Can understanding the mechanics of the throwing motion help to understand why it may cause shoulder pain, the symptoms of a shoulder problem, the diagnosis, and the treatment options available?
Throwing a Ball and Shoulder Pain
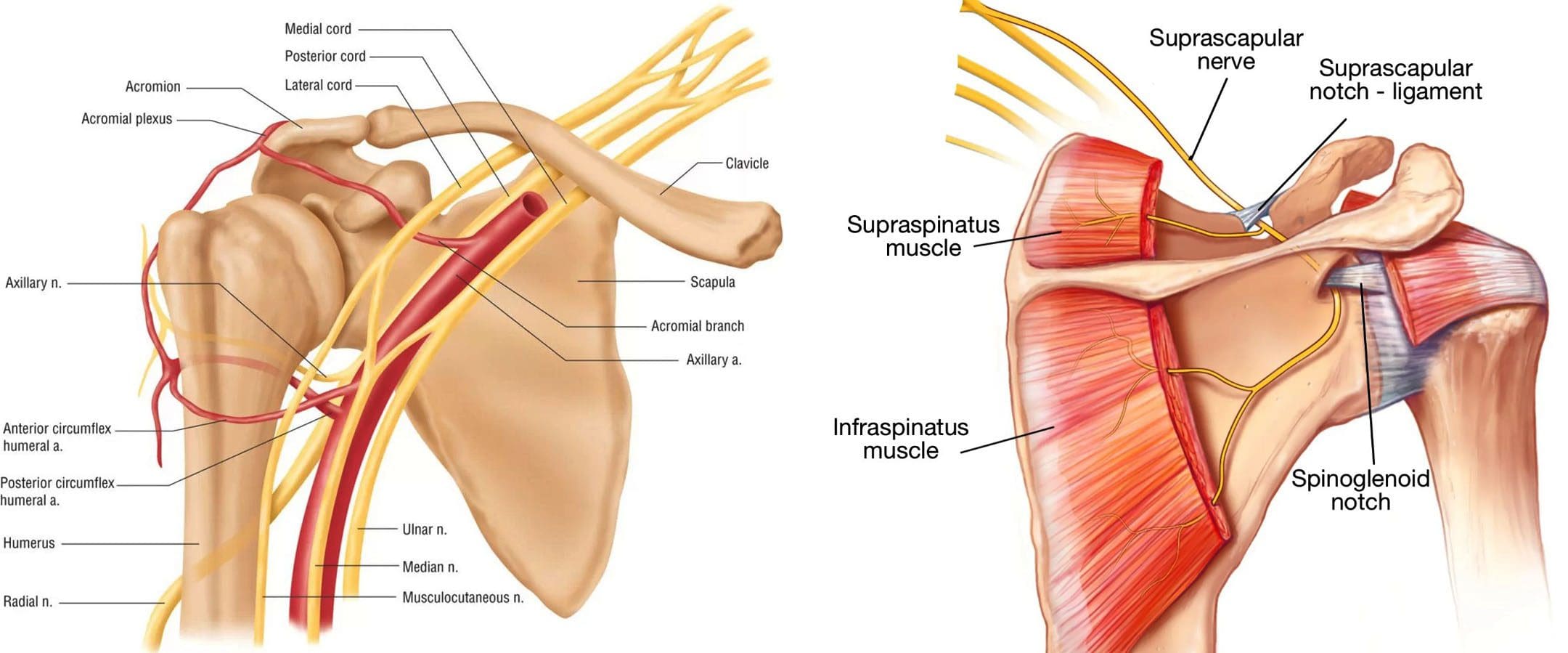
The throwing motion is a complex shoulder movement that requires the mechanics of muscles, tendons, joints, ligaments, and bones. They all must move in a synchronized and stable pattern to move the shoulder joint. When these mechanics are interrupted or altered, inflammation can result in pain symptoms. (Wardell M., Creighton D., & Kovalcik C., 2022)
The labrum stabilizes the ball in the socket of the shoulder.
The shoulder blade rotation coordinates with the arm to ensure mobility. (Itoigawa Y. et al., 2023)
The throwing motion generates high torque and acceleration forces acting on the shoulder joint and the surrounding muscles, ligaments, and tendons.
Causes of Pain
Pain when throwing can come from the:
Shoulder blade
Shoulder joint – cartilage and labrum
Rotator cuff muscles and tendons
Nerves that control the muscles’ function
The shoulder blade is attached to the upper back by ligaments, muscles, and tendons. The various muscles and tendons that control the movement of the shoulder blade impact movements. Abnormalities of any area can lead to shoulder dysfunction and pain when throwing. (Wardell M., Creighton D., & Kovalcik C., 2022) The most common is the tightness of the posterior shoulder capsule, causing a loss of normal internal rotation of the shoulder. If this is causing pain, individuals may notice that they can’t reach up as high on the side with the painful shoulder when reaching behind their back.
Symptoms
Whether an athlete or playing catch in the backyard, shoulder function abnormalities can cause significant pain. Some symptoms include.
Aching Pain
Often deep in the shoulder or extending down the upper arm.
Dead Arm
Lack of strength in the throwing motion.
Pain at Night
Pain can awaken you from sleep.
Diagnosis
Finding a healthcare provider familiar with sports injuries can be helpful. They can best determine if a structural abnormality needs to be addressed. (American Academy of Orthopaedic Surgeons, 2021)
Treatment
Most can improve with nonsurgical treatments. The earliest phase of treatment is resting the joint and reducing inflammation. Treatments can include:
Ice
Anti-inflammatory medications
Cortisone injection
Once the inflammation has subsided, the source of the discomfort can be addressed.
Physical Therapy
Therapy can include:
A structured shoulder stretching and strengthening program will help.
The physical therapist will focus on scapular mobility when managing shoulder joint problems.
Stretching to improve internal rotation or any other lost motion can help allow a more normal throwing motion.
Strength exercises are often aimed at the rotator cuff, as these muscles initiate proper shoulder movements and stabilize the shoulder joint.
Maintaining flexibility and strength of the periscapular muscles (muscles that attach to the scapula bone) is important to ensure that the scapular movements are coordinated with the throwing motion.
If improvements are not made within three months of therapy, or individuals can’t return to competitive sports within six months. In that case, the individual may need to return to their healthcare provider or see an orthopedic specialist who may recommend surgery. (American Academy of Orthopaedic Surgeons, 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
As a Family Practice Nurse Practitioner, Dr. Jimenez combines advanced medical expertise with chiropractic care to address various conditions.
Wellness & Nutrition: Personalized plans to optimize health and prevent disease.
Chronic Pain Management: Non-invasive solutions for fibromyalgia, sciatica, and low back pain.
Personal Injury & Auto Accident Care: Tailored rehabilitation for whiplash, soft tissue injuries, and more.
Sports Injuries & Orthopedic Care: Treatment for sprains, strains, and complex injuries.
Functional Medicine: Root-cause analysis for chronic disorders, incorporating nutrition, lifestyle, and environmental factors.
Neuromusculoskeletal Health: Care for neck pain, migraines, herniated discs, and scoliosis.
Our clinic integrates Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine to create customized care plans that promote natural healing, mobility, and long-term wellness. By focusing on flexibility, agility, and strength, we empower patients to thrive, regardless of age or health challenges.
At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately focus on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities. We use in-person and virtual health coaching and comprehensive care plans to ensure every patient’s personalized care and wellness outcomes.
Lumbar Spine Injuries in Sports: Chiropractic Healing
References
Wardell, M., Creighton, D., & Kovalcik, C. (2022). Glenohumeral Instability and Arm Pain in Overhead Throwing Athletes: A Correlational Study. International journal of sports physical therapy, 17(7), 1351–1357. https://doi.org/10.26603/001c.39800
Itoigawa, Y., Koga, A., Morikawa, D., Kubota, A., Uehara, H., Maruyama, Y., Takazawa, Y., & Ishijima, M. (2023). Posterior shoulder stiffness was associated with shoulder pain during throwing in college baseball players: assessment of shear wave elastography. European journal of orthopaedic surgery & traumatology: orthopedie traumatologie, 33(4), 1237–1244. https://doi.org/10.1007/s00590-022-03286-z
American Academy of Orthopaedic Surgeons. (2021). Shoulder Injuries in the Throwing Athlete. https://orthoinfo.aaos.org/en/diseases–conditions/shoulder-injuries-in-the-throwing-athlete/
American Academy of Orthopaedic Surgeons. (2024). Shoulder Impingement/Rotator Cuff Tendinitis. https://orthoinfo.aaos.org/en/diseases–conditions/shoulder-impingementrotator-cuff-tendinitis
Dr. Alex Jimenez: Pioneering Integrative Care as a Chiropractor and Nurse Practitioner
Dr. Alex Jimenez, a licensed chiropractor and board-certified nurse practitioner based in El Paso, Texas, brings over 25 years of expertise to his Injury Medical & Chiropractic Clinic practice. His dual licensure provides unique insights into the etiologies, pathogenesis, and treatment of complex clinical conditions, enabling him to deliver patient-centered, integrative care that bridges physical medicine, functional medicine, and advanced diagnostics. Combining chiropractic expertise with nurse practitioner-driven medical management, Dr. Jimenez offers comprehensive treatment protocols tailored to acute and chronic conditions, promoting metabolic resilience, longevity, and whole-person wellness.
Dual Expertise: Chiropractic and Nurse Practitioner Roles
Dr. Jimenez’s practice stands out due to his ability to integrate the biomechanical focus of chiropractic care with a nurse practitioner’s diagnostic and therapeutic scope. As a chiropractor, he specializes in restoring musculoskeletal function, particularly after trauma, neck, back, spine, and soft tissue injuries. His chiropractic interventions emphasize non-invasive techniques, such as spinal decompression, manual adjustments, and functional rehabilitation, to alleviate pain and enhance mobility.
As a board-certified nurse practitioner, Dr. Jimenez employs evidence-based medicine to address systemic and metabolic dysfunctions. His expertise extends to managing chronic degenerative disorders, hormonal imbalances, weight loss, sexual health, and pain syndromes. This dual perspective allows him to identify underlying disease causes, from biomechanical misalignments to physiological imbalances, and design treatment regimens that address symptoms and root causes.
The synergy of these roles enables Dr. Jimenez to offer a holistic approach that is particularly effective for complex conditions such as sciatica, fibromyalgia, disc herniation, spondylolisthesis, and chronic neck or back pain. His integrative protocols combine functional medicine assessments, lifestyle interventions, and advanced diagnostics to achieve homeostasis and physiological balance.
Treatment Protocols: Evidence-Based and Patient-Centered
Drawing from integrative protocols outlined on his website, www.chiromed.com, Dr. Jimenez employs a multidisciplinary approach to patient care. His treatment plans are grounded in evidence-based medicine, functional medicine, and lifestyle wellness strategies, tailored to each patient’s unique health profile, lifestyle, and medical history. Below are key components of his integrative care model:
1. Chiropractic Care and Functional Rehabilitation
Spinal Decompression: Non-surgical decompression therapy is used to relieve pressure on spinal discs, addressing conditions like disc herniation, sciatica, and spinal stenosis. This modality promotes healing by improving blood flow and nutrient delivery to affected areas.
Manual Adjustments: Targeted adjustments correct spinal misalignments, reduce nerve compression, and restore joint mobility. These are particularly effective for whiplash, scoliosis, and poor posture.
Functional Strength Training: Dr. Jimenez designs conditioning programs to enhance recovery and prevent re-injury. These programs are tailored for athletes and individuals seeking optimal performance and incorporate mobility, flexibility, and agility training.
2. Functional Medicine Assessments
Functional medicine tools evaluate metabolic, hormonal, and nutritional status. These assessments identify the root causes of conditions such as fatigue, weight gain, or chronic pain, enabling precise interventions.
Advanced diagnostic protocols, including blood panels and imaging, provide data-driven insights into etiologies and pathogenesis. This allows Dr. Jimenez to address underlying dysfunctions rather than merely masking symptoms.
3. Lifestyle and Nutritional Interventions
Weight Loss and Metabolic Resilience: Dr. Jimenez integrates nutritional counseling and metabolic optimization strategies to support sustainable weight loss and prevent chronic diseases like diabetes or cardiovascular disorders.
Hormone and Sexual Health: Personalized regimens address hormonal imbalances and sexual dysfunction, improving quality of life and overall wellness.
Pain Management: Nutritional and lifestyle modifications complement physical therapies to manage chronic pain syndromes, reducing reliance on pharmaceuticals.
4. Specialized Care for Complex Conditions
Sciatica and Disc Injuries: Dr. Jimenez employs targeted decompression and rehabilitation protocols to alleviate nerve compression and restore function.
Chronic Degenerative Disorders: Conditions like fibromyalgia, arthritis, and spondylolisthesis are managed through integrative plans that combine physical therapy, nutritional support, and metabolic optimization.
Sports and Auto Accident Injuries: Tailored rehabilitation programs address soft tissue damage, shoulder injuries, and whiplash, ensuring rapid recovery and long-term resilience.
5. Advanced Wellness Programs
Dr. Jimenez’s clinic offers comprehensive wellness programs on longevity, skin care, and hair loss. These programs integrate nutritional supplementation, lifestyle coaching, and cutting-edge therapies to promote vitality and aesthetic health.
High-level conditioning programs optimize performance for athletes, incorporating functional strength training and recovery-focused interventions.
Integrative Team and Clinic Highlights
Injury Medical & Chiropractic Clinic is El Paso’s largest mobility, flexibility, and agility center, integrating chiropractors, nurse practitioners, registered nurses, nutritionists, and physical performance trainers. The clinic’s multidisciplinary team collaborates to deliver personalized care, ensuring patients achieve measurable health outcomes. Key services include:
Acupuncture: A Complementary therapy to reduce pain and promote relaxation.
Advanced Nutritional Programs: Evidence-based dietary plans to support metabolic health and recovery.
Physical Performance Training: Programs to enhance fitness, prevent injuries, and optimize athletic performance.
The clinic accepts major insurances, including Aetna, Blue Cross Blue Shield, Cigna, and First Health, making care accessible to a broad patient base.
Insights from Dual Licensure
Dr. Jimenez’s licensure as both a chiropractor and nurse practitioner provides him with a comprehensive understanding of disease processes and treatment modalities. His chiropractic training equips him to address biomechanical dysfunctions, while his nurse practitioner expertise allows him to manage systemic conditions with a medical lens. This dual perspective enhances his ability to:
Clarify Etiologies: By combining musculoskeletal assessments with metabolic and hormonal evaluations, Dr. Jimenez identifies multifactorial causes of conditions, ensuring targeted interventions.
Understand Pathogenesis: His knowledge of disease progression informs proactive treatment plans that halt or reverse degenerative processes.
Design Appropriate Regimens: Integrating physical, nutritional, and medical therapies, Dr. Jimenez creates synergistic treatment plans that address both symptoms and underlying dysfunctions.
This integrative approach is particularly valuable for patients with chronic or multifactorial conditions, as it addresses the interplay between physical, metabolic, and lifestyle factors.
Patient-Centered Care: In-Person and Online
Dr. Jimenez’s practice emphasizes personalized attention, whether patients visit in person at 11860 Vista Del Sol, Suite 128, El Paso, TX 79936, or engage through telehealth. His functional medicine series, accessible via www.dralexjimenez.com, educates patients on holistic health principles, covering topics from spinal health to metabolic optimization. The website features:
Informative Content: Blog posts, articles, and videos provide insights into chiropractic care, functional medicine, and injury rehabilitation.
Patient Testimonials: Success stories highlight the transformative impact of Dr. Jimenez’s care, showcasing outcomes for conditions like sciatica, sports injuries, and chronic pain.
Appointment Booking: A user-friendly interface allows patients to schedule in-person or online consultations, with clear guidance on what to expect during their first visit.
Commitment to Education and Community Health
Dr. Jimenez is dedicated to empowering patients through education. His website is comprehensive, offering evidence-based information on health conditions, treatment options, and wellness strategies. By fostering health literacy, Dr. Jimenez enables patients to make informed decisions and take charge of their well-being.
His commitment extends to the El Paso community, where he aims to expand access to integrative care. Dr. Jimenez promotes proactive health management and preventive care through workshops, online content, and community outreach.
Conclusion
Dr. Alex Jimenez’s dual expertise as a chiropractor and nurse practitioner positions him as a leader in integrative medicine. His ability to bridge physical medicine with systemic health management allows him to address complex clinical issues with precision and compassion. Dr. Jimenez delivers personalized care that promotes healing, resilience, and longevity by leveraging evidence-based protocols, advanced diagnostics, and lifestyle interventions.
For more information or to schedule an appointment, visit www.dralexjimenez.com or contact the clinic at +1-915-412-6677.
What is a bone density test, how is it performed, and what do the results mean?
Bone Density Test
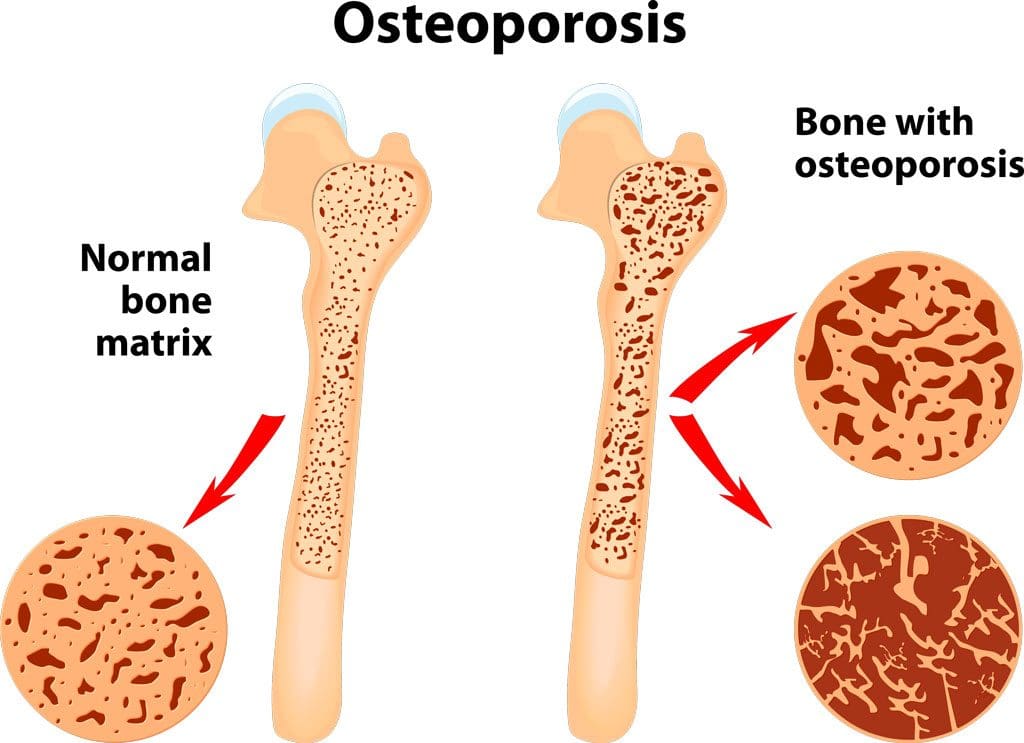
A bone density test examines bone mass, which indicates overall bone strength. Assessing bone density or mass is necessary for diagnosing osteopenia or osteoporosis, conditions that increase the risk of broken bones. The scan is performed through dual-energy X-ray absorptiometry (DEXA), which examines the thickness of the bones. Results from DEXA scans are compared to standardized values to determine whether bone density is lower than normal and whether osteopenia or osteoporosis is present.
Examination
The procedure examines bone density, or bone mass. The bones’ density, or mass, is an overall indicator of bone strength. The greater the bone density, the thicker and stronger the bones are. The test is used to diagnose osteoporosis, a condition characterized by brittle bones at risk of breaking due to significantly low bone density. A bone density test can also diagnose osteopenia, a condition characterized by lower than normal bone mass that can lead to osteoporosis. (National Institute of Arthritis and Musculoskeletal and Skin Diseases, 2025) It is recommended that all women aged 65 and older and all men aged 70 and older have a bone density scan to screen for bone loss to help prevent fractures. (Kling J. M., Clarke B. L., & Sandhu N. P. 2014)
Bone density scans can establish a baseline level of bone density and track changes over time.
For individuals with osteoporosis or osteopenia, a bone density scan can help track how well their bones respond to treatment.
During a DEXA scan, the patient will lie on their back on a table with their legs elevated on a padded platform.
An X-ray scanner will pass over the spine and hips while another scans beneath.
While the scan takes place, the patient will be asked to hold very still to obtain an accurate image.
The scan will obtain bone density readings from the spine and hip, the two most commonly fractured bones, and generally takes less than 30 minutes.
Results
A DEXA scan measures bone density in grams per centimeter squared (g/cm²). This number indicates how densely bone cells are packed together in a specific area of bone. This bone density reading is then compared to a standardized value to determine if bone density is within a normal range or lower than average.
Between minus 1.0 and minus 2.5: Low bone density (osteopenia)
Equal to minus 2.5 or below: Osteoporosis
Bone density values are reported as a Z score for women who have not undergone menopause and men under 50 years old.
Z scores are compared to bone density levels of individuals of the same age and sex.
A Z score of minus 2.0 or lower indicates low bone density, which can be caused by factors other than aging, such as medication side effects, nutritional deficiencies, or thyroid problems.
Arthritis Diagnosis
Because a DEXA scan only measures the thickness of bones, it doesn’t work to diagnose arthritis. An X-ray of the affected joint is currently the most accurate way to diagnose arthritis. The Kellgren-Lawrence classification system categorizes the extent of arthritis based on the severity of joint damage seen on an X-ray. According to this system, arthritis can be classified as: (Kohn M. D., Sassoon A. A., & Fernando N. D. 2016)
Grade 1 (minor)
Minimal or no joint space narrowing, with possible bone spur formation.
Grade 2 (mild)
Possible joint space narrowing, with definite bone spur formation.
Grade 3 (moderate)
Definite joint space narrowing, moderate bone spur formation, mild sclerosis (abnormal thickening of bone), and possible deformation of bone ends.
Grade 4 (severe)
Severe joint space narrowing, large bone spur formation, marked sclerosis, and definite deformation of bone ends.
Injury Medical Chiropractic & Functional Medicine Clinic
Exercise can be incredibly beneficial for improving bone density, joint mobility, and the strength of surrounding muscles, which support and protect joints and bones. Talk to a healthcare provider to learn what interventions and available treatment options would be the most effective. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Osteoporosis
References
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2025). Bone mineral density tests: what the numbers mean. Retrieved from https://www.niams.nih.gov/health-topics/bone-mineral-density-tests-what-numbers-mean
Kling, J. M., Clarke, B. L., & Sandhu, N. P. (2014). Osteoporosis prevention, screening, and treatment: a review. Journal of women’s health (2002), 23(7), 563–572. https://doi.org/10.1089/jwh.2013.4611
Kohn, M. D., Sassoon, A. A., & Fernando, N. D. (2016). Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clinical orthopaedics and related research, 474(8), 1886–1893. https://doi.org/10.1007/s11999-016-4732-4
Can adding fartlek training improve speed and endurance for runners and running enthusiasts?
Running Fartlek Training
Fartlek training, which means speed play in Swedish, is a form of running training that involves alternating between bursts of fast running and slower recovery jogging.
It is a form of interval or speed conditioning.
It involves varying one’s pace throughout their run, alternating between fast treks and slow jogs.
Workouts are unstructured and allow runners to decide the duration and intensity of the fast and slow sections.
Unlike formal interval training, this flexibility offers a new way to improve speed, endurance, mental preparedness, and stamina.
Training Benefits
Traditional interval training uses specific timed or measured segments. Fartleks are more unstructured, with work-rest intervals based on how the body feels. With fartlek training, individuals can experiment with pace and endurance as they run, which helps them tune in to their body and adjust how it performs. Many runners enjoy the training because it involves speed work and is more flexible and less demanding.
A stopwatch is not needed for time intervals.
Training doesn’t have to be done on a track and can be performed on all terrain, such as roads, trails, or hills.
The training stresses the body’s systems, leading to faster speeds and improving anaerobic threshold. (Bacon, A. P. et al., 2013)
Improves the anaerobic threshold and increases the body’s ability to train longer at higher intensities. (Mazurek K. et al., 2016)
This is due to an increased VO2 max, which measures how much oxygen the body can take in and use.
Training includes a higher risk of injury and strain.
Beginners are more prone to shin splints.
The training is demanding, so it should not be done daily.
Workout
The method is to vary brief periods of slightly higher pace into regular runs (Kumar P. 2015). Maintain a faster pace for a short distance or time interval, such as 200 meters or 30 seconds. Intervals can vary throughout the workout, and landmarks such as streetlights or telephone poles can be used to mark segments instead of measuring miles or meters. Once a fast segment is completed, slow to below-normal running cadence until the body fully recovers and breathing returns to normal. Return to running normally and incorporate slightly faster intervals later in the run.
Fartleks should be short because they are intense.
The actual higher-pace portion of the run should last up to 30 seconds.
Gradually add more time to the faster-paced portion as conditioning improves, up to 60 seconds.
Training Example
An example of a 40- to 45-minute fartlek workout suitable for beginners.
10-minute warm-up at a light pace
1 minute on (fast pace)
2 minutes off (easy)
2 minutes on
1 minute off
Repeat the set 3 to 4 times
10-minute cooldown at an easy pace
Remember that beginners should go slow when introducing fartlek training into their workouts. It is more intense and can increase the risk of injuries and strains, such as shin splints. Get help from a running coach or trainer if you are unsure how to incorporate the training into your routine.
Training on a Treadmill
Speed play can be done on a treadmill. The idea is to find ways to create speed variation intervals and help relieve treadmill boredom. Some examples include:
If watching television, use commercials to go into speed intervals.
At the gym, make a game out of the sprints and/or
Speed up during certain parts of songs where you can feel the energy moving you faster.
One precaution is learning to use the treadmill’s buttons to increase and decrease the pace. This can slow you down and disrupt form, so maybe do longer durations for each phase so there is less contact with the control panel.
Injury Medical Chiropractic & Functional Medicine Clinic
Fartlek training is an excellent way to add variety, fun, and interest to running. This speed work can also enhance performance, increase cardiovascular output, and allow individuals to run at higher intensities for longer periods. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. We can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Building a Stronger Body
References
Bacon, A. P., Carter, R. E., Ogle, E. A., & Joyner, M. J. (2013). VO2max trainability and high-intensity interval training in humans: a meta-analysis. PloS one, 8(9), e73182. https://doi.org/10.1371/journal.pone.0073182
Mazurek, K., Zmijewski, P., Krawczyk, K., Czajkowska, A., Kęska, A., Kapuściński, P., & Mazurek, T. (2016). High-intensity interval and moderate continuous cycle training in a physical education programme improves health-related fitness in young females. Biology of Sport, 33(2), 139–144. https://doi.org/10.5604/20831862.1198626
Scribbans, T. D., Vecsey, S., Hankinson, P. B., Foster, W. S., & Gurd, B. J. (2016). The Effect of Training Intensity on VO2max in Young Healthy Adults: A Meta-Regression and Meta-Analysis. International journal of exercise science, 9(2), 230–247. https://doi.org/10.70252/HHBR9374
Kumar, P. (2015). Effect of fartlek training for developing endurance ability among athletes. Int J Phys Ed Sports Health., 2(2), 291-293. https://www.kheljournal.com/archives/2015/vol2issue2/PartE/3-3-75-957.pdf
For individuals dealing with digestive issues and conditions, can incorporating Tai Chi help improve gut health?
Tai Chi For Gut Health
Tai Chi is an exercise that has been referred to as moving meditation. The practice is rooted in Chinese medicine, which fuses martial arts and meditation. The art of Tai Chi is used to improve physical health. It can also positively impact gut health by improving digestive function, reducing inflammation, and influencing the gut microbiota composition. The slow, controlled movements and deep breathing can stimulate abdominal and pelvic organs, promoting digestion. Additionally, it has been shown to reduce inflammation in the gut and increase the diversity of gut bacteria, including beneficial butyrate-producing bacteria. (Kang D., Wang X., & Wang J., 2023)
Types
The idea is to slow down your mind and body by repeating rhythmic choreography and breathwork for about 30 to 60 minutes, culminating in finding a sense of inner peace and tranquility.
Primary Forms/Styles
These include Chen, Yang, Wu, Sun, and Wu/Hao. Each follows the same origins and principles with variations. (Tai Chi for Health Institute, 2007)
Chen Style
Considered the oldest and original style, the Chen style is characterized by explosive power, low stances, and a combination of fast and slow movements, including jumping, kicking, and striking.
Chen also utilizes a movement called “silk reeling,” a spiral-esque, flowing movement that starts at the feet and moves into the hands.
Yang Style
Yang is often considered the most popular form of Tai Chi and is practiced worldwide.
Yang Tai Chi focuses more on improving flexibility through grand, sweeping movements executed slowly and gracefully.
Wu Style
Wu Tai Chi emphasizes small, compact movements and a medium stance. Its focus is on extending the body by leaning forward and backward.
Sun Style
Sun Tai Chi combines elements of Tai Chi, Xing Yi, and Ba Gua, resulting in a unique style with fluid, circular movements.
Hao Style
This style is characterized by small-frame movements focusing on accurate position and internal strength.
Tai Chi can indirectly benefit gut health by reducing stress levels.
Its emphasis on slow movements and deep breathing can help reduce stress.
Combining meditative practices with physical movement can help calm the mind, improve focus, and even trigger the release of endorphins.
Improved Digestion
Gentle, flowing movements, particularly those involving the diaphragm, can massage and stimulate the abdominal and pelvic organs, aiding the digestive process.
Reduced Inflammation
Tai Chi can help reduce gut inflammation, a common issue in conditions like inflammatory bowel disease (IBD).
Gut Microbiota Changes
Tai Chi has been found to positively influence the gut microbiota composition, increasing the diversity and abundance of beneficial bacteria.
Improved Gut Barrier Function
Tai Chi may help improve the integrity of the gut barrier, which is essential for preventing harmful substances from entering the bloodstream and causing inflammation.
Increased Butyrate Production
Tai Chi can promote the growth of butyrate-producing bacteria, which are important for intestinal health and can reduce inflammation.
Overall Health Benefits
Increases Cognitive Function
In addition to improving your mental well-being, Tai Chi has also been found to boost cognitive abilities.
A meta-analysis stated that physical exercise, in general, improves cognitive function, and researchers specifically recommended Tai Chi for elderly individuals since it’s a gentler and more accessible form of physical exercise that also combines mental exercises through repeated choreography. (Yin Wu, et al., 2013)
Increases Flexibility and Agility
Similar to yoga, Tai Chi often involves body extensions that can improve flexibility and agility.
This is useful in daily activities and makes you more agile and capable in other sports.
Improves Balance and Coordination
In addition to improving flexibility and agility, the intricate movements can help balance and coordination.
This skill is useful in daily life.
It can help with fine motor skills and even prevent trips, stumbles, falls, and other sports.
Enhances Strength and Stamina
As with any form of physical exercise, Tai Chi can build upon existing strength and stamina.
With ongoing practice, individuals become leaner, their muscles are more defined, and they can exercise longer.
Injury Medical Chiropractic & Functional Medicine Clinic
Talk to a healthcare provider to learn what interventions would help the most. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Body Maintenance
References
Kang, D., Wang, X., & Wang, J. (2023). Intervention study of tai chi training on the intestinal flora of college student basketball players. Medicine, 102(36), e35044. https://doi.org/10.1097/MD.0000000000035044
Wu Y, W. Y., Burgess EO, Wu J. (2013). The effects of Tai Chi exercise on cognitive function in older adults: A meta-analysis. Journal of Sport and Health Science, 2(4), 193-203. https://doi.org/https://doi.org/10.1016/j.jshs.2013.09.001
Tai Chi for Health Institute. (2018). History of Tai Chi. https://taichiforhealthinstitute.org/history-of-tai-chi/#:~:text=Based%20on%20Qigong%20and%20martial%20art%20techniques,It%20contains%20explosive%20power%20and%20low%20stances.
Children walking with their toes pointed in may be pigeon-toed. What are the causes, conditions associated with it, and treatments?
Pigeon-toed Walking
If a child walks with their feet turned inward at the toes, it is usually described as being pigeon-toed. This pointing inward of the feet occasionally occurs as a child learns to walk and may continue through toddlerhood. It is noticed more often in children than adults, but older individuals can experience it. Pigeon-toed walking is rarely a major orthopedic problem and usually disappears without treatment. However, there are times when it may impact a child’s lower extremities and hips. Bracing or surgery may be necessary in these cases to correct the problem. (Paramanandam V. et al., 2019) This condition is common and typically is caused by abnormal birth positions in utero. Sometimes, slight issues may lead to noticeable functional characteristics. Mild changes in bone shape and positioning usually cause pigeon toes. Often, it subsides in a few years as the child continues to develop.
What Does It Mean?
There is usually no need to worry, as this condition is likely not permanent and will go away in a few years. (Paramanandam V. et al., 2019) However, it is recommended that you check in with your healthcare provider to ensure the child is developing normally. Some adults walk with their toes turned in. This may be due to a birth defect, a weakness, or a rare case of pigeon-toed walking as a youth that was left untreated or did not go away.
Causes
There are various reasons for pigeon-toed walking. To determine the cause, a healthcare provider can assess the child’s condition and make a diagnosis, including:
Metatarsus Adductus
A condition where the front part of the foot is turned inward.
The metatarsals are the long bones of the forefoot.
This is when the bones of the foot point inward, leading to pigeon-toed walking.
A clinical examination and X-ray can confirm the metatarsus adducts as a cause of pigeon-toed walking.
Tibial Torsion
A twisted shinbone (tibia) can cause the feet to turn inward in younger children.
The shinbone/tibia in some children may be slightly twisted.
The tibia can either turn outward or inward.
When it twists inward, it may manifest as a pigeon-toed gait.
Tibial torsion may accompany femoral anteversion.
It is diagnosed with an X-ray.
Children with tibial torsion typically grow out of the problem, and the pigeon-toed disappears by age 4. (Uden H., & Kumar S. 2012)
Femoral Anteversion
A common cause, especially in older children, is when the thighbone/femur is twisted inward.
If the femur turns inward and forward unnaturally, where the femoral neck meets the body of the femur, it is called femoral anteversion.
An outward and backward rotation of the femur is called femoral retroversion.
Many children with femoral anteversion appear knock-kneed with a large gap between their feet when standing with knees together, and when they walk, they appear pigeon-toed.
A clinical examination and X-ray diagnose it.
Symptoms
In most cases, the child does not complain of any pain. However, if pain is felt, it can include:
Tightness in the calf muscles
Aching on the outer edges of the feet
Knee pain
Usually, parents will notice pigeon-toes when their child is first learning to walk. Rest assured, the child most likely is not experiencing pain. They have feet and knees that turn inward when they walk and run. (Uden H., & Kumar S., 2012)
A pediatrician or primary care provider can assess the situation and make recommendations. Most pigeon-toed children begin walking and running normally after age 3 or 4, so a watch-and-wait approach is used. Parents may have to take their child to a specialist, like an orthopedic surgeon, if they complain of pain while walking. A specialist may be referred if the child cannot walk due to the inward turn of their feet.
Risk Factors
Pigeon-toed walking is not a preventable condition but rather one that develops during pregnancy. Causes may include: (Scorcelletti M. et al., 2020)
A pregnancy with twins or multiple births
Large fetus
Breech position in utero when the baby is positioned feet first.
Typically, a normal gait will appear by age 3 or 4. Other treatments may include:
Physical Therapy Exercises and Gait Training
Exercises to stretch tight lower extremity muscles and strengthen hip and leg muscles can help improve walking gait.
See a pediatric specialist before starting, as research shows that parental stretching of a newborn with metatarsus adductus offers little benefit. (Eamsobhana P. et al., 2017)
Bracing or Casting
Braces
Serial casting is a procedure that helps children improve their range of movement and may be done to place their lower extremities in an optimum position as they develop. (Uden H., & Kumar S., 2012)
Surgery
For cases in which tibial torsion is the cause, osteotomy surgery, which involves cutting and/or removing bone, may be recommended to correct the structural deformity of the shinbone.
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Foot Pronation
References
Paramanandam, V., Lizarraga, K. J., Soh, D., Algarni, M., Rohani, M., & Fasano, A. (2019). Unusual gait disorders: a phenomenological approach and classification. Expert review of neurotherapeutics, 19(2), 119–132. https://doi.org/10.1080/14737175.2019.1562337
Uden, H., & Kumar, S. (2012). Non-surgical management of a pediatric “intoed” gait pattern – a systematic review of the current best evidence. Journal of Multidisciplinary Healthcare, 5, 27–35. https://doi.org/10.2147/JMDH.S28669
Scorcelletti, M., Reeves, N. D., Rittweger, J., & Ireland, A. (2020). Femoral anteversion: significance and measurement. Journal of Anatomy, 237(5), 811–826. https://doi.org/10.1111/joa.13249
Eamsobhana, P., Rojjananukulpong, K., Ariyawatkul, T., Chotigavanichaya, C., & Kaewpornsawan, K. (2017). Does the parental stretching programs improve metatarsus adductus in newborns?. Journal of Orthopaedic Surgery (Hong Kong), 25(1), 2309499017690320. https://doi.org/10.1177/2309499017690320
Join the calisthenics movement and experience a versatile approach to fitness designed for all skill levels.
Introduction
Many people might suffer musculoskeletal ailments due to their stressful schedules and habits. Anyone at any age may be affected by it, from muscular imbalances to low back discomfort; therapy is required when people have overlapping risk profiles. Many patients begin seeking therapy for musculoskeletal diseases to lessen the pain they experience. Many would choose surgical treatment to alleviate the overlapping risk profiles depending on the degree. Others, conversely, could attempt non-surgical methods to alleviate musculoskeletal discomfort. Since musculoskeletal issues are one of the main causes of disability, non-surgical therapies may safely and affordably relieve the body’s misdirected pain. By aligning the spine and extending the afflicted muscles, non-surgical therapies such as chiropractic adjustments may help alleviate musculoskeletal problems. However, to assist patients in healing over the long term, chiropractors will create a personalized treatment plan that includes active movement exercises—where calisthenics comes in—to help rebuild muscle strength and mobility function.
What is Calisthenics?
Also known as bodyweight training, calisthenics utilizes the person’s body to build muscle strength and increase flexibility while enhancing neuromuscular control. When people start incorporating regular physical activity into their routine, they will notice their health and quality of life improved, their fitness levels will increase, and the risk of several chronic diseases associated with the musculoskeletal body will be reduced. (Bellissimo et al., 2022) The best way to think about calisthenics is to think like push-ups, planks, squats, and dynamics stretches when working out. Additionally, calisthenics can be scalable and adaptable to any person’s fitness level without heavy gym equipment or HIIT workouts. For individuals dealing with musculoskeletal conditions like low back pain or associated pain symptoms, calisthenics is a safer and more effective option. Calisthenics can even help with cognitive decline associated with musculoskeletal disorders by reducing comorbidities correlated with the muscles and cognitive function. (Osuka et al., 2020)
How It Supports Musculoskeletal Health?
Musculoskeletal pain is a multi-factorial condition that involves environmental factors that cause long-term pain and disability. (Caneiro et al., 2021) Everyday motions can cause strain and fatigue to the various muscle groups and, over time, can affect the joints in the extremities. For individuals dealing with musculoskeletal disorders, calisthenics can offer numerous benefits to reduce pain-like symptoms associated with the musculoskeletal system:
Improved Core Stability: Calisthenics can help strengthen the core muscles, providing the necessary stability to reduce low back pain. (Zemkova & Zapletalova, 2022)
Enhanced Mobility: Calisthenics can utilize gentle functional movements within the upper and lower extremities to help preserve the joint’s range of motion.
Injury Prevention: Individuals incorporating calisthenics for muscle pain will notice that their postural muscles are getting stronger, thus improving body biomechanics and reducing compensatory movements.
Neuromuscular Re-education: Calisthenic exercises help retrain muscles to fire appropriately, which is excellent for individuals with a sedentary lifestyle. Individuals with a sedentary lifestyle who start doing calisthenic exercises will notice a positive effect on energy expenditure, endothelial function, and muscle improvement. (Mear et al., 2022)
Can Core Exercises Help With Back Pain?-Video
Calisthenics Integrated With Chiropractic Care
When it comes to incorporating non-surgical treatment with calisthenics, chiropractic care can help many individuals deal with overlapping pain symptoms associated with musculoskeletal disorders. Chiropractic care incorporates mechanical and manual spinal manipulation to help realign the spine and remobilize the body while reducing muscle pain. (Coulter et al., 2018) When chiropractors address the structural misalignment of the person’s spine through adjustments, they can pinpoint the causes and start to assess the individual by coming up with a personalized treatment plan that includes calisthenics as part of their active rehabilitation to reengage their musculoskeletal system to maintain the improvements. In chiropractic and functional medicine settings, calisthenics is often prescribed as part of active rehabilitation. After addressing structural misalignments through manual adjustments, patients are encouraged to reengage their musculoskeletal system to maintain improvements.
Here’s how calisthenics fits in:
Post-Adjustment Stabilization: Exercises help “lock in” structural corrections by reinforcing proper posture and movement.
Corrective Exercise Protocols: Practitioners may prescribe targeted calisthenics to improve muscular imbalances contributing to pain.
Home Programs: These exercises are ideal for patients to perform safely at home with little to no equipment.
Calisthenic Exercises For Low Back Pain
For individuals dealing with acute or chronic low back pain, these beginner-friendly calisthenics exercises can help relieve muscle tension in the lower back while promoting postural stability. It is always important to consult a doctor before starting a new exercise routine.
Glute Bridge
Glute bridges can help decompress the lumbar spine while strengthening the glutes and hamstrings.
How to do it:
Laying down on your back with knees bent and feet flat on the floor.
By engaging the core muscles, lift the hips towards the ceiling.
Hold the position for 5 seconds, then lower slowly.
Repeat 10–15 times for three sets.
Bird-Dog
Bird-Dog can be an excellent exercise to help individuals improve their spinal stability by engaging their core and multifidus muscles to reduce back pain.
How to do it:
Be on a mat on your hands and knees to have a neutral spine alignment.
Simultaneously extend the right arm and left leg while keeping your spine neutral.
Hold the position for 5-10 seconds, then slowly switch sides.
Perform 10 reps per side for three sets.
Wall Sit
Wall sit exercises are excellent for individuals with low back pain. They help strengthen the surrounding muscles in the lumbar spine and activate the quadriceps to support neutral pelvic alignment.
How to do it:
Stand up straight with your back against a wall and slide to a seated position with the thighs parallel to the floor
Engage the core muscles and hold between 10-30 seconds. Tip: Gradually increase the time for an effective workout.
Repeat 3–5 times for three sets.
Pelvic Tilt
For individuals dealing with tension and low back pain in their lumbar spine, pelvic tilts can help provide relief while improving core muscle control.
How to do it:
Lay on your back with bent knees on a mat.
Gently lower your lower back into the mat while engaging the core muscles.
Hold the position for 10 seconds before relaxing.
Repeat the motion for 10–15 times for three sets.
Conclusion
Calisthenics is more than simply a bodyweight exercise; it’s a fantastic therapeutic technique that can be used in conjunction with chiropractic adjustments. By using exercises to reenergize the musculoskeletal system and lessen muscular soreness, calisthenics may motivate people to take charge of their health and wellbeing. Calisthenic exercises may hasten rehabilitation, avert more injuries, and enhance general functional ability since the body’s primary function is mobility. People who begin using calisthenics into their everyday practice will see that their movement improves and that their fitness objectives are met.
Injury Medical & Functional Medicine Clinic
We associate with certified medical providers who understand the importance of assessing individuals with musculoskeletal disorders affecting their daily routines. When asking important questions to our associated medical providers, we advise patients to incorporate exercises like calisthenics to help reengage the musculoskeletal system while reducing muscle pain within the lumbar region. Dr. Alex Jimenez, D.C., uses this information as an academic service. Disclaimer.
References
Bellissimo, G. F., Ducharme, J., Mang, Z., Millender, D., Smith, J., Stork, M. J., Little, J. P., Deyhle, M. R., Gibson, A. L., de Castro Magalhaes, F., & Amorim, F. (2022). The Acute Physiological and Perceptual Responses Between Bodyweight and Treadmill Running High-Intensity Interval Exercises. Front Physiol, 13, 824154. https://doi.org/10.3389/fphys.2022.824154
Caneiro, J. P., Bunzli, S., & O’Sullivan, P. (2021). Beliefs about the body and pain: the critical role in musculoskeletal pain management. Braz J Phys Ther, 25(1), 17-29. https://doi.org/10.1016/j.bjpt.2020.06.003
Coulter, I. D., Crawford, C., Hurwitz, E. L., Vernon, H., Khorsan, R., Suttorp Booth, M., & Herman, P. M. (2018). Manipulation and mobilization for treating chronic low back pain: a systematic review and meta-analysis. Spine J, 18(5), 866-879. https://doi.org/10.1016/j.spinee.2018.01.013
Mear, E., Gladwell, V. F., & Pethick, J. (2022). The Effect of Breaking Up Sedentary Time with Calisthenics on Neuromuscular Function: A Preliminary Study. Int J Environ Res Public Health, 19(21). https://doi.org/10.3390/ijerph192114597
Osuka, Y., Kojima, N., Sasai, H., Ohara, Y., Watanabe, Y., Hirano, H., & Kim, H. (2020). Exercise Types and the Risk of Developing Cognitive Decline in Older Women: A Prospective Study. J Alzheimers Dis, 77(4), 1733-1742. https://doi.org/10.3233/JAD-200867
Zemkova, E., & Zapletalova, L. (2022). The Role of Neuromuscular Control of Postural and Core Stability in Functional Movement and Athlete Performance. Front Physiol, 13, 796097. https://doi.org/10.3389/fphys.2022.796097
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine