1. Kaur J. A comprehensive review on metabolic syndrome.<br />
Cardiol Res Pract 2014:943162, http://dx.doi.org/10.1155/<br />
2014/943162.<br />
2. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic<br />
syndrome among US adults. Findings from the Third National<br />
Health and Nutrition Examination Survey. J Am Med Assoc<br />
2006;287:356�9.<br />
3. Boyle JP, Thompson TJ, Gregg EW, Barker LE, Williamson<br />
DF. Projection of the year 2050 burden of diabetes in the US<br />
adult population: dynamic modeling of incidence, mortality,<br />
and prediabetes prevalence. Popul Health Metr 2010;8:29,<br />
http://dx.doi.org/10.1186/1478-7954-8-29.<br />
4. [Internet]Centers for Disease Control and Prevention.<br />
Adult Obesity Facts. Atlanta: CDC; 2014. [Available from<br />http://www.cdc.gov/obesity/data/adult.html].<br />
5. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of<br />
childhood and adult obesity in the United States, 2011�2012.<br />
JAMA 2014;311(8):806�14.<br />
6. Riksman JS, Williamson OD, Walker BF. Delineating<br />
inflammatory and mechanical sub-types of low back pain: a<br />
pilot survey of fifty low back pain patients in a chiropractic<br />
setting. Chiropr Man Therap 2011;19(1):5, http://dx.doi.org/<br />
10.1186/2045-709X-19-5.<br />
7. Dobretsov M, Ghaleb AH, Romanovsky D, Pablo CS, Stimers<br />
JR. Impaired insulin signaling as a potential trigger of<br />
pain in diabetes and prediabetes. Int Anesthesiol Clin<br />
2007;45(2):95�105.<br />
8. Mantyselka P, Miettola J, Niskanen L, Kumpusalo E. Glucose<br />
regulation and chronic pain at multiple sites. Rheumatology<br />
2008;47(8):1235�8.<br />
9. M�ntyselk� P, Miettola J, Niskanen L, Kumpusalo E.<br />
Persistent pain at multiple sites�connection to glucose<br />
derangement. Diabetes Res Clin Pract 2009;84(2):e30�2.<br />
10. Mantyselka P, Kautianen H, Vanhala M. Prevalence of neck<br />
pain in subjects with metabolic syndrome�a cross-sectional<br />
population-based study. BMC Musculoskelet Disord 2010;11:<br />
171, http://dx.doi.org/10.1186/1471-2474-11-171.<br />
11. Rechardt M, Shiri R, Karppinen J, Jula A, Heli�vaara M,<br />
Viikari-Juntura E. Lifestyle and metabolic factors in relation<br />
to shoulder pain and rotator cuff tendinitis: a population-based<br />
study. BMC Musculoskelet Disord 2010;11:165.<br />
12. Gaida JE, Alfredson L, Kiss ZS, Wilson AM, Alfredson H,<br />
Cook JL. Dyslipidemia in Achilles tendinopathy is<br />
characteristic of insulin resistance. Med Sci Sports Exerc<br />
2009;41:1194�7.<br />
13. Malliaras P, Cook JL, Kent PM. Anthropometric risk factors<br />
for patellar tendon injury among volleyball players. Br J<br />
Sports Med 2007;41:259�63.<br />
14. Skrzynski S. DSC study of collagen in disc disease. J Biophys<br />
2009;2009:819635, http://dx.doi.org/10.1155/2009/819635.<br />
15. Luevano-Contreras C, Chapman-Novakofski K. Dietary<br />
advanced glycation end products and aging. Nutrients<br />
2010;2(12):1247�65 [2009;2009:819635].<br />
16. Abate M, Schiavone C, Pelotti P, Salini V. Limited joint<br />
mobility (LJM) in elderly subjects with type II diabetes<br />
mellitus. Arch Gerontol Geriatrics 2011;53:135�40.<br />
17. Sakellaridis N. The influence of diabetes mellitus on lumbar<br />
intervertebral disk herniation. Surg Neurol 2006;66:152�4.<br />
18. Shepherd PR, Kahn BB. Glucose transporters and insulin<br />
action: implications for insulin resistance and diabetes<br />
mellitus. New Eng J Med 1999;341(4):248�57.<br />
19. Abdul-Ghani MA, DeFronzo RA. Pathogenesis of insulin<br />
resistance in skeletal muscle. J Biomed Biotechnol 2010:19,<br />
http://dx.doi.org/10.1155/2010/476279 [Article ID 476279].<br />
20. [Internet]American Heart Association. About metabolic<br />
syndrome. Dallas: The Association; 2014. [Available from<br />http://www.heart.org/HEARTORG/Conditions/More/<br />MetabolicSyndrome/About-Metabolic-Syndrome_UCM_<br />301920_Article.jsp].<br />
21. Hotamisligil GS. Inflammation and metabolic disorders.<br />
Nature 2006;444:860�7.<br />
22. Glass CK, Olefsky JM. Inflammation and lipid signaling in the<br />
etiology of insulin resistance. Cell Metab 2012;15(5):635�45.<br />
23. Reaven GM. All obese individuals are not created equal:<br />
insulin resistance is the major determinant of cardiovascular<br />
disease in overweight/obese individuals. Diabetes Vasc Dis<br />
Res 2005;2:105�12.<br />
24. Ritov VB, Menshikova EV, He J, Ferrell RE, Goodpaster<br />
BH, Kelley DE. Deficiency of subsarcolemmal mitochondria<br />
in obesity and type 2 diabetes. Diabetes 2005;54:8�14.<br />
25. Corcoran MP, Lamon-Fava S, Fielding RA. Trans fats and<br />
insulin resistance: skeletal muscle lipid deposition and insulin<br />
resistance: effect of dietary fatty acids and exercise. Am J Clin<br />
Nutr 2007;85:662�77.<br />
26. Schipper HS, Prakken B, Kalkhoven E, Boes M. Adipose<br />
tissue-resident immune cells: key players in immunometabolism.<br />
Trends Endocrinol Metab 2012;23:407�15.<br />
27. Antuna-Puente B, Feve B, Fellahi S, Bastard JP. Adipokines:<br />
the missing link between insulin resistance and obesity.<br />
Diabetes Metab 2008;34:2�11.<br />
28. Grimble RF. Inflammatory status and insulin resistance. Curr<br />
Opin Clin Nutr Metab Care 2003;5:551�9.<br />
29. Tilg H, Moschen AR. Inflammatory mechanisms in<br />
the regulation of insulin resistance. Mol Med 2008;3�4:222�31.<br />
30. Johnson DR, O’Conner JC, Satpathy A, Freund GG.<br />
Cytokines in type 2 diabetes. Vitam Horm 2006;74:405�41.<br />
31. Ridker PM, Wilson PW, Grundy SM. Should C-reactive<br />
protein be added to the metabolic syndrome and to<br />
assessment of global cardiovascular risk? Circulation 2004;<br />
109:2818�25.<br />
32. Gelaye B, Revilla L, Lopez T, et al. Association between<br />
insulin resistance and c-reactive protein among Peruvian<br />
adults. Diabetol Metab Syn 2010;2:30.<br />
33. Singh VP, Bali A, Singh N, et al. Advanced glycation end<br />
products and diabetic complications. Korean J Physiol<br />
Pharmacol 2014;18(1):1�14.<br />
34. Baker RG, Hayden MS. NF-kB, inflammation and metabolic<br />
disease. Cell Metab 2011;13(1):11�22.<br />
35. Purkayastha S, Cair D. Neuroinflammatory basis of metabolic<br />
syndrome. Mol Metab Nov 2013;2(4):356�63.<br />
36. Ehse JA, Boni-Schnetzler M, Faulenbach M, Donath MY.<br />
Macrophages, cytokines and beta-cell death in type 2 diabetes.<br />
Biochem Soc Trans 2008;36(3):340�2.<br />
37. Boni-Schnetzler M, Ehses JA, Faulenbach M, Donath MY.<br />
Insulitis in type 2 diabetes. Diabetes Obes Metab 2008;10<br />
(Suppl 4):201�4.<br />
38. Donath MY, Schumann DM, Faulenbach M, Ellingsgaard H,<br />
Perren A, Ehses JA. Islet inflammation in type 2<br />
diabetes: from metabolic stress to therapy. Diabetes Care<br />
2008;31(Suppl 2):S161�4.<br />
39. Donath MY, Boni-Schnetzler M, Ellingsgaard H, Ehses JA.<br />
Islet inflammation impairs the pancreatic beta-cell in type 2<br />
diabetes. Physiology 2009;24:325�31.<br />
40. Harford KA, Reynolds CM, McGillicuddy FC, Roche HM.<br />
Fats, inflammation and insulin resistance: insights to the role<br />
of macrophage and T-cell accumulation in adipose tissue.<br />
Proc Nutr Soc 2011;70:408�17.<br />
41. Munoz A, Costa M. Nutritionally mediated oxidative stress and<br />
inflammation. Oxid Med Cell Longev 2013;2013:610950, http://<br />
dx.doi.org/10.1155/2013/610950.<br />
42. Wisse BE, Schwartz MW. Does hypothalamic inflammation<br />
cause obesity? Cell Metab 2009;10(4):241�2.<br />
43. Purkayastha S, Cair D. Neuroinflammatory basis of metabolic<br />
syndrome. Mol Metab Nov 2013;2(4):356�63.<br />
44. Calegari VC, Torsoni AS, Vanzela EC, Ara�jo EP, Morari<br />
J, Zoppi CC, et al. Inflammation of the hypothalamus leads<br />
to defective pancreatic islet function. J Biol Chem 2011;<br />
286(15):12870�80.<br />
45. Cordain L, Eaton SB, Sebastian A, et al. Origins and evolution<br />
of the Western diet: health implications for the 21st century.<br />
Am J Clin Nutr 2005;81:341�54.<br />
46. Barclay AW, Petocz P, McMillan-Price J, et al. Glycemic<br />
index, glycemic load, and chronic disease risk�a metaanalysis<br />
of observational studies. Am J Clin Nutr<br />
2008;87:627�37.<br />
47. Facchini FS, Hua N, Abbasi F, Reaven GM. Insulin resistance<br />
as a predictor of age-related disease. J Clin Endocrinol Metab<br />
2001;86:3574�8.<br />
48. Lin H, Lee B, Ho Y, et al. Postprandial glucose improves the<br />
risk prediction of cardiovascular death beyond the metabolic<br />
syndrome in the nondiabetic population. Diabetes Care Sep<br />
2009;32(9):1721�6.<br />
49. O’Keefe JH, Bell DS. Postprandial hyperglycemia/<br />
hyperlipidemia (postprandial dysmetabolism) is a cardiovascular<br />
risk factor. Am J Cardiol 2007;100:899�904.<br />
50. Cao H. Adipocytokines in obesity and metabolic disease.<br />
J Endocrinol 2014;220(2):T47�59.<br />
51. Nah SS, Choi IY, Lee CK, et al. Effects of advanced glycation<br />
end products on the expression of COX2, PGE2 and NO in human osteoarthritic chondrocytes. Rheumatology (Oxford)<br />
2008;47(4):425�31.<br />
52. Abate M, Schiavone C, Pelotti P, Salini V. Limited joint<br />
mobility (LJM) in elderly subjects with type II diabetes<br />
mellitus. Arch Gerontol Geriatr 2011;53:135�40.<br />
53. Robinson D, Mirovsky Y, Halperin N, Evron Z, Nevo Z.<br />
Changes in proteoglycans of intervertebral disc in diabetic<br />
patients: a possible cause of increased back pain. Spine<br />
1998;23:849�56.<br />
54. Sakellaridis N, Androulis A. Influence of diabetes mellitus on<br />
cervical intervertebral disc herniation. Clin Neurol Neurosurg<br />
2008;110:810�2.<br />
55. Jhawar BS, Fuchs CS, Colditz GA, Stampfer MJ. Cardiovascular<br />
risk factors for physician-diagnosed lumbar disc<br />
herniation. Spine J 2006;6:684�91.<br />
56. Lotan R, Oron A, Anekstein Y, Shalmon E, Mirovsky Y.<br />
Lumbar stenosis and systemic diseases: is there any relevance.<br />
J Spinal Disord Tech 2008;21:247�51.<br />
57. Anekstein Y, Smorgick Y, Lotan R, et al. Diabetes mellitus as<br />
a risk factor for the development of lumbar spinal stenosis. Isr<br />
Med Assoc J 2010;12:16�20.<br />
58. Choi KM. Sarcopenia and sarcopenic obesity. Endocrinol<br />
Metab (Seoul) 2013;28(2):86�9.<br />
59. D’hooge R, Cagnie B, Crombez G, et al. Increased<br />
intramuscular fatty infiltration without differences in lumbar<br />
muscle cross-sectional area during remission of unilateral<br />
recurrent low back pain. Man Ther 2012 Dec;17(6):5584�8.<br />
60. Chen YY, Pao JL, Liaw CK, et al. Image changes of paraspinal<br />
muscles and clinical correlations in patients with unilateral<br />
lumbar spinal stenosis. Eur Spine J 2014;23(5):999�1006.<br />
61. Kim Y, Park H. Does regular exercise without weight loss<br />
reduce insulin resistance in children and adolescents? In J<br />
Endocrinol 2013:402592, http://dx.doi.org/10.1155/2013/<br />
402592 [Epub 2013 Dec 12].<br />
62. Strasser B, Siebert U, Schobersberger W. Resistance training<br />
in the treatment of the metabolic syndrome: a systematic<br />
review and meta-analysis of the effect of resistance training on<br />
metabolic clustering in patients with abnormal glucose<br />
metabolism. Sports Med 2010;40:397�415.<br />
63. Sharman MJ, Volek JS. Weight loss leads to reductions in<br />
inflammatory biomarkers after a very-low-carbohydrate diet<br />
and a low-fat diet in overweight men. Clin Sci (Lond)<br />
2004;13:365�9.<br />
64. Teng KT, Chang CY, Chang LF, et al. Modulation of obesityinduced<br />
inflammation by dietary fats: mechanisms and<br />
clinical evidence. Nutr J 2014;13:12, http://dx.doi.org/<br />
10.1186/1475-2891-13-12.<br />
65. Tzotzas T, Evangelou P, Kiortsis DN. Obesity, weight loss<br />
and conditional cardiovascular risk factors. Obes Rev 2011;12<br />
(5):e282�9.<br />
66. Stone N, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA<br />
Guideline on the Treatment of Blood Cholesterol to Reduce<br />
Atherosclerotic Cardiovascular Risk in Adults: A report of<br />
the American College of Cardiology/American Heart<br />
Association Task Force on practice guidelines. Circulation<br />
2014;129(25 Suppl 2):S1�S45.<br />
67. P�rez-Guisado J, Mu�oz-Serrano A. A pilot study of the<br />
Spanish ketogenic Mediterranean diet: an effective therapy for<br />
the metabolic syndrome. J Med Food 2011;14(7�8):681�7.<br />
68. P�rez-Guisado J, Mu�oz-Serrano A, Alonso-Moraga A.<br />
Spanish ketogenic Mediterranean diet: a healthy cardiovascular<br />
diet for weight loss. Nutr J 2008;7:30, http://dx.doi.org/<br />
10.1186/1475-2891-7-30.<br />
69. Jonsson T, Granfeldt Y, Lindeberg S, et al. Subjective satiety<br />
and other experiences of a Paleolithic diet compared to a<br />
diabetes diet in patients with T2DM. Nutr J 2013;12:105,<br />
http://dx.doi.org/10.1186/1475-2891-12-105.<br />
70. Jonsson T, Granfeldt Y, Ahren B, et al. Beneficial effects of a<br />
Paleolithic diet on cardiovascular risk factors in T2DM: a<br />
randomized cross-over pilot study. Cardiovasc Diabetol<br />
2009;8:35, http://dx.doi.org/10.1186/1475-2840-8-35.<br />
71. Nicklas BJ, You T, Pahor M. Behavioural treatments<br />
for chronic system inflammation: effects of dietary<br />
weight loss and exercise training. Can Med Assoc J<br />
2005;172(9):1199�209.<br />
72. O’Keefe JH, Gheewala NM, O’Keefe JO. Dietary<br />
strategies for improving post-prandial glucose, lipids, inflammation,<br />
and cardiovascular health. J Am Coll Cardiol<br />
2008;51:249�55.<br />
73. O’Keefe Jr JH, Cordain L. Cardiovascular disease resulting<br />
from a diet and lifestyle at odds with our Paleolithic genome:<br />
how to become a 21st-century hunter�gatherer. Mayo Clin<br />
Proc 2004;79(1):101�8.<br />
74. Ames BN. Low micronutrient intake may accelerate the<br />
degenerative diseases of aging through allocation of scarce<br />
micronutrients by triage. Proc Natl Acad Sci U S A 2006;103<br />
(47):17589�94.<br />
75. Holick MF, Chen TC. Vitamin D deficiency: a worldwide<br />
problem with health consequences. Am J Clin Nutr<br />
2008;87:1080S�6S [Suppl.].<br />
76. Toubi E, Shoenfeld Y. The role of vitamin D in regulating<br />
immune responses. Isr Med Assoc J 2010;12(3):174�5.<br />
77. King DE, Mainous AG, Geesey ME, Egan BM, Rehman S.<br />
Magnesium supplement intake and C-reactive protein levels<br />
in adults. Nutr Res 2006;26:193�6.<br />
78. Rosanoff A, Weaver CM, Rude RK. Suboptimal magnesium<br />
status in the United States: are the health consequences<br />
underestimated? Nutr Rev 2012;70(3):153�64.<br />
79. Simopoulos AP. Omega-3 fatty acids in inflammation and<br />
autoimmune diseases. J Am Coll Nutr 2002;21(6):495�505.<br />
80. Simopoulos AP. The importance of the omega-6/omega-3<br />
fatty acid ratio in cardiovascular disease and other chronic<br />
diseases. Exp Biol Med 2008;233:674�88.<br />
81. Fung GJ, Steffen LM, Zhou X, et al. Vitamin D intake is<br />
inversely related to risk of developing metabolic syndrome<br />
in African American and white men and women over 20 y:<br />
the Coronary Artery Risk Development in Young Adults<br />
study. Am J Clin Nutr 2012;96(1):24�9 [Published online<br />2012 May 30].<br />
82. Palomer X, Gonzalez-Clemente JM, Blanco-Vaca F, Mauricio<br />
D. Role of vitamin D in the pathogenesis of type 2 diabetes<br />
mellitus. Diabetes Obes Metab 2008;10:185�97.<br />
83. Guadarrama-Lopez AL, Valdes-Ramos R, Martinex-Carrillo<br />
BE. T2DM, PUFAs, and vitamin D: their relation to<br />
inflammation. J Immunol Res 2014;2014:860703, http://dx.<br />
doi.org/10.1155/2014/860703.<br />
84. Cannell JJ, Hollis BW. Use of vitamin D in clinical practice.<br />
Altern Med Rev 2008;13(1):6�20.<br />
85. Davidson MB, Duran P, Lee ML, Friedman TC. High-dose<br />
vitamin D supplementation in people with prediabetes and<br />
hypovitaminosis D. Diabetes Care 2013;36(2):260�6, http://<br />
dx.doi.org/10.2337/dc12-1204.<br />
86. Schwalfenberg G. Vitamin D, and diabetes: improvement of<br />
glycemic control with vitamin D3 repletion. Can Fam<br />
Physician 2008;54:864�6.<br />
87. Kim DJ, Xun P, Liu K, et al. Magnesium intake in relation to<br />
systemic inflammation, insulin resistance, and the incidence<br />
of diabetes. Diabetes Care 2010;33(12):2604�10, http://dx.<br />
doi.org/10.2337/dc10-0994.<br />
88. Guerrero-Romero F, Tamez-Perez HE, Gonz�lez-Gonz�lez G,<br />
et al. Oral magnesium supplementation improves insulin<br />
sensitivity in non-diabetic subjects with insulin resistance. A<br />
double-blind placebo-controlled randomized trial. Diabetes<br />
Metab 2004;30(3):253�8.<br />
89. Rodr�guez-Mor�n M, Guerrero-Romero F. Oral magnesium<br />
supplementation improves insulin sensitivity and metabolic<br />
control in type 2 diabetic subjects: a randomized double-blind<br />
controlled trial. Diabetes Care 2003;26(4):1147�52.<br />
90. Song Y, He K, Levitan EB, Manson JE, Liu S. Effects of oral<br />
magnesium supplementation on glycaemic control in type 2<br />
diabetes: a meta-analysis of randomized double-blind controlled<br />
trials. Diabet Med 2006;23(10):1050�6.<br />
91. Mooren FC, Kr�ger K, V�lker K, Golf SW,Wadepuhl M, Kraus<br />
A. Oral magnesium supplementation reduces insulin resistance<br />
in non-diabetic subjects�a double-blind, placebo-controlled,<br />
randomized trial. Diabetes Obes Metab 2011;13(3):281�4.<br />
92. Aggarwal BB. Targeting inflammation induced obesity and<br />
metabolic diseases by curcumin and other nutraceuticals.<br />
Annu Rev Nutr 2010;30:173�9.<br />
93. Alappat L, Awad AB. Curcumin and obesity: evidence and<br />
mechanisms. Nutr Rev 2010;68(12):729�38.<br />
94. Gonzales AM, Orlando RA. Curcumin and resveratrol inhibit<br />
nuclear factor-kappaB-mediated cytokine expression in adipocytes.<br />
Nutr Metab 2008;5:17, http://dx.doi.org/10.1186/<br />
1743-7075-5-17.<br />
95. Sahebkar A. Why it is necessary to translate curcumin into<br />
clinical practice for the prevention and treatment of metabolic<br />
syndrome? Biofactors 2012, http://dx.doi.org/10.1002/<br />
biof.1062 [Epub ahead of print].<br />
96. Hsu CH, Cheng AL. Clinical studies with curcumin. Adv Exp<br />
Med Biol 2007;595:471�80.<br />
97. Chuengsamarn S, Rattanamongkolgul S, Luechapudiporn R,<br />
Phisalaphong C, Jirawatnotai S. Curcumin extract for prevention<br />
of type 2 diabetes. Diabetes Care 2012;35(11):2121�7.<br />
98. Jurenka JS. Anti-inflammatory properties of curcumin, a<br />
major constituent of curcuma longa: a review of preclinical<br />
and clinical research. Altern Med Rev 2009;14(2):141�53.<br />
99. Leach M. Gymnema sylvestre for diabetes mellitus: a systematic<br />
review. J Altern Complement Med 2007;13(9):977�83.<br />
100. Chattopadhyay R. A comparative evaluation of some blood<br />
sugar lowering agents of plant origin. J Ethnopharmacol<br />
1999;67:367�72.<br />
101. Nahas R, Moher M. Complementary and alternative medicine<br />
for the treatment of type 2 diabetes. Can Fam Physician<br />
2009;55:591�6.<br />
102. Vanadium/Vanadyl sulfate: monograph. Altern Med Rev<br />
2009;14:17�80.<br />
103. Boden G, Chen X, Ruiz J, et al. Effects of vanadyl sulfate<br />
on carbohydrate and lipid metabolism in patients with noninsulin-dependent<br />
diabetes mellitus. Metabolism 1996;45:<br />
1130�5.<br />
104. Jacques-Camarena O, Gonz�lez-Ortiz M, Mart�nez-Abundis E,<br />
et al. Effect of vanadium on insulin sensitivity in patients with<br />
impaired glucose tolerance. Ann Nutr Metab 2008;53:195�8.<br />
105. Vincent JB. The biochemisty of chromium. J Nutr<br />
2000;130:715�8.<br />
106. Anderson RA. Chromium and insulin resistance. Nutr Res<br />
Rev 2003;16:267�75.<br />
107. Vincent JB. Chromium: celebrating 50 years as an essential<br />
element? Dalton Trans 2010;39:3787�94.<br />
108. Office of Dietary Supplements. [Internet]. Dietary supplement<br />
fact sheet: Chromium. Washington, DC: United States<br />
Department of Health and Human Services. http://ods.od.nih.<br />
gov/factsheets/chromium/. Reviewed November 4, 2013.<br />
109. Anderson RA. Chromium, glucose intolerance and diabetes.<br />
J Am Coll Nutr 1998;17(6):548�55.<br />
110. Cefalu WT, Rood J, Patricia Pinsonat P, et al. Characterization<br />
of the metabolic and physiologic response to chromium<br />
supplementation in subjects with type 2 diabetes mellitus.<br />
Metab Clin Exp 2010;59:755�62.<br />
111. Heimbach JT, Anderson RA. Chromium: recent studies regarding<br />
nutritional roles and safety. Nutr Today 2005;40(4):180�95.<br />
112. Shay KP, Moreau RF, Smith EJ, Smith AR, Hagen TM.<br />
Alpha-lipoic acid as a dietary supplement: molecular<br />
mechanisms and therapeutic potential. Biochim Biophys<br />
Acta 2009;1790:1149�60.<br />
113. Morikawa T, Yasuno R, Wada H. Do mammalian cells<br />
synthesize lipoic acid? Identification of a mouse cDNA<br />
encoding a lipoic acid synthase located in mitochondria.<br />
FEBS Lett 2001;498:16�21.<br />
114. Singh U, Jialal I. Alpha-lipoic acid supplementation and<br />
diabetes. Nutr Rev 2008;66(11):646�57.<br />
115. Padmalayam I, Hasham S, Saxena U, Pillarisetti S. Lipoic acid<br />
synthase (LASY): a novel role in inflammation, mitochondrial<br />
function, and insulin resistance. Diabetes 2009;58:600�8.<br />
116. Capasso I, Esposito E, Maurea N, et al. Combination of<br />
inositol and alpha lipoic acid in metabolic syndrome-affected<br />
women: a randomized placebo-controlled trial. Trial<br />
2013;14:273, http://dx.doi.org/10.1186/1745-6215-14-273.<br />
117. Udupa A, Nahar P, Shah S, et al. A comparative study of<br />
effects of omega-3 fatty acids, alpha lipoic acid and vitamin E<br />
in T2DM. Ann Med Health Sci Res 2013;3(3):442�6.



 PubMed was searched from the earliest possible date to May 2014 to identify review articles that outlined the pathophysiology of MetS and T2DM. This led to further search refinements to identify inflammatory mechanisms that occur in the pancreas, adipose tissue, skeletal muscle, and hypothalamus. Searches were also refined to identify relationships among diet, supplements, and glycemic regulation. Both animal and human studies were reviewed. The selection of specific supplements was based on those that were most commonly used in the clinical setting, namely, gymnema sylvestre, vanadium, chromium and ?-lipoic acid.
PubMed was searched from the earliest possible date to May 2014 to identify review articles that outlined the pathophysiology of MetS and T2DM. This led to further search refinements to identify inflammatory mechanisms that occur in the pancreas, adipose tissue, skeletal muscle, and hypothalamus. Searches were also refined to identify relationships among diet, supplements, and glycemic regulation. Both animal and human studies were reviewed. The selection of specific supplements was based on those that were most commonly used in the clinical setting, namely, gymnema sylvestre, vanadium, chromium and ?-lipoic acid.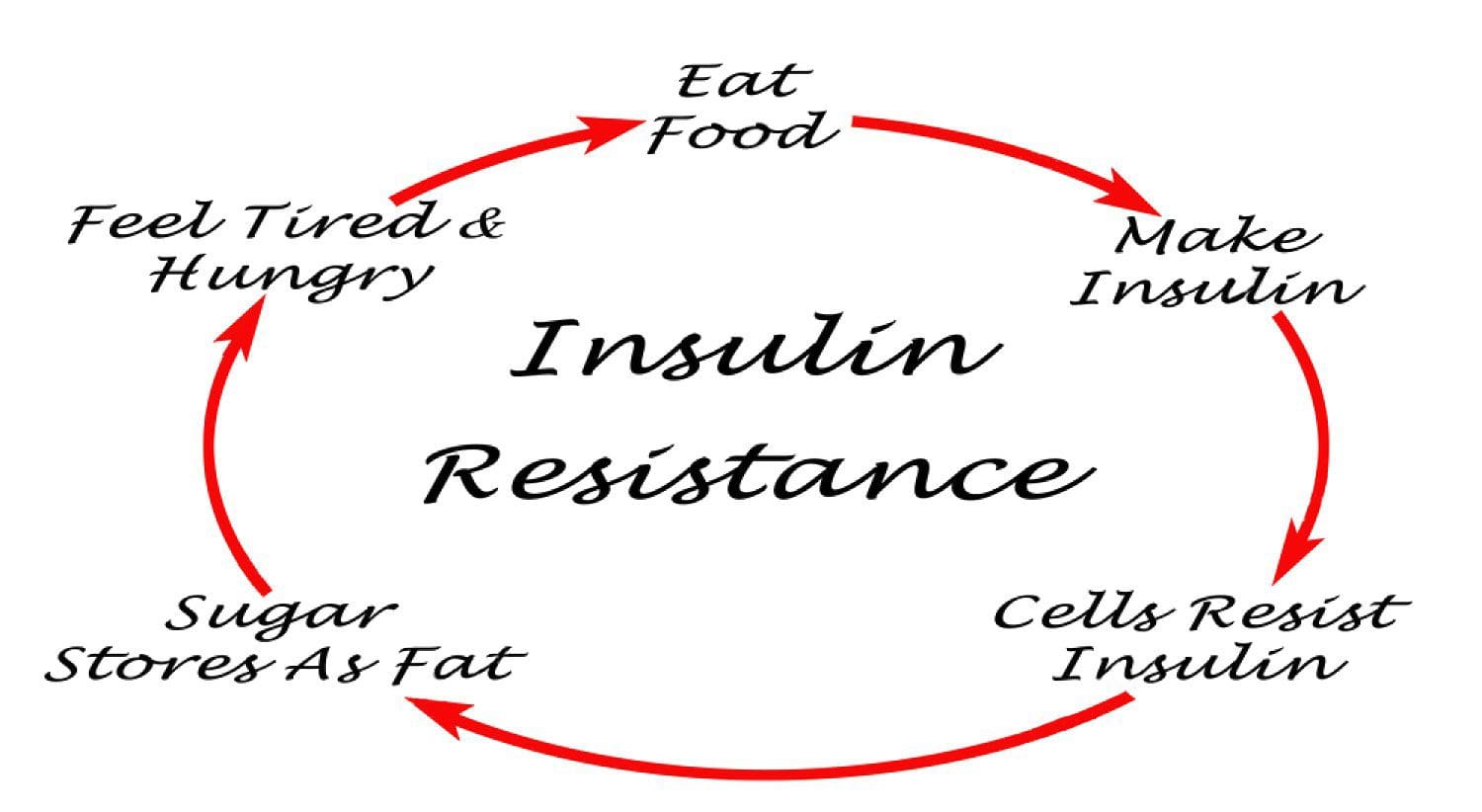 Under normal conditions, skeletal muscle, hepatic, and adipose tissues require the action of insulin for cellular glucose entry. Insulin resistance represents an inability of insulin to signal glucose passage into insulin-dependent cells. Although a genetic predisposition can exist, the�etiology of insulin resistance has been linked to chronic low-grade inflammation.1 Combined with insulin resistance-induced hyperglycemia, chronic low-grade inflammation also sustains MetS pathophysiology.1
Under normal conditions, skeletal muscle, hepatic, and adipose tissues require the action of insulin for cellular glucose entry. Insulin resistance represents an inability of insulin to signal glucose passage into insulin-dependent cells. Although a genetic predisposition can exist, the�etiology of insulin resistance has been linked to chronic low-grade inflammation.1 Combined with insulin resistance-induced hyperglycemia, chronic low-grade inflammation also sustains MetS pathophysiology.1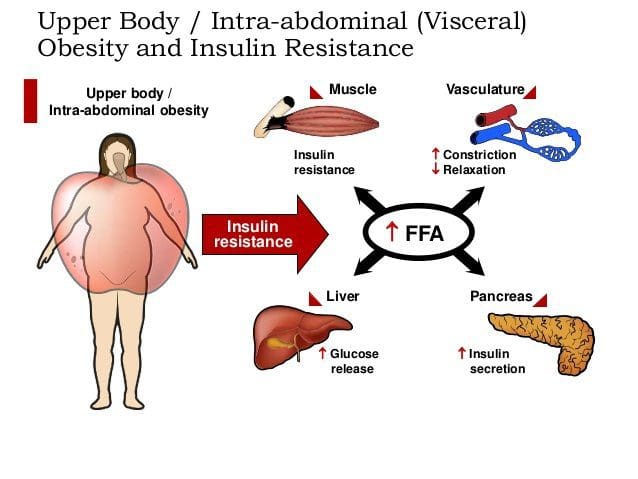 Caloric excess and a sedentary lifestyle contribute to the accumulation of subcutaneous and visceral adipose tissue. Adipose tissue was once thought of as a metabolically inert passive energy depot. A large body of evidence now demonstrates that excess visceral adipose tissue acts as a driver of chronic low-grade inflammation and insulin resistance.27,34
Caloric excess and a sedentary lifestyle contribute to the accumulation of subcutaneous and visceral adipose tissue. Adipose tissue was once thought of as a metabolically inert passive energy depot. A large body of evidence now demonstrates that excess visceral adipose tissue acts as a driver of chronic low-grade inflammation and insulin resistance.27,34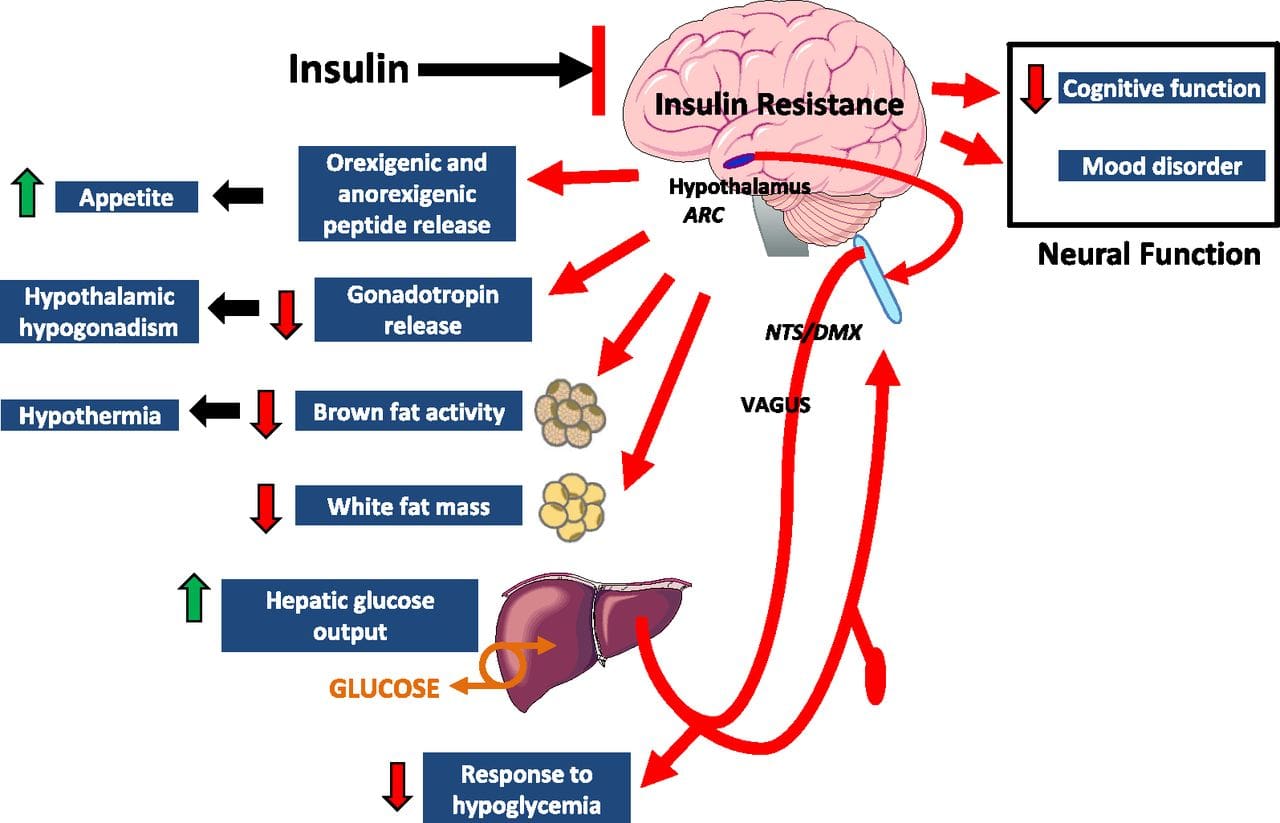 Eating behavior in the obese and overweight has been popularly attributed to a lack of will power or genetics. However, recent research has demonstrated a link between hypothalamic inflammation and increased body weight.41,41
Eating behavior in the obese and overweight has been popularly attributed to a lack of will power or genetics. However, recent research has demonstrated a link between hypothalamic inflammation and increased body weight.41,41 Feeding generally leads to a short-term increase in both oxidative stress and inflammation. 41 Total�calories consumed, glycemic index, and fatty acid profile of a meal all influence the degree of postprandial inflammation. It is estimated that the average American consumes approximately 20% of calories from refined sugar, 20% from refined grains and flour, 15% to 20% from excessively fatty meat products, and 20% from refined seed/legume oils.45 This pattern of eating contains a macronutrient composition and glycemic index that promote hyperglycemia, hyperlipemia, and an acute postprandial inflammatory response. 46 Collectively referred to as postprandial dysmetabolism, this pro-inflammatory response can sustain levels of chronic low-grade inflammation that leads to excess body fat, coronary heart disease (CHD), insulin resistance, and T2DM.28,29,47
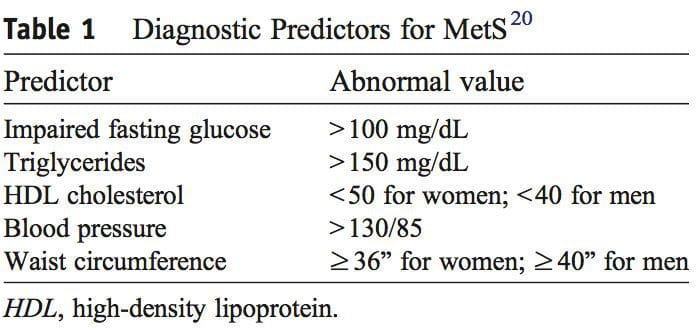
Feeding generally leads to a short-term increase in both oxidative stress and inflammation. 41 Total�calories consumed, glycemic index, and fatty acid profile of a meal all influence the degree of postprandial inflammation. It is estimated that the average American consumes approximately 20% of calories from refined sugar, 20% from refined grains and flour, 15% to 20% from excessively fatty meat products, and 20% from refined seed/legume oils.45 This pattern of eating contains a macronutrient composition and glycemic index that promote hyperglycemia, hyperlipemia, and an acute postprandial inflammatory response. 46 Collectively referred to as postprandial dysmetabolism, this pro-inflammatory response can sustain levels of chronic low-grade inflammation that leads to excess body fat, coronary heart disease (CHD), insulin resistance, and T2DM.28,29,47 Diagnosis of MetS has been linked to an increased risk of developing T2DM and cardiovascular disease over the following 5 to 10 years. 1 It further increases a patient’s risk of stroke, myocardial infarction, and death from any of the aforementioned conditions.1
Diagnosis of MetS has been linked to an increased risk of developing T2DM and cardiovascular disease over the following 5 to 10 years. 1 It further increases a patient’s risk of stroke, myocardial infarction, and death from any of the aforementioned conditions.1 Research has identified nutrients that play key roles in promoting proper insulin sensitivity, including vitamin D, magnesium, omega-3 (n-3) fatty acids, curcumin, gymnema, vanadium, chromium, and ?-lipoic acid. It is possible to get adequate vitamin D from sun exposure and adequate amounts of magnesium and omega-3 fatty acids from food. Contrastingly, the therapeutic levels of chromium and ?-lipoic acid that affect insulin sensitivity and reduce�insulin resistance cannot be obtained in food and must be supplemented.
Research has identified nutrients that play key roles in promoting proper insulin sensitivity, including vitamin D, magnesium, omega-3 (n-3) fatty acids, curcumin, gymnema, vanadium, chromium, and ?-lipoic acid. It is possible to get adequate vitamin D from sun exposure and adequate amounts of magnesium and omega-3 fatty acids from food. Contrastingly, the therapeutic levels of chromium and ?-lipoic acid that affect insulin sensitivity and reduce�insulin resistance cannot be obtained in food and must be supplemented.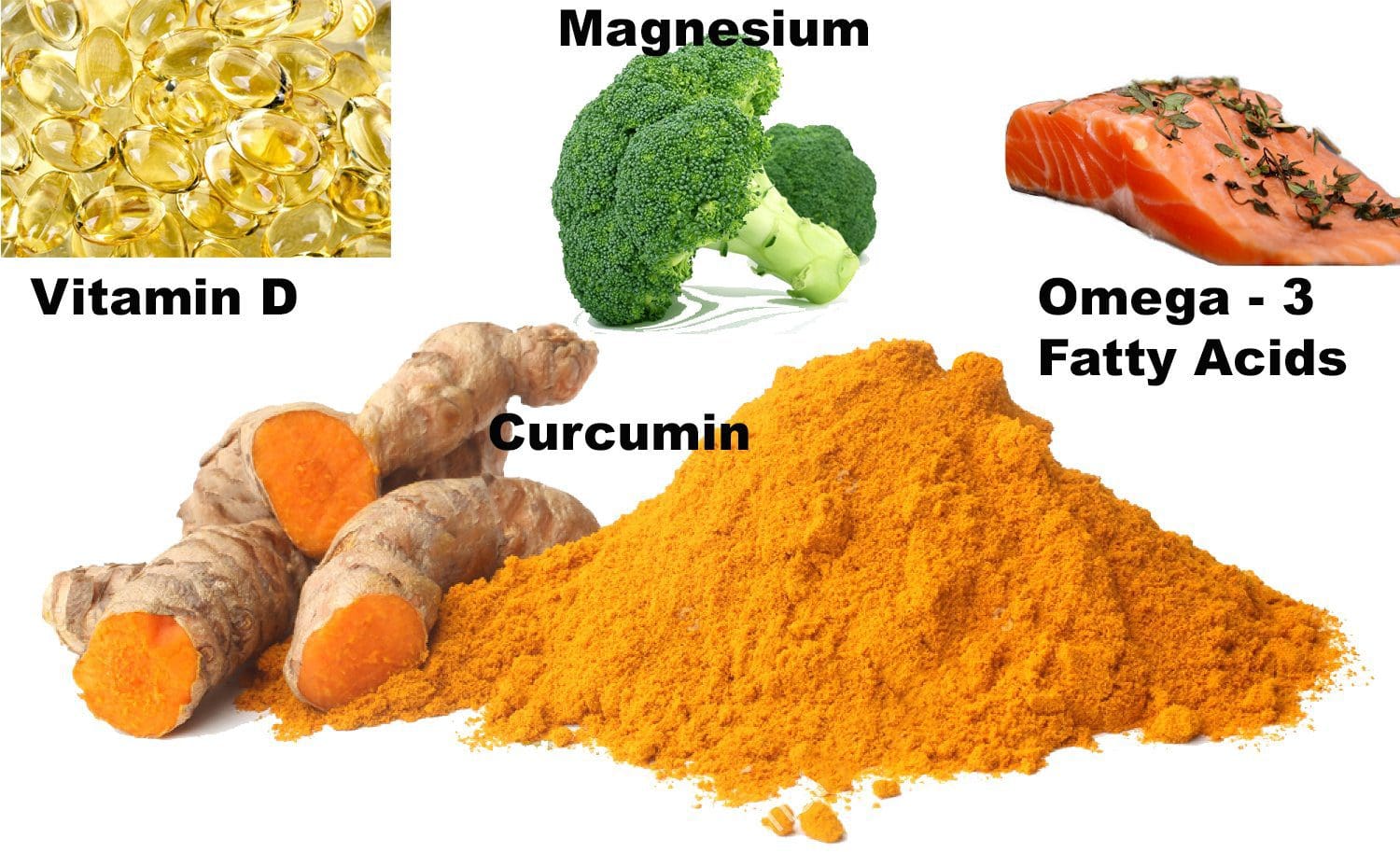 Vitamin D, magnesium, and n-3 fatty acids have multiple functions, and generalized inflammation reduction is a common mechanism of action.74�80 Their supplemental use should be considered in the context of low-grade inflammation reduction and health promotion, rather than as a specific treatment for MetS or T2DM.
Vitamin D, magnesium, and n-3 fatty acids have multiple functions, and generalized inflammation reduction is a common mechanism of action.74�80 Their supplemental use should be considered in the context of low-grade inflammation reduction and health promotion, rather than as a specific treatment for MetS or T2DM. Gymnemic acids are the active component of the G sylvestre plant leaves. Gymnemic acids are the active component of the G sylvestre plant leaves. Studies evaluating G sylvestre’s effects on diabetes in humans have generally been of poor methodological quality. Experimental animal studies have found that gymnemic acids may decrease glucose uptake in the small intestine, inhibit gluconeogenesis, and reduce hepatic and skeletal muscle insulin resistance.99 Other animal studies suggest that gymnemic acids may have comparable efficacy in reducing blood sugar levels to the first-generation sulfonylurea, tolbutamide.100
Gymnemic acids are the active component of the G sylvestre plant leaves. Gymnemic acids are the active component of the G sylvestre plant leaves. Studies evaluating G sylvestre’s effects on diabetes in humans have generally been of poor methodological quality. Experimental animal studies have found that gymnemic acids may decrease glucose uptake in the small intestine, inhibit gluconeogenesis, and reduce hepatic and skeletal muscle insulin resistance.99 Other animal studies suggest that gymnemic acids may have comparable efficacy in reducing blood sugar levels to the first-generation sulfonylurea, tolbutamide.100 Vanadyl sulfate has been reported to prolong the events of insulin signaling and may actually improve insulin sensitivity.101 Limited data suggest that it inhibits gluconeogenesis, possibly ameliorating hepatic insulin resistance. 100,101 Uncontrolled clinical trials have reported improvements in insulin sensitivity using 50 to 300 mg daily for periods ranging from 3 to 6 weeks. 101�103 Contrastingly, a recent randomized, double-blind, placebo-controlled trial found that 50 mg of vanadyl sulfate twice daily for 4 weeks had no effect in individuals with impaired glucose tolerance. 104 Limited clinical and experimental data exist supporting the use of vanadyl sulfate to improve insulin resistance,�and further research is warranted regarding its safety and efficacy.
Vanadyl sulfate has been reported to prolong the events of insulin signaling and may actually improve insulin sensitivity.101 Limited data suggest that it inhibits gluconeogenesis, possibly ameliorating hepatic insulin resistance. 100,101 Uncontrolled clinical trials have reported improvements in insulin sensitivity using 50 to 300 mg daily for periods ranging from 3 to 6 weeks. 101�103 Contrastingly, a recent randomized, double-blind, placebo-controlled trial found that 50 mg of vanadyl sulfate twice daily for 4 weeks had no effect in individuals with impaired glucose tolerance. 104 Limited clinical and experimental data exist supporting the use of vanadyl sulfate to improve insulin resistance,�and further research is warranted regarding its safety and efficacy. Diets high in refined sugar and flour are deficient in chromium (Cr) and lead to an increased urinary excretion of chromium. 105,106 The progression of MetS is not likely caused by a chromium deficiency, 107 and dosages that benefit glycemic regulation are not achievable through food. 106,108,109
Diets high in refined sugar and flour are deficient in chromium (Cr) and lead to an increased urinary excretion of chromium. 105,106 The progression of MetS is not likely caused by a chromium deficiency, 107 and dosages that benefit glycemic regulation are not achievable through food. 106,108,109 Humans derive ?-lipoic acid through dietary means and from endogenous synthesis. 111 The foods richest in ?-lipoic acid are animal tissues with extensive metabolic activity such as animal heart, liver, and kidney, which are not consumed in large amounts in the typical American diet. 111 Supplemental amounts of ?-lipoic acid used in the treatment of T2DM (300-600 mg) are likely to be as much as 1000 times greater than the amounts that could be obtained from the diet.112
Humans derive ?-lipoic acid through dietary means and from endogenous synthesis. 111 The foods richest in ?-lipoic acid are animal tissues with extensive metabolic activity such as animal heart, liver, and kidney, which are not consumed in large amounts in the typical American diet. 111 Supplemental amounts of ?-lipoic acid used in the treatment of T2DM (300-600 mg) are likely to be as much as 1000 times greater than the amounts that could be obtained from the diet.112 This is a narrative overview of the topic of MetS. A systematic review was not performed; therefore, there may be relevant information missing from this review. The contents of this overview focuses on the opinions of the authors, and therefore, others may disagree with our opinions or approaches to management. This overview is limited by the studies that have been published. To date, no studies have been published that identify the effectiveness of a combination of a dietary intervention, such as the Spanish
This is a narrative overview of the topic of MetS. A systematic review was not performed; therefore, there may be relevant information missing from this review. The contents of this overview focuses on the opinions of the authors, and therefore, others may disagree with our opinions or approaches to management. This overview is limited by the studies that have been published. To date, no studies have been published that identify the effectiveness of a combination of a dietary intervention, such as the Spanish 
 The prevalence of obesity in the United States has been increasing for almost 50 years. Currently, more than two-thirds of adults and almost one-third of children and adolescents are
The prevalence of obesity in the United States has been increasing for almost 50 years. Currently, more than two-thirds of adults and almost one-third of children and adolescents are 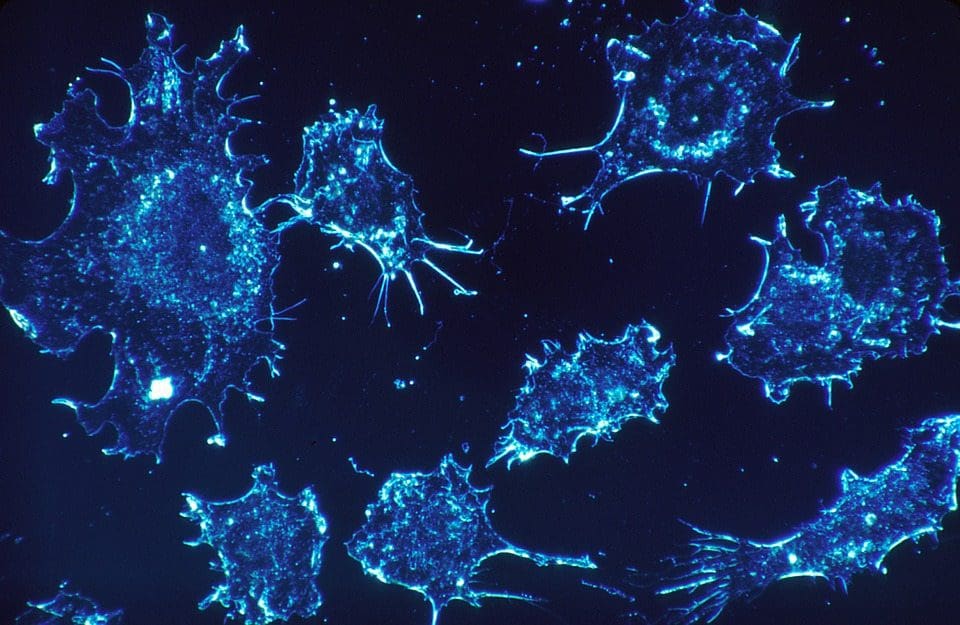
 From 2005 to 2014, there was a 1.4% annual increase in cancers related to overweight and obesity among individuals aged 20 to 49 years and a 0.4% increase in these cancers among individuals aged 50 to 64 years. For example, if cancer rates had stayed the same in 2014 as they were in 2005, there would have been 43?000 fewer cases of colorectal cancer but 33?000 more cases of other cancers related to overweight and obesity. Nearly half of all cancers in people younger than 65 years were associated with overweight and obesity. Overweight and obesity among younger people may exact a toll on individuals� health earlier in their lifetimes.
From 2005 to 2014, there was a 1.4% annual increase in cancers related to overweight and obesity among individuals aged 20 to 49 years and a 0.4% increase in these cancers among individuals aged 50 to 64 years. For example, if cancer rates had stayed the same in 2014 as they were in 2005, there would have been 43?000 fewer cases of colorectal cancer but 33?000 more cases of other cancers related to overweight and obesity. Nearly half of all cancers in people younger than 65 years were associated with overweight and obesity. Overweight and obesity among younger people may exact a toll on individuals� health earlier in their lifetimes.
 The
The  Implementation of clinical interventions, including screening, counseling, and referral, has major challenges. Since 2011, Medicare has covered behavioral counseling sessions for weight loss in primary care settings. However, the benefit has not been widely utilized.
Implementation of clinical interventions, including screening, counseling, and referral, has major challenges. Since 2011, Medicare has covered behavioral counseling sessions for weight loss in primary care settings. However, the benefit has not been widely utilized. Achieving sustainable weight loss requires comprehensive strategies that support patients� efforts to make significant lifestyle changes. The availability of clinical and community programs and services to which to refer patients is critically important. Although such programs are available in some communities, there are gaps in availability. Furthermore, even when these programs are available, enhancing linkages between clinical and community care could improve patients� access. Linking community obesity prevention, weight management, and physical activity programs with clinical services can connect people to valuable prevention and intervention resources in the communities where they live, work, and play. Such linkages can give individuals the encouragement they need for the lifestyle changes that maintain or improve their health.
Achieving sustainable weight loss requires comprehensive strategies that support patients� efforts to make significant lifestyle changes. The availability of clinical and community programs and services to which to refer patients is critically important. Although such programs are available in some communities, there are gaps in availability. Furthermore, even when these programs are available, enhancing linkages between clinical and community care could improve patients� access. Linking community obesity prevention, weight management, and physical activity programs with clinical services can connect people to valuable prevention and intervention resources in the communities where they live, work, and play. Such linkages can give individuals the encouragement they need for the lifestyle changes that maintain or improve their health. The high prevalence of overweight and obesity in the United States will continue to contribute to increases in health consequences related to obesity, including cancer. Nonetheless, cancer is not inevitable; it is possible that many cancers related to overweight and obesity could be prevented, and physicians have an important responsibility in educating patients and supporting patients� efforts to lead healthy lifestyles. It is important for all health care professionals to emphasize that along with quitting or avoiding tobacco, achieving and maintaining a healthy weight are also important for reducing the risk of cancer.
The high prevalence of overweight and obesity in the United States will continue to contribute to increases in health consequences related to obesity, including cancer. Nonetheless, cancer is not inevitable; it is possible that many cancers related to overweight and obesity could be prevented, and physicians have an important responsibility in educating patients and supporting patients� efforts to lead healthy lifestyles. It is important for all health care professionals to emphasize that along with quitting or avoiding tobacco, achieving and maintaining a healthy weight are also important for reducing the risk of cancer.







