Back problems and discomfort symptoms are a common ailment that many types of healthcare providers diagnose and treat it. Can knowing a little about what each back pain specialist does and what they have to offer help in choosing a provider?
Back Pain Specialists
Nowadays individuals have options for treating back pain. Primary healthcare providers, general practitioners, pediatricians, and emergency room workers are usually the first to examine the injury or problem. If they are unable to properly diagnose or treat the injury, they will refer the individual to a specialist. Specialists include:
Osteopaths
Chiropractors
Orthopedists
Rheumatologists
Neurologists
Neurosurgeons.
They specialize in chronic conditions and diseases like arthritis or problems like herniated discs. Complementary and alternative providers treat individuals solely or with help from a care team. They look at the whole body and focus on improving overall function.
Family and General Practitioners
When neck or back pain begins a regular doctor that’s usually a family or general practitioner/GP or primary care provider PCP is a recommended place to start. They will:
Order diagnostic tests.
Recommend exercises and stretches.
Prescribe medication.
Refer the patient to a physical therapist or other back pain specialist.
However, studies suggest general providers can be uninformed and slow to adopt new back treatments. (Paul B. Bishop, Peter C. Wing. 2006) It is recommended to research possible treatment options, ask a lot of questions during an appointment, and ask or request a referral to a specialist.
Pediatricians
Pediatricians diagnose and treat children. They cover a wide range of issues including back problems and injuries. As with a general practitioner or primary care provider, a child’s pediatrician is the place to start. Depending on the child’s needs, they’ll refer them to the proper specialist.
Emergency Healthcare Providers
When there is serious neck or back trauma, individuals need to go to the emergency room. Trauma can include automobile collisions, sports accidents, work accidents, and/or personal home accidents. Someone with a possible spinal injury should not be moved. (W Yisheng, et al., 2007) Go to the ER if there is back pain with loss of bowel or bladder control, or the legs become progressively weaker. These are symptoms of an emergency condition known as cauda equina syndrome. (American Association of Neurological Surgeons. 2023)
Orthopedists
Orthopedists and orthopedic surgeons treat the musculoskeletal system, which includes:
Muscles
Bones
Joints
Connective tissues
Cartilage
Common orthopedic issues include:
Repetitive stress injuries
Sports injuries
Bursitis
Tendonitis
Ruptured discs
Nerve impingement
Scoliosis
Osteoporosis
Osteoarthritis
Orthopedics can overlap with other specialties. As orthopedists and rheumatologists both treat arthritis and orthopedic surgeons and neurosurgeons do some of the same procedures that include spinal fusions and discectomies.
Rheumatologists
A rheumatologist treats autoimmune, inflammatory, and musculoskeletal conditions that can include different types of arthritis, lupus, and Sjogren’s syndrome. A primary care provider may refer a patient to a rheumatologist if they have symptoms that include:
Sacroiliitis – inflammation of the sacroiliac joint at the base of the spine.
Axial spondylosis – a form of spinal arthritis.
Axial spondylosis – spinal arthritis that causes the bones to fuse together.
Rheumatologists can also treat spinal stenosis or advanced osteoarthritis as they overlap with orthopedists.
Neurologists
A neurologist specializes in the function of the nervous system. They treat disorders of the brain, spinal cord, and nerves that include:
Parkinson’s disease
Multiple sclerosis
Alzheimer’s disease
Chronic back or neck pain
They are experts in the origins of pain. (David Borsook. 2012) However, a neurologist does not perform spine surgery.
Neurosurgeons
A neurosurgeon specializes in nervous system surgical procedures that include the brain, spine, and spinal cord. However, neurosurgeons do not provide overall treatment for back pain because they are usually the last to be seen after exhausting all other treatment options.
Osteopaths
An osteopath is a licensed physician who practices medicine using conventional treatments and osteopathic manipulative medicine. They have the same education as an MD plus 500 hours of musculoskeletal system studies. (National Library of Medicine. 2022) They take the same exams and are licensed as an MD. Many osteopaths are primary care providers. For back pain, they will focus on:
Posture rehabilitation and training.
Stretching
Therapeutic massage
Spinal manipulation
The goal is to relieve pain and muscle tension, increase mobility, and improve musculoskeletal function.
Physiatrists
Physiatrists are holistic providers that focus on physical function. They can be thought of as a primary care provider plus a physical therapist. These back pain specialists provide rehabilitation for various types of conditions and injuries including:
Back pain
Sports injuries
Stroke
Often they will coordinate a team of specialists to develop a targeted treatment plan.
Chiropractor
Chiropractic is a hands-on alternative medicine. The goal is to restore neuromusculoskeletal function by realigning the spine to its proper form. They do this with spinal manipulations, non-surgical mechanical decompression, traction, and massage techniques. (Michael Schneider, et al., 2016)
The purpose of most chiropractic adjustments is to relax and retrain tight muscles and increase flexibility.
Chiropractic helps to relieve stiff muscles and restore range of motion.
Individuals may not be referred to a chiropractor if they:
Have loose-joints
Have connective tissue problems or conditions.
Have osteoporosis/thinning bones
All types of back pain specialists provide various forms of therapy that may be able to help.
Spinal Decompression in Depth
References
Bishop, P. B., & Wing, P. C. (2006). Knowledge transfer in family physicians managing patients with acute low back pain: a prospective randomized control trial. The spine journal : official journal of the North American Spine Society, 6(3), 282–288. https://doi.org/10.1016/j.spinee.2005.10.008
Yisheng, W., Fuying, Z., Limin, W., Junwei, L., Guofu, P., & Weidong, W. (2007). First aid and treatment for cervical spinal cord injury with fracture and dislocation. Indian journal of orthopaedics, 41(4), 300–304. https://doi.org/10.4103/0019-5413.36991
Schneider, M., Murphy, D., & Hartvigsen, J. (2016). Spine Care as a Framework for the Chiropractic Identity. Journal of chiropractic humanities, 23(1), 14–21. https://doi.org/10.1016/j.echu.2016.09.004
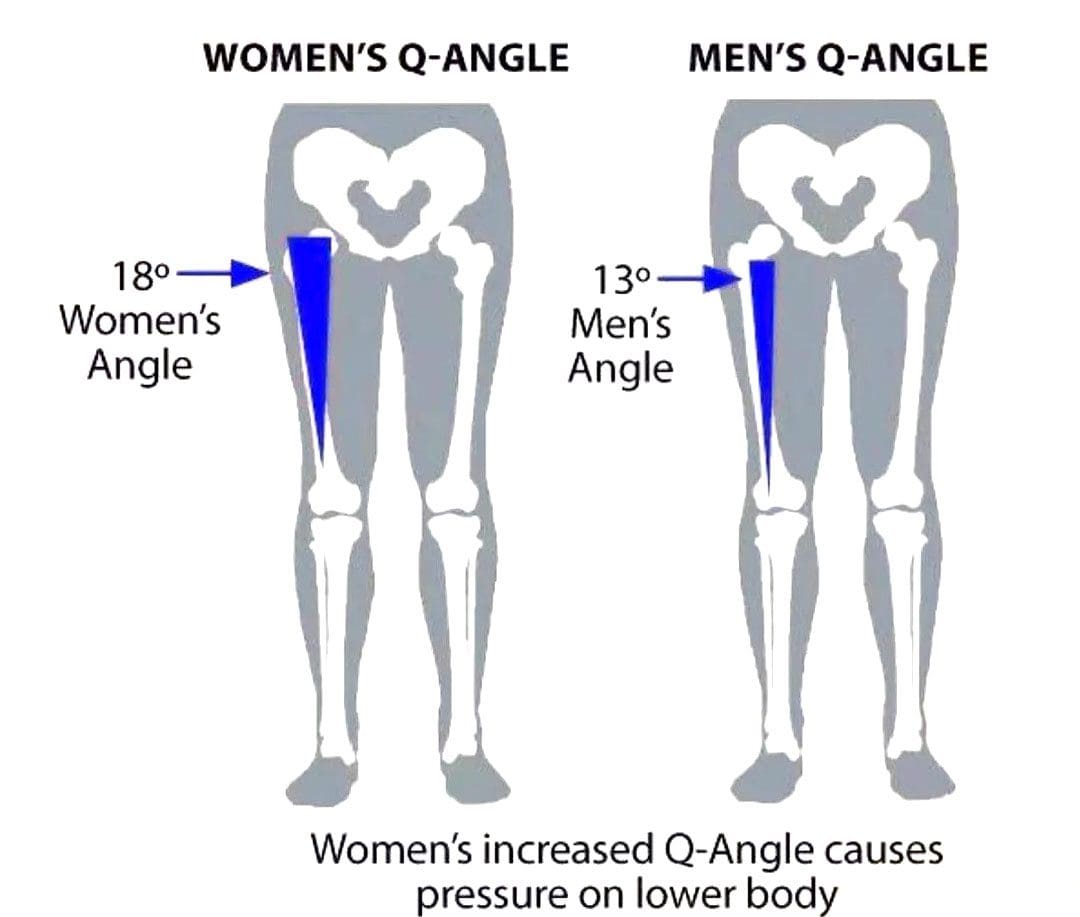
The Q or quadriceps angle is a measurement of pelvic width that is believed to contribute to the risk of sports injuries in women athletes. Can non-surgical therapies and exercises help rehabilitate injuries?
Quadriceps Q – Angle Injuries
The Q angle is the angle where the femur/upper leg bone meets the tibia/lower leg bone. It is measured by two intersecting lines:
One from the center of the patella/kneecap to the anterior superior iliac spine of the pelvis.
The other is from the patella to the tibial tubercle.
On average the angle is three degrees higher in women than men.
Women have biomechanical differences that include a wider pelvis, making it easier to give birth. However, this difference can contribute to knee injuries when playing sports, as an increased Q angle generates more stress on the knee joint, as well as leading to increased foot pronation.
Injuries
Various factors can increase the risk of injury, but a wider Q angle has been linked to the following conditions.
Patellofemoral Pain Syndrome
An increased Q angle can cause the quadriceps to pull on the kneecap, shifting it out of place and causing dysfunctional patellar tracking.
With time, this can cause knee pain (under and around the kneecap), and muscle imbalance.
Foot orthotics and arch supports could be recommended.
Some researchers have found a link, while others have not found the same association. (Wolf Petersen, et al., 2014)
Chondromalacia of the Knee
This is the wearing down of the cartilage on the underside of the kneecap.
An increased Q angle can be a factor that increases stress and causes the knee to lose its stability.
However, this remains controversial, as some studies have found no association between the Q angle and knee injuries.
Chiropractic Treatment
Strengthening Exercises
ACL injury prevention programs designed for women have resulted in reduced injuries. (Trent Nessler, et al., 2017)
The vastus medialis obliquus or VMO is a teardrop-shaped muscle that helps move the knee joint and stabilize the kneecap.
Strengthening the muscle can increase the stability of the knee joint.
Strengthening may require a specific focus on muscle contraction timing.
Closed-chain exercises like wall squats are recommended.
Glute strengthening will improve stability.
Stretching Exercises
Stretching tight muscles will help relax the injured area, increase circulation, and restore range of motion and function.
Muscles commonly found to be tight include the quadriceps, hamstrings, iliotibial band, and gastrocnemius.
Foot Orthotics
Custom-made, flexible orthotics decrease the Q angle and reduce pronation, relieving the added stress on the knee.
A custom orthotic ensures that the foot and leg dynamics are accounted for and corrected.
Motion-control shoes can also help correct overpronation.
Knee Rehabilitation
References
Khasawneh, R. R., Allouh, M. Z., & Abu-El-Rub, E. (2019). Measurement of the quadriceps (Q) angle with respect to various body parameters in young Arab population. PloS one, 14(6), e0218387. https://doi.org/10.1371/journal.pone.0218387
Petersen, W., Ellermann, A., Gösele-Koppenburg, A., Best, R., Rembitzki, I. V., Brüggemann, G. P., & Liebau, C. (2014). Patellofemoral pain syndrome. Knee surgery, sports traumatology, arthroscopy: Official journal of the ESSKA, 22(10), 2264–2274. https://doi.org/10.1007/s00167-013-2759-6
Vaienti, E., Scita, G., Ceccarelli, F., & Pogliacomi, F. (2017). Understanding the human knee and its relationship to total knee replacement. Acta bio-medica : Atenei Parmensis, 88(2S), 6–16. https://doi.org/10.23750/abm.v88i2-S.6507
Mitani Y. (2017). Gender-related differences in lower limb alignment, range of joint motion, and the incidence of sports injuries in Japanese university athletes. Journal of Physical Therapy Science, 29(1), 12–15. https://doi.org/10.1589/jpts.29.12
Nessler, T., Denney, L., & Sampley, J. (2017). ACL Injury Prevention: What Does Research Tell Us? Current reviews in musculoskeletal medicine, 10(3), 281–288. https://doi.org/10.1007/s12178-017-9416-5
In individuals with herniated discs, how does non-surgical decompression compare to traditional surgery repair the spine?
Introduction
When many individuals begin to add unnecessary pressure on their backs, it can lead to damaging results to their spine. The spine is the backbone of the body, allowing the upper and lower sections to be mobile and stabilizing the axial weight overload without the person feeling pain or discomfort. The spinal structure is surrounded by muscles, soft tissues, ligaments, nerve roots, and joints that support the spine. In between the spinal facet joints and structure are flat discs that absorb the shock and pressure from the axial overload. However, when unwanted stress starts to compress the disc, it can lead to the development of herniation. Depending on the location, it can cause pain-like symptoms like lower back and neck pain or sciatica. Other times, herniated discs can be due to natural degeneration, where the spinal disc height decreases, and it can crack under pressure, leading to disc dehydration, which, to this point, causes spinal issues to many individuals, thinking they are experiencing referred pain in different body locations. Coincidentally, many people can find the relief they seek through non-surgical treatments to restore the disc height and repair herniated discs. Today’s article focuses on the casing effects of herniated discs and how spinal decompression, a form of non-surgical treatment, can help reduce pain-like symptoms associated with herniated discs. Additionally, we communicate with certified medical providers who incorporate our patients’ information to reduce herniated disc pain, causing many musculoskeletal issues. We also inform them that non-surgical treatments can help mitigate the referred pain-like symptoms related to herniated discs and restore disc height in their spines. We encourage our patients to ask amazing educational questions for our associated medical providers about their referred pain correlating with herniated discs. Dr. Jimenez, D.C., incorporates this information as an educational service. Disclaimer
The Changing Effects Of Herniated Discs
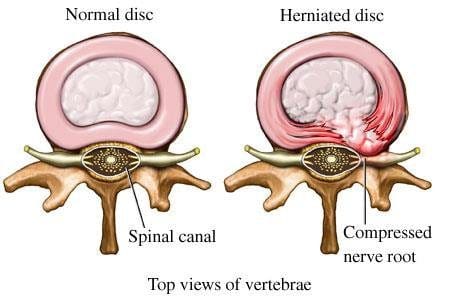
Have you experienced unwanted pain in your upper and lower extremities after a long work day? What about experiencing pain within your spines that are causing symptoms of numbness or tingling sensations in your hands, feet, or legs? Or are you dealing with excruciating lower back pain that is affecting your ability to work? Many individuals don’t realize that the pain-like symptoms they are experiencing are not low back, neck, or shoulder pain, but they correlate to herniated discs in their spines. Herniated discs are when the nucleus pulposus (inner disc portion) starts to protrude out of its original position from the intervertebral space. (Dydyk, Ngnitewe Massa, & Mesfin, 2023) Herniated discs are one of the common causes of lower back pain, and often, many individuals will remember what caused the herniation in their spine.
Some of the effects that lead to disc herniation are that many people will carry heavy objects constantly from one location to another, and the shifting weight can cause the disc to be continuously compressed and thus lead to herniation. Additionally, when the intervertebral disc starts showing signs of stiffness, it can result in abnormal spinal motion. (Haughton, Lim, & An, 1999) This causes morphologic changes within the intervertebral disc and causes it to be dehydrated. The chondroitin sulfation of the proteoglycan in the disc goes through changes in the disc itself, and when degeneration is associated with herniated discs, it can lead to musculoskeletal disorders. (Hutton et al., 1997)
The Root Cause Of Pain- Video
When degenerative changes start to affect the intervertebral discs, it can lead to intervertebral height loss, abnormal pain signaling, and nerve root entrapment associated with disc disruption. (Milette et al., 1999) This causes a cascading effect as the outer annulus of the spinal disc is cracked or ruptured, causing pain to the spine. When the outer annulus of the spinal disc starts to have nerve ingrowth in the affected discs, which then leads to individuals dealing with musculoskeletal disorders associated with pain. (Freemont et al., 1997) Many people will seek non-surgical therapies when finding treatment to alleviate the pain caused by herniated discs due to their cost-effectiveness and how it’s safe for their spine. Chiropractic care, massage therapy, spinal decompression, and traction therapy are available treatments that can be used in a personalized, inclusive treatment care plan to mitigate any pain the person is dealing with. The video explains how these treatments can use functional wellness principles to identify where the pain is located and treat any health issues with any potential underlying causes.
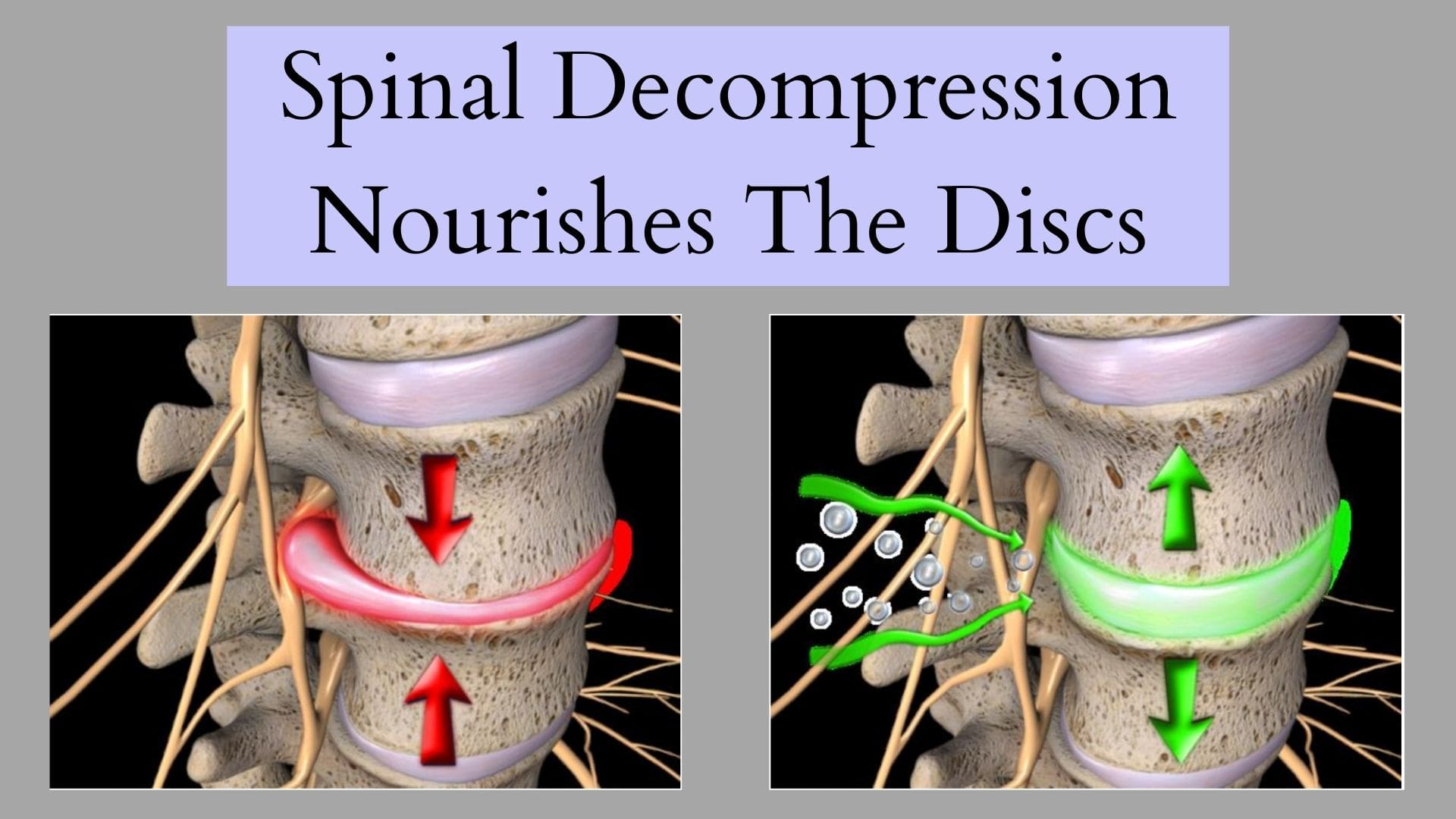
Spinal Decompression Reducing Herniated Disc
Regarding non-surgical treatments reducing herniated discs, spinal decompression can help mitigate the pain affecting the spine’s mobility. Spinal decompression utilizes mechanical traction to gently stretch the spine and allow the herniated disc to return to its original position. Spinal decompression incorporates negative pressure, which helps the nutrients increase the disc’s regenerative factors. (Choi et al., 2022) This allows the facet joints and aggravated nerves to have reduced pressure and increased disc space height. At the same time, spinal decompression can be combined with physical therapy to reduce the pain-like symptoms associated with herniated discs and provide beneficial results. (Amjad et al., 2022) Some of the beneficial factors related to spinal decompression include:
Pain improvement in the upper and lower extremities
Spinal range of motion
Muscle endurance restored
Joint ROM restored
When many individuals become more mindful of how different factors are causing spinal issues, they can make small routine changes in their daily lives, and that can reduce the chances of pain from returning. This allows them to enjoy life fully and continue their health and wellness journey.
References
Amjad, F., Mohseni-Bandpei, M. A., Gilani, S. A., Ahmad, A., & Hanif, A. (2022). Effects of non-surgical decompression therapy in addition to routine physical therapy on pain, range of motion, endurance, functional disability and quality of life versus routine physical therapy alone in patients with lumbar radiculopathy; a randomized controlled trial. BMC Musculoskelet Disord, 23(1), 255. https://doi.org/10.1186/s12891-022-05196-x
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P.-B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. https://doi.org/10.1155/2022/6343837
Freemont, A. J., Peacock, T. E., Goupille, P., Hoyland, J. A., O’Brien, J., & Jayson, M. I. (1997). Nerve ingrowth into diseased intervertebral disc in chronic back pain. Lancet, 350(9072), 178-181. https://doi.org/10.1016/s0140-6736(97)02135-1
Haughton, V. M., Lim, T. H., & An, H. (1999). Intervertebral disk appearance correlated with stiffness of lumbar spinal motion segments. AJNR Am J Neuroradiol, 20(6), 1161-1165. https://www.ncbi.nlm.nih.gov/pubmed/10445464
Hutton, W. C., Elmer, W. A., Boden, S. D., Horton, W. C., & Carr, K. (1997). Analysis of chondroitin sulfate in lumbar intervertebral discs at two different stages of degeneration as assessed by discogram. Journal of Spinal Disorders, 10(1), 47-54. https://www.ncbi.nlm.nih.gov/pubmed/9041496
Milette, P. C., Fontaine, S., Lepanto, L., Cardinal, E., & Breton, G. (1999). Differentiating lumbar disc protrusions, disc bulges, and discs with normal contour but abnormal signal intensity. Magnetic resonance imaging with discographic correlations. Spine (Phila Pa 1976), 24(1), 44-53. https://doi.org/10.1097/00007632-199901010-00011
Can the effects of vertebral decompression relieve individuals with herniated discs and reduce intradiscal pressure on the spine?
Introduction
The spine’s main job is to maintain the vertical pressure of the body without feeling pain or discomfort, especially when a person is in motion. The spinal discs are between the spinal joints, which are shock absorbers when pressure is implemented when a person is carrying a heavy object. The spinal column also has the spinal cord and nerve roots that are spread out from each section and have nerve root signals to be transmitted back and forth from the muscles to the brain to carry out its function. However, as the body ages, so does the spine, as many individuals are constantly adding unwanted pressure on their spines by doing normal factors and developing musculoskeletal disorders. At the same time, the spinal discs are also being affected as the unwanted pressure compresses them constantly, causing them to crack and herniate out of their position. To that point, the herniated disc aggravates the spinal nerve roots, leading to pain-like symptoms affecting the upper and lower body extremities. When this happens, many people will begin to experience musculoskeletal pain and cause overlapping risk profiles that cause their bodies to be misaligned. However, non-surgical treatments can be implemented as part of a daily routine for individuals dealing with herniated discs to reduce intradiscal pressure off the affected muscles in the upper and lower body extremities and restore functionality to the body. Today’s article focuses on why herniated disc affects many people and how vertebral traction can reduce intradiscal pressure off the spine while relieving the musculoskeletal system. Additionally, we work hand-in-hand with certified medical providers who incorporate our patient’s information to reduce intradiscal stress correlating with herniated discs. We also inform them that vertebral traction therapy (spinal decompression) can help mitigate the pain-like symptoms associated with herniated discs and provide relief to the body. We encourage our patients to ask profound questions while seeking education from our associated medical providers about their pain-like issues. Dr. Alex Jimenez, D.C., incorporates this information as an educational service. Disclaimer
Why Does Herniated Disc Affect People?
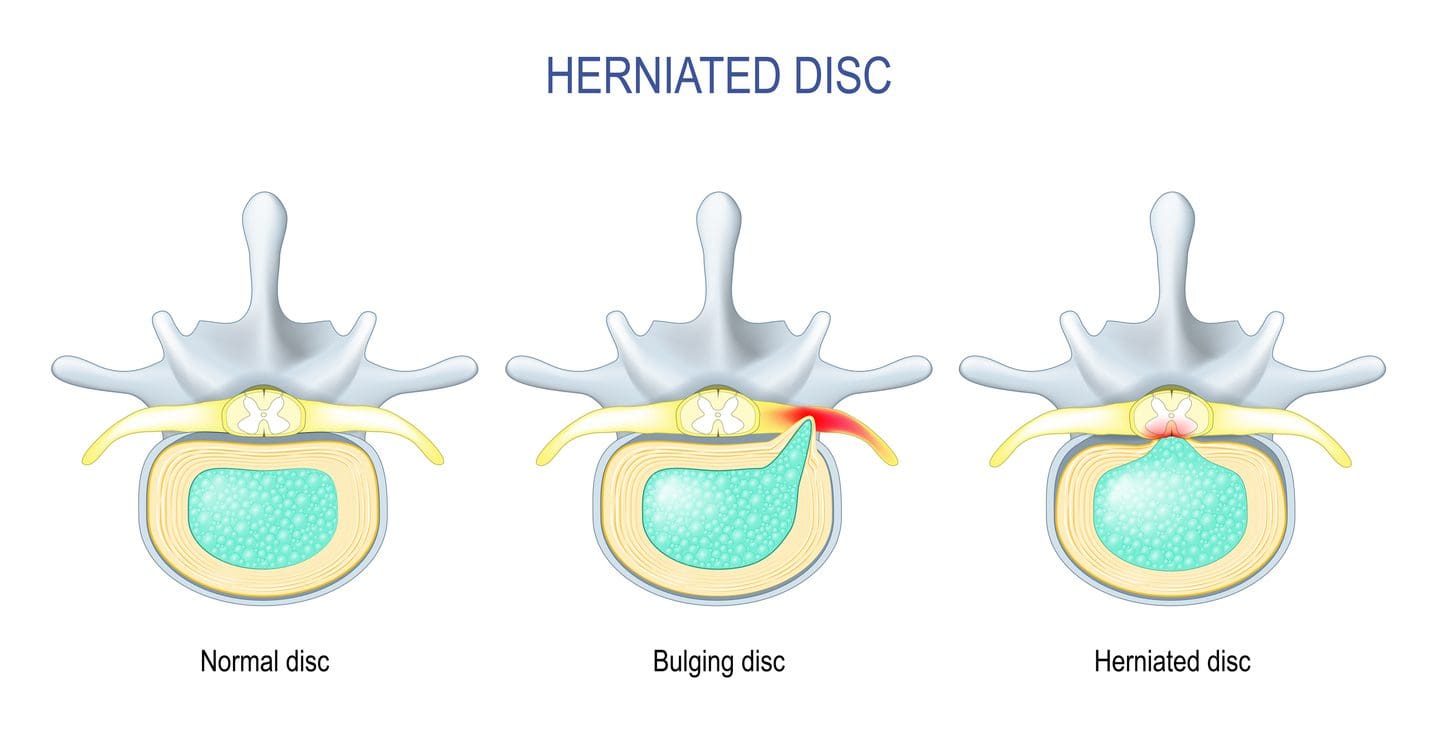
Have you or your loved ones been dealing with muscle aches or strains in their back, neck, or shoulders after carrying/lifting a heavy object? Do you feel a numbing or tingling sensation in your hands, legs, or feet after a long day after work? Or have you been constantly dealing with muscle and joint stiffness after a long workday? At some point in their lives, everyone has dealt with pain affecting their upper and lower extremities, leading to herniated discs in the spine’s upper, middle, or lower portions. As stated earlier, the body and the spine age naturally, leading to the development of herniated discs in the spine. Disc herniation occurs when the nucleus pulposus (inner disc layer) starts to break through the weaker annulus fibrosus (outer disc layer) and compress the surrounding nerve root, leading to an overlapping risk profile to the upper and lower body portions. (Ge et al., 2019) Disc herniation is developed when the spine goes through a natural degeneration, which causes them to be more susceptible to microtears. When individuals start to do normal activities like lifting or carrying heavy objects, it can enhance the progression further, leading to musculoskeletal disorders. Additionally, the spinal degeneration associated with disc herniation can cause inflammatory responses when the protruding disc is compressing the nerve roots, which then causes symptoms of pain and numbness to the upper and lower extremities. (Cunha et al., 2018)
Why do herniated discs cause inflammatory responses to the compressed nerve roots that cause pain-like symptoms to the upper and lower body extremities? Well, when many individuals are experiencing pain associated with herniated discs, they believe they are dealing with upper or lower pain, depending on where the herniated disc is located. This causes referred pain symptoms where the pain is being perceived in one location than the site where the pain is originating. Coincidentally, when individuals are doing repetitive motions associated with herniated discs can cause the adjacent nerve root to be compressed, which then causes the surrounding muscles, ligaments, and soft tissues to be in pain. (Blamoutier, 2019) Pain developing from herniated discs can reduce a person’s quality of life and make them miss out on important life events.
Disc Herniation Overview-Video
Many factors associated with a herniated disc can lead to its development and range from mild to severe depending on where the disc is herniated. Since the spine and spinal disc do degenerate over time naturally, it can cause the disc to crack and dehydrate. This leads to restricted movement, the development of neck, back, and shoulder pain, a decrease in muscle strength in the extremities, and numbness. (Jin et al., 2023) These are some results when herniated discs are not being treated right away. Luckily there are non-surgical treatments to alleviate the pain-like symptoms associated with herniated discs and help reduce intradiscal pressure in the spine while restoring spinal mobility and muscle strength. Spinal decompression, chiropractic care, massage therapy, and physical therapy are some non-surgical treatments that can help alleviate herniated discs and its associated symptoms. Non-surgical treatments can help pull the herniated disc off the compressed nerve root through manual and mechanical manipulation and return it to its original position. Additionally, non-surgical treatments can be part of a daily health and wellness routine combined with other therapies to reduce pain-like symptoms associated with herniated discs and help restore the spine’s mobility. The video above explains the causes, factors, and symptoms associated with herniated discs and how these treatments can alleviate the pain.
The Effects Of Vertebral Traction On Disc Herniation
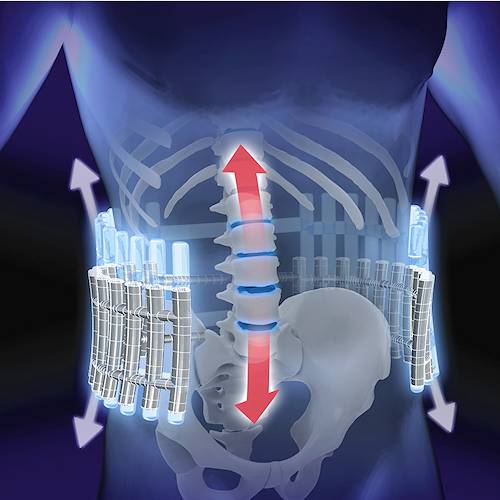
Non-surgical treatments like vertebral decompression can provide a positive outlook when reducing the effects of herniated discs. Vertical or spinal decompression can help reduce the underlying problem associated with herniated discs by relieving the pain and intradiscal pressure off the vital structures of the spine. (Ramos & Martin, 1994) Additionally, vertebral decompression uses gentle traction to relieve nerve pain associated with herniated discs. It helps reduce the compression force on the affected spinal discs, reducing nerve compression by expanding the disc height in the spine. (Wang et al., 2022)
With spinal decompression being incorporated to reduce the effects of herniated discs, individuals are strapped into a traction machine in a supine position. They will feel a mechanical pull to their spines as the herniated disc returns to its original position and the height of the spinal disc increases. (Oh et al., 2019) This allows the negative pressure from the traction to increase the body’s blood flow for the nutrients and fluids to rehydrate the discs while allowing the body’s natural healing process to kick into full gear. (Choi et al., 2022) After a few consecutive sessions with spinal decompression, many individuals will notice that the pain in their neck, back, and shoulders has decreased and that they can return to their daily activities. Spinal decompression allows the individual to regain their health and well-being while also reminding them to be more mindful of what certain factors can cause the pain to return to the spine. By being more aware of what is affecting a person’s body, they have the tools to continue their health and wellness journey.
References
Blamoutier, A. (2019). Nerve root compression by lumbar disc herniation: A french discovery? Orthop Traumatol Surg Res, 105(2), 335-338. https://doi.org/10.1016/j.otsr.2018.10.025
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P. B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. https://doi.org/10.1155/2022/6343837
Cunha, C., Silva, A. J., Pereira, P., Vaz, R., Goncalves, R. M., & Barbosa, M. A. (2018). The inflammatory response in the regression of lumbar disc herniation. Arthritis Res Ther, 20(1), 251. https://doi.org/10.1186/s13075-018-1743-4
Ge, C. Y., Hao, D. J., Yan, L., Shan, L. Q., Zhao, Q. P., He, B. R., & Hui, H. (2019). Intradural Lumbar Disc Herniation: A Case Report and Literature Review. Clin Interv Aging, 14, 2295-2299. https://doi.org/10.2147/CIA.S228717
Jin, Y. Z., Zhao, B., Zhao, X. F., Lu, X. D., Fan, Z. F., Wang, C. J., Qi, D. T., Wang, X. N., Zhou, R. T., & Zhao, Y. B. (2023). Lumbar Intradural Disc Herniation Caused by Injury: A Case Report and Literature Review. Orthopaedic Surgery, 15(6), 1694-1701. https://doi.org/10.1111/os.13723
Oh, H., Choi, S., Lee, S., Choi, J., & Lee, K. (2019). Effects of the flexion-distraction technique and drop technique on straight leg raising angle and intervertebral disc height of patients with an intervertebral disc herniation. Journal of Physical Therapy Science, 31(8), 666-669. https://doi.org/10.1589/jpts.31.666
Ramos, G., & Martin, W. (1994). Effects of vertebral axial decompression on intradiscal pressure. J Neurosurg, 81(3), 350-353. https://doi.org/10.3171/jns.1994.81.3.0350
Wang, W., Long, F., Wu, X., Li, S., & Lin, J. (2022). Clinical Efficacy of Mechanical Traction as Physical Therapy for Lumbar Disc Herniation: A Meta-Analysis. Comput Math Methods Med, 2022, 5670303. https://doi.org/10.1155/2022/5670303
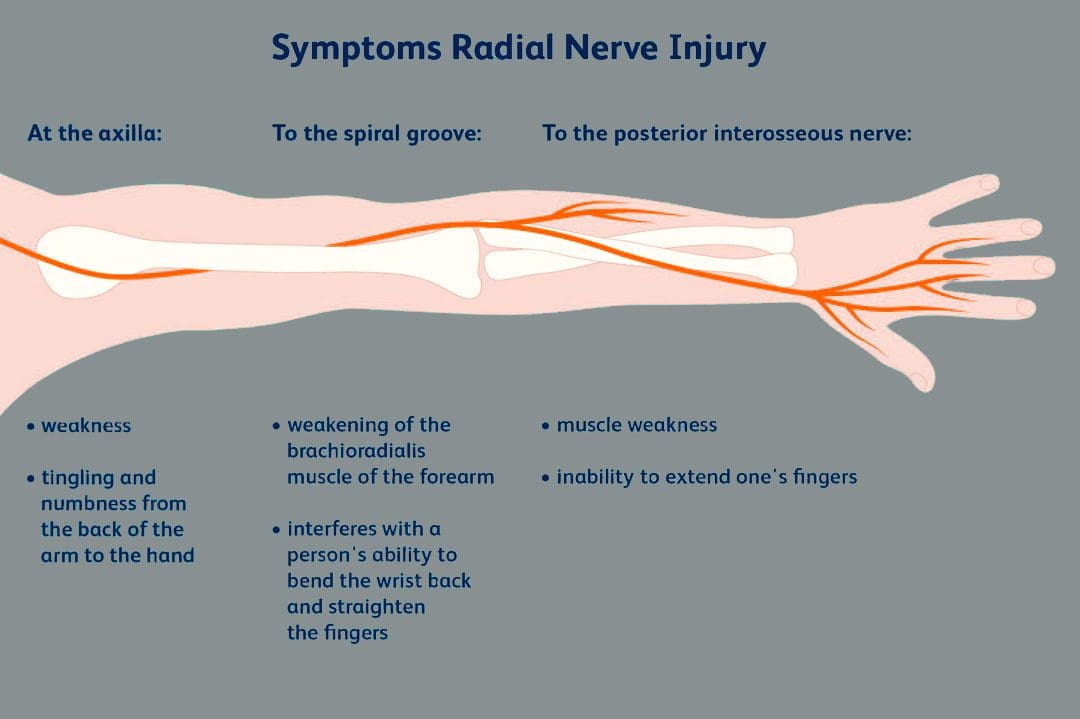
The brachial plexus is a network of nerves that begin in the cervical/neck spinal cord and travel down the cervicoaxillary canal into the armpit. Forming in the area of the shoulder joint at the branch junction of the brachial plexus, the radial nerve extends down the arm, through the elbow joint, into the forearm, across the wrist, and tips of the fingers. The nerves are susceptible to injury that can cause abnormal function leading to unusual sensations and impaired muscle function.
Radial Nerve
One of the major nerves of the upper extremity.
There is one brachial plexus on each side of the body that carries the nerves to each arm.
The radial nerve has two major functions.
One is to provide sensations in the hands, forearms, arms, and fingers.
The other is to deliver messages to muscles about when to contract.
Motor Function
The radial nerve transmits signals to the muscles of the back of the arm and forearm on when to contract.
Individuals who have abnormal radial nerve function can experience weakness of the muscles and symptoms like wrist drop.
A wrist drop occurs when the back forearm muscles cannot support the wrist, causing the individual to hold the wrist in a flexed posture.
Abnormal radial nerve function can cause symptoms of numbness or tingling in the back of the hand.
Conditions
Associated conditions to the radial nerve include lacerations, contusions, fractures, and palsies.
Nerve Contusion
A contusion typically occurs through blunt force trauma that can crush and smash the nerve area.
This causes abnormal or no function.
A nerve contusion can occur from a personal, work, or sports injury or other conditions that generate intense pressure on the nerve/s.
Nerve Lacerations
A laceration occurs when there is a penetrating injury that cuts and/or severs the nerve.
This injury can occur from stab wounds or sliced by broken glass, metal, etc.
Fractures
Broken bones of the upper extremity can lead to extended damage to the nerves near the damaged bone.
The most common type of fracture associated with radial nerve malfunction is fractures to the humerus bone.
The nerve wraps tightly around the humerus and can be injured with a fracture.
Most fracture-related radial nerve injuries heal on their own and do not require surgery.
However, the way the injury heals can be the difference between normal function and chronic pain.
Crutch Palsy
Crutch palsy is pressure on the radial nerve in the armpit resulting from using crutches incorrectly.
To use crutches properly, the individual needs to support their body weight through the hands.
However, many tend to place pressure around the armpit at the top of the crutch, causing irritation to the nerve in that area.
Padding the top of crutches and using the proper form can prevent the condition.
Saturday Night Palsy
Saturday night palsy is the abnormal function of the radial nerve after sleeping in a position that causes direct pressure against the nerve.
This often occurs when an individual falls asleep with their arm draped over an armrest on a chair.
The name comes from when individuals are intoxicated and fall asleep in a location other than the bed and in awkward positions.
Treatment
Nerve injuries often cause symptoms at different locations other than where the nerve damage is, complicating diagnosis. Determining the specific location of nerve damage is the first step in developing an appropriate treatment plan. Once the location has been identified, steps can be taken to prevent worsening damage to the nerve.
The objective is to relieve the pressure from the irritation or compression.
Massage to relax the area and increase blood circulation.
Decompression to physically restore alignment.
Adjustments to restore body balance.
Exercises and stretches to maintain treatment, strengthen the muscles, and prevent injuries.
In cases where there is structural damage, surgery may be necessary to remove pressure or repair damage.
Avoid Surgery
References
Ansari FH, Juergens AL. Saturday Night Palsy. [Updated 2023 Apr 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557520/
Barton, N J. “Radial nerve lesions.” The Hand vol. 5,3 (1973): 200-8. doi:10.1016/0072-968x(73)90029-6
Daly, Michael, and Chris Langhammer. “Radial Nerve Injury in Humeral Shaft Fracture.” The Orthopedic Clinics of North America vol. 53,2 (2022): 145-154. doi:10.1016/j.ocl.2022.01.001
DeCastro A, Keefe P. Wrist Drop. [Updated 2022 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532993/
Eaton, C J, and G D Lister. “Radial nerve compression.” Hand Clinics vol. 8,2 (1992): 345-57.
Glover NM, Murphy PB. Anatomy, Shoulder and Upper Limb, Radial Nerve. [Updated 2022 Aug 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534840/
Ljungquist, Karin L et al. “Radial nerve injuries.” The Journal of hand surgery vol. 40,1 (2015): 166-72. doi:10.1016/j.jhsa.2014.05.010
In many people with facet joint syndrome, how does spinal decompression compare to traditional spinal surgery alleviate low back pain?
Introduction
Many people around the globe experience lower back pain for various reasons, such as lifting or carrying heavy objects, sedentary jobs, or traumatic events that can cause spinal injuries. The spine has a crucial role in providing mobility and flexibility without discomfort. The facet joints and spinal discs work together to generate healthy movement and stability within each segment. However, when the muscles, ligaments, and tissues surrounding the spinal disc are overstretched or compressed due to normal or traumatic factors, it can aggravate the nerve roots and cause discomfort. As we age or carry excess weight, our spinal discs can experience wear and tear, leading to facet joint syndrome. This syndrome is often associated with lower back pain caused by injured facet joints. This article will explore how facet joint syndrome is linked to lower back pain and how non-surgical treatments can help alleviate it. We work with certified medical providers who use our patients’ valuable information to treat individuals suffering from facet joint syndrome affecting spine mobility and causes low back pain. We also inform them about non-surgical treatments to regain spinal mobility and reduce pain-like symptoms that correlate with this spinal condition. We encourage patients to ask essential questions and seek education from our associated medical providers about their situation. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
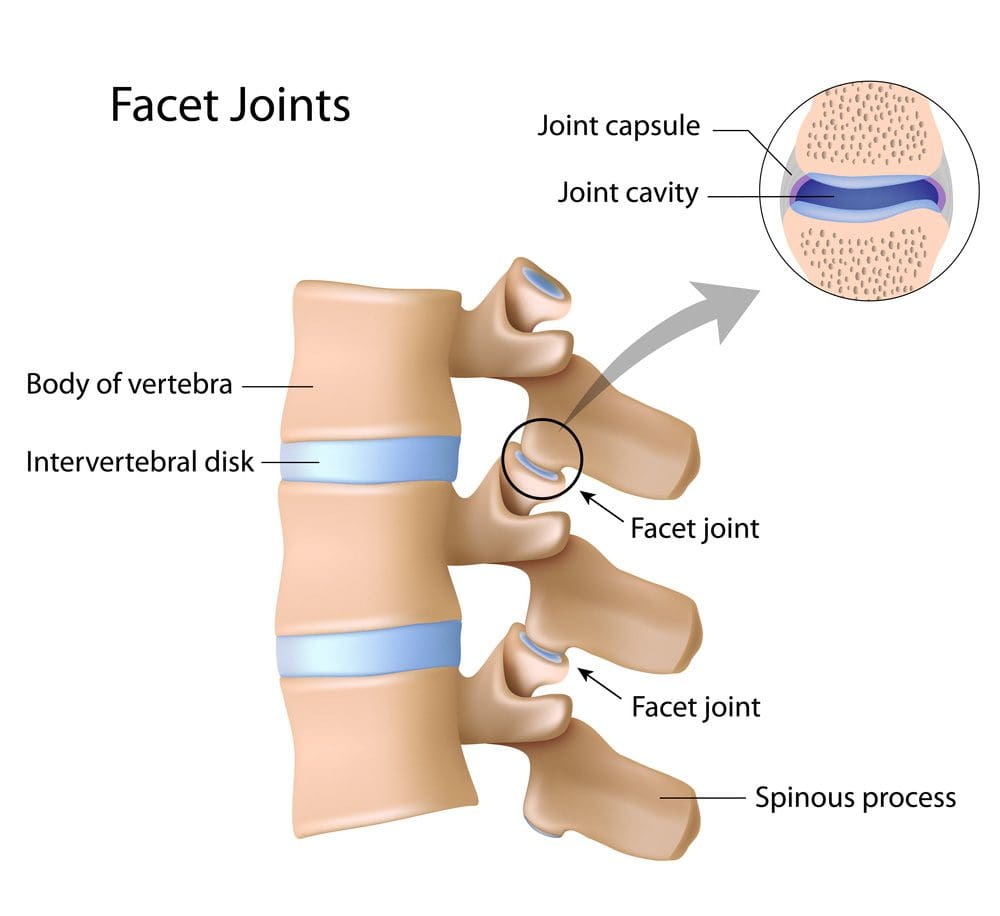
Facet Joint Syndrome
Are you experiencing pain that radiates down to your legs, especially when standing? Do you constantly hunch over, affecting your posture during everyday activities? Have you noticed numbness or loss of sensation in your feet or buttocks? As we age or experience traumatic injuries, the facet joints on either side of our spine can become damaged, resulting in a condition called facet joint syndrome. Research indicates that environmental conditions can cause joint degeneration, leading to symptoms similar to other spinal conditions. Cartilage erosion and inflammation on the spine are common signs of facet joint syndrome, often associated with musculoskeletal disorders like low back pain.
Low Back Pain Associated With Facet Syndrome
Research studiesmusculoskeletal disorders like low back pain are associated with facet syndrome. When the facet joints start to degenerate from repetitive overuse motions caused by everyday activities, it can cause micro instabilities to the facet joints while compressing the surrounding nerve roots. When this happens, many individuals will experience low back pain and sciatic nerve pain conditions that cause them to be unstable while walking. Additional research studies stated that low back pain associated with facet syndrome can cause symptoms of restricted movement, reduce the quality of life and greatly impact the entire lumbar vertebral structure. Since low back pain is a common problem many individuals have, the combination with facet syndrome can trigger reactive muscle spasms, a protective mechanism in the spine to cause the individual to have difficulty moving comfortably and experience severe sudden pain. To that point, low back pain associated with facet syndrome causes the person to be dealing with constant ongoing pain, making a normal lifestyle almost difficult.
Discover The Benefits Of Chiropractic Care-Video
Low back pain associated with facet joint syndrome should not make life difficult. Numerous treatments pertain to relieving the pain-like symptoms and help slow the process of facet syndrome from causing more issues to the spine. Non-surgical treatments like chiropractic care can help reduce the effects of facet syndrome as they can provide benefits to restore spinal mobility. The video above explores the benefits of chiropractic care, as chiropractors will discuss the recommended course of personalized treatment with you. Non-surgical treatments are safe, gentle on the spine, and cost-effective as they help regain your body’s mobility from facet syndrome. At the same time, non-surgical treatments like chiropractic care can be combined with other non-surgical therapies that can help restart the body’s natural healing process to allow the compressed spinal disc and joint to be rehydrated.
Spinal Decompression Alleviating Facet Syndrome
According to research studies, non-surgical treatments like spinal decompression can help reduce the effects of facet syndrome as it can help improve the spine;’s mobility through gentle traction and can help stretch out the affected muscles associated with low back pain by taking pressure off the aggravating nerve root. In “The Ultimate Spinal Decompression,” Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., mentioned that when individuals are going in for spinal decompression, they might experience a “popping sensation” as the jammed facet joints are being open for treatment. This is normal for early facet arthropathy and can occur within the first few treatment sessions. At the same time, spinal decompression can gently stretch the adjacent compressed nerve root and find instant relief. After the treatment, many individuals can combine other treatments like physical therapy to reduce the painful symptoms from returning. Non-surgical treatments like spinal decompression and chiropractic care can help revitalize the spine affected by facet joint syndrome and help restore a person’s quality of life.
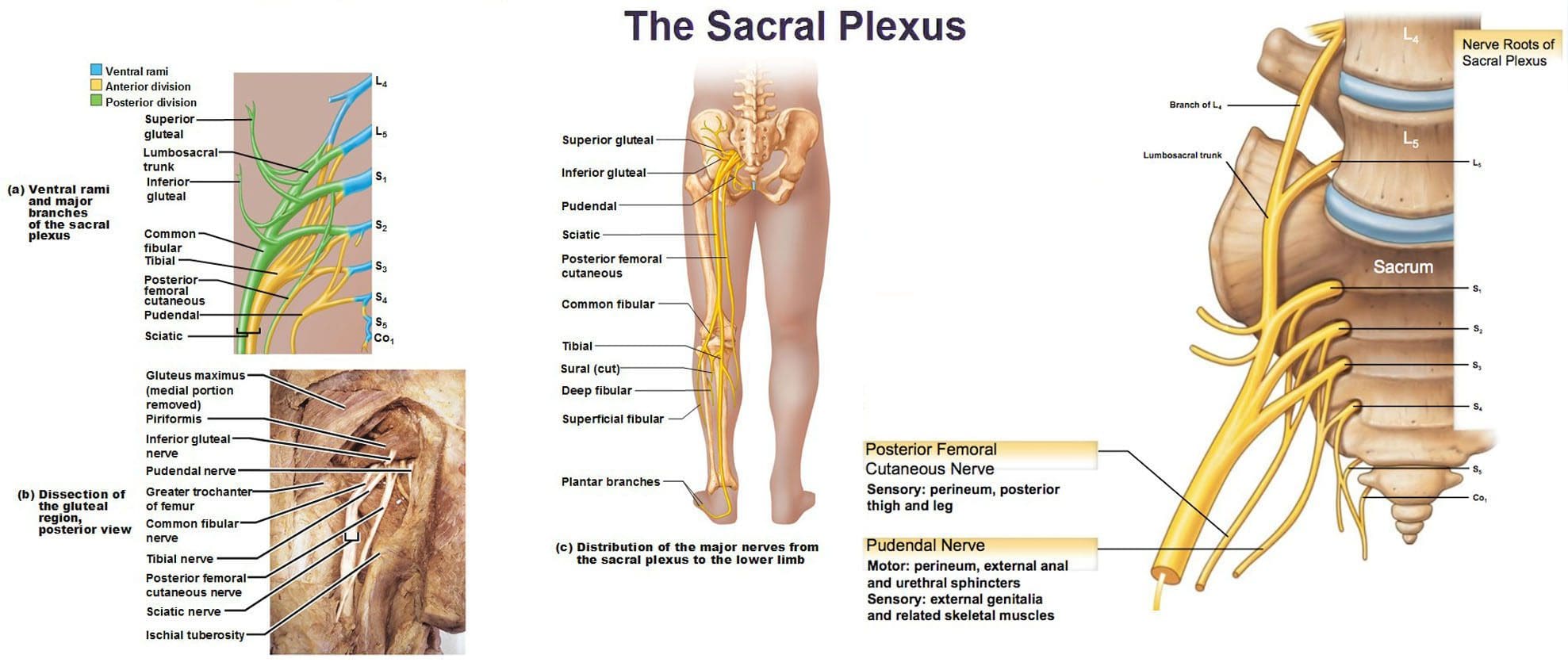
The lumbosacral plexus is located on the posterolateral wall of the lesser pelvis, next to the lumbar spine. A plexus is a network of intersecting nerves that share roots, branches, and functions. The sacral plexus is a network that emerges from the lower part of the spine. The plexus then embeds itself into the psoas major muscle and emerges in the pelvis. These nerves provide motor control to and receive sensory information from portions of the pelvis and leg. Sacral nerve discomfort symptoms, numbness, or other sensations and pain can be caused by an injury, especially if the nerve roots are compressed, tangled, rubbing, and irritated. This can cause symptoms like back pain, pain in the back and sides of the legs, sensory issues affecting the groin and buttocks, and bladder or bowel problems. Injury Medical Chiropractic and Functional Medicine Clinic can develop a personalized treatment plan to relieve symptoms, release the nerves, relax the muscles, and restore function.
Sacral Plexus
Anatomy
The sacral plexus is formed by the lumbar spinal nerves, L4 and L5, and sacral nerves S1 through S4.
Several combinations of these spinal nerves merge together and then divide into the branches of the sacral plexus.
Everybody has two sacral plexi – plural of plexus – one on the right side and left side that is symmetrical in structure and function.
Structure
There are several plexi throughout the body. The sacral plexus covers a large area of the body in terms of motor and sensory nerve function.
Spinal nerves L4 and L5 make up the lumbosacral trunk, and the anterior rami of sacral spinal nerves S1, S2, S3, and S4 join the lumbosacral trunk to form the sacral plexus.
Anterior rami are the branches of the nerve that are towards the front of the spinal cord/front of the body.
At each spinal level, an anterior motor root and a posterior sensory root join to form a spinal nerve.
Each spinal nerve then divides into an anterior – ventral – and a posterior – dorsal – rami portion.
Each can have motor and/or sensory functions.
The sacral plexus divides into several nerve branches, which include:
Superior gluteal nerve – L4, L5, and S1.
Inferior gluteal nerve – L5, S1, and S2.
The sciatic nerve – is the largest nerve of the sacral plexus and among the largest nerves in the body – L4, L5, S1, S2, and S3
The common fibular nerve – L4 through S2, and tibial nerves – L4 through S3 are branches of the sciatic nerve.
Posterior femoral cutaneous nerve – S1, S2, and S3.
Pudendal nerve – S2, S3, and S4.
The nerve to the quadratus femoris muscle is formed by L4, L5, and S1.
The obturator internus muscle nerve – L5, S1, and S2.
The piriformis muscle nerve – S1 and S2.
Function
The sacral plexus has substantial functions throughout the pelvis and legs. The branches provide nerve stimulation to several muscles. The sacral plexus nerve branches also receive sensory messages from the skin, joints, and structures of the pelvis and legs.
Motor
Motor nerves of the sacral plexus receive signals from the brain that travel down the column of the spine, out to the motor nerve branches of the sacral plexus to stimulate muscle contraction and movement. Motor nerves of the sacral plexus include:
Superior Gluteal Nerve
This nerve provides stimulation to the gluteus minimus, gluteus medius, and tensor fascia lata, which are muscles that help move the hip away from the center of the body.
Inferior Gluteal Nerve
This nerve provides stimulation to the gluteus maximus, the large muscle that moves the hip laterally.
Sciatic Nerve
The sciatic nerve has a tibial portion and a common fibular portion, which have motor and sensory functions.
The tibial portion stimulates the inner part of the thigh and activates muscles in the back of the leg and the sole of the foot.
The common fibular portion of the sciatic nerve stimulates and moves the thigh and knee.
The common fibular nerve stimulates muscles in the front and sides of the legs and extends the toes to straighten them out.
Pudendal Nerve
The pudendal nerve also has sensory functions that stimulate the muscles of the urethral sphincter to control urination and the muscles of the anal sphincter to control defecation.
The nerve to the quadratus femoris stimulates the muscle to move the thigh.
The nerve to the obturator internus muscle stimulates the muscle to rotate the hips and stabilize the body when walking.
The nerve to the piriformis muscle stimulates the muscle to move the thigh away from the body.
Conditions
The sacral plexus, or areas of the plexus, can be affected by disease, traumatic injury, or cancer. Because the nerve network has many branches and portions, symptoms can be confusing. Individuals may experience sensory loss or pain in regions in the pelvis and leg, with or without muscle weakness. Conditions that affect the sacral plexus include:
Injury
A traumatic injury of the pelvis can stretch, tear, or harm the sacral plexus nerves.
Bleeding can inflame and compress the nerves, causing malfunction.
Neuropathy
Nerve impairment can affect the sacral plexus or parts of it.
Neuropathy can come from:
Diabetes
Vitamin B12 deficiency
Certain medications – chemotherapeutic meds
Toxins like lead
Alcohol
Metabolic illnesses
Infection
An infection of the spine or the pelvic region can spread to the sacral plexus nerves or produce an abscess, causing symptoms of nerve impairment, pain, tenderness, and sensations around the infected region.
Cancer
Cancer developing in the pelvis or spreading to the pelvis from somewhere else can compress or infect the sacral plexus nerves.
Treatment of the Underlying Medical Condition
Rehabilitation begins with the treatment of the underlying medical condition causing the nerve problems.
Cancer treatment – surgery, chemotherapy, and/or radiation.
Antibiotic treatment for infections.
Neuropathy treatment can be complicated because the cause may be unclear, and an individual can experience several causes of neuropathy simultaneously.
Major pelvic trauma like a vehicle collision can take months, especially if there are multiple bone fractures.
Motor and Sensory Recovery
Sensory problems can interfere with walking, standing, and sitting.
Adapting to sensory deficits is an important part of treatment, rehabilitation, and recovery.
Chiropractic, decompression, massage, and physical therapy can relieve symptoms, restore strength, function, and motor control.
Sciatica Secrets Revealed
References
Dujardin, Franck et al. “Extended anterolateral transiliac approach to the sacral plexus.” Orthopaedics & traumatology, surgery & research: OTSR vol. 106,5 (2020): 841-844. doi:10.1016/j.otsr.2020.04.011
Eggleton JS, Cunha B. Anatomy, Abdomen and Pelvis, Pelvic Outlet. [Updated 2022 Aug 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557602/
Garozzo, Debora et al. “In lumbosacral plexus injuries can we identify indicators that predict spontaneous recovery or the need for surgical treatment? Results from a clinical study on 72 patients.” Journal of brachial plexus and peripheral nerve injury vol. 9,1 1. 11 Jan. 2014, doi:10.1186/1749-7221-9-1
Gasparotti R, Shah L. Brachial and Lumbosacral Plexus and Peripheral Nerves. 2020 Feb 15. In: Hodler J, Kubik-Huch RA, von Schulthess GK, editors. Diseases of the Brain, Head and Neck, Spine 2020–2023: Diagnostic Imaging [Internet]. Cham (CH): Springer; 2020. Chapter 20. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554335/ doi: 10.1007/978-3-030-38490-6_20
Norderval, Stig, et al. “Sacral nerve stimulation.” Tidsskrift for den Norske laegeforening : tidsskrift for praktisk medicin, ny raekke vol. 131,12 (2011): 1190-3. doi:10.4045/tidsskr.10.1417
Neufeld, Ethan A et al. “MR Imaging of the Lumbosacral Plexus: A Review of Techniques and Pathologies.” Journal of Neuroimaging: official journal of the American Society of Neuroimaging vol. 25,5 (2015): 691-703. doi:10.1111/jon.12253
Staff, Nathan P, and Anthony J Windebank. “Peripheral neuropathy due to vitamin deficiency, toxins, and medications.” Continuum (Minneapolis, Minn.) vol. 20,5 Peripheral Nervous System Disorders (2014): 1293-306. doi:10.1212/01.CON.0000455880.06675.5a
Yin, Gang, et al. “Obturator Nerve Transfer to the Branch of the Tibial Nerve Innervating the Gastrocnemius Muscle for the Treatment of Sacral Plexus Nerve Injury.” Neurosurgery vol. 78,4 (2016): 546-51. doi:10.1227/NEU.0000000000001166
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine