Louie Martinez has been a Wrestling trainer, coaching athletes ranging from 8 to 15 years, for about 15 years. Louie Martinez shares how he met Dr. Alex Jimenez 10 years ago after he experienced an initial injury. Coach Martinez has suffered a variety of accidents throughout his training career, from shoulder injuries to spine injuries, and every moment, Dr. Alex Jimenez has assisted Coach Martinez to�regain his health. Before meeting Dr. Jimenez, Louie Martinez did not comprehend the significance of seeing a chiropractor. Louie Martinez urges Dr. Alex Jimenez as the non-invasive choice for sports injuries.
Sports Injuries
When visiting a chiropractor for sports injuries, a physical exam will help pinpoint the health problem to produce an individualized treatment plan to treat it. Chiropractic care has been observed to decrease the healing time of sports accidents, as well as help stop future sports accidents. It’s important to understand your chiropractor. The healthcare professional may have useful suggestions that can keep you healthy as you work to reach your objectives.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
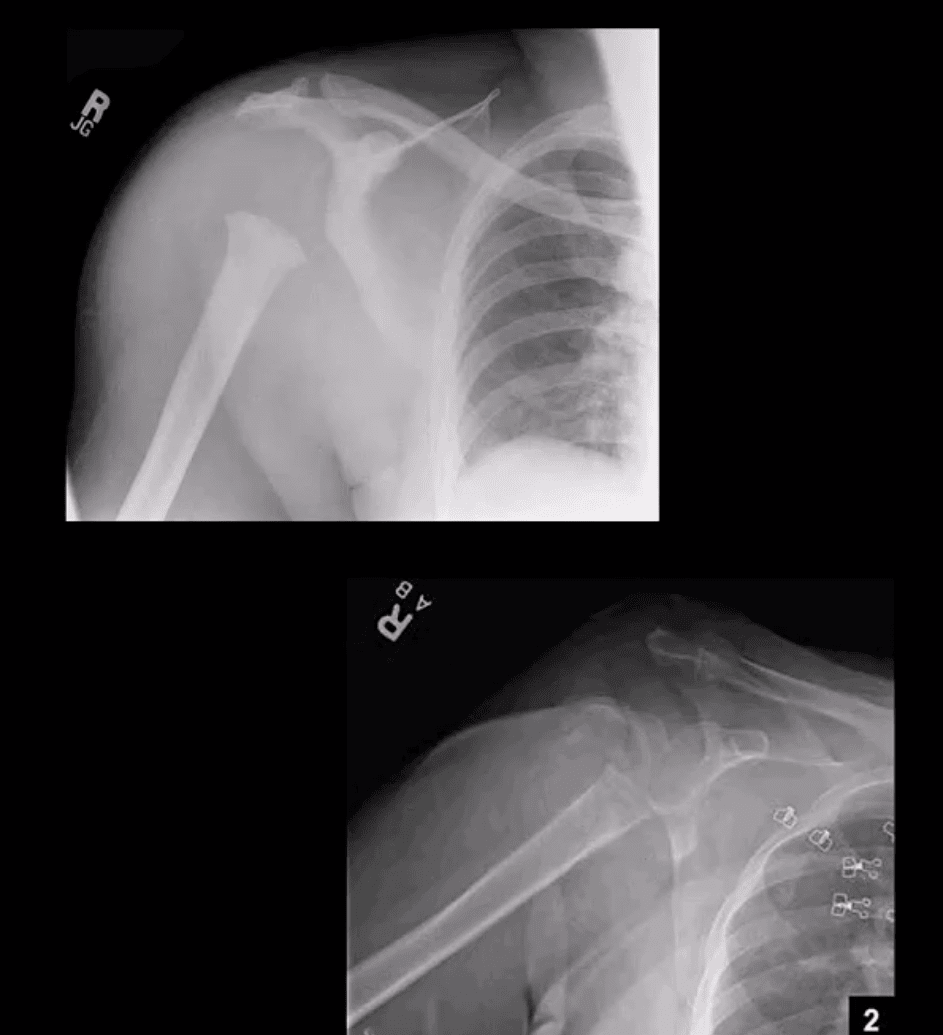
Proximal humeral Fx account for 4-6% of all Fxs. Osteoporotic (OSP) Fx in >60 y.o associated with minimal trauma with F: M 2:1 ratio. In young patients, acute high energy trauma predominates.
Complications: AVN humeral head, Axillary N paralysis.
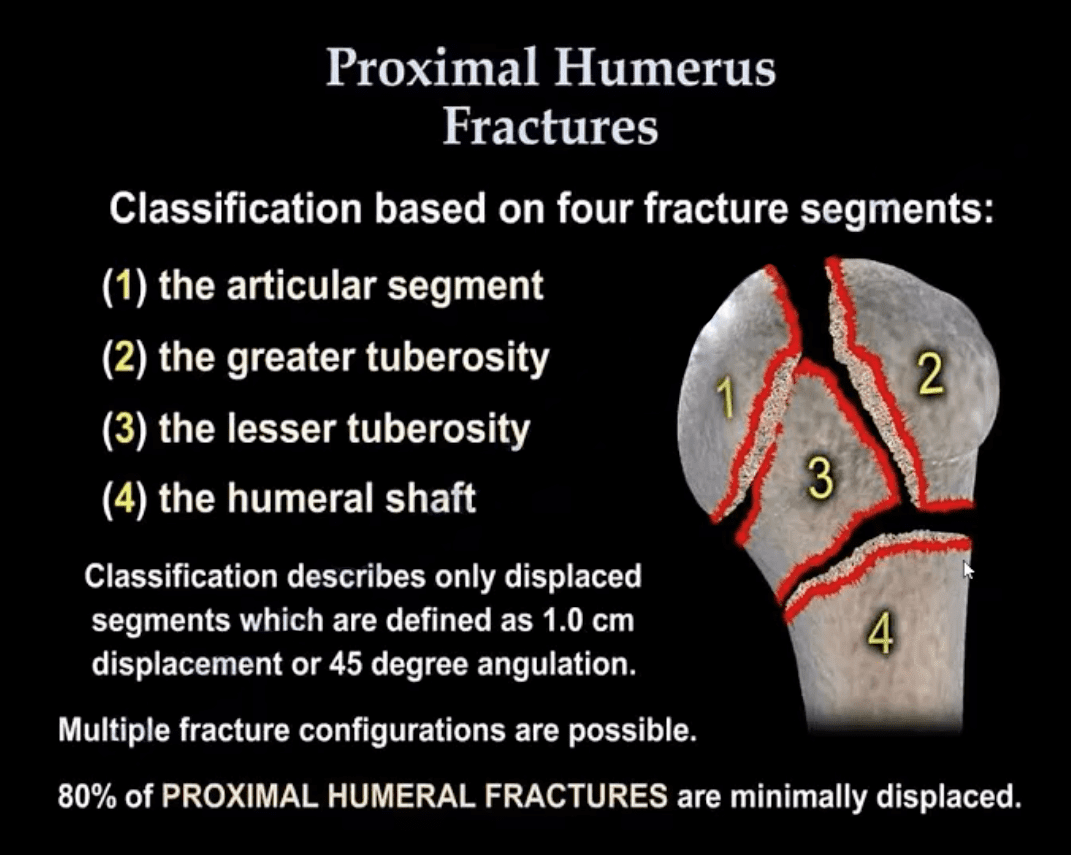
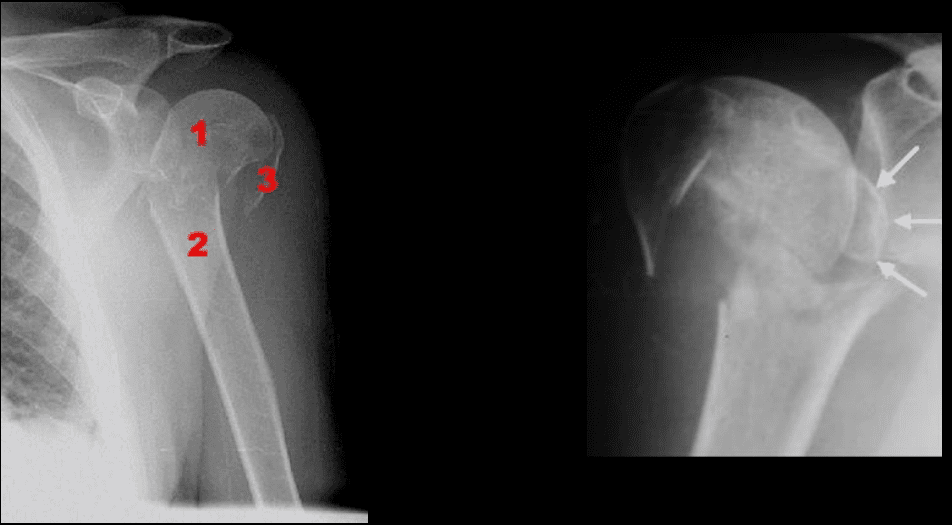
Neer Classification: considers fractures along 4-anatomical lines with or w/o displacement >1-cm & 45-degree angulation
One part Neer Fx- no displacement or very minimal <1-cm/45-degree. Can affect 1-4 lines and M/C at greater tuberosity. 80% of proximal humeral Fx are one-part Neer.
Two-part Fx: 1-part is displaced >1-cm/45-degrees. m/c involves the surgical neck
Three-part Fx: 2-parts are displaced >1-cm/45-degrees.
Four-part Fx: all 4-parts can be displaced. Uncommon <1%
Imaging: 1st step-radiography, CT may be used in more complex cases. Orthopedic referral
Management: Neer one-part Fx is treated with Sling Immobilisation and progressive rehab
The vast majority of Fx in the elderly are treated non-operatively
Younger patients (40-65) may occasionally require hemiarthroplasty if 3 or 4-part Neer Fx present. Greater risk of AVN
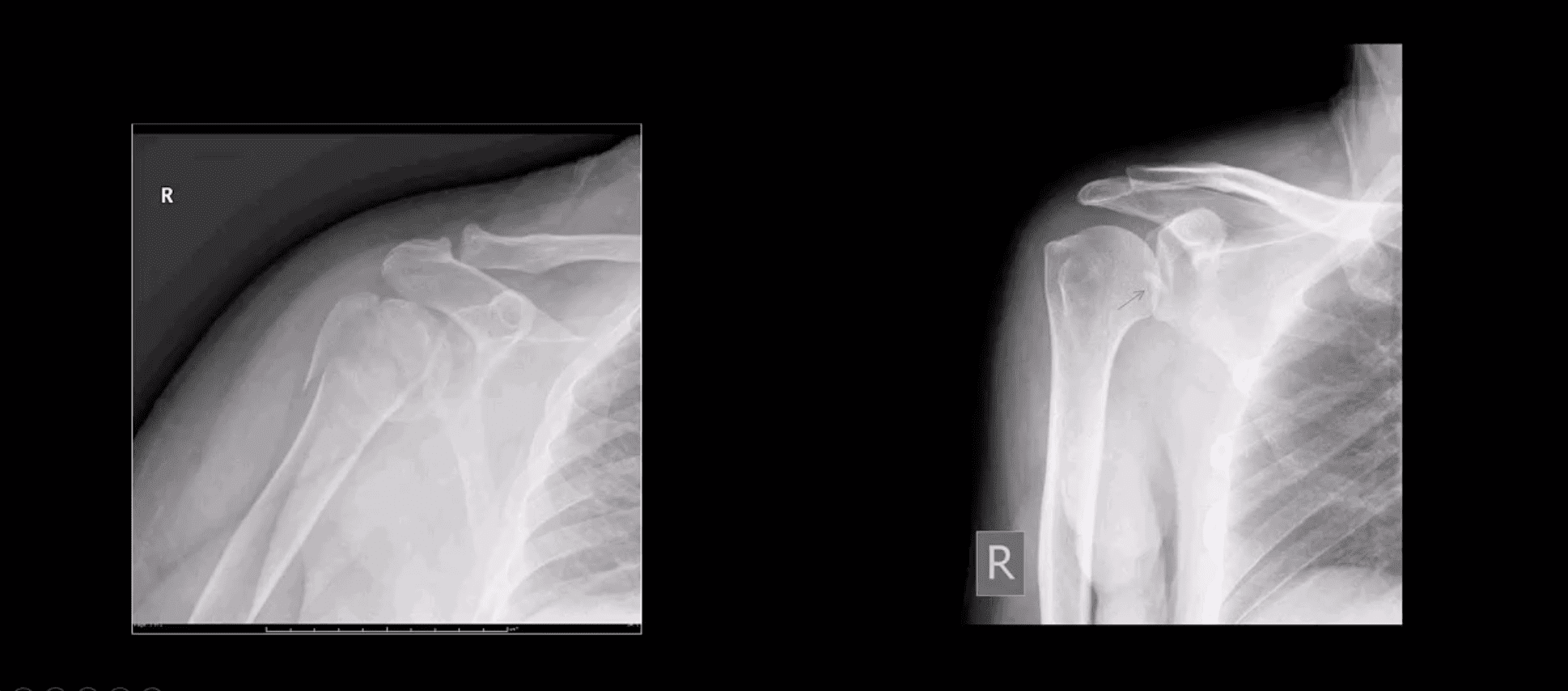
Proximal Humerus Fractures
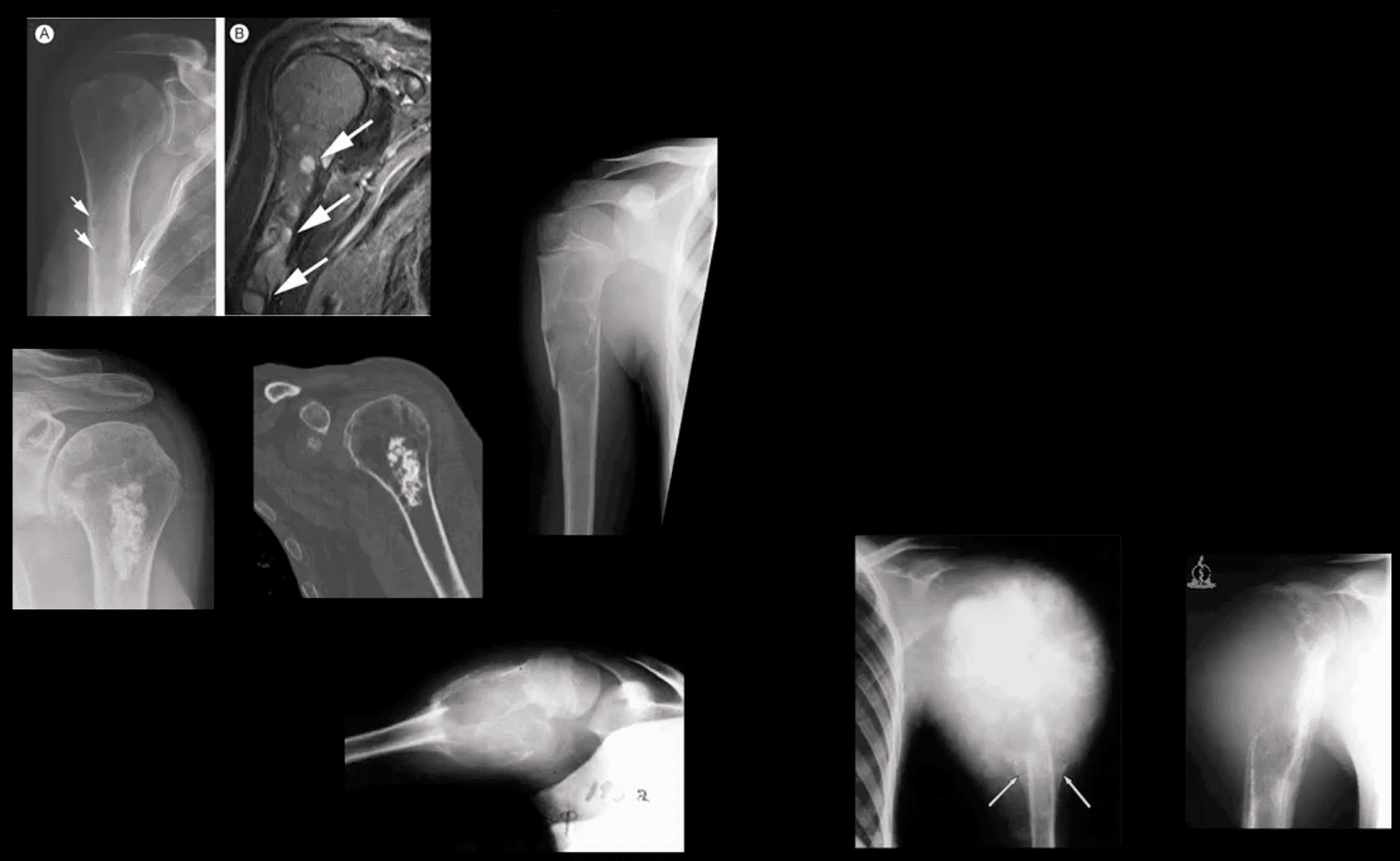
Note: Left image: Fx involving the anatomical neck and the greater tuberosity with minimal displacement <1-cm/45-degree thus Dx as one-part Fx. Right image: Small avulsion Fx of the greater tuberosity with significant displacement (>45-degrees & 1-cm) thus Dx as two-part Fx
Note: three-part Neer Fx (left) and four-part Neer Fx (right)> Management: operative in most cases in younger (40-65) patients
Refers to complete separation of the humerus from scapula glenoid. In 20-40s M: F 9:1 ratio, in60-80S M: F 3:1
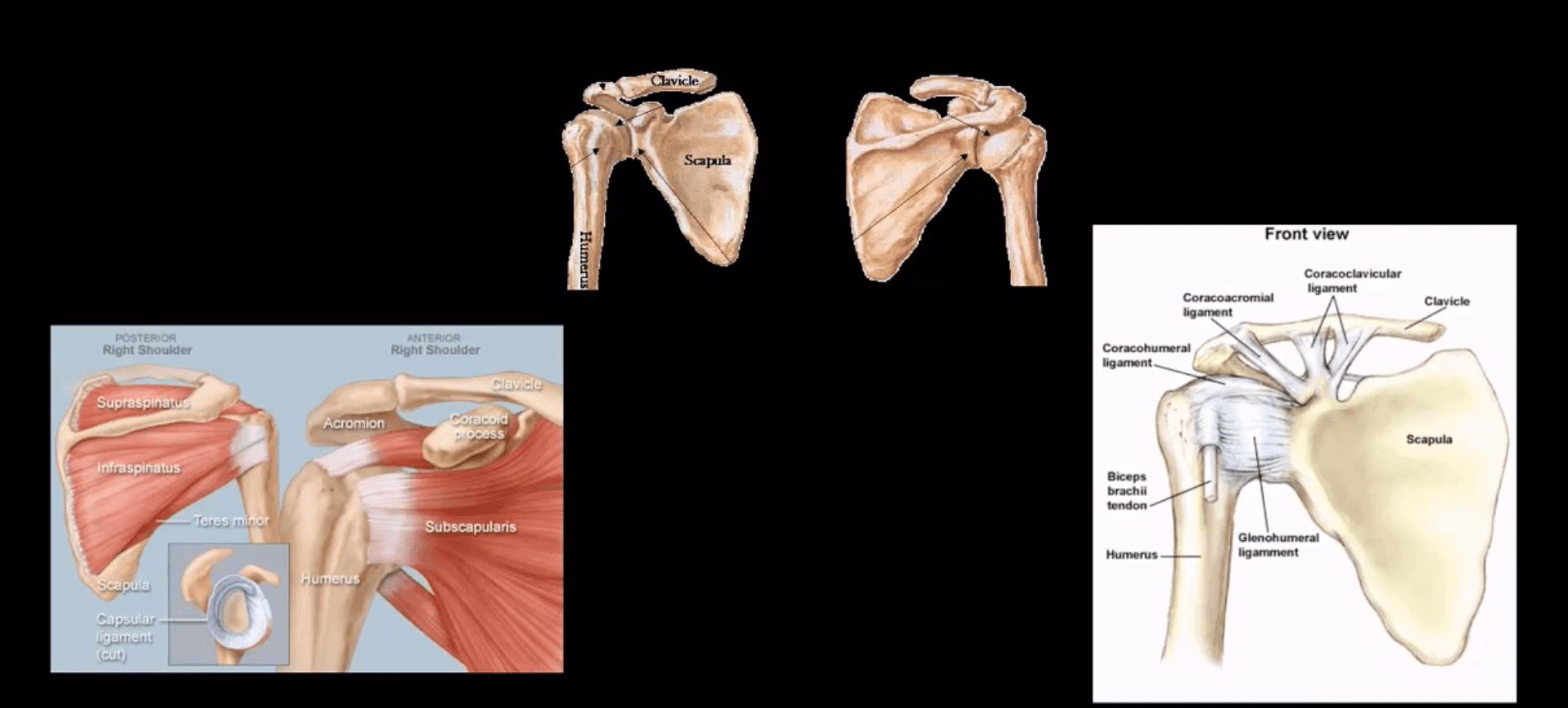
Anatomy: Shoulder stability is sacrificed for mobility, and overall GHJD is the m/c among large joints in the body
Protective falls (e.g., FOOSH) and MVA are m/c causes. GHJ is most vulnerable in abduction, extension and external rotation. Anatomical factors: shallow glenoid, laxed ant-inferior capsule and GH ligaments. GHJD will induce severe tearing of major GHJ restraints. Associated osseous and labral injuries are common and may lead to chronic instability, DJD,�and functional changes
3-types: Anterior GHJD (95%)
Posterior GHJD (4%) especially associated with epileptic seizures, electrocution and can occur b/l
Inferior GHJD aka Laxatio Erecta (<1%) associated with severe trauma
Clinically: AGHJD presents with severe pain, the arm is externally rotated and adducted, severe limitation of movement. GHJD may persist as chronic dislocation.
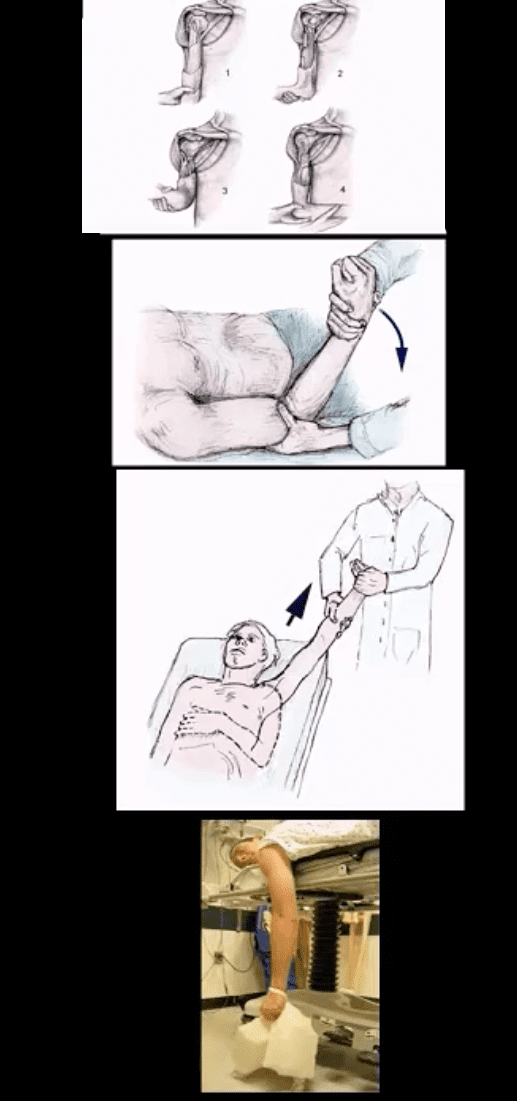
Management: prompt reduction in ED under anesthesia or heavy sedation with Kocher technique top image (not used), External rotation method (middle) or Milch technique (can be used w/o anesthesia) and a few other methods. Delay in reduction correlates with greater risk of immediate and long-term�complications
Diagnostic Imaging Approach
Shoulder series x-radiography is sufficient. Additional Imaging with CT scanning and MRI may be helpful to Dx osseous, cartilage, labral/ligaments pathology
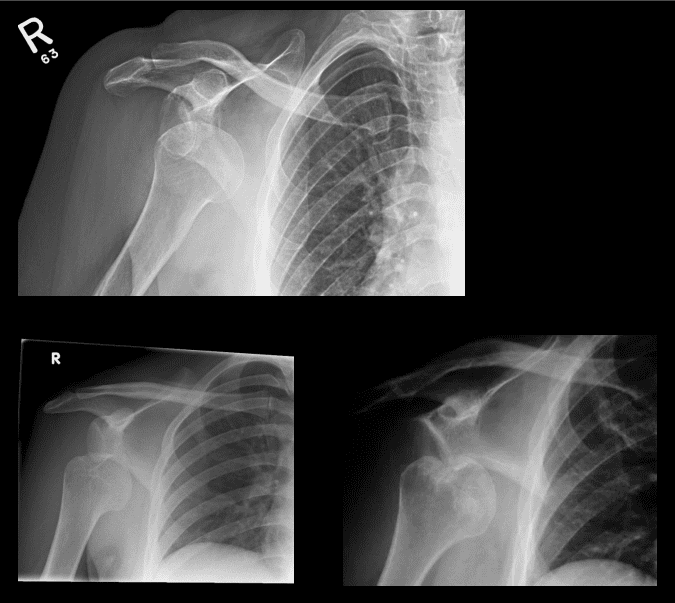
Anterior GHJD (95%). Subcoracoid position(top right) of the humerus is the m/c
Anterior GHJD may also occur as subglenoid(bottom left)and infrequently as subclavicular
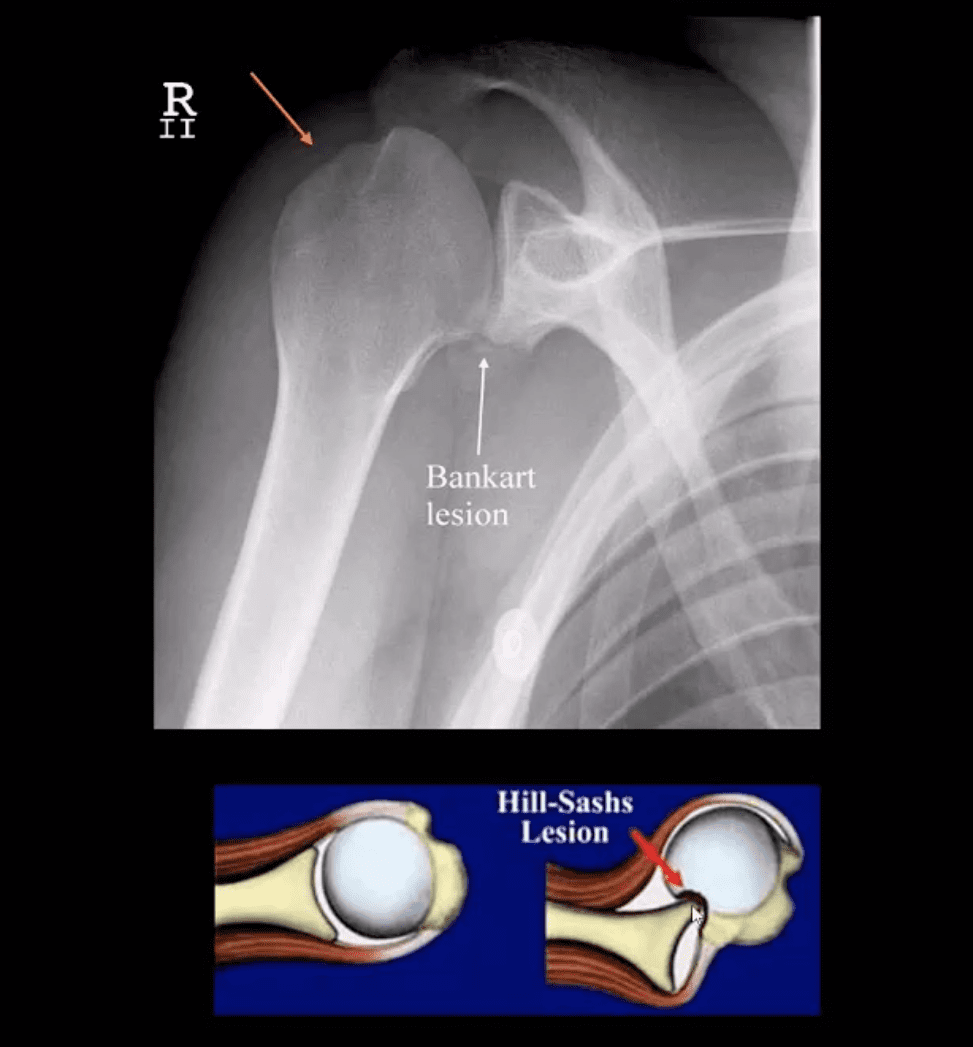
Key to radiographic search is to evaluate associated Bankart and Hill-Sachs injuries
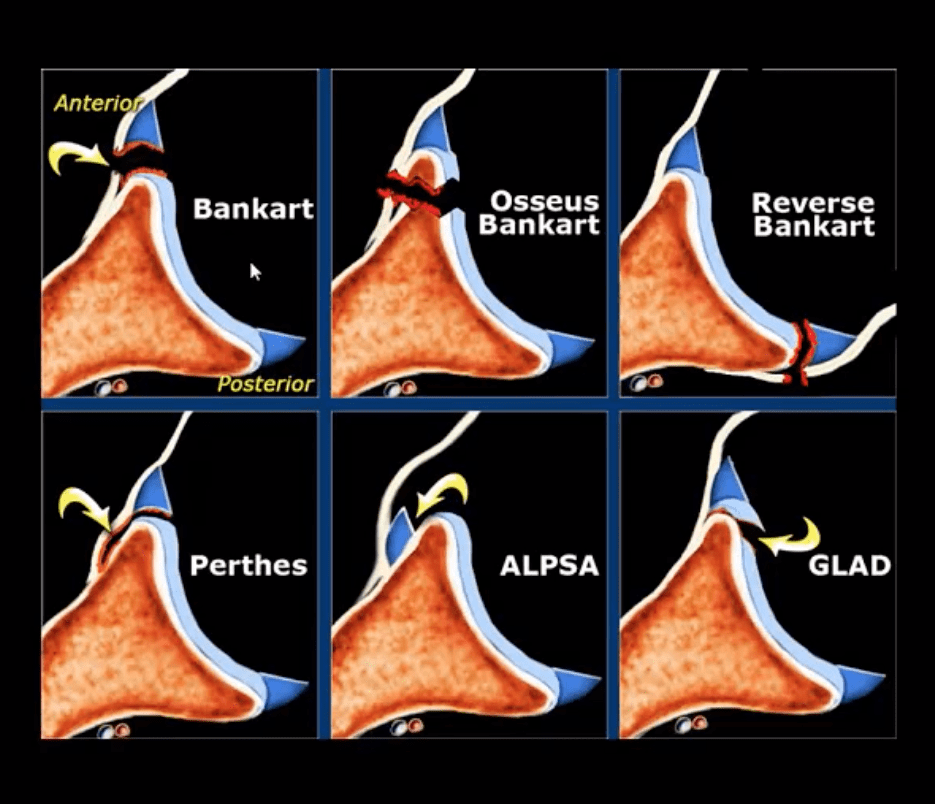
Bankart Lesion
Occurs during anterior GHJD d/t impaction of the head into anterior-inferior glenoid. Variations exist (see next slide). BonyBankart can be seen on x-rays. So-called soft tissue Bankart requires MRI. Cartilage (soft)Bankart is the m/c.
Hill-Sachs aka Hatchet deformity (arrow postreduction)occurs during the same mechanism as Bankart, i.e., compression and impaction of posterolateral aspect of the head against the glenoid producing wedge-shape Fx. Hill-Sachs lesion may predispose to recurrent/chronic GHJD.
Bankart lesion may heal, but operative suture anchors are needed sometimes
CT arthrogram and MRI may be helpful
Types of Bankart Lesion
Note different types of Bankart lesion. Onlyosseous Bankart can be seen radiographically. Soft tissue Bankart requires MRI with and without intra-articular gadolinium(arthrogram).
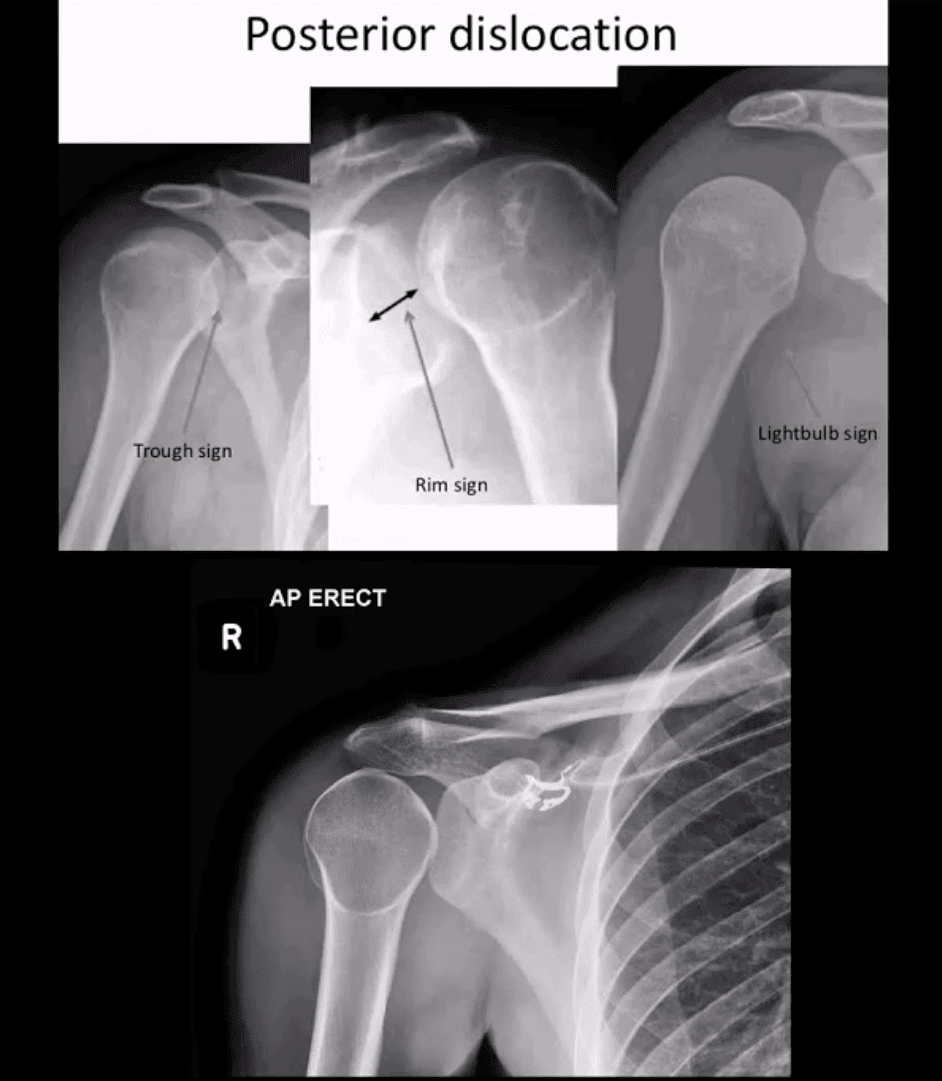
Posterior Dislocation
Note: posterior GHJD with its characteristic signs:
Trough sign aka reverse Hill-Sachs. Occurs d/t anterolateral head impaction Fx
Rim sign: only occurs in the PGHJD d/t posterior position of the head and anterior glenoid-to humeral head distance 6-mm or greater
Light-bulb sign: d/t acute internal rotation of the humerus (head)
Inferior GHJD
Inferior GHJD aka Laxatio Erecta
Severe hyperabduction and inferior displacement of the humerus. Greater chances of severe neurovascular injury and acromial Fx
The dislocated arm is hyperabducted and fixed with the elbow flexed and the arm above the head
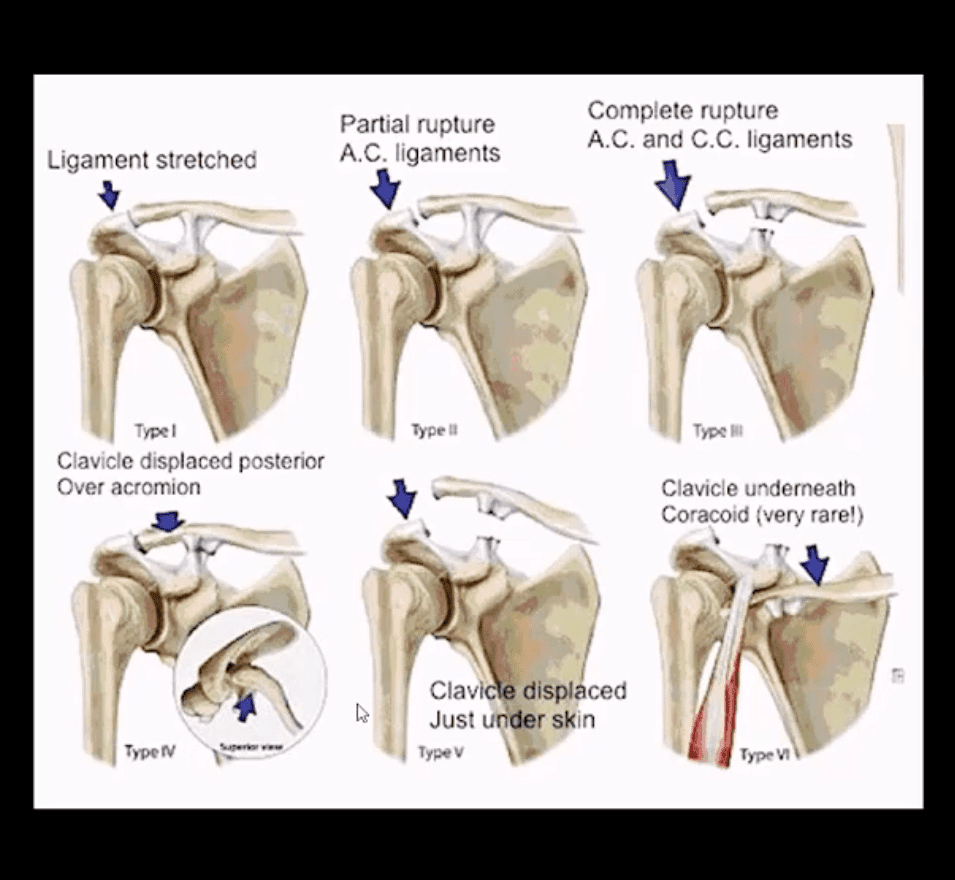
ACJ Dislocation (ACJD)
ACJD: common injury, 9% of shoulder girdle injuries esp. in male athletes by a direct blow
Rockwood classification (left) evaluates tearing of AC and CC ligaments and regional muscles
Type1, 2, 3 among the m/c
Type 1: sprain of ACL w/o tearing
Type 2: tear of ACL and sprain of CCL
Type 3: tear of AC & CCL. The clavicle is elevated above the acromion. If <2-cm good results with conservative Rx.
Imaging: x-radiography with b/l ACJ views with and w/o weights to compare both ACJs. In complex cases CT scanning esp. if Fx is considered
Management: Type 3 (>2-cm) & Types 4-6Operative
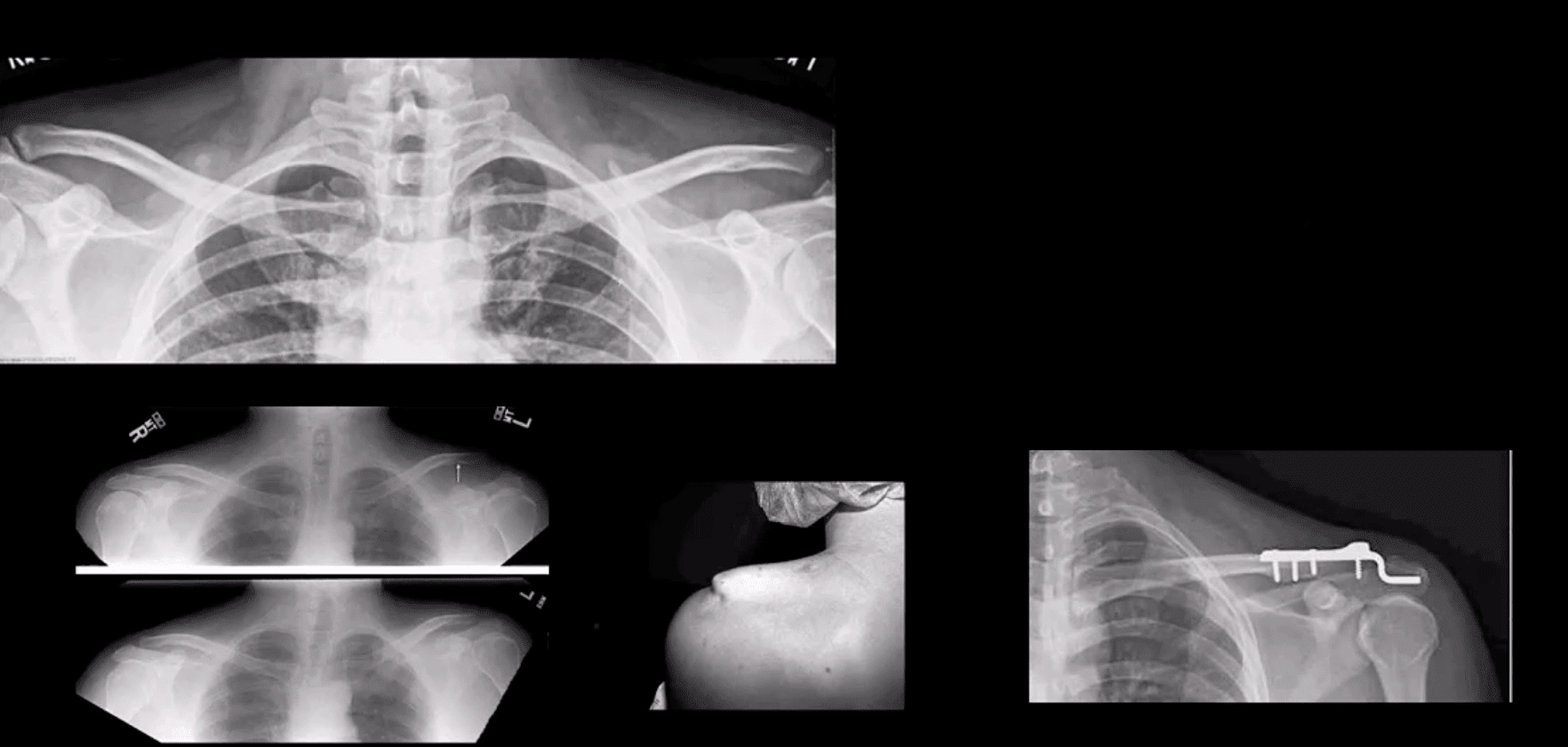
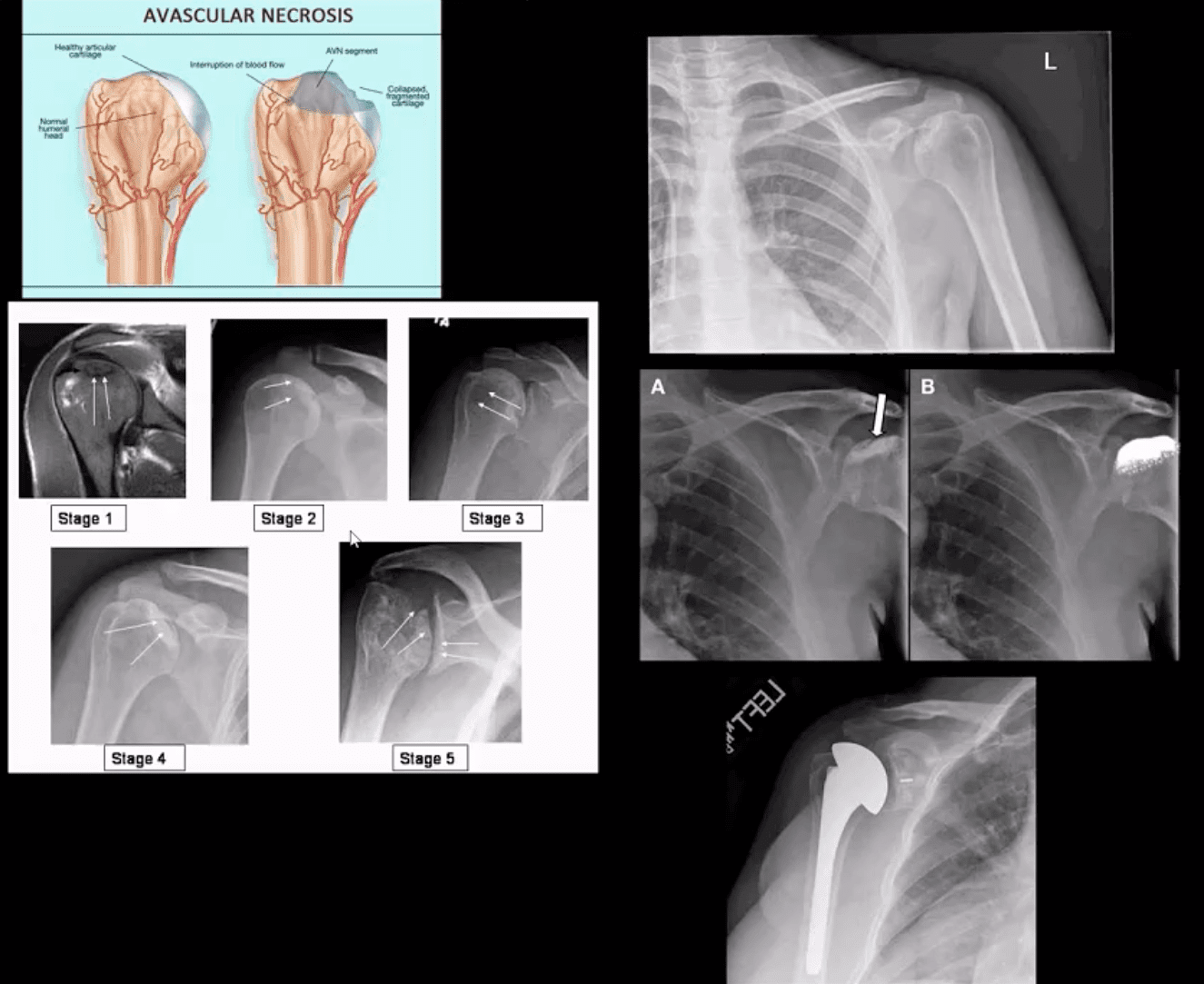
Type 3 ACJ Separation
Type 3 ACJ separation (top left)
More significant ACJD (bottom images) with clinical sign of acromion under the skin and resultant ORIF
Rotator Cuff Muscles (RCM) Pathology
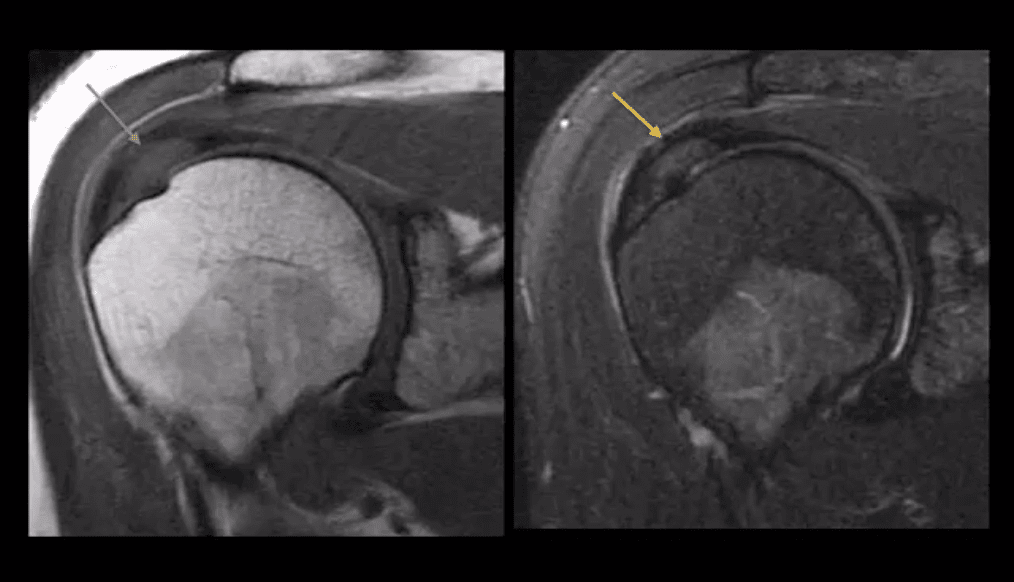
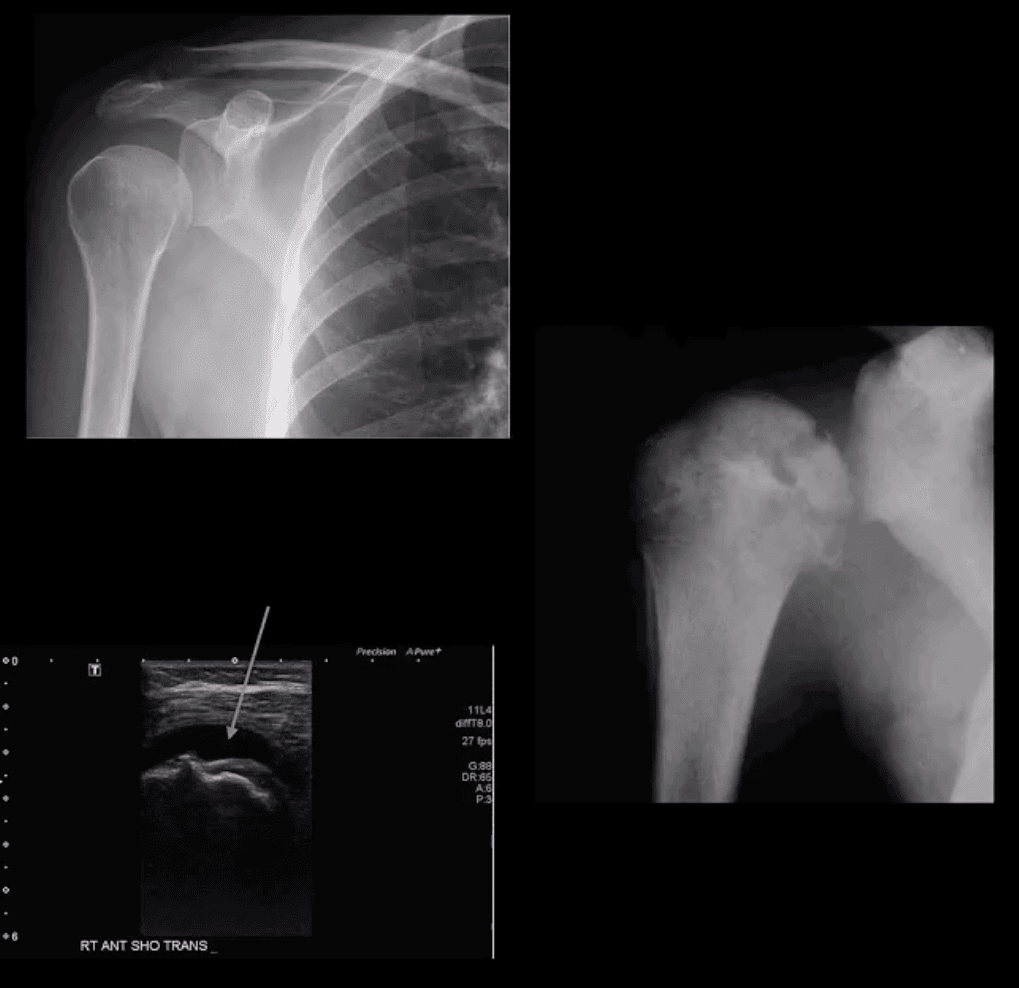
RCM tendinopathy: collagenous degeneration of RCM particularly Supraspinatus M. tendon(SSMT) d/t overuse/degeneration-micro tearing with collagenous replacement. Impingement syndrome is a 2nd extrinsic cause. Presented clinically as pain and limited ROM
Imaging Dx: MSK US can be as accurate as MRI and better in some cases d/t dynamic evaluation v. cost effective
Key MRI clue is thickened inhomogeneous SSMTwith increased signal on all pulse sequences d/t fatty degeneration and inflammation (left images: T1 & T2 FS)
MSKUS findings: thickening of the SSMTsubstance with a change�in normal echogenicity.MSKUS is good to DDx with SSMT tears. US advantages are that it allows dynamic evaluation of painful structures
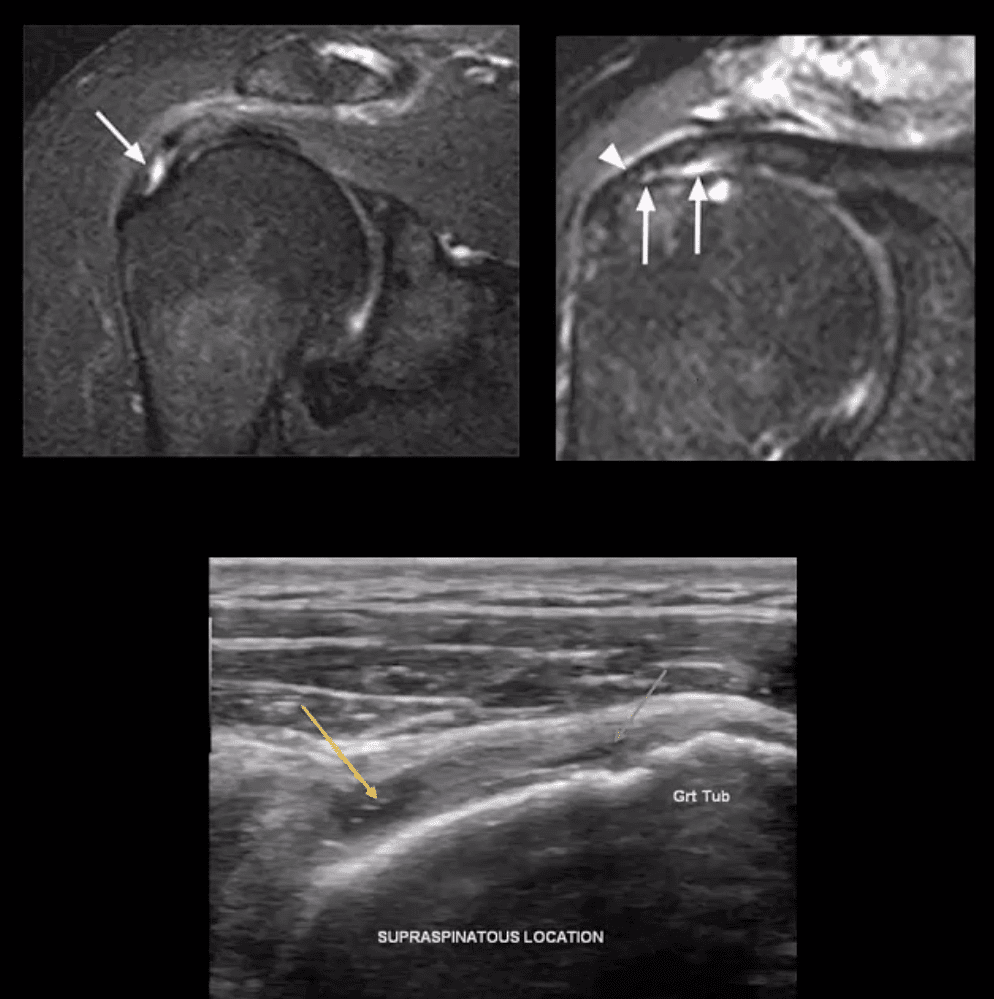
Partial tear of SSMT: partial (incomplete) tear ofSSMT may occur at the bursal and articular surface or interstitial, i.e., intra-substance/noncommunicating. Etiology: sub-acromial impingement, acute strain, and chronic microtrauma tendinosis
Clinically: pain on abd and flexion, impingement tests, Hawkins-Kennedy tests, etc. Pearls: partial tears can be more painful than complete tears
Imaging Dx: MSKUS is as good as MRI (N.B.some studies indicated MSKUS is more superior to MRI). Key MRI findings: gap/incomplete tear of SSMT filled with joint fluid +/- granulation tissue
MSKUS: decreased echogenicity of SSMT, thinning and partial tearing filled with fluid(anechoic areas arrows). Lost convexity of tendon bursal or articular interface.
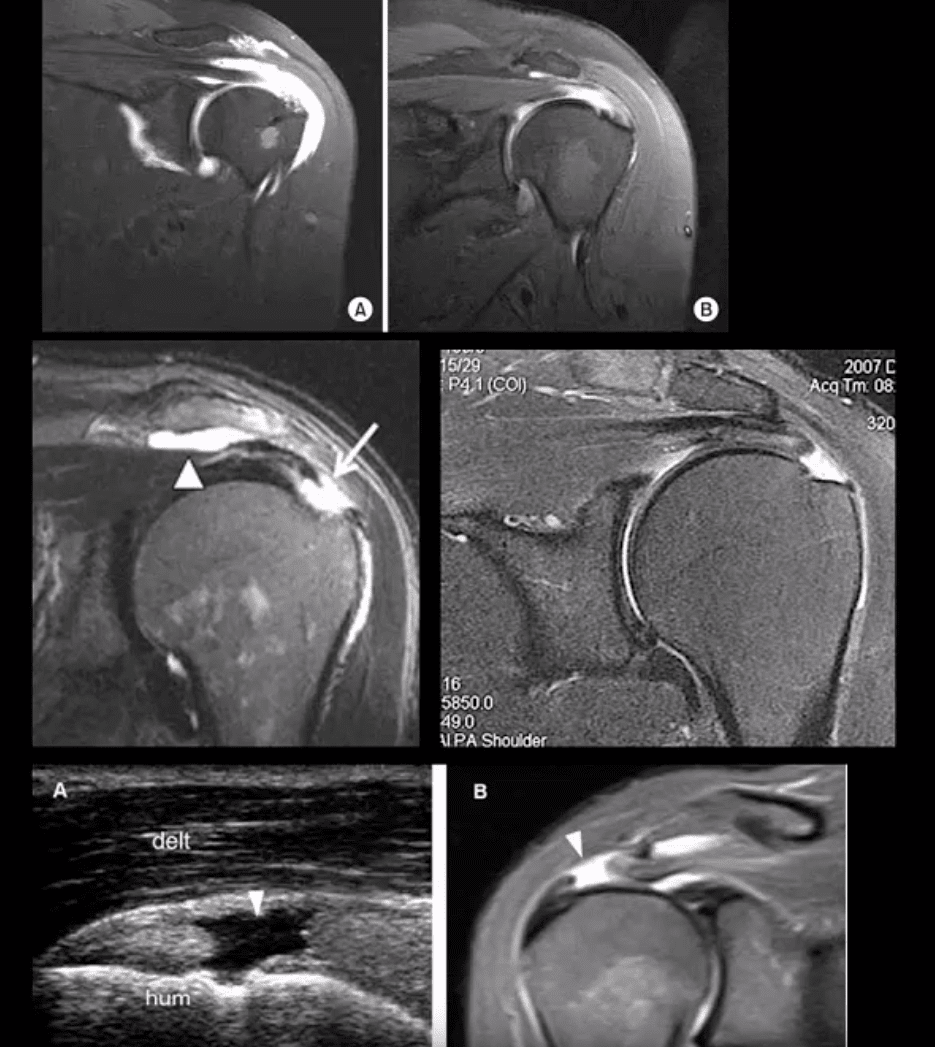
Full Thickness SSMT (rot cuff) tear: degeneration/tearing of rot cuff. 2nd to impingement by Hooked acromion, overhead overuse or acute trauma. 7-25% of shoulder pain in the general population. Clinically: pain on impingement tests.
Imaging Dx: MSKUS is as good as MRI.Limitations: poor Dx of labral pathology. Key USDx: focal tendon interruption, an anechoic gap (fluid filled), hypoechoic tendon, tendon retraction, uncovered cartilage sign (bottom left, A: US B: MRI)
MRI: key Dx: insertional tear extending through entire SSMT crescent, retraction with fatty degeneration of SSMT and the muscle. If retraction is at 12 o�clock or greater (top images), it may not be anchored operatively
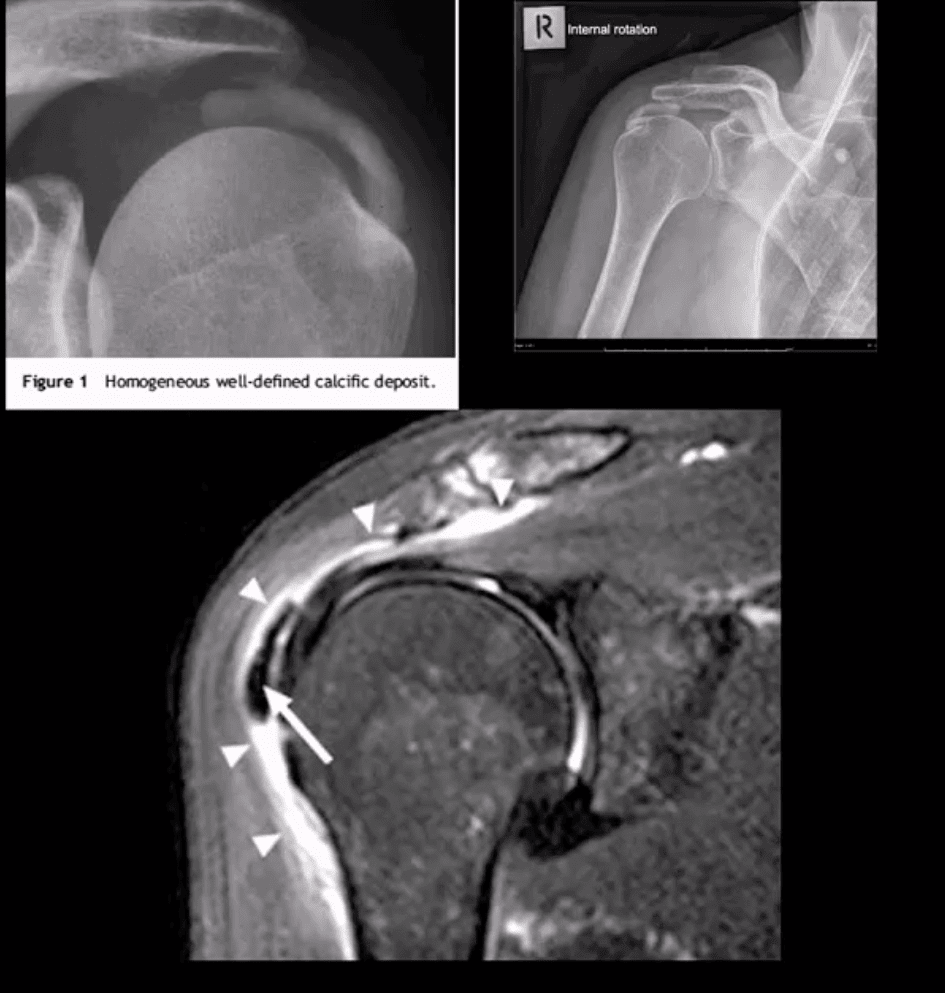
Rotator Cuff (RTC) Calcific Tendinitis: usually d/t calcium HADD crystals. Middle-aged women are most affected. Ranges from asymptomatic imaging finding to severe destructive arthropathy or Milwaukee shoulder(infrequent)
HADD has 3-pathological phases: formation resting-resorption.Mild-to-moderate pain esp. in resting phase.
Imaging: x-radiography: homogenous ovoid mineralization within RTCMT, m/c in SSMT. MRI: ovoid/globular decreased signal on all pulse sequences often with surrounding edema (bottom left)
Rx: self-resolution occurs. Advanced cases: operative aspiration etc.
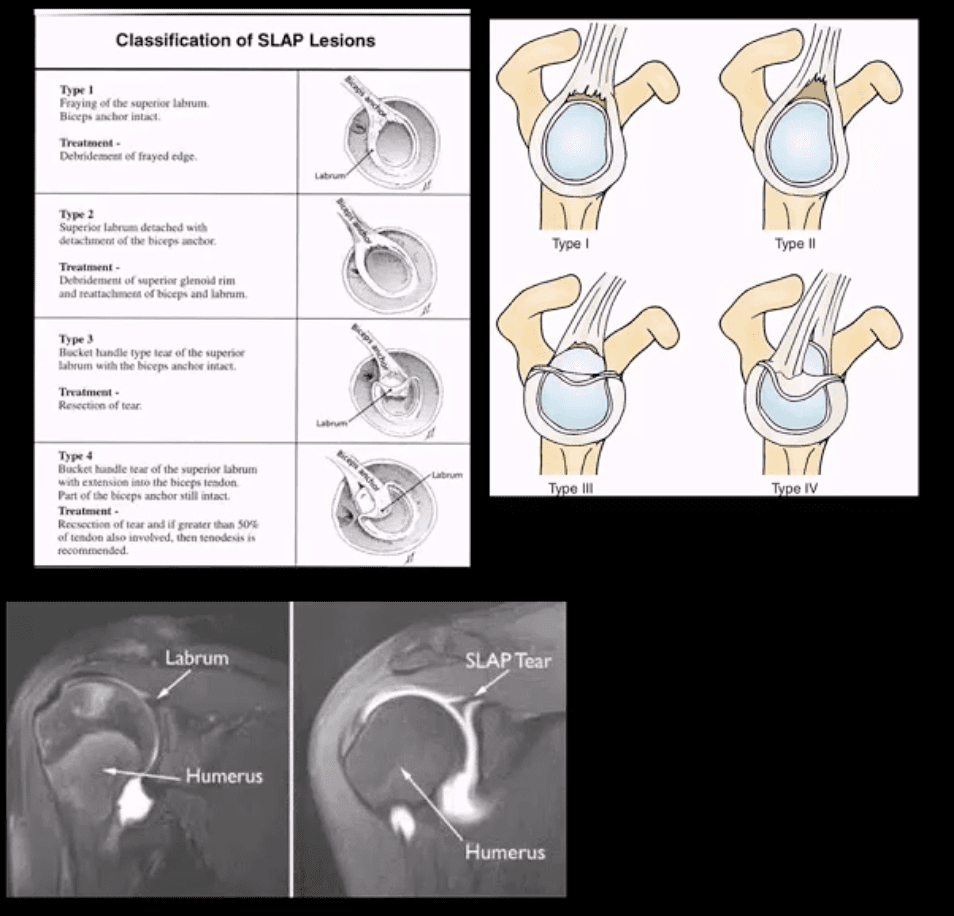
Superior Labrum Anterior to Posterior (SLAP) Lesions/Tears
SLAP tears: FOOSH and throwing sports or chronic shoulder instability aka Multidirectional shoulder instability (in 20%). Type 1-9 exist but the M/C areType 1-4
In all 4-types superior labrum is affected with or w/oLHBMT anchor tear (see pictures). Clinically: pain, limitation of AROM with active compression tests, typically non-specific findings mimicking RTCpathology
Imaging is crucial: best imaging is MRI arthrography. Key signs: hyperintense linear fluid signal within superior labrum +/- extending along the LHBT on fat-suppressed fluid sensitive imaging and FS T1 arthrogram. Best observed on coronal slices.
Rx: small tears may heal, but unstable tears require operative care.
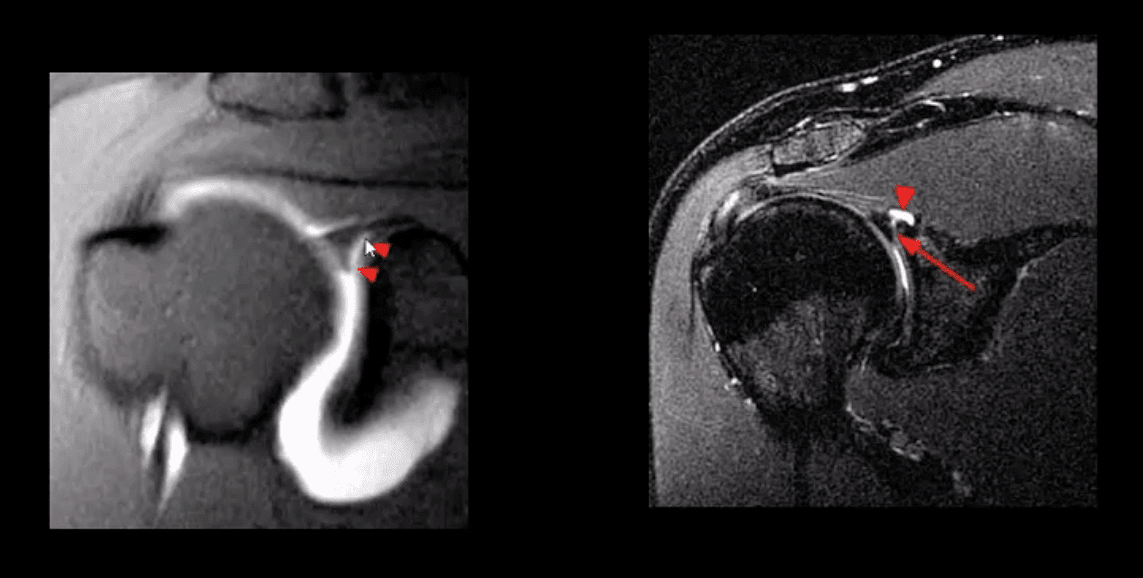
Key DDx: anatomical variants like Buford complex andSub-labral foramen
SLAP tear with a paralabral cyst (bottom right)
Normal variant DDx: sub labral foramen(bottom left) note: MR arthrography with contrast undercutting the labrum but w/o extending posteriorly to the LHBT
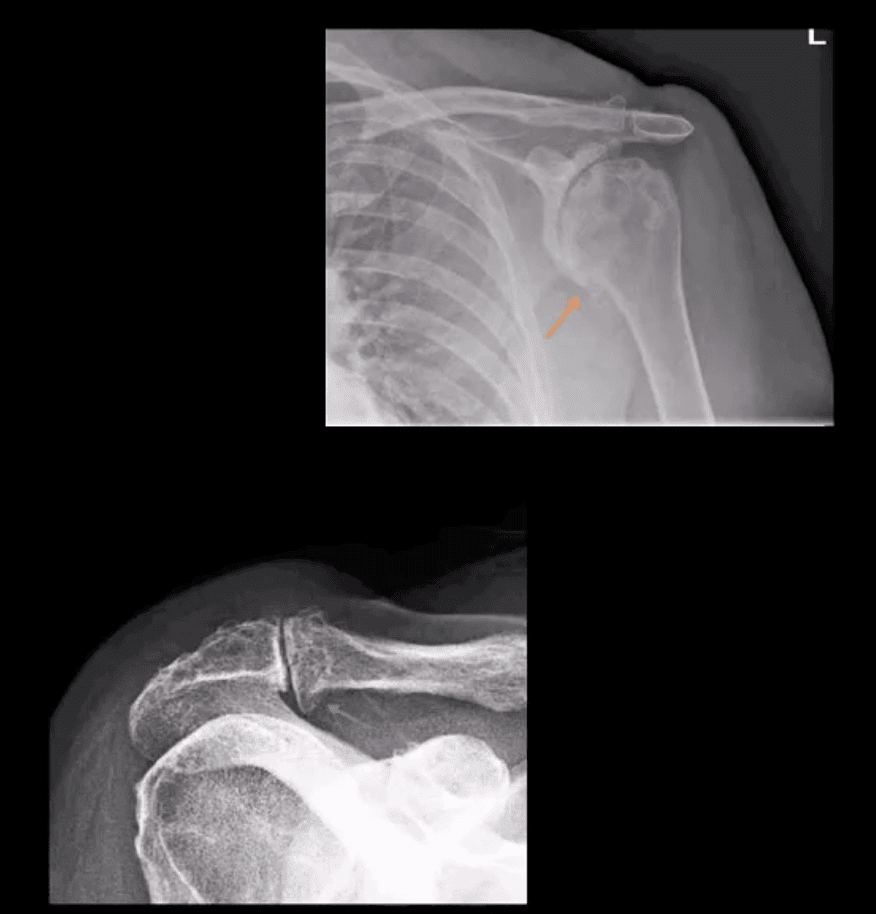
Shoulder Arthritis
GHJ DJD: usually associated with a 2nd cause: trauma, instability, AVN, CPPD, etc. Presented with pain, crepitus and decreased ROM/function. Associated RTC disease may be present. Imaging; x-radiography is sufficient and provides grading/care planning.Major findings: joint narrowing, osteophytosis esp. at the inferior-medial head (orange arrow), subchondral sclerosis/cysts. Often noted superior head migration d/t RTC disease.
ACJ OA: common and typically primary with aging. Presents with ACJ loss and osteophytes. Osteophytes along the undersurface of the ACJ �keel osteophytes�(blue arrow) may lead to RTC muscle tear. Regional bursitis is other clinical feature of ACJ arthrosis.
Management: usually conservative depending on clinical signs/symptoms
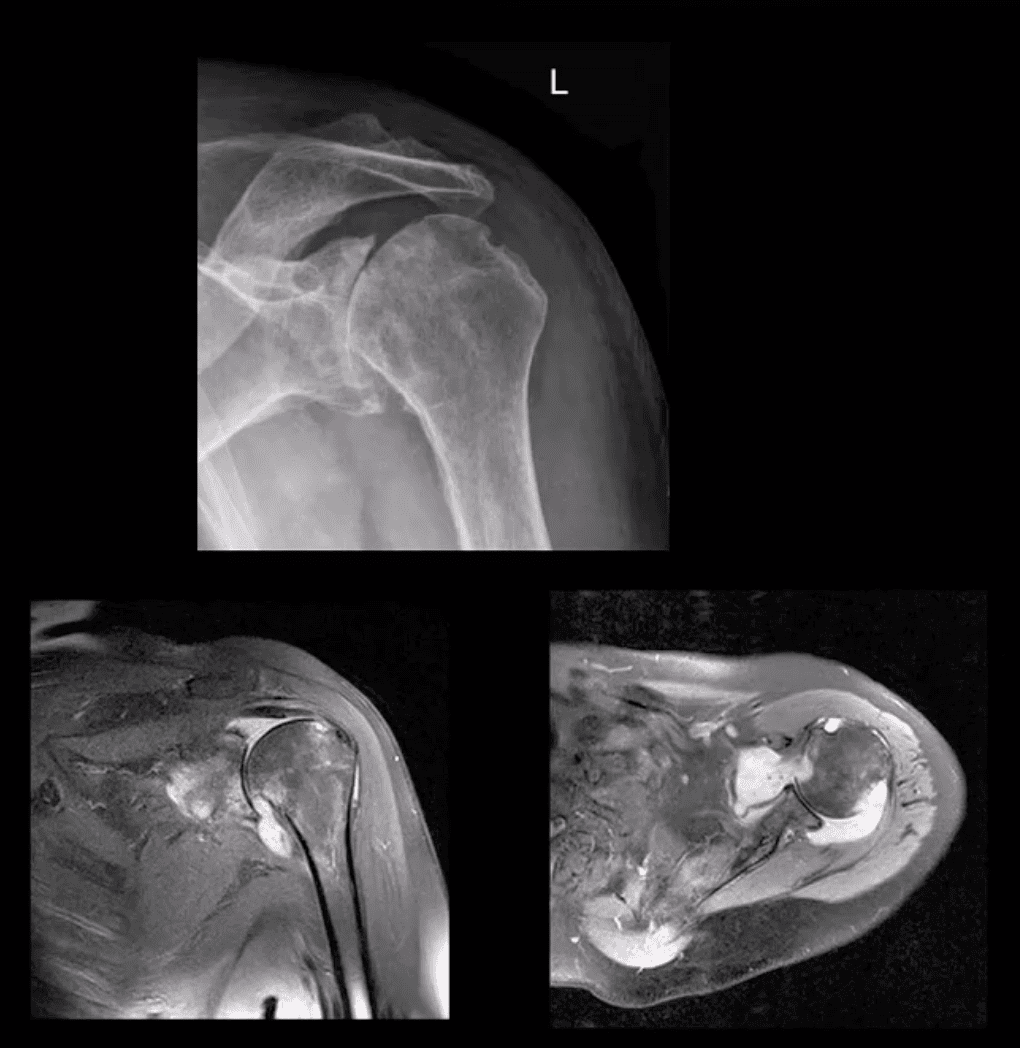
Rheumatoid Arthritis GHJ: RA is a multisystem inflammatory disease affecting multiple joints lined by the synovium. GHJ RA is common (m/c large joints in RA knees/shoulders). Clinically: pain, limited ROM and instability, muscle weakness/wasting. Hands, feet,�and wrists are m/c affected. Imaging: x-radiography reveals periarticular erosions, uniform joint space loss, juxta-articular osteoporosis, subluxations,�and soft tissue swelling. MRI can help detect�commonly associated RTC tearing and instability. Early changes can be detected by MSKUS esp. with power Doppler use indicating hyperemia/inflammation.
Note: L shoulder x-ray revealing cartilage destruction and symmetrical joint loss, multiple erosions, and likely loss of RTCM support with superior head migration, ST effusion present.
Note: PDFS coronal and axial MRI slices of GHJ RA indicating marked inflammatory joint effusion, bone erosion/edema, synovial pannus formation and likely tear in RTC m. Management: Rheumatological referral and pharmacotherapy with DMARD. Operative care asRTCM repair. 10% of patients are disabled d/t RA
Neuropathic Osteoarthropathy aka Charcot’s shoulder: d/t neurovascular and neural periarticular damage. Multiple causes exist.M/c develops in diabetics in midfoot. Shoulder Charcot is m/c in Syringomyelia (25%), trauma paralysis, MS, etc. Dx: clinical(50% pain/swelling 50% painless destruction). Imaging is crucial. X-radiography is sufficient in well-established cases, but early Dx is challenging. MRI may help with early Dx and delayed complications. Rad Dx: Shoulder Charcot is m/c presented as atrophic type destructive arthropathy with humeral head appearing as if surgically amputated along with intra-articular debris, density, distention, dislocation, and other key features
Septic Shoulder: shoulder is the 3rd m/c followingknee>hips. Patients at risk: diabetics, RA pts, immunocompromised, I.V. drug users, indwelling catheters, etc. Routes: hematogenous (m/c), direct inoculation (iatrogenic, trauma etc.) adjacent spread(e.g. OM). Staph. Aureus (>50%) m/c.
Clinically: joint pain and dec. ROM, fever 60% only, toxemia, inc. ESR/CRP. Dx: imaging and joint aspiration/culture. RadDx: early x-rays often unremarkable except ST effusion/fat planes obscuration, joint widening. Later7-12 days patchy osteopenia, moth-eaten/permeating bone resorption, articular destruction, joint narrowing. May progress to severe joint destruction and ankyloses. Early Dx & I.V. antibiotics are crucial even before culture. Operative irrigation and joint drainage in some cases. Complications are possible esp. if Rx is delayed. MSKUS with needle aspiration may help. Note: (top image) non-traumatic joint widening with inferolateral head displacement d/t septic A dx: by needle aspiration Staph. Aures.
Ischemic Osteonecrosis
Ischemic Osteonecrosis of the humeral head may occur d/t trauma (Neer four-part Fx), Steroids, Lupus, Sickle cell, Alcoholism, Diabetes,�and many other conditions. Imaging is crucial: MRI detects earliest changes as intraosseous edema. X-ray features are late, presented as a collapse of subchondral bone with sclerosis �snow cap� sign, fragmentation, and progressive severe DJD
Management: orthopedic referral, core decompression in early cases, hemiarthroplasty in moderate and total arthroplasty in severe cases.
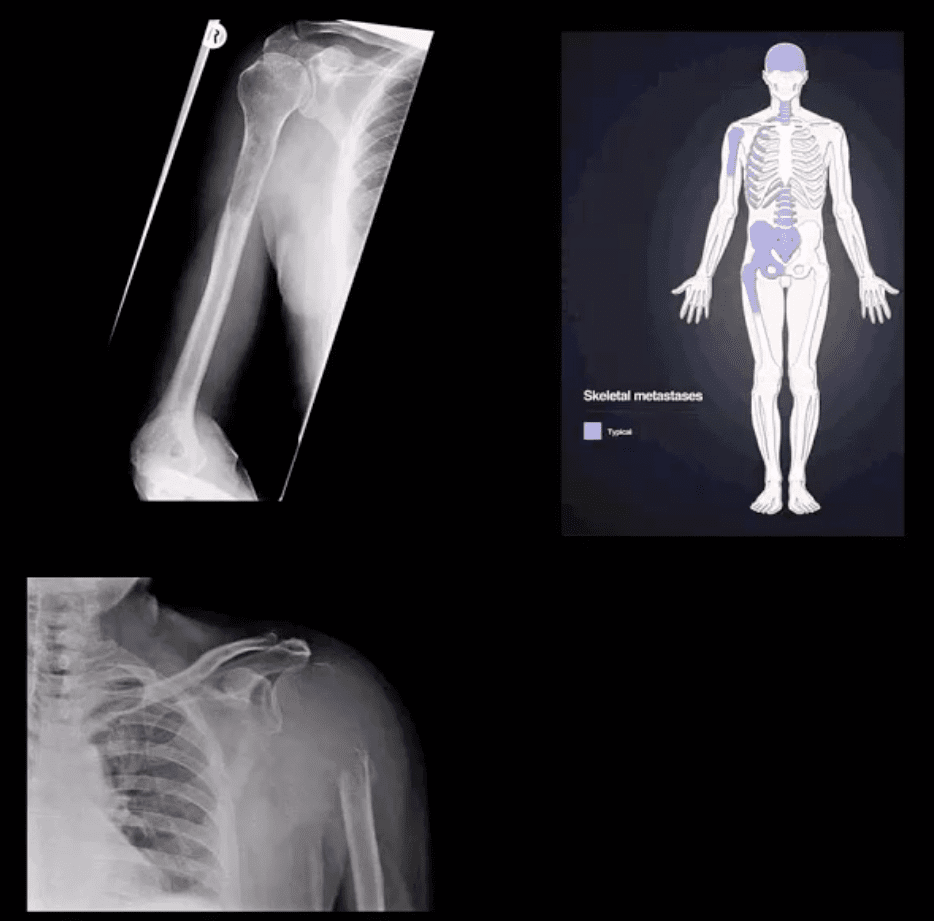
Shoulder Neoplasms
In adults >40, bone Mets d/t lung, breast, renal cell, thyroid CA & prostate are the m/c causes. Clinically: may mimic pain resemblingRTC/joint changes. Should be evaluated carefully. Key to Dx: Hx, PE and Imaging esp.in pts with known primary
Imaging: 1st step x-rays, MRI can help, Tc99bone scintigraphy helps to detect regional and distant disease. X-ray features: destructive lytic changes typically in prox humerus(red marrow) with or w/o path Fx. DDx: Mets, MM, lymphoma
Clinically: night pain, pain at rest, etc. Lab tests: unrewarding, in severe cases hypercalcemia may be noted.
Primary Malignant bone neoplasms (shoulder) Adults: M. Myeloma or Solitary plasmacytoma, Chondrosarcoma may transform from an enchondroma and some others. In children/teenagers: OSA vs. Ewing�s
Primary benign bone neoplasms (shoulder). Adults: Enchondroma (patients in their 20-30s)GCT. In children: Simple bone cyst (Unicameral Bone cyst), Osteochondroma, Aneurysmal Bone Cyst, Chondroblastoma (rare)
Imaging: 1st step x-radiography
MRI is essential to Dx. Especially in cases of primary malignant neoplasms Evaluate extent, soft tissue invasion, preoperative planning, staging, etc.
Running Shoes: Feet are important. By the time the typical American reaches the age of 50, they will have walked 75,000 miles.
Runners put even more miles on their feet, and stress. Your feet are your foundation. A problem with your feet can throw your entire body out of balance. That is why when it comes to running shoes, it is important to find the right type. This guide will help you find the running shoes that are right for you.
Running Shoes
Before You Shop
Know the type of runner you are.
Different types of running require different features in shoes.
Some questions to consider:
Do you run or jog?
What surface do you run on � asphalt, treadmill, or trails?
A larger person will not move and run the same way a thin, wiry person does. An overweight person will put more stress on their feet � and shoes.
Know your running style.
The way you run, the motion of your stride and how your foot strikes the ground has great bearing on the type of running shoe you need. When your foot comes in contact with the ground, what hits first? Does the inside of your forefoot hit first? The center of your heel? The outside of your heel? Where your foot first hits is where you really want the cushion.
Know what injuries you may have sustained from running.
Plantar fasciitis, shin splints, tendonitis, and blisters are a few common injuries can be reversed or improved when you wear running shoes that fit properly.
Know the type of arch you have.
Whether you supinate (foot rolls to the outside) or pronate (foot rolls to the inside) is determined, at least in part, by the shape of your arch. While supinators are rare, quite a few people over pronate. This can be the source of injuries due to overuse.
When You Shop
Give it the 360-degree test.
When people try on shoes they typically check for fit in the toe box, but look no further than that. When you try on running shoes, you do need to make sure you have adequate space in the toe box, but you also need to check that your entire foot fits on the shoe�s platform.
Give your foot enough space.
The upper should have enough room but should not be loose. It shouldn�t squeeze your foot either though. It should fit well with no pinching or binding.
Shop later in the day.
Throughout the day your feet swell. When you run they also swell so when you shop for shoes, going when your feet are the largest will help ensure that you get the most accurate and more comfortable fit possible.
Bring your old running shoes along when you shop.
Having your old shoes with you when you shop will help the sales person determine what kind of running shoe you need. They can look at the wear on the shoe to see your running patterns and help you find a shoe that works best for you.
Get your foot measured.
As you age your feet actually change; they can expand or flatten. Don�t every assume your shoe size, get your foot measured every time. A comfortable fit is dependent upon wearing the right size shoe. You also need to keep in mind that shoe sizes may differ from brand to brand.
Dress for the run.
When you are shopping for a new pair of running shoes, dress as you would when you run. Don�t show up wearing flip flops or when you are dressed for the office. Definitely don�t show up without socks.
Forget the latest trend or what�s fashionable; think functionality.
There are plenty of sharp looking shoes, but that doesn�t mean they are the right running shoe for you. Go for fit and functionality first and fashion second.
Take them for a test drive.
Once you have settled on a pair or two, try them both on and try them out. Many stores that specialize in running shoes have a treadmill or area where runners can try their shoes. That is the only way you can tell for shoe if the shoe is right for you.
Concussions are traumatic brain injuries that affect brain function. Effects from these injuries are often temporary but can include headaches, problems with concentration, memory, balance and coordination. Concussions are usually caused by a blow to the head or violent shaking of the head and upper body. Some concussions cause loss of consciousness, but most do not. And it is possible to have a concussion and not realize it. Concussions are common in contact sports, such as football. However, most people gain a full recovery after a concussion.
Can also happen due to excessive shaking of the head or acceleration/deceleration
Mild injuries (mTBI/concussions) are the most common type of brain injury
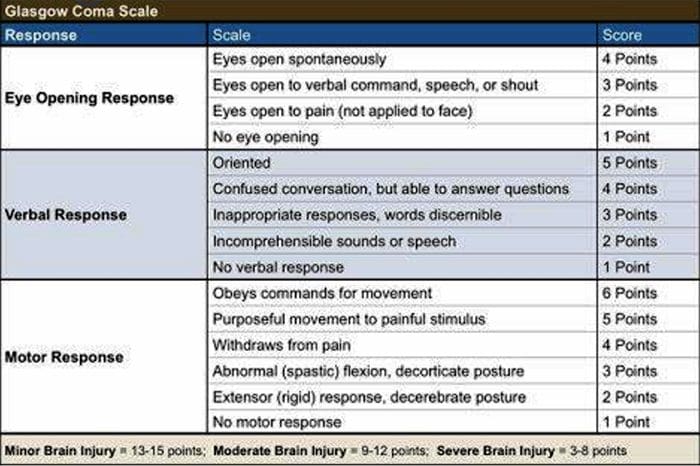
Glasgow Coma Scale
Common Causes Of Concussion
Motor vehicle collisions
Falls
Sports injuries
Assault
Accidental or intentional discharge of weapons
Impact with objects
Prevention
Prevention of concussive injuries can be paramount
Encourage Patients To Wear Helmets
Competitive sports, especially boxing, hokey, football and baseball
Horseback riding
Riding bicycles, motorcycles, ATVs, etc.
High elevation activates such as rock climbing, zip lining
Skiing, snowboarding
Encourage Patients To Wear Seatbelts
Discuss the importance of wearing seatbelts at all times in vehicles with all of your patients
Also encourage use of appropriate booster or car seats for children to ensure adequate fit and function of seat belts.
Driving Safely
Patients should never drive while under the influence of drugs, including certain medications or alcohol
Never text and drive
Make Spaces Safer For Children
Install baby gates and window latches in the home
May in areas with shock-absorbing material, such as hardwood mulch or sand
Supervise children carefully, especially when they�re near water
Prevent Falls
Clearing tripping hazards such as loose rugs, uneven flooring or walkway clutter
Using nonslip mats in the bathtub and on shower floors, and installing grab bars next to the toilet, tub and shower
Ensure appropriate footwear
Installing handrails on both sides of stairways
Improving lighting throughout the home
Balance training exercises
Balance Training
Single leg balance
Bosu ball training
Core strengthening
Brain balancing exercises
Concussion Verbiage
Concussion vs. mTBI (mild traumatic brain injury)
mTBI is the term being used more commonly in medical settings, but concussion is a more largely recognized term in the community by sports coaches, etc.
The two terms describe the same basic thing, mTBI is a better term to use in your charting
Evaluating Concussion
Remember that there does not always have to be loss of consciousness for there to be a concussion
Post-Concussion Syndrome can occur without LOC as well
Symptoms of concussion may not be immediate and could take days to develop
Monitor for 48 post head injury watching for red flags
Blurred eyesight or other vision problems, such as dilated or uneven pupils
Confusion
Dizziness
Ringing in the ears
Nausea or vomiting
Slurred speech
Delayed response to questions
Memory loss
Fatigue
Trouble concentrating
Continued or persistent memory loss
Irritability and other personality changes
Sensitivity to light and noise
Sleep problems
Mood swings, stress, anxiety or depression
Disorders of taste and smell
Mental/Behavioral Changes
Verbal outbursts
Physical outbursts
Poor judgment
Impulsive behavior
Negativity
Intolerance
Apathy
Egocentricity
Rigidity and inflexibility
Risky behavior
Lack of empathy
Lack of motivation or initiative
Depression or anxiety
Symptoms In Children
Concussions can present differently in children
Excessive crying
Loss of appetite
Loss of interest in favorite toys or activities
Sleep issues
Vomiting
Irritability
Unsteadiness while standing
Amnesia
Memory loss and failure to form new memories
Retrograde Amnesia
Inability to remember things that happened before the injury
Due to failure in recall
Anterograde Amnesia
Inability to remember things that happened after the injury
Due to failure to formulate new memories
Even short memory losses can be predictive of outcome
Amnesia may be up to 4-10 times more predictive of symptoms and cognitive deficits following concussion than is LOC (less than 1 minute)
Return To Play Progression
Baseline: No Symptoms
As the baseline step of the Return to Play Progression, the athlete needs to have completed physical and cognitive rest and not be experiencing concussion symptoms for a minimum of 48 hours. Keep in mind, the younger the athlete, the more conservative the treatment.
Step 1: Light Aerobic Activity
The Goal: Only to increase an athlete�s heart rate.
The Time: 5 to 10 minutes.
The Activities: Exercise bike, walking, or light jogging.
Absolutely no weight lifting, jumping or hard running.
Step 2: Moderate activity
The Goal: Limited body and head movement.
The Time: Reduced from typical routine.
The Activities: Moderate jogging, brief running, moderate-intensity stationary biking, and moderate-intensity weightlifting
Step 3: Heavy, non-contact activity
The Goal: More intense but non-contact
The Time: Close to typical routine
The Activities: Running, high-intensity stationary biking, the player�s regular weightlifting routine, and non- contact sport-specific drills. This stage may add some cognitive component to practice in addition to the aerobic and movement components introduced in Steps 1 and 2.
Step 4: Practice & full contact
The Goal: Reintegrate in full contact practice.
Step 5: Competition
The Goal: Return to competition.
Microglial Priming
After head trauma microglial cells are primed and can become over active
To combat this, you must mediate the inflammation cascade
Prevent repeated head trauma
Due to priming of the foam cells, response to follow-up trauma may be far more severe and damaging
What Is Post-Concussion Syndrome (PCS)?
Symptoms following head trauma or mild traumatic brain injury, that can last weeks, months or years after injury
Symptoms persist longer than expected after initial concussion
More common in women and persons of advanced age who suffer head trauma
Severity of PCS often does not correlate to severity of head injury
PCS Symptoms
Headaches
Dizziness
Fatigue
Irritability
Anxiety
Insomnia
Loss of concentration and memory
Ringing in the ears
Blurry vision
Noise and light sensitivity
Rarely, decreases in taste and smell
Concussion Associated Risk Factors
Early symptoms of headache after injury
Mental changes such as amnesia or fogginess
Fatigue
Prior history of headaches
Evaluation Of PCS
PCS is a diagnosis of exclusion
If patient presents with symptoms after head injury, and other possible causes have been ruled out => PCS
Use appropriate testing and imaging studies to rule out other causes of symptoms
Headaches In PCS
Often �tension� type headache
Treat as you would for tension headache
Reduce stress
Improve stress coping skills
MSK treatment of the cervical and thoracic regions
Constitutional hydrotherapy
Adrenal supportive/adaptogenic herbs
Can be migraine, especially in people who had pre-existing migraine conditions prior to injury
Reduce inflammatory load
Consider management with supplements and or medications
Reduce light and sound exposure if there is sensitivity
Dizziness In PCS
After head trauma, always assess for BPPV, as this is the most common type of vertigo after trauma
Dix-Hallpike maneuver to diagnose
Epley�s maneuver for treatment
Light & Sound Sensitivity
Hypersensitivity to light and sound is common in PCS and typically exacerbates other symptoms such as headache and anxiety
Management of excess mesencephalon stimulation is crucial in such cases
Sunglasses
Other light blocking glasses
Earplugs
Cotton in ears
Treatment Of PCS
Manage each symptom individually as you otherwise would
Manage CNS inflammation
Curcumin
Boswelia
Fish oil/Omega-3s � (***after r/o bleed)
Cognitive behavioral therapy
Mindfulness & relaxation training
Acupuncture
Brain balancing physical therapy exercises
Refer for psychological evaluation/treatment
Refer to mTBI specialist
mTBI Specialists
mTBI is difficult to treat and is an entire specialty both in the allopathic and complementary medicine
Primary objective is to recognize and refer for appropriate care
Pursue training in mTBI or plan to refer to TBI specialists
Sources
�A Head for the Future.� DVBIC, 4 Apr. 2017, dvbic.dcoe.mil/aheadforthefuture.
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
�Heads Up to Health Care Providers.� Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 16 Feb. 2015, www.cdc.gov/headsup/providers/.
�Post-Concussion Syndrome.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 28 July 2017, www.mayoclinic.org/diseases-conditions/post- concussion-syndrome/symptoms-causes/syc-20353352.
Injured: In 2014, there were 2.8 million occupational injuries. This crossed all industries, but 75 percent were in those that provided a service.
These injuries can lead to time lost at work, decrease in production, depression, and temporary (or permanent) disability. These injuries can be caused by slip and fall, vehicle collisions, electrocution, struck by hazards, and caught in or between accidents. However, work related injury can also be caused by sitting at a desk or hunched over a computer for extended periods of time. Chiropractic has been shown to help workers who have been injured on the job, so they can return to work faster.
Injured
Common Occupational Injuries
Occupational injuries are vast and varied with a host of causes and many different symptoms. They can range from minor annoyances to significant damage that can lead to temporary or permanent disability. Some may require surgery while others require extended physical therapy, braces, and intensive medical treatments.
Thoracic outlet syndrome � This injury is caused by flexing the shoulder, carrying loads on your shoulders, and extending your arms above shoulder height for a prolonged period of time. It is marked by swelling, pain, dull ache, weakness, or a burning sensation in the affected area.
Elbow tendonitis (Epicondylitis) � This injury is caused by forceful or repeated forearm rotation while simultaneously bending the wrist. It is marked by swelling, dull ache, pain, burning, and weakness in the affected area.
Carpal tunnel syndrome � This injury can be caused by several things including vibratory tools, repetitive motion, and secondary factors. It is marked by numbness, pain, tingling, wasting of muscles at the thumb base, and burning.
DeQuervain�s disease � This injury is caused by forceful gripping and repetitive hand twisting. It is marked by pain at the thumb base.
Tendonitis/tenosynovitis � This injury is caused by sustained hyperextension of the knee, repetitive motion, and prolonged load overuse. It is marked by numbness, pain, and swelling in the hands.
Back and neck pain � This injury can have a wide variety of causes from repetitive motion to accident to improper equipment. It is the most common work related injury.
Preventing Workplace Injuries
While a few work related injuries are unavoidable, many can be prevented with a little extra attention and care. The American Chiropractic Association recommends the following practices to reduce the risk of a workplace injury.
Get regular exercise. This helps prevent back injuries by keeping your body strong, fit, and flexible.
If you do desk work, get a chair that fits you. This means that there should be two inches between the backs of your knees and the front edge of the seat. Your knees should be level with your hips or slightly below, never higher.
When doing computer work, use a foot rest for support and keep your knees between a 90 degree and 120-degree angle.
If your job requires you to sit for extended periods of time, take breaks at least every two hours to walk and stretch.
When you lift something heavy or awkward, don�t bend over to do it. Bend at your knees and hips, squatting as you pick up the object and let your legs do the work and keeping the object close to your body while your back remains straight. Do not let your body twist while you are trying to lift.
Of course, you should also follow all recommended and required safety guidelines for your workstation and place of employment.
Chiropractic For Workplace Injuries
Chiropractic care can help speed your recovery, improve your posture, and restore your mobility and strength. Through various chiropractic techniques, many of the occupational injuries listed here can be effectively treated. Chiropractic is a proven method for managing pain for the back and neck, but it has also been proven to be very beneficial for conditions like carpal tunnel, elbow tendonitis, and knee injuries.
Chiropractic�s whole body approach helps injured workers not only manage their pain and help heal their injury through adjustments, it can also help with soft tissue rehabilitation and other noninvasive therapies that improve range of motion. In short, chiropractic can help workers get back to work faster so less time is lost from work and the financial impact is greatly decreased.
Injury Medical Clinic: Accident Treatment & Recovery
Malik Decquir is an athlete who has learned how to accomplish anything he sets his mind to through chiropractic rehabilitation. The trainer’s at Push have taught Malik never to give up, always being there to help him achieve his fitness goals and offering nutritional as well as fitness advice when he needs it. Malik Decquir has found tremendous mental and physical support with the trainers at Push.
Chiropractic Rehabilitation
Sports medicine, also referred to as sport and exercise medicine is a branch of medicine that deals with physical fitness and the treatment and prevention of injuries related to exercise and sports. Although most sports clubs have used team doctors for several years, it is only because the late 20th century that sports medicine has emerged as a distinct field of healthcare in order to help treat sports injuries.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Whiplash Injuries: If you have ever had to deal with the pain of whiplash, you know how it can impact every aspect of your life. Whiplash can cause chronic pain and keep you from doing many activities you enjoy. Daily tasks can be painful or even impossible to carry out. Even milder cases can make turning your head from side to side complex.
Chiropractic is a very effective treatment for whiplash injuries that helps with pain management and enables you to heal faster. Your chiropractor can recommend exercises you can do at home between treatments and other lifestyle changes that will facilitate your healing and improve flexibility.
Whiplash Injuries
What Is Whiplash?
Whiplash is a term that describes an injury that is typically focused on the neck and spine. It is caused when the head and neck are thrown in one direction unexpectedly and quickly, then thrust in the opposite direction. The head is rapidly whipped, usually front to back. It can be whipped from side to side, though.
Most people associate whiplash with car accidents, but even turning one way while a child tugs your arm in another direction can cause it. Anything that jerks your head suddenly can cause whiplash.
What Damage Does Whiplash Cause?
The damage that is caused by whiplash is called vertebral subluxation. This type of subluxation is caused by injury, and a chiropractor can diagnose the injury and treat it. It is the most common source of discomfort and pain caused by injuries due to whiplash. There are different kinds caused by tension and emotional stress, poor sleeping, lousy posture, weak muscles, and inadequate diet.
The injury from whiplash is in the neck and spine, but the pain can extend to the head, arms, shoulders, hips, and legs. You can experience frequent headaches, numbness, and tingling in your hands and have difficulty walking or moving about. The pain can range from stiffness and soreness to stabbing and sharpness. The injury can affect various nerves, causing blurred vision, dizziness, low back pain, ear ringing, and even problems with your internal organs.
Chiropractic Treatment For Whiplash
Chiropractors will use different techniques to relieve the pain of whiplash and help with healing.
Chiropractic Adjustment The chiropractor performs spinal manipulation to move the joints into alignment gently. This will help to align the body to relieve pain and encourage healing.
Muscle Stimulation and Relaxation This involves stretching the affected muscles, relieving tension, and helping them relax. Finger pressure techniques may also be combined with trying to alleviate pain.
McKenzie Exercises These exercises help with disc derangement that whiplash causes. They are first performed in the chiropractor’s office, but the patient can be taught how to do them at home. This helps the patient have some degree of control in their healing.
Each whiplash case is different. Instances of varying whiplash have various symptoms. A chiropractor will evaluate the patient and determine the appropriate treatment case-by-case basis. The chiropractor will determine the best course of treatment that will relieve your pain and restore your mobility and flexibility.
Whiplash can be far more severe than you may realize. Any accident that causes whiplash injuries can result in the vertebrae moving out of alignment. This can damage and irritate the spinal nerves. Even whiplash from years ago can still affect you if you never saw a chiropractor. Your spine can still be out of alignment, and injury or trauma from years ago can cause problems that seem unrelated.
Injury Medical Clinic: Accident Treatment & Recovery
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine










 We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.






