Can individuals dealing with sciatica pain find the relief they need from acupuncture to restore low back mobility?
Introduction
The body’s lower extremities provide stability and movement to the individual as they are moving from one location to another without pain or discomfort. The lower extremities consist of the hips, lower back, legs, thighs, pelvis, knees, and feet; each has various muscles, nerve roots, and ligaments with a specific job to each muscle quadrant. The spinal column in the musculoskeletal system helps provide proper posture while protecting the spinal cord from injuries. However, more often than not, the lower extremities can succumb to injuries as many individuals incorporate repetitive motions that can compress the nerve roots that are spread out to the lower extremities, which can invoke pain. The most common pain that seems to affect the lower back and legs is sciatica, and when not treated, it can cause overlapping risk profiles to the lower extremities. Today’s article examines how sciatica is correlated with the lower back and how non-surgical treatments can help reduce the effects of sciatic pain. We talk with certified medical providers who consolidate our patients’ information to provide numerous treatments to relieve sciatica pain affecting their lower extremities. We also inform and guide patients on how non-surgical treatments can help reduce sciatica pain from the lower musculoskeletal extremities. We encourage our patients to ask their associated medical providers intricated and important questions about the pain-like symptoms they are experiencing from sciatica that are causing them pain. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
How Does Sciatica Correlate With The Lower Back?
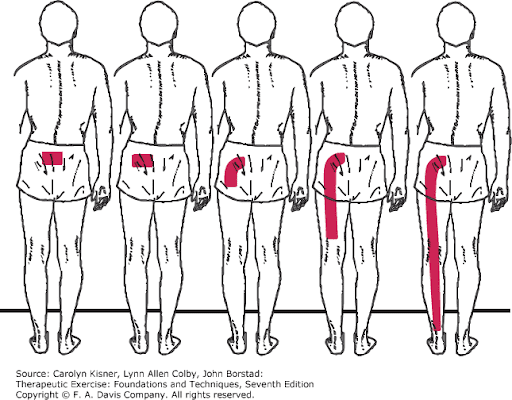
Do you often experience numb or tingling sensations running down your leg that cause your leg or foot to lose sensation briefly? Do you feel shooting pain in your lower back after excessive sitting at your desk? Or do you find that stretching your legs or back temporarily relieves the pain, only for it to come back? Many individual who are experiencing shooting pain running down their legs are dealing with sciatica. When it comes to the lower extremities in the musculoskeletal system, many individuals make repetitive motions on their spine that can cause the spinal discs to become compressed and herniated under pressure. When the spinal disc is herniated in the lumbar spine, that disc will start to press on the surrounding nerve roots, thus sending radiating pain down the legs. Sciatica is defined as when individuals are experiencing pain coming from the lumbosacral nerve root and causing either a burning, heaviness, or tightness sensation. (Aguilar-Shea et al., 2022) Sciatica can range from mild to severe, forcing many individuals to think their foot is asleep. However, the sciatic nerve root is compressed, trapped, stuck, or pinched, which causes muscle spasms within the lower back, buttock, or legs. Hence, many individuals will explain that they are experiencing low back or leg pain when it is sciatica.
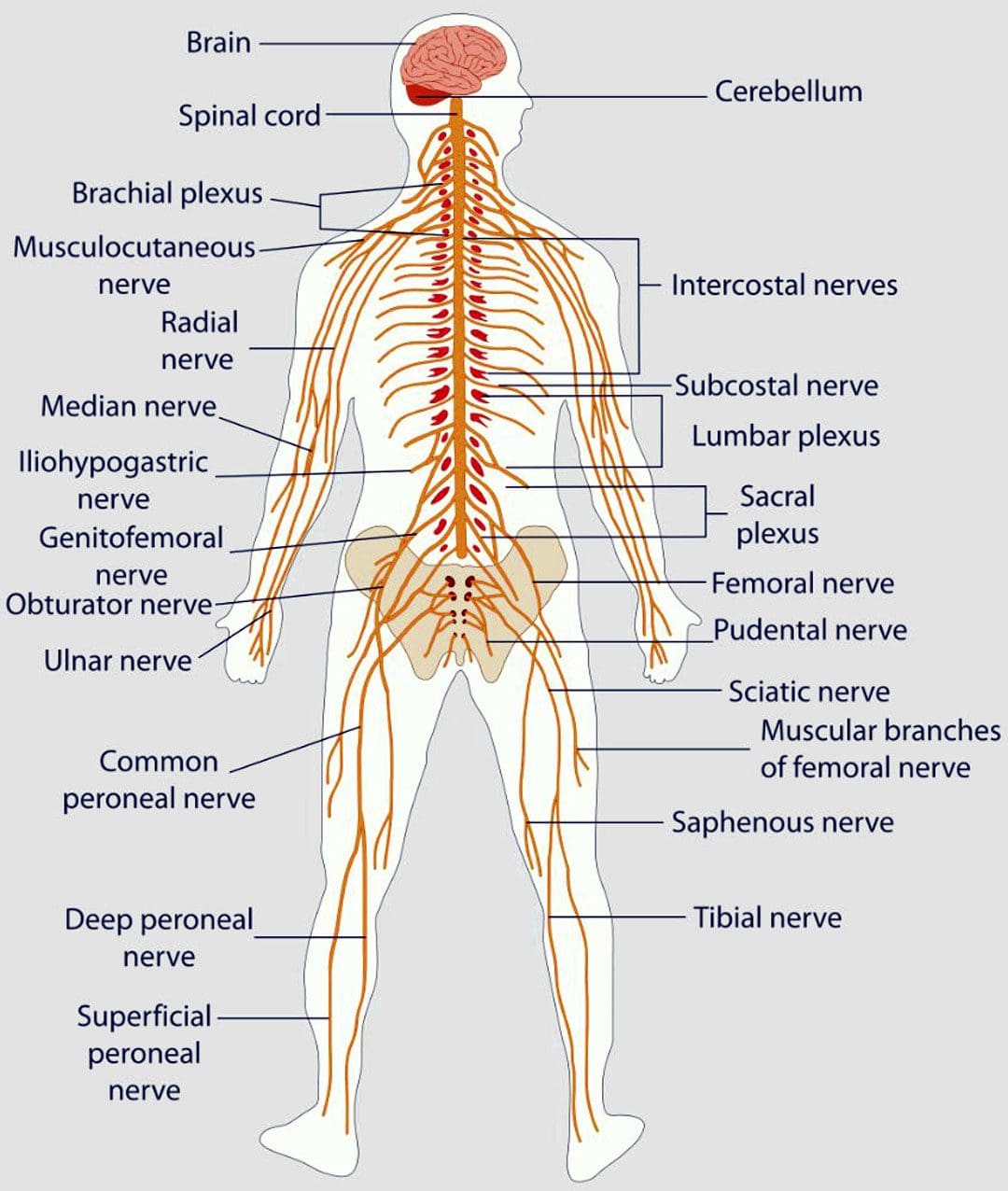
Since the sciatic nerve is a long, thick nerve in the human body, it travels from the lumbar region down to the knee and connects to other nerves to reach the foot. Sciatica pain can be two conditions with the same pain-like symptom effects known as true or sciatica-like conditions. True sciatica is where an injury is directly affecting the sciatic nerve. This can relate to a slipped disc caused by environmental factors like lifting a heavy object, aggravating the sciatic nerve root, and causing pain that worsens. (Siddiq et al., 2020) For sciatica-like conditions, this is where other musculoskeletal conditions are causing sciatic pain-like symptoms on the lower extremities. Musculoskeletal conditions like piriformis syndrome can cause sciatica pain-like symptoms where the piriformis muscle is irritated or inflamed, pressing on the sciatic nerve, which causes many people to report pain along the gluteal region that may shoot a burning, aching sensations down the back of the legs. (Hicks et al., 2024) However, there are ways to treat sciatica and reduce the pain-like effects causing mobility issues.
Sciatica, Causes, Symptoms and Tips- Video
Non-surgical Treatments For Sciatica
When it comes to reducing sciatica pain, many individuals will seek out treatment that is cost-effective and customized to the person’s pain. Some treatments, like neural mobilization, can apply mechanical forces to the nerve roots to restore healthy movement to the legs and lower extremities. (Peacock et al., 2023) Other treatments, like spinal decompression, use gentle traction on the spinal disc to lay off the pressure on the sciatic nerve to provide relief. Non-surgical treatments are favorable to many people due to how affordable it is and personalized to the person’s pain as they help reduce pain and disability. (Liu et al., 2023) Luckily, a form of non-surgical treatment can help relieve sciatica and its associated pain-like symptoms.
Acupuncture Relieving Sciatic Pain
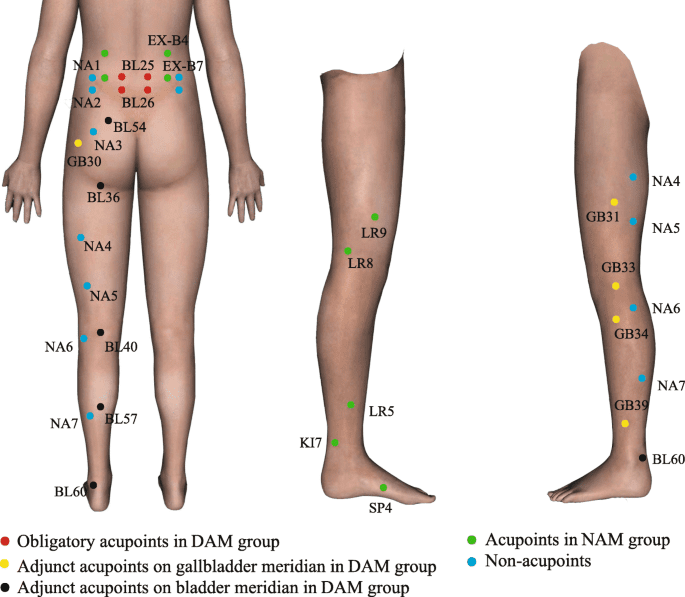
Acupuncture is one of the oldest forms of non-surgical treatments in which trained professionals use thin, solid needles to be inserted and placed on the affected area, causing pain. Acupuncture can help reduce the distortion of the affected nerve roots, and local inflammatory cytokines correlated with sciatica. (Yu et al., 2021) What this does is that it normalizes the neuron signals to a default mode from aggravating the surrounding muscle fibers and descending the pain. Additionally, acupuncture can help restore the body’s qi or energy by reducing the pain by placing the needles on the acupoint of the vital organs that share a relationship with the sciatic nerve. (Yu et al., 2022) This is known as somato-visceral, where the vital organs could be the affected area, causing overlapping muscle and nerve risk profiles. Acupuncture is an excellent form of non-surgical treatment that can be combined with other various therapies to help restore the body’s natural healing factor and allow people to be more mindful of how to take care of their bodies easily to prevent sciatica pain-like symptoms from arising.
References
Aguilar-Shea, A. L., Gallardo-Mayo, C., Sanz-Gonzalez, R., & Paredes, I. (2022). Sciatica. Management for family physicians. J Family Med Prim Care, 11(8), 4174-4179. https://doi.org/10.4103/jfmpc.jfmpc_1061_21
Liu, C., Ferreira, G. E., Abdel Shaheed, C., Chen, Q., Harris, I. A., Bailey, C. S., Peul, W. C., Koes, B., & Lin, C. C. (2023). Surgical versus non-surgical treatment for sciatica: systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://doi.org/10.1136/bmj-2022-070730
Peacock, M., Douglas, S., & Nair, P. (2023). Neural mobilization in low back and radicular pain: a systematic review. J Man Manip Ther, 31(1), 4-12. https://doi.org/10.1080/10669817.2022.2065599
Siddiq, M. A. B., Clegg, D., Hasan, S. A., & Rasker, J. J. (2020). Extra-spinal sciatica and sciatica mimics: a scoping review. Korean J Pain, 33(4), 305-317. https://doi.org/10.3344/kjp.2020.33.4.305
Yu, F. T., Liu, C. Z., Ni, G. X., Cai, G. W., Liu, Z. S., Zhou, X. Q., Ma, C. Y., Meng, X. L., Tu, J. F., Li, H. W., Yang, J. W., Yan, S. Y., Fu, H. Y., Xu, W. T., Li, J., Xiang, H. C., Sun, T. H., Zhang, B., Li, M. H., . . . Wang, L. Q. (2022). Acupuncture for chronic sciatica: protocol for a multicenter randomised controlled trial. BMJ Open, 12(5), e054566. https://doi.org/10.1136/bmjopen-2021-054566
Yu, F. T., Ni, G. X., Cai, G. W., Wan, W. J., Zhou, X. Q., Meng, X. L., Li, J. L., Tu, J. F., Wang, L. Q., Yang, J. W., Fu, H. Y., Zhang, X. C., Li, J., Wang, Y. F., Zhang, B., Zhang, X. H., Zhang, H. L., Shi, G. X., & Liu, C. Z. (2021). Efficacy of acupuncture for sciatica: study protocol for a randomized controlled pilot trial. Trials, 22(1), 34. https://doi.org/10.1186/s13063-020-04961-4
Can individuals dealing with hip pain, find the relief they are looking for from spinal decompression to reduce their sciatica pain?
Introduction
When it comes to individuals doing everyday movements, the body can be in weird positions without pain or discomfort. Hence, people can stand or sit for prolonged periods and feel all right when doing strenuous activities. However, as the body ages, the surrounding muscles and ligaments can become weak and tight, while the spinal joints and discs start to be compressed and wear and tear. This is because many individuals make repetitive motions on their bodies that cause pain-like symptoms in the back, hips, neck, and body extremities, leading to referred pain in different body locations. When individuals are experiencing musculoskeletal pain in their bodies, it can cause overlapping risk profiles that can hinder the individual and cause them to be miserable. Additionally, when people experience musculoskeletal pain in their bodies, many will seek treatment to reduce the referred pain-like symptoms associated with the musculoskeletal pain. Today’s article will examine one type of musculoskeletal pain on the hips, how it can cause sciatica pain-like problems, and how treatments like decompression can reduce the pain-like effects of hip pain correlated with sciatica. We talk with certified medical providers who consolidate our patients’ information to provide numerous treatments to relieve hip pain associated with sciatica. We also inform and guide patients on how decompression can help reduce pain-like symptoms like sciatica and restore hip mobility. We encourage our patients to ask their associated medical providers intricated and important questions about the pain-like symptoms they are experiencing from hip pain. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
Hip Pain Associated With Sciatica
Do you often experience stiffness in your lower back and hips after sitting down for an excessive period? How about feeling radiating pain running down from your lower back to your legs? Or do you think your hip and thigh muscles become tight and weak, which is affecting your gait stability? Many individuals experiencing these pain-like issues are experiencing hip pain, and it can be an issue when it is not treated over time. Since hip pain is a common and disabling condition that is challenging to diagnose, many individuals often express localized pain in one of the three anatomic regions: the anterior, posterior, and lateral hip sections. (Wilson & Furukawa, 2014) When individuals are dealing with hip pain, they will also experience referred pain in their lower backs, which causes them to be in distress and miserable. At the same time, simple ordinary movements like sitting or standing can affect the muscles and ligaments surrounding the hips and can be damaging. This can cause hip pain to be referred from the lumbar spine and spine problems, which then cause musculoskeletal issues in the lower extremities. (Lee et al., 2018)
So, how would hip pain be associated with sciatica and causing pain in many lower extremities? The hip areas in the musculoskeletal system have numerous muscles surrounding the pelvic bone area that can become tight and weak, causing referred musculoskeletal pain from intrapelvic and gynecologic issues. (Chamberlain, 2021) This means that musculoskeletal disorders like piriformis syndromes associated with hip pain can lead to sciatica. The sciatic nerve travels down from the lumbar region and the buttocks and behind the leg. When a person is dealing with sciatica and is going to their primary doctor to get treated for the pain, their doctors will do a physical examination to see what factors are causing the pain. Some of the common findings during a physical exam were tenderness and palpation of the greater sciatic notch and the reproduction of pain along the hips. (Son & Lee, 2022) This causes associated symptoms that correlate with sciatica and hip pain, including:
Tingling/numbing sensations
Muscle tenderness
Pain while sitting or standing
Discomfort
Is Motion The Key To Healing- Video
Spinal Decompression Reducing Hip Pain
However, many individuals will find non-surgical treatments to help reduce sciatica associated with hip pain. Non-surgical treatments are customized to a person’s pain and are cost-effective while being gentle on the spine. Spinal decompression can help reduce hip pain associated with sciatica. Decompression on the spine allows gentle traction to stretch out weak muscles along the lower back and hips while the spinal discs are experiencing negative pressure. When a person is dealing with sciatica pain associated with hip pain and trying decompression for the first time, they are provided with the relief they deserve. (Crisp et al., 1955)
Additionally, many individuals who incorporate decompression for their hip pain can begin to feel its effects as it helps improve blood flow circulation back to the hips to start the natural healing process. (Hua et al., 2019) When people begin incorporating decompression for their hip pain, they can relax as they feel all their aches and pain gradually disappear as mobility and rotation are back on the lower extremities.
Crisp, E. J., Cyriax, J. H., & Christie, B. G. (1955). Discussion on the treatment of backache by traction. Proc R Soc Med, 48(10), 805-814. https://www.ncbi.nlm.nih.gov/pubmed/13266831
Hua, K. C., Yang, X. G., Feng, J. T., Wang, F., Yang, L., Zhang, H., & Hu, Y. C. (2019). The efficacy and safety of core decompression for the treatment of femoral head necrosis: a systematic review and meta-analysis. J Orthop Surg Res, 14(1), 306. https://doi.org/10.1186/s13018-019-1359-7
Lee, Y. J., Kim, S. H., Chung, S. W., Lee, Y. K., & Koo, K. H. (2018). Causes of Chronic Hip Pain Undiagnosed or Misdiagnosed by Primary Physicians in Young Adult Patients: a Retrospective Descriptive Study. J Korean Med Sci, 33(52), e339. https://doi.org/10.3346/jkms.2018.33.e339
Son, B. C., & Lee, C. (2022). Piriformis Syndrome (Sciatic Nerve Entrapment) Associated With Type C Sciatic Nerve Variation: A Report of Two Cases and Literature Review. Korean J Neurotrauma, 18(2), 434-443. https://doi.org/10.13004/kjnt.2022.18.e29
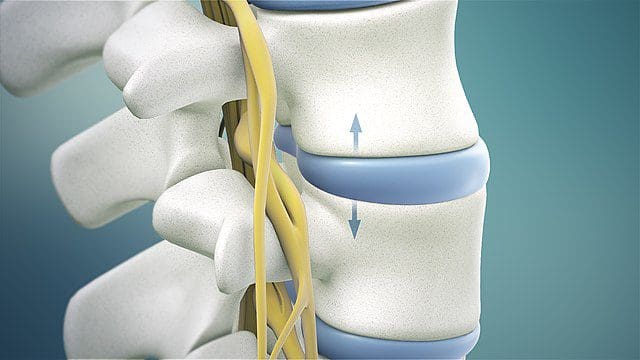
The discs between the spine’s vertebrae provide cushioning and shock absorption in the spine and the rest of the body. Degenerative changes to the discs are believed to be the start of spinal stenosis. When the discs lack sufficient hydration/water and disc height decreases over time, the cushioning and shock absorption becomes less and less effective. The vertebrae can then become compressed, causing friction. Degenerative spinal stenosis can also develop from excess scar tissue and bone spurs (growth that develops on the edge of a bone) that can form after injury or spinal surgery.
Assessment
A physician will make a diagnosis of spinal stenosis. The doctor will take an imaging scan of the spine to determine the exact location of the degeneration and to measure how narrow the openings have become. Pain, stiffness, limited mobility, and loss of range of motion are often present. If spinal stenosis has caused nerve compression, there may also be pain, numbness, tingling, or weakness in the buttocks (sciatica), thighs, and lower legs. A physical therapist will determine the degree by assessing the following:
Vertebrae mobility – how the spine bends and twists in different directions.
Ability to change positions.
The strength of the core, back, and hip muscles.
Balance
Posture
Gait pattern
Nerve compression to determine if there are any symptoms in the legs.
Milder cases usually do not involve nerve compression, as back stiffness is more common.
In more severe cases, there may be significant pain, limited mobility, and nerve compression, causing leg weakness.
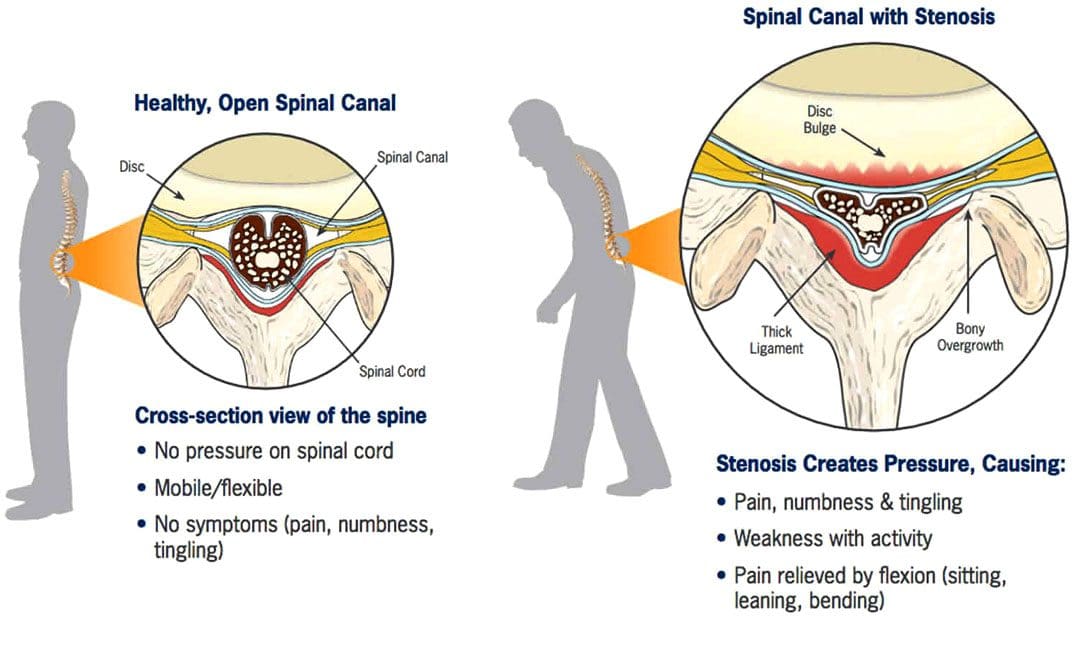
The most common symptom of spinal stenosis is increased pain with backward bending or extension of the lumbar spine. This includes positions that extend the spine, such as standing, walking, and lying on the stomach. Symptoms usually improve when bending forward and when the spine is positioned more into a flexed or bent position, like when sitting and reclining. These body positions open up the spaces in the central spinal canal.
Surgery
Spinal stenosis is the most common reason for undergoing surgery in adults 65 and older. However, surgery is almost always performed as a last resort if pain, symptoms, and disability persist after trying conservative therapies, including chiropractic, non-surgical decompression, and physical therapy, for months or years. The severity of symptoms and current state of health will determine whether a doctor will recommend surgery. (Zhuomao Mo, et al., 2018). Conservative measures can be safer and just as effective. A systematic review or study based on all available primary research found that physical therapy and exercise resulted in similar outcomes to surgery for improving pain and disability. (Zhuomao Mo, et al., 2018). Except for severe cases, surgery is often not necessary.
Physical Therapy for Spinal Stenosis
The objective of physical therapy includes:
Decreasing pain and joint stiffness.
Relieving nerve compression.
Reducing tightness in the surrounding muscles.
Improving the range of motion.
Improving postural alignment.
Strengthening the core muscles.
Improving leg strength to help with balance and overall function.
Stretching of the back muscles, including those running vertically along the spine and those running diagonally from the pelvis to the lumbar spine, helps relieve muscle tightness and pain and can improve overall mobility and range of motion of the lumbar spine.
Stretching the hip muscles, including the hip flexors in the front, the piriformis in the back, and the hamstrings that run from the back of the hip down the leg to the knee, is also important as these muscles are attached to the pelvis, which directly connects to the spine.
Exercises for strengthening the abdominal core muscles, including the muscles in the trunk, pelvis, lower back, hips, and abdomen, help stabilize the spine and protect it from excessive movement and compressive forces.
With spinal stenosis, the core muscles often become weak and inactive and unable to do their job to support the spine. Core exercises often begin by activating the deep abdominal muscles while lying flat on the back with the knees bent.
Exercises will progress as the individual gains more strength and control as the spine stabilizes.
Spinal stenosis physical therapy will also involve balance training and glute exercises for strengthening the leg muscles.
Prevention
Working with a physical therapist can help prevent future problems by maintaining spinal mobility, keeping the individual active, and exercising to maintain strength and stability to provide a solid foundation to support the lower back and prevent symptoms from worsening.
Severe Spinal Stenosis Physical Therapy
Physical therapy usually involves performing stretches for the lower back, hips, and legs, mobility exercises, and core strengthening exercises to improve spinal support and decrease pain. Treatments like heat or electrical stimulation may also be used on a case-by-case basis if there is significant pain or tightness in the back muscles. However, there is not enough clinical evidence to support that there are additional benefits. (Luciana Gazzi Macedo, et al., 2013) The effectiveness of physical therapy is high because surgery alone cannot strengthen the muscles that stabilize the spine, increase the mobility or flexibility of the surrounding muscles, and improve postural alignment.
The Root Causes of Spinal Stenosis
References
Lurie, J., & Tomkins-Lane, C. (2016). Management of lumbar spinal stenosis. BMJ (Clinical research ed.), 352, h6234. https://doi.org/10.1136/bmj.h6234
Mo, Z., Zhang, R., Chang, M., & Tang, S. (2018). Exercise therapy versus surgery for lumbar spinal stenosis: A systematic review and meta-analysis. Pakistan journal of medical sciences, 34(4), 879–885. https://doi.org/10.12669/pjms.344.14349
Macedo, L. G., Hum, A., Kuleba, L., Mo, J., Truong, L., Yeung, M., & Battié, M. C. (2013). Physical therapy interventions for degenerative lumbar spinal stenosis: a systematic review. Physical therapy, 93(12), 1646–1660. https://doi.org/10.2522/ptj.20120379
Individuals that have gone through a back injury may develop a synovial spinal cyst as a way to protect the spine that could cause pain symptoms and sensations. Can knowing the signs help healthcare providers develop a thorough treatment plan to relieve pain, prevent worsening of the condition and other spinal conditions?
Spinal Synovial Cysts
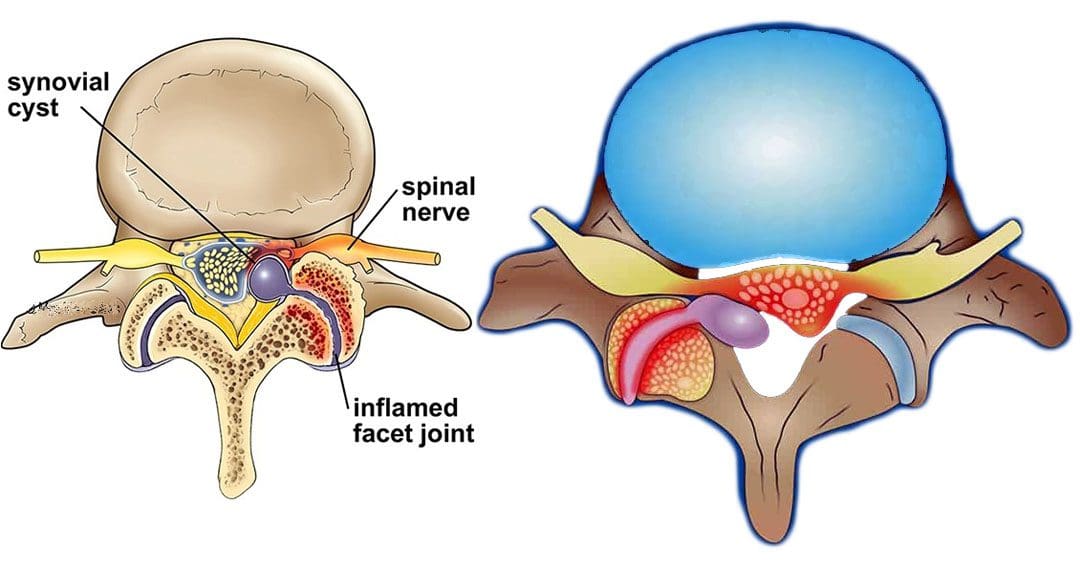
Spinal synovial cysts are benign fluid-filled sacs that develop in the spine’s joints. They form because of spinal degeneration or injury. The cysts can form anywhere in the spine, but most occur in the lumbar region/lower back. They typically develop in the facet joints or junctions that keep the vertebrae/spinal bones interlocked.
Symptoms
In most cases, synovial cysts don’t cause symptoms. However, the doctor or specialist will want to monitor for signs of degenerative disc disease, spinal stenosis, or cauda equina syndrome. When symptoms do present, they typically cause radiculopathy or nerve compression, which can cause back pain, weakness, numbness, and radiating pain caused by the irritation. The severity of symptoms depends on the size and location of the cyst. Synovial cysts can affect one side of the spine or both and can form at one spinal segment or at multiple levels.
Effects Can Include
Radiculopathy symptoms can develop if the cyst or inflammation caused by the cyst comes into contact with a spinal nerve root. This can cause sciatica, weakness, numbness, or difficulty controlling certain muscles.
Neurogenic claudication/impingement and inflammation of spinal nerves can cause cramping, pain, and/or tingling in the lower back, legs, hips, and buttocks. (Martin J. Wilby et al., 2009)
If the spinal cord is involved, it may cause myelopathy/severe spinal cord compression that can cause numbness, weakness, and balance problems. (Dong Shin Kim et al., 2014)
Symptoms related to cauda equina, including bowel and/or bladder problems, leg weakness, and saddle anesthesia/loss of sensation in the thighs, buttocks, and perineum, can present but are rare, as are synovial cysts in the middle back and neck. If thoracic and cervical synovial cysts develop, they can cause symptoms like numbness, tingling, pain, or weakness in the affected area.
Causes
Spinal synovial cysts are generally caused by degenerative changes like osteoarthritis that develop in a joint over time. With regular wear and tear, facet joint cartilage/the material in a joint that provides protection, a smooth surface, friction reduction, and shock absorption begins to waste away. As the process continues, the synovium can form a cyst.
Traumas, large and small, have inflammatory and degenerative effects on joints that can result in the formation of a cyst.
Around a third of individuals who have a spinal synovial cyst also have spondylolisthesis.
This condition is when a vertebrae slips out of place or out of alignment onto the vertebra underneath.
It is a sign of spinal instability.
Instability can occur in any spine area, but L4-5 are the most common levels.
This segment of the spine takes most of the upper body weight.
Epidural corticosteroid injections can reduce inflammation and could be an option to relieve pain.
Patients are recommended to receive no more than three injections per year.
Surgical Options
For severe or persistent cases, a doctor may recommend decompression surgery to remove the cyst and surrounding bone to relieve pressure on the nerve root. Surgical options range from minimally invasive endoscopic procedures to larger, open surgeries. The best surgical option varies based on the severity of the situation and whether associated disorders are present. Surgical options include:
Laminectomy – Removal of the bony structure that protects and covers the spinal canal/lamina.
Hemilaminectomy – A modified laminectomy where a smaller portion of the lamina is removed.
Facetectomy – The removal of part of the affected facet joint where the synovial cyst is located, usually following a laminectomy or hemilaminectomy.
Fusionof the facet joints and vertebra – Decreases vertebral mobility in the injured area.
Most individuals experience immediate pain relief following a laminectomy or hemilaminectomy.
Fusion can take six to nine months to heal completely.
If surgery is performed without fusion where the cyst originated, the pain could return, and another cyst could form within two years.
Surgery Complications include infection, bleeding, and injury to the spinal cord or nerve root.
How I Gained My Mobility Back With Chiropractic
References
Wilby, M. J., Fraser, R. D., Vernon-Roberts, B., & Moore, R. J. (2009). The prevalence and pathogenesis of synovial cysts within the ligamentum flavum in patients with lumbar spinal stenosis and radiculopathy. Spine, 34(23), 2518–2524. https://doi.org/10.1097/BRS.0b013e3181b22bd0
Kim, D. S., Yang, J. S., Cho, Y. J., & Kang, S. H. (2014). Acute myelopathy caused by a cervical synovial cyst. Journal of Korean Neurosurgical Society, 56(1), 55–57. https://doi.org/10.3340/jkns.2014.56.1.55
Epstein, N. E., & Baisden, J. (2012). The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surgical neurology international, 3(Suppl 3), S157–S166. https://doi.org/10.4103/2152-7806.98576
Individuals who have gone through recent low back surgery, like a lumbar laminectomy and discectomy, could they benefit from physical therapy for full recovery? (Johns Hopkins Medicine. 2008)
Rehabilitation Exercise Program
A lumbar laminectomy and discectomy is a surgical procedure performed by an orthopedic or neurologic surgeon to help decrease pain, relieve associated symptoms and sensations, and improve flexibility and mobility. The procedure involves cutting away disc and bone material that presses against, irritates, and damages the spinal nerves. (Johns Hopkins Medicine. 2023)
Post-Surgery
The therapist will work with the individual to develop a rehabilitation exercise program. The objective of a rehabilitation exercise program is to help the individual:
Relax their muscles to prevent muscle tensing and becoming over-cautious
Regain full range of motion
Strengthen their spine
Prevent injuries
A guide on what to expect in physical therapy.
Postural Retraining
After back surgery, individuals have to work to maintain proper posture when sitting and standing. (Johns Hopkins Medicine. 2008)
Postural control is important to learn as it maintains the lower back in the optimal position to protect and expedite the healing of lumbar discs and muscles.
A physical therapist will teach the individual how to sit with proper posture and use lumbar support.
Attaining and maintaining proper posture is one of the most important things to help protect the back and prevent future back problems.
Walking helps to improve cardiovascular health and blood circulation throughout the body.
This helps to provide added oxygen and nutrients to the spinal muscles and tissues as they heal.
It is an upright exercise that puts the spine in a natural position, which helps to protect the discs.
The therapist will help set up a program tailored to the individual’s condition.
Prone Press Up
One of the exercises to protect the back and lumbar discs is prone press-ups. (Johns Hopkins Medicine. 2008) This exercise helps keep the spinal discs situated in the proper position. It also helps to improve the ability to bend back into lumbar extension.
To perform the exercise:
Lie facing down on a yoga/exercise mat and place both hands flat on the floor under the shoulders.
Keep the back and hips relaxed.
Use the arms to press the upper part of the body up while allowing the lower back to remain against the floor.
There should be a slight pressure in the lower back while pressing up.
Hold the press-up position for 2 seconds.
Slowly lower back down to the starting position.
Repeat for 10 to 15 repetitions.
Sciatic Nerve Gliding
Individuals who had leg pain coming from the back prior to surgery may have been diagnosed with sciatica or an irritation of the sciatic nerve. Post-surgery, individuals may notice their leg feels tight whenever straightening it out all the way. This could be a sign of an adhered/trapped sciatic nerve root, a common problem with sciatica.
After lumbar laminectomy and discectomy surgery, a physical therapist will prescribe targeted exercises called sciatic nerve glides to stretch and improve how the nerve moves. (Richard F. Ellis, Wayne A. Hing, Peter J. McNair. 2012)
Nerve glides can help free the stuck nerve root and allow for normal motion.
To perform the exercise:
Lie on the back and bend one knee up.
Grab underneath the knee with the hands.
Straighten the knee while supporting it with the hands.
Once the knee is fully straightened, flex and extend the ankle about 5 times.
Return to the starting position.
Repeat the sciatic nerve glide 10 times.
The exercise can be performed several times to help improve how the nerve moves and glides in the lower back and leg.
Supine Lumbar Flexion
After surgery, gentle back flexion exercises can help safely stretch the low-back muscles and gently stretch the scar tissue from the surgical incision. Supine lumbar flexion is one of the simplest exercises to improve lumbar flexion range of motion.
To perform the exercise:
Lie on the back with the knees bent.
Slowly lift the bent knees towards the chest and grasp the knees with both hands.
Gently pull the knees toward the chest.
Hold the position for 1 or 2 seconds.
Slowly lower the knees back to the starting position.
Perform for 10 repetitions.
Stop the exercise if experiencing an increase in pain in the lower back, buttocks, or legs.
Hip and Core Strengthening
Once cleared, individuals can progress to an abdominal and core strengthening program. This involves performing specific motions for the hips and legs while maintaining a pelvic neutral position. Advanced hip strengthening exercises help generate strength and stability in the muscles that surround the pelvic area and lower back. A physical therapist can help decide which exercises are recommended for the specific condition.
Return-to-Work and Physical Activities
Once individuals have gained an improved lumbar range of motion, hip, and core strength, their doctor and therapist may recommend working on specific activities to help them return to their previous level of work and recreation. Depending on job occupation, individuals may need to:
Work on proper lifting techniques.
Require an ergonomic evaluation if they spend time sitting at a desk or workstation.
Some surgeons may have restrictions on how much an individual can bend, lift, and twist from two to six weeks after surgery.
Low-back surgery can be difficult to rehab properly. Working with a healthcare provider and physical therapist, individuals can be sure to improve their range of motion, strength, and functional mobility to return to their previous level of function quickly and safely.
Ellis, R. F., Hing, W. A., & McNair, P. J. (2012). Comparison of longitudinal sciatic nerve movement with different mobilization exercises: an in vivo study utilizing ultrasound imaging. The Journal of orthopaedic and sports physical therapy, 42(8), 667–675. https://doi.org/10.2519/jospt.2012.3854
Individuals feeling tingling or pins and needles sensations that overtake the arms or legs could be experiencing paresthesia, which occurs when a nerve has been compressed or damaged. Can knowing the symptoms and causes help in diagnosis and treatment?
Paresthesia Body Sensations
The numbness or tingling feeling when an arm, leg, or foot has fallen asleep is not so much about blood circulation but nerve function.
Paresthesia is an abnormal sensation felt in the body due to the compression or irritation of nerves.
It can be a mechanical cause like a compressed/pinched nerve.
Or it may be due to a medical condition, injury, or illness.
The symptoms typically last for 30 minutes or less.
Shaking the affected limb often relieves the sensations.
Paresthesia usually affects only one arm or leg at a time.
However, both arms and legs can be affected, depending on the cause.
Consult a healthcare provider if the symptoms last for more than 30 minutes. Treatment may be required if paresthesia body sensations are brought on by a serious underlying cause.
Causes
Sitting with incorrect and unhealthy postures can compress a nerve and generate symptoms. However, some causes are more concerning and can include:
If the symptoms don’t go away after 30 minutes or keep returning for unknown reasons, call a healthcare provider to find out what is causing the abnormal sensations. A worsening case should be monitored by a healthcare provider.
Peripheral neuropathy caused by diabetes usually begins with a feeling of paresthesia in the foot/feet and can worsen and lead to other complications.
A healthcare provider will work with the individual to understand the symptoms and perform the appropriate diagnostic tests to determine the cause. A healthcare provider will choose the tests based on a physical examination. Common diagnostic procedures include: (Merck Manual Professional Version. 2022)
Magnetic resonance imaging – MRI of the spine, brain, or extremities.
X-ray to rule out bone abnormalities, like a fracture.
Blood tests.
Electromyography – EMG studies.
Nerve conduction velocity – NCV test.
If paresthesia is accompanied by back or neck pain, a healthcare provider may suspect a compressed/pinched spinal nerve.
If the individual has a history of diabetes that is poorly controlled, they may suspect peripheral neuropathy.
Treatment
Treatment for paresthesia depends on the diagnosis. A healthcare provider can help determine the best course of action for the specific condition.
Nervous System
If symptoms are triggered by a central nervous condition like MS, individuals will work closely with their healthcare provider to get the appropriate treatment.
If paresthesia is caused by compression of a spinal nerve, like sciatica, individuals may be referred to a chiropractor and physical therapy team to release the nerve and pressure. (Julie M. Fritz, et al., 2021)
A physical therapist may prescribe spinal exercises to relieve compression of the nerve and restore normal sensations and motion.
Strengthening exercises to restore flexibility and mobility may be prescribed if weakness presents along with paresthesia body sensations.
Herniated Disc
If a herniated disc is causing the abnormal sensations, and there has been no improvement with conservative measures, a healthcare provider may suggest surgery to relieve pressure on the nerve/s. (American Association of Neurological Surgeons. 2023)
In surgical procedures like a laminectomy or discectomy, the objective is to restore nerve function.
Post-surgery, individuals may be recommended to a physical therapist to help regain mobility.
National Institute of Neurological Disorders and Stroke. (2023) Paresthesia.
American Association of Neurological Surgeons. (2023) Herniated disc.
National Institute of Diabetes and Digestive and Kidney Diseases. (2018) Peripheral neuropathy.
Merck Manual Professional Version. (2022) Numbness.
Razazian, N., Yavari, Z., Farnia, V., Azizi, A., Kordavani, L., Bahmani, D. S., Holsboer-Trachsler, E., & Brand, S. (2016). Exercising Impacts on Fatigue, Depression, and Paresthesia in Female Patients with Multiple Sclerosis. Medicine and science in sports and exercise, 48(5), 796–803. https://doi.org/10.1249/MSS.0000000000000834
Fritz, J. M., Lane, E., McFadden, M., Brennan, G., Magel, J. S., Thackeray, A., Minick, K., Meier, W., & Greene, T. (2021). Physical Therapy Referral From Primary Care for Acute Back Pain With Sciatica : A Randomized Controlled Trial. Annals of internal medicine, 174(1), 8–17. https://doi.org/10.7326/M20-4187
Can combining chiropractic treatment with the common therapies of medication, exercise, and/or physical therapy help relieve sciatic endometriosis pain symptoms?
Sciatic Endometriosis
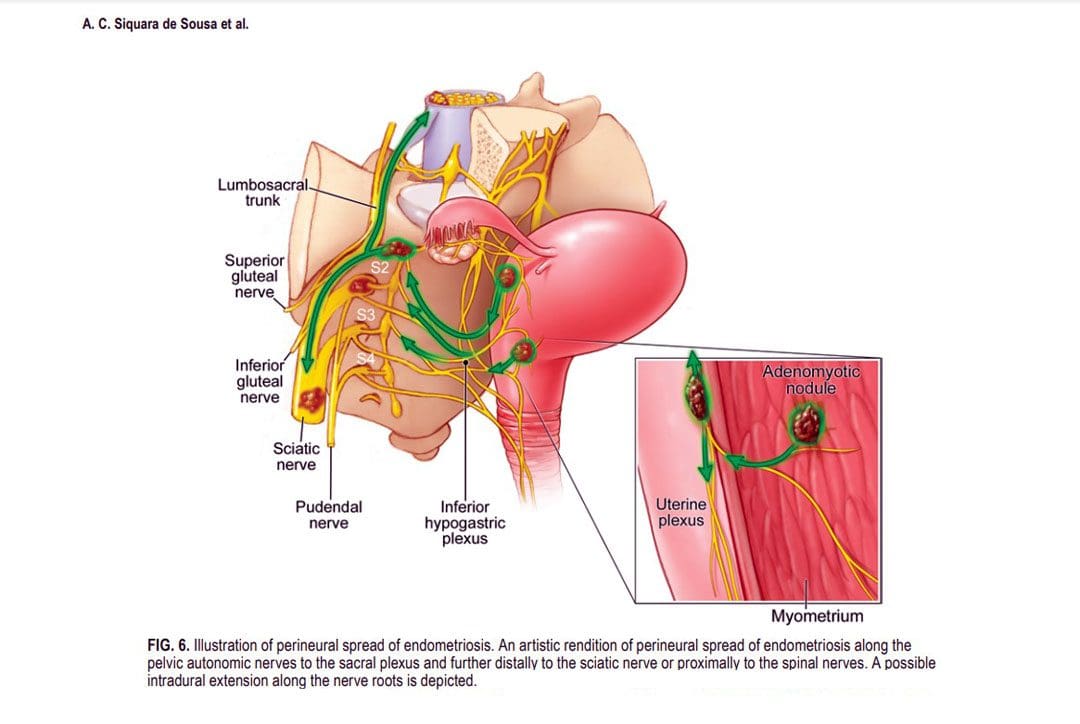
Sciatic endometriosis is a condition in which endometrial cells (tissue that resembles the lining of the uterus) grow outside of the uterine lining and compress the sciatic nerve. This places stress and pressure on the nerve causing back, pelvic, hip, and leg pain, especially before and during the menstrual cycle. It can also cause pain, irregular periods, and infertility. (The American College of Obstetricians and Gynecologists. 2021)
These areas of endometrial tissue growth are also known as lesions or implants.
Women with sciatic endometriosis often experience leg pain and weakness around the time of their menstrual cycle. (Lena Marie Seegers, et al., 2023)
Sciatic endometriosis can also cause pain when urinating, during a bowel movement, during sex, and fatigue, and irregular vaginal bleeding.
The abnormal growth may be caused by higher-than-normal levels of estrogen.
Researchers believe that endometriosis is related to retrograde menstruation, which causes menstrual blood to flow back into the pelvis instead of out through the vagina. (World Health Organization. 2023)
Sometimes, the cells grow in the area of the pelvis right above the sciatic nerve. (Adaiah Yahaya, et al., 2021)
The sciatic nerve is the longest nerve in the body and travels down the back of each leg. (Johns Hopkins Medicine. 2023)
When endometrial lesions place pressure on the sciatic nerve, they can cause irritation and inflammation leading to severe pelvic pain, which makes it harder to conceive. (Liang Yanchun, et al., 2019)
Symptoms
Some women with endometriosis experience no symptoms or misinterpret the symptoms as typical premenstrual syndrome/PMS signs. The most common signs and symptoms of sciatic endometriosis include:
Difficulty walking or standing.
Loss of sensation, muscle weakness, and reflex alteration.
Limping.
Balance problems.
Bloating and nausea.
Constipation or diarrhea before or after a period.
Painful, heavy, and/or irregular periods.
Bleeding between periods.
Pain during sex, urination, and bowel movements.
Pain in the stomach, pelvis, lower back, hips, and buttocks. (MedlinePlus. 2022)
Weakness, numbness, tingling, burning, or dull aching sensations in the back of one or both legs.
Endometriosis, including sciatic endometriosis, typically cannot be diagnosed with a pelvic examination or ultrasound by themselves. A healthcare provider may need to perform a biopsy using laparoscopy and discuss menstrual cycles, symptoms, and medical history.
The laparoscopy procedure involves making tiny incisions and taking a tissue sample with tools attached to a thin tube with a camera. (MedlinePlus. 2022)
Imaging tests, like magnetic resonance imaging/MRI, and computed tomography/CT scans, can help provide essential information about the location and size of any endometrial lesions. (The American College of Obstetricians and Gynecologists. 2021)
Treatment
Symptoms can sometimes be temporarily relieved with over-the-counter/OTC pain relievers. Depending on the condition and severity a healthcare provider may prescribe hormonal treatment to prevent new endometrial implants from growing. These can include:
Hormonal birth control.
Progestin – a synthetic form of progesterone.
Gonadotropin-releasing hormone – GnRH agonists.
If pain persists or worsens, individuals may need to undergo surgery to remove the tissue.
The American College of Obstetricians and Gynecologists. Endometriosis.
Seegers, L. M., DeFaria Yeh, D., Yonetsu, T., Sugiyama, T., Minami, Y., Soeda, T., Araki, M., Nakajima, A., Yuki, H., Kinoshita, D., Suzuki, K., Niida, T., Lee, H., McNulty, I., Nakamura, S., Kakuta, T., Fuster, V., & Jang, I. K. (2023). Sex Differences in Coronary Atherosclerotic Phenotype and Healing Pattern on Optical Coherence Tomography Imaging. Circulation. Cardiovascular imaging, 16(8), e015227. https://doi.org/10.1161/CIRCIMAGING.123.015227
World Health Organization. Endometriosis.
Yahaya, A., Chauhan, G., Idowu, A., Sumathi, V., Botchu, R., & Evans, S. (2021). Carcinoma arising within sciatic nerve endometriosis: a case report. Journal of surgical case reports, 2021(12), rjab512. https://doi.org/10.1093/jscr/rjab512
Johns Hopkins Medicine. Sciatica.
Yanchun, L., Yunhe, Z., Meng, X., Shuqin, C., Qingtang, Z., & Shuzhong, Y. (2019). Removal of an endometrioma passing through the left greater sciatic foramen using a concomitant laparoscopic and transgluteal approach: case report. BMC women’s health, 19(1), 95. https://doi.org/10.1186/s12905-019-0796-0
MedlinePlus. Endometriosis.
Center for Endometriosis Care. Sciatic endometriosis.
Chen, S., Xie, W., Strong, J. A., Jiang, J., & Zhang, J. M. (2016). Sciatic endometriosis induces mechanical hypersensitivity, segmental nerve damage, and robust local inflammation in rats. European journal of pain (London, England), 20(7), 1044–1057. https://doi.org/10.1002/ejp.827
Siquara de Sousa, A. C., Capek, S., Howe, B. M., Jentoft, M. E., Amrami, K. K., & Spinner, R. J. (2015). Magnetic resonance imaging evidence for perineural spread of endometriosis to the lumbosacral plexus: report of 2 cases. Neurosurgical focus, 39(3), E15. https://doi.org/10.3171/2015.6.FOCUS15208
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine