Temporomandibular Joint Disorder, or TMJ, is a common condition that affects the jaw. It can be extremely painful and many people are turning to methods other than medication or surgery to relieve that pain. While lifestyle changes such as diet may help, chiropractic care has been cited as a viable treatment for TMJ pain.
At first, this may seem counter-intuitive simply because it is widely believed that chiropractors only treat the spine and neck. This commonly held belief is not entirely accurate. Chiropractors treat all joints, including the spine and neck. A chiropractor may treat ankles, wrists, knees, and, yes, even the jaw. Sometimes the neck and spine can be contributing factors and they can be treated with chiropractic care as well.
What Is Temporomandibular Joint Disorder?
The joint that connects your jaw to your skull and allows you to open and close your mouth is the temporomandibular joint. When you have problems with the muscles or joint in that area it is called TMJ, or more accurately temporomandibular disorders, or TMD.
This disorder is characterized by pain and stiffness on one or both sides of the jaw. The jaw may also lock or get stuck in either a closed or open position. Patients may also notice a popping, clicking, or grating sound in the jaw when chewing, yawning, or when closing or opening their mouth. They may also have trouble chewing and even experience swelling.
Doctors don�t know what causes TMJ. It seems to be linked to trauma to the neck, such as with whiplash, but it also can be caused by:
Arthritis in the jaw
Grinding the teeth
Stress that causes clenching of the jaw
Movement of the disc, or soft cushion, that lies between the socket and ball of the jaw
Diagnosis & Treatment For Temporomandibular Joint Disorder
Many conditions can mimic the symptoms of TMD. After taking a medical history, your doctor will check the joints in the jaw for popping, clicking, or grating sounds. He will also assess the patient�s pain or tenderness level and check for any stiffness. During the exam, the doctor will assess the job and its ability to function properly. X-rays may also be a part of the examination.
If the doctor can pinpoint the probable cause of the TMJ, he may prescribe certain treatments or make recommendations that will help. Medication is one option, mainly stress or anti-anxiety medication to help the patient relax. A night guard or splint is another option. It helps to put the patient�s teeth in the correct position. A splint is worn all the time and a night guard is worn only at night. Dental work is another option and in come more serious cases, surgery.
Chiropractic Care For Temporomandibular Joint Disorder
Chiropractic for TMJ is not only common, but very effective. The chiropractor may perform neck or spine adjustment as well as adjustments to the jaw. This means that the patient may experience pressure on their skull, jaw, upper spine, or neck as the chiropractor treat the condition. There are also soft tissue treatments that the chiropractor may perform during the course of treatment for TMJ.
The chiropractor will often recommend lifestyle and diet changes to patients. This offers the patient the opportunity to treat the whole body as opposed to just one area. They may apply cold packs or heat packs to the area, recommend supplements, and teach the exercises designed to lessen the pain and encourage healing. Chiropractic is a safe, effective, and non-invasive treatment for TMJ.
So if you or a loved one have been diagnosed with TMD and/or are experiencing TMJ pain, give us a call. Our Doctor of Chiropractic is here to help!
Chiropractic Clinic Extra: Neck Pain Care & Treatments
Shoulder Treatment: About two years ago, Denise was involved in an automobile accident which resulted in upper body issues, including shoulder pain. Due to her painful symptoms, Denise was unable to engage in her regular physical activities. While she continued to experience problems with her auto accident injuries, she decided to seek chiropractic shoulder treatment with Dr. Alex Jimenez. Since her first treatment session, Denise noticed tremendous changes to her symptoms and she was once again able to return to her original routines prior to the incident. Denise positively recommends Dr. Alex Jimenez as the non surgical choice for shoulder pain treatment since finding relief.
Upper body issues, such as shoulder pain, are some of the most common reasons for doctor visits. The shoulder is the most mobile joint in the human body, however, because of its increased range of motion, it is also the most unstable joint. This can increase the risk of joint injury, often leading to the degeneration of the soft tissues surrounding the shoulders. Shoulder pain can be categorized as localized or referred, with other health issues causing shoulder pain. The force from the impact of an accident, such as an automobile accident or a sports injury, is a well-known cause for shoulder issues.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You & God Bless.
Back Pain Management: Denise was involved in an auto accident which resulted in low back pain. When she realized she couldn’t sit, walk or sleep for extended periods of time without experiencing painful symptoms, Denise found chiropractic care with Dr. Alex Jimenez in El Paso, TX. Once she received treatment for her auto accident injuries, Denise experienced relief from her symptoms and she was able to perform her everyday activities once again. Thanks to the education and care Dr. Alex Jimenez provided, Denise regained her original health and wellness.
Back pain is common, with roughly nine out of ten adults experiencing it at some time in their life, and five from ten working adults developing it every year. Some estimate around 95 percent of Americans will experience back pain at some time in their lifetime. It’s by far the usual cause of chronic pain, as it is also a significant contributor of missed work and disability. In the United States alone, acute cases of lower back pain are the fifth most common reason for physician visits and causes 40 percent of missed days off work. Furthermore, it is the only leading cause of disability globally. Back pain management is possible through chiropractic treatment.�For Answers to any questions you may have please call Dr. Jimenez at 915-850-0900
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Truide Torres, office manager, developed facet syndrome from participating in gymnastics at a young age. Due to the additional stress being placed on her spine, Mrs. Torres was forced to reduce her engagement in exercise and physical activities. In order to continue being involved in fitness, Truide Torres found facet syndrome pain treatment with Dr. Alex Jimenez, D.C. in El Paso, TX. Mrs. Torres was well-informed and properly treated by Dr. Jimenez for her face syndrome and she was able to participate in her exercise and physical activities once again. Truide Torres recommends Dr. Alex Jimenez and his staff as the non-surgical choice for facet syndrome pain treatment, describing them as a caring, knowledgeable and qualified group of healthcare professionals.
Facet syndrome (also popularly known as facet joint disease, facet osteoarthritis, facet hypertrophy or aspect arthritis) is a syndrome where the facet joints (synovial diarthroses, from C2 to S1) degenerate to the purpose of causing debilitating symptoms. In conjunction with degenerative disk disease, a distinct but related illness, aspect syndrome is thought to be one of the most frequent causes of lower back pain. The signs of facet joint syndrome rely almost entirely about the location of this degenerated joint, the severity of the harm and the amount of pressure that is being put on the surrounding nerve roots. It is essential to note that the amount of pain a person experiences does not correlate well with the amount of degeneration that has occurred within the joint. A lot of men and women experience little or no pain while others, with the specific same amount of damage, experience chronic pain.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Truide Torres, office manager, first received chiropractic care with Dr. Alex Jimenez during her pregnancy for her lower back pain. Mrs. Torres experienced aggravating symptoms throughout the progression of her pregnancy, which led her to seek a natural treatment approach for her own health as well as that of her own baby. Once Truide Torres started chiropractic treatment with Dr. Alex Jimenez, she recovered her quality of life and was able to return to her original state of well-being. As an office manager, Truide Torres also receives regular chiropractic care for any lower back pain which may occur as a result of her job. Mrs. Truide expresses how important it is to continue her spinal maintenance and she highly recommends Dr. Alex Jimenez as the non-surgical choice for a variety of health issues.
Low back pain (LBP) is a frequent health issue involving the muscles, nerves, and bones of the spine. Pain may differ from a dull persistent pain to a sudden sharp sensation. Low back pain can be classified by length and severity (pain lasting less than 6 months), sub-chronic (6 to 12 months), or chronic (over 12 months). The status could be further categorized by the underlying cause as both bodily, non-mechanical, or referred pain. The symptoms of low back pain may generally improve in a couple weeks from the time they begin, however, some cases may require additional treatment. In the majority of episodes of lower back pain, a specific underlying cause isn’t identified or properly cared for, and healthcare professionals may attribute it to mechanical issues like joint or muscle strain.
Prenatal Yoga Exercises For Low Back Pain
Back Clinic News Extra: Migraine Pain Treatment With Chiropractic
Damaris Foreman suffered from migraines for about 23 years. After receiving traditional treatment for her migraine pain without much improvement, she was finally recommended to seek migraine pain treatment with Dr. Alex Jimenez, a chiropractor in El Paso, TX. Damaris greatly benefitted from chiropractic care and she experienced a tremendous sense of relief following her first spinal adjustment and manual manipulation. Damaris Foreman was able to confront many of her misconceptions and she learned very much about her migraine pain. Damaris describes Dr. Alex Jimenez’s migraine pain treatment as one of the best treatment she’s received and she highly recommends chiropractic care as the best non-surgical choice for improving and managing her migraines.
A migraine can be identified as a primary headache disorder characterized by recurrent headaches characterized from moderate to severe in intensity. Typically, the headaches affect one half of the head, are pulsating in nature, and can last from two to 72 hours. Associated symptoms may include nausea, vomiting, and sensitivity to light, sound, or smell. The pain may be aggravated by physical activity. Up to one-third of people who suffer from migraines experience migraine with aura: typically a brief period of visual disturbance that signals that the headache will soon happen. An aura can occur with little or no headache pain following it.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
George Lara, now retired, found relief with Dr. Alex Jimenez, back pain specialist and chiropractor, for his degenerative disk disease following two back injuries he experienced several years ago. After using drugs/medications and experiencing constant symptoms due to his DDD, Mr. Lara describes how Dr. Jimenez’s chiropractic treatment greatly helped restore his quality of life as well as promote his overall health and wellness. George Lara highly recommends Dr. Alex Jimenez as a non-surgical treatment choice for degenerative disc disease, and praises his dedication for treating his patients.
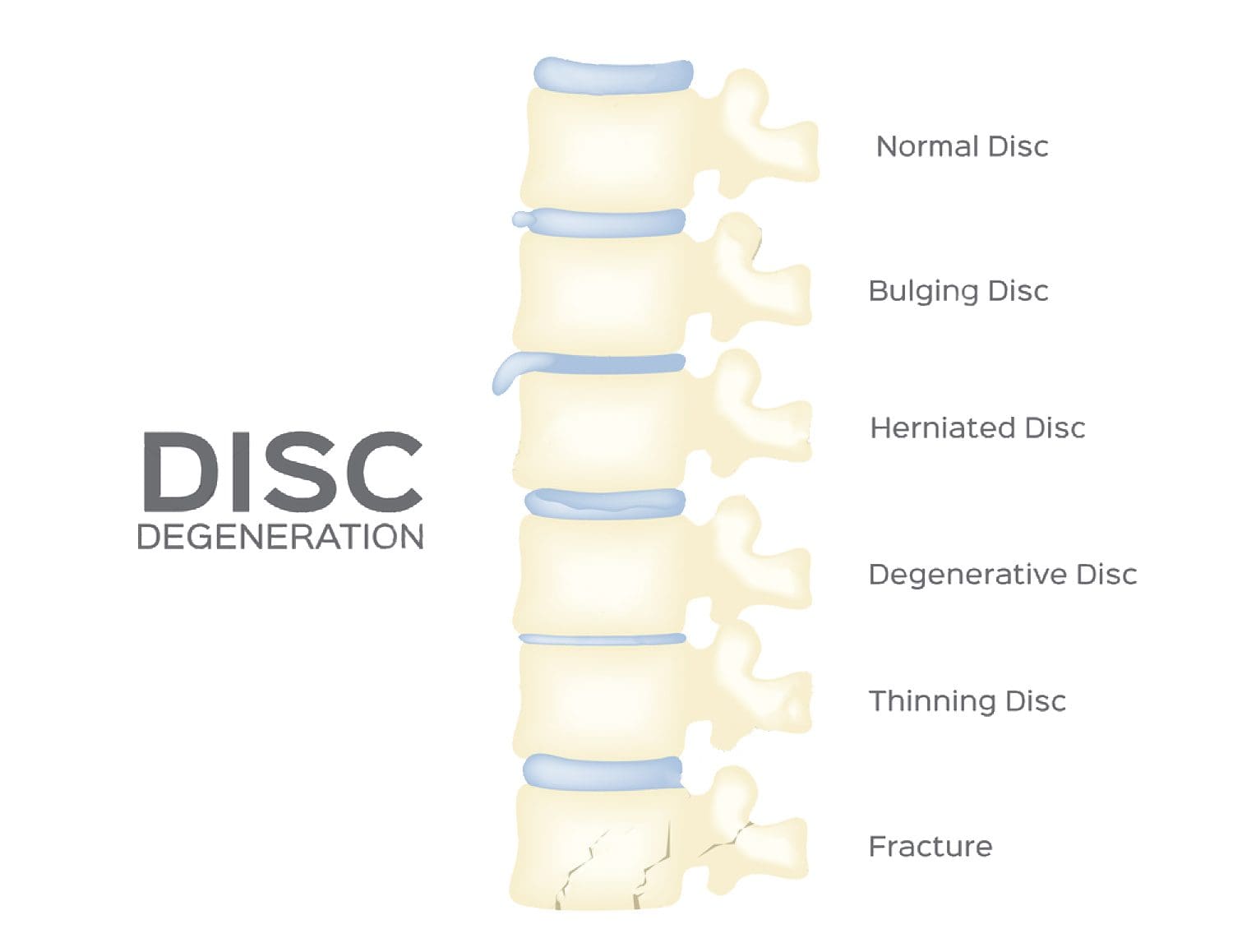
Degenerative disk disease, or DDD, refers to the natural breakdown of an intervertebral disk of the spine. Despite its title, DDD isn’t regarded as a disorder, nor is it degenerative. To the contrary, disk degeneration is frequently the consequence of ordinary daily stresses and minor accidents that cause spinal disks to slowly eliminate water in the anulus fibrosus, or even through the stiff outer layer of a disk. As water content decreases, they start to collapse. This could lead to pressure being placed on the nerves causing weakness and pain. While not necessarily symptomatic, DDD may lead to acute or chronic low back or neck pain in addition to nerve pain based on the positioning of the affected disk and the amount of strain it puts around the surrounding nerve roots.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Chiropractic Helps:Tendonitis is a condition that occurs when a tendon that connects bone to muscle is injured, overused, or used improperly. The result is inflammation, pain and sometimes swelling. In the case of an injury where the tendon is stressed to otherwise injured, soft tissue around the area may also become involved. Each year more than 4 million people in the U.S. seek medical treatment for symptoms of tendonitis.
Common types of tendonitis include runner�s knee, tennis elbow, and pitcher�s shoulder. However, other tendons in the body can also experience tendonitis symptoms. The Achilles tendon, ankle, wrist, and even fingers can all become inflamed from the condition.
Often a primary care physician diagnoses the injury, but once there is a definitive diagnosis, the best treatment is one that is natural and holistic. Chiropractic care is an outstanding choice for treatment.
Chiropractic Helps: Thorough Healing
Tendonitis often recurs in many people. This is due, at least in part to improper or incomplete healing. Many people will resume normal activities as soon as the pain subsides when they should continue caring for the injury so that it can heal completely. This leads to inflammation of the area again as the original injury is aggravated, but it can also lead to re-injury in that same area. Chiropractic care can help tendonitis heal completely and help prevent re-injury to the area.
Chiropractic Helps: Tendonitis
Since tendonitis symptoms can mimic other serious conditions, the first step in treatment is confirming the diagnosis. The doctor may use X-rays, MRIs, or CAT scans to make a positive diagnosis of tendonitis.
From there, the chiropractor will work with the patient to develop a treatment plan that is natural and effective, tailored to the patient�s unique needs. At the core of this treatment is a targeted plan that treats the cause of the problem, not just the symptoms.
If there is a great deal of inflammation the chiropractor may employ inflammation reducing techniques such as bracing, rest, ice, electrical muscle stimulation, and other therapies. This helps to loosen the tendon and lessen the inflammation so that treatment can progress.
Once the inflammation is under control, the chiropractor may begin massage, physical therapy, joint manipulation, or strengthening exercises. If the patient has diminished or limited joint mobility then joint manipulation or adjustments may be the best option.
Chiropractic Helps: Length Of Treatment
The initial pain may subside or even disappear within the first two to three weeks. However, that does not mean that the patient is out of the woods. This is where many patients go wrong. They mistakenly believe that once the pain is gone the condition is healed.
This is not true. While the inflammation may indeed decrease over the first three weeks, the complete healing takes around six weeks and often longer. Scar tissue is formed during this time which helps the body repair the injury. Once the injury is repaired though, that scar tissue must be broken down in order for the area to regain its mobility and flexibility.
The chiropractor will use various techniques including massage and ultrasound to break down the scar tissue. Mild stretches may be incorporated into the treatment plan. Once the tissues are fully healed, exercise can aid in breaking down the scar tissue even more. These exercises will work the muscles but they won�t involve the tendons.
Chiropractic Helps: Healing Tendonitis For Good
Tendonitis can be healed completely and a good chiropractor can help. Most chiropractors take a whole body approach, including diet, specific supplements, and lifestyle choices that will help the healing process of tendonitis. Once chiropractic treatment is complete for tendonitis, the patient can usually return to normal activities without the risk of re-injury or re-inflammation.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 This disorder is characterized by pain and stiffness on one or both sides of the jaw. The jaw may also lock or get stuck in either a closed or open position. Patients may also notice a popping, clicking, or grating sound in the jaw when chewing, yawning, or when closing or opening their mouth. They may also have trouble chewing and even experience swelling.
This disorder is characterized by pain and stiffness on one or both sides of the jaw. The jaw may also lock or get stuck in either a closed or open position. Patients may also notice a popping, clicking, or grating sound in the jaw when chewing, yawning, or when closing or opening their mouth. They may also have trouble chewing and even experience swelling.

 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You & God Bless.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You & God Bless.
 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.