over into driving
Traffic jams are a major trigger. Drivers may make sudden lane changes or accelerate to pass slower vehicles, creating dangerous situations for everyone nearby.
When these actions combine with high speed, reaction time drops sharply. A driver going much faster than surrounding traffic has far less time to stop or steer away from trouble.
The Real Hazards of Speed and Aggression
Higher speeds make crashes much more severe. The chance of dying or suffering serious injury rises quickly as speed increases. Research shows this risk can double for every 10 miles per hour over 50 mph. At higher speeds, the force of impact grows dramatically, and safety features like guardrails and seat belts become less effective at protecting people.
Aggressive moves such as tailgating and erratic lane changes further reduce the time everyone has to react. These crashes often produce stronger forces on the body, leading to more serious damage to muscles, ligaments, discs, and nerves.
In Texas and across the country, officials track these behaviors because they contribute to a large share of serious injury and fatal crashes. Resources from the Texas Department of Insurance and the Governors Highway Safety Association offer practical tips for staying safe and reporting dangerous drivers.
Common Injuries After Speeding and Aggressive Driving Crashes
High-impact collisions frequently cause:
Whiplash and neck strain
Herniated or bulging discs in the spine
Soft tissue damage to muscles, tendons, and ligaments
Pinched nerves that send pain, numbness, or tingling into the arms or legs
Joint injuries in the shoulders, hips, or back
These injuries can feel minor at first but often worsen over days or weeks. Without proper care, scar tissue can form, leading to long-term stiffness, chronic pain, and reduced mobility.
How Integrative Chiropractic Clinics Support Healing
Integrative clinics focus on restoring the body’s natural function rather than masking symptoms. They combine structural care with advanced tissue repair therapies. This approach helps people recover from the specific trauma caused by high-speed and aggressive driving crashes.
At Injury Medical Clinic PA (also known as El Paso Back Clinic) in El Paso, Texas, care is built around a multidisciplinary model. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, brings more than 30 years of experience treating thousands of patients with neck, back, and soft-tissue injuries resulting from car accidents. His clinical observations show that combining precise chiropractic adjustments with regenerative and rehabilitative therapies often helps patients regain mobility and reduce pain while lowering the chance of long-term problems.
Dr. Maria Guadalupe Cardenas, MD, a board-certified internal medicine physician with over 40 years of experience (NPI #1164426749, Texas MD License #J2933), serves as Medical Director and Collaborative Physician. She provides medical oversight for the entire care team. This setup is common in integrative injury clinics. The MD ensures that treatments are safe for patients with other health conditions, while the chiropractor focuses on alignment and nervous system function. Together with functional medicine, personal injury documentation, and rehabilitation services, the team creates personalized plans that address both the immediate injury and the whole person.
Specific Therapies Used for High-Impact Accident Recovery
Clinics like this one use several proven methods together:
Spinal Decompression gently creates negative pressure in the spine. This helps relieve pressure on compressed discs and pinched nerves in the neck and back, easing both local and radiating pain.
MLS Laser Therapy uses specific wavelengths of light to support cellular repair. It can reduce inflammation and calm damaged soft tissues without surgery or drugs.
Shockwave Therapy delivers deep acoustic waves to injured muscles and tendons. It helps break up painful scar tissue and encourages fresh blood flow to the area, speeding the body’s natural repair process.
Regenerative Therapies (PRP, PFP, and MFAT) use the patient’s own healing elements. Platelet-Rich Plasma (PRP) and Platelet-Poor Plasma (PFP) concentrate growth factors from blood to support ligament and tendon repair. Micro-Fragmented Adipose Tissue (MFAT) uses processed fat tissue to provide cushioning and healing signals to damaged joints. These treatments are especially beneficial after the forceful impacts common in speeding-related crashes.
Epidural Spinal Injections, administered under direct medical supervision, deliver anti-inflammatory medication to the area around irritated nerves. They can calm severe spinal inflammation when other steps need extra support.
IV Infusion Therapy delivers hydration, vitamins, and minerals straight into the bloodstream. This supports the body’s internal healing environment and helps combat the fatigue that often follows major trauma.
Chiropractic Care uses targeted manual adjustments to restore proper joint movement, ease nervous system stress, and improve range of motion. It forms the foundation for structural recovery.
When these therapies work together under coordinated medical and chiropractic oversight, many patients experience faster relief and better long-term function.
Why a Team Approach Matters
Recovering from injuries caused by speeding or aggressive drivers is rarely simple. Pain in one area can affect posture, sleep, and daily movement. An integrated team addresses these connections.
Dr. Cardenas’s medical direction helps guide care for patients with complex health histories. Dr. Jimenez’s dual training as a chiropractor and nurse practitioner allows seamless blending of structural correction with functional and rehabilitative strategies. The result is care that treats the whole injury, not just the painful spot. Early intervention is especially important because it can limit scar tissue formation and help prevent chronic pain patterns.
Staying Safe and Starting Recovery
Prevention remains the best protection. Simple habits help: leave extra space in front of your vehicle, avoid tailgating, use turn signals, and manage stress before getting behind the wheel. If another driver acts aggressively, do not engage. Stay calm, keep distance, and report serious threats to authorities when it is safe.
If you have already been in a crash involving speeding or aggressive driving, even a “minor” one, get evaluated promptly. Delayed symptoms are common with whiplash and spinal injuries. A thorough assessment can catch problems before they become harder to treat.
Integrative clinics in El Paso and similar communities offer coordinated care that combines chiropractic precision, regenerative support, and medical oversight. This approach gives many people a clearer path back to comfortable movement and daily life.
Car Accident Shoulder and Arm Injury Care in El Paso
Motor vehicle accidents happen suddenly and can have a lasting impact on your body. Seatbelts save lives, but the forces involved often cause arm and shoulder injuries. These problems range from strains that heal with time to more serious tears that affect work, sleep, and daily activities. At El Paso Back Clinic, patients receive caring, complete support to address these injuries and get back to feeling like themselves.
This guide explains common arm and shoulder injuries from car crashes, why they occur, which symptoms to watch for, and how an integrative approach can help with healing. The focus is on clear, practical steps for recovery right here in El Paso.
How Car Accidents Lead to Shoulder and Arm Problems
In a crash, your body stops or changes direction rapidly. Seatbelts hold you in place but can press hard across the shoulder. Your arms may hit the steering wheel, dashboard, or door. Bracing for impact by gripping the wheel tightly adds strain. Even whiplash from the neck can send pain into the shoulders and arms.
Main causes include:
Direct impact from inside the vehicle.
Seatbelt restraint pulling on the shoulder.
Sudden jarring or twisting motions.
Airbag deployment or bracing reactions.
The shoulder is a complex ball-and-socket joint. It allows a wide range of motion but becomes vulnerable in accidents. At El Paso Back Clinic, experts understand these patterns and create personalized plans for El Paso residents and visitors.
Common Types of Injuries After a Crash
A diverse array of arm and shoulder injuries results from auto accident trauma. The precise nature of the harm depends on how the body is jolted and where impact occurs.
Rotator Cuff Tears: These involve the muscles and tendons that stabilize the shoulder. Tears cause pain when lifting the arm, weakness, and nighttime discomfort. Partial or full tears are common in crashes.
Fractures: The collarbone, upper arm bone, or shoulder blade can break. Symptoms include sharp pain, swelling, and trouble moving the arm. Proper imaging and care are essential.
Dislocations and Instability: The upper arm bone may shift out of the socket. This leads to severe pain and limited motion. Follow-up care prevents future problems.
Sprains, Strains, and Soft Tissue Damage: Ligaments, muscles, and tendons can stretch or tear. Bruising and inflammation add to the pain. Nerve irritation may cause numbness or tingling down the arm.
Early diagnosis at a local clinic like El Paso Back Clinic helps prevent small issues from becoming long-term problems.
Symptoms That Should Not Be Ignored
Pain might not show up immediately due to the body’s stress response. Delayed symptoms are very common.
Typical warning signs:
Aching or sharp pain in the shoulder or upper arm.
Weakness or difficulty raising the arm.
Swelling, bruising, or stiffness.
Clicking or grinding feelings during movement.
Pain that worsens at night or with overhead activities.
Numbness or tingling in the arm or hand.
If these appear after an accident, seek evaluation soon. Prompt care supports better healing and stronger documentation for insurance or personal injury needs.
Comprehensive Care at El Paso Back Clinic
Motor vehicle accidents frequently result in arm and shoulder trauma. These collisions can lead to debilitating pain that needs multifaceted treatment. El Paso Back Clinic offers a full continuum of care by blending chiropractic adjustments with advanced regenerative and supportive therapies.
Chiropractic Adjustments: Gentle, precise movements realign the spine and joints. This reduces pressure on nerves, eases muscle tension, and improves overall mobility—key for accident recovery.
Regenerative and Advanced Therapies
Platelet-Rich Plasma (PRP), Platelet-Fibrin Products (PFP), and Microfragmented Adipose Tissue (MFAT) use the body’s own materials to promote natural repair.
Shockwave therapy, MLS laser therapy, spinal decompression, Graston technique, and cupping reduce inflammation and support tissue healing.
IV infusion therapies deliver nutrients to speed recovery.
Targeted injections and physical rehabilitation rebuild strength and function.
This integrative model works well for personal injury cases common in El Paso, including whiplash, work-related issues, and auto accidents.
Collaborative Medical Leadership in El Paso
At Injury Medical Clinic PA / El Paso Back Clinic, care is provided by a coordinated team. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CCST, CFMP, IFMCP, ATN, leads with deep experience in chiropractic and advanced practice. His clinical insights emphasize whole-person recovery that addresses root causes rather than just symptoms.
Dr. Maria Guadalupe Cardenas, MD (Board Certified in Internal Medicine, NPI #1164426749, Texas MD License #J2933), with over 40 years of experience, serves as Medical Director and Collaborative Physician. This multidisciplinary setup is standard in quality integrative clinics. The MD provides medical oversight and internal medicine expertise, while chiropractic and regenerative services focus on alignment, repair, and rehabilitation. The team also supports functional medicine, personal injury documentation, and tailored rehab plans for patients in El Paso.
Patients benefit from convenient, comprehensive care at one location in El Paso, Texas—reducing the need to visit multiple offices.
Steps Toward Better Recovery
Healing takes patience, but the right support makes it achievable. Many people at El Paso Back Clinic regain strength and comfort through consistent care.
Practical tips for recovery:
Follow your personalized treatment plan.
Do recommended home exercises to maintain progress.
Use ice or heat as advised for pain and swelling.
Eat nutrient-rich foods and stay hydrated.
Communicate openly with your care team about progress or concerns.
Whether your injury is recent or lingering from an older crash, integrative options can help when standard approaches plateau.
Moving Forward After an Accident in El Paso
Shoulder and arm injuries from car accidents are common but manageable with expert help. El Paso Back Clinic combines proven chiropractic methods with modern regenerative therapies to support cellular repair, relieve pain, and restore function.
If you or someone you know is dealing with post-accident shoulder or arm pain, reach out to the team at El Paso Back Clinic. Their experienced staff understands local needs and focuses on getting patients back to the activities they love. Early action often leads to the best outcomes.
Contact El Paso Back Clinic today to schedule an evaluation and start your personalized recovery journey.
Hip Injuries in Motor Vehicle Accidents: Understanding the Trauma and Finding Healing
Car accidents send powerful forces through the body in seconds. The hips often absorb much of that energy because they connect the legs to the pelvis and spine. Even when the crash does not look severe, hip injuries can appear right away or develop days later. These injuries range from bone fractures and dislocations to tears in soft tissues such as cartilage and muscle.
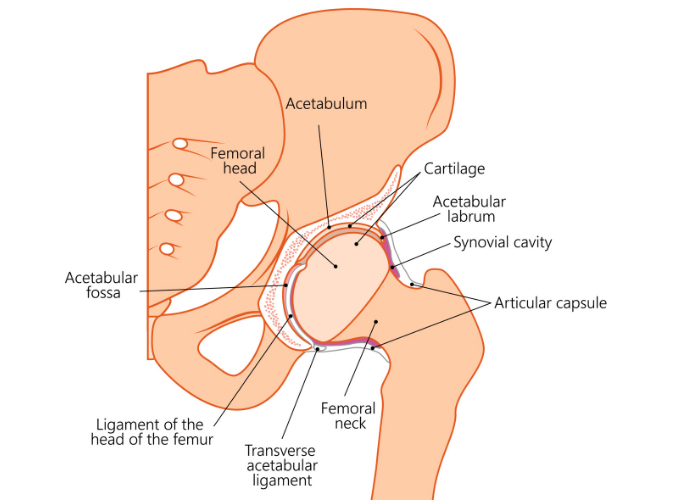
The hip works as a ball-and-socket joint. The ball is the rounded top of the thigh bone. The socket is a deep cup in the pelvis. Strong ligaments and muscles, along with a ring of special cartilage called the labrum, keep the joint stable and smooth. It takes considerable force to damage this sturdy setup. That is why hip problems after a crash are often serious and need careful attention.
Understanding what can happen helps you know when to seek care and what options are available for recovery.
Common Hip Injuries from Motor Vehicle Accidents
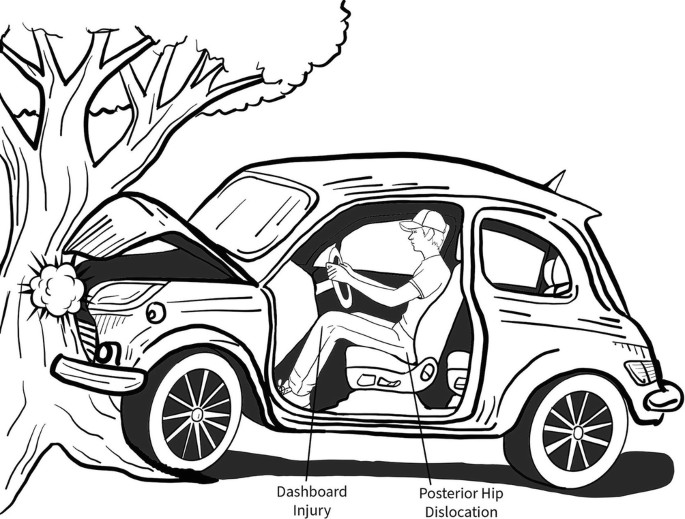
The exact injury often depends on body position at impact. Legs braced, knees hitting the dashboard, or side forces from a T-bone crash all create different patterns of damage.
A classic dashboard injury happens in head-on crashes. The knee slams forward into the dashboard. This drives the thigh bone backward and pops the ball out of the socket. This is called a posterior hip dislocation. It causes immediate, severe pain. The leg may look shorter or rotated. You usually cannot put weight on it (American Academy of Orthopaedic Surgeons, n.d.).
Quick medical help is needed to put the joint back in place. Even after reduction, the labrum, ligaments, or blood supply to the ball can be damaged. Some people later face arthritis or bone death in the ball if blood flow is interrupted.
Acetabular Fractures
The socket itself can crack or shatter. High-energy dashboard hits or side impacts drive the ball forcefully into the cup. These breaks change the smooth surface the ball glides on. Many need surgery to restore the socket shape so the joint moves correctly again (OrthoInfo – AAOS, n.d.).
Femoral Head Fractures
The ball on top of the thigh bone can crack, crush, or break into pieces. This often occurs with a dislocation from the same dashboard force. The ball shears against the socket rim as it pops out or gets driven back in. These injuries raise the risk of long-term joint problems.
Labral Tears
The labrum is the cartilage rim that deepens the socket and helps seal joint fluid. A sudden dislocation, twist, or even strong bracing against the floor or seatbelt can tear it. People experience groin pain, clicking or catching, or a sensation that the hip gives way. Pain often worsens with sitting, walking, or twisting (Mayo Clinic, n.d.).
Muscle Strains, Sprains, and Soft Tissue Damage
Not every injury breaks a bone. Violent jerking or bracing can strain the hip flexor muscles or sprain ligaments around the joint. Seatbelt pressure or direct impact can inflame the bursa (a fluid-filled sac) on the side of the hip, causing trochanteric bursitis. These bring pain with movement, swelling, stiffness, and weakness. They heal more slowly when walking patterns are avoided due to pain (High Mountain Orthopedics, n.d.).
Why These Injuries Matter Long-Term
The hip joint is deep and well-protected, but damage here can affect walking, standing, and balance. Untreated dislocations or fractures can lead to arthritis years later. Labral tears and chronic muscle imbalance change how you move and stress the low back, knees, and opposite hip. Early care reduces these risks.
Doctors diagnose with physical exams plus imaging. X-rays show bone position and breaks. CT scans give detailed fracture pictures. MRI reveals labral tears, muscle damage, and soft tissue injury.
How Integrative Chiropractic Care Supports Recovery
Many hip injuries, especially soft-tissue and labral problems, or those requiring support after initial bone care, respond well to non-surgical approaches. An integrative chiropractic clinic combines hands-on structural work with regenerative therapies that use your body’s own healing tools. The goal is to reduce inflammation, repair tissue, and restore smooth movement without surgery when possible.
Chiropractic adjustments gently realign the pelvis, spine, and hip. This improves joint motion, eases tight muscles, and reduces nerve irritation. Better alignment helps blood flow and healing signals reach the injured area more effectively.
Regenerative therapies add biological support:
PRP (Platelet-Rich Plasma): A small amount of your blood is spun to concentrate platelets rich in growth factors. The concentrate is injected into the hip area to signal repair in tendons, ligaments, the labrum, and cartilage while calming inflammation.
PFP (Platelet-Fibrin Products): Similar to PRP but includes fibrin for slower, longer release of healing factors. This gives sustained support during recovery.
MFAT (Microfragmented Adipose Tissue): A tiny amount of your fat tissue is processed into micro pieces containing healing cells and natural cushioning material. It is injected to support regeneration and provide padding in the joint or around damaged tissues.
These injections are often guided by ultrasound for accuracy. When paired with chiropractic adjustments, they address both structure and biology. Adjustments keep the joint moving correctly so new tissue forms in the right pattern. Regenerative support reduces pain and swelling, so adjustments work better and last longer (Health Coach Clinic, n.d.).
Patients often notice gradual improvement over weeks as tissues rebuild. Many regain mobility and return to daily activities with less pain and lower risk of future problems.
The Collaborative Care Team
At Injury Medical Clinic PA in El Paso, Texas, care is built on teamwork. Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, brings extensive experience treating personal injury and motor vehicle accident cases. His clinical observations show that patients with hip trauma from crashes often achieve better long-term function and less chronic pain when structural corrections and regenerative support are started early. He focuses on whole-person recovery, including rehabilitation exercises and addressing posture or gait changes that develop after an accident.
Dr. Maria Guadalupe Cardenas, MD, board-certified in Internal Medicine with more than 40 years of experience, serves as Medical Director and Collaborative Physician. She provides medical oversight for the practice. This includes reviewing complex cases, ensuring safety for regenerative procedures and injections, managing any underlying medical factors that affect healing, and collaborating on care plans. This MD-DC partnership is common in quality integrative and injury clinics. It combines precise medical direction with specialized chiropractic and regenerative expertise.
The broader team integrates functional medicine, rehabilitation, and personal injury support. This multidisciplinary setup helps patients heal thoroughly by addressing root causes rather than only symptoms.
What to Expect on the Road to Healing
Recovery time depends on the type and severity of the injury. Simple strains may improve in a few weeks with adjustments and guided movement. Labral tears or post-reduction care often take several months. Regenerative injections typically show progressive benefits over 4 to 12 weeks. The focus stays on restoring comfortable movement, strength, and daily function.
Early attention matters. Waiting can allow scar tissue or changed movement patterns to set in, making later recovery harder. A thorough evaluation helps create a clear plan tailored to your injury and goals.
Moving Forward After a Crash
Hip injuries from motor vehicle accidents do not have to mean ongoing pain or major surgery. Many people regain good function through integrative care that works with the body’s natural healing abilities—proper alignment, regenerative signals from your tissues, and expert guidance every step of the way.
If hip pain continues after a car accident, consider a clinic experienced in these injuries and equipped with both structural and regenerative options. In El Paso, the team at Injury Medical Clinic PA provides this comprehensive approach. Knowing what happened to your hip is the first step toward restoring your mobility and quality of life.
El Paso’s Integrated Injury Clinic: One-Stop Care for Faster Recovery and Strong Legal Support
If you got hurt in a car crash or at work in El Paso, Texas, you know how frustrating it can be. You go to one place for an exam, another for therapy, and still another for special treatments. Papers get lost. Your story gets told many times. Healing slows down. An integrated, multidisciplinary injury clinic solves this problem. Everything happens under one roof. A team of experts works together on your care. They handle medical checks, hands-on therapy, and advanced healing methods. At the same time, they build clear, complete records that help your legal or workers’ compensation case.
This kind of care is different from going to separate offices. You get faster answers, smoother progress, and stronger support for your claim.
Why an Integrated Health System Works Better
Ordinary clinics often focus on one thing. You might get only adjustments or only medications. An integrated clinic brings many experts together in the same place. They share one plan for you. This stops gaps in care and mixed messages.
Here are the main advantages:
One team, one story: Every provider sees your full history and current progress. No one works in the dark.
Faster decisions: If you need a new test or different therapy, the group talks it over quickly.
Better healing: Treatments work in tandem. Chiropractic care improves movement while medical oversight watches your overall health.
Clear records from day one: Everything gets written down in one system. This matters a lot for insurance and legal needs.
Patients who use this model often feel less stressed. They spend less time driving between offices and more time actually getting better.
How the Team Works Together for You
In a true multidisciplinary setup, each expert brings their skills. Nurse practitioners handle full health evaluations. They can order tests, manage medications as needed, and monitor for other health issues that might slow healing.
Physical therapists, massage therapists, and chiropractors team up on your body’s movement. They improve flexibility, strength, and posture. Chiropractic adjustments help the spine and joints work better. Physical therapy builds safe exercises. Massage eases tight muscles. Together, they create a plan that fits your exact injuries.
This is not random care. It is coordinated. Everyone knows what the others are doing. That teamwork often leads to quicker pain relief and better long-term results.
Special Treatments That Help Serious or Lasting Injuries
Some injuries need more than basic care. Car accidents and work injuries can damage deep tissues, nerves, or joints. An integrated clinic offers modern options that directly target the problem.
Here are treatments often used together:
Spinal decompression: A special table gently stretches your spine. This takes pressure off pinched nerves and bulging discs. Many people feel relief from sciatica or radiating leg pain.
MLS laser and shockwave therapy: These use light or sound waves to wake up your body’s healing cells. They lower swelling and help soft tissues repair without drugs or surgery.
Epidural injections: When nerves are very irritated, guided injections can calm the area so you can move and heal.
Regenerative therapies: Treatments such as PRP (platelet-rich plasma), PRF (platelet-rich fibrin), and MFAT (micro-fragmented adipose tissue) use components of your blood or fat. They are placed exactly where tissue is damaged to support natural repair.
These options go beyond what a basic clinic usually offers. They aim at the root of the injury rather than merely masking pain.
Strong Medical-Legal Documentation That Protects Your Case
When your injury comes from a car accident or a job, good records are just as important as good treatment. Insurance companies and lawyers need proof. They want to see what happened, how bad it is, and that the care you received was necessary.
An integrated team creates one complete file. It includes:
Your accident story and first exam findings
Objective tests like range of motion, strength checks, and imaging
Daily notes on how you feel and what treatments you receive
Progress reports that show improvement or ongoing limits
A final summary that explains the lasting effects on your life and work
This kind of documentation helps personal injury lawyers build a stronger case. It shows a clear link between the crash or incident and your injuries. It also proves you followed a real treatment plan.
Many clinics work directly with attorneys. They send updates quickly and often handle cases on a lien basis. This means you can focus on healing while the legal side stays organized.
Expert Care Led by Dr. Alex Jimenez and Dr. Maria Guadalupe Cardenas in El Paso
At Injury Medical Clinic PA in El Paso, this integrated model is led by experienced professionals who understand both health and legal needs.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, CCST, CFMP, IFMCP, ATN, is dual-licensed as a chiropractor and board-certified family nurse practitioner. He has spent decades helping people with car accident injuries, work injuries, whiplash, sciatica, and soft tissue damage. His clinical observations focus on treating the whole person. He looks at root causes, not just symptoms. He stresses careful documentation with clear findings and progress measures, especially when a case involves an auto or work injury claim. His practice combines chiropractic care, functional medicine, rehabilitation, and regenerative options under one roof.
Working alongside him is Dr. Maria Guadalupe Cardenas, MD. She is board-certified in internal medicine with over 40 years of experience. Her NPI is 1164426749, and her Texas MD license is J2933. She serves as Medical Director and Collaborative Physician. In this multidisciplinary setting, she provides medical oversight, reviews overall health, guides advanced procedures, and helps ensure compliance with Texas rules.
Together, they create a powerful team. Chiropractic care from Dr. Jimenez addresses alignment, nerves, and movement. Medical direction from Dr. Cardenas provides safety, diagnostic, and medication management as needed. Functional medicine, personal injury documentation, and rehabilitation services all connect in the same location. This is the kind of collaborative model common in high-quality integrative injury clinics.
Your Simple Path to Recovery in El Paso
Here is what the journey usually looks like:
You call or come in for an evaluation. A nurse practitioner or medical director, along with the chiropractic team, sees you together.
They create one clear plan that may include adjustments, therapy, advanced treatments, or regenerative options.
You receive care in one place. Notes stay organized from the first visit to the last.
Progress is tracked and shared with your lawyer or insurance when needed.
You heal with less stress and stronger support for your claim.
Many patients notice they move better sooner and have less confusion about next steps.
Choose Coordinated Care for Your Injury
If you want care that treats your injury and protects your legal position, an integrated multidisciplinary clinic in El Paso is worth considering. You get medical diagnostics, physical therapy, advanced healing therapies, and solid documentation all in one coordinated system. Dr. Alex Jimenez and Dr. Maria Guadalupe Cardenas lead a team that puts your recovery and your case first.
You do not have to piece your care together alone. One roof, one team, one clear plan can make a real difference in how fast you feel better and how well your case is supported.
Regenerative Therapies Combined with Chiropractic Care Offer New Hope for Sports and Auto Accident Injuries in El Paso
Many people in El Paso deal with ongoing pain and limited movement after sports injuries or car accidents. Simple rest or basic physical therapy often helps at first, but sometimes healing stalls. Tissues stay inflamed, joints feel stiff, and daily life or sports become difficult again. When that happens, more people look for advanced options that work with the body instead of just covering up symptoms.
Regenerative therapies and integrative chiropractic care team up to tackle these tough problems. They focus on real repair at the tissue level while also fixing how the body moves. This combined approach helps many patients get back to feeling better and moving easier without jumping straight to surgery.
Why Standard Treatments Sometimes Fall Short
Injuries from sports collisions or car crashes often damage more than one area. Muscles tear, ligaments stretch, tendons become inflamed, and spinal discs or joints become irritated. Swelling and scar tissue can block normal blood flow and healing signals.
Physical therapy and rest build strength and reduce pain for many people. Yet when progress plateaus, underlying tissue damage or poor joint alignment may still be holding back recovery. That is when patients often seek care that actively supports the body’s repair systems instead of only managing symptoms.
What Regenerative Therapies Actually Do
Regenerative medicine uses materials from your body to kick-start healing. These treatments deliver growth factors and helpful cells directly to the damaged area. The goal is to lower inflammation, encourage new tissue growth, and improve long-term function.
Three main options stand out for musculoskeletal and spinal injuries:
PRP (platelet-rich plasma) comes from a small sample of your blood. The blood is spun in a machine to concentrate platelets, which carry natural growth factors. Doctors inject this concentrated solution into tendons, ligaments, joints, or around nerves. The growth factors signal cells to repair and rebuild.
PFP (platelet-fibrin products) uses protein concentrates from your blood. These capture growth factors and create a stronger, longer-lasting healing signal for tissues that have not responded well to simpler treatments.
MFAT (microfragmented adipose tissue) takes a small amount of your own fat tissue, processes it into tiny fragments, and injects it. The fat contains supportive cells and signaling factors that cushion joints and help repair cartilage, tendons, and soft tissues.
These are called orthobiologics because they come from your biology. They carry a low risk of allergic reactions or rejection since they use your materials.
Epidural injections sometimes join the plan for spine-related pain and nerve irritation. Under careful medical guidance, they reduce inflammation around spinal nerves while the regenerative injections work to repair deeper tissue.
How Chiropractic Care Completes the Picture
Injections alone help tissues heal, but they do not fix how the bones, joints, and muscles line up or move. That is where chiropractic adjustments come in. Gentle, precise realignments improve joint mobility, ease muscle tension, and restore better posture and movement patterns.
When regenerative injections and chiropractic care happen together, the results often last longer. The injections create a better healing environment inside the tissues. The adjustments keep the joints moving correctly so that new tissue forms properly and does not get stressed again. This partnership addresses both the biology of repair and the mechanics of the body.
The Strength of a True Multidisciplinary Team
Patients get the best results when they receive care from a well-established integrative and functional medicine clinic that brings different experts together under one roof. At Injury Medical Clinic PA in El Paso, Texas, the team combines advanced regenerative procedures with chiropractic expertise, functional medicine, rehabilitation, and personal injury support.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST, leads the clinical approach. With decades of experience as a chiropractor and additional training as a board-certified family nurse practitioner, he focuses on whole-person recovery. His clinical observations show that patients with sports trauma or old auto accident injuries often improve when care targets both tissue repair and nervous system function. He uses detailed exams, imaging, and personalized plans that include regenerative injections, adjustments, rehabilitation, and lifestyle support.
Dr. Maria Guadalupe Cardenas, MD, a board-certified internal medicine physician with over 40 years of experience (NPI #1164426749, Texas MD License #J2933), serves as Medical Director and Collaborative Physician. She provides medical oversight for procedures, ensures safety and compliance, manages complex health factors, and brings an internal medicine perspective to every case. This collaboration means patients receive both expert spinal and musculoskeletal care from Dr. Jimenez and broad medical direction from Dr. Cardenas.
This setup is common in high-quality integrative injury clinics. The MD handles medical aspects and procedure oversight while the chiropractor and nurse practitioner team deliver hands-on treatment and functional strategies. Everyone works from the same records and goals, so care stays coordinated and thorough.
Clear Benefits Patients Notice
People who choose this combined path often report several practical improvements:
Noticeable drops in pain and swelling without relying only on medications
Better tissue repair that supports longer-lasting results
Improved joint movement and daily function
Faster return to work, sports, or normal activities when healing had stalled
Lower chance of needing more invasive procedures later
Thorough documentation that helps with insurance and legal needs after personal injury cases
Because the treatments use your own biological materials, side effects stay minimal for most people. Soreness at the injection site usually fades within a few days.
The functional medicine side of care looks at nutrition, inflammation levels, sleep, and stress. These factors influence how well tissues heal. Addressing them alongside the injections and adjustments gives the body every advantage.
What a Typical Care Journey Looks Like
Most patients start with a full evaluation that includes history, physical exam, and any needed imaging. The team identifies exactly which tissues need help and whether alignment issues are slowing progress.
Next comes a customized plan. This may include one or more regenerative injections (PRP, PFP, or MFAT), chiropractic adjustments over several weeks, guided rehabilitation exercises, and supportive therapies such as shockwave treatment when appropriate. Follow-up visits track progress and adjust the plan as tissues respond.
Many people begin to feel meaningful relief within weeks, with continued improvement over the next few months as repair progresses. The team stays involved through the entire process.
Who Benefits Most from This Approach
This type of care often helps adults dealing with:
Lingering pain after sports collisions or overuse injuries
Whiplash, back strain, or nerve irritation from car accidents
Old injuries that never fully settled
Joint or tendon problems that limit activity
It works especially well when conventional treatments have already been tried, and progress has slowed. The focus stays on restoring real function rather than temporary relief.
Moving Forward with Confidence
Healing from serious injuries takes time and the right tools. Regenerative therapies give tissues the biological signals they need. Integrative chiropractic care helps the body use those new repairs by improving movement and alignment. When both occur within a coordinated team that includes medical direction, functional medicine, and personal injury expertise, patients often regain greater comfort and capability than they expected.
If you or someone you know in the El Paso area continues to struggle after sports trauma or an auto accident, consider learning more about these combined options. A thorough evaluation at a clinic experienced in both regenerative procedures and chiropractic care can show whether this path fits your situation. Many people find it opens the door to meaningful, lasting improvement.
Dashboard Knee Injury in Motor Vehicle Accidents: PCL Tears, Symptoms, and Integrative Care Options in El Paso
Car accidents often cause injuries that do not show up right away. One common but sometimes overlooked problem is called a dashboard knee injury. This happens when a bent knee slams into the car’s dashboard during a crash. The force violently pushes the shinbone backward. The result can include a torn posterior cruciate ligament (PCL), damage to the kneecap, and problems with the cartilage that cushions the joint.
People in El Paso and nearby areas like Horizon City who have been in motor vehicle accidents sometimes deal with ongoing knee pain, instability, or trouble walking. Understanding what happens and getting the right kind of care can make a big difference in recovery. Integrative clinics that combine medical oversight with chiropractic care and regenerative therapies offer a full approach to healing.
What Happens During a Dashboard Knee Injury
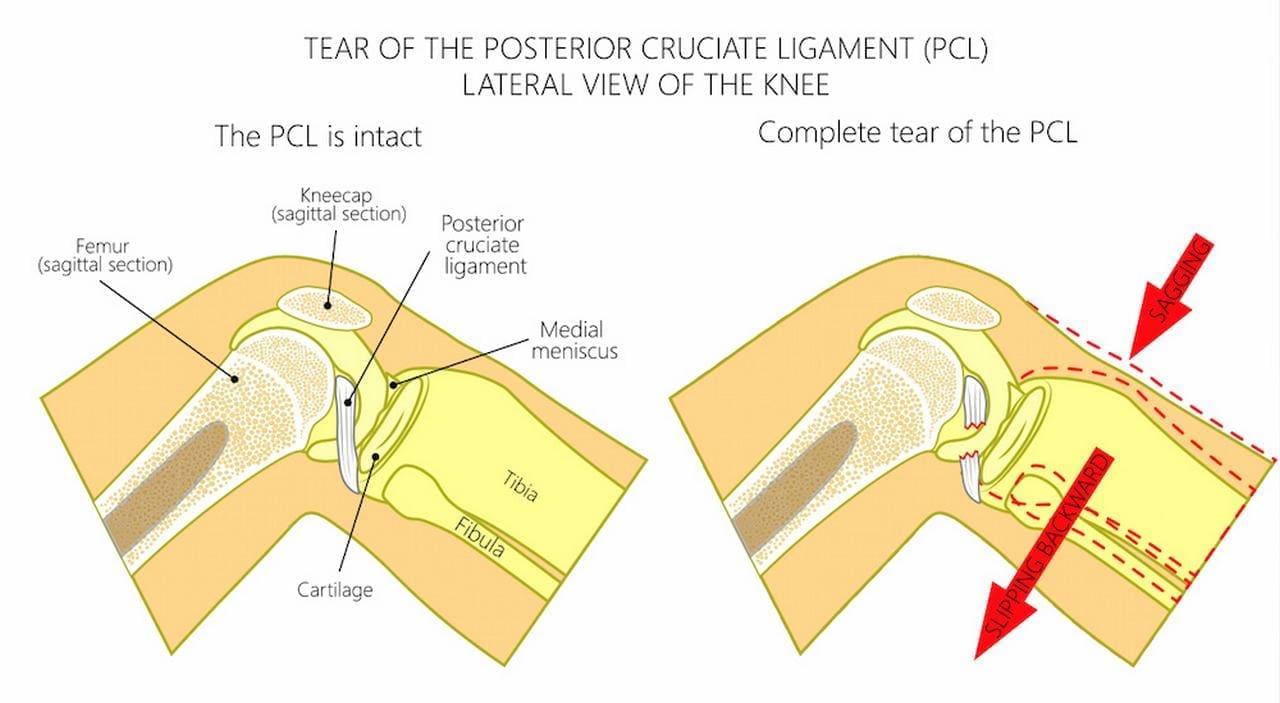
In a front-end collision, your body keeps moving forward even after the car stops. If your knee is bent, it hits the dashboard hard. This drives the top of the shinbone (tibia) backward relative to the thigh bone (femur).
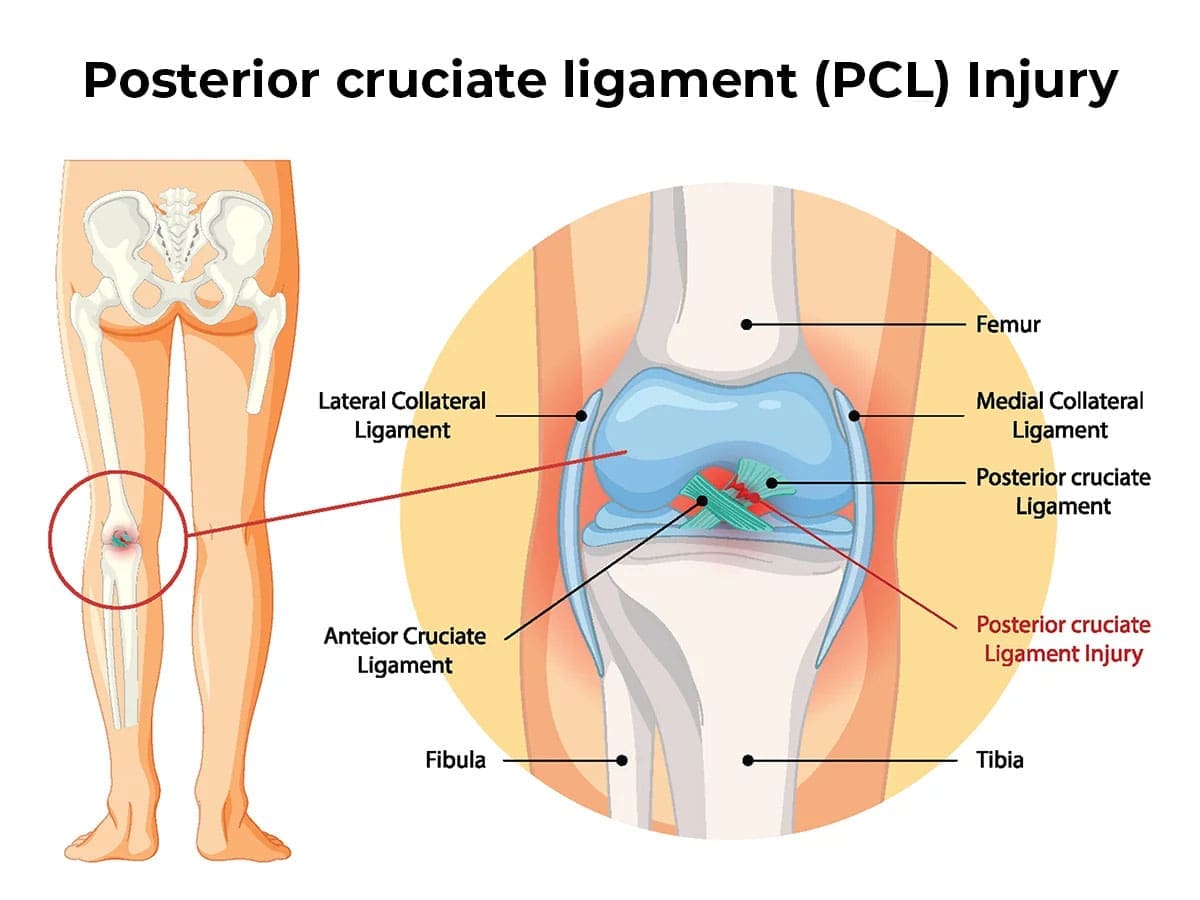
The PCL is a strong band of tissue inside the knee that normally stops the shin from sliding too far back. When the dashboard impact happens, this ligament can stretch, partially tear, or completely rupture. At the same time, the direct blow can fracture the kneecap (patella) or damage the smooth cartilage on the ends of the bones. These injuries often occur together.
The damage does not always feel severe at first. Swelling and pain may appear hours or even days later. That is why some people do not realize the full extent of the injury until they try to return to normal activities.
Common Problems That Come with Dashboard Knee Injuries
Dashboard impacts frequently cause more than one issue inside the knee:
PCL tear or rupture: This is the most common ligament injury from this type of crash. It can make the knee feel loose or unstable, especially when going down stairs, pivoting, or changing direction.
Patellar fractures: The kneecap takes the direct hit and can crack or break. This causes sharp pain in the front of the knee, swelling, and difficulty straightening the leg.
Cartilage damage: The protective covering on the joint surfaces can bruise, tear, or wear down. Untreated cartilage injuries raise the risk of arthritis later in life.
These problems can lead to long-term stiffness, weakness, and difficulty with daily tasks like walking, driving, or working if they are not addressed properly.
Signs and Symptoms to Watch For
After a car accident, pay attention to these possible signs of a dashboard knee injury:
Pain in the front or back of the knee that gets worse with movement
Swelling that may appear immediately or develop over 24–72 hours
A feeling that the knee is unstable or “gives way”
Trouble bending or straightening the knee fully
Pain when walking, climbing stairs, or standing for long periods
Stiffness or locking sensations
Some people notice only mild discomfort at first and assume it will go away. Because early signs can be subtle, many dashboard knee injuries are missed without proper imaging. If you were in a crash and your knee hit the dashboard, it is wise to get checked, even if the pain seems minor.
How Doctors Diagnose These Injuries
X-rays are usually the first step. They can reveal fractures in the kneecap or other bones. However, X-rays do not show ligaments or cartilage well.
An MRI scan is the best tool for detecting PCL tears, cartilage damage, and other soft-tissue injuries. MRI gives detailed pictures that help doctors understand exactly what is torn or bruised. In some cases, doctors also perform physical tests to check knee stability.
Getting the right diagnosis early helps prevent chronic pain and long-term joint problems. Diagnostic challenges exist because swelling can be minimal at first and range of motion may still look normal, which is why imaging is so important.
Standard Treatment Options
Treatment depends on how severe the damage is:
Mild to moderate PCL tears: Doctors often recommend bracing to support the knee, rest, ice, compression, elevation (RICE), anti-inflammatory medication, and physical therapy. Therapy focuses on strengthening the quadriceps and other muscles that support the knee.
Severe tears, fractures, or major cartilage damage: Surgery may be needed to reconstruct the PCL, repair the kneecap, or clean up damaged cartilage. Recovery after surgery usually includes months of physical therapy.
Ongoing rehabilitation: No matter the path, guided exercises help restore strength, balance, and movement.
Healing takes time. Rushing back to normal activities too soon can worsen the injury or lead to new problems in the hips, back, or ankles due to altered walking patterns.
How Integrative Care Supports Better Recovery
Many people benefit from care that goes beyond just the knee. Integrative clinics combine medical doctors, nurse practitioners, chiropractors, and regenerative therapies. This team looks at the whole body and how the injury affects movement, alignment, and healing.
Medical Oversight: A physician or nurse practitioner first assesses all injuries from the accident. They review imaging, identify ligament and cartilage tears, and coordinate any needed medical steps. This oversight ensures nothing is missed, and that care stays safe and appropriate.
Regenerative Injections Clinics may offer injections that use your body’s healing cells. Platelet-rich plasma (PRP) concentrates growth factors from your blood to support torn ligaments and damaged cartilage. PFP (platelet-free plasma) and MFAT (micro-fragmented adipose tissue) are other options that can help tissue repair in areas with limited blood supply. These treatments aim to speed healing and sometimes reduce the need for surgery.
Targeted Tissue Repair: Shockwave therapy uses sound waves to break up scar tissue and stimulate new blood flow and collagen production. MLS laser therapy reduces deep inflammation and encourages cellular repair. Both are non-invasive and can be added to the recovery plan to help tissues heal faster.
Spine and Joint Mechanics: When the knee hurts, people often limp or shift weight. This creates extra stress on the spine, hips, and ankles. Chiropractic adjustments restore proper alignment in these areas. Correcting compensatory movement patterns takes pressure off the healing knee and improves overall function. Many patients notice better knee stability and less pain once the whole lower body moves correctly again.
Dr. Alex Jimenez and Dr. Maria Guadalupe Cardenas: A Collaborative Team in El Paso
At Injury Medical Clinic PA in El Paso, Texas, Dr. Alexander Jimenez, DC, APRN, FNP-BC, provides chiropractic care, functional medicine, regenerative procedures, and personal injury rehabilitation. His clinical observations emphasize that addressing the entire chain of movement—from the spine to the ankles—leads to more complete recovery after car accident injuries, including dashboard knee problems.
Working alongside him is Dr. Maria Guadalupe Cardenas, MD, a board-certified internal medicine physician with over 40 years of experience (NPI #1164426749, Texas MD License #J2933). She serves as Medical Director and Collaborative Physician. In this multidisciplinary setup, Dr. Cardenas provides medical direction, helps evaluate complex cases, and supports the team with internal medicine expertise.
This model blends chiropractic adjustments and rehabilitation (led by Dr. Jimenez) with medical oversight and coordination (led by Dr. Cardenas). Functional medicine principles—looking at inflammation, nutrition, and whole-body factors—are also part of the care. The result is a personalized plan that treats the knee injury while supporting overall healing, especially useful for patients with personal injuries and motor vehicle accidents in the El Paso area.
Local Clinics Offering This Type of Integrated Care
In Horizon City and the broader El Paso region, clinics such as Injury Medical & Chiropractic Clinic and El Paso Chiropractic & Personal Injury Group specialize in medically integrated personal injury rehabilitation. These centers bring together medical oversight, regenerative options, chiropractic adjustments, and rehabilitation in one coordinated approach. Patients receive thorough evaluations, clear explanations of their options, and ongoing support to regain function and return to daily life.
Moving Forward After a Dashboard Knee Injury
Dashboard knee injuries from car accidents can affect your mobility, work, and quality of life. The combination of a PCL tear, possible kneecap fracture, and cartilage damage needs careful attention. Early diagnosis with MRI and a treatment plan that includes medical oversight, regenerative support, tissue repair therapies, and chiropractic alignment often leads to better outcomes than treating the knee in isolation.
If you have knee pain after a motor vehicle accident—especially if your knee hit the dashboard—consider an integrative evaluation. Clinics in El Paso that combine the expertise of physicians like Dr. Maria Guadalupe Cardenas and chiropractors like Dr. Alex Jimenez can guide you through diagnosis, treatment choices, and rehabilitation. With the right team, many people regain strength, stability, and confidence in their movement.
Healing takes patience and the right support. Addressing both the specific knee damage and how the rest of your body compensates provides you the best chance of lasting recovery.
El Paso’s 100 Deadliest Days: Teen Driving Risks and Integrative Recovery at El Paso Back Clinic
Summer in El Paso means more time on the road for young drivers heading to work, friends, or trips across town and beyond. But this season also brings greater danger. The stretch from Memorial Day to Labor Day is known as the 100 Deadliest Days because fatal crashes involving young drivers rise sharply. At El Paso Back Clinic, our team sees the real impact when these accidents happen. Many patients come in weeks later with pain that started small but grew because of how the body reacts to sudden trauma. Learning the risks and knowing the right place for complete recovery helps families in El Paso stay safer and heal better if trouble strikes.
What Are the 100 Deadliest Days?
The 100 Deadliest Days run from Memorial Day through Labor Day, about 100 days when the number of deadly crashes with young drivers jumps across the country and right here in El Paso. National numbers show that more than 30 percent of fatal crashes involving a young driver occur during this summer window. On average, eight people die each day in these crashes in summer compared to seven the rest of the year. In 2023, roughly one-third of the yearly total happened in these months alone.
El Paso faces the same spike plus local challenges. Highways like I-10 and Loop 375, busy streets such as Mesa and Montana, and long summer drives to places like White Sands or Ruidoso pose additional risks for drivers who are still gaining experience.
Why Summer Brings Higher Risks for Young Drivers in El Paso
Several things come together once school lets out and young people drive more on their own.
More driving without close supervision. Extra free time means more trips to jobs or social plans. Young drivers often log miles without an adult nearby to remind them to slow down or stay alert.
Extra passengers create distraction. One or two friends in the car can draw attention away from the road by talking or moving. Texas rules for drivers ages 16 and 17 already limit non-family passengers under 21, yet summer plans often test these limits.
Phones and summer plans add distraction. Quick texts or calls happen more when schedules are loose. Even a few seconds of looking away can cause a rear-end crash on busy local roads.
Night driving and longer trips increase fatigue. Low light on I-10 or Loop 375 slows reactions. Heat over 100 degrees can also cause tire trouble that surprises new drivers on long stretches.
Speeding and following too closely. Open roads tempt higher speeds. Tailgating on busy streets like those near Airway or Sunland Park leads to sudden stops and chain-reaction crashes.
These patterns explain why the same careful driver faces greater danger during summer freedom.
Expert Tips to Help Young Drivers Stay Safe
Groups like the National Road Safety Foundation and AAA Texas give simple steps that work. The focus is on cutting distractions and building good habits early.
Buckle up on every single ride. Seat belts greatly lower the chance of serious injury or death.
Keep phones away or turn on do-not-disturb mode while driving. Even one message can lead to a crash.
Limit young passengers. Follow Texas rules that allow only one non-family passenger under 21 for provisional drivers.
Plan routes together before leaving. Review exits, construction, and safe stops on highways like I-10.
Check tires, brakes, and fluids before summer trips. Extreme El Paso heat wears tires faster.
Set clear rules about speed, rest, and no drinking. Parents who drive calmly set the best example.
These habits help turn risky summer miles into safer ones for everyone on El Paso roads.
What Happens When a Crash Occurs?
Even careful drivers can end up in an accident on I-10, at a busy intersection, or in a rear-end on Mesa Street. Right after the crash, adrenaline and endorphins often mask the full extent of the damage. Many people feel okay at the scene, only to notice problems hours or days later. At El Paso Back Clinic, we see patients whose neck stiffness, headaches, or back pain started small but worsened as swelling and inflammation slowly built up in the deeper tissues. Some symptoms even appear weeks later as the body compensates or scar tissue forms.
Common delayed signs include ongoing headaches from neck strain, neck or back stiffness and pain, radiating numbness or tingling into arms or legs, unusual fatigue, brain fog or trouble focusing, dizziness or balance issues, shoulder or hip discomfort, sleep problems, and mood changes. Ignoring these signals can turn a minor issue into long-term pain or changed movement patterns that affect driving, work, and daily life.
That is why prompt, thorough care matters. The right clinic helps the body heal from both the direct physical trauma and the whole-system stress the crash creates.
How El Paso Back Clinic Supports Integrative Recovery
At El Paso Back Clinic, we specialize in helping car accident victims recover fully, especially when pain shows up later. Our integrative approach treats the musculoskeletal injuries and the broader effects on inflammation, nerve function, sleep, and tissue repair. This combination often leads to faster relief, better movement, and fewer long-term problems.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, leads the team with years of experience in personal injury and spinal trauma. His clinical observations show that patients with delayed symptoms improve significantly when care targets spinal alignment early and supports the body’s natural repair processes. Gentle chiropractic adjustments restore joint movement, relieve nerve pressure, and reduce muscle guarding. Myofascial release loosens tight tissues so the body stops compensating in ways that create new pain.
We also offer advanced options when deeper support is needed. Regenerative injections such as platelet-rich plasma (PRP) use the patient’s own concentrated platelets to release growth factors that help build collagen, improve blood flow, and repair ligaments, tendons, and muscles. Spinal decompression gently stretches the spine to ease pressure on discs and nerves, helping with radiating pain or sciatica-like symptoms. Ultrasound and shockwave therapy boost circulation and calm inflammation without surgery. Rehabilitation exercises rebuild strength and stability so patients return to normal activities with lower risk of setbacks.
Working alongside Dr. Jimenez is Dr. Maria Guadalupe Cardenas, MD. She is board-certified in internal medicine with over 40 years of experience. Her NPI number is 1164426749, and her Texas medical license is J2933. As Medical Director and Collaborative Physician at the clinic, she provides medical oversight, reviews overall health, guides complex cases, and ensures everything stays safe and compliant. This multidisciplinary setup, common in strong injury clinics, means chiropractic care, functional support, and medical direction happen in one place with consistent records.
One of the biggest benefits for El Paso families is the detailed documentation we create. Clear notes link the crash to the injuries, record objective measures like range of motion and strength, track daily limitations such as driving or working, and show steady progress. These records help insurance claims move smoothly and give personal injury attorneys the credible timeline they need for fair settlements. Many patients appreciate that everything from the first exam to final recovery notes stays in one location, reducing stress during an already difficult time.
Our team focuses on whole-person healing so the body can repair at the cellular level. Early attention prevents small problems from becoming chronic pain or altered posture that lasts for years. Patients often report less ongoing discomfort, easier movement, and a quicker return to family life and work.
Taking the Next Step Toward Safety and Healing
The 100 Deadliest Days remind us that summer driving in El Paso carries real risks for young drivers. More freedom, extra passengers, phones, and longer trips on local highways all raise the chances of trouble. Simple habits like buckling up, limiting distractions, and planning routes can prevent many crashes.
When an accident does happen, know that delayed pain is common and can be treated. At El Paso Back Clinic, we provide integrative care that addresses both visible injuries and hidden stress on the body. With Dr. Alex Jimenez’s expertise in spinal trauma and delayed symptoms, Dr. Maria Guadalupe Cardenas’s medical oversight, and a full range of chiropractic, regenerative, and rehabilitation services, patients receive complete support and strong documentation for insurance or legal needs.
Summer should bring cherished memories, not lasting pain. Understanding the risks and choosing thorough recovery care at El Paso Back Clinic helps young drivers and their families in El Paso move forward with confidence.
If you or someone you care about was in a summer car accident and is now feeling delayed pain or stiffness, contact our team today. Call 915-850-0900 or visit elpasobackclinic.com to schedule a consultation. We are here to help you heal fully and get back to living, loving, and thriving.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine