Individuals experiencing shooting, aching pain in the lower extremities, and intermittent leg pain could be suffering from neurogenic claudication. Can knowing the symptoms help healthcare providers develop an effective treatment plan?
Neurogenic Claudication
Neurogenic claudication occurs when spinal nerves become compressed in the lumbar or lower spine, causing intermittent leg pain. Compressed nerves in the lumbar spine can cause leg pain and cramps. The pain usually worsens with specific movements or activities like sitting, standing, or bending backward. It is also known as pseudo-claudication when the space within the lumbar spine narrows. A condition known as lumbar spinal stenosis. However, neurogenic claudication is a syndrome or group of symptoms caused by a pinched spinal nerve, while spinal stenosis describes the narrowing of the spinal passages.
Symptoms
Neurogenic claudication symptoms can include:
Leg cramping.
Numbness, tingling, or burning sensations.
Leg fatigue and weakness.
A sensation of heaviness in the leg/s.
Sharp, shooting, or aching pain extending into the lower extremities, often in both legs.
There may also be pain in the lower back or buttocks.
Neurogenic claudication is different from other types of leg pain, as the pain alternates – ceasing and beginning randomly and worsens with specific movements or activities. Standing, walking, descending stairs, or flexing backward can trigger pain, while sitting, climbing stairs, or leaning forward tends to relieve pain. However, every case is different. Over time, neurogenic claudication can affect mobility as individuals try to avoid activities that cause pain, including exercise, lifting objects, and prolonged walking. In severe cases, neurogenic claudication can make sleeping difficult.
Neurogenic claudication and sciatica are not the same. Neurogenic claudication involves nerve compression in the central canal of the lumbar spine, causing pain in both legs. Sciatica involves compression of nerve roots exiting from the sides of the lumbar spine, causing pain in one leg. (Carlo Ammendolia, 2014)
Causes
With neurogenic claudication, compressed spinal nerves are the underlying cause of the leg pain. In many cases, lumber spinal stenosis – LSS is the cause of pinched nerve. There are two types of lumbar spinal stenosis.
Central stenosis is the main cause of neurogenic claudication. With this type, the central canal of the lumbar spine, which houses the spinal cord, narrows, causing pain in both legs.
Lumbar spinal stenosis can be acquired and develop later in life due to spine deterioration.
Congenital means the individual is born with the condition.
Both can lead to neurogenic claudication in different ways.
Foramen stenosis is another type of lumbar spinal stenosis that causes the narrowing of spaces on either side of the lumbar spine where nerve roots branch off the spinal cord. The associated pain is different in that it is either in the right or left leg.
The pain corresponds to the side of the spinal cord where the nerves are being pinched.
Acquired Lumbar Spinal Stenosis
Lumbar spinal stenosis is usually acquired due to the degeneration of the lumbar spine and tends to affect older adults. The causes of the narrowing can include:
Spinal trauma, such as from a vehicle collision, work, or sports injury.
Disc herniation.
Spinal osteoporosis – wear-and-tear arthritis.
Ankylosing spondylitis – a type of inflammatory arthritis that affects the spine.
Osteophytes – bone spurs.
Spinal tumors – non-cancerous and cancerous tumors.
Congenital Lumbar Spinal Stenosis
Congenital lumbar spinal stenosis means an individual is born with abnormalities of the spine that may not be apparent at birth. Because the space within the spinal canal is already narrow, the spinal cord is vulnerable to any changes as the individual ages. Even individuals with mild arthritis can experience symptoms of neurogenic claudication early on and develop symptoms in their 30s and 40s instead of their 60s and 70s.
Diagnosis
Diagnosis of neurogenic claudication is largely based on the individual’s medical history, physical examination, and imaging. The physical examination and review identify where the pain is presenting and when. The healthcare provider may ask:
Is there a history of lower back pain?
Is the pain in one leg or both?
Is the pain constant?
Does the pain come and go?
Does the pain get better or worse when standing or sitting?
Do movements or activities cause pain symptoms and sensations?
Are there any usual sensations while walking?
Treatment
Treatments can consist of physical therapy, spinal steroid injections, and pain meds. Surgery is a last resort when all other therapies are unable to provide effective relief.
Physical Therapy
A treatment plan will involve physical therapy that includes:
Daily stretching
Strengthening
Aerobic exercises
This will help improve and stabilize the lower back muscles and correct posture problems.
Occupational therapy will recommend activity modifications that cause pain symptoms.
This includes proper body mechanics, energy conservation, and recognizing pain signals.
Back braces or belts may also be recommended.
Spinal Steroid Injections
Healthcare providers may recommend epidural steroid injections.
This delivers a cortisone steroid to the outermost section of the spinal column or the epidural space.
Pain medications are used to treat intermittent neurogenic claudication. These include:
Over-the-counter analgesics like acetaminophen.
Nonsteroidal anti-inflammatory drugs or NSAIDs like ibuprofen or naproxen.
Prescription NSAIDs may be prescribed if needed.
NSAIDs are used with chronic neurogenic pain and should only be used when required.
The long-term use of NSAIDs can increase the risk of stomach ulcers, and the overuse of acetaminophen can lead to liver toxicity and liver failure.
Surgery
If conservative treatments are unable to provide effective relief and mobility and/or quality of life are affected, surgery known as a laminectomy may be recommended to decompress the lumbar spine. The procedure may be performed:
Laparoscopically – with small incisions, scopes, and surgical instrumentation.
Open surgery – with a scalpel and sutures.
During the procedure, facets of the vertebra are partially or completely removed.
To provide stability, the bones are sometimes fused with screws, plates, or rods.
Success rates for both are more or less the same.
Between 85% and 90% of individuals undergoing the surgery achieve long-lasting and/or permanent pain relief. (Xin-Long Ma et al., 2017)
Movement Medicine: Chiropractic Care
References
Ammendolia C. (2014). Degenerative lumbar spinal stenosis and its imposters: three case studies. The Journal of the Canadian Chiropractic Association, 58(3), 312–319.
Munakomi S, Foris LA, Varacallo M. (2024). Spinal Stenosis and Neurogenic Claudication. [Updated 2023 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430872/
Ma, X. L., Zhao, X. W., Ma, J. X., Li, F., Wang, Y., & Lu, B. (2017). Effectiveness of surgery versus conservative treatment for lumbar spinal stenosis: A system review and meta-analysis of randomized controlled trials. International journal of surgery (London, England), 44, 329–338. https://doi.org/10.1016/j.ijsu.2017.07.032
Can individuals with leg and back pain find the relief by incorporating decompression to reduce pain-like associated symptoms?
Introduction
The lower extremities help stabilize the upper body’s weight and provide movement to the individual. The lower body portions include the lower back, pelvis, hips, thighs, legs, and feet, as they all have specific jobs to do and have an outstanding relationship with each other. However, their lower back and legs are susceptible to injuries. When environmental factors or injuries start to cause issues in the musculoskeletal system, it can lead to referred pain and overlapping risk profiles that can cause a person to have mobility and stability issues. The affected muscles, tissues, ligaments, and nerve roots can become irritated, weak, and tight when environmental factors start to compress the spine and lead to pain over time. Today’s article looks at how the back and legs work together in the body, how they are impacted by pain from environmental factors, and how spinal decompression can reduce leg and back pain. We talk with certified medical providers who consolidate our patients’ information to provide numerous treatments to minimize back and leg pain affecting their mobility. We also inform and guide patients on how treatments like decompression can help reduce pain-like symptoms within the legs and back. We encourage our patients to ask their associated medical providers intricated and important questions about the referred pain-like symptoms they are experiencing from their legs and since that is disrupting their daily routine. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
How The Back & Legs Work Together?
Do you feel radiating pain in your back that is affecting your ability to walk? Do you experience muscle aches or tiredness in your legs after a long workday? Or do you feel stiffness in your back and legs after waking up? Many of these scenarios are correlated with leg and back pain that can impact a person’s gait and lead to associated pain-like symptoms. The back and leg muscles work together through the sciatic nerve, a long nerve from the lumbar spinal region, past the gluteal muscles, traveling down the back of the legs and stopping at the knees. The back consists of the core muscles and the lumbar spinal region, allowing the person to bend, twist, and extend.
Meanwhile, the leg muscles help a person become mobile while stabilizing the person’s weight. These two muscle groups have an outstanding relationship in the lower extremities, as people need to be mobile when doing activities. However, they can also become vulnerable to injuries and pain that can cause disability issues.
How Pain Is Associated With The Back & Legs?
When it comes to the lower back and the legs, environmental factors and traumatic injuries can affect the surrounding muscles, tendons, ligaments, and nerve roots. For example, when working individuals routinely lift heavy objects, it can increase the risk of developing lower back pain while causing whole-body vibrations in the legs. (Becker & Childress, 2019) This is because what the heavy loading object does to the lower back is that it causes the spine to be compressed and contract the surrounding muscle. When it is repeated constantly, it can cause the spinal disc to herniate and aggravate the nerve roots. When these nerve roots become aggravated, it can lead to nerve entrapment and inflammation, thus causing individuals to experience chronic leg pain, foot drop, or ankle stability that affects their mobility. (Fortier et al., 2021)
Additionally, back and leg pain can even happen when the spine starts to experience degeneration, a natural process when the spinal disc shrinks over time. When the spinal disc in the lumbar spinal region degenerates over time, the nutrient supplies and changes in the extracellular composition cause the discs to be less capable of maintaining their load distribution function in the lower extremities. (Kim et al., 2020) However, many people who are experiencing leg and back pain can seek treatment to reduce the pain-like symptoms.
Chiropractic Care For Leg Instability- Video
Spinal Decompression Reducing Pain On The Legs & Back
When it comes to treating leg and back pain, many individuals will start to seek affordable treatment that can reduce pain-like symptoms. Many non-surgical treatments like spinal decompression are excellent for reducing pain that is affecting the back and legs. Spinal decompression uses a traction machine that can help stretch out the tight muscles from the lower back and provide negative pressure to the affected disc by increasing the blood nutrient flow back to the disc while reducing pressure off the aggravated nerve root. (Choi et al., 2022) Spinal decompression can be combined with core stabilizing exercises that can help reduce pain and disability and improve stability in the legs and lower extremities. (Hlaing et al., 2021) With spinal decompression to reduce back and leg pain, many individuals can notice positive results after consecutive treatment, and their mobility is improved. (Vanti et al., 2021) When individuals who are experiencing leg and back pain and are looking for treatment can find the benefits of spinal decompression to be incorporated into their daily routine since it can be customizable and help them be more mindful of what movements and environmental factors are causing them pain. Making these small changes over time can improve their health and help them live healthier lives.
References
Becker, B. A., & Childress, M. A. (2019). Nonspecific Low Back Pain and Return To Work. American Family Physician, 100(11), 697-703. https://www.ncbi.nlm.nih.gov/pubmed/31790184
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P. B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. https://doi.org/10.1155/2022/6343837
Fortier, L. M., Markel, M., Thomas, B. G., Sherman, W. F., Thomas, B. H., & Kaye, A. D. (2021). An Update on Peroneal Nerve Entrapment and Neuropathy. Orthop Rev (Pavia), 13(2), 24937. https://doi.org/10.52965/001c.24937
Hlaing, S. S., Puntumetakul, R., Khine, E. E., & Boucaut, R. (2021). Effects of core stabilization exercise and strengthening exercise on proprioception, balance, muscle thickness and pain related outcomes in patients with subacute nonspecific low back pain: a randomized controlled trial. BMC Musculoskelet Disord, 22(1), 998. https://doi.org/10.1186/s12891-021-04858-6
Kim, H. S., Wu, P. H., & Jang, I. T. (2020). Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature. Int J Mol Sci, 21(4). https://doi.org/10.3390/ijms21041483
Vanti, C., Turone, L., Panizzolo, A., Guccione, A. A., Bertozzi, L., & Pillastrini, P. (2021). Vertical traction for lumbar radiculopathy: a systematic review. Arch Physiother, 11(1), 7. https://doi.org/10.1186/s40945-021-00102-5
Individuals suffering from hip, thigh, and/or groin pain could be experiencing iliopsoas syndrome. Could knowing the symptoms and causes help in diagnosis and treatment?
Iliopsoas Syndrome
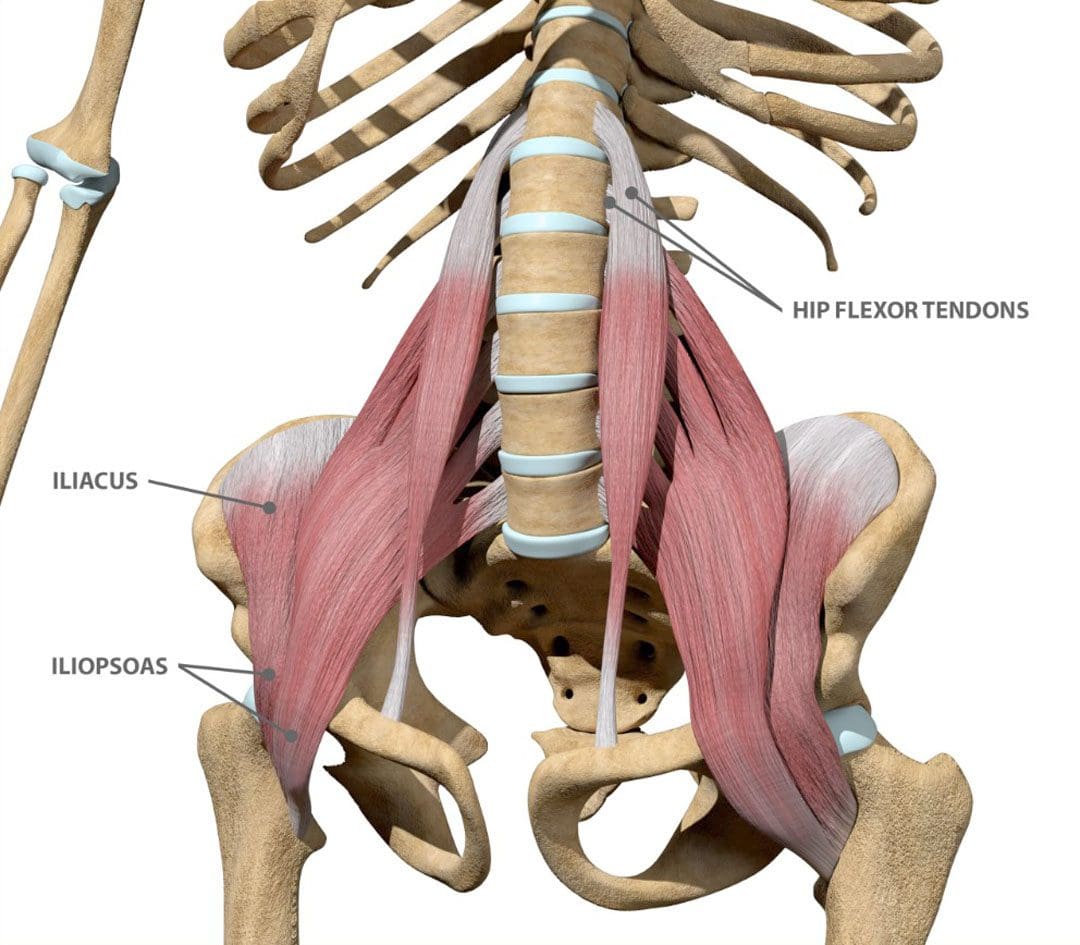
Iliopsoas syndrome encompasses several conditions that affect the inner hip muscle and can cause hip and thigh pain. The muscle helps to bend the leg toward the body.
The condition is usually caused by overuse injuries and commonly affects individuals who perform repeated hip flexion movements, like cyclists, gymnasts, dancers, runners, and soccer players. (Liran Lifshitz, et al., 2020)
The term is often used interchangeably with psoas syndrome, iliopsoas tendonitis, snapping hip syndrome, and iliopsoas bursitis. However, there are clinical differences.
Hip or groin clicking or snapping that can be heard and/or felt during movement.
Pain and/or stiffness in the hip and thigh area.
Pain that worsens when bending the hip – walking, climbing stairs, squatting, sitting.
Movements that involve bringing the knee toward the chest can worsen the pain.
Causes
The iliopsoas muscles are hip muscles on the front of the hip. They are made up of the psoas major, the psoas minor, and the iliacus. Small, fluid-filled sacs/bursae are within the hip joint between bones and soft tissues. The bursae reduce friction and provide cushioning to help the tendons, muscles, and other structures move smoothly over the bony prominences.
Iliopsoas bursitis happens when the bursa, which is located between the iliopsoas tendon and the inside of the hip joint, becomes inflamed and irritated.
Iliopsoas tendonitis/hip tendonitis happens when the tendon that attaches the thigh bone to the iliopsoas muscle becomes inflamed and irritated.
Iliopsoas bursitis and tendonitis are commonly caused by overuse injuries and intense activities like cycling, running, rowing, or strength training.
Diagnosis
Healthcare providers can diagnose iliopsoas syndrome based on symptom history and a hip examination.
Imaging tests – MRI and X-rays may be used to rule out other injuries or conditions like muscle tears. (Paul Walker, et al., 2021)
Avoid putting weight on the hip for a few days after the injury.
Ice
Apply ice immediately after the injury to bring the swelling down.
Use a cold pack for 20 minutes at a time, several times a day.
Do not apply ice directly on the skin.
Compression
Wrap the area in a soft bandage or use compression shorts to prevent further swelling.
Elevation
Rest as often as possible with the leg raised higher than the heart.
Medical Treatment
Non-steroidal anti-inflammatory drugs like ibuprofen and naproxen sodium can alleviate pain and reduce inflammation. (Paul Walker, et al., 2021)
Steroid injections can be used if symptoms continue or come back with additional injections administered as necessary. (Paul Walker, et al., 2021)
After pain and swelling subside, physical therapy may be recommended, as well as mild exercises to gradually improve hip strength and flexibility. (Paul Walker, et al., 2021)
A healthcare provider may recommend surgery in severe cases where pain persists, and conservative treatments don’t provide enough relief.
Lifshitz, L., Bar Sela, S., Gal, N., Martin, R., & Fleitman Klar, M. (2020). Iliopsoas the Hidden Muscle: Anatomy, Diagnosis, and Treatment. Current sports medicine reports, 19(6), 235–243. https://doi.org/10.1249/JSR.0000000000000723
Walker, P., Ellis, E., Scofield, J., Kongchum, T., Sherman, W. F., & Kaye, A. D. (2021). Snapping Hip Syndrome: A Comprehensive Update. Orthopedic reviews, 13(2), 25088. https://doi.org/10.52965/001c.25088
American Association of Orthopedic Surgeons. OrthoInfo. Hip strains.
Can combining chiropractic treatment with the common therapies of medication, exercise, and/or physical therapy help relieve sciatic endometriosis pain symptoms?
Sciatic Endometriosis
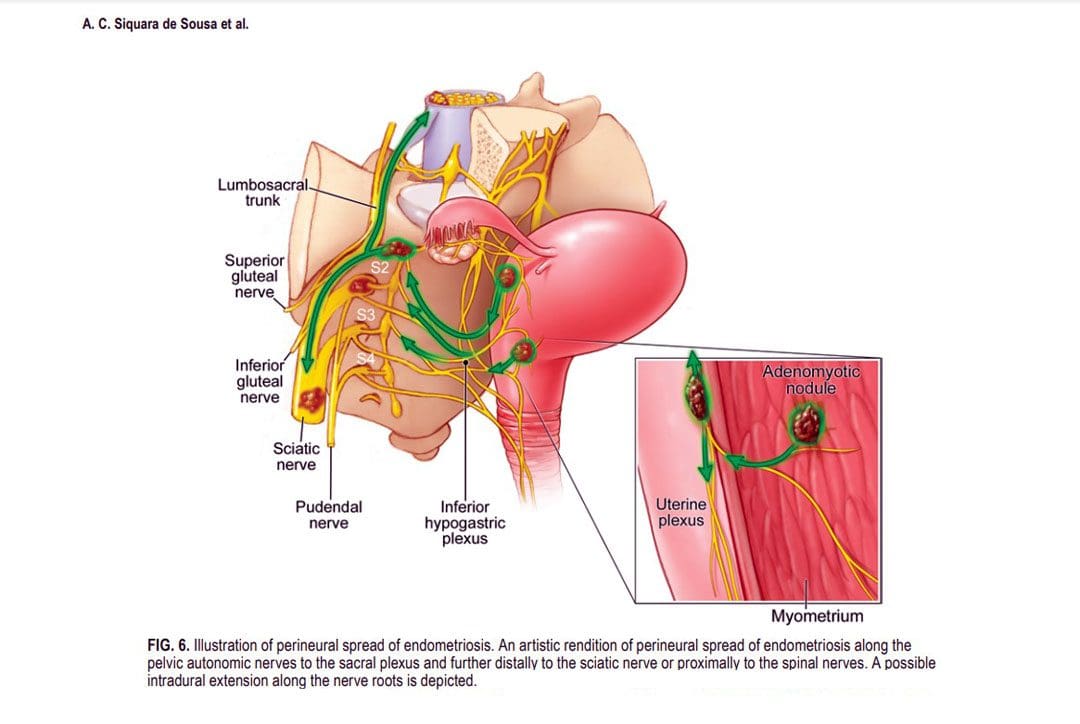
Sciatic endometriosis is a condition in which endometrial cells (tissue that resembles the lining of the uterus) grow outside of the uterine lining and compress the sciatic nerve. This places stress and pressure on the nerve causing back, pelvic, hip, and leg pain, especially before and during the menstrual cycle. It can also cause pain, irregular periods, and infertility. (The American College of Obstetricians and Gynecologists. 2021)
These areas of endometrial tissue growth are also known as lesions or implants.
Women with sciatic endometriosis often experience leg pain and weakness around the time of their menstrual cycle. (Lena Marie Seegers, et al., 2023)
Sciatic endometriosis can also cause pain when urinating, during a bowel movement, during sex, and fatigue, and irregular vaginal bleeding.
The abnormal growth may be caused by higher-than-normal levels of estrogen.
Researchers believe that endometriosis is related to retrograde menstruation, which causes menstrual blood to flow back into the pelvis instead of out through the vagina. (World Health Organization. 2023)
Sometimes, the cells grow in the area of the pelvis right above the sciatic nerve. (Adaiah Yahaya, et al., 2021)
The sciatic nerve is the longest nerve in the body and travels down the back of each leg. (Johns Hopkins Medicine. 2023)
When endometrial lesions place pressure on the sciatic nerve, they can cause irritation and inflammation leading to severe pelvic pain, which makes it harder to conceive. (Liang Yanchun, et al., 2019)
Symptoms
Some women with endometriosis experience no symptoms or misinterpret the symptoms as typical premenstrual syndrome/PMS signs. The most common signs and symptoms of sciatic endometriosis include:
Difficulty walking or standing.
Loss of sensation, muscle weakness, and reflex alteration.
Limping.
Balance problems.
Bloating and nausea.
Constipation or diarrhea before or after a period.
Painful, heavy, and/or irregular periods.
Bleeding between periods.
Pain during sex, urination, and bowel movements.
Pain in the stomach, pelvis, lower back, hips, and buttocks. (MedlinePlus. 2022)
Weakness, numbness, tingling, burning, or dull aching sensations in the back of one or both legs.
Endometriosis, including sciatic endometriosis, typically cannot be diagnosed with a pelvic examination or ultrasound by themselves. A healthcare provider may need to perform a biopsy using laparoscopy and discuss menstrual cycles, symptoms, and medical history.
The laparoscopy procedure involves making tiny incisions and taking a tissue sample with tools attached to a thin tube with a camera. (MedlinePlus. 2022)
Imaging tests, like magnetic resonance imaging/MRI, and computed tomography/CT scans, can help provide essential information about the location and size of any endometrial lesions. (The American College of Obstetricians and Gynecologists. 2021)
Treatment
Symptoms can sometimes be temporarily relieved with over-the-counter/OTC pain relievers. Depending on the condition and severity a healthcare provider may prescribe hormonal treatment to prevent new endometrial implants from growing. These can include:
Hormonal birth control.
Progestin – a synthetic form of progesterone.
Gonadotropin-releasing hormone – GnRH agonists.
If pain persists or worsens, individuals may need to undergo surgery to remove the tissue.
The American College of Obstetricians and Gynecologists. Endometriosis.
Seegers, L. M., DeFaria Yeh, D., Yonetsu, T., Sugiyama, T., Minami, Y., Soeda, T., Araki, M., Nakajima, A., Yuki, H., Kinoshita, D., Suzuki, K., Niida, T., Lee, H., McNulty, I., Nakamura, S., Kakuta, T., Fuster, V., & Jang, I. K. (2023). Sex Differences in Coronary Atherosclerotic Phenotype and Healing Pattern on Optical Coherence Tomography Imaging. Circulation. Cardiovascular imaging, 16(8), e015227. https://doi.org/10.1161/CIRCIMAGING.123.015227
World Health Organization. Endometriosis.
Yahaya, A., Chauhan, G., Idowu, A., Sumathi, V., Botchu, R., & Evans, S. (2021). Carcinoma arising within sciatic nerve endometriosis: a case report. Journal of surgical case reports, 2021(12), rjab512. https://doi.org/10.1093/jscr/rjab512
Johns Hopkins Medicine. Sciatica.
Yanchun, L., Yunhe, Z., Meng, X., Shuqin, C., Qingtang, Z., & Shuzhong, Y. (2019). Removal of an endometrioma passing through the left greater sciatic foramen using a concomitant laparoscopic and transgluteal approach: case report. BMC women’s health, 19(1), 95. https://doi.org/10.1186/s12905-019-0796-0
MedlinePlus. Endometriosis.
Center for Endometriosis Care. Sciatic endometriosis.
Chen, S., Xie, W., Strong, J. A., Jiang, J., & Zhang, J. M. (2016). Sciatic endometriosis induces mechanical hypersensitivity, segmental nerve damage, and robust local inflammation in rats. European journal of pain (London, England), 20(7), 1044–1057. https://doi.org/10.1002/ejp.827
Siquara de Sousa, A. C., Capek, S., Howe, B. M., Jentoft, M. E., Amrami, K. K., & Spinner, R. J. (2015). Magnetic resonance imaging evidence for perineural spread of endometriosis to the lumbosacral plexus: report of 2 cases. Neurosurgical focus, 39(3), E15. https://doi.org/10.3171/2015.6.FOCUS15208
How does spinal decompression help reduce somatosensory pain associated with individuals dealing with back and leg pain?
Introduction
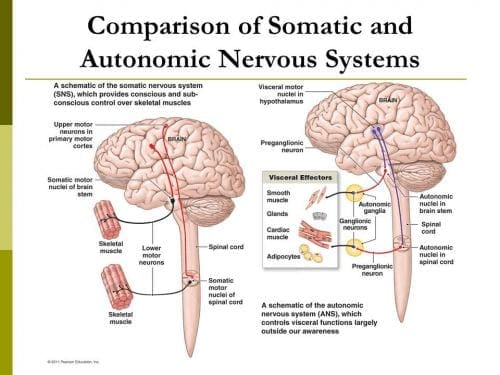
As we all know, the human body is a complex system that works together to perform various actions without feeling pain or discomfort. With muscles, organs, tissues, ligaments, bones, and nerve roots, each component has its job and interacts with other body parts. For instance, the spine collaborates with the central nervous system to instruct the muscles and organs to function correctly. Meanwhile, the nerve roots and muscles work together to provide mobility, stability, and flexibility to the upper and lower body extremities. However, as time passes, the body ages naturally, and this can lead to unwanted issues. Normal and traumatic factors can interfere with the neuron signals from the brain and cause somatosensory pain in the upper and lower extremities. This pain-like sensation can affect each body section, making the individual miserable. Luckily, there are ways to reduce somatosensory pain and provide relief to the body. Today’s article explores how somatosensory pain can impact the lower extremities, particularly the legs and back, and how non-surgical treatments like spinal decompression can alleviate somatosensory pain in the lower extremities. At the same time, we work hand-in-hand with certified medical providers who use our patient’s information to treat and mitigate somatosensory pain affecting the legs and back. We also inform them that non-surgical treatments like spinal decompression can help alleviate residual pain-like symptoms from the lower extremities. We encourage our patients to ask essential and important questions while seeking education from our associated medical providers about their pain. Dr. Alex Jimenez, D.C., incorporates this information as an educational service. Disclaimer
How Does Somatosensory Pain Affect The Legs & Back?
Are you experiencing numbness or tingling in your legs or back that disappears after a few minutes? Do you feel questionable pain in your lumbar spine after work? Or do you feel a warm sensation in the back of your legs that turns into sharp shooting pain? These issues may be related to the somatosensory system within the central nervous system, which provides voluntary reflexes to muscle groups. When normal movements or traumatic forces cause problems to the somatosensory system over time, it can lead to pain that affects the body’s extremities. (Finnerup, Kuner, & Jensen, 2021) This pain may be accompanied by burning, pricking, or squeezing sensations that affect the lumbar region. Many factors can be associated with somatosensory pain, which is part of the central nervous system and works with the spinal cord. When the spinal cord becomes compressed or aggravated due to injury or normal factors, it can lead to low back and leg pain. For example, a herniated disc in the lumbosacral area can cause nerve roots to send pain signals to the brain and cause abnormalities in the back and legs. (Aminoff & Goodin, 1988)
When people are dealing with back and leg pain from somatosensory pain, it can cause them to be miserable by reducing their quality of life and leading to a life of disability. (Rosenberger et al., 2020) At the same time, individuals dealing with somatosensory pain will also begin to feel inflammatory effects from the affected muscle area in the legs and back. Since inflammation is a body’s natural response when dealing with pain, the inflammatory cytokines can cause a cascading effect from the brain through the spinal cord, causing leg and back pain. (Matsuda, Huh, & Ji, 2019) To that point, somatosensory pain is associated with inflammation caused by normal or traumatic factors that can cause overlapping risk factors contributing to leg and back pain. Luckily, numerous treatments can reduce these overlapping risk factors caused by somatosensory pain and help restore the lower body extremities’ function.
Move Better, Live Better- Video
When the body is dealing with somatosensory pain, it can cause many individuals to think they are only dealing with one source of pain from one muscle area. Still, it can lead to multifactorial issues that affect different body locations. This is known as referred pain, where one body section deals with pain but is in a different area. Referred pain can also be combined with somato-visceral/visceral-somatic pain, where the affected muscle or organ affects one or the other, causing more pain-like issues. However, numerous treatments can reduce somatosensory pain from causing more leg and back problems. Non-surgical therapies like chiropractic care and spinal decompression can help mitigate the effects of somatosensory pain affecting the lower body extremities causing leg and back pain. These treatments allow the pain specialist to incorporate various therapeutic techniques to stretch the affected muscles and realign the spine to its original position. Many individuals can see an improvement in their mobility and daily activities as the pain-like symptoms associated with somatosensory pain are reduced. (Gose, Naguszewski, & Naguszewski, 1998) When individuals dealing with somatosensory pain start thinking about their health and wellness to ease the pain they are experiencing, they can look into non-surgical treatments as they are cost-effective, safe, and provide a positive outcome. Additionally, non-surgical treatments can be personalized to the individual’s pain and begin to see improvement after a few treatment sessions. (Saal & Saal, 1989) Check out the video above to learn more about how non-surgical treatments can be combined with other therapies to improve a person’s well-being.
Spinal Decompression Reduces Somatosenosory Pain
Now spinal decompression is a non-surgical treatment that can help reduce somatosensory pain affecting the legs and back. Since somatosensory pain correlates with the spinal cord, it can affect the lumbosacral spine and lead to back and leg pain. With spinal decompression, it utilizes gentle traction to gently pull the spine, which then can reduce the symptoms associated with somatosensory pain. Spinal decompression can help improve the somatosensory system by reducing pain and alleviating aggravated nerve root compression to relieve the legs and back. (Daniel, 2007)
Additionally, spinal decompression can be combined with other non-surgical treatments, like chiropractic, as it can help with reducing the effects of nerve entrapment and help restore the joint’s ROM (range of motion). (Kirkaldy-Willis & Cassidy, 1985) Spinal decompression can create a positive experience for many individuals dealing with leg and back pain associated with somatosensory pain while getting back their health and wellness.
References
Aminoff, M. J., & Goodin, D. S. (1988). Dermatomal somatosensory evoked potentials in lumbosacral root compression. J Neurol Neurosurg Psychiatry, 51(5), 740-742. https://doi.org/10.1136/jnnp.51.5.740-a
Daniel, D. M. (2007). Non-surgical spinal decompression therapy: does the scientific literature support efficacy claims made in the advertising media? Chiropr Osteopat, 15, 7. https://doi.org/10.1186/1746-1340-15-7
Finnerup, N. B., Kuner, R., & Jensen, T. S. (2021). Neuropathic Pain: From Mechanisms to Treatment. Physiol Rev, 101(1), 259-301. https://doi.org/10.1152/physrev.00045.2019
Gose, E. E., Naguszewski, W. K., & Naguszewski, R. K. (1998). Vertebral axial decompression therapy for pain associated with herniated or degenerated discs or facet syndrome: an outcome study. Neurol Res, 20(3), 186-190. https://doi.org/10.1080/01616412.1998.11740504
Kirkaldy-Willis, W. H., & Cassidy, J. D. (1985). Spinal manipulation in the treatment of low-back pain. Can Fam Physician, 31, 535-540. https://www.ncbi.nlm.nih.gov/pubmed/21274223
Matsuda, M., Huh, Y., & Ji, R. R. (2019). Roles of inflammation, neurogenic inflammation, and neuroinflammation in pain. J Anesth, 33(1), 131-139. https://doi.org/10.1007/s00540-018-2579-4
Rosenberger, D. C., Blechschmidt, V., Timmerman, H., Wolff, A., & Treede, R. D. (2020). Challenges of neuropathic pain: focus on diabetic neuropathy. J Neural Transm (Vienna), 127(4), 589-624. https://doi.org/10.1007/s00702-020-02145-7
Saal, J. A., & Saal, J. S. (1989). Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy. An outcome study. Spine (Phila Pa 1976), 14(4), 431-437. https://doi.org/10.1097/00007632-198904000-00018
The lumbosacral plexus is located on the posterolateral wall of the lesser pelvis, next to the lumbar spine. A plexus is a network of intersecting nerves that share roots, branches, and functions. The sacral plexus is a network that emerges from the lower part of the spine. The plexus then embeds itself into the psoas major muscle and emerges in the pelvis. These nerves provide motor control to and receive sensory information from portions of the pelvis and leg. Sacral nerve discomfort symptoms, numbness, or other sensations and pain can be caused by an injury, especially if the nerve roots are compressed, tangled, rubbing, and irritated. This can cause symptoms like back pain, pain in the back and sides of the legs, sensory issues affecting the groin and buttocks, and bladder or bowel problems. Injury Medical Chiropractic and Functional Medicine Clinic can develop a personalized treatment plan to relieve symptoms, release the nerves, relax the muscles, and restore function.
Sacral Plexus
Anatomy
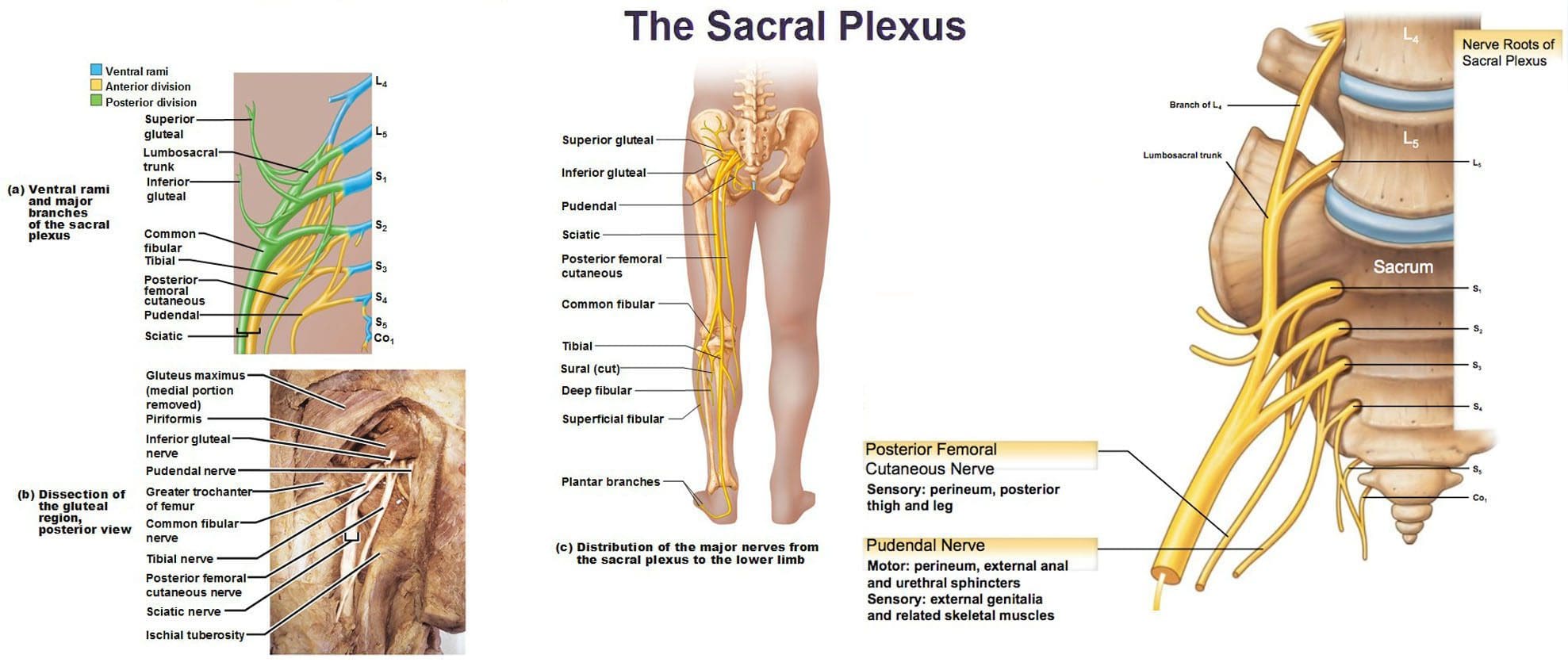
The sacral plexus is formed by the lumbar spinal nerves, L4 and L5, and sacral nerves S1 through S4.
Several combinations of these spinal nerves merge together and then divide into the branches of the sacral plexus.
Everybody has two sacral plexi – plural of plexus – one on the right side and left side that is symmetrical in structure and function.
Structure
There are several plexi throughout the body. The sacral plexus covers a large area of the body in terms of motor and sensory nerve function.
Spinal nerves L4 and L5 make up the lumbosacral trunk, and the anterior rami of sacral spinal nerves S1, S2, S3, and S4 join the lumbosacral trunk to form the sacral plexus.
Anterior rami are the branches of the nerve that are towards the front of the spinal cord/front of the body.
At each spinal level, an anterior motor root and a posterior sensory root join to form a spinal nerve.
Each spinal nerve then divides into an anterior – ventral – and a posterior – dorsal – rami portion.
Each can have motor and/or sensory functions.
The sacral plexus divides into several nerve branches, which include:
Superior gluteal nerve – L4, L5, and S1.
Inferior gluteal nerve – L5, S1, and S2.
The sciatic nerve – is the largest nerve of the sacral plexus and among the largest nerves in the body – L4, L5, S1, S2, and S3
The common fibular nerve – L4 through S2, and tibial nerves – L4 through S3 are branches of the sciatic nerve.
Posterior femoral cutaneous nerve – S1, S2, and S3.
Pudendal nerve – S2, S3, and S4.
The nerve to the quadratus femoris muscle is formed by L4, L5, and S1.
The obturator internus muscle nerve – L5, S1, and S2.
The piriformis muscle nerve – S1 and S2.
Function
The sacral plexus has substantial functions throughout the pelvis and legs. The branches provide nerve stimulation to several muscles. The sacral plexus nerve branches also receive sensory messages from the skin, joints, and structures of the pelvis and legs.
Motor
Motor nerves of the sacral plexus receive signals from the brain that travel down the column of the spine, out to the motor nerve branches of the sacral plexus to stimulate muscle contraction and movement. Motor nerves of the sacral plexus include:
Superior Gluteal Nerve
This nerve provides stimulation to the gluteus minimus, gluteus medius, and tensor fascia lata, which are muscles that help move the hip away from the center of the body.
Inferior Gluteal Nerve
This nerve provides stimulation to the gluteus maximus, the large muscle that moves the hip laterally.
Sciatic Nerve
The sciatic nerve has a tibial portion and a common fibular portion, which have motor and sensory functions.
The tibial portion stimulates the inner part of the thigh and activates muscles in the back of the leg and the sole of the foot.
The common fibular portion of the sciatic nerve stimulates and moves the thigh and knee.
The common fibular nerve stimulates muscles in the front and sides of the legs and extends the toes to straighten them out.
Pudendal Nerve
The pudendal nerve also has sensory functions that stimulate the muscles of the urethral sphincter to control urination and the muscles of the anal sphincter to control defecation.
The nerve to the quadratus femoris stimulates the muscle to move the thigh.
The nerve to the obturator internus muscle stimulates the muscle to rotate the hips and stabilize the body when walking.
The nerve to the piriformis muscle stimulates the muscle to move the thigh away from the body.
Conditions
The sacral plexus, or areas of the plexus, can be affected by disease, traumatic injury, or cancer. Because the nerve network has many branches and portions, symptoms can be confusing. Individuals may experience sensory loss or pain in regions in the pelvis and leg, with or without muscle weakness. Conditions that affect the sacral plexus include:
Injury
A traumatic injury of the pelvis can stretch, tear, or harm the sacral plexus nerves.
Bleeding can inflame and compress the nerves, causing malfunction.
Neuropathy
Nerve impairment can affect the sacral plexus or parts of it.
Neuropathy can come from:
Diabetes
Vitamin B12 deficiency
Certain medications – chemotherapeutic meds
Toxins like lead
Alcohol
Metabolic illnesses
Infection
An infection of the spine or the pelvic region can spread to the sacral plexus nerves or produce an abscess, causing symptoms of nerve impairment, pain, tenderness, and sensations around the infected region.
Cancer
Cancer developing in the pelvis or spreading to the pelvis from somewhere else can compress or infect the sacral plexus nerves.
Treatment of the Underlying Medical Condition
Rehabilitation begins with the treatment of the underlying medical condition causing the nerve problems.
Cancer treatment – surgery, chemotherapy, and/or radiation.
Antibiotic treatment for infections.
Neuropathy treatment can be complicated because the cause may be unclear, and an individual can experience several causes of neuropathy simultaneously.
Major pelvic trauma like a vehicle collision can take months, especially if there are multiple bone fractures.
Motor and Sensory Recovery
Sensory problems can interfere with walking, standing, and sitting.
Adapting to sensory deficits is an important part of treatment, rehabilitation, and recovery.
Chiropractic, decompression, massage, and physical therapy can relieve symptoms, restore strength, function, and motor control.
Sciatica Secrets Revealed
References
Dujardin, Franck et al. “Extended anterolateral transiliac approach to the sacral plexus.” Orthopaedics & traumatology, surgery & research: OTSR vol. 106,5 (2020): 841-844. doi:10.1016/j.otsr.2020.04.011
Eggleton JS, Cunha B. Anatomy, Abdomen and Pelvis, Pelvic Outlet. [Updated 2022 Aug 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557602/
Garozzo, Debora et al. “In lumbosacral plexus injuries can we identify indicators that predict spontaneous recovery or the need for surgical treatment? Results from a clinical study on 72 patients.” Journal of brachial plexus and peripheral nerve injury vol. 9,1 1. 11 Jan. 2014, doi:10.1186/1749-7221-9-1
Gasparotti R, Shah L. Brachial and Lumbosacral Plexus and Peripheral Nerves. 2020 Feb 15. In: Hodler J, Kubik-Huch RA, von Schulthess GK, editors. Diseases of the Brain, Head and Neck, Spine 2020–2023: Diagnostic Imaging [Internet]. Cham (CH): Springer; 2020. Chapter 20. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554335/ doi: 10.1007/978-3-030-38490-6_20
Norderval, Stig, et al. “Sacral nerve stimulation.” Tidsskrift for den Norske laegeforening : tidsskrift for praktisk medicin, ny raekke vol. 131,12 (2011): 1190-3. doi:10.4045/tidsskr.10.1417
Neufeld, Ethan A et al. “MR Imaging of the Lumbosacral Plexus: A Review of Techniques and Pathologies.” Journal of Neuroimaging: official journal of the American Society of Neuroimaging vol. 25,5 (2015): 691-703. doi:10.1111/jon.12253
Staff, Nathan P, and Anthony J Windebank. “Peripheral neuropathy due to vitamin deficiency, toxins, and medications.” Continuum (Minneapolis, Minn.) vol. 20,5 Peripheral Nervous System Disorders (2014): 1293-306. doi:10.1212/01.CON.0000455880.06675.5a
Yin, Gang, et al. “Obturator Nerve Transfer to the Branch of the Tibial Nerve Innervating the Gastrocnemius Muscle for the Treatment of Sacral Plexus Nerve Injury.” Neurosurgery vol. 78,4 (2016): 546-51. doi:10.1227/NEU.0000000000001166
Lying down on the couch or bed when the lower leg seizes with intense sensations and pain that doesn’t stop, and the muscle could be hard to the touch. When trying to move the leg, it feels paralyzed. Nocturnal leg cramps, called muscle spasms or Charley horses, occur when one or more leg muscles tighten involuntarily. Individuals can be awake or asleep when a leg cramp strikes. Chiropractic treatment, decompression, and massage therapies can help relieve symptoms, stretch and relax the muscles, and restore function and health.
Nocturnal Leg Cramps
Nocturnal leg cramps most often affect the gastrocnemius/calf muscle. However, they can also affect the muscles in the front of the thigh/quadriceps and the back of the thigh/hamstrings.
Often, the tight muscle relaxes in less than 10 minutes.
The leg and area can feel sore and tender afterward.
Frequent calf cramps at night can cause sleep problems.
Nocturnal leg cramps are more common among women and older adults.
Causes
There are no known exact cause/s, making most cases idiopathic. However, there are known factors that can increase the risk. These can include:
Prolonged Sitting and Position
Sitting with the legs crossed or the toes pointed for long periods shortens/pulls the calf muscles, which can cause cramping.
Prolonged Standing and Posture
Individuals standing for long periods are likelier to experience nocturnal cramps from the stressed muscles.
Muscle Overexertion
Too much exercise can create an overworked muscle and can contribute to cramps.
Muscles need to be stretched regularly to function correctly.
Lack of physical activity for long periods weakens the muscles, making them more susceptible to injury.
Shortening The Tendons
The tendons, which connect muscles and bones, shorten naturally over time.
Without stretching, this could lead to cramping.
Cramps may be related to foot position when sleeping, with the feet and toes extending away from the body, known as plantar flexion.
This shortens the calf muscles, making them more susceptible to cramping.
Leg cramps at night are unlikely a sign of a more serious medical condition, but they are associated with the following conditions:
Musculoskeletal disorders.
Structural issues – flat feet or spinal stenosis.
Metabolic disorders like diabetes.
Pregnancy.
Medications – statins and diuretics.
Neurological disorders, like motor neuron disease or peripheral neuropathy.
Neurodegenerative disorders.
Liver, kidney, and thyroid conditions.
Cardiovascular conditions.
Chiropractic and Physical Therapy
Rehabilitation with chiropractic, massage, and physical therapy depends on the severity of the injury and condition. A chiropractic treatment plan can include the following:
Calf muscle stretching.
Targeted Stretch Exercises.
Progressive calf stretching exercises – a regular stretching and flexibility program will increase the range of motion and prevent future calf injuries.
Foam rolling – gentle self-massage with a foam roller can help reduce spasms and improve blood circulation.
Percussive massage.
Muscle strengthening exercises will build muscle strength and coordination to prevent future strain injuries.
At-home therapy can include:
Maintain Hydration
Fluids allow for normal muscle function.
Individuals may need to adjust how much fluid is drunk based on weather, age, activity level, and medications.
Change Sleeping Position
Individuals should avoid sleeping in positions in which the feet are pointing downward.
Try sleeping on the back with a pillow behind the knees.
Self Massage
Massaging the affected muscles will help them relax.
Use one or both hands or a massage gun to knead and loosen the muscles gently.
Stretching
Various stretches will maintain the treatment, help keep the muscles relaxed and retrain the muscles.
Stationary Cycle
A few minutes of easy pedaling can help loosen the leg muscles before bed.
Walking on the Heels
This will activate the muscles on the other side of the calf, allowing the calves to relax.
Supportive Footwear
Poor footwear can aggravate issues with the nerves and muscles in the feet and legs.
Orthotics may help.
Heat Application
Heat can soothe tight muscles and increases blood flow to the area.
Apply a hot towel, water bottle, heating pad, or muscle topical cream to the affected area.
A warm bath or shower (if available, shower massage setting) can also help.
Sciatica Secrets Revealed
References
Allen, Richard E, and Karl A Kirby. “Nocturnal leg cramps.” American family physician vol. 86,4 (2012): 350-5.
Butler, J V et al. “Nocturnal leg cramps in older people.” Postgraduate medical journal vol. 78,924 (2002): 596-8. doi:10.1136/pmj.78.924.596
Garrison, Scott R et al. “Magnesium for skeletal muscle cramps.” The Cochrane Database of systematic reviews vol. 2012,9 CD009402. Sep 12, 2012, doi:10.1002/14651858.CD009402.pub2
Giuffre BA, Black AC, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2023 May 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482431/
Handa, Junichi, et al. “Nocturnal Leg Cramps and Lumbar Spinal Stenosis: A Cross-Sectional Study in the Community.” International Journal of general medicine vol. 15 7985-7993. Nov 1 2022, doi:10.2147/IJGM.S383425
Hsu D, Chang KV. Gastrocnemius Strain. [Updated 2022 Aug 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534766/
Mayo Clinic Staff. (2019). Night leg cramps. mayoclinic.org/symptoms/night-leg-cramps/basics/causes/sym-20050813
Monderer, Renee S et al. “Nocturnal leg cramps.” Current Neurology and Neuroscience report vol. 10,1 (2010): 53-9. doi:10.1007/s11910-009-0079-5
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine