Spinal stenosis is the term used to describe a narrowing spine. Treatments vary because everybody’s case is different. Some individuals experience mild symptoms, while others experience severe symptoms. Can knowing treatment options help the patient and healthcare team customize and personalize a treatment plan to the individual’s condition?
Spinal Stenosis Treatments
Spaces within the spine can become narrower than they’re supposed to be, which can cause pressure on nerve roots and the spinal cord. Anywhere along the spine can be affected. The narrowing can cause pain, burning, and/or aching in the back and weakness in the legs and feet. Spinal stenosis has several primary treatments. When working through spinal stenosis treatments, a healthcare provider will assess symptoms and start treatment with first-line therapy, such as pain medication and/or physical therapy. These are often the first among individuals with the disease.
Medication
Chronic pain is one of the main symptoms. The first-line treatment often involves using pain-relieving medication/s. Commonly prescribed medications are nonsteroidal anti-inflammatories or NSAIDs. These medications reduce pain and inflammation. However, NSAIDs are not recommended for long-term use, and other medications may need to be used to relieve pain that includes: (Sudhir Diwan et al., 2019)
Tylenol – acetaminophen
Gabapentin
Pregabalin
Opioids for severe cases
Exercise
Exercise can reduce spinal stenosis symptoms by taking pressure off the nerves, which can reduce pain and improve mobility. (Andrée-Anne Marchand et al., 2021) Healthcare providers will recommend the most effective exercises for the individual. Examples include:
Another primary spinal stenosis treatment is physical therapy, which is often used alongside pain medications. Typically, individuals undergo six to eight weeks of physical therapy, with sessions two to three times a week. Utilizing physical therapy has been shown to (Sudhir Diwan et al., 2019)
Reduce pain
Increase mobility
Reduce pain medications.
Reduce mental health symptoms like anger, depression, and mood changes.
For severe cases, physical therapy following surgery can reduce recovery times.
Back Braces
Back braces can help reduce movement and pressure on the spine. This is helpful because even small spinal movements can lead to nerve irritation, pain, and worsening symptoms. Over time, the bracing can lead to a positive increase in mobility. (Carlo Ammendolia et al., 2019)
Injections
Epidural steroid injections may be recommended to relieve severe symptoms. Steroids act as anti-inflammatories to reduce pain and swelling caused by inflammation and irritation of the spinal nerves. They are considered nonsurgical medical procedures. According to research, injections can effectively manage pain for two weeks and up to six months, and some research has found that after a spinal injection, relief can last 24 months. (Sudhir Diwan et al., 2019)
Thickened Ligaments Decompression Procedure
Some individuals may be recommended to undergo a decompression procedure. This procedure involves using a thin needle tool inserted into the back. The thickened ligament tissue is removed to reduce the pressure on the spine and nerves. Research has found that the procedure can reduce symptoms and the need for more invasive surgery. (Nagy Mekhail et al., 2021)
Alternative Treatments
In addition to first-line treatments, individuals may be referred to alternative therapies for symptom management, including:
Acupuncture
This involves the insertion of thin-tipped needles into various acupoints to relieve symptoms.
Some research has found that acupuncture may be more effective at reducing symptoms than physical therapy alone. Both options are viable and can improve mobility and pain. (Hiroyuki Oka et al., 2018)
Chiropractic
This therapy reduces pressure on nerves, maintains spinal alignment, and helps to improve mobility.
Massage
Massage helps to increase circulation, relax the muscles, and reduce pain and stiffness.
New Treatment Options
As spinal stenosis research continues, new therapies are emerging to help relieve and manage symptoms in individuals who don’t respond to traditional medicine or cannot partake in conventional therapies for various reasons. However, some evidence presented is promising; medical insurers may consider them experimental and not offer coverage until their safety has been proven. Some new treatments include:
Acupotomy
Acupotomy is a form of acupuncture that uses thin needles with a small, flat, scalpel-type tip to relieve tension in painful areas. Research on its effects is still limited, but preliminary data shows it could be an effective complementary treatment. (Ji Hoon Han et al., 2021)
Stem Cell Therapy
Stem cells are the cells from which all other cells originate. They act as the raw material for the body to create specialized cells with specific functions. (National Institutes of Health. 2016)
Individuals with spinal stenosis can develop soft tissue damage.
Stem cell therapy uses stem cells to help repair injured or diseased tissues.
Stem cell therapy can help repair or improve the damaged areas and provide symptom relief.
Clinical studies for spinal stenosis report that it could be a viable treatment option for some.
However, more research is needed to confirm whether the therapy is effective enough to be widely used. (Hideki Sudo et al., 2023)
Dynamic Stabilization Devices
LimiFlex is a medical device undergoing research and analysis for its ability to restore mobility and stability in the spine. It is implanted into the back through a surgical procedure. According to research, individuals with spinal stenosis who receive the LimiFlex often experience a higher reduction in pain and symptoms than with other forms of treatment. (T Jansen et al., 2015)
Lumbar Interspinous Distraction Decompression
Lumbar interspinous distraction decompression is another surgical procedure for spinal stenosis. The surgery is performed with an incision above the spine and places a device between two vertebrae to create space. This reduces movement and pressure on the nerves. Preliminary results show positive short-term relief from symptoms; long-term data is not yet available as it is a relatively new spinal stenosis treatment option. (UK National Health Service, 2022)
Surgical Procedures
There are several surgical procedures are available for spinal stenosis. Some include: (NYU Langone Health. 2024) Surgery for spinal stenosis is often reserved for individuals with severe symptoms, like numbness in the arms or legs. When these symptoms develop, it indicates a more notable compression of the spinal nerves and the need for a more invasive treatment. (NYU Langone Health. 2024)
Laminectomy
A laminectomy removes part or all of the lamina, the vertebral bone covering the spinal canal.
The procedure is designed to reduce pressure on nerves and the spinal cord.
Laminotomy and Foraminotomy
Both surgeries are used if an individual’s spinal stenosis negatively affects an opening in the vertebral foramen.
Ligaments, cartilage, or other tissues that constrict the nerves are removed.
Both reduce pressure on the nerves traveling through the foramen.
Laminoplasty
A laminoplasty relieves pressure on the spinal cord by removing parts of the spinal canal’s lamina.
This surgical procedure involves removing herniated or bulging discs that are placing pressure on the spinal cord and nerves.
Spinal fusion
Spinal fusion involves joining two vertebrae using metal pieces like rods and screws.
The vertebrae are more stable because the rods and screws act as a brace.
Which Treatment Is The Right One?
Because all treatment plans differ, determining the most effective is best suited for a healthcare provider. Each approach will be personalized to the individual. To decide what therapy is best, healthcare providers will assess: (National Institute of Arthritis and Musculoskeletal and Skin Diseases. 2023)
The severity of symptoms.
The current level of overall health.
The level of damage that’s occurring in the spine.
The level of disability and how mobility and quality of life are affected.
Injury Medical Chiropractic and Functional Medicine Clinic will work with an individual’s primary healthcare provider and/or specialists to help determine the best treatment options and concerns regarding medications or other forms of treatment.
Unlocking Wellness
References
Diwan, S., Sayed, D., Deer, T. R., Salomons, A., & Liang, K. (2019). An Algorithmic Approach to Treating Lumbar Spinal Stenosis: An Evidenced-Based Approach. Pain medicine (Malden, Mass.), 20(Suppl 2), S23–S31. https://doi.org/10.1093/pm/pnz133
Marchand, A. A., Houle, M., O’Shaughnessy, J., Châtillon, C. É., Cantin, V., & Descarreaux, M. (2021). Effectiveness of an exercise-based prehabilitation program for patients awaiting surgery for lumbar spinal stenosis: a randomized clinical trial. Scientific reports, 11(1), 11080. https://doi.org/10.1038/s41598-021-90537-4
Ammendolia, C., Rampersaud, Y. R., Southerst, D., Ahmed, A., Schneider, M., Hawker, G., Bombardier, C., & Côté, P. (2019). Effect of a prototype lumbar spinal stenosis belt versus a lumbar support on walking capacity in lumbar spinal stenosis: a randomized controlled trial. The spine journal : official journal of the North American Spine Society, 19(3), 386–394. https://doi.org/10.1016/j.spinee.2018.07.012
Mekhail, N., Costandi, S., Nageeb, G., Ekladios, C., & Saied, O. (2021). The durability of minimally invasive lumbar decompression procedure in patients with symptomatic lumbar spinal stenosis: Long-term follow-up. Pain practice : the official journal of World Institute of Pain, 21(8), 826–835. https://doi.org/10.1111/papr.13020
Oka, H., Matsudaira, K., Takano, Y., Kasuya, D., Niiya, M., Tonosu, J., Fukushima, M., Oshima, Y., Fujii, T., Tanaka, S., & Inanami, H. (2018). A comparative study of three conservative treatments in patients with lumbar spinal stenosis: lumbar spinal stenosis with acupuncture and physical therapy study (LAP study). BMC complementary and alternative medicine, 18(1), 19. https://doi.org/10.1186/s12906-018-2087-y
Han, J. H., Lee, H. J., Woo, S. H., Park, Y. K., Choi, G. Y., Heo, E. S., Kim, J. S., Lee, J. H., Park, C. A., Lee, W. D., Yang, C. S., Kim, A. R., & Han, C. H. (2021). Effectiveness and safety of acupotomy on lumbar spinal stenosis: A pragmatic randomized, controlled, pilot clinical trial: A study protocol. Medicine, 100(51), e28175. https://doi.org/10.1097/MD.0000000000028175
Sudo, H., Miyakoshi, T., Watanabe, Y., Ito, Y. M., Kahata, K., Tha, K. K., Yokota, N., Kato, H., Terada, T., Iwasaki, N., Arato, T., Sato, N., & Isoe, T. (2023). Protocol for treating lumbar spinal canal stenosis with a combination of ultrapurified, allogenic bone marrow-derived mesenchymal stem cells and in situ-forming gel: a multicentre, prospective, double-blind randomised controlled trial. BMJ open, 13(2), e065476. https://doi.org/10.1136/bmjopen-2022-065476
National Institutes of Health. (2016). Stem cell basics. U.S. Department of Health and Human Services. Retrieved from https://stemcells.nih.gov/info/basics/stc-basics
Jansen, T., Bornemann, R., Otten, L., Sander, K., Wirtz, D., & Pflugmacher, R. (2015). Vergleich dorsaler Dekompression nicht stabilisiert und dynamisch stabilisiert mit LimiFlex™ [A Comparison of Dorsal Decompression and Dorsal Decompression Combined with the Dynamic Stabilisation Device LimiFlex™]. Zeitschrift fur Orthopadie und Unfallchirurgie, 153(4), 415–422. https://doi.org/10.1055/s-0035-1545990
UK National Health Service. (2022). Lumbar decompression surgery: How It’s performed. https://www.nhs.uk/conditions/lumbar-decompression-surgery/what-happens/
NYU Langone Health. (2024). Surgery for spinal stenosis. https://nyulangone.org/conditions/spinal-stenosis/treatments/surgery-for-spinal-stenosis
Columbia Neurosurgery. (2024). Cervical laminoplasty procedure. https://www.neurosurgery.columbia.edu/patient-care/treatments/cervical-laminoplasty
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Spinal stenosis: Diagnosis, treatment and steps to take. Retrieved from https://www.niams.nih.gov/health-topics/spinal-stenosis/diagnosis-treatment-and-steps-to-take
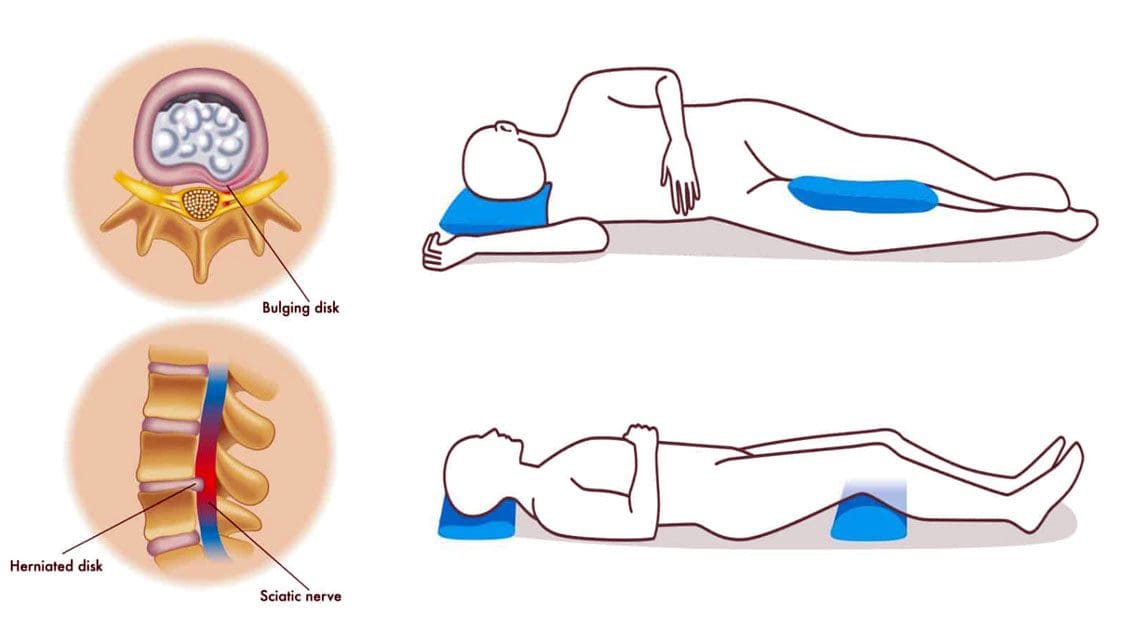
For individuals with back pain, can sleeping with a pillow between or under their knees help bring relief during sleep?
Sleep With A Pillow Between The Legs
Healthcare providers may recommend that individuals with back pain due to pregnancy or conditions like a herniated disc and sciatica sleep with a pillow between their legs. Sleeping with a pillow between the legs may help relieve back and hip pain, as the position helps maintain pelvis and spinal alignment. Proper spinal alignment can help relieve back stress and pain.
The Benefits
Some potential benefits of sleeping with a pillow between the knees.
Reduce Back and Hip Pain
When sleeping on the side, the spine, shoulders, and hips may twist to maintain the position because the center of gravity is elevated, causing instability. (Gustavo Desouzart et al., 2015) Placing a pillow between the knees may help maintain stability and reduce back and hip pain. (Gustavo Desouzart et al., 2015) The pillow neutralizes the position of the pelvis by slightly elevating the leg on top. This decreases the pressure on the lower back and hip joints, which may help reduce pain and allow for improved sleep.
Reduce Sciatica Symptoms
Sciatica nerve pain travels from the lower back down one leg due to a compressed spinal nerve root in the lower back. (American Academy of Orthopaedic Surgeons, 2021) Sleeping with a pillow between the knees may help reduce symptoms and sensations. A pillow between the legs can help prevent twisting the back, rotating the spine, or tilting the pelvis during sleep.
Reduce Herniated Disc Symptoms
A herniated disc can pressure the spinal nerves, leading to pain and numbness. (Penn Medicine. 2024) Sleeping on the side can worsen herniated disc pain; however, placing a pillow between the knees keeps the pelvis in neutral alignment and prevents spinal rotation. Sleeping on the back with a pillow under the knees can also help reduce pressure on the disc. (University of Central Florida. N.D.)
Improve Posture
Maintaining healthy posture while sitting or standing is important to neuromusculoskeletal health and injury prevention. Proper alignment during sleep can help improve posture (Doug Cary et al., 2021). According to one study, individuals spend more than half of their time sleeping in a side-lying posture. (Eivind Schjelderup Skarpsno et al., 2017) Sleeping on the side with the top leg frequently falls forward, bringing the pelvis into a forward tilt that places added pressure on the hips and spine connective tissues. This position disrupts the body’s natural alignment. (Doug Cary et al., 2021) Placing a pillow between the knees improves sleeping posture by lifting the top leg and prevents forward shifting. (University of Rochester Medical Center. 2024)
Increased weight leads to increased pressure on joints.
Significant change in the center of gravity.
Hormonal changes make connective tissues more lax.
Pregnant women with hip or back pain are often recommended to sleep with a pillow between their knees to relieve pain and discomfort. Doctors agree that lying on the left side is the best sleep position during the second and third trimesters. This position ensures optimal blood flow for the mother and baby and helps kidney function. (Standford Medicine, 2024) Placing a pillow between the knees can help reduce the pressure on the joints and also help maintain the left-side lying position. (O’Brien LM, Warland J. 2015) (Standford Medicine, 2024) Larger maternity pillows supporting the abdomen and lower back can provide more comfort.
Consult a healthcare provider about sleeping with a pillow between the knees to see if it is right for you.
What Causes Disc Herniation?
References
Desouzart, G., Matos, R., Melo, F., & Filgueiras, E. (2015). Effects of sleeping position on back pain in physically active seniors: A controlled pilot study. Work (Reading, Mass.), 53(2), 235–240. https://doi.org/10.3233/WOR-152243
American Academy of Orthopaedic Surgeons. (2021). Sciatica. OrthoInfo. https://orthoinfo.aaos.org/en/diseases–conditions/sciatica
Penn Medicine. (2024). Herniated disc disorders. Penn Medicine. https://www.pennmedicine.org/for-patients-and-visitors/patient-information/conditions-treated-a-to-z/herniated-disc-disorders
University of Central Florida. (N.D.). The best sleeping position for lower back pain (and the worst). UFC Health Services. https://ucfhealth.com/our-services/lifestyle-medicine/best-sleeping-position-for-lower-back-pain/
Cary, D., Jacques, A., & Briffa, K. (2021). Examining relationships between sleep posture, waking spinal symptoms and quality of sleep: A cross sectional study. PloS one, 16(11), e0260582. https://doi.org/10.1371/journal.pone.0260582
Skarpsno, E. S., Mork, P. J., Nilsen, T. I. L., & Holtermann, A. (2017). Sleep positions and nocturnal body movements based on free-living accelerometer recordings: association with demographics, lifestyle, and insomnia symptoms. Nature and science of sleep, 9, 267–275. https://doi.org/10.2147/NSS.S145777
University of Rochester Medical Center. (2024). Good sleeping posture helps your back. Health Encyclopedia. https://www.urmc.rochester.edu/encyclopedia/content.aspx?ContentTypeID=1&ContentID=4460
Casagrande, D., Gugala, Z., Clark, S. M., & Lindsey, R. W. (2015). Low Back Pain and Pelvic Girdle Pain in Pregnancy. The Journal of the American Academy of Orthopaedic Surgeons, 23(9), 539–549. https://doi.org/10.5435/JAAOS-D-14-00248
Standford Medicine. (2024). Sleeping positions during pregnancy. Standford Medicine Children’s Health. https://www.stanfordchildrens.org/en/topic/default?id=sleeping-positions-during-pregnancy-85-P01238
O’Brien, L.M., Warland, J. (2015). Maternal sleep position: what do we know where do we go? BMC Pregnancy Childbirth, 15, Article A4 (2015). https://doi.org/doi:10.1186/1471-2393-15-S1-A4
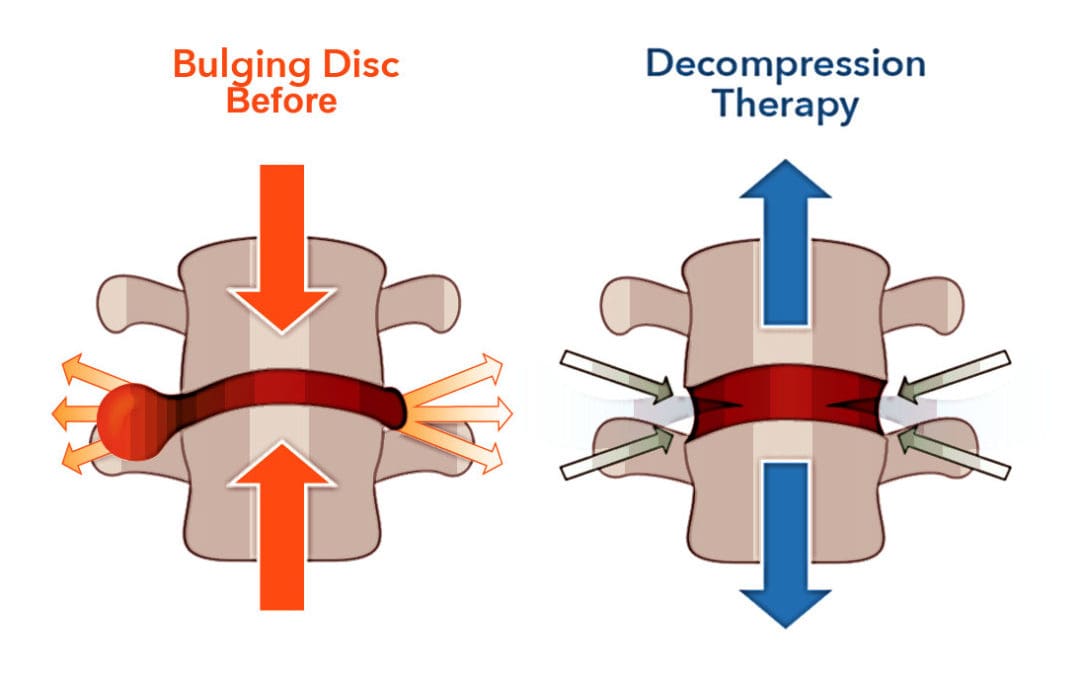
Can individuals with spinal pain in their necks and back utilize decompression therapy to restore spinal disc height and find relief?
Introduction
Many people don’t realize that as the body gets older, so does the spine. The spine is part of the musculoskeletal system that provides structural support to the body by keeping it upright. The surrounding muscles, ligaments, and tissues surrounding the spine help with stability and mobility, while the spinal disc and joints provide shock absorption from the sheer vertical weight. When a person is on the move with their daily activities, the spine can allow the individual to be mobile without pain or discomfort. However, as time passes, the spine goes through degenerative changes that can cause pain and discomfort to the body, thus leaving the individual to deal with overlapping risk profiles that can affect their neck and back. To that point, many people seek out treatments to reduce the pain affecting their spine and restore the disc height in their bodies. Today’s article looks at how spinal pain affects a person’s neck and back and how treatments like spinal decompression can reduce spinal pain and restore disc height. We talk with certified medical providers who consolidate our patients’ information to assess how spinal pain can significantly impact a person’s well-being and quality of life in their bodies. We also inform and guide patients on how integrating spinal decompression can help reduce spinal pain and restore spinal disc height. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating non-surgical treatments into a health and wellness routine to relieve spinal pain and regain their quality of life. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
How Spinal Pain Affects A Person’s Neck & Back
Do you feel constant muscle aches and pains in your neck and back? Have you experienced stiffness and limited mobility when you are twisting and turning? Or do heavy objects cause muscle strain when moving from one location to another? Many individuals will be on the move and be in weird positions without feeling pain and discomfort when it comes to the spine. This is due to the surrounding muscles and tissues being stretched and the spinal discs taking on the vertical pressure on the spine. However, when environmental factors, traumatic injuries, or natural aging start to affect the spine, it can lead to the development of spinal pain. This is because the outer portion of the spinal disc is intact, and the inner portion of the disc is being affected. When abnormal stresses start to reduce the water intake within the disc, it can internally stimulate the pain receptors without nerve root symptoms inside the disc. (Zhang et al., 2009) This causes many individuals to deal with neck and back pain in their bodies and reduces their quality of life.
Spinal pain can lead to overlapping risk profiles that cause many individuals to deal with severe low back pain and neck pain, which then causes the surrounding muscles to become weak, tight, and overstretched. At the same time, the surrounding nerve roots are also affected as the nerve fibers surround the outer and inner parts of the spinal disc, which causes nociceptive pain properties to the neck and back region and leads to discogenic pain. (Coppes et al., 1997) When many individuals are dealing with muscle pain correlated with the spinal discs, it causes a pain-spasm-pain cycle that can affect their bodies due to not moving enough and causing painful muscular activities when trying to be mobile. (Roland, 1986) When a person has limited mobility cause they are experiencing spinal pain, their natural disc height slowly degenerates, causing more issues to their bodies and socioeconomic burdens. Fortunately, when many individuals are dealing with spinal pain, numerous treatments can reduce spinal pain and restore their disc height.
Movement Medicine- Video
How Spinal Decompression Reduces Spinal Pain
When people are seeking treatments for their spinal pain, many will seek surgical treatments to reduce their pain, but it will be a bit pricey. However, many individuals will opt for non-surgical treatments due to their affordability. Non-surgical treatments are cost-effective and customizable to a person’s pain and discomfort. From chiropractic care to acupuncture, depending on the severity of the person’s pain, many will find the relief they seek. One of the most innovative treatments for reducing spinal pain is spinal decompression. Spinal decompression allows the individual to be strapped into a traction table. This is because it gently pulls on the spine to realign the spinal disc by reducing the pressure on the spine to invoke the body’s natural healing process to relieve pain. (Ramos & Martin, 1994) Additionally, when many individuals are using spinal decompression, the gentle traction provides a motorized distraction to the spine that may induce physical changes to the spinal disc and help restore a person’s range of motion, flexibility, and mobility. (Amjad et al., 2022)
Spinal Decompression Restoring Spinal Disc Height
When a person is being strapped into the spinal decompression machine, the gentle traction helps the spinal disc return to the spine, allowing the fluids and nutrients to rehydrate the spine, increasing the spine’s disc height. This is because spinal decompression creates negative pressure on the spine, allowing the spinal disc to return to its original height and providing relief. Plus, the amazing thing that spinal decompression does is that it can be combined with physical therapy to help stretch and strengthen the surrounding muscles near the spine to provide more stability and flexibility. (Vanti et al., 2023) This allows the individual to be more mindful of their bodies and start incorporating small habit changes to reduce the pain from returning. When many people begin to think about their health and wellness by going to treatment, they will regain their quality of life and get back to their daily routine without the issues affecting their spine.
References
Amjad, F., Mohseni-Bandpei, M. A., Gilani, S. A., Ahmad, A., & Hanif, A. (2022). Effects of non-surgical decompression therapy in addition to routine physical therapy on pain, range of motion, endurance, functional disability and quality of life versus routine physical therapy alone in patients with lumbar radiculopathy; a randomized controlled trial. BMC Musculoskelet Disord, 23(1), 255. https://doi.org/10.1186/s12891-022-05196-x
Coppes, M. H., Marani, E., Thomeer, R. T., & Groen, G. J. (1997). Innervation of “painful” lumbar discs. Spine (Phila Pa 1976), 22(20), 2342-2349; discussion 2349-2350. https://doi.org/10.1097/00007632-199710150-00005
Ramos, G., & Martin, W. (1994). Effects of vertebral axial decompression on intradiscal pressure. J Neurosurg, 81(3), 350-353. https://doi.org/10.3171/jns.1994.81.3.0350
Roland, M. O. (1986). A critical review of the evidence for a pain-spasm-pain cycle in spinal disorders. Clin Biomech (Bristol, Avon), 1(2), 102-109. https://doi.org/10.1016/0268-0033(86)90085-9
Vanti, C., Saccardo, K., Panizzolo, A., Turone, L., Guccione, A. A., & Pillastrini, P. (2023). The effects of the addition of mechanical traction to physical therapy on low back pain? A systematic review with meta-analysis. Acta Orthop Traumatol Turc, 57(1), 3-16. https://doi.org/10.5152/j.aott.2023.21323
Zhang, Y. G., Guo, T. M., Guo, X., & Wu, S. X. (2009). Clinical diagnosis for discogenic low back pain. Int J Biol Sci, 5(7), 647-658. https://doi.org/10.7150/ijbs.5.647
Individuals experiencing shooting, aching pain in the lower extremities, and intermittent leg pain could be suffering from neurogenic claudication. Can knowing the symptoms help healthcare providers develop an effective treatment plan?
Neurogenic Claudication
Neurogenic claudication occurs when spinal nerves become compressed in the lumbar or lower spine, causing intermittent leg pain. Compressed nerves in the lumbar spine can cause leg pain and cramps. The pain usually worsens with specific movements or activities like sitting, standing, or bending backward. It is also known as pseudo-claudication when the space within the lumbar spine narrows. A condition known as lumbar spinal stenosis. However, neurogenic claudication is a syndrome or group of symptoms caused by a pinched spinal nerve, while spinal stenosis describes the narrowing of the spinal passages.
Symptoms
Neurogenic claudication symptoms can include:
Leg cramping.
Numbness, tingling, or burning sensations.
Leg fatigue and weakness.
A sensation of heaviness in the leg/s.
Sharp, shooting, or aching pain extending into the lower extremities, often in both legs.
There may also be pain in the lower back or buttocks.
Neurogenic claudication is different from other types of leg pain, as the pain alternates – ceasing and beginning randomly and worsens with specific movements or activities. Standing, walking, descending stairs, or flexing backward can trigger pain, while sitting, climbing stairs, or leaning forward tends to relieve pain. However, every case is different. Over time, neurogenic claudication can affect mobility as individuals try to avoid activities that cause pain, including exercise, lifting objects, and prolonged walking. In severe cases, neurogenic claudication can make sleeping difficult.
Neurogenic claudication and sciatica are not the same. Neurogenic claudication involves nerve compression in the central canal of the lumbar spine, causing pain in both legs. Sciatica involves compression of nerve roots exiting from the sides of the lumbar spine, causing pain in one leg. (Carlo Ammendolia, 2014)
Causes
With neurogenic claudication, compressed spinal nerves are the underlying cause of the leg pain. In many cases, lumber spinal stenosis – LSS is the cause of pinched nerve. There are two types of lumbar spinal stenosis.
Central stenosis is the main cause of neurogenic claudication. With this type, the central canal of the lumbar spine, which houses the spinal cord, narrows, causing pain in both legs.
Lumbar spinal stenosis can be acquired and develop later in life due to spine deterioration.
Congenital means the individual is born with the condition.
Both can lead to neurogenic claudication in different ways.
Foramen stenosis is another type of lumbar spinal stenosis that causes the narrowing of spaces on either side of the lumbar spine where nerve roots branch off the spinal cord. The associated pain is different in that it is either in the right or left leg.
The pain corresponds to the side of the spinal cord where the nerves are being pinched.
Acquired Lumbar Spinal Stenosis
Lumbar spinal stenosis is usually acquired due to the degeneration of the lumbar spine and tends to affect older adults. The causes of the narrowing can include:
Spinal trauma, such as from a vehicle collision, work, or sports injury.
Disc herniation.
Spinal osteoporosis – wear-and-tear arthritis.
Ankylosing spondylitis – a type of inflammatory arthritis that affects the spine.
Osteophytes – bone spurs.
Spinal tumors – non-cancerous and cancerous tumors.
Congenital Lumbar Spinal Stenosis
Congenital lumbar spinal stenosis means an individual is born with abnormalities of the spine that may not be apparent at birth. Because the space within the spinal canal is already narrow, the spinal cord is vulnerable to any changes as the individual ages. Even individuals with mild arthritis can experience symptoms of neurogenic claudication early on and develop symptoms in their 30s and 40s instead of their 60s and 70s.
Diagnosis
Diagnosis of neurogenic claudication is largely based on the individual’s medical history, physical examination, and imaging. The physical examination and review identify where the pain is presenting and when. The healthcare provider may ask:
Is there a history of lower back pain?
Is the pain in one leg or both?
Is the pain constant?
Does the pain come and go?
Does the pain get better or worse when standing or sitting?
Do movements or activities cause pain symptoms and sensations?
Are there any usual sensations while walking?
Treatment
Treatments can consist of physical therapy, spinal steroid injections, and pain meds. Surgery is a last resort when all other therapies are unable to provide effective relief.
Physical Therapy
A treatment plan will involve physical therapy that includes:
Daily stretching
Strengthening
Aerobic exercises
This will help improve and stabilize the lower back muscles and correct posture problems.
Occupational therapy will recommend activity modifications that cause pain symptoms.
This includes proper body mechanics, energy conservation, and recognizing pain signals.
Back braces or belts may also be recommended.
Spinal Steroid Injections
Healthcare providers may recommend epidural steroid injections.
This delivers a cortisone steroid to the outermost section of the spinal column or the epidural space.
Pain medications are used to treat intermittent neurogenic claudication. These include:
Over-the-counter analgesics like acetaminophen.
Nonsteroidal anti-inflammatory drugs or NSAIDs like ibuprofen or naproxen.
Prescription NSAIDs may be prescribed if needed.
NSAIDs are used with chronic neurogenic pain and should only be used when required.
The long-term use of NSAIDs can increase the risk of stomach ulcers, and the overuse of acetaminophen can lead to liver toxicity and liver failure.
Surgery
If conservative treatments are unable to provide effective relief and mobility and/or quality of life are affected, surgery known as a laminectomy may be recommended to decompress the lumbar spine. The procedure may be performed:
Laparoscopically – with small incisions, scopes, and surgical instrumentation.
Open surgery – with a scalpel and sutures.
During the procedure, facets of the vertebra are partially or completely removed.
To provide stability, the bones are sometimes fused with screws, plates, or rods.
Success rates for both are more or less the same.
Between 85% and 90% of individuals undergoing the surgery achieve long-lasting and/or permanent pain relief. (Xin-Long Ma et al., 2017)
Movement Medicine: Chiropractic Care
References
Ammendolia C. (2014). Degenerative lumbar spinal stenosis and its imposters: three case studies. The Journal of the Canadian Chiropractic Association, 58(3), 312–319.
Munakomi S, Foris LA, Varacallo M. (2024). Spinal Stenosis and Neurogenic Claudication. [Updated 2023 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430872/
Ma, X. L., Zhao, X. W., Ma, J. X., Li, F., Wang, Y., & Lu, B. (2017). Effectiveness of surgery versus conservative treatment for lumbar spinal stenosis: A system review and meta-analysis of randomized controlled trials. International journal of surgery (London, England), 44, 329–338. https://doi.org/10.1016/j.ijsu.2017.07.032
For individuals looking to improve their spinal health, can understanding the anatomy of the intervertebral foramen help in injury rehabilitation and prevention?
Intervertebral Foramen
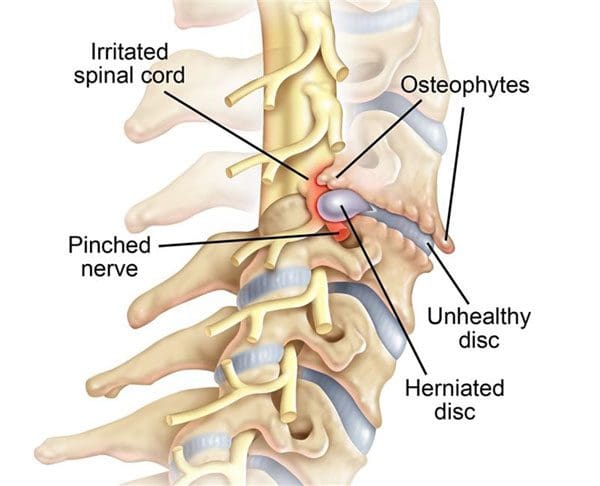
The intervertebral foramen, aka neural foramen, is the opening between the vertebrae through which spinal nerve roots connect and exit to other body areas. If the foramina narrows, it can place added pressure on the nerve roots near and around them, causing pain symptoms and sensations. This is known as neuroforaminal stenosis. (Sumihisa Orita et al., 2016)
Anatomy
The vertebrae comprise the spinal column.
They protect and support the spinal cord and most of the weight placed on the spine.
Foramen is the singular form, and foramina is the plural form.
Structure
The body is the large, round part of the bone that makes up each vertebra.
The body of each vertebra is attached to a bony ring.
Stenosis can occur in the spinal canal, known as central canal stenosis, and the foramina.
Pain brought on by neuroforaminal spinal stenosis and arthritis-related bone growth/bone spurs/osteophytes that are present in one or more foramen rub against the nerve root that passes through the space, causing radicular pain.
Pain accompanied by other sensations, like tingling or numbness, is known as radiculopathy. (Young Kook Choi, 2019)
The main symptom is pain.
Numbness and/or tingling can present depending on the injury.
Neurogenic claudication occurs as a result of ischemia or a lack of blood circulation to the nerves and typically presents with a heaviness in the legs.
It is typically associated with central stenosis rather than foraminal stenosis.
Most individuals with spinal stenosis feel better when flexing or bending forward and worse when arching their backs.
Stenosis treatment aims to relieve pain and prevent nerve symptoms from occurring or worsening. Conservative treatments are recommended and can be highly effective.
These include:
Myelopathy in the neck and/or upper or mid-back (myelopathy symptoms are spinal cord related and occur in central canal stenosis) (Cleveland Clinic. 2021)
Intense incapacitating pain
Different surgical techniques include:
Decompression laminectomy – entails removing the buildup of bone in the spinal canal.
Spinal fusion – when there is instability of the spine or severe foraminal stenosis.
Orita, S., Inage, K., Eguchi, Y., Kubota, G., Aoki, Y., Nakamura, J., Matsuura, Y., Furuya, T., Koda, M., & Ohtori, S. (2016). Lumbar foraminal stenosis, the hidden stenosis including at L5/S1. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie, 26(7), 685–693. https://doi.org/10.1007/s00590-016-1806-7
American Academy of Orthopaedic Surgeons. (2020). Spine Basics (OrthoInfo, Issue. https://orthoinfo.aaos.org/en/diseases–conditions/spine-basics/
American Academy of Orthopaedic Surgeons. (2021). Lumbar spinal stenosis (OrthoInfo, Issue. https://orthoinfo.aaos.org/en/diseases–conditions/lumbar-spinal-stenosis/
Choi Y. K. (2019). Lumbar foraminal neuropathy: an update on non-surgical management. The Korean journal of pain, 32(3), 147–159. https://doi.org/10.3344/kjp.2019.32.3.147
Lee, S. Y., Kim, T. H., Oh, J. K., Lee, S. J., & Park, M. S. (2015). Lumbar Stenosis: A Recent Update by Review of Literature. Asian spine journal, 9(5), 818–828. https://doi.org/10.4184/asj.2015.9.5.818
Lurie, J., & Tomkins-Lane, C. (2016). Management of lumbar spinal stenosis. BMJ (Clinical research ed.), 352, h6234. https://doi.org/10.1136/bmj.h6234
For individuals suffering from back pain, can knowing basic chiropractic terminology help in understanding diagnosis and treatment plan development?
Chiropractic Terminology
The chiropractic principle is that a properly aligned spine positively affects an individual’s overall health. One of the main aspects of chiropractic care is applying calculated force to the spinal joints to restore correct spinal alignment. Chiropractic terminology describes specific types of techniques and care.
General Subluxation
A subluxation can mean different things for various doctors. In general, a subluxation is a significant structural displacement or an incomplete or partial dislocation of a joint or organ.
To medical doctors, a subluxation refers to a partial dislocation of a vertebrae.
This is a serious condition, usually brought on by trauma, that can result in a spinal cord injury, paralysis, and/or death.
X-rays show a conventional subluxation as an obvious disconnect between the vertebrae.
Chiropractic Subluxation
The chiropractic interpretation is more subtle and refers to the misalignment of adjacent spinal vertebrae.
Subluxation in this context refers to position changes in the joints and soft tissues of the spine.
Vertebral misalignment is believed to lead to pain and abnormal intervertebral joint motion.
This difference between the serious subluxation medical condition and the chiropractic version may cause individuals to dismiss seeking back pain treatments.
Motion Segment
Chiropractors and surgeons use it as a technical term.
Motion segment refers to two adjacent vertebrae and the intervertebral disc between them.
This is the area chiropractors assess and adjust.
Adjustment
The chiropractor performs a spinal manual adjustment to realign joint subluxations.
Adjustments involve applying force to motion segments to bring them back into a centered alignment.
The goal for adjustments and realigning the vertebrae includes:
Spinal manipulation is a technique used by chiropractors to provide relief for musculoskeletal pain related to the back and neck. Manipulation provides mild to moderate relief and works as well as some conventional treatments like pain-relieving medications. (Sidney M. Rubinstein et al., 2012)
Spinal manipulation is divided into grades of mobilization.
Depending on their training, practitioners of various medical disciplines may be licensed to perform grade 1 to grade 4 mobilizations.
Only physical therapists, osteopathic physicians, and chiropractors are licensed to perform grade 5 mobilizations, which are high-velocity thrust techniques.
Most massage therapists, athletic trainers, and personal trainers are not licensed to perform spinal manipulations.
Based on a systematic review, the effectiveness of these treatments found that there is quality evidence that manipulation and mobilization can help reduce pain and improve function for individuals with chronic low back pain, with manipulation appearing to produce a more profound effect than mobilization. Both therapies are safe, with multimodal treatments potentially being an effective option. (Ian D. Coulter et al., 2018)
As with any treatment, results vary from person to person and with different chiropractors. There are also potential risks with spinal manipulation. Though rare, cervical, carotid, and vertebral artery dissections have occurred with cervical/neck manipulation. (Kelly A. Kennell et al., 2017) Individuals with osteoporosis may be advised to avoid chiropractic adjustments or manipulation because of the increased risk of injury. (James M. Whedon et al., 2015)
Many individuals choose chiropractic treatment for a variety of conditions. Understanding chiropractic terminology and reasoning allows individuals to ask questions as they discuss their symptoms to develop a personalized treatment plan and restore function and wellness.
What Causes Disc Herniation?
References
Henderson C. N. (2012). The basis for spinal manipulation: chiropractic perspective of indications and theory. Journal of electromyography and kinesiology : official journal of the International Society of Electrophysiological Kinesiology, 22(5), 632–642. https://doi.org/10.1016/j.jelekin.2012.03.008
Blanchette, M. A., Stochkendahl, M. J., Borges Da Silva, R., Boruff, J., Harrison, P., & Bussières, A. (2016). Effectiveness and Economic Evaluation of Chiropractic Care for the Treatment of Low Back Pain: A Systematic Review of Pragmatic Studies. PloS one, 11(8), e0160037. https://doi.org/10.1371/journal.pone.0160037
Rubinstein, S. M., Terwee, C. B., Assendelft, W. J., de Boer, M. R., & van Tulder, M. W. (2012). Spinal manipulative therapy for acute low-back pain. The Cochrane database of systematic reviews, 2012(9), CD008880. https://doi.org/10.1002/14651858.CD008880.pub2
Coulter, I. D., Crawford, C., Hurwitz, E. L., Vernon, H., Khorsan, R., Suttorp Booth, M., & Herman, P. M. (2018). Manipulation and mobilization for treating chronic low back pain: a systematic review and meta-analysis. The spine journal : official journal of the North American Spine Society, 18(5), 866–879. https://doi.org/10.1016/j.spinee.2018.01.013
Kennell, K. A., Daghfal, M. M., Patel, S. G., DeSanto, J. R., Waterman, G. S., & Bertino, R. E. (2017). Cervical artery dissection related to chiropractic manipulation: One institution’s experience. The Journal of family practice, 66(9), 556–562.
Whedon, J. M., Mackenzie, T. A., Phillips, R. B., & Lurie, J. D. (2015). Risk of traumatic injury associated with chiropractic spinal manipulation in Medicare Part B beneficiaries aged 66 to 99 years. Spine, 40(4), 264–270. https://doi.org/10.1097/BRS.0000000000000725
For individuals trying to maintain a healthy spine, can understanding the causes and prevention of rotated vertebrae help protect the spine from harmful rotation of vertebrae?
Spinal Rotation
Healthy spine rotation is an important aspect of injury prevention, and rotated vertebrae or a twisted spine can result from spine, nerve, or muscle disease or certain movements.
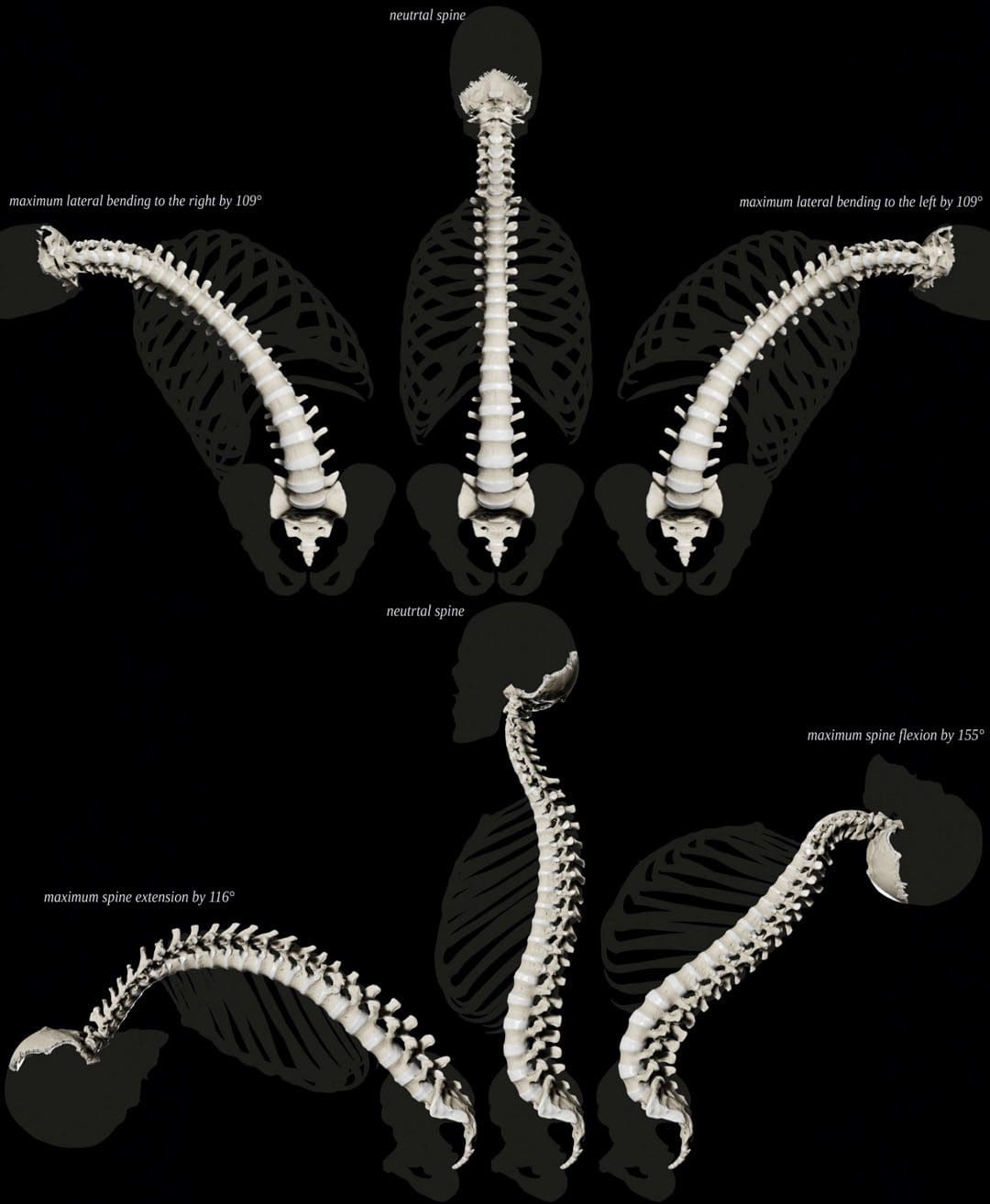
Normal Spine Twisting Capability
The spine can move in several ways. Spine movements include:
Bending – Rounding forward
Extending – Arching backward
Tilting sideways is powered by muscles that aid in twisting.
Although the spine can move in many directions, there are limits to how far it can and should go. (Xinhai Shan et al., 2013). This is especially true with twisting. The spinal column is made of 26 interconnected bones called vertebrae. When moving, each vertebrae bone moves accordingly. Rotated or twisted vertebrae, especially when bending forward like lifting heavy objects, are associated with a risk of back injuries like strain and herniated discs.
How Rotation Works
Rotation is a basic movement in which individuals can turn their spinal column. When twisting, the spine also bends to the side. The muscles involved in spine rotation include:
The internal oblique abdominals and the external oblique abdominals don’t directly attach to the spine but are the primary muscles responsible for powering spinal rotation in the lower back.
Intrinsic muscles, including the multifidus and longissimus, contribute to twisting movement as well.
The multifidus helps the spine twist when one side is contracted/activated and extends the lumbar spine when both sides contract.
The multifidus helps control the movement, and the longissimus provides the movement with some extension.
Age and The Spine
As individuals age, the body accumulates tension and/or weakness in the oblique abdominal and other trunk muscles. Sedentary habits primarily bring on these changes. (Pooriput Waongenngarm et al., 2016)
Chronically tight back and abdominal muscles impair the range of motion of the trunk, as well as twisting ability.
Muscle weakness and tightness affect spinal movements.
Weakened muscles can decrease support for spinal movement and decrease overall trunk stability.
Spinal Rotation and Scoliosis
Scoliosis is a common condition that causes a lateral curve of the spine. Some of the vertebrae become displaced to the side. Often, abnormal vertebral rotation underlies this displacement. Treatment often focuses on controlling vertebral rotation with medical guidance and physical therapy. (John P. Horne et al., 2014)
Over-Rotating The Spine
Many individuals over-rotate their spines with manual work, which can increase the risk of back injuries. (National Institutes of Health. 2020). Over-rotation can happen with activities like digging or shoveling.
Exercise For A Healthy Spine
A recommended way to achieve optimal rotation of the spine is with daily back exercises. (National Spine Health Foundation. 2015). An effective back exercise program will consist of movements in every direction.
Yoga is recommended because it places emphasis on developing flexibility and strength in all directions.
Pilates does the same.
An injury prevention exercise program will work the hip and pelvic muscles as well.
Individuals with a spine condition should consult their healthcare provider or physical therapist about how to exercise the spine safely, as rotation exercises could worsen back problems like bulging or herniated discs.
Core Strength For A Pain-Free Back
References
Shan, X., Ning, X., Chen, Z., Ding, M., Shi, W., & Yang, S. (2013). Low back pain development response to sustained trunk axial twisting. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 22(9), 1972–1978. https://doi.org/10.1007/s00586-013-2784-7
Waongenngarm, P., Rajaratnam, B. S., & Janwantanakul, P. (2016). Internal Oblique and Transversus Abdominis Muscle Fatigue Induced by Slumped Sitting Posture after 1 Hour of Sitting in Office Workers. Safety and health at work, 7(1), 49–54. https://doi.org/10.1016/j.shaw.2015.08.001
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine