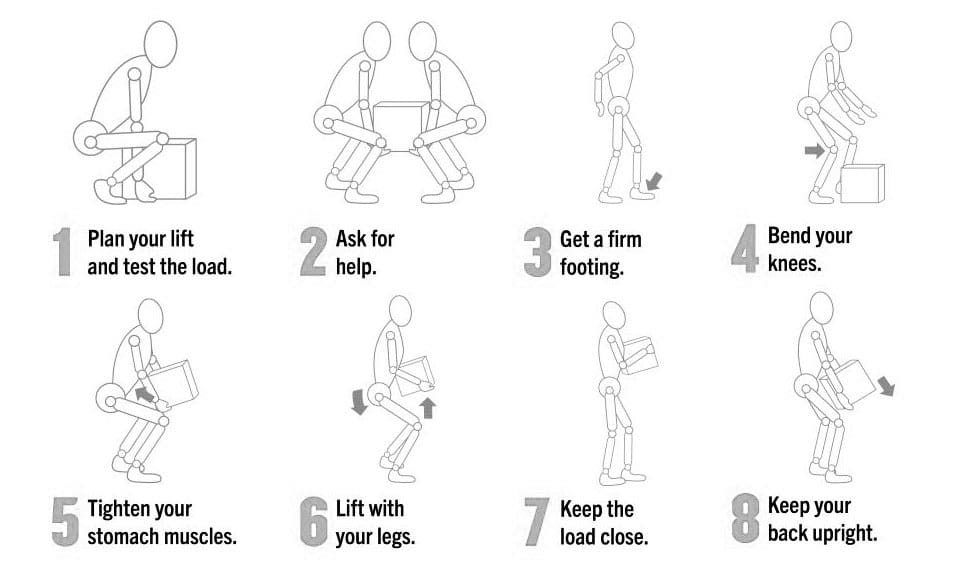
Incorrect manual handling and lifting is a leading cause of workplace injuries. Can health and safety training help reduce injuries and lost workdays?
Correct Manual Lifting Technique
Manually lifting objects using incorrect techniques can lead to acute back injuries, herniated discs, sciatica, and long-term issues like increased risk of reinjury, body misalignment, and chronic back pain. Individuals can prevent spinal disc compression and/or lower back muscle strain by learning to use correct manual lifting techniques. (CDC. The National Institute for Occupational Safety and Health (NIOSH). 2007)
Lifting Guide
Individuals can protect their backs and prevent injury by following simple steps when lifting objects.
Support Base
Ensure there is a healthy support base from which to lift.
Keep feet shoulder-width apart with one foot slightly in front of the other.
Ask For Help
If coworkers or colleagues are available, ask for assistance.
If the load is too heavy, ask for help lifting and moving the object/s.
Use Mechanical Assistant Devices
Use hand trucks, dollies, or pushcarts whenever possible for uneven and heavy loads.
Squat To Lift Object
Bend at the hips and knees only, not the back.
Put one knee on the ground to ensure stability before lifting.
Check Posture
Looking straight ahead, maintain posture upright with the chest out, shoulders back, and lower back slightly arched.
Lift Slowly
Lift with the knees and hips only, gradually straightening the lower back.
Load Positioning
Once upright, hold the load close to the body around the stomach.
Move and Maintain Alertness
Always take small steps.
Maintain alertness as to where you are going.
Keep the shoulders square with the hips when changing directions to avoid twisting and losing or shifting balance.
Rest
If you are fatigued, set the load/object down and rest for a few minutes until you can fully engage in the task.
Squat To Set Object Down
Squat with the knees and hips and set the load down slowly.
Avoid quickly rising and jerking movements, and allow the legs, hips, and back muscles to reset.
Planning and Tips
Lifting anything heavy takes planning to prevent muscle spasms, back strain, and other musculoskeletal injuries. Considerations to keep in mind:
Make a Plan Before Lifting
Knowing what object/s are being lifted and where they are going will prevent individuals from making awkward movements while holding and carrying something heavy.
Set and clear a path.
If lifting something with another person, ensure both agree and understand the plan.
Lift Close to The Body
Individuals are stronger and more stable lifters if the object is held close to their body rather than at the end of their reach.
Make sure there is a firm hold on the object.
It is easier to maintain balance close to the body.
Maintain Feet Shoulder-Width Apart
Keep the feet about shoulder-width apart.
Having a solid base of support is important while lifting.
Placing the feet too close together will cause instability while placing them too far apart will hinder movement.
Take short steps.
Visualize The Motions Involved and Practice The Motions Before Lifting
Think about the motion before lifting.
Practice the lifting motion before lifting the object.
Focus on keeping the spine straight.
Raise and lower to the ground by bending the knees.
Avoid bending at the waist or hips.
Tighten the Stomach Muscles
Tightening the abdominal muscles will hold the back in a healthy lifting position and help prevent excessive force on the spine.
Lift With the Legs
The legs are stronger than the back muscles, so let the leg strength do the work.
Lower yourself to the ground by bending the knees, not the back.
Keep Eyes Up
Looking slightly upwards will help maintain a better spine position and help keep the back straight.
Avoid Twisting or Bending
Face in the direction you are walking.
Stop, take small steps, and continue walking if turning is required.
Back Belts
It has become common for many who work in jobs requiring manual lifting to wear back belts or support. However, research does not show that they decrease the risk of a lifting injury. (CDC and The National Institute for Occupational Safety and Health, 2023) Instead, it is recommended that the belt be thought of as a reminder of where the back muscles are positioned to keep the individual aligned, combined with the correct lifting techniques.
Injury Medical Chiropractic and Functional Medicine Clinic
Training the body and maintaining its optimal health for correct manual lifting techniques requires daily efforts through practice, conscious position corrections, and ergonomics. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Care For Injury Recovery
References
CDC. The National Institute for Occupational Safety and Health (NIOSH). (2007). Ergonomic Guidelines for Manual Material Handling. (No. 2007-131). Retrieved from https://www.cdc.gov/niosh/docs/2007-131/pdfs/2007-131.pdf
CDC. The National Institute for Occupational Safety and Health (NIOSH) (2023). Back Belts – Do They Prevent Injury? (No. 94-127). Retrieved from https://www.cdc.gov/niosh/docs/94-127/
Can the Oswestry Low Back Pain Disability Questionnaire help assess how low back pain impacts individuals’ ability to perform everyday tasks and activities and help physical therapists incorporate the outcome measure into an effective treatment plan?
Oswestry Disability Questionnaire
The Oswestry Disability Questionnaire, also known as the Oswestry Disability Index, provides objective data about an individual’s lower back pain. It determines the severity of the pain and how much it limits their daily activities. The questionnaire is a validated measure backed by research that can be used to justify the need for medical treatment. It includes questions regarding the symptoms and severity of low back pain and how these symptoms interfere with regular activities. Lower back pain can result from various causes (National Institute of Neurological Disorders and Stroke, 2020)
Arthritis, including inflammatory types of arthritis like psoriatic arthritis and ankylosing spondylitis.
Lumbar vertebrae compression fractures – usually from trauma or osteoporosis.
Low back surgery – including spinal fusions, discectomies, and laminectomies.
Spinal stenosis
Spondylolisthesis
Scoliosis
How The Questionnaire Works
The Oswestry Disability Questionnaire consists of 10 questions about the impact of lower back pain on daily life. The questions are divided into the following categories: (American Academy of Orthopedic Surgeons, N.D.)
Pain Intensity
How intense is the pain?
If painkillers are used, how much symptom relief do they provide?
Personal Care
Can the patient perform self-care activities like bathing and dressing when experiencing significant pain or limitations?
Whether physical assistance from another person is needed?
Lifting
Can the patient lift objects like weights with or without pain?
Can lifting be performed from the floor or a higher surface like a table if the objects are light, moderate, or heavy?
Walking
If and to what extent does the pain limit the patient’s walking distance and independence?
If an assistive device like a cane or crutches are needed?
Sitting
If so, how much pain limits the patient’s sitting tolerance?
Standing
If so, how much pain limits the patient’s standing tolerance?
Sleeping
If so, how much pain limits a patient’s sleeping duration?
Whether pain medication is needed to help the patient sleep comfortably?
Social Life
If and to what extent a patient’s social activities are limited because of pain symptoms?
Traveling
If so, to what extent does pain limit a patient’s ability to travel?
Employment and/or Homemaking Duties
Does pain limit a patient’s ability to perform job-related and/or household activities, including physically demanding and light duties?
Patients self-report the information and complete it on their own based on their understanding of the extent of their lower back pain and disability.
Each question can be scored between 0 and 5, with 0 indicating no limitations and 5 indicating complete disability.
The scores from all the questions are added together for a cumulative total score of 50 points.
Scores
The Oswestry Disability Questionnaire assesses how much a patient’s lower back pain limits daily activities. This information is used in clinical documentation for medical services. A higher score indicates a greater level of disability, according to the following scoring criteria:
0–4: No disability
5–14: Mild disability
15–24: Moderate disability
25–34: Severe disability
35–50: Completely disabled
Physical therapists must create individualized goals for each patient to develop a treatment plan and receive authorization from insurance companies. One of the most important aspects of a physical therapy goal is that it must be measurable. The Oswestry Disability Questionnaire provides a numerical score to track functional limitations and monitor the range of motion and strength testing. A baseline measurement is taken at the beginning of treatment, and progress is tracked in follow-up visits. A new score is used as a treatment goal. According to a study, the minimal clinically important difference (MCID) for the Oswestry Disability Questionnaire is 12.88. The MCID is the minimum score healthcare providers need to confirm a patient’s progress in function due to treatment. (Johnsen, L. G. et al., 2013)
By tracking changes in the total score before, during, and after treatment, healthcare providers can better assess whether treatment improves symptoms. A decrease in total score by 13 points or more would indicate that treatment is helping to improve a patient’s lower back pain and level of disability. Along with physical examination results, the patient’s score and the severity of symptoms can help healthcare providers determine an appropriate treatment plan.
No Disability
Treatment is unnecessary other than providing advice for lifting mechanics and general physical activity to maintain health.
Mild Disability
Conservative measures, such as physical therapy, exercise, hot or cold therapy, pain medication, and rest, are needed to help alleviate symptoms.
Moderate Disability
More aggressive intervention is needed, which can include extensive physical therapy services and pain management.
Severe Disability
Significant medical intervention is needed, including surgery, pain management, equipment like wheelchairs, and help from a caretaker.
Completely Disabled
Patients are either bedbound or have worsening symptoms, and a caretaker is needed to complete daily activities and self-care tasks.
Injury Medical Chiropractic and Functional Medicine Clinic
Improvements in range of motion, strength, and quality of movement and a decrease in total score can help show the treatment’s positive impact in managing lower back pain. A thorough medical exam and diagnostic tests, such as X-ray, MRI, or EMG, can help determine the underlying causes, discover the cause of the problem, and develop an effective treatment plan. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop personalized treatment programs. Using an integrated approach to treating injuries and chronic pain syndromes to improve flexibility, mobility, and agility and help individuals return to normal activities. Our providers use Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers.
Optimizing Your Wellness
References
National Institute of Neurological Disorders and Stroke. (2020). Low Back Pain Fact Sheet. Retrieved from https://www.ninds.nih.gov/sites/default/files/migrate-documents/low_back_pain_20-ns-5161_march_2020_508c.pdf
American Academy of Orthopedic Surgeons. (N.D.). Oswestry Low Back Pain Disability Questionnaire. https://www.aaos.org/globalassets/quality-and-practice-resources/patient-reported-outcome-measures/spine/oswestry-2.pdf
Johnsen, L. G., Hellum, C., Nygaard, O. P., Storheim, K., Brox, J. I., Rossvoll, I., Leivseth, G., & Grotle, M. (2013). Comparison of the SF6D, the EQ5D, and the oswestry disability index in patients with chronic low back pain and degenerative disc disease. BMC musculoskeletal disorders, 14, 148. https://doi.org/10.1186/1471-2474-14-148
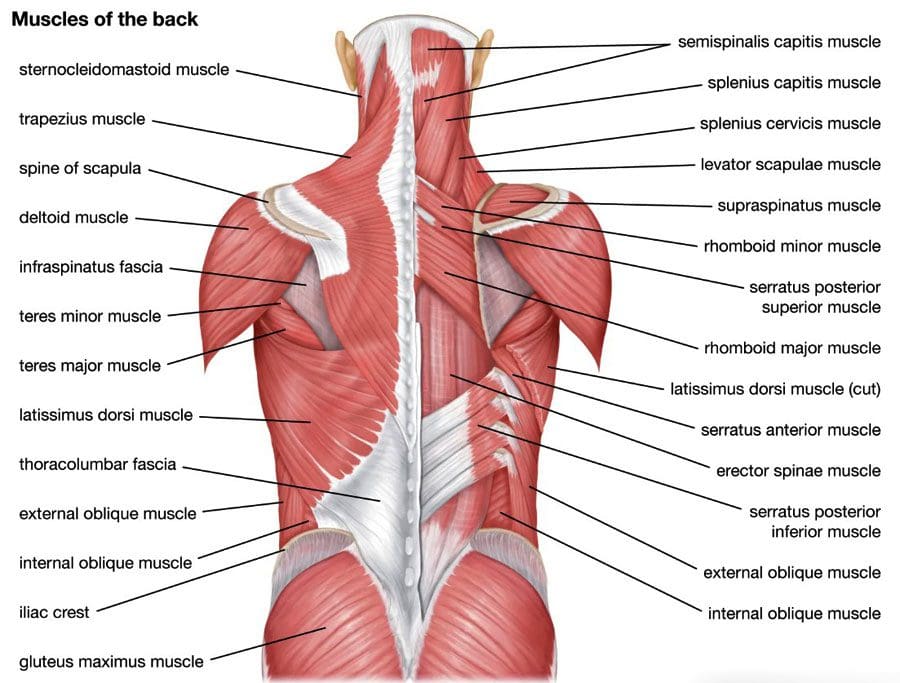
Can the thoracolumbar fascia cause or contribute to lower back pain and inflammation?
Thoracolumbar Fascia
Tissue behind the spinal column, positioned at both the lower back and mid-back levels, is connected to the thoracolumbar fascia, also called the lumbodorsal fascia or LF. The fascia is a thick connective tissue that covers and supports all the body’s muscles, bones, tendons, ligaments, and organs. The fascia also contains nociceptive nerve endings, also known as free nerve endings, that arise from the central nervous system, i.e., the brain and spinal cord, which may be responsible for some forms of back pain and stiffness caused by injury or inflammation.
Anatomy
The thoracolumbar fascia is divided into three layers:
Many of the back muscles attach to the thoracolumbar fascia. The erector spinae muscle group, known as the paraspinals, runs longitudinally down the spine. They are attached to the thoracolumbar fascia and the bony spine. The lumbar part of the posterior layer of the thoracolumbar fascia extends from the lowest rib to the top of the hip bone or the iliac crest. On the same path, it connects with the transverse abdominal muscle. The thoracolumbar fascia connections help bridge the back muscles to the abdominal wall muscles. The latissimus dorsi, a large back muscle that bears and moves the body’s weight with the arms and shoulders, is also connected to the thoracolumbar fascia, with the fibers extending outward from the fascia. The front part of the thoracolumbar fascia, or anterior layer, covers a muscle called the quadratus lumborum. This muscle bends the trunk to the side, helps maintain a healthy posture, and is often focused on muscle-related lower back pain.
What the Fascia Does
The thoracolumbar fascia, examined from the back of an anatomical drawing or diagram, is diamond-shaped. Its shape, large size, and central location uniquely position it to unify and synchronize the upper body’s movements with the lower body’s. The fascia’s fibers are very strong, enabling the tissue sheath to lend support (Willard, F. H. et al., 2012) . The tissue is also flexible, enabling it to help circulate forces of movement and contralateral movements as the back muscles contract and relax. An example is walking.
Back Pain
Scientists and doctors don’t know for sure, but it’s possible that the thoracolumbar fascia may contribute to lower back pain. A study found that the fascia may generate back pain based on: (Wilke, J. et al., 2017)
Sustaining micro-injuries and/or inflammation, which are often related, may cause signal changes in the free nerve endings in the fascia. Nerve endings acquire information from the outer areas of the body, like skin and other fascia, and relay it back to the central nervous system. The theory is that when the fascia close to the skin becomes injured, damaged, and/or backed up with inflammatory chemicals and substances, it is communicated as pain and other sensations back to the brain and spinal cord.
After a back injury, tissues tighten and stiffen. Some studies of patients with back pain noted alterations in their thoracolumbar fascia.
Injuries tend to stimulate nerves, which can lead to increased sensitivity.
Injury Medical Chiropractic and Functional Medicine Clinic focuses on and treats injuries and chronic pain syndromes through personalized care plans that improve ability through flexibility, mobility, and agility programs to relieve pain. Our providers use an integrated approach to create personalized care plans for each patient, including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Our goal is to relieve pain naturally by restoring health and function to the body. If other treatment is needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Sciatica, Causes, Symptoms, and Tips
References
Willard, F. H., Vleeming, A., Schuenke, M. D., Danneels, L., & Schleip, R. (2012). The thoracolumbar fascia: anatomy, function and clinical considerations. Journal of anatomy, 221(6), 507–536. https://doi.org/10.1111/j.1469-7580.2012.01511.x
Wilke, J., Schleip, R., Klingler, W., & Stecco, C. (2017). The Lumbodorsal Fascia as a Potential Source of Low Back Pain: A Narrative Review. BioMed research international, 2017, 5349620. https://doi.org/10.1155/2017/5349620
Individuals may discover a lump, bump, or nodule under the skin around their lower back, hips, and sacrum that can cause pain by compressing nerves and damaging the fascia. Can knowing the conditions linked to them and their symptoms help healthcare providers determine a correct diagnosis and develop an effective treatment plan for them?
Painful Bumps, Nodules Around Low Back, Hips, and Sacrum
Painful masses in and around the hips, the sacrum, and the lower back are lumps of fat or lipomas, fibrous tissue, or other types of nodules that move when pressed on. Some healthcare providers and chiropractors, in particular, use the non-medical term back mice (In 1937, the term was used to describe lumps associated with episacroiliac lipoma) to describe the bumps. Some healthcare professionals argue against calling the masses mice because it is not specific and could lead to misdiagnoses or incorrect treatment.
Most show up in the lower back and hip area.
In some cases, they protrude or herniate through the lumbodorsal fascia or the network of connective tissue that covers the deep muscles of the lower and middle back.
Other lumps can develop in the tissue under the skin.
Today, many conditions are associated with back mice lumps, including:
Iliac crest pain syndrome
Multifidus triangle syndrome
Lumbar fascial fat herniation
Lumbosacral (sacrum) fat herniation
Episacral lipoma
Related Conditions
Iliac Crest Pain Syndrome
Also known as iliolumbar syndrome, iliac crest pain syndrome develops when a tear in the ligament occurs.
The ligament band connects the fourth and fifth lumbar vertebrae with the ilium on the same side. (Dąbrowski, K. Ciszek, B. 2023)
Causes include:
Tearing the ligament from repeated bending and twisting.
Trauma or fracture of the ilium bone caused by a fall or vehicle collision accident.
Multifidus Triangle Syndrome
Multifidus triangle syndrome develops when the multifidus muscles along the spine weaken and diminish function or ability.
These muscles can atrophy, and intramuscular fatty tissue can replace the muscle.
The lumbodorsal fascia is a thin fibrous membrane covering the back’s deep muscles.
Lumbar fascial fat herniation is a painful mass of fat that protrudes or herniates through the membrane, gets trapped and inflamed, and causes pain.
The causes of this type of herniation are currently unknown.
Lumbosacral (Sacrum) Fat Herniation
Lumbosacral describes where the lumbar spine meets the sacrum.
Lumbosacral fat herniation is a painful mass like lumbar facial herniation in a different location around the sacrum.
The causes of this type of herniation are currently unknown.
Episacral Lipoma
Episacral lipoma is a small painful nodule under the skin that primarily develops over the top outer edges of the pelvic bone. These lumps occur when a portion of the dorsal fat pad protrudes through a tear in the thoracodorsal fascia, the connective tissue that helps hold the back muscles in place. (Erdem, H. R. et al., 2013) A healthcare provider may refer an individual to an orthopedist or orthopedic surgeon for this lipoma. An individual may also find pain relief from a massage therapist familiar with the condition. (Erdem, H. R. et al., 2013)
Symptoms
Back lumps can often be seen under the skin. They are typically tender to the touch and can make sitting in a chair or lying on the back difficult, as they often appear on the hip bones and sacroiliac region. (Bicket, M. C. et al., 2016) The nodules may:
Be firm or tight.
Have an elastic feel.
Move under the skin when pressed.
Cause intense, severe pain.
The pain results from pressure on the lump, which compresses the nerves.
Damage to the underlying fascia can also cause pain symptoms.
Diagnosis
Some individuals do not realize they have nodules or lumps until pressure is applied. Chiropractors and massage therapists often find them during treatments but do not diagnose the abnormal fatty growth. The chiropractor or massage therapist will refer the patient to a qualified dermatologist or medical professional who can perform imaging studies and a biopsy. Determining what the lumps are can be challenging because they are non-specific. Healthcare providers sometimes diagnose the nodules by injecting them with a local anesthetic. (Bicket, M. C. et al., 2016)
Differential Diagnosis
The fatty deposits can be any number of things, and the same applies to the sources of nerve pain. A healthcare provider may further diagnose by ruling out other causes, which can include:
Sebaceous Cysts
A benign, fluid-filled capsule between the layers of skin.
Subcutaneous Abscess
A collection of pus beneath the skin.
Usually painful.
It can become inflamed.
Sciatica
Radiating nerve pain down one or both legs that is caused by a herniated disc, bone spur, or spasming muscles in the lower back.
Liposarcoma
Malignant tumors can sometimes appear as fatty growths in the muscles.
Liposarcoma is typically diagnosed by biopsy, where some tissue is removed from the nodule and examined for cancer cells. (Johns Hopkins Medicine. 2024)
An MRI or CT scan may also be performed to determine the exact location of the nodule.
Painful lipomas are also associated with fibromyalgia.
Treatment
Back nodules are usually benign, so there’s no reason to remove them unless they’re causing pain or mobility problems (American Academy of Orthopedic Surgeons: OrthoInfo. 2023). However, they should be examined to make sure they are not cancerous. Treatment usually involves injected anesthetics, such as lidocaine or corticosteroids, as well as over-the-counter pain relievers like NSAIDs.
Surgery
If pain is severe, surgical removal may be recommended. This involves cutting out the mass and repairing the fascia for lasting relief. However, removal may not be recommended if there are many nodules, as some individuals can have hundreds. Liposuction may be effective if the lumps are smaller, more extensive, and comprise more fluid. (American Family Physician. 2002) Complications of surgical removal can include:
Scarring
Bruising
Uneven skin texture
Infection
Complementary and Alternative Treatment
Complimentary and Alternative Medicine treatments like acupuncture, dry needling, and spinal manipulation can help. Many chiropractors believe back nodules can be successfully treated with complementary and alternative therapies. A common approach uses acupuncture and spinal manipulation in combination. A case study reported that anesthetic injections followed by dry needling, which is similar to acupuncture, improved pain relief. (Bicket, M. C. et al., 2016)
Injury Medical Chiropractic and Functional Medicine Clinic specializes in progressive therapies and functional rehabilitation procedures focused on restoring normal body functions after trauma and soft tissue injuries and the complete recovery process. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols. If the individual requires other treatment, they will be referred to a clinic or physician best suited for their condition, as Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers.
Beyond the Surface
References
Dąbrowski, K., & Ciszek, B. (2023). Anatomy and morphology of iliolumbar ligament. Surgical and radiologic anatomy : SRA, 45(2), 169–173. https://doi.org/10.1007/s00276-022-03070-y
Seyedhoseinpoor, T., Taghipour, M., Dadgoo, M., Sanjari, M. A., Takamjani, I. E., Kazemnejad, A., Khoshamooz, Y., & Hides, J. (2022). Alteration of lumbar muscle morphology and composition in relation to low back pain: a systematic review and meta-analysis. The spine journal : official journal of the North American Spine Society, 22(4), 660–676. https://doi.org/10.1016/j.spinee.2021.10.018
Erdem, H. R., Nacır, B., Özeri, Z., & Karagöz, A. (2013). Episakral lipoma: Bel ağrısının tedavi edilebilir bir nedeni [Episacral lipoma: a treatable cause of low back pain]. Agri : Agri (Algoloji) Dernegi’nin Yayin organidir = The journal of the Turkish Society of Algology, 25(2), 83–86. https://doi.org/10.5505/agri.2013.63626
Bicket, M. C., Simmons, C., & Zheng, Y. (2016). The Best-Laid Plans of “Back Mice” and Men: A Case Report and Literature Review of Episacroiliac Lipoma. Pain physician, 19(3), 181–188.
American Academy of Orthopedic Surgeons: OrthoInfo. (2023). Lipoma. https://orthoinfo.aaos.org/en/diseases–conditions/lipoma
American Family Physician. (2002). Lipoma excision. American Family Physician, 65(5), 901-905. https://www.aafp.org/pubs/afp/issues/2002/0301/p901.html
Individuals experiencing shooting, aching pain in the lower extremities, and intermittent leg pain could be suffering from neurogenic claudication. Can knowing the symptoms help healthcare providers develop an effective treatment plan?
Neurogenic Claudication
Neurogenic claudication occurs when spinal nerves become compressed in the lumbar or lower spine, causing intermittent leg pain. Compressed nerves in the lumbar spine can cause leg pain and cramps. The pain usually worsens with specific movements or activities like sitting, standing, or bending backward. It is also known as pseudo-claudication when the space within the lumbar spine narrows. A condition known as lumbar spinal stenosis. However, neurogenic claudication is a syndrome or group of symptoms caused by a pinched spinal nerve, while spinal stenosis describes the narrowing of the spinal passages.
Symptoms
Neurogenic claudication symptoms can include:
Leg cramping.
Numbness, tingling, or burning sensations.
Leg fatigue and weakness.
A sensation of heaviness in the leg/s.
Sharp, shooting, or aching pain extending into the lower extremities, often in both legs.
There may also be pain in the lower back or buttocks.
Neurogenic claudication is different from other types of leg pain, as the pain alternates – ceasing and beginning randomly and worsens with specific movements or activities. Standing, walking, descending stairs, or flexing backward can trigger pain, while sitting, climbing stairs, or leaning forward tends to relieve pain. However, every case is different. Over time, neurogenic claudication can affect mobility as individuals try to avoid activities that cause pain, including exercise, lifting objects, and prolonged walking. In severe cases, neurogenic claudication can make sleeping difficult.
Neurogenic claudication and sciatica are not the same. Neurogenic claudication involves nerve compression in the central canal of the lumbar spine, causing pain in both legs. Sciatica involves compression of nerve roots exiting from the sides of the lumbar spine, causing pain in one leg. (Carlo Ammendolia, 2014)
Causes
With neurogenic claudication, compressed spinal nerves are the underlying cause of the leg pain. In many cases, lumber spinal stenosis – LSS is the cause of pinched nerve. There are two types of lumbar spinal stenosis.
Central stenosis is the main cause of neurogenic claudication. With this type, the central canal of the lumbar spine, which houses the spinal cord, narrows, causing pain in both legs.
Lumbar spinal stenosis can be acquired and develop later in life due to spine deterioration.
Congenital means the individual is born with the condition.
Both can lead to neurogenic claudication in different ways.
Foramen stenosis is another type of lumbar spinal stenosis that causes the narrowing of spaces on either side of the lumbar spine where nerve roots branch off the spinal cord. The associated pain is different in that it is either in the right or left leg.
The pain corresponds to the side of the spinal cord where the nerves are being pinched.
Acquired Lumbar Spinal Stenosis
Lumbar spinal stenosis is usually acquired due to the degeneration of the lumbar spine and tends to affect older adults. The causes of the narrowing can include:
Spinal trauma, such as from a vehicle collision, work, or sports injury.
Disc herniation.
Spinal osteoporosis – wear-and-tear arthritis.
Ankylosing spondylitis – a type of inflammatory arthritis that affects the spine.
Osteophytes – bone spurs.
Spinal tumors – non-cancerous and cancerous tumors.
Congenital Lumbar Spinal Stenosis
Congenital lumbar spinal stenosis means an individual is born with abnormalities of the spine that may not be apparent at birth. Because the space within the spinal canal is already narrow, the spinal cord is vulnerable to any changes as the individual ages. Even individuals with mild arthritis can experience symptoms of neurogenic claudication early on and develop symptoms in their 30s and 40s instead of their 60s and 70s.
Diagnosis
Diagnosis of neurogenic claudication is largely based on the individual’s medical history, physical examination, and imaging. The physical examination and review identify where the pain is presenting and when. The healthcare provider may ask:
Is there a history of lower back pain?
Is the pain in one leg or both?
Is the pain constant?
Does the pain come and go?
Does the pain get better or worse when standing or sitting?
Do movements or activities cause pain symptoms and sensations?
Are there any usual sensations while walking?
Treatment
Treatments can consist of physical therapy, spinal steroid injections, and pain meds. Surgery is a last resort when all other therapies are unable to provide effective relief.
Physical Therapy
A treatment plan will involve physical therapy that includes:
Daily stretching
Strengthening
Aerobic exercises
This will help improve and stabilize the lower back muscles and correct posture problems.
Occupational therapy will recommend activity modifications that cause pain symptoms.
This includes proper body mechanics, energy conservation, and recognizing pain signals.
Back braces or belts may also be recommended.
Spinal Steroid Injections
Healthcare providers may recommend epidural steroid injections.
This delivers a cortisone steroid to the outermost section of the spinal column or the epidural space.
Pain medications are used to treat intermittent neurogenic claudication. These include:
Over-the-counter analgesics like acetaminophen.
Nonsteroidal anti-inflammatory drugs or NSAIDs like ibuprofen or naproxen.
Prescription NSAIDs may be prescribed if needed.
NSAIDs are used with chronic neurogenic pain and should only be used when required.
The long-term use of NSAIDs can increase the risk of stomach ulcers, and the overuse of acetaminophen can lead to liver toxicity and liver failure.
Surgery
If conservative treatments are unable to provide effective relief and mobility and/or quality of life are affected, surgery known as a laminectomy may be recommended to decompress the lumbar spine. The procedure may be performed:
Laparoscopically – with small incisions, scopes, and surgical instrumentation.
Open surgery – with a scalpel and sutures.
During the procedure, facets of the vertebra are partially or completely removed.
To provide stability, the bones are sometimes fused with screws, plates, or rods.
Success rates for both are more or less the same.
Between 85% and 90% of individuals undergoing the surgery achieve long-lasting and/or permanent pain relief. (Xin-Long Ma et al., 2017)
Movement Medicine: Chiropractic Care
References
Ammendolia C. (2014). Degenerative lumbar spinal stenosis and its imposters: three case studies. The Journal of the Canadian Chiropractic Association, 58(3), 312–319.
Munakomi S, Foris LA, Varacallo M. (2024). Spinal Stenosis and Neurogenic Claudication. [Updated 2023 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430872/
Ma, X. L., Zhao, X. W., Ma, J. X., Li, F., Wang, Y., & Lu, B. (2017). Effectiveness of surgery versus conservative treatment for lumbar spinal stenosis: A system review and meta-analysis of randomized controlled trials. International journal of surgery (London, England), 44, 329–338. https://doi.org/10.1016/j.ijsu.2017.07.032
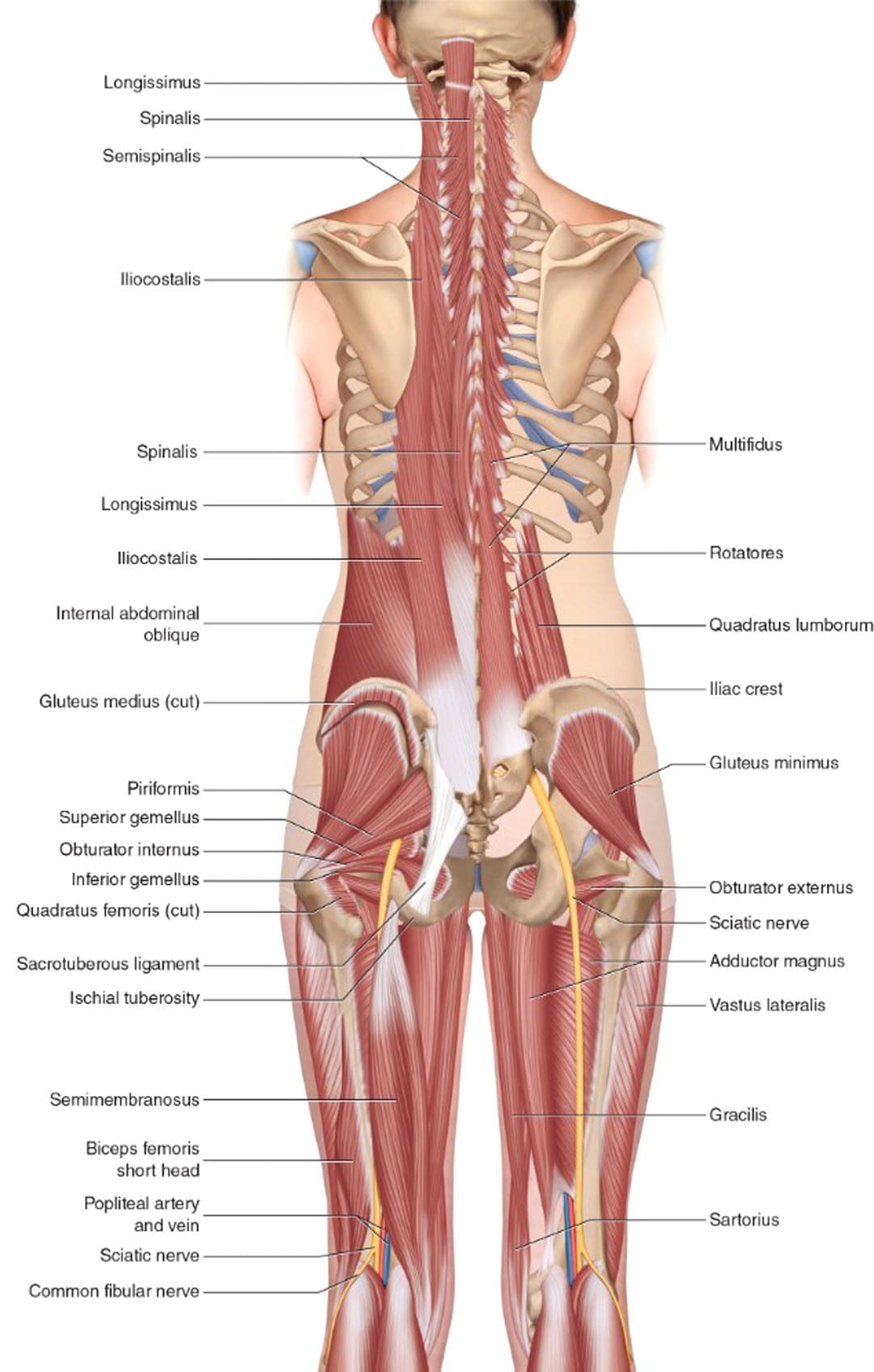
For individuals experiencing lower back pain can understanding the anatomy and function of the multifidus muscle help in injury prevention and in the development of a highly effective treatment plan?
Multifidus Muscle
The multifidus muscles are long and narrow on either side of the spinal column, which helps stabilize the lower region of the spine or lumbar spine. (Maryse Fortin, Luciana Gazzi Macedo 2013) Sitting too much, practicing unhealthy postures, and lack of movement can progress to the multifidus muscle weakening or atrophy, which can lead to spinal instability, vertebral compression, and back pain. (Paul W. Hodges, Lieven Danneels 2019)
Anatomy
Known as the deep layer, it is the innermost layer of the three muscle layers of the back and controls the movement of the spine. The other two layers, known as the intrinsic and superficial, are responsible for the thoracic cage/rib cage and shoulder movement. (Anouk Agten et al., 2020) The multifidus has attachment points at:
The thoracic spine of the middle back.
The lumbar spine of the lower back.
The iliac spine – the base of the wing-shaped iliac bone of the pelvis.
Sacrum – series of bones at the base of the spine connected to the tailbone.
When standing or moving, the multifidus muscle works with the transversus abdominus and pelvic floor muscles to stabilize the lumbar spine. (Christine Lynders 2019)
Muscle Function
The main function is to stabilize the lower back, but it also helps extend the lower spine whenever reaching or stretching. (Jennifer Padwal et al., 2020) Because the muscle has numerous attachment points and is serviced by a specific branch of nerves known as the posterior rami, it allows each vertebra to work individually and more efficiently.
The multifidus muscle works with two other deep muscle groups to stabilize and move the spine. (Jeffrey J Hebert et al., 2015)
The rotatores muscle enables unilateral rotation, turning from side to side, and bilateral extension or bending backward and forward.
The semispinalis muscle above the multifidus allows extension and rotation of the head, neck, and upper back.
The multifidus muscle ensures spinal strength because it has more attachment points to the spine than the other layers, which reduces spinal flexibility and rotation but increases strength and stability. (Anouk Agten et al., 2020)
Lower Back Pain
A weak multifidus muscle destabilizes the spine and provides less support to the vertebra. This adds pressure on muscles and connective tissues between and adjacent to the spinal column, increasing the risk of lower back pain symptoms. (Paul W. Hodges, Lieven Danneels 2019) The loss of muscle strength and stability can cause atrophy or wasting away. This can cause compression and other back problems. (Paul W. Hodges et al., 2015) Back problems associated with multifidus muscle deterioration include (Paul W. Hodges, Lieven Danneels 2019)
Herniated discs – also bulging or slipped discs.
Nerve entrapment or compression pinched nerve.
Sciatica
Referred pain – nerve pain originating from the spine felt in other areas.
Osteoarthritis – wear-and-tear arthritis
Spinal osteophytes – bone spurs
Weak abdominal or pelvic floor muscles can compromise the core, increasing the risk of chronic lower back pain and injury.
Individuals are recommended to consult a physical therapist and chiropractor who can help develop the appropriate treatment, rehabilitation, and strengthening plan based on age, injury, underlying conditions, and physical abilities.
Can Core Exercises Help with Back Pain?
References
Fortin, M., & Macedo, L. G. (2013). Multifidus and paraspinal muscle group cross-sectional areas of patients with low back pain and control patients: a systematic review with a focus on blinding. Physical therapy, 93(7), 873–888. https://doi.org/10.2522/ptj.20120457
Hodges, P. W., & Danneels, L. (2019). Changes in Structure and Function of the Back Muscles in Low Back Pain: Different Time Points, Observations, and Mechanisms. The Journal of orthopaedic and sports physical therapy, 49(6), 464–476. https://doi.org/10.2519/jospt.2019.8827
Agten, A., Stevens, S., Verbrugghe, J., Eijnde, B. O., Timmermans, A., & Vandenabeele, F. (2020). The lumbar multifidus is characterised by larger type I muscle fibres compared to the erector spinae. Anatomy & cell biology, 53(2), 143–150. https://doi.org/10.5115/acb.20.009
Lynders C. (2019). The Critical Role of Development of the Transversus Abdominis in the Prevention and Treatment of Low Back Pain. HSS journal : the musculoskeletal journal of Hospital for Special Surgery, 15(3), 214–220. https://doi.org/10.1007/s11420-019-09717-8
Padwal, J., Berry, D. B., Hubbard, J. C., Zlomislic, V., Allen, R. T., Garfin, S. R., Ward, S. R., & Shahidi, B. (2020). Regional differences between superficial and deep lumbar multifidus in patients with chronic lumbar spine pathology. BMC musculoskeletal disorders, 21(1), 764. https://doi.org/10.1186/s12891-020-03791-4
Hebert, J. J., Koppenhaver, S. L., Teyhen, D. S., Walker, B. F., & Fritz, J. M. (2015). The evaluation of lumbar multifidus muscle function via palpation: reliability and validity of a new clinical test. The spine journal : official journal of the North American Spine Society, 15(6), 1196–1202. https://doi.org/10.1016/j.spinee.2013.08.056
Hodges, P. W., James, G., Blomster, L., Hall, L., Schmid, A., Shu, C., Little, C., & Melrose, J. (2015). Multifidus Muscle Changes After Back Injury Are Characterized by Structural Remodeling of Muscle, Adipose and Connective Tissue, but Not Muscle Atrophy: Molecular and Morphological Evidence. Spine, 40(14), 1057–1071. https://doi.org/10.1097/BRS.0000000000000972
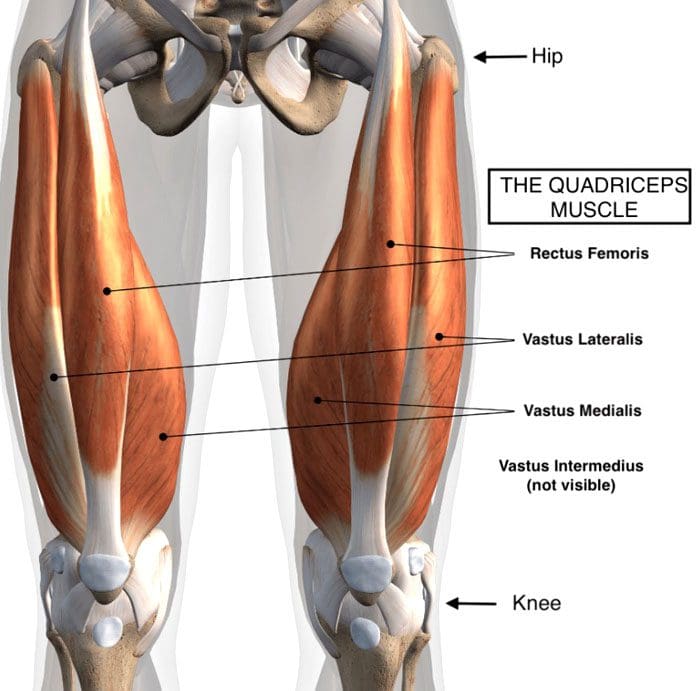
For individuals dealing with lower back pain, it could be quadricep muscle tightness causing the symptoms and posture problems. Can knowing the signs of quadricep tightness help prevent pain and avoid injury?
Quadriceps Tightness
Quadriceps muscles are in the front of the thigh. Forces that could be creating chronic pain and posture problems could be happening at the same time are:
Quadricep tightness causes lower back pain as the pelvis gets pulled down.
Tight quadriceps lead to weakened hamstring muscles.
These are the opposing muscles behind the thigh.
Stress and pressure on the hamstrings can cause back pain and problems.
The rectus femoris attaches to the pelvis at the anterior superior iliac spine, which is the front part of the hip bone.
The rectus femoris is the only muscle in the group that crosses over the hip joint, which also affects movement.
When the quadriceps, especially the rectus femoris, become tight, they pull down on the hips.
The pelvis tilts downward or forward, technically referred to as the anterior tilt of the pelvis. (Anita Król et al., 2017)
The spine is between the pelvis, and if the pelvis tilts forward, the lumbar spine compensates by arching.
A larger arch in the lower back is referred to as excessive lordosis and often causes tightness and pain in the back muscles. (Sean G. Sadler et al., 2017)
Hamstring Compensation
When the quadriceps tighten and the pelvis gets pulled down, the back has an abnormal lift. This puts the hamstring on a consistent stretch that can cause pain symptoms.
Healthy posture and hamstring muscle tone help maintain correct pelvic positioning in the back.
This is correct because it helps maintain a comfortable position.
Quadricep tightness can set off a reaction as the pelvis tilts down in front and up in the back while overly stretching the hamstrings.
Pain and soreness are the usual result
Lack of hamstring strength and quadriceps stretching can cause the hamstrings to lose their ability to support correct pelvic and spinal positions. (American Council on Exercise. 2015)
Knowing When Quads Are Tightening
Individuals often don’t realize their quadriceps are tight, especially those who spend most of the day sitting.
The more time spent in a chair can cause the quadriceps and lower back muscles to tighten steadily.
Individuals can try a few tests at home:
Standing Up
Push the hips forward.
Push from the sitting bones so you’re at the correct level.
How far forward do the hips go?
What is felt?
Pain could indicate tight quadriceps.
In A Lunge Position
With one leg forward and bent in front of the other.
The back leg is straight.
How far forward does the leg go?
What is felt?
How does the front of the hip on the back leg feel?
Standing Bent Leg
Stand with the front leg bent and the back leg straight.
Discomfort in the back leg could mean tight quadriceps.
In A Kneeling Position
Arch the back
Grab the ankles
Modify the position to adjust for any pain or joint issues.
If you have to prop yourself up or modify the pose to reduce pain, it could be tight quadriceps.
Helping to understand the condition can help in communication with a healthcare provider.
A healthcare provider and/or physical therapist can conduct a posture evaluation examination to test the quadriceps.
Understanding Academic Low Back Pain: Impact and Chiropractic Solutions
References
Kripa, S., Kaur, H. (2021). Identifying relations between posture and pain in lower back pain patients: a narrative review. Bulletin of Faculty of Physical Therapy, 26(34). https://doi.org/doi: 10.1186/s43161-021-00052-w
Król, A., Polak, M., Szczygieł, E., Wójcik, P., & Gleb, K. (2017). Relationship between mechanical factors and pelvic tilt in adults with and without low back pain. Journal of back and musculoskeletal rehabilitation, 30(4), 699–705. https://doi.org/10.3233/BMR-140177
Sadler, S. G., Spink, M. J., Ho, A., De Jonge, X. J., & Chuter, V. H. (2017). Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: a systematic review of prospective cohort studies. BMC musculoskeletal disorders, 18(1), 179. https://doi.org/10.1186/s12891-017-1534-0
American Council on Exercise. (2015). 3 Stretches for Opening Up Tight Hips (Fitness, Issue. https://www.acefitness.org/resources/everyone/blog/5681/3-stretches-for-opening-up-tight-hips/
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




 What the Fascia Does
What the Fascia Does