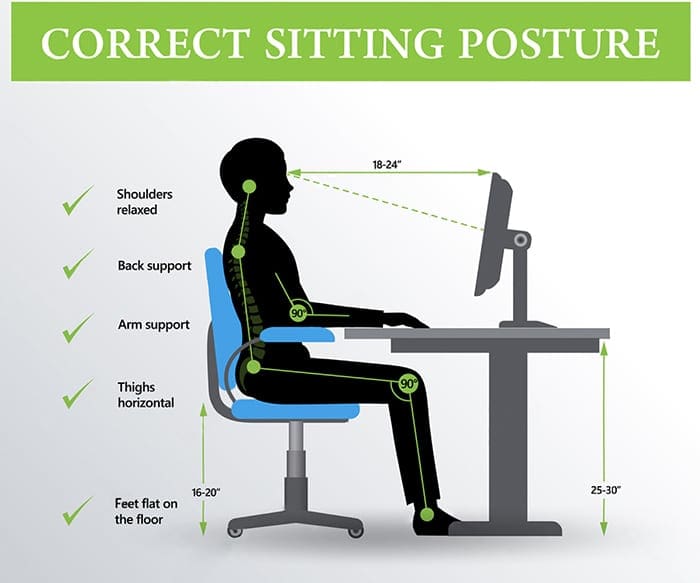
Question: I work at a desk all day and have started to feel pain in my neck, back, shoulders and arms. Can chiropractors help with sitting posture and general posture?
El Paso, TX. Chiropractor, Dr. Alexander Jimenez provides insight into proper sitting posture and general posture through chiropractic.
Have people asked you about using a posture brace to help correct their sitting habits? Chiropractic patients with moderate posture problems, meaning that they may be chronic but are not tied to any spinal column or other medical condition, may benefit from a posture back brace to improve this condition. There are a number of great ones available, and you can see more information about some of the top ones here.
A patient such as this will almost certainly enjoy the quick referral as well as the relatively fast results, and chiropractors get an easy opportunity to help people, which explains why many enter the profession in the first place.
But if the patient does have an underlying chiropractic ailment, a back brace will probably do little if any good. These issues are usually easily diagnosed using a quick examination, and afterwards, treatment is relatively straightforward as well.
Diagnosing Conditions
All good exams begin with thorough health history, because in most cases, family history is among the most powerful indicators about current issues.
Next, observe the individual’s gait, as how someone walks shows a number of issues. For instance, those who stand or walk with their legs abnormally spread might have fallen arches. Because the bottom of the foot isn’t in appropriate contact with the floor, the whole body has been thrown off kilter, resulting in poor posture. While it isn’t really a chiropractic condition, fallen arches are, as simple as, a referral to an orthopedist.
Moreover, if the patient is experiencing pain, the location can be an indicator as to where the muscles may be weak and there is too much strain on the spine or a different region of the body. Muscle weakness is among the leading causes of poor posture. So, follow-up tests that measure muscle strength and range of movement are usually a good idea.
If the gait examination signals issues in a particular area of the body, the professional should concentrate further diagnostic efforts in that region.
Ultimately, one of the most simple and effective evaluations is just holding a yardstick or comparable object against the patient’s back, so the two of you can definitely see any abnormalities. This comprehensive approach generally describes some of the very frequent chiropractic posture issues, including:
Tissue Damage:
If the neck, lower back, mid back, or any other area is weak and/or inflexible, the individual will probably not see very much posture improvement until these conditions are adjusted and the muscles have been strengthened.
Kyphosis:
Hunchback is a degenerative spine condition that’s very prevalent in women over 60. While more advanced cases may be life threatening and may require spinal fusion surgery, most men and women respond well to therapeutic adjustments and other treatments.
Scoliosis:
This condition is much like genetically-induced kyphosis, since there’s no cure but there are several therapies available. In extreme cases, surgery may be necessary.
Un-Level Pelvis/Pelvic Tilt:
A pelvic tilt, a lower sacral base, and a femur head discrepancy can indicate a lower extremity source, but not�whether it is an anatomical or functional short leg. A clinical postural exam with lower extremity screening is the only way to make this determination.
Forward Head Posture:
The anterior positioning of the cervical spine. This posture is sometimes called Scholar’s Neck, Wearsie Neck, Hunch & or Reading Neck.It is a posture problem that is due to several factors including sleeping with the head raised too high, prolonged use of computers and cellphones, lack of developed back muscle strength and deficiency of nutrients like calcium. Potential negative effects include tingling and numbness in the arms, and a burning pain between the shoulder blades.
Treatment
As stated previously, back braces frequently mend postural issues, like slouching. As for structural problems, like scoliosis, more aggressive treatments are needed.
Conventional treatment consists of:
Heat
Massage
Stretching
Strength exercises
Supportive braces
There are a number of biofeedback tools that accurately evaluate patient progress.
As a chiropractor, your patients count on you to get much better. That almost always means accurately assessing the problem, which also means a quick and capable referral or an aggressive and well thought out therapy regimen.
The Narrative Of JFK Shows The Difficulty In Diagnosing & Treating Spinal Disorders.
At age 43, John F. Kennedy was the youngest president elected into U.S. workplace, and has been depicted as full of youth and vitality. But he was far from healthy, and spent most of his adult life fighting with many medical issues, including back pain which started during college and continued until his death, according to a recent review article from the Journal of Neurosurgery: Spine.
John F. Kennedy’s back pain is thought to have started following a football injury, while Kennedy was in undergraduate school at Harvard, clarified coauthor Justin T. Dowdy, MD, who is a neurosurgeon at Hot Springs Neurosurgery Clinic, in Hot Springs, Arkansas.
Based on 10 years of study on Kennedy’s medical documents and reported symptoms, senior author T. Glenn Pait, MD, believes Kennedy had discogenic disease stemming from an accident in his childhood that began a cascade of problems in his low back. Dr. Pait is Director of the Jackson T. Stephens Spine and Neurosciences Institute at the University of Arkansas for Medical Sciences.
Kennedy was originally rejected when trying to enlist in the Army due to his medical issues, such as back pain, but was eventually accepted in the U.S. Naval Reserve during his dad’s connections. “This is a testament to his decision to serve his country,” Dr. Pait said. “Kennedy was originally given a desk job, but that was not enough for him, and he was later admitted into a patrol torpedo program.”
Kennedy’s back issues worsened when his naval boat was hit by a Japanese destroyer, and Kennedy drifted for 5 hours to a nearby island while towing an injured crewman to shore by holding the ring of the man’s life jacket between his teeth, Drs. Dowdy and Pait noted in their newspaper.
The review article refers to a series of 4 ineffective surgeries, including a sacroiliac (SI) and lumbosacral fusion. Various doctors who treated Kennedy had different theories about the reason for his back pain, also suggested a variety of different treatments ranging from trigger point injections and an exercise program (swimming and weight lifting), to massage and a back brace, to methamphetamine-containing shots. The exercise program, started later in his life, produced “dramatic” improvement, according to the researchers. The program consisted of weight lifting three times each week and everyday swimming plus massage and heat therapy.
“JFK’s narrative illustrates the difficulty and complexity in diagnosing and treating spinal disorders, especially in the context of chronic pain,” Dr. Dowdy advised SpineUniverse. “Our spines age as we age if it’s degenerative disk disease, pinched nerves, or spinal stenosis–imaging abnormalities are certain to appear later in life. Treating and preventing these disorders is just as much of an art as it’s a science, particularly in determining those individuals who will probably benefit from surgery.”
Dr. Dowdy noted that much progress has been made in how spinal conditions are diagnosed and treated as the time when Kennedy sought attention, such as “that the refinement of both less-invasive spine surgery methods and diagnostic imaging.” Dr. Dowdy also emphasized an important point that applies to any era: “the significance of having a trusted spine surgeon who is prepared and capable of supplying the right surgery in the appropriate conditions.”
John F. Kennedy’s story also suggests that “the most beneficial methods to prevent chronic back pain may be accessible and affordable,” Dr. Dowdy stated. “Often the most appropriate strategy for chronic low back pain is actively pursuing proper spine hygiene: maintaining healthy body weight, refraining from smoking, and pursuing a nutritious diet and exercise–especially workouts comprising yoga-style stretches,” Dr. Dowdy emphasized. “It boils down to pursuing a healthy and active way of life.”
“Individuals who suffer from chronic pain may hopefully be inspired to know that Kennedy remained physically energetic and driven to accomplish his goals despite his annoyance,” Dr. Dowdy concluded.
Herniated discs are a common condition that can occur anywhere along the back or spine, but most often affects the lower back or neck region of the spine.
Also known as a slipped disc or ruptured disc, a herniated disc develops when one or several of the pads found between the vertebrae moves from position and presses on adjacent nerves, resulting in a variety of painful symptoms.
Herniated discs are caused by overuse injuries or trauma to the spine, nonetheless, disc conditions can also develop as a result of the normal aging process or due to degeneration. It’s also understood that there is a genetic element that leads to the development of disc herniation and disc degeneration.
Symptoms of a herniated disc may generally include sharp or dull pain and discomfort, muscle spasm or cramping, fatigue, tingling sensations, numbness or referred pain.
But here is something to consider: From time to time, a disc does not cause any symptoms . That’s called an asymptomatic herniated disc. Your intervertebral disc could be bulging or herniated, but it won’t cause any symptoms, such as pain, unless it is pressing on the spinal cord, its nerve roots or individual nerves.
This brings up a fantastic point about herniated disc symptoms: Your symptoms are dependent on where you’ve got a herniated disc.
Cervical Herniated Disc Symptoms
If you’ve got a herniated disc or bulging disc on your neck (cervical spine), then you will experience:
Neck pain
Muscle tightness or cramping on your neck
Pain which radiates (or travels) down your arm(s) (this can be called referred pain or cervical radiculopathy)
Tingling in your arm(s) or hand(s)
Weakness in your arm(s) or hand(s)
Lumbar Herniated Disc Symptoms
A herniated disc in the low back (lumbar spine) may cause the following symptoms:
Low back pain
Muscle tightness or cramping in your back
Pain that radiates down your leg(s) (this can be known as referred pain, lumbar radiculopathy, or sciatica)
Tingling in your leg(s) or foot/feet
Weakness in your leg(s) or foot/feet
Really infrequent: Loss of bowel or bladder control (Please, even if this occurs, seek prompt medical care.)
A Note on Referred Pain Brought on by a Herniated Disc
Referred pain means that you’ve got pain in another part of your body as a result of the intervertebral disc issue. As an example, in case you’ve got a bulging disc or a herniated disc in your low back (lumbar spine), you may have known pain in your leg. This is called lumbar radiculpathy or sciatica, a shooting pain that can extend from the buttock into the leg and to the foot. Only one leg is typically affected.
When you’ve got a herniated disc in your neck (cervical spine), then you may have referred pain down your arm and into your hand. Arm and shoulder pain caused by a herniated disc is also called radiculopathy.
Lower Back Pain: Causes & Symptoms (Video)
Herniated Disc Symptoms: When Should You Find a Doctor?
The pain from a herniated disc can make it hard to enjoy your daily life; it may make it tough to walk, sit, or even sleep comfortably. If your disc symptoms linger for more than fourteen days, you should make a doctor appointment. Should you experience unexpected onset of pain (after lifting something heavy incorrectly, as an instance), call your physician.
It’s very rare, but herniated discs can sometimes affect bowel or bladder control (as mentioned above). If this occurs, seek medical attention immediately for a proper diagnosis, followed up by treatment.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sciatica
Lower back pain is one of the most commonly reported symptoms among the general population. Sciatica, is well-known group of symptoms, including lower back pain, numbness and tingling sensations, which often describe the source of an individual’s lumbar spine issues. Sciatica can be due to a variety of injuries and/or conditions, such as spinal misalignment, or subluxation, disc herniation and even spinal degeneration.
Chiropractor, Dr. Alex Jimenez looks at lumbar spine disc herniation. What are the Likely signs and symptoms associated with disc herniation, and what would be the selection criteria for micro-discectomy operation in athletes? Complaint in the young college age athlete and professional athlete, and it’s been estimated that over 30% of athletes complain of back pain at least once in the profession(1).
Lumbar spinal disc herniation is one kind Of lumbar injury that can’t just cause painful low back pain, but can also compress nerve roots and create radicular referral of pain into the lower leg with related sensation changes and muscle contraction. This injury will not only influence the short-term opponent ability of the athlete, but might also reoccur and eventually become persistent possibly causing a career ending injury.
Managing disc herniation from the athlete Usually begins with conservative therapy and if this fails, surgical solutions are considered. But often elite athletes will request a quicker resolution to their symptoms to minimize time away from competitors. Therefore, providing the criteria for lumbar spine surgery are suggested, the conservative period will often be compressed, and surgery will be sought earlier. The favored surgical process for the athlete with a disc herniation is that the lumbar disc micro-discectomy.
Anatomy & Biomechanics
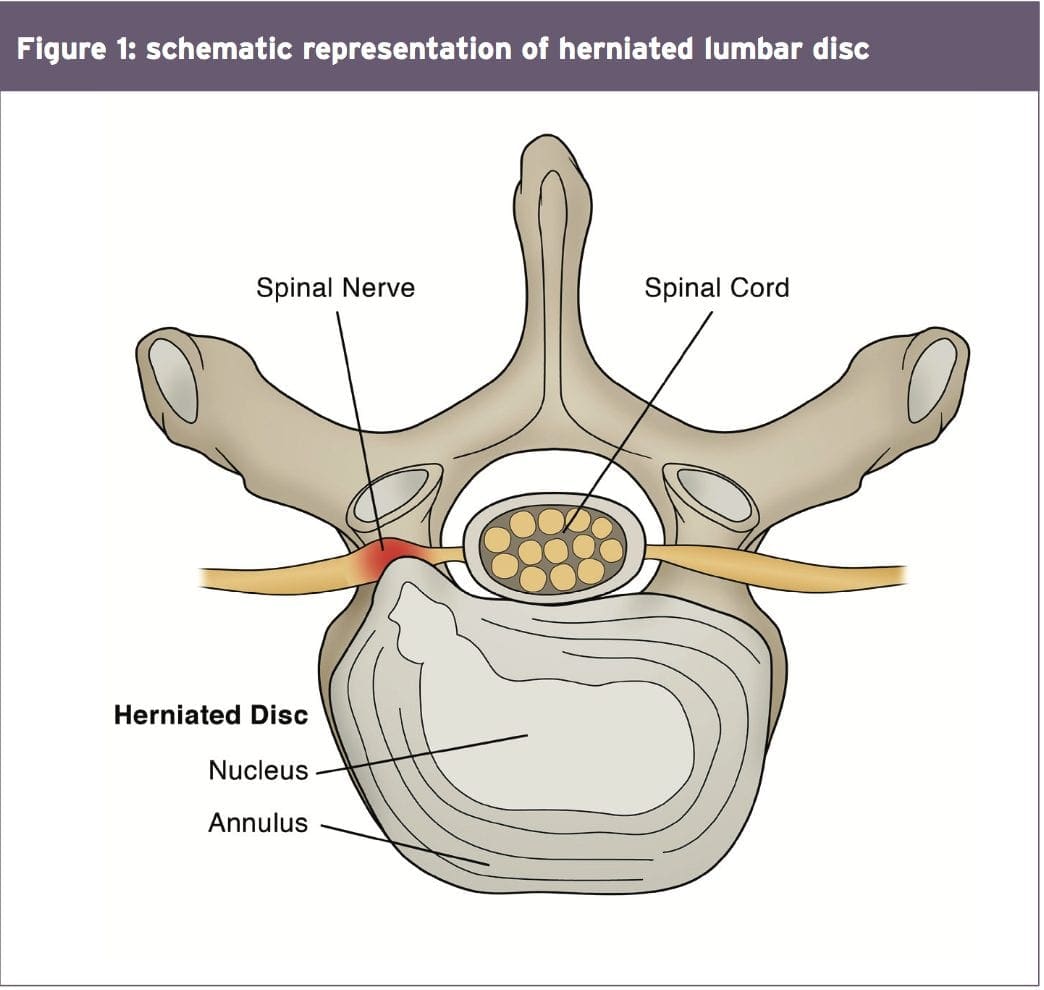
A significant biomechanical role in the spine, allowing for motion between the spinal segments while spreading compressive, shear, and torsional forces(2). These discs include a thick outer ring of fibrous cartilage termed the annulus fibrosis (akin to the onion rings enclosing the center of the onion), which encompasses a more gelatinous core called the nucleus pulposus, which is included within the cartilage end plates inferiorly and superiorly.
The intervertebral disc consists of Cells and substances such as collagen, proteoglycans, and thin fibrochondrocytic tissues, which enable transmission and absorption of forces arising from body weight and muscle activity. To do so, the disc depends mainly on the structural condition of the nucleus pulposus, annulus fibrosis and the vertebra lend plate. If the disc is normal and is functioning optimally, then forces are spread across the disc evenly(3).
But disc degeneration (mobile Degradation, lack of hydration( disc failure) may decrease the capacity of the disc to withstand extrinsic forces, as forces are no longer distributed and spread evenly. Tears and fissures from the annulus can lead, and with adequate external forces, the disc material may herniate. Alternatively, a sizable biomechanical force set on a healthy, ordinary disc may cause extrusion of disc material as a result of crushing failure of this annular fibers — illustrations include a hefty compression type mechanism because of a fall on the tailbone, or strong muscle contraction such as heavy weight lifting(4).
Herniations represent protrusions of Disc material beyond the confines of this annular lining and in the spinal canal (see Figure 1)(5). If the protrusion does not invade the canal or undermine nerve roots then back pain may be the only symptom.
Endoscopic Discectomy 3D Simulation
The pain associated with lumbar Radiculopathy happens due to a mix of nerve root ischemia (due to compression) and inflammation (because of neurochemical inflammatory mediators released from the disc). Throughout a herniation, the nucleus pulposus puts pressure on weakened regions of the annulus, and proceeds through the diminished websites in the annulus in which it ultimately forms a herniation(6 ft). It follows from this that some kind of disc degeneration may exist prior to the disc may really herniated(7).
In contrast to other respiratory Tissues, discs have a inclination to degenerate earlier in life, with some studies demonstrating adolescents presenting signs of degeneration between the ages of 11 to 16(8). With increasing age, there’s further degeneration of the intervertebral discs.
While the disc might be in danger of harm in All fundamental planes of motion, it’s particularly susceptible during repetitive flexion, or hyper-flexion, combined with lateral bending or rotation(10). Traumatic events such as excessive axial compression may also damage the inner structure of the disc. This can occur as a result of a fall or powerful muscular forces developed during tasks such as heavy lifting.
Athletes are generally exposed to high loading conditions. Examples of this include:
1. World-class power lifters, in which the calculated compressive loads on the backbone are involving 18800 Newtons (N) and also 36400N acting in the L3-4 motion segment(11).
2. Elite level football linesmen who have Been proven to present time-related hypertrophy of this disc and changes in vertebrae endplate in response to this repetitive high loading and axial pressure(12).
3. Long distance runners have been Shown to undergo significant strain into the intervertebral disc, indicated by a reduction in disc height(13).
Herniations could be classified depending on Ultimately, herniations are also identified based on level, with most herniations happening at the L4/5 and L5/S1 intervertebral disc level; these can then in turn affect the L5 and S1 nerve roots resulting in clinical sciatica(15). Upper level herniations are less common, and when they do occur with radiculopathy, they will affect the femoral nerve. Finally, the prevalence of disc injury rises increasingly caudally, with the best numbers at the L5/S1 degrees(16).
Herniation In Athletes
The offending movements implicated in The 20-35 age group are the most common group to herniate a disc, most likely because of the fluid nature of the nucleus pulposis and due to behavior(18). This age group are more likely to participate in sports which need high lots of flexion and spinning or are reckless with their positions and positions during loading.
The sports most at risk of disc herniation are:
Hockey
Wrestling
Soccer
Swimming
Basketball
Golf
Tennis
Weightlifting
Rowing
Throwing events
These are the sports that involve either significant Furthermore, those who take part in more and more severe training regimes seem to be at higher risk of spinal pathologies, as do people involved in sports.
Signs & Symptoms Indicating Discectomy
The efficacy of management programs for lumbar spine disc herniation — in terms of the decision to operate or treat conservatively — will be discussed in greater depth in part 2 of this series. However, the decision to operate within an athlete is generally driven by the motivation and approaching goals the athlete has put themselves. They may in fact favor a comparatively simple micro-discectomy instead of waiting for symptoms to abate through an extended period of rehabilitation.
This conservative period of Management may involve medicine therapy, epidural injections, relative back and back muscle recovery, acupuncture, osteo/chiropractic interventions. On the other hand, the normal presenting symptoms and signs that suggest a substantial disc herniation that will require surgical intervention in the athlete comprise:
Low back pain with pain radiating down one or both legs
Positive straight leg raise test
Radicular pain and neurological signs consistent with the nerve root level affected
Mild weakness of distal muscles such as extensor hallucis longus, peroneals, tibialis anterior and soleus. These would fit with the myotome relevant for the disc level
MRI confirming a disc herniation
Possible bladder and bowel symptoms
Failed conservative rehabilitation
Time span in which to enable conservative rehabilitation to be effective. In the overall population, medical practitioners will most likely prescribe a minimal 6-week traditional period of treatment with an overview at 6 weeks as to whether to expand the rehabilitation a further 6 weeks or to seek a specialist opinion. The expert may then attempt more medically orientated interventions such as epidural injections.
The athlete nevertheless will have these They might be more inclined to experience an epidural very early in the conservative period to assess the effectiveness of this procedure. If no signs of progress are evident in a couple of weeks then they may choose to get an immediate lumbar spine micro- discectomy.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques. From the El Paso, TX. Spine Center.
Imaging
MRI remains the favored system of Identifying lumbar spine disc herniation, since it’s also very sensitive to detecting nerve root impingements(23). However, abnormal MRI scans can occur in otherwise asymptomatic patients(25); hence, clinical correlation is always essential before any surgical thought. What’s more, patients can present with clinical signs and symptoms which suggest the diagnosis of acute herniated disc, and yet lack evidence of sufficient pathology on MRI to warrant operation.
Therefore it has been proposed that a Volumetric analysis of a herniated disc on MRI may be potentially beneficial in checking the suitability for operation. Several writers have previously mentioned the possible value of volumetric evaluation of herniated disc on MRI as part of their selection criteria for lumbar surgery(26).
In a survey conducted in Michigan State University, it was found that the size and positioning of the herniated disc determined that the likelihood for operation with what researchers called ‘types 2-B’ and ‘types 2-AB’ being the most likely candidates for surgery(27).
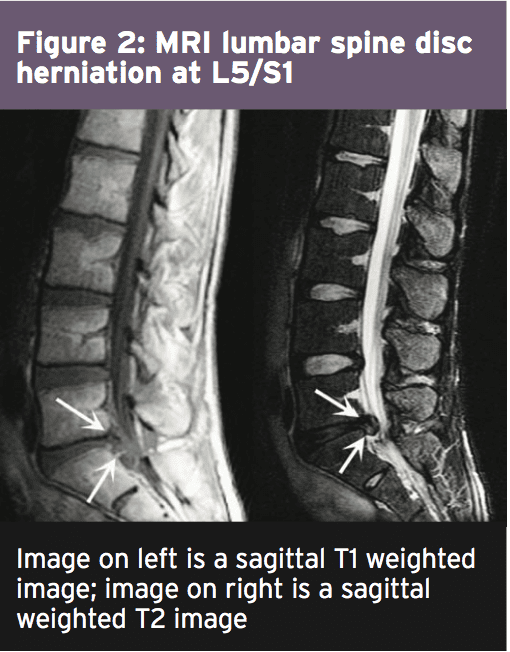
The MRI protocol to your lumbar spine consists of (see Figure 2)
1.Sagittal plane echo T1- weighted sequence
2. Sagittal fast spin echo proton density sequence
3. Sagittal fast spin echo inversion recovery sequence
4.Axial spin echo T1- weighted sequence
Summary
Disc herniations are not a common Complaint in athletes, but they do happen in sports which involve high loads or repetitive flexion and rotation movements. Sufferers of a disc herniation will normally feel focused low-back pain, maybe with referral in the lower limb with associated neurological symptoms if the nerve root was compressed.
Managing a disc herniation within an General population as frequently the risk of a Protracted failed rehabilitation period is Bypassed for the protected and low risk Micro-discectomy procedure. In the Discuss the exact surgical alternatives involved Observing a lumbar spine micro-discectomy.
References
1. Sports Med. 1996;21(4):313�20
2. Radiology. Oct 2007;245(1):62-77
3. Arthritis Research & Therapy. 2003;5(3):120-30
4. The Journal of Bone and Joint Surgery. American volume. Feb 2004;86-A(2):382 � 96
5. Radiology. Oct 2007;245(1):43-61
6. Spine. Sep 15 1996;21(18):2149-55
7. Spine. May-Jun 1982;7(3):184-91
8. Spine. Dec 1 2002;27(23):2631-44
9. Lancet 1986;2:1366�7
10. Disease-A-Month:DM. Dec 2004;50(12):636-69
11. Spine. Mar 1987;12(2):146-9
12. The American Journal of Sports Medicine. Sep 2004;32(6):1434-9
13. The Journal of International Medical Research. 2011;39(2):569-79
14. Spine. 2001;26:E93-113
15. Spine. 1990;15:679-82
16. British Journal of Sports Medicine. Jun 2003;37(3):263-6
17. Prim Care. 2005;32(1):201�29
18. McGill, S.M. Low back disorders: Evidence based prevention and rehabilitation, Human Kinetics Publishers, Champaign, IL, U.S.A., 2002. Second Edition, 2007
19. Spine. Apr 1991;16(4):437-43
20. Skeletal radiology. Jul 2006;35(7):503-9
21. British Journal of Sports Medicine. Nov 2007;41(11):836-41
22. The American Journal of Sports Medicine. Jun 2009;37(6):1208-13
23. Spine. Mar 15 1995;20(6):699-709
24. Phys Sportsmed. 2005;33(4):21�7
25. J Bone Joint Surg Am 1990 . 2:403�408
26. J Orthop Surg (Hong Kong) 2001. 9:1�7
27. Eur Spine J (2010) 19:1087�1093
This paper explores the relationship between traumatic ligament laxity of the spine and the resultant instability that may occur. Within, there is a discussion of the various spinal ligamentous structures that may be affected by both macro and micro traumatic events, as well as the neurologic and musculoskeletal effects of instability. There is detailed discussion of the diagnosis, quantification, and documentation as well.
Soft tissue cervical and lumbar sprain/strains are the most common injury in motor vehicle collisions, with 28% to 53% of collision victims sustaining this type of injury (Galasko et al., 1993; Quinlan et al., 2000). The annual societal costs of these injuries in the United States are estimated to be between 4.5 and 8 billion dollars (Kleinberger et al., 2000; Zuby et al., 2010). Soft tissue injuries of the spinal column very often become chronic, with the development of long-term symptoms, which can inevitably adversely affect the victim�s quality of life. Research has indicated that 24% of motor vehicle collision victims have symptoms 1 year after an accident and 18% after 2 years (Quinlan et al., 2004). Additionally, it has been found that between 38% and 52% of motor vehicle collision cases involved rear-impact scenarios
It is well known that the major cause of chronic pain due to these injuries is directly related to the laxity of spinal ligamentous structures (Ivancic, et al., 2008). One must fully understand the structure and function of ligaments in order to realize the effects of traumatic ligament laxity. Ligaments are fibrous bands or sheets of connective tissue which link two or more bones, cartilages, or structures together. We know that one or more ligaments provide stability to a joint during rest as well as movement. Excessive movements such as hyper-extension or hyper-flexion, which occur during a traumatic event such as a motor vehicle collision, may be restricted by ligaments, unless these forces are beyond the tensile-strength of these structures; this will be discussed later in this paper.
Ligament Laxity Spine Injury Background
Three of the more important ligaments in the spine are the ligamentum flavum, the anterior longitudinal ligament, and the posterior longitudinal ligament (Gray�s Anatomy, 40th Edition). The ligamentum flavum forms a cover over the dura mater, which is a layer of tissue that protects the spinal cord. This ligament connects under the facet joints to create a small curtain, so to speak, over the posterior openings between vertebrae (Gray�s Anatomy, 40th edition). The anterior longitudinal ligament attaches to the front (anterior) of each vertebra and runs vertical or longitudinal (Gray�s Anatomy, 40th edition). The posterior longitudinal ligament also runs vertically or longitudinally behind (posterior) the spine and inside the spinal canal (Gray�s Anatomy, 40th Edition). Additional ligaments include facet capsular ligaments, interspinous ligaments, supraspinous ligaments, and intertransverse ligaments. The aforementioned ligaments limit flexion and extension, with the exception of the ligament, which limits lateral flexion. The ligamentum nuchae, which is a fibrous membrane, limits flexion of the cervical spine (Gray�s Anatomy, 40th Edition). The four ligaments of the sacroiliac joints:
(iliolumbar, sacroiliac, sacrospinus, sacrotuberous), provide stability and some motion. The upper cervical spine has its own ligamentous structures or systems; occipitoatlantal ligament complex, occipitoaxial ligament complex, atlantoaxial ligament complex, and the cruciate ligament complex (Gray�s Anatomy, 40th Edition). The upper cervical ligament system is especially important in stabilizing the upper cervical spine from the skull to C2 (axis) (Stanley Hoppenfeld, 1976). It is important to note, that although the cervical vertebrae are the smallest, the neck has the greatest range of motion.
Causes of Ligament Laxity Injuries in the Spine
Ligament laxity may happen as a result of a �macro trauma�, such as a motor vehicle collision, or may develop overtime as a result of repetitive use injuries, or work-related injuries. The cause of this laxity develops through similar mechanisms, which leads to excessive motion of the facet joints, and will cause various degrees of physical impairment. When ligament laxity develops over time, it is defined as �creep� and refers to the elongation of a ligament under a constant or repetitive stress (Frank CB, 2004). Low-level ligament injuries, or those where the ligaments are simply elongated, represent the vast majority of cases and can potentially incapacitate a patient due to disabling pain, vertigo, tinnitus, etc.. Unfortunately, these types of strains may progress to sub-failure tears of ligament fibers, which will lead to instability at the level of facet joints (Chen HB et al., 2009). Traumatic or repetitive causes of ligament laxity will ultimately produce abnormal motion and function between vertebrae under normal physiological loads, inducing irritation to nerves, possible structural deformation, and/or incapacitating pain.
Patients�, who have suffered a motor vehicle collision or perhaps a work-related injury, very often have chronic pain syndromes due to ligament laxity. The ligaments surrounding the facet joints of the spinal column, known as capsular ligaments, are highly innervated mechanoreceptive and nociceptive free nerve endings. Therefore, the facet joint is thought of as the primary source of chronic spinal pain (Boswell MV et al., 2007; Barnsley L et al., 1995). When the mechanoreceptors and nociceptors are injured or even simply irritated the overall joint function of the facet joints are altered (McLain RF, 1993).
One must realize that instability is not similar to hyper-mobility. Instability, in the clinical context, implies a pathological condition with associated symptomatology, whereas joint hypermobility alone, does not. Ligament laxity which produces instability refers to a loss of �motion stiffness�, so to speak, in a particular spinal segment when a force is applied to this segment, which produces a greater displacement than would be observed in a normal motion segment. When instability is present, pain and muscular spasm can be experienced within the patient�s range of motion and not just at the joint�s end-point. In Chiropractic, we understand that there is a �guarding mechanism�, which is triggered after an injury, which is the muscle spasm. These muscle spasms can cause intense pain and are the body�s response to instability, since the spinal supporting structures, the ligamentous structures, act as sensory organs, which initiate a ligament-muscular reflex. This reflex is a �protective reflex� or �guarding mechanism�, produced by the mechanoreceptors of the joint capsule and these nerve impulses are ultimately transmitted to the muscles. Activation of surrounding musculature, or guarding, will help to maintain or preserve joint stability, either directly by muscles crossing the joint or indirectly by muscles that do not cross the joint, but limit joint motion (Hauser RA et al., 2013). This reflex is fundamental to the understanding of traumatic injuries.
This reflex is designed to prevent further injury. However, the continued feedback and reinforcement of pain and muscle spasm, will delay the healing process. The �perpetual loop� may continue for a long period of time, making further injury more likely due to muscle contraction. Disrupting this cycle of pain and inflammation is key to resolution.
When traumatic ligament laxity produces joint instability, with neurologic compromise, it is understood that the joint has sustained considerable damage to its stabilizing structures, which could include the vertebrae themselves. However, research indicates that joints that are hypermobile demonstrate increased segmental mobility, but are still able to maintain their stability and function normally under physiological loads (Bergmann TF et al., 1993).
Clinical Diagnosis
Clinicians classify instability into 3 categories, mild, moderate, and severe. Severe instability is associated with a catastrophic injury, such as a motor vehicle collision. Mild or moderate clinical instability is usually without neurologic injury and is most commonly due to cumulative micro-trauma, such as those associated with repetitive use injuries; prolonged sitting, standing, flexed postures, etc..
In a motor vehicle collision, up to 10 times more force is absorbed in the capsular ligaments versus the intervertebral disc (Ivancic PC et al., 2007). This is true, because unlike the disc, the facet joint has a much smaller area in which to disperse this force. Ultimately, as previously discussed, the capsular ligaments become elongated, resulting in abnormal motion in the affected spinal segments (Ivancic PC et al., 2007; Tominaga Y et al., 2006). This sequence has been clearly documented with both in vitro and in vivo studies of segmental motion characteristics after torsional loads and resultant disc degeneration (Stokes IA et al., 1987; Veres SP et al., 2010). Injury to the facet joints and capsular ligaments has been further confirmed during simulated whiplash traumas (Winkelstein BA et al., 2000).
Maximum ligament strains occur during shear forces, such as when a force is applied while the head is rotated (axial rotation). While capsular ligament injury in the upper cervical spine region can occur from compressive forces alone, exertion from a combination of shear, compression and bending forces is more likely and usually involves much lower loads to causes injury (Siegmund GP et al., 2001). If the head is turned during whiplash trauma, the peak strain on the cervical facet joints and capsular ligaments can increase by 34% (Siegmund GP et al., 2008). One research study reported that during an automobile rear-impact simulation, the magnitude of the joint capsule strain was 47% to 196% higher in instances when the head was rotated 60 degrees during impact compared with those when the head was forward facing (Storvik SG et al., 2011). Head rotation to 60 degrees is similar to an individual turning his/her head to one side while checking for on-coming traffic and suddenly experiences a rear-end collision. The impact was greatest in the ipsilateral facet joints, such that head rotation to the left caused higher ligament strain at the left facet joint capsule.
Other research has illustrated that motor vehicle collision trauma has been shown to reduce ligament strength (i.e., failure force and average energy absorption capacity) compared with controls or computational models (Ivancic PC et al., 2007; Tominaga Y et al., 2006). We know that this is particularly true in the case of capsular ligaments, since this type of trauma causes capsular ligament laxity. Interestingly, one research study conclusively demonstrated that whiplash injury to the capsular ligaments resulted in an 85% to 275% increase in ligament elongation (laxity), compared to that of controls (Ivancic PC et al., 2007).
The study also reported evidence that tension of the capsular ligaments due to trauma, requisite for producing pain from the facet joint. Whiplash injuries cause compression injuries to the posterior facet cartilage. This injury also results in trauma to the synovial folds, bleeding, inflammation, and of course pain. Simply stated, this stretching injury to the facet capsular ligaments will result in joint laxity and instability.
Traumatic ligament laxity resulting in instability is a diagnosis based primarily on a patient�s history (symptoms) and physical examination. Subjective findings are the patient�s complaints in their own words, or their perception of pain, sensory changes, motor changes, or range of motion alterations. After the patient presents their subjective complaints to the clinician, these subjective findings, must be correlated and confirmed through a proper and thorough physical examination, including the utilization of imaging diagnostics that explain a particular symptom, pattern, or area of complaint objectively. Without some sort of concrete evidence that explains a patient�s condition, we merely have symptoms with no forensic evidence. Documentation is key, as well as quantifying the patient�s injuries objectively.
In order to adequately quantify the presence of instability due to ligament laxity, the clinician could utilize functional computerized tomography, functional magnetic resonance imaging scans, as well as digital motion x-ray (Radcliff K et al., 2012; Hino H et al., 1999). Studies using functional CT for diagnosing ligamentous injuries have demonstrated the ability of this technique to shoe excess movement during axial rotation of the cervical spine (Dvorak J et al., 1988; Antinnes J et al., 1994).
This is important to realize when patients have the signs and symptoms of instability, but have normal MRI findings in the neutral position. Functional imaging technology, as opposed to static standard films, is necessary for the adequate radiologic depiction of instability because they provide dynamic imaging during movement and are extremely helpful for evaluating the presence and degree of instability.
Although functional imaging maybe superior plain-film radiography is still a powerful diagnostic tool for the evaluation of instability due to ligament laxity. When a patient presents status-post motor vehicle collision, it is common practice to perform a �Davis Series� of the cervical spine. This x-ray series consists of 7 views: anterior-posterior open mouth, anterior-posterior, lateral, oblique views, and flexion-extension views. The lumbar spine is treated in similar fashion. X-ray views will include: anterior-posterior, lateral, oblique views, and flexion-extension views. The flexion-extension views are key in the diagnosis of instability. It is well known, that the dominant motion of the cervical and lumbar spine, where most pathological changes occur, is flexion-extension. Translation of one vertebral segment in relation to the one above and/or below will be most evident on these views. Translation is the total anterior-posterior movement of vertebral segments. After the appropriate views are taken, the images may be evaluated utilizing CRMA or Computed Radiographic Mensuration Analysis. These measurements are taken to determine the presence of ligament laxity. In the cervical spine, a 3.5mm or greater translation of one vertebra on another is an abnormal and ratable finding, indicative of instability (AMA Guides to the Evaluation of Permanent Impairment, 6th Edition).
Alteration of Motion Segment Integrity (AOMSI) is extremely crucial as it relates to ligament laxity. The AMA Guides to the Evaluation of Permanent Impairment 6th Edition, recognize linear stress views of radiographs, as the best form of diagnosing George�s Line (Yochum & Rowe�s Essentials of Radiology, page 149), which states that if there is a break in George�s Line on a radiograph, this could be a radiographic sign of instability due to ligament laxity.
Discussion
Our discussion of ligament laxity and instability continues with the �Criteria for Rating Impairment Due to Cervical and Lumbar Disorders�, as described in the AMA Guides to the Evaluation of Permanent Impairment, 6th Edition. According to the guidelines, a DRE (Diagnosed Related Estimate) Cervical Category IV is considered to be a 25% to 28% impairment of the whole person. Category IV is described as, �alteration of motion segment integrity or bilateral or multilevel radiculopathy; alteration of motion segment integrity is defined from flexion and extension radiographs, as at least 3.5mm of translation of one vertebra on another, or angular motion of more than 11 degrees greater than at each adjacent level; alternatively, the individual may have loss of motion of a motion segment due to a developmental fusion or successful or unsuccessful attempt at surgical arthrodesis; radiculopathy as defined in Cervical Category III need not be present if there is alteration of motion segment integrity; or fractures: (1) more than 50% compression of one vertebral body without residual neural compromise. One can compare a 25% to 28% cervical impairment of the whole person to the 22% to 23% whole person impairment due to an amputation at the level of the thumb at or near the carpometacarpal joint or the distal third of the first metacarpal.
Additionally, according to the guidelines, a DRE (Diagnosed Related Estimate) Lumbar Category IV is considered to be a 20% to 23% impairment of the whole person. Category IV is described as, �loss of motion segment integrity defined from flexion and extension radiographs as at least 4.5mm of translation of one vertebra on another or angular motion greater than 15 degrees at L1-2, L2-3, and L3-4, greater than 20 degrees at L4-5, and greater than 25 degrees at L5-S1; may have complete or near complete loss of motion of a motion segment due to developmental fusion, or successful or unsuccessful attempt at surgical arthrodesis or fractures: (1) greater than 50% compression of one vertebral body without residual neurologic compromise. One can compare a 20% to 23% Lumbar Impairment of the whole person to the 20% whole person impairment due to an amputation of the first metatarsal bone.
Conclusions
After careful interpretation of the AMA Guides to the Evaluation of Permanent Impairment, 6th Edition, regarding whole person impairment due to ligament laxity/instability of the cervical and lumbar spine, one can certainly see the severity and degree of disability that occurs. Once ligament laxity is correctly diagnosed, it will objectively quantify a patient�s spinal injury regardless of symptoms, disc lesions, range of motion, reflexes, etc. When we quantify the presence of ligament laxity, we also provide a crucial element with which to demonstrate instabilities in a specific region. Overall, clarification and quantification of traumatic ligament laxity will help the patient legally, objectively, and most importantly, clinically.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References
AMA Guides to the Evaluation of Permanent Impairment, 6th Edition
Antinnes J, Dvorak J, Hayek J, Panjabi MM, Grob D. The value of functional computed tomography in the evaluation of soft-tissue injury in the upper cervical spine. Eur Spine J. 1994; 98-101. [PubMed]
Barnsley L, Lord SM, Wallis BJ, Bogduk N. The prevalence of cervical zygapophaseal joint pain after whiplash. Spine (Phila Pa 1976). 1995;20: 20-5. [PubMed]
Bergmann TF, Peterson DH. Chiropractic technique principles and procedures, 3rd ed. New York Mobby Inc. 1993
Boswell MV, Colson JD, Sehgal N, Dunbar EE, Epter R. A systematic review of therapeutic facet joint interventions in chronic spinal pain. Pain Physician. 2007;10(1): 229-53. [PubMed]
Chen HB, Yang KH, Wang ZG. Biomechanics of whiplash injury. Chin J Traumatol.2009;12(5): 305-14. [PubMed]
Dvorak J, Penning L, Hayek J, Panjabi MM, Grob D, Zehnder R. Functional diagnostics of the cervical spine using computer tomography. Neuroradiology. 1988;30: 132-7. [PubMed]
Examination of the Spine and Extremities, Stanley Hoppenfeld, 1976
Frank CB. Ligament structure, physiology, and function. J Musculoskelet Neuronal Interact. 2004;4(2): 199-201. [PubMed]
Galasko, C.S., P.M. Murray, M. Pitcher, H. Chanter, S. Mansfield, M. Madden, et. al Neck sprains after road traffic accidents: a modern epidemic. Injury 24(3): 155-157, 1993
American Medical Association. (2009). Guides to the evaluation of permanent impairment,
6th edition. Chicago, Il:AMA
Antinnes, J., Dvorak, J., Hayek, J., Panjabi, M.M., & grob, D. (1994). The value of functional
Computed tomography in the evaluation of soft tissue injury in the upper cervical
spine. European Spine Journal, 98-101.
Barnsley, L., Lord, S.M., Wallis, B.J., & Bogduk, N. (1995). The prevalence of cervical zygaphaseal
facet capsule and its role in whiplash injury: A biomechanical investigation. Spine,
25(10), 1238-1246.
Additional Topics: Preventing Spinal Degeneration
Spinal degeneration can occur naturally over time as a result of age and the constant wear-and-tear of the vertebrae and other complex structures of the spine, generally developing in people over the ages of 40. On occasion, spinal degeneration can also occur due to spinal damage or injury, which may result in further complications if left untreated. Chiropractic care can help strengthen the structures of the spine, helping to prevent spinal degeneration.
A chiropractor is a doctor who specializes in musculoskeletal and nervous system problems. It is the belief of the chiropractic community that problems in these areas can cause adverse health issues, including lowered resistance to disease, illness, and injury.
Chiropractors manipulate the spine to realign spinal joints in their patients. By doing so, patients are expected to experience optimum health without the assistance of drugs or surgery. Instead, chiropractors expect the body will heal itself once the spine and spinal joints are in proper alignment. Additionally, chiropractors consider and address other lifestyle factors which are commonly recognized as significantly affecting health such as diet, rest, exercise, heredity, and environmental factors. They also make other recommendations for changes which are expected to improve the patient�s overall health.
Chiropractors perform many of the same tasks as other general and specialty doctors. Patient health histories are gathered, physical, neurological, and orthopedic examinations are performed, and various laboratory tests, x-rays, and diagnostic imaging tools are used to diagnose and analyze the patient�s condition. Other forms of treatment may be used or recommended by the chiropractor including ultrasound, massage, heat, water, acupuncture, or electric currents. Prescription drugs and surgery are not part of the services provided by chiropractors. Chiropractors may recommend patients to see other doctors or specialists to address health issues or concerns outside of their area of expertise. Some chiropractors choose to specialize in a certain type of practice, such as orthopedics, neurology, sports injuries, internal disorders, diagnostic imaging, or pediatrics.
The Bureau of Labor Statistics predicts a job growth increase of 17% in the chiropractic field over the next seven years. An increasing public interest in alternative healthcare methods is beneficial to the chiropractic field. The public is seeking healthy living options which do not include prescription medicines or surgery; instead, a substantial number of people are searching for solutions which emphasize healthy lifestyles. The non-invasive procedures provided by chiropractors in answer to their patients health issues and concerns appeals to the segment of the public looking for these types of answers.
SELECTING THE RIGHT CHIROPRACTIC COLLEGE
Chiropractor students should select a college which offers a strong science degree or pre-medical program. Some colleges may have an affiliation with chiropractic training schools, which all future chiropractors must successfully complete. Research chiropractic schools to determine which one you are most interested in attending; this will help you to determine if the school is linked to any of the colleges you are considering. Courses in biology, chemistry, and physics will be important to individuals looking to work in a medical field. Electives may be concentrated in health, fitness, and nutrition. Students should, if given the opportunity, study topics and courses related to kinesiology and sports medicine. Courses in psychology and sociology will also help students to gain a more comprehensive understanding of people and society, better preparing them to serve the public. Additionally, business courses ensure that future professionals understand how to successfully manage a business in the complex healthcare field, as medical professionals must understand finances, medical insurance processing, business laws, business practices, business ethics, and medical records maintenance.
CHIROPRACTIC SCHOOLS
Students must attend chiropractic college in order to enter the profession. Upon completion of the program, students will have earned a doctorate in chiropractic medicine. The Council on Chiropractic Education, or CCE, is the nationally recognized accrediting agency by the United States Secretary of Education which regulates the quality of the curriculum offered at chiropractic colleges. Currently there are 15 CCE accredited chiropractic institutions in the United States. These include, as listed on the CCE website:
Students attend chiropractic college for four years. During this time, students are taught the scientific and academic skills and knowledge required to become experts in the field of chiropractic medicine. The final year is spent in practice, performing the functions of a chiropractic doctor under the supervision of an experienced professional. The curriculum includes intensive study of neuromusculoskeletal conditions, nutritional and holistic health, specialized and focused curriculum in areas of acupuncture and oriental medicine, applied nutrition, and various other disciplines. Students will complete extensive course hours in diagnosis, biochemistry, anatomy, chiropractic technique, and philosophy and ancillary therapeutic procedures.
TAKING THE NATIONAL BOARD EXAM
The National Board Exam for chiropractors is administered by the NBCE. The test is given twice each year. The exam consists of three parts. Part one is 110 multiple choice questions relating to general anatomy, spinal anatomy, physiology, chemistry, pathology, microbiology, and public health. The second part also consists of 110 multiple choice questions, but in the areas of general diagnosis, neuromusculoskeletal diagnosis, diagnostic imaging, and principles of chiropractic, chiropractic practice, and associated clinical sciences. Part three of the test consists of another 110 multiple choice questions and 10 case vignettes covering the areas of diagnosis or clinical impression, clinical laboratory and special studies examination, chiropractic techniques, case management, physical examination, case history, and roentgenologic examination. Each part of the test is timed. Additional specialized testing is offered for applicants who choose to pursue an area of specialization.
LICENSING FOR CHIROPRACTORS
After successful completion of an accredited chiropractic program, graduates will need to obtain a license to practice in their resident state or the state in which they intend to practice. State licensure regulations may vary from state to state. It is important to research your state�s regulations prior to completion of the doctor of chiropractic program to ensure all conditions are met. The Federation of Chiropractic Licensing Boards is a nonprofit organization which provides a link to the licensure information in all states. Locate information for each state through this directory.
The information provided includes licensing fees, renewal requirements, national board testing requirements, security and criminal check requirements, additional certification requirements, continuing education, and malpractice insurance requirements. A link to each state licensing board is also provided.
CONTINUING EDUCATION FOR CHIROPRACTORS
The chiropractic field is experiencing an increase in advancements in technology and knowledge through research and academic exploration. Changing regulations are also an area in which chiropractic doctors will need to remain current. Each state maintains their own continuing education requirements upon which licensing will be contingent. Twenty-four credit hours of continuing education every two years is a common requirement. All programs must be board approved and conducted by approved colleges or chiropractic associations or organizations. Check with your state licensing board to determine if the program has been approved prior to enrollment.
PRACTICING AS A CHIROPRACTOR
After obtaining a doctorate and passing the licensing examination, a new chiropractor has many options ahead of them. Most chiropractors will end up working solo or in a group practice, with about one in three being self-employed. A small group will work in hospitals or physicians� offices. The median pay for Chiropractors in 2016 was $67,520, with the lowest 10 percent earning less than $32,380, and the highest earning more than $141,030. Chiropractors can further increase their salary by building up a strong client base and developing their own practice. Many times, chiropractors will work in the evening or on weekends to accommodate their patients.
DAY TO DAY PRACTICE
Chiropractors will spend a lot of time on their feet as they examine and treat patients. Some of the most important qualities that a chiropractor can have include decision-making, detail-oriented, dexterity, empathy, and interpersonal skills. If the chiropractor is operating his or her own practice, the ability to manage a staff of employees like secretaries and nurses is vital to the success of the practice. An understanding of the current healthcare system is also important, as that will determine what kind of payments a chiropractor may be able to receive, unless they work in a cash-only system. More information can be found in the Occupational Outlook Handbook provided by the BLS.
CHIROPRACTIC SPECIALTIES AND CERTIFICATIONS
Another way for chiropractors to increase their annual earnings or skills would be to specialize in one or more areas. Specializations can help a chiropractor better diagnose and treat chronic illnesses, sports injuries, and/or complex occupational injuries. The American Chiropractic Association and American Board of Chiropractic Specialties (ABCS) lists 14 specialties and provides guidance to maintain standards of chiropractic certification. These include, as listed on the American Chiropractic Association website:
Chiropractic Physiotherapy and Rehabilitation (DACRB) Specialist
Has had extensive postgraduate training in physiologic therapeutics and rehabilitation to better treat injuries that may have resulted from an accident or a sports injury.
Treats a wide variety of health conditions that include all body systems and tissues, and focuses special attention on the relationship between the spine, nervous system, and the meridian system.
Is trained to encourage and promote a more advanced knowledge and use of nutrition in the practice of chiropractic for the maintenance of health and the prevention of disease.
Has special knowledge of both the normal function and diseases of the bones, joints, capsules, discs, muscles, ligaments, and tendons, as well as their complete neurological components, referred organ systems and contiguous tissues, and is able to diagnose and treat the conditions related to them.
Diplomate of the American Board of Forensic Professionals (DABFP)
Performs an orderly analysis, investigation, inquiry, test, inspection, and examination in an attempt to obtain the facts of a case, from which to form an expert opinion.
Is trained in chiropractic sports medicine and exercise science in order to treat sports injuries, enhance athletic performance, and promote physical fitness.
Chiropractic Occupational Health (DACBOH) Specialist
A DC trained in health care diagnosis and treatment choices for workplace neuromusculoskeletal injuries who is able to provide a broad range of work-related injury and illness prevention services for employee populations.
Diplomate in Clinical Chiropractic Pediatrics (DICCP)
Support members who take care of children in their chiropractic practices, and to promote the acceptance and advancement of pediatric chiropractic care.
These specialty �degrees� are given by their corresponding boards, which also maintain the level of expected qualifications and standards of excellency.
Title: The chiropractic management of cervical Myelomalacia
Abstract: To examine the diagnosis and condition of a patient suffering from neck pain and radiation of pain into arms following a motor vehicle accident. Diagnostic studies include the chiropractic orthopedic and neurological examination, digital x-rays, range of motion and cervical MRI.
Introduction: On 10/10/2016, a 38-year-old male presented to our office for injuries he had sustained in an MVA on 10/01/2016. The patient stated that he was stopped at an intersection when the pickup behind him hit him at a fast speed, pushing him through the intersection. The patient stated that he had neck pain and stiffness the radiated into the trapezius area. He also complained about �tingling� into both hands. He also complained of lower back pain that he felt more than the neck. His review of systems was benign, other than the current symptoms of neck and back pain and tingling.
The patients Social/Family Medical History included his mother having high blood pressure and Diabetes.
Clinical Findings of Chiropractic and Myelomalacia
The patient is 6�0�. The patient weighs 211 pounds. The sitting blood pressure measured was 122/74.
An evaluation and management exam was performed. The exam consisted of a visual inspection of the spinal ranges of motion, digital palpation, manual testing of muscles, deep tendon reflexes and orthopedic and neurological findings. The Cervical exam showed the following decreased motion on visual exam in flexion, extension, left rotation, right rotation, right lateral flexion and left lateral flexion. All of the above motions produced pain.
When digital palpation was performed in the cervical and thoracic spinal areas, there was moderate spasm noted bilaterally in paraspinal areas with moderate tenderness noted.
In performing the cervical orthopedic and neurological testing, positive findings were present bilaterally with Foraminal Compression and Foraminal Decompression. Soto Hall test was positive when performed in the thoracic spine area. Manual, subjectively rated muscle testing was performed on certain muscles of the upper extremities. Based on the AMA Guides to the Evaluation of Permanent Impairment, 4th Ed., 1993/5th ed. 2001, differences were noted using the rating scale of five to zero. Five is full Range of Motion/Maximum Strength, Four is Full Range of motion with Moderate Resistance, Three is Full Range of Motion/Perceptible Weakness. The Deltoids and Triceps tested normally bilaterally at 5. The Biceps, forearm muscles and the intrinsic hand muscles all tested as a four on the right and a three on the left.
Grip Strength tests the strength of the hands which indicate nerve integrity from the cervical spine. In evaluation, the normal would be for a difference of strength in the preferred hand of 10% more. More than that would be a weakness in the opposite hand, less than that would be a weakness in the preferred hand. The preferred hand for this patient is the right hand. The testing below shows a definite decrease in strength in the left hand.
Hand tested
Rep one
Rep two
Rep three
Right
28
30
30
Left
18
18
20
Deep Tendon Reflexes were performed on the patient and were noted at a plus two bilaterally.
Using a Whartenburg pinwheel, dermatomes showed normal findings except for C8, which was hyposensitive on the left.
A Lumbar orthopedic and neurological exam was then performed. Upon visual examination, there was decreased motion in flexion, extension. right and left lateral flexion with pain present on all of the motions.
Lasegue�s Straight Leg Raising test was performed and was negative with 80 degree movement. Braggards test was performed and was negative bilaterally.
Kemps was done with the patient on both sides and was noted as negative. Ely test was noted as negative.
Digital palpation was performed and there was severe tenderness and spasm bilaterally in the lumbar paraspinal muscles.
Manual, subjectively rated muscle testing was performed on certain muscles of the lower extremities. Based on the AMA Guides to the Evaluation of Permanent Impairment, 4th Ed., 1993/5th ed. 2001, differences were noted using the rating scale of five to zero. Five is full Range of Motion/Maximum Strength, Four is Full Range of motion with Moderate Resistance, Three is Full Range of Motion/Perceptible Weakness. Muscle testing was done bilaterally in the Quadriceps, Hamstrings, Calf Muscles and Extensor Hallicus Longus and showed Full ROM and Strength.
Deep Tendon Reflexes were performed. They negative in the Achilles bilaterally, but +3 in the Patella bilaterally.
Based on the ortho/neuro findings and the history, the following x-rays were ordered:
AP/Lat/Flex/Ext/Bilateral Oblique�s/ APOM of the cervical spine, AP/Lat Thoracic
AP/Lat/Lateral Flexion/Oblique Lumbar�s. The x-rays were read and the Lumbar spine showed the discs were of a normal height and Georges line was un-interrupted. There the Lumbar curve appeared to be hypolordotic. On visual inspection, there was a decrease in the lateral bending bilaterally.
The Cervical spine showed that there was anterior spurring present in the C5/6 region of the cervical spine. In the lateral view, the normal curvature of the spine was no longer lordotic, but noted as a �Military Neck.� There was decreased range of motion noted in the flexion as well as the extension views. Also, noted on flexion and extension was paradoxical motion present at C1. Disc spaces were normal throughout the spine, except for narrowing of the disc space at C5/6, as well as spurring noted in the anterior part of the vertebral body.
Due to the injuries, orthopedic and neurological and x-ray findings, a cervical MRI was ordered. I recommended that the patient receive palliative therapy until a Cervical MRI could be obtained.
The MRI was obtained and personally reviewed. The Cervical MRI performed on 10/14/2016 revealed that C1/2 was unremarkable. There was a mild disc bulge at C2/3 and a moderate disc bulge which abuts the ventral cord and results in mild spinal canal stenosis at C3/4. There is also bilateral uncovertebral hypertrophy with moderate bilateral neural foraminal narrowing noted at C3/4. At C4/5, There is a mild disc bulge which abuts the ventral cord. There is a mild spinal canal stenosis. There is a bilateral uncovertebral hypertrophy with moderate bilateral neural foraminal narrowing. At C5/6, There is a moderate disc bulge which indents the ventral cord and results in severe spinal canal stenosis. There is a resultant T2 weighted hyperintense (high) signal abnormality in the spinal cord at this level. This may represent edema or myelomalacia. C6/7 shows that there is a mild disc bulge which abuts the ventral cord and results in mild spinal canal stenosis. There is bilateral uncovertebral hypertrophy with moderate bilateral neural foraminal narrowing. C7/T1 presents as unremarkable.
Test Study Treatment Impressions
At C5/6, there is a moderate disc bulge which indents the ventral cord and results in severe spine canal stenosis. There is resultant abnormal signal in the spinal cord at C5/6, which may represent myelomalacia or edema.
An alert was placed on this study.
Fig.1 (A) Sagittal T2 MRI of Cervical Spine
(B) Axial T2 MRI of the Cervical Spine.
A
B
The patient was notified of the MRI findings. The patient was informed that care would be discontinued until a consultation was done with a neurosurgeon. The patient stated that he was going to do that. He continued to try to get care, but we refused. The patient was instructed to go to the emergency room. The patient became angry stating that he wanted his records, that he was going to go to another chiropractor for them to �crack his neck�. The patient went to another chiropractor and based on our records, also refused to see the patient. The patient finally decided to go to the surgeon where disc surgery was performed to decompress the spinal cord.
The patient contacted our office and thanked us for being so adamant about his treatment.
Discussion of Results
There is much discussion in the MRI report concerning �bulges� and one must first have a handle on what is a bulge and herniation.
General radiologists often utilize various nomenclature such as bulge, protrusion, prolapse, herniation and a myriad of other descriptors. However, the nomenclature has been standardized and accepted by the North American Spine Society, the American Spine Society of Radiology and the American Society of Radiology by Fardone, Williams, Dohring, Murtagh, Rothman and Sze (2014):
�Degeneration may include any or all of the following: desiccation, fibrosis, narrowing of the disc space, diffuse bulging of the annulusbeyond the disc space, fissuring (i.e.., annular fissures), mucinous degeneration of the annulus, intradiscal gas, osteophytes of the vertebral apophyses, defects, inflammatory changes, and sclerosis of the endplates.� pg. 2528(1)
1. A disc in which the contour of the outer annulus extends, or appears to extend, in the horizontal (axial) plane beyond the edges of the disc space, usually greater than 25% (90�) of the circumference of the disc and usually less than 3 mm beyond the edges of the vertebral body apophysis.
2. (Nonstandard) A disc in which the outer margin extends over a broad base beyond the edges of the disc space.
3. (Nonstandard) Mild, diffuse, smooth displacement of disc.
4. (Nonstandard) Any disc displacement at the discal level.
Note: Bulging is an observation of the contour of the outer disc and is not a specific diagnosis. Bulging has been variously ascribed to redundancy of the annulus, secondary to the loss of disc space height, ligamentous laxity, response to loading or angular motion, remodeling in response to adjacent pathology, unrecognized and atypical herniation, and illusion from volume averaging on CT axial images. Mild, symmetric, posterior disc bulging may be a normal finding at L5�S1. Bulging may or may not represent pathological change, physiological variant, or normalcy. Bulging is not a form of herniation; discs known to be herniated should be diagnosed as herniation or, when appropriate, as specific types of herniation.� Pg. 2537(1)
Studin and Owens discuss this �nomenclature� in their article �Bulging Discs and Trauma: Causality and a Risk Factor�.
�There is now, based upon the literature and well respected experts, categories of disc bulges that can be deemed as direct sequella from trauma vs. those cases where there is pre-existing degeneration. It can also now be concluded, again based upon the literature that those patients can have an aggravation of the pre-existing condition that could persist a lifetime requiring perpetual care. To conclude these findings, a doctor trained in understanding the underlying pathology and sequella must be consulted to be able to render an accurate diagnosis that is demonstrable.�2 Pg. 26
Understanding Cervical Myelomalacia
What is Myelomalacia? According to the MedicoLexicon, it is simply the �softening of the spinal cord�.3 Basically, it is ischemia that takes place in the spinal cord from abnormal pressure placed upon it. If left untreated, then that continues to spread and cause further damage to the cord. Once the cord has been damaged, there is no repair. Brandy Carrelli gives us a concise definition and the ramifications of it left untreated:
�The myelomalacia definition, strictly speaking is the �softening of the spinal cord�. After an acute injury, bleeding of the spinal cord may occur. As a result, there is �subsequent softening of normal tissues�. Myelomalacia can be caused by trauma or disease, but if it worsens, and if the bleeding reaches the cervical region of the body, it can be fatal. Bleeding can make the tissue necrotic. Fractured vertebrae can lead to bleeding in the spinal cord, as can some back surgery. Osteoporosis may also contribute to spinal instability and hemorrhaging. Sometimes circulatory problems can lead to a deterioration of tissues and bleeding. Myelomalacia can progress into impairment in the functioning of the lower extremities, below-normal or absent reflexes of the anus and pelvic limbs, loss of pain perception in the caudal region (near the coccyx), depression, respiratory problems due to �diaphragmatic paralysis�, and even neurological issues. Death could result from the respiratory paralysis. Damage occurs to the central nervous system. At first, the spinal cord damage may be minor. The most commonly injured areas are the lumbar spine (lower back) and cervical vertebrae (upper spine area).4
Disc degeneration, herniations (all variations) and bulging all describe what has happened to the disc itself. Once you have established a definitive diagnosis, then the question becomes, how is the disc affecting surrounding neurological components? Myelomalacia is the effect of that disc when the cord is affected by pressure. If there is bleeding into the cord, then the cord begins a degenerative spiral that can happen rather quickly. As you have read above, it can take what may simply appear as a minor issue to the patient that can lead to major neurological compromise and in extreme cases may lead to paralysis or death. Therefore, it is important carefully analyze the clinical indicators and image accordingly.
Myelomalacia is a relatively rare occurrence. According to Zhou, Kim, Vo and Riew,
�The overall prevalence of cervical myelomalacia was relatively low in the studied population, and it was affected by age, sex, and the specialties/subspecialties of referring providers. These results may help direct treatment guidelines and allow for informed discussions with patients in terms of the risk versus the benefit of surgery.�5 Pg. E252
It is a very common occurrence for the presence of disc bulging and herniations in chiropractic practices. It is of utmost importance for the chiropractor to not only order MRI when clinically indicated, it is important to be able to interpret those images as well. Once the clinical indicators begin to show a different story than presented by the patient symptomatically, it is the responsibility of the chiropractor to make the appropriate diagnosis, prognosis and treatment plan. In this case, that is an immediate neurosurgical referral. Although not a common finding in a chiropractic office, one must still be alert to the possibility of Myelomalacia. Managing the patient based upon an accurate diagnosis is your ultimate goal, and sometimes adjusting the patient isn�t the best first option as diagnosis and prognosis supersede treatment.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
REFERENCES:
Fardon, D. F., Williams, A. L., Dohring, E. J., Murtagh, F. R., Gabriel Rothman, S. L., & Sze, G. K.
Studin M., Owens W. (2016) Bulging Discs and Trauma: Causality and a Risk Factor, American Chiropractor 34(6) 18, 20,22-24, 26, 28
http://www.medilexicon.com/dictionary/58294
Carrelli, B (2016) What is Myelomalacia? https://www.echiropractor.org/myelomalacia/
Zhou, Yihua; Kim, Sang D.; Vo, Katie; Riew, K. Daniel (2015) Prevalence of cervical myelomalacia in adult patients requiring a cervical magnetic resonance imagingSpine (Phila Pa 1976). 2015 Feb 15;40(4):E248-252.
Additional Topics: Recovering from Auto Injuries
After being involved in an automobile accident, many victims frequently report neck or back pain due to damage, injury or aggravated conditions resulting from the incident. There’s a variety of treatments available to treat some of the most common auto injuries, including alternative treatment options. Conservative care, for instance, is a treatment approach which doesn’t involve surgical interventions. Chiropractic care is a safe and effective treatment options which focuses on naturally restoring the original dignity of the spine after an individual suffered an automobile accident injury.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine