Can incorporating explosive strength training help develop power for athletes and sports enthusiasts who need to generate maximum energy quickly?
Explosive Training
Explosive strength training exercises help develop power and athletic abilities by challenging the nervous and muscular systems. The focus is on the number of sets, repetitions, and rest periods to maximize gains. Explosive exercises typically use fewer repetitions 3–6 and more sets 3–5 to allow for maximum power output. Adequate rest periods, 2–3 minutes, are allotted between sets to prevent fatigue and reduce the risk of injury. Explosive training combines strength and speed to increase an individual’s power output and can be helpful for various sports, including track and field, court sports, cycling, and football.
Exercises
Explosive strength training uses large muscle movements that can include:
Squats
Power cleans
Weighted or unweighted vertical jumps
Heavy ball throws
Hill sprinting
Smaller muscle exercises can also build power, but results may be limited. These can include:
Bench presses
Pushups
Sample Exercises
Training exercises to develop power include:
Sprints
Agility drills
Weighted step ups
Overhead walking lunges
Plyometrics
Squats
Explosive training exercises should be selected to match individual fitness and sports goals. Exercise choices should simulate the movement patterns specific to the sport. Explosive training is unlikely to lead to injury if you train slowly, listen to your body for signs and symptoms of injury, and work with a qualified professional. Some evidence suggests that regularly engaging in explosive strength training can decrease the risk of injury.
Explosive strength exercises are movements that require an athlete to produce maximum or near-maximum output in a short time.
Explosive training aims to build enough power to ultimately move heavy weights quickly.
It is recommended to start with light weights and use slow, controlled movements.
The amount of weight used during a workout and the speed at which they are lifted should be increased over several weeks and training sessions.
Benefits
Research supports that explosive speed and strength exercise builds power but is more effective when combined with other training. For example, in a study, researchers showed that a mixed maximal and explosive strength training program was more effective than traditional approaches like circuit training in increasing overall fitness and adaptive processes that are helpful when increasing training loads, such as runners training for a marathon. (Taipale, R. S. et al., 2014) Other reports suggest that to maximize strength, power, and speed, a combination of heavy and light explosive exercise provides optimal results compared to training only in one style. (Baker D. 2003) The first training phase should focus on increasing maximum strength and building a solid foundation to maximize power output or movement speed. The second phase is devoted to power and speed training. (DeWeese B. H. et al., 2015)
Programs
The first five weeks of a 12-week training program to increase power and speed may consist primarily of heavy strength training. The next six weeks would consist of heavy and high-power explosive exercise training, and the final week would be high-power movements. Individuals are recommended to work with a coach or personal trainer specializing in this type of training when developing a program. A qualified professional can choose sport-specific exercises that will help improve performance. Correct form is essential for safety. A professional trainer can observe alignment throughout each exercise and provide adjustments and tips for safety and efficiency.
Injury Medical Chiropractic
At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you and strive to create fitness and better the body through research methods and total wellness programs. These programs use the body’s ability to achieve improvement goals, and athletes can condition themselves to excel in their sport through proper fitness and nutrition. Our providers use an integrated approach to create personalized programs, often including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles.
Chiropractic Sport Rehabilitation
References
Taipale, R. S., Mikkola, J., Salo, T., Hokka, L., Vesterinen, V., Kraemer, W. J., Nummela, A., & Häkkinen, K. (2014). Mixed maximal and explosive strength training in recreational endurance runners. Journal of strength and conditioning research, 28(3), 689–699. https://doi.org/10.1519/JSC.0b013e3182a16d73
Baker D. (2003). Acute effect of alternating heavy and light resistances on power output during upper-body complex power training. Journal of strength and conditioning research, 17(3), 493–497. https://doi.org/10.1519/1533-4287(2003)017<0493:aeoaha>2.0.co;2
DeWeese, B. H., Hornsby, G., Stone, M., & Stone, M. H. (2015). The training process: Planning for strength–power training in track and field. Part 2: Practical and applied aspects. Journal of Sport and Health Science, 4(4), 318–324. doi:10.1016/j.jshs.2015.07.002
Individuals who engage in sports and physical activities that involve lunging forward while running or jumping can sustain a plantaris muscle injury. Can understanding the anatomy of the back of the leg and the symptoms help diagnose and treat plantar muscle injuries?
Plantaris Muscle
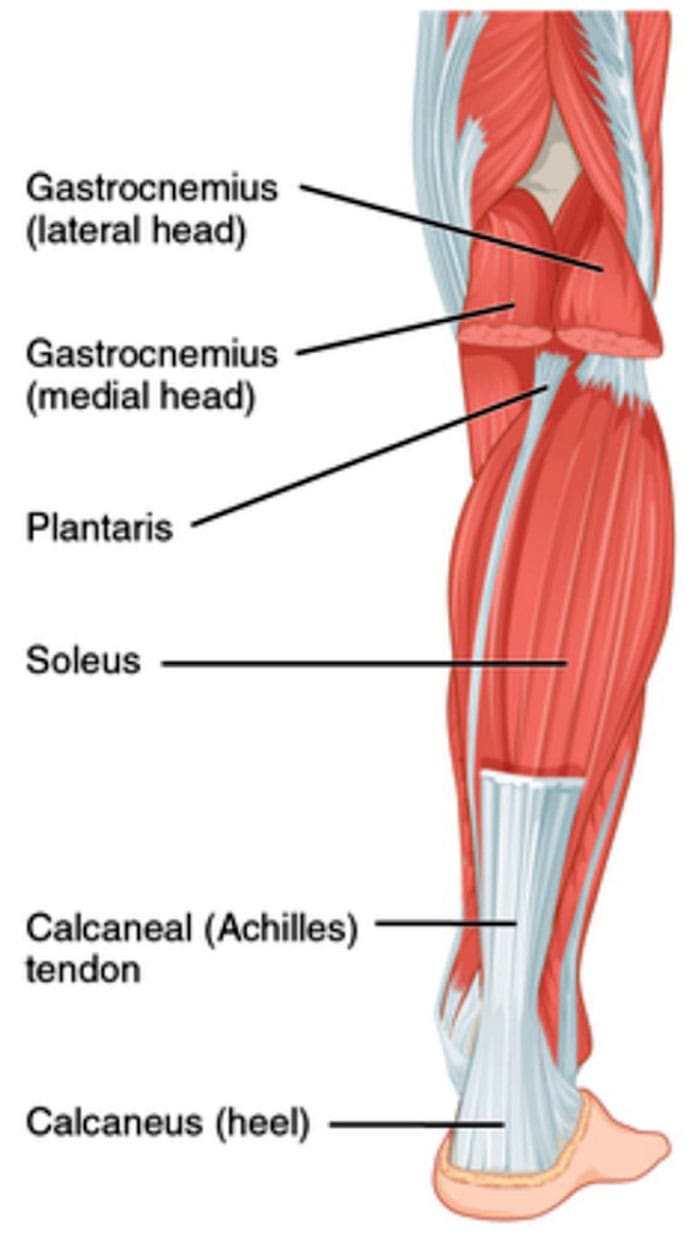
The plantaris muscle is a long, narrow muscle in the calf that runs along the back of the leg. It’s part of the Triceps Surae, a group of muscles in the calf that, along with the gastrocnemius and soleus muscles, makes up the bulk of the back of the leg. It is located in the superficial posterior compartment of the leg. Strains or tears of the plantaris muscle at the back of the leg can cause pain and swelling, similar to a calf strain or Achilles tendon tear. Individuals may feel immediate pain, cramping, and other symptoms.
Anatomy
The gastrocnemius and soleus muscles are the major muscles, with the soleus located deeper in the leg. Together, they form the Achilles tendon, which blends into a tendon in the back of the heel and attaches to the heel bone/calcaneus. When the calf muscles contract, they point the foot downward, propelling the body forward when walking, running, and sprinting. The plantaris muscle and tendon sit more or less in the center of the calf, between the two heads of the gastrocnemius. Around 7% to 20% of the population are born without plantaris muscles. There are variations, such as having a double- or triple-headed plantaris muscle. (Olewnik Ł. et al., 2020) However, individuals that do not have the muscle or have a variation have not been shown to affect long-term or short-term mobility.
Symptoms
Plantaris muscle ruptures are the most common injury and occur often during running or jumping. (Spang C. et al., 2016) Many who sustain this injury are athletes who have to lunge forward. Common symptoms include:
Swelling and bruising in the back of the calf area.
Cramping in the calf muscle.
Spasm sensations of the calf muscle.
Symptoms of a plantaris muscle strain are less severe, with the common signs being tightness and pain during and after physical activity.
Diagnosis
Plantaris muscle tears differ from Achilles tendon tears because the foot can be pointed downward following the rupture, whereas an Achilles tear cannot. Plantaris ruptures can also be confused with a blood clot in the large veins of the calf, called deep vein thrombosis/DVT. (Rohilla S. et al., 2013) Tests like MRI or ultrasound can be performed to confirm or exclude a plantaris rupture. Both can be useful for verifying whether the injury is a strain or tear and identifying other possible causes of calf pain.
Treatment
Treatment is typically non-surgical. While the injuries can cause pain and disability, the symptoms almost always resolve with conservative treatments and therapies. Rest, ice, compression, and elevation are the first line used and may be all that is needed for a muscle strain. Short-term use of NSAIDs may be recommended for a strain or tear to reduce pain and inflammation. (Morelli K. M. et al., 2018) If the pain is profound or there is a tear, patients may require short-term immobilization or the use of a crutch for the pain to subside. With the assistance of a physical therapist, sports chiropractor, and athletic trainer, gradual increases in mobility and strength can be obtained. Symptoms usually gradually resolve over several weeks. Full recovery may take up to eight weeks, depending on the severity of the injury.
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop customized treatment programs through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility, relieving pain, and helping individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Control Foot Motion with Custom Orthotics
References
Olewnik, Ł., Zielinska, N., Karauda, P., Tubbs, R. S., & Polguj, M. (2020). A three-headed plantaris muscle: evidence that the plantaris is not a vestigial muscle?. Surgical and radiologic anatomy : SRA, 42(10), 1189–1193. https://doi.org/10.1007/s00276-020-02478-8
Spang, C., Alfredson, H., Docking, S. I., Masci, L., & Andersson, G. (2016). The plantaris tendon: a narrative review focusing on anatomical features and clinical importance. The bone & joint journal, 98-B(10), 1312–1319. https://doi.org/10.1302/0301-620X.98B10.37939
Rohilla, S., Jain, N., & Yadav, R. (2013). Plantaris rupture: why is it important?. BMJ case reports, 2013, bcr2012007840. https://doi.org/10.1136/bcr-2012-007840
Morelli, K. M., Brown, L. B., & Warren, G. L. (2018). Effect of NSAIDs on Recovery From Acute Skeletal Muscle Injury: A Systematic Review and Meta-analysis. The American journal of sports medicine, 46(1), 224–233. https://doi.org/10.1177/0363546517697957
Individuals who have sustained trauma to the knee area from work, physical activity, or a motor vehicle collision can experience significant pain and mobility impairment. Can physical therapy help heal and strengthen the PLC?
Posterolateral Corner Knee Injury
The posterolateral corner, or PLC, comprises muscles, tendons, and ligaments in the back of the knee that help support and stabilize the outside region. The primary role of the PLC is to prevent the knee from excessive amounts of rotation or bowing/turning outward. (Chahla J. et al., 2016) Posterolateral corner injuries can cause significant pain and can dramatically impact an individual’s ability to walk, work, or maintain independence. Treatment options will depend on the severity of the injury.
The Posterolateral Corner
The posterolateral corner comprises multiple structures that support and stabilize the outside of the knee. The structures are subdivided into primary and secondary stabilizers. The primary group includes:
The primary role is to prevent the knee from excessively turning outward, so the grouping provides secondary assistance in preventing the lower leg bone/tibia from shifting forward or backward on the thighbone/femur. Occasionally, one or several posterolateral corner structures can be sprained, strained, or torn.
How Injury Occurs
An injury occurs when a direct blow to the inner portion of the front of the knee causes the leg to bow outward. A posterolateral corner injury may also be sustained without contact, for example, if the knee hyperextends or buckles away from the other leg into a varus/bow leg position. Because the knee usually moves during a PLC, concurrent sprains or tears to the anterior cruciate ligament/ACL or posterior cruciate ligament/PCL are also common. (Chahla J. et al., 2016) Other situations that can also cause PLC injuries include automobile crashes and falls from elevated surfaces. (Shon O. J. et al., 2017) When this type of trauma causes a posterolateral corner injury, bone fractures are also common.
Symptoms
Depending on the severity of the injury, multiple symptoms may be present, including:
For individuals who suspect that they have sustained a PLC injury or have any of the symptoms listed, it is critical to be seen by an orthopedic specialist or emergency room physician. A healthcare provider will properly evaluate the leg and develop the appropriate treatment.
Diagnosis
Diagnosis begins with a comprehensive examination. In addition to looking for the symptoms noted, a healthcare provider will move the legs in different directions to assess for any instability. The dial test may be performed, which involves having the patient lie on their stomach while the healthcare professional assesses the side-to-side rotation in the leg to check for excessive motion. (Shon O. J. et al., 2017) Imaging is frequently ordered to determine which anatomical structures are affected more accurately. X-rays can help rule out concurrent fractures and check for excessive laxity in the knee area. MRIs are also useful for visualizing the various tendons and ligaments, helping the healthcare provider look closely at any sprains or tears that may have occurred. However, MRIs may be less accurate in diagnosing PLC injuries after 12 weeks, so they should be obtained as soon as possible. Based on this evaluation, the injury may be classified using the following system (Shon O. J. et al., 2017)
Grade 1
0 to 5 degrees of rotational or varus/bowing instability.
Incompletely torn posterolateral corner.
Grade 2
6 to 10 degrees of rotational or varus/bowing instability.
Incompletely torn posterolateral corner.
Grade 3
Eleven or more degrees of rotational or varus/bowing instability.
Completely torn posterolateral corner.
Treatment
The care received after a posterolateral corner injury can vary depending on the structures involved and the overall severity.
Nonsurgical
Nonsurgical treatment is typically reserved for isolated grade 1 or 2 PLC injuries. (Shon O. J. et al., 2017) Depending on which structures are affected, a stabilizing brace may be worn, and crutches are often needed to decrease the strain on the knee. Physical therapy is also commonly prescribed and focuses on the following goals:
Gradually reintroducing specific movements like running and jumping.
Surgery
Non-surgical treatment tends not to work with grade 3 injuries. If surgery is not performed, individuals may also suffer from chronic knee instability or develop long-term osteoarthritis. (Chahla J. et al., 2019) Surgical treatment is often recommended for grade 3 injuries. The damaged primary stabilizers are surgically reconstructed using a graft from another body region. Surgical repairs may also be performed on any secondary stabilizers to improve stability. (Chahla J. et al., 2019) Any other ligament injuries, such as ACL, PCL, or concurrent fractures, will also be addressed. Following the procedure, individuals immobilize their knee with a brace and do not place weight on the affected leg to protect the surgical area. Depending on the surgeon’s recommendations, this can last six weeks or more. Physical therapy is also initiated after a surgical procedure. Though rehabilitation progresses slowly, the goals are often the same as when treating milder PLC injuries. Returning to work, sports, and/or physical activity after surgery may take six months of therapy or more. (Shon O. J. et al., 2017)
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized treatment program through an integrated approach to treat injuries and chronic pain syndromes, improve flexibility, mobility, and agility, relieve pain, and help individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Knee Injury Rehabilitation
References
Chahla, J., Moatshe, G., Dean, C. S., & LaPrade, R. F. (2016). Posterolateral Corner of the Knee: Current Concepts. The archives of bone and joint surgery, 4(2), 97–103.
Shon, O. J., Park, J. W., & Kim, B. J. (2017). Current Concepts of Posterolateral Corner Injuries of the Knee. Knee surgery & related research, 29(4), 256–268. https://doi.org/10.5792/ksrr.16.029
Chahla, J., Murray, I. R., Robinson, J., Lagae, K., Margheritini, F., Fritsch, B., Leyes, M., Barenius, B., Pujol, N., Engebretsen, L., Lind, M., Cohen, M., Maestu, R., Getgood, A., Ferrer, G., Villascusa, S., Uchida, S., Levy, B. A., Von Bormann, R., Brown, C., … Gelber, P. E. (2019). Posterolateral corner of the knee: an expert consensus statement on diagnosis, classification, treatment, and rehabilitation. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA, 27(8), 2520–2529. https://doi.org/10.1007/s00167-018-5260-4
For individuals experiencing piriformis syndrome. Can knowing the causes and what it feels like help in diagnosis and treatment?
Managing Piriformis Syndrome
Piriformis syndrome is where spasms occur in the piriformis muscle located in the buttocks. These muscle spasms can cause pain and numbness in the buttocks and the back of the leg. (Cedars Sinai, 2022)
What Is It?
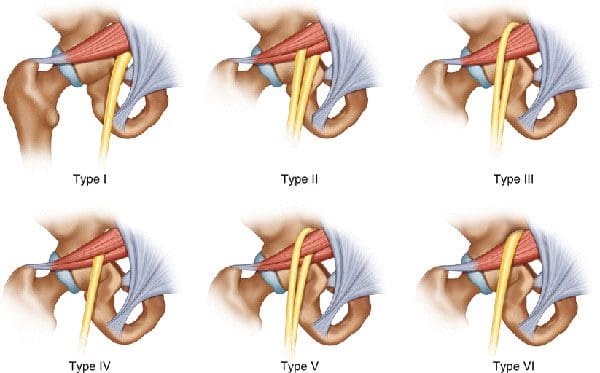
Piriformis syndrome is an irritation of the sciatic nerve from the piriformis muscle. Although the piriformis muscle is small compared to other muscles around the hip and thigh, it supports the hip joint’s external rotation or turning out. The sciatic nerve supplies the lower extremities with motor and sensory functions. The piriformis tendon and sciatic nerve cross each other behind the hip joint in the deep buttock. Both are about one centimeter in diameter. The piriformis muscle spasms can irritate the sciatic nerve, causing sciatica symptoms. (Cedars Sinai, 2022)
Triggers
A piriformis syndrome diagnosis means the piriformis tendon binds or spasms around the sciatic nerve, causing irritation and symptoms. Many doctors and specialists support the theory that when the piriformis muscle and its tendon tighten, this can cause compression and pinch the nerve. This can decrease blood circulation and irritate the nerve due to pressure. (Cass S. P. 2015) Many doctors also believe that piriformis syndrome occurs from anatomic variation of the muscle and tendon. It is thought this muscle-tendon variation irritates the nerve in some, leading to sciatica symptoms.
How It Feels
Common signs and symptoms experienced include (Cass S. P. 2015)
Pain in the buttocks.
Pain behind the hip.
Electric shock pains traveling down the back of the lower extremity.
Numbness in the lower extremity.
Tenderness with pressure that often causes pain when sitting.
Some develop symptoms abruptly, while others gradually increase in symptoms in the back of their thighs.
Most who are diagnosed with piriformis syndrome are generally active individuals who experience increasing difficulty with certain types of physical activity.
Testing
There are no specific tests that accurately diagnose piriformis syndrome. Doctors will order tests, including MRI and nerve conduction studies. Because it can be difficult to diagnose, there are likely many misdiagnosis cases. This means that some with the condition don’t have a piriformis diagnosis. In addition, some with vague hip pain may receive this diagnosis even if they don’t have the condition. (Cass S. P. 2015) An injection is often administered into the piriformis muscle when the diagnosis is uncertain. (Jankovic D. et al., 2013) Performing an injection can help determine the specific location of the discomfort. When an injection is given into the piriformis muscle or tendon, it is administered by ultrasound guidance to ensure the needle delivers medication to the correct location. (Bardowski E. A., and Byrd J. W. T. 2019)
Differential Diagnosis
Some other conditions with buttock pain can have similar symptoms. Other causes can include:
Radiculopathy/Sciatica
Herniated discs
Hip bursitis
Spinal stenosis
The diagnosis of piriformis syndrome is given when these diagnoses are eliminated as possible causes of pain.
Treatment
Managing piriformis syndrome is quite general, and it is often difficult to recover from. Common treatment and management suggestions include the following. (Jankovic D. et al., 2013)
Rest
Avoiding activities that cause symptoms for at least a few weeks.
Physical Therapy
Focuses on stretching and strengthening the hip rotator muscles.
Anti-inflammatory Medication
To decrease inflammation around the tendon.
Deep Massage
Used to relax the piriformis muscle and help release the compressed nerve.
Cortisone Injections
It can help decrease inflammation and swelling.
Botulinum Toxin Injection
It can paralyze the piriformis muscle to reduce pain and discomfort.
In severe cases, surgery can be performed to loosen the piriformis tendon, known as a piriformis release (Cass S. P. 2015). This surgical procedure is recommended when conservative treatments have been tried for at least six months and other causes of pain have been evaluated and ruled out. Recovery takes several months.
The goal of managing piriformis syndrome is to improve the range of motion and flexibility around the hip and diminish inflammation around the sciatic nerve. Working with a professional chiropractic team can help relieve pain, return individuals to normal function, and expedite healing. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a customized treatment program through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Piriformis Syndrome Treatment Chiropractor
References
Cedars Sinai. Sinai, C. (2022). Piriformis syndrome. https://www.cedars-sinai.org/health-library/diseases-and-conditions/p/piriformis-syndrome.html
Cass S. P. (2015). Piriformis syndrome: a cause of nondiscogenic sciatica. Current sports medicine reports, 14(1), 41–44. https://doi.org/10.1249/JSR.0000000000000110
Jankovic, D., Peng, P., & van Zundert, A. (2013). Brief review: piriformis syndrome: etiology, diagnosis, and management. Canadian journal of anaesthesia = Journal canadien d’anesthesie, 60(10), 1003–1012. https://doi.org/10.1007/s12630-013-0009-5
Bardowski, E. A., & Byrd, J. W. T. (2019). Piriformis Injection: An Ultrasound-Guided Technique. Arthroscopy techniques, 8(12), e1457–e1461. https://doi.org/10.1016/j.eats.2019.07.033
An annular fissure is caused by age-related changes to the spine, which often do not cause symptoms but can cause back pain. Can understanding the causes help individuals manage lower back pain and help healthcare providers develop an effective treatment program?
Annular Fissure
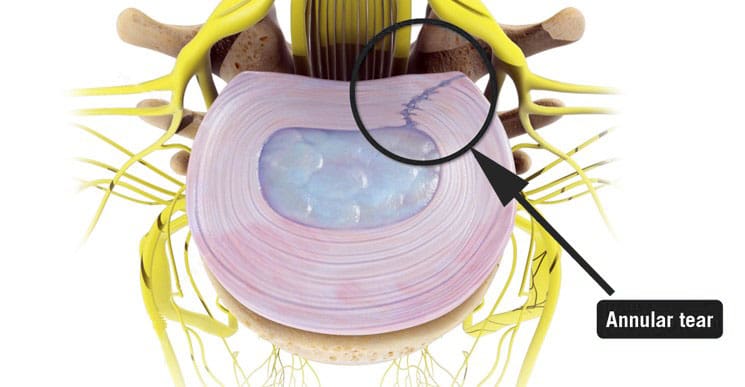
An annular fissure is a discogenic condition that affects the spine and can cause lower back pain. Also called an annular tear, it’s usually a wear-and-tear condition that happens over time rather than a condition caused by trauma. It usually happens when the fibers that make up the annulus or the tough outer covering of the intervertebral disc break or separate. To manage it, healthcare providers may recommend:
Making lifestyle changes.
Staying aware of how you go about daily activities and take steps to make adjustments, such as being mindful of unhealthy posture.
Start doing exercises that help make the back stronger.
Medical care if pain and other symptoms need to be managed.
Symptoms
Lower back pain may be a sign of an annular fissure, or there may be no symptoms. Symptoms can include:
Pain
Weakness
Numbness
Electrical sensations travel down one leg or arm if a cervical/neck tear is present.
Numbness and weakness may be caused by the nerves getting irritated or compressed near an annular tear. (Stadnik, T. W. et al., 1998)
These symptoms can also be similar to a herniated disc, which can be a complication of an annular fissure.
However, studies have shown that annular tears and herniated discs often go unnoticed because they have few obvious symptoms. (Jarvik, J. G. et al., 2005)
Annulus Function
The annulus comprises several layers of tough fibers/fibrocartilage that surround, contain, and protect the soft, liquid nucleus inside the disc. The layers of the annulus fibrosus crisscross to provide support. The nucleus is a shock absorber cushions the body’s weight on the spinal joints when sitting, standing, or moving. Its strength also allows the disc to buffer the jolts and jars it experiences. It also helps maintain the integrity of the intervertebral joint by supporting the space between the two vertebrae. When an annular fissure occurs, the fibers separate or tear off from insertion on the nearby spinal bone. A fissure can also be a break in the fibers of one or more layers. (Jarvik, J. G. et al., 2005)
Causes
An annular tear is not the standard term medical professionals use to describe or diagnose a fissure because the word tear suggests that trauma has led to the separation or break in the fibers. While an injury can cause an annular fissure, it’s usually caused by long-term wear and tear. (Guterl, C. C. et al., 2013) The tears are typically caused by age-related degenerative changes in the disc, which can also lead to degeneration in other areas of the spine. Wear and tear are caused by annular fissures due to an individual’s daily living habits, such as sitting, standing, walking, climbing stairs, and performing other routine movements.
Treatment
While a large annular fissure is not likely to improve without treatment, a small one could heal independently. However, once an area has torn, it becomes more likely to continue tearing. (Virginia Spine Institute, N.D.) Conservative treatment is usually enough to control pain and symptoms. Physical therapy and anti-inflammatory medication are the first line of treatment. (Cheng, J. et al., 2019) Medication can be over-the-counter or prescription. Physical therapy treatment includes exercises, traction, and other therapies. If these do not help with the symptoms, the provider may suggest a steroid injection to reduce inflammation and pain. It can take three to six months to recover from degenerative disc problems if doing a standard treatment plan that includes rest, low-impact therapy exercises, and anti-inflammatory treatments. (Cheng, J. et al., 2019)
In severe cases, surgery may be recommended, including disc replacement surgery. An annular tear is not a reason to have disc replacement surgery alone; it is only when there are degenerative changes in the vertebral disc that surgery might be necessary. (Yue, J. J. et al., 2012)
Improving Body Alignment
Not paying attention and being aware of how the body performs everyday activities can, over time, set the stage for an annular fissure and other musculoskeletal injuries. However, fixing daily movement and posture habits to prevent injuries can be done through simple adjustments. For example, strengthening the core and back muscles can reduce pressure on the spine and help prevent injuries. (Camp, C. L. et al., 2016) The idea is to improve joint and overall body alignment. Activities can include:
Strength training
Walking
Pilates classes
Yoga
Tai chi
Somatic exercises
These activities help with muscle balance and joint alignment, which are recommended prevention strategies that physical therapists use when working with individuals who need help with spinal problems.
Visiting a chiropractic and physical therapy team can help treat injuries and chronic pain syndromes, relieve pain, resolve musculoskeletal issues, and prevent future symptoms. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized care program for each patient through an integrated approach to treating injuries, improving flexibility, mobility, and agility to help return to normal and optimal function. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Back Pain Specialist
References
Stadnik, T. W., Lee, R. R., Coen, H. L., Neirynck, E. C., Buisseret, T. S., & Osteaux, M. J. (1998). Annular tears and disk herniation: prevalence and contrast enhancement on MR images in the absence of low back pain or sciatica. Radiology, 206(1), 49–55. https://doi.org/10.1148/radiology.206.1.9423651
Jarvik, J. G., Hollingworth, W., Heagerty, P. J., Haynor, D. R., Boyko, E. J., & Deyo, R. A. (2005). Three-year incidence of low back pain in an initially asymptomatic cohort: clinical and imaging risk factors. Spine, 30(13), 1541–1549. https://doi.org/10.1097/01.brs.0000167536.60002.87
Guterl, C. C., See, E. Y., Blanquer, S. B., Pandit, A., Ferguson, S. J., Benneker, L. M., Grijpma, D. W., Sakai, D., Eglin, D., Alini, M., Iatridis, J. C., & Grad, S. (2013). Challenges and strategies in the repair of ruptured annulus fibrosus. European cells & materials, 25, 1–21. https://doi.org/10.22203/ecm.v025a01
Virginia Spine Institute. (N.D.). Annular disc tear Understanding the Symptoms, Causes, and Treatments. https://www.spinemd.com/conditions/annular-disc-tear/
Cheng, J., Santiago, K. A., Nguyen, J. T., Solomon, J. L., & Lutz, G. E. (2019). Treatment of symptomatic degenerative intervertebral discs with autologous platelet-rich plasma: follow-up at 5-9 years. Regenerative medicine, 14(9), 831–840. https://doi.org/10.2217/rme-2019-0040
Yue, J. J., Telles, C., Schlösser, T. P., Hermenau, S., Ramachandran, R., & Long, W. D., 3rd (2012). Do presence and location of annular tear influence clinical outcome after lumbar total disc arthroplasty? A prospective 1-year follow-up study. International journal of spine surgery, 6, 13–17. https://doi.org/10.1016/j.ijsp.2011.09.001
Camp, C. L., Conti, M. S., Sgroi, T., Cammisa, F. P., & Dines, J. S. (2016). Epidemiology, Treatment, and Prevention of Lumbar Spine Injuries in Major League Baseball Players. American journal of orthopedics (Belle Mead, N.J.), 45(3), 137–143.
Can neurological physical therapy help individuals diagnosed with a recently acquired or chronic neurological condition gain strength and functioning?
Neurological Physical Therapy
Neurological physical therapy can be extremely beneficial. It aims to restore functional mobility, strength, balance, and coordination in those with neurological conditions that affect their quality of life and ability to move around. It also helps recover from neurological injuries or prevent the progression and worsening of chronic neurological conditions. Depending on the severity of the condition, individuals may receive this therapy as an inpatient or outpatient. Exercise can help improve mobility, increase independence, and decrease the need for assistance, all of which can improve one’s quality of life.
Process
Neurological physical therapy is geared toward treating individuals with conditions affecting the brain and spinal cord, such as stroke, spinal cord injury, and Parkinson’s disease, to help restore mobility and function. The therapy is performed in hospitals, private practice physical therapy clinics, doctors’ offices, rehabilitation facilities, or at a patient’s home. Whether an individual needs inpatient or outpatient physical therapy will depend on the severity of the neurological condition.
Newly acquired neurological conditions such as strokes or traumas like spinal cord injuries and traumatic brain injuries or TBIs often require inpatient rehabilitation.
Once the patient gains enough strength, coordination, and independence with movements like standing and walking, they can progress to outpatient physical therapy.
The patient will undergo a physical exam after a physical therapist has gathered enough information about medical history during the initial evaluation.
The therapist will check muscle strength, coordination, range of motion, reflexes, and the muscle tone of the arms and legs. They may also perform neurological tests to examine coordination, such as following moving objects with the eyes, touching the finger to the nose, and rapidly alternating movements.
The individual general level of attention, cognition, and sensation will also be assessed to determine if these areas have been affected by the neurological condition. (Cleveland Clinic, 2022)
The therapist will then assess the patient’s ability to perform movements called transfers, which are transitions to and from positions such as lying down to sitting up or standing up to sitting.
They will note if the patient can perform these movements independently or if they need assistance.
The initial evaluation will also include an assessment of balance, quality of gait, and whether the therapist needs to assist.
Depending on the severity of the neurological condition, the therapist may provide the patient with or recommend purchasing an assistive device to help walk.
Treatment Sessions
During therapy sessions, patients may receive the following interventions:
Gait Training
To improve walking ability, proper instruction on using assistive devices such as canes, walkers, and crutches.
Balance Training
To improve static/stationary and dynamic/while moving balance, both sitting unsupported to improve core control and standing upright with or without handheld support.
Therapeutic Activities
To improve independence with bed mobility skills like rolling and sitting up from lying down and transfers on and off beds, chairs, and toilets.
Therapeutic exercises for stretching and strengthening muscles and improving coordination and motor control.
Endurance Training
This can be done with cardiovascular equipment like treadmills, stationary bicycles, and ellipticals.
Vestibular Therapy Interventions
Balance exercises with head movements and exercises to treat a common cause of dizziness are used to improve eye movement control.
Examples are the Dix-Hallpike and Epley maneuvers.
Conditions
Neurological physical therapy can treat various conditions. Some neurological conditions are progressive, worsening over time, and require regular physical therapy and at-home exercises to maintain optimal health and wellness. Neurological conditions that can be treated with physical therapy include: (Cleveland Clinic, 2022)
Strokes – loss of blood supply to the brain.
Spinal cord injuries – damage to part of the central nervous system resulting in loss of movement and control.
Polyneuropathies – damage to the peripheral nerves.
Traumatic brain injuries – for example, concussions.
Cerebral palsy – a group of disorders affecting movement, balance, and posture.
Multiple sclerosis – a disabling disease of the brain and spinal cord.
Parkinson’s disease – a progressive nervous system disorder.
Guillain-Barre syndrome – an autoimmune disease attacking the nerves.
Amyotrophic lateral sclerosis/ALS, also known as Lou Gehrig’s disease.
Vertigo, including benign paroxysmal positional vertigo or BPPV.
Neurological conditions, like an automobile collision, can occur suddenly or be progressive, such as Parkinson’s. Physical therapy helps those individuals by increasing their use of weakened muscles, improving their motor control, coordination, and balance, and facilitating their independence with daily tasks and movements. Always seek immediate medical attention for any sudden, unexplained muscle weakness. Individuals who experience skeletal muscle weakness should discuss the type and duration of symptoms with their doctor, specialist, physical therapist, or chiropractor, as this might be a sign of a medical condition such as a neuromuscular disorder. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized treatment program through an integrated approach to treat injuries and chronic pain syndromes, improving flexibility, mobility, and agility, relieving pain, and helping individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
For individuals who are feeling back pain, neck pain, or shoulder pain, can using postural techniques help decrease pain and develop strategies to maintain correct posture?
Maintaining Correct Posture
Exercise and postural correction are two of the most important strategies to manage pain. (Robin McKenzie, the great spine guru PT, (May S. and Donelson R. 2008) However, it is not easy to maintain correct posture as the day progresses. While working or driving, most of us forget to be mindful of our posture; we slip back into unhealthy habits of sitting slouched, to the side, forward, etc, which often leads to continued pain and movement limitations. Studies on postural correction and its effect on overall back or neck pain levels are limited. (Lederman E. 2011) However, some studies show that a forward-head posture increases stress and load on the neck. (Hansraj K. K. 2014) If an individual has pain that improves with sitting upright, perhaps checking posture as the day progresses could be beneficial. There are ways to start changing posture and maintain the change. First, visit a physical therapist, spine specialist, or chiropractor to learn how to sit or stand to manage posture problems. They can teach individuals how to attain healthy posture and manage their condition. These strategies can then be used to maintain correct posture.
Lumbar Support
A lumbar roll/support is one of the simplest ways to attain and maintain a healthy sitting posture. These specialized pillows can help maintain the forward curve in the lower back. Maintaining the lumbar lordosis curve is essential for keeping stress off the back muscles, joints, and discs. Lumbar support pillows can be found in various stores, office supply stores, or purchased online. A physical therapist PT can help train individuals to use a lumbar roll properly.
Utilize the Slouch Overcorrect Exercise
The slouch overcorrect exercise is a simple maneuver for training the body to find and maintain its neutral position. It involves slowly shifting from a slouched position to an overcorrected postural position. Once posture is overcorrected, a slight relaxation from a fully erect posture will return to sitting properly. Practicing this exercise daily can help train the body to feel the muscles, listen to the body, and maintain proper posture. The muscles have memory, and the more often the body is placed in optimal posture, the muscles memorize their healthy, pain-free positioning.
Kinesiology Tape
Kinesiology tape is a flexible cotton adhesive that facilitates muscle contractions and inhibits muscle spasms and pain. (Han J. T. et al., 2015) Using the tape is a simple way to help facilitate the postural support muscles. The tape can be applied to the middle trapezius and rhomboid muscles to help support the shoulder blades and spine. Kinesiology tape for postural control also gently pulls on the muscles when slouching to remind the individual to sit up or stand straight.
Scapular Stabilization Exercises
A physical therapist or chiropractor can help improve posture through targeted exercises. Strengthening the muscles attached to the shoulder blades can help individuals better control their posture. (Shiravi S. et al., 2019) Exercises like the prone T, I, or Y can help improve the muscles’ neuromuscular recruitment to maintain correct posture.
Use an Alarm
Setting an alarm while working can help train the body to maintain correct posture. Most of us sit at a computer, desk, or workstation with proper posture, but depending on what we’re working on, we eventually slouch, lean to the side, or have a forward head posture. Pretty much all computers and phones have an alarm setting or app. Use the alarm or timer to go off every 20 to 30 minutes. When the alarm rings, look at your posture to recognize what you’re doing, get up and move around to stretch the body, sit and readjust, reset the alarm, and continue working. As you get better at maintaining appropriate posture, you won’t need the alarm anymore, and readjusting will become automatic.
Chiropractic Team
Sitting and standing with unhealthy posture can significantly cause back, neck, and shoulder pain. By visiting a chiropractic and physical therapy team and learning to attain and maintain correct posture, you can quickly relieve pain, resolve musculoskeletal issues, and prevent future pain symptoms. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized care plan for each patient through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility programs to relieve pain and help return to normal and optimal function. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Scapular Winging In-Depth
References
May, S., & Donelson, R. (2008). Evidence-informed management of chronic low back pain with the McKenzie method. The spine journal : official journal of the North American Spine Society, 8(1), 134–141. https://doi.org/10.1016/j.spinee.2007.10.017
Lederman E. (2011). The fall of the postural-structural-biomechanical model in manual and physical therapies: exemplified by lower back pain. Journal of bodywork and movement therapies, 15(2), 131–138. https://doi.org/10.1016/j.jbmt.2011.01.011
Hansraj K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical technology international, 25, 277–279.
Han, J. T., Lee, J. H., & Yoon, C. H. (2015). The mechanical effect of kinesiology tape on rounded shoulder posture in seated male workers: a single-blinded randomized controlled pilot study. Physiotherapy theory and practice, 31(2), 120–125. https://doi.org/10.3109/09593985.2014.960054
Shiravi, S., Letafatkar, A., Bertozzi, L., Pillastrini, P., & Khaleghi Tazji, M. (2019). Efficacy of Abdominal Control Feedback and Scapula Stabilization Exercises in Participants With Forward Head, Round Shoulder Postures and Neck Movement Impairment. Sports health, 11(3), 272–279. https://doi.org/10.1177/1941738119835223
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine