Can Affect Lower Back Muscles and Cause Hamstring Spasms
Lower back muscles, including those like the quadratus lumborum, can be affected by paraspinal spasms. (Hospital for Special Surgery, 2024)
The spasms can cause these muscles to tighten or spasm, potentially pulling on the hamstring muscles.
This can lead to hamstring spasms and tightness, further contributing to pain and potential nerve irritation.
Entrapment of the Sciatic Nerve
Piriformis syndrome is a common condition where the piriformis muscle (located in the buttock) spasms and compresses the sciatic nerve. (Cedars-Sinai, 2025)
The sciatic nerve runs from the lower back down the back of the thigh and into the leg, making it vulnerable to compression by surrounding muscles.
If the paraspinal and hamstring spasms create enough tension on the piriformis muscle or surrounding tissues, it can lead to sciatic nerve entrapment. (Hospital for Special Surgery, 2024)
How acupuncture helps relieve sciatica
Acupuncture can help relieve sciatica pain by stimulating specific points on the body, which can trigger the release of endorphins, reduce inflammation, improve blood flow, and relax tight muscles that could be compressing the sciatic nerve. By modulating the nervous system and promoting the body’s natural healing processes, acupuncture can help alleviate pain and improve overall function. (Qin, Z. et al., 2015)
Releases endorphins
Acupuncture stimulates the nervous system, triggering the release of endorphins, the body’s natural painkillers.
Reduces inflammation
Acupuncture can help reduce inflammation in the area surrounding the sciatic nerve, which can contribute to pain and nerve irritation. (Natural Care Chiropractic, 2022)
Improves circulation
By increasing blood flow to the affected area, acupuncture can help deliver nutrients and oxygen to the sciatic nerve and surrounding tissues, promoting faster healing.
Relaxes tight muscles
Sciatica pain can be exacerbated by tight muscles compressing the nerve. Acupuncture can help relax these muscles, reducing pressure on the sciatic nerve and alleviating pain.
Regulates the nervous system
Acupuncture can help regulate the nervous system, positively impacting pain perception and overall well-being. (Qin, Z. et al., 2015)
Promotes regeneration
Some evidence suggests that acupuncture can promote sciatic nerve regeneration, potentially leading to long-term pain relief. (Natural Care Chiropractic, 2022)
Needling Types
Distal needling
Acupuncture can also involve using points that are further away from the site of pain, which can also help to reduce pain and inflammation.
Local needling
Points are also selected on or near the sciatic nerve’s path, which can help directly address the source of pain and inflammation. (Qin, Z. et al., 2015)
Holistic approach
Acupuncture is often viewed as a holistic approach to pain management, addressing the symptoms of sciatica and the underlying causes and imbalances in the body.
Injury Medical Chiropractic and Functional Medicine Clinic
As a Family Practice Nurse Practitioner, Dr. Jimenez combines advanced medical expertise with chiropractic care to address various conditions. Our clinic integrates Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine to create customized care plans that promote natural healing, mobility, and long-term wellness. By focusing on flexibility, agility, and strength, we empower patients to thrive, regardless of age or health challenges. At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately focus on treating patients after injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities. We use in-person and virtual health coaching and comprehensive care plans to ensure every patient’s personalized care and wellness outcomes.
Noonan, A. M., & Brown, S. H. M. (2021). Paraspinal muscle pathophysiology associated with low back pain and spine degenerative disorders. JOR spine, 4(3), e1171. https://doi.org/10.1002/jsp2.1171
Hospital for Special Surgery. (2024). Sciatica. https://www.hss.edu/condition-list_sciatica.asp
Qin, Z., Liu, X., Wu, J., Zhai, Y., & Liu, Z. (2015). Effectiveness of Acupuncture for Treating Sciatica: A Systematic Review and Meta-Analysis. Evidence-based complementary and alternative medicine: eCAM, 2015, 425108. https://doi.org/10.1155/2015/425108
Natural Care Chiropractic, D. M. F. (2022). Acupuncture for Sciatica Pain Relief. https://www.naturalcarechiropractic.com/post/acupuncture-for-sciatica-pain-relief
For individuals with lower back pain when walking, could they have injured a muscle or have an underlying condition affecting the joints, ligaments, or nerves?
Back Pain When Walking
Lower back pain when walking can occur for a variety of reasons. It can result from poor posture, injuries, muscle fatigue, or an underlying condition. Specific injuries, like muscle strains, can affect the ligaments in the spine and cause pain. Muscles that have not been used often can result in fatigue and pain. Specific health conditions, such as degenerative disc disease, spinal stenosis, herniated discs, sciatica, or even sacroiliac joint dysfunction, can cause lower back pain. Factors like overexertion or improper gait can exacerbate it.
Muscle Issues
Muscle strains, ligament sprains, or fatigue can cause lower back pain when walking. Pain can occur after walking or come on gradually from wear and tear without an apparent cause, as follows (American Association of Neurological Surgeons, 2024)
Strains
Occur when the fibers in the back are overstretched or torn.
Pain from muscle strains is usually worse during activity and better when resting.
Sprains
It occurs when the ligaments that connect bone to bone become detached.
If the muscles do not adequately support the spine, the spinal joints absorb more pressure, which can lead to injury to the spinal ligaments.
Fatigue
It can happen from overexertion and lead to lower back pain when walking.
It could occur when walking longer than the body is used to, on uneven surfaces that make the muscles work harder to help maintain balance, or climbing hills that cause you to lean forward while walking.
Degenerative Disc Disease
Between each vertebra is a disc that provides cushioning between the bones.
As the disc wears down, surrounding muscles, ligaments, joints, and nerves in the spine absorb more pressure, causing damage.
Degenerative disc disease is a wear-and-tear condition that becomes more common as individuals age and is a common cause of lower back pain.
Healthcare providers recommend walking as a low-impact activity for individuals with the disease. However, if the condition is more severe, individuals could experience pain from this exercise, especially when walking on hard surfaces. (Hospital for Special Surgery, 2024)
Sciatica
Sciatica pain occurs when a nerve exiting the spine in the lower back becomes compressed or pinched. It is a common symptom of a herniated disc, in which a disc moves out of place and puts pressure on nearby nerves. In addition to lower back pain, sciatica can cause pain in the hip, the back of the thigh, and down the leg. Sciatica can also cause: (American Academy of Orthopaedic Surgeons, 2021)
Numbness
Tingling
Muscle cramps
Leg muscle weakness
Healthcare providers often recommend walking as a safe form of physical activity for individuals with sciatica. However, individuals should avoid twisting or bending forward. (American Academy of Orthopaedic Surgeons, 2021) To decrease pain, avoid walking on uneven surfaces or uphill.
Lumbar Spinal Stenosis
Spinal stenosis is a wear-and-tear condition that often affects the lumbar spine/five vertebrae in the lower back.
It causes the space surrounding the spinal cord to narrow.
Lumbar spinal stenosis typically causes pain when standing upright, including when walking.
Many with this condition find that leaning slightly forward helps to reduce the pain by opening up the compressed areas.
Hyperlordosis
Lordosis describes the normal curve in the spine in the lower back. However, when this curve is exaggerated, it causes hyperlordosis or swayback. (American Academy of Orthopaedic Surgeons, 2020) Hyperlordosis affects the range of motion, putting abnormal pressure on the muscles, ligaments, and joints. It also reduces the spine’s ability to absorb shock correctly when walking, leading to pain. (Cedars-Sinai, 2025)
Prevention Strategies
Individuals can take steps to reduce their risk of lower back pain when walking, even if they’ve been diagnosed with a condition that can potentially cause this symptom. Walking can decrease chronic low back pain for some. (Suh J. H. et al., 2019) As with any new exercise program, check with a healthcare provider to ensure that walking for exercise is appropriate for the injury, condition, or disease and is safe. Recommended tips: (Harvard Health Publishing, 2015)
Wear shoes made for walking.
Perform gentle lower back stretches before walking.
Start slowly by walking for a few minutes, then gradually increase the time.
Walk on a smooth surface, such as a sidewalk or athletic track, or indoors, such as in a shopping center or mall.
Warm up and cool down by walking slowly at the beginning and end of the walk.
This allows the back and leg muscles to warm up before exercise and recover afterward.
Walk at a slow to moderate pace/speed that allows one to converse.
Standing up straight while walking or standing upright reduces pressure on the lower back.
Alternative Exercise
If there is still back pain when walking, it might not be an appropriate exercise for the individual and/or how their condition presents symptoms. Alternate activities can include: (Hospital for Special Surgery, 2023)
Elliptical Trainer
This exercise keeps the feet in contact with the pedals, putting less shock-absorbing pressure on the spine than walking.
Recumbent Biking
will keep the back upright, which is recommended if there is more pain when bending forward.
Upright Stationary Biking
This is recommended if the back pain improves when bending forward.
Walking In A Pool
This activity provides benefits while reducing pressure on the spine.
To target different muscles, try walking laps in waist-deep water in multiple directions (forward, backward, and side to side).
Water Aerobics
This activity provides cardiovascular health benefits with decreased pressure on the back.
Injury Medical Chiropractic & Functional Medicine Clinic
See a physical therapist for a personalized exercise program to reduce back pain and appropriate for your condition. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Beyond Adjustments: Chiropractic and Integrative Healthcare
References
American Association of Neurological Surgeons. (2024). Low back strain and sprain. https://www.aans.org/patients/conditions-treatments/low-back-strain-and-sprain/
Hospital for Special Surgery. (2024). Degenerative disc disease. https://www.hss.edu/condition-list_degenerative-disc-disease.asp
American Academy of Orthopaedic Surgeons. (2021). Sciatica. https://orthoinfo.aaos.org/en/diseases–conditions/sciatica
American Academy of Orthpaedic Surgeons. (2021). Lumbar spinal stenosis. https://orthoinfo.aaos.org/en/diseases–conditions/lumbar-spinal-stenosis/
American Academy of Orthopaedic Surgeons. (2020). Spine basics. https://orthoinfo.aaos.org/en/diseases–conditions/spine-basics/
Suh, J. H., Kim, H., Jung, G. P., Ko, J. Y., & Ryu, J. S. (2019). The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine, 98(26), e16173. https://doi.org/10.1097/MD.0000000000016173
Harvard Health Publishing. (2015). 5 tips for getting started with a walking program. https://www.health.harvard.edu/exercise-and-fitness/get-started
Hospital for Special Surgery. (2023). Best types of exercise for back pain. https://www.hss.edu/article_best-exercise-lower-back-pain.asp
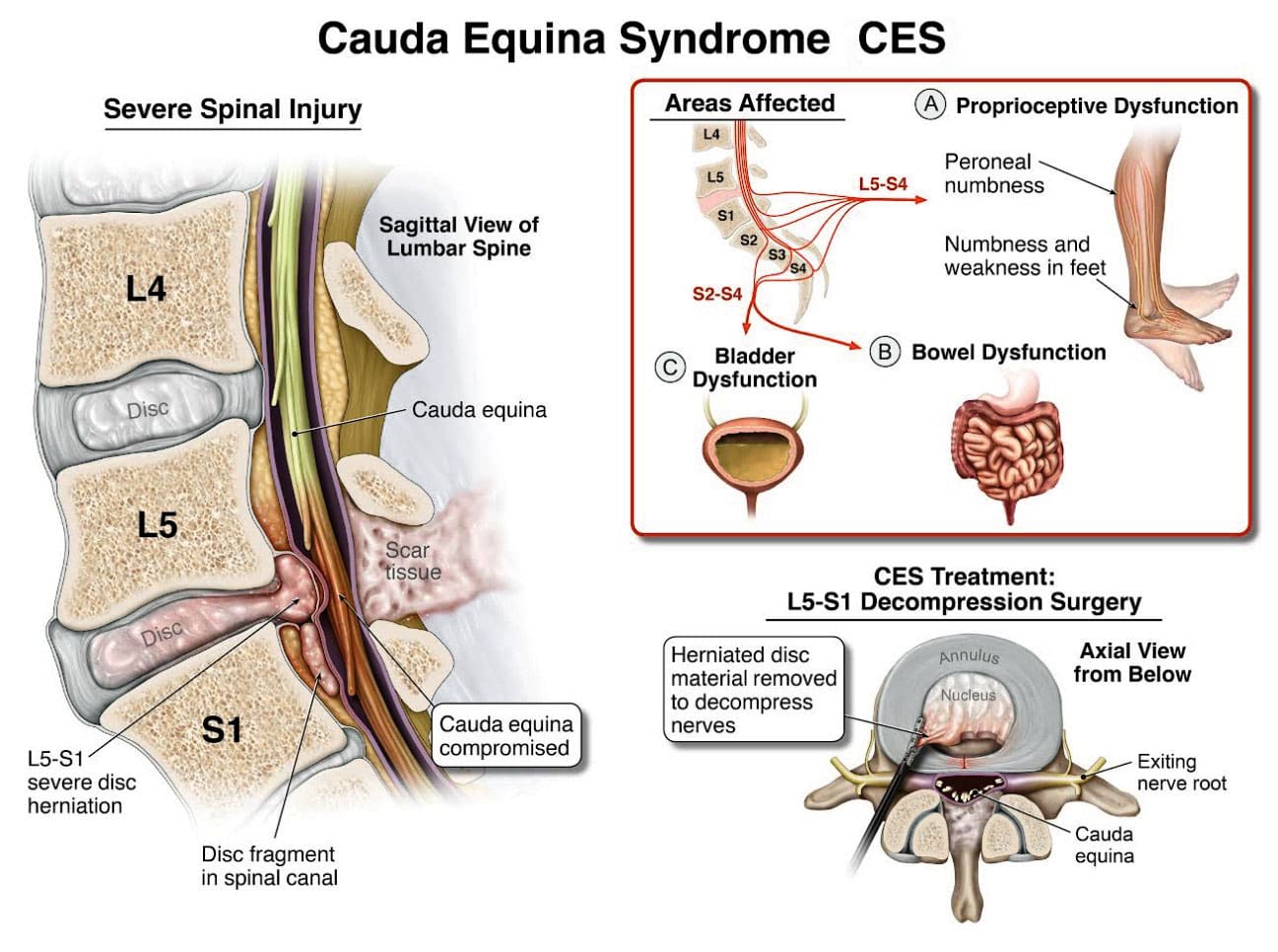
Cauda equina syndrome/CES is a rare condition in which the nerves in the lower back are compressed. It can include sciatica as one of its symptoms. Individuals presenting with symptoms that could be CES are advised to see a healthcare provider as soon as possible, as delaying treatment can lead to permanent damage.
Cauda Equina Syndrome
A cluster of nerve roots called the cauda equina, Latin for horse’s tail, sends and receives messages to the legs, bladder, and other body parts. Cauda equina syndrome is a rare condition in which nerve roots in the lower spinal cord are compressed. This compresses the nerves and disrupts motor and sensory function in the bladder and lower extremities. The most common cause is a ruptured or herniated disc in the lumbar area. This usually occurs when a severe disc herniation compresses the nerve bundle at the base of the spinal cord, causing significant neurological dysfunction like bladder/bowel issues and numbness in the saddle area. If found early, it is treated with surgery within 24 to 48 hours of symptom onset.
This is characterized by symptoms that include unusual urinary sensation, loss of desire to urinate, poor urinary stream, and having to strain to urinate. (Gardner A., Gardner E., & Morley T. 2011)
Pott’s paralysis is a neurological complication of tuberculosis (TB) of the spine.
TB is a bacterial infection that usually affects the lungs but can spread to the spine.
Iatrogenic Side Effects
Injuries or illnesses that result from medical or surgical treatment
Spinal Lesions or Malignant Tumors
A spinal lesion refers to any abnormal growth or damage within the spine.
It can include benign (noncancerous) and malignant (cancerous) tumors.
A malignant tumor is a cancerous growth within the spine; essentially, a malignant tumor is a type of spinal lesion with the potential to spread to other parts of the body.
Spinal Infection, Inflammation, Hemorrhage, or Fracture
A spinal infection refers to a bacterial, fungal, or viral infection that occurs within the bones of the spine (vertebrae) or the surrounding tissues, potentially causing pain, inflammation, and, in severe cases, neurological complications like weakness or paralysis;
Spinal inflammation is a general term for swelling or irritation within the spinal column.
Spinal hemorrhage” indicates bleeding within the spinal canal.
A spinal fracture refers to a break in one or more of the vertebrae in the spine.
Spinal Arteriovenous Malformations (AVMs)
A spinal arteriovenous malformation (AVM) is a rare condition in which the arteries and veins in the spinal cord tangle abnormally.
This can damage the spinal cord over time.
Complications from Lumbar Surgery
Lumbar surgery can have several complications, including infections, blood clots, nerve damage, and spinal fluid leaks.
Spinal Anesthesia
Spinal anesthesia is a regional anesthesia that blocks pain and sensation in the lower body.
It involves injecting a local anesthetic medication into the subarachnoid space surrounding the spinal cord.
The exact cause is not fully understood, but it can involve direct nerve root injury from the needle, inflammation caused by the anesthetic, or a spinal hematoma compressing the nerve roots.
Infection of the tissues (meninges) that cover the cauda equina and spinal cord.
An abscess pressing on the cauda equina.
Diagnosis
Diagnosis requires a medical history of symptoms, general health, activity level, and a physical exam to assess strength, reflexes, sensation, stability, alignment, and motion. (American Association of Neurological Surgeons, 2024) Testing includes:
X-ray or computerized tomography (CT) imaging is enhanced by the injection of contrast material into the cerebrospinal fluid spaces, which can show displacement of the spinal cord or spinal nerves.
Specialized Nerve Testing
This could be nerve conduction velocity tests and testing electrical activity in muscles or electromyography.
Treatment
The extent of urinary problems can determine treatment protocols. A CES diagnosis is usually followed by emergency surgery within 24 to 48 hours to relieve compression of the nerves. Moving quickly is essential to prevent permanent complications such as nerve damage, incontinence, or leg paralysis. (American Association of Neurological Surgeons, 2024)
Depending on the cause, corticosteroids also may be prescribed to reduce swelling.
Antibiotics may be needed if an infection is responsible for CES.
For situations in which a tumor is the cause, surgery to remove it may be necessary, followed by chemotherapy and/or radiation.
The outcome with CES-I during surgery is generally favorable.
Those whose CES has deteriorated to CES-R tend to have a less favorable prognosis.
Post Surgery Therapy
After surgery, CES can be challenging to deal with. If bladder function has been impaired, recovery of control can take time.
Frequent urinary infections are also a potential complication.
Loss of bladder or bowel control can be psychologically distressing, impacting social life, work, and relationships.
Sexual dysfunction can also occur, contributing to relationship difficulties or depression.
Therapy with a mental health professional may be recommended. When damage is permanent, it will be important to include family and friends in the adjustment to living with a chronic condition. Psychological counseling and/or a support group can be helpful. Other specialists who can help include: (American Academy of Orthopaedic Surgeons, 2024)
Occupational therapist
Physical therapist
Physiotherapist
Sex therapist
Social worker
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and mitigate issues through adjustments that help the body realign itself. The clinic can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Disc Herniation
References
American Association of Neurological Surgeons. (2024). Cauda Equina Syndrome. https://www.aans.org/patients/conditions-treatments/cauda-equina-syndrome/
Gardner, A., Gardner, E., & Morley, T. (2011). Cauda equina syndrome: a review of the current clinical and medico-legal position. European Spine Journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 20(5), 690–697. https://doi.org/10.1007/s00586-010-1668-3
Fairbank, J., & Mallen, C. (2014). Cauda equina syndrome: implications for primary care. The British journal of general practice: the journal of the Royal College of General Practitioners, 64(619), 67–68. https://doi.org/10.3399/bjgp14X676988
American Academy of Orthopaedic Surgeons. (2024). Cauda equina syndrome. https://orthoinfo.aaos.org/en/diseases–conditions/cauda-equina-syndrome
For individuals who are looking to lower blood pressure, can walking help?
Walking To Lower Blood Pressure
A walking regimen is an accessible workout that can be done almost anywhere at no cost, effectively lowering blood pressure and improving overall health. Studies show that individuals who use walking as a workout for three months have improved systolic blood pressure, which is the top number that measures the pressure in the arteries as the heart beats. (McMullan S., Nguyen C., & Smith D. K. 2022)
How It Works
Walking is an excellent way to get active. It can be done almost anywhere, including on a treadmill, outdoors, or around the house. Exercising lowers blood pressure by strengthening the heart, leading to the heart pumping blood more effectively when it is stronger. This causes less resistance to the blood vessels, which lowers overall blood pressure. (Hegde S. M., & Solomon S. D. 2015) The benefits of walking include: (American Heart Association, 2024)
Weight loss and management
Lowers stress
Improves mental health by reducing anxiety.
Improves sleep quality
Improves cognition
Strengthens the heart
Promotes bone health and reduces the risk of osteoporosis.
Knowing When to Take A Blood Pressure Reading
Various factors can affect blood pressure readings and can include:
Nervousness
Eating a meal
Drinking caffeine
Exercise can affect blood pressure readings.
Knowing how and when to take a blood pressure reading after walking can help prevent false elevated numbers. According to the CDC, individuals should wait at least 30 minutes after exercise before taking a reading (Centers for Disease Control and Prevention, 2024). Exercise and walking have been shown to cause an immediate reduction in systolic blood pressure. This is known as post-exercise hypotension and is normal. The reduction lasts around 24 hours after exercising and is more noticeable in those with high blood pressure. Consistent exercise and walking will cause a longer, more sustained blood pressure reduction. (Hegde S. M., & Solomon S. D. 2015)
It is recommended not to talk while the blood pressure is being taken.
Apply the blood pressure cuff snugly around the arm.
Place your arm on a table, level with your heart.
Sit in a chair, keep your feet flat on the floor, and do not cross your legs or lean back on the chair.
It is recommended not to eat or drink 30 minutes before and to have an empty bladder.
Pace and Intensity
A study found that walking three to five times weekly for 20 to 40 minutes at a moderate pace for three months can lower systolic blood pressure. However, various groups determined BP rates differently by measuring heart rate, VO2 max/the maximum volume of oxygen you can use simultaneously, and walking speed. (McMullan S., Nguyen C., & Smith D. K. 2022)
Increasing Workout Intensity
Individuals with hypertension who walk may want to increase workout intensity to challenge themselves for added fitness. This can include:
Walk faster
Use intervals – walk as fast as you can for a minute or two at a time.
Add inclines
Use ankle or wrist weights or a weighted vest.
Walking with someone to challenge each other to push a little harder.
Try other places to walk.
Always talk to a healthcare provider if you are starting a walking workout for the first time, want to increase walking intensity, and take medications prescribed by a healthcare provider.
Hypertensive Crisis
A hypertensive crisis is when a person’s blood pressure is extremely high, can cause life-threatening conditions like stroke, and is a medical emergency. It is a blood pressure of 180/120 mm Hg or higher. (American Heart Association, 2024) If you get a blood pressure reading of 180/120 mm Hg or higher at home, wait five minutes and take another reading. If the blood pressure is still high, immediately contact a healthcare provider. (American Heart Association, 2024) If the individual is experiencing the below symptoms, call 911 (American Heart Association, 2024)
Chest pain
Shortness of breath
Vision changes
Difficulty speaking
Weakness
Numbness
Back pain
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Hypertension Explained
References
McMullan, S., Nguyen, C., & Smith, D. K. (2022). Can Walking Lower Blood Pressure in Patients With Hypertension?. American family physician, 105(1), 22–23.
Hegde, S. M., & Solomon, S. D. (2015). Influence of Physical Activity on Hypertension and Cardiac Structure and Function. Current hypertension reports, 17(10), 77. https://doi.org/10.1007/s11906-015-0588-3
American Heart Association. (2024). Getting active to control high blood pressure. https://www.heart.org/en/health-topics/high-blood-pressure/changes-you-can-make-to-manage-high-blood-pressure/getting-active-to-control-high-blood-pressure
Centers for Disease Control and Prevention. (2024). Measure your blood pressure. Retrieved from https://www.cdc.gov/high-blood-pressure/measure/
American Heart Association. (2024). Understanding blood pressure readings. https://www.heart.org/en/health-topics/high-blood-pressure/understanding-blood-pressure-readings
American Heart Association. Association, A. H. (2024). When to call 911 about high blood pressure. https://www.heart.org/en/health-topics/high-blood-pressure/understanding-blood-pressure-readings/hypertensive-crisis-when-you-should-call-911-for-high-blood-pressure
Sleeping with lower back pain and sciatica can be difficult and frustrating. What are ways to get more comfortable sleep?
Sleeping With Lower Back Pain and Sciatica
Various factors can affect sleeping with lower back pain and sciatica, including age, injury and medical history, the mattress (e.g., soft vs. firm mattress), and sleep positions. Unfortunately, there’s no one-cure-all solution for this problem, and depending on the underlying cause/s, they can worsen the pain and cause sleep problems. For example, if a herniated disc places added pressure on the nerves in the lower back, twisting the spine can worsen the lower back pain, and sleeping in a fetal position can exacerbate the nerve pain. (UCF Health, N.D.)
Lower-Back Pain
Low-back pain can be activity-related, intermittent, or constant. (American Association of Neurological Surgeons, 2024) For some, it only occurs occasionally, such as when performing specific movements. For others, it can be excruciating, chronic, and disabling. Low-back pain is unique for everybody and can differ depending on the cause. Some low-back pain symptom descriptions include (Förster M. et al., 2013)
Aching pain deep in the back
Shooting pain flare-ups
Pain caused by slight pressure
Burning
Tingling
Sciatica Not Present
For some, low-back pain may be confined to a specific area known as axial back pain. (Förster M. et al., 2013) The pain may be felt in a band along the lower back and does not radiate down the legs or anywhere else.
Sensory changes radiating down the leg – numbness, burning, and or tingling
Sleep Tools
Consider changing the mattress to improve sleeping with lower back pain and sciatica. For the best spinal support, choose a medium to firm mattress. Pillows, wedges, and other tools can also help improve sleep. (UCF Health, N.D.) It is recommended that individuals who sleep on their backs place a small pillow under their knees to reduce pressure on their lower backs. For those who sleep on their side, placing a pillow between the knees can keep the spine in a neutral/straight position. To relieve lower back pain, consider sleeping in a reclined, angled position with the head and shoulders higher than the hips. This can be accomplished with an adjustable bed or a wedge to prop the body in a regular bed.
Back Sleeping
Easing back pain while sleeping involves maintaining the body in a neutral or straight position. Extending the muscles, tendons, and ligaments too far in any one direction while sleeping with lower back pain and sciatica can cause stiffness, muscle spasms, and pain. Sleeping on the back puts the spine in neutral alignment with the least stress on the neck and back. It evenly distributes body weight to avoid exerting pressure on the joints and prevent backaches. In addition, a supine position allows outstretched ligaments to shrink and recover to their normal positions. (Keck Medicine of USC, 2019)
Chiropractic Assessment
Chiropractic care aims to help individuals improve movement with less pain due to condition, after injury, or surgery. A chiropractic physical therapy team may be best for individuals with acute back, neck, and musculoskeletal pain and discomfort symptoms. A chiropractor can quickly assess your condition and develop a customized treatment plan to expedite pain relief and improve mobility. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Sciatica, Causes, Symptoms and Tips
References
UCF Health. (N.D.). The best sleeping position for lower back pain (and the worst). https://ucfhealth.com/our-services/lifestyle-medicine/best-sleeping-position-for-lower-back-pain/
American Association of Neurological Surgeons. (2024). Low back pain. https://www.aans.org/patients/conditions-treatments/low-back-pain/
Förster, M., Mahn, F., Gockel, U., Brosz, M., Freynhagen, R., Tölle, T. R., & Baron, R. (2013). Axial low back pain: one painful area–many perceptions and mechanisms. PloS one, 8(7), e68273. https://doi.org/10.1371/journal.pone.0068273
North American Spine Society. (2020). Evidence-based clinical guidelines for multidisciplinary spine care: Diagnosis and treatment of low back pain. North American Spine Society. https://www.spine.org/Portals/0/assets/downloads/ResearchClinicalCare/Guidelines/LowBackPain.pdf
American Academy of Orthopaedic Surgeons. (2021). Sciatica. https://orthoinfo.aaos.org/en/diseases–conditions/sciatica
Keck Medicine of USC. (2019). The best -and worst – sleep positions for back pain. Keck Medicine of USC Blog. https://www.keckmedicine.org/blog/the-best-and-worst-sleep-positions-for-back-pain/
For individuals trying to retrain their body movements for back health improvement, what is the spinal area that helps the body twist, bend, and stand upright?
Lumbosacral Joint L5-S1
The L5-S1, also called the lumbosacral joint, is a term used to describe a part of the spine. It is where the lumbar spine ends and the sacral spine begins, and it connects these bones. The lumbosacral joint is also susceptible to misalignment and injury, such as disc herniation or a spinal disorder called spondylolisthesis.
The spinal column is the structure that allows the body to stand upright and helps you twist, bend, and alter trunk and neck position. Typically, 24 movable bones in the spine connect to the sacrum and the coccyx, or the tailbone. The sacrum and the coccyx each have multiple bones that fuse over time. L5-S1 consists of the last bone in the lumbar spine, called L5, and the triangle-shaped bone under it, known as the sacrum. S1 is at the top of the sacrum and comprises five fused bones.
Risk of Injury
Each area of the spine has a curve that goes in opposite directions. The places where the spinal curve directions change are junctional levels. The risk of injuries may be higher at junctional levels because the body weight shifts direction as the curves shift. The L5-S1 junction is located between the lumbar curve and the sacral curve. The lumbar curve sweeps forward, and the sacral curve goes backward.
The lumbosacral joint L5-S1 junction is highly vulnerable to misalignment, wear and tear, and injury. This is because the top of the sacrum is positioned at an angle for most individuals. Aging and injury increase the vulnerability of the L5-S1 junction even more. Pain coming from L5-S1 is usually treated with:
Heat and/or ice
Over-the-counter anti-inflammatory medications
Prescription pain medications
Muscle relaxers
Physical therapy
Chiropractic adjustments
Epidural steroid injections
If these therapies do not help, surgery may be recommended. L5-S1 is one of the two most common sites for back surgery.
Conditions
Disc herniation at L5-S1 is a common injury and cause of sciatica, which can cause pain and other issues (MedlinePlus, 2024). The L5-S1 junction is often the site of a condition known as spondylolisthesis.
Disc Herniation
Discs separate the vertebrae, cushioning the spinal column and allowing movement between vertebrae. A disc herniation means the disc slips out of place. (MedlinePlus, 2022) A disc herniation at L5-S1 is a common cause of sciatica. Symptoms of sciatica include:
Burning
Numbness
Pain or tingling that radiates from the buttock down the leg to the knee or foot.
Disc herniation can also cause chronic back pain and stiffness and trigger painful muscle spasms. Bowel problems are also possible with disc issues at L5-S1. Research links irritable bowel syndrome to herniated discs in the lower back. (Bertilson BC, Heidermakr A, Stockhaus M. 2015) Additional studies found disc problems at L5-S1 can lead to difficulty with sphincter control. (Akca N. et al., 2014) Initial treatments for disc herniation include rest and pain relievers to reduce inflammation and swelling, then physical therapy. Most recover with conservative interventions, and those who don’t may require a steroid injection or surgery. (MedlinePlus, 2022)
Spondylolisthesis
Spondylolisthesis occurs when a vertebra slips forward relative to the bone below it. The most common form of this condition is degenerative spondylolisthesis, which generally begins when the spine wears down with age. Isthmic spondylolisthesis is another common variation and starts as a tiny fracture in the pars interarticularis, a bone that connects the adjoining parts of the facet joint. (American Academy of Orthopaedic Surgeons, 2020) These fractures often occur before age 15, but symptoms do not develop until adulthood. Degeneration of the spine in later adulthood can further worsen the condition.
The angle of the sacrum can also contribute to spondylolisthesis. This is because the S1 tips down in the front and up in the back rather than being horizontal. Individuals with a greater tilt are usually at a higher risk of spondylolisthesis. (Gong S. et al., 2019) However, individuals with spondylolisthesis may not have any symptoms. Those who do may experience: (American Academy of Orthopaedic Surgeons, 2020)
Back stiffness
Standing difficulties
Walking difficulties
Lower back pain
Hamstring tightness
Spondylolisthesis is typically treated with non-surgical interventions that can include:
Pain medications
Heat and/or ice application
Physical therapy
Epidural steroid injections
Usually, non-surgical care is tried for at least six months. If pain and symptoms persist, surgery may be an option. Spinal fusion surgery can be effective but requires a long recovery time and can have additional risks.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Healing After Trauma
References
MedlinePlus. (2024). Sciatica. Retrieved from https://medlineplus.gov/sciatica.html
MedlinePlus. (2022). Herniated disk. Retrieved from https://medlineplus.gov/ency/article/000442.htm
American Association of Neurological Surgeons. (2024). Herniate disc. https://www.aans.org/patients/conditions-treatments/herniated-disc/
Bertilson, B. C., Heidermark, A., & Stockhaus, M. (2015). Irritable Bowel Syndrome–a Neurological Spine Problem. Journal of Advances in Medicine and Medical Research, 4(24), 4154–4168. https://doi.org/10.9734/BJMMR/2014/9746
Akca, N., Ozdemir, B., Kanat, A., Batcik, O. E., Yazar, U., & Zorba, O. U. (2014). Describing a new syndrome in L5-S1 disc herniation: Sexual and sphincter dysfunction without pain and muscle weakness. Journal of craniovertebral junction & spine, 5(4), 146–150. https://doi.org/10.4103/0974-8237.147076
American Academy of Orthopaedic Surgeons. (2020). Spondylolysis and spondylolisthesis. https://orthoinfo.aaos.org/en/diseases–conditions/spondylolysis-and-spondylolisthesis/
Gong, S., Hou, Q., Chu, Y., Huang, X., Yang, W., & Wang, Z. (2019). Anatomical factors and pathological parts of isthmic fissure and degenerative lumbar spondylolisthesis.
For individuals dealing with newly formed or chronic lower back pain, can making daily walks a part of a weekly routine help relieve pain and discomfort symptoms and prevent strains and injuries?
Walking For Low Back Pain Relief
Walking is recommended to treat and prevent chronic or recurrent lower back pain. A study found that a personalized and progressive weekly walking program that builds up to 130 minutes of moderate intensity can significantly relieve severe lower back pain and prevent future flare-ups. (Pocovi N. C. et al., 2024) Walking is a cost-effective and easily accessible way to relieve lower back pain and prevent recurring or future injuries. It strengthens the back muscles, improves posture, and stabilizes the spine. (Suh JH, et al., 2019) Other benefits include improved overall physical health, posture, and circulation.
How Walking Helps
Walking for low back pain relief and general movement is better than not engaging in physical activities for individuals with recurrent lower back pain. Being sedentary can worsen back pain symptoms. (National Library of Medicine. 2019) Walking is second nature and is easy to incorporate into a weekly routine to help relieve back pain and improve overall health (Macquarie University, 2024)
Increases Spinal Flexibility
Walking and gentle movements increase the lower back’s functional range of motion, improve spinal flexibility, and reduce stiffness. (Smith J. A. et al., 2022)
Stabilizes Lumbar/Low Back Muscles
Walking builds muscle endurance and strength in the paraspinal muscles, increasing lumbar spinal stabilization. (Suh JH, et al., 2019)
Strengthens Core Muscles
Walking increases the body load and strengthens core muscles like the transversus abdominis, which lowers the risk of chronic lower back pain. (Lee J. S. and Kang S. J. 2016)
Improves Posture
Movement of the legs during walking enhances bodily awareness and helps correct posture.(Henry M. and Baudry S. 2019)
Increases Blood Circulation
Walking increases blood circulation to the muscles, supplying essential nutrients to spinal discs. It also reduces the frequency and severity of lower back muscle spasms. (Sitthipornvorakul E. et al., 2018)
Lubricates Spinal joints
Low-impact walking improves synovial fluid production and circulation, lubricating the lumbar spine’s facet joints and other joints that tend to get achy, such as the knees. (Zhang S. L. et al., 2013)
Relieves Inflammation
Walking helps reduce the presence of pro-inflammatory cytokines, like (IL-8 and TNF-alpha) associated with chronic lower back pain. (Slouma M. et al., 2023)
Promotes Weight Loss
Walking and a healthy diet can help individuals lose excess fat, which puts added strain on the lower back and correlates with lumbar intervertebral disc degeneration. (Wang M. et al., 2024)
Stress Relief
Regular walking can reduce mental stress associated with chronic lower back pain. (Choi S. et al., 2021)
Releases Endorphins
Moderate to vigorous physical activity, like walking at about 3 miles per hour for a half-hour daily, stimulates the release of endorphins, the body’s natural pain relievers. (Bruehl S. et al., 2020)
Walking Correctly
To get all the benefits of walking for low back pain relief, it is recommended to practice the following (Macquarie University, 2024)
Start slowly.
Gradually build intensity.
Stay consistent with the walking program.
Track progress to maintain motivation.
Healthcare Provider Consultation
Walking is a low-risk, low-impact activity well-tolerated by most individuals with nonspecific low back pain. (Pocovi N. C. et al., 2022) Because it doesn’t involve twisting or vigorous movements, it is considered a safe exercise for individuals with back pain symptoms (Gordon R. and Bloxham S. 2016). However, individuals experiencing severe lower back pain due to a traumatic injury or medical condition should consult a healthcare provider before starting a regular walking program.
Limit High Impact Activities
High-impact activities like running on hard surfaces or playing sports can exacerbate chronic lower back pain. If there is chronic lower back pain, it is recommended to limit activities that involve: (Al-Otaibi S. T. 2015)
Heavy lifting
Repetitive bending
Twisting motions
Injury Medical Chiropractic and Functional Medicine Clinic
Walking for low back pain relief. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Movement as Medicine
References
Pocovi, N. C., Lin, C. C., French, S. D., Graham, P. L., van Dongen, J. M., Latimer, J., Merom, D., Tiedemann, A., Maher, C. G., Clavisi, O., Tong, S. Y. K., & Hancock, M. J. (2024). Effectiveness and cost-effectiveness of an individualised, progressive walking and education intervention for the prevention of low back pain recurrence in Australia (WalkBack): a randomised controlled trial. Lancet (London, England), 404(10448), 134–144. https://doi.org/10.1016/S0140-6736(24)00755-4
Suh, J. H., Kim, H., Jung, G. P., Ko, J. Y., & Ryu, J. S. (2019). The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine, 98(26), e16173. https://doi.org/10.1097/MD.0000000000016173
National Library of Medicine., & InformedHealth.org [Internet]. Cologne, G. I. f. Q. a. E. i. H. C. I. (2022). Low back pain: Learn More – Why movement is so important for back pain. https://www.ncbi.nlm.nih.gov/books/NBK284944/
Macquarie University. (2024). Macquarie University. Walking to combat back pain: world-first study shows dramatic improvement. https://lighthouse.mq.edu.au/article/june-2024/walking-away-from-pain-world-first-study-shows-dramatic-improvement-in-lower-back-trouble
Smith, J. A., Stabbert, H., Bagwell, J. J., Teng, H. L., Wade, V., & Lee, S. P. (2022). Do people with low back pain walk differently? A systematic review and meta-analysis. Journal of sport and health science, 11(4), 450–465. https://doi.org/10.1016/j.jshs.2022.02.001
Suh, J. H., Kim, H., Jung, G. P., Ko, J. Y., & Ryu, J. S. (2019). The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine, 98(26), e16173. https://doi.org/10.1097/MD.0000000000016173
Lee, J. S., & Kang, S. J. (2016). The effects of strength exercise and walking on lumbar function, pain level, and body composition in chronic back pain patients. Journal of exercise rehabilitation, 12(5), 463–470. https://doi.org/10.12965/jer.1632650.325
Henry, M., & Baudry, S. (2019). Age-related changes in leg proprioception: implications for postural control. Journal of neurophysiology, 122(2), 525–538. https://doi.org/10.1152/jn.00067.2019
Sitthipornvorakul, E., Klinsophon, T., Sihawong, R., & Janwantanakul, P. (2018). The effects of walking intervention in patients with chronic low back pain: A meta-analysis of randomized controlled trials. Musculoskeletal science & practice, 34, 38–46. https://doi.org/10.1016/j.msksp.2017.12.003
Zhang, S. L., Liu, H. Q., Xu, X. Z., Zhi, J., Geng, J. J., & Chen, J. (2013). Effects of exercise therapy on knee joint function and synovial fluid cytokine levels in patients with knee osteoarthritis. Molecular medicine reports, 7(1), 183–186. https://doi.org/10.3892/mmr.2012.1168
Slouma, M., Kharrat, L., Tezegdenti, A., Metoui, L., Ghazouani, E., Dhahri, R., Gharsallah, I., & Louzir, B. (2023). Pro-inflammatory cytokines in patients with low back pain: A comparative study. Reumatologia clinica, 19(5), 244–248. https://doi.org/10.1016/j.reumae.2022.07.002
Wang, M., Yuan, H., Lei, F., Zhang, S., Jiang, L., Yan, J., & Feng, D. (2024). Abdominal Fat is a Reliable Indicator of Lumbar Intervertebral Disc Degeneration than Body Mass Index. World neurosurgery, 182, e171–e177. https://doi.org/10.1016/j.wneu.2023.11.066
Choi, S., Nah, S., Jang, H. D., Moon, J. E., & Han, S. (2021). Association between chronic low back pain and degree of stress: a nationwide cross-sectional study. Scientific reports, 11(1), 14549. https://doi.org/10.1038/s41598-021-94001-1
Bruehl, S., Burns, J. W., Koltyn, K., Gupta, R., Buvanendran, A., Edwards, D., Chont, M., Wu, Y. H., Qu’d, D., & Stone, A. (2020). Are endogenous opioid mechanisms involved in the effects of aerobic exercise training on chronic low back pain? A randomized controlled trial. Pain, 161(12), 2887–2897. https://doi.org/10.1097/j.pain.0000000000001969
Pocovi, N. C., de Campos, T. F., Christine Lin, C. W., Merom, D., Tiedemann, A., & Hancock, M. J. (2022). Walking, Cycling, and Swimming for Nonspecific Low Back Pain: A Systematic Review With Meta-analysis. The Journal of orthopaedic and sports physical therapy, 52(2), 85–99. https://doi.org/10.2519/jospt.2022.10612
Gordon, R., & Bloxham, S. (2016). A Systematic Review of the Effects of Exercise and Physical Activity on Non-Specific Chronic Low Back Pain. Healthcare (Basel, Switzerland), 4(2), 22. https://doi.org/10.3390/healthcare4020022
Al-Otaibi S. T. (2015). Prevention of occupational Back Pain. Journal of family & community medicine, 22(2), 73–77. https://doi.org/10.4103/2230-8229.155370
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine