Postural orthostatic tachycardia syndrome is a medical condition that causes lightheadedness and palpitations after standing. Can lifestyle adjustments and multidisciplinary strategies help reduce and manage symptoms?
Postural Orthostatic Tachycardia Syndrome – POTS
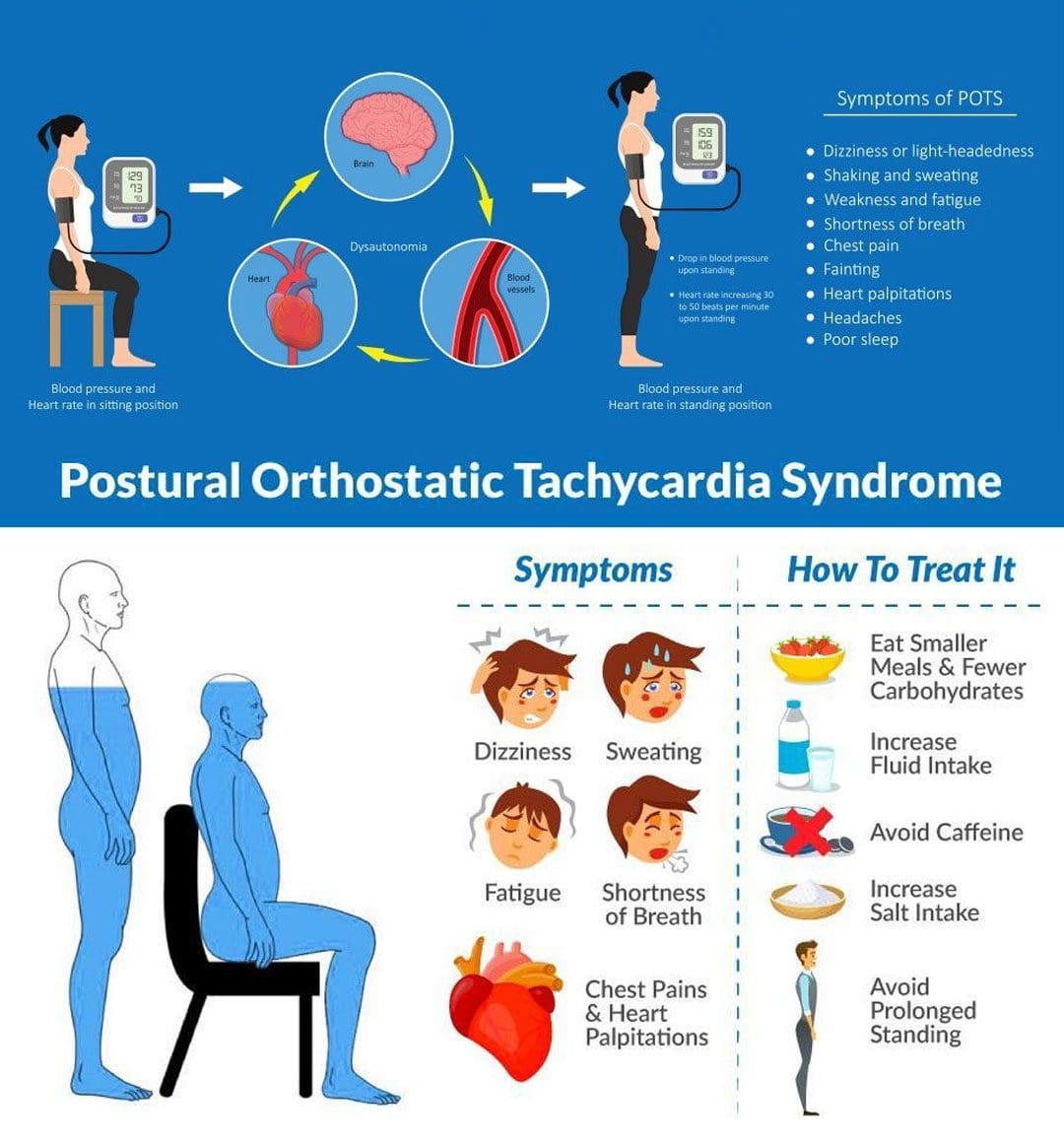
Postural orthostatic tachycardia syndrome, or POTS, is a condition that varies in severity from relatively mild to incapacitating. With POTS:
The heart rate increases dramatically with body position.
This condition often affects young individuals.
Most individuals with postural orthostatic tachycardia syndrome are women between the ages of 13 and 50.
Some individuals have a family history of POTS; some individuals report POTS began after an illness or stressor, and others report it began gradually.
It usually resolves over time.
Treatment can be beneficial.
Diagnosis is based on assessing blood pressure and pulse/heart rate.
Symptoms
Postural orthostatic tachycardia syndrome can affect young individuals who are otherwise healthy and can begin suddenly. It usually happens between the ages of 15 and 50, and women are more likely to develop it than men. Individuals can experience various symptoms within a few minutes of standing up from a lying or seated position. The symptoms can occur regularly and daily. The most common symptoms include: (National Institutes of Health. National Center for Advancing Translational Sciences. Genetic and Rare Diseases Information Center. 2023)
Anxiety
Lightheadedness
A feeling like you’re about to pass out.
Palpitations – sensing rapid or irregular heart rate.
Dizziness
Headaches
Blurred vision
Legs turn to reddish-purple.
Weakness
Tremors
Fatigue
Sleep problems
Trouble concentrating/brain fog.
Individuals may also experience recurrent episodes of fainting, usually without any trigger/s other than standing up.
Individuals can experience any combination of these symptoms.
Sometimes, individuals cannot handle sports or exercise and may feel light-headed and dizzy in response to mild or moderate physical activity, which can be described as exercise intolerance.
Associated Effects
Postural orthostatic tachycardia syndrome can be associated with other dysautonomia or nervous system syndromes, like neurocardiogenic syncope.
Individuals are often co-diagnosed with other conditions like:
Chronic fatigue syndrome
Ehlers-Danlos syndrome
Fibromyalgia
Migraines
Other autoimmune conditions.
Bowel conditions.
Causes
Usually, standing up causes blood to rush from the torso to the legs. The sudden change means less blood is available for the heart to pump. To compensate, the autonomic nervous system sends signals to the blood vessels to constrict to push more blood to the heart and maintain blood pressure and a normal heart rate. Most individuals do not experience significant changes in blood pressure or pulse when standing up. Sometimes, the body is unable to perform this function correctly.
If blood pressure drops from standing and causes symptoms like lightheadness, it is known as orthostatic hypotension.
If the blood pressure remains normal, but the heart rate gets faster, it is POTS.
The exact factors that cause postural orthostatic tachycardia syndrome are different in individuals but are related to changes in:
The autonomic nervous system, adrenal hormone levels, total blood volume, and poor exercise tolerance. (Robert S. Sheldon et al., 2015)
Autonomic Nervous System
The autonomic nervous system controls blood pressure and heart rate, which are the areas of the nervous system that manage internal bodily functions like digestion, respiration, and heart rate. It is normal for blood pressure to drop slightly and the heart rate to speed up a little when standing. With POTS, these changes are more pronounced.
POTS is considered a type of dysautonomia, which is diminished regulation of the autonomic nervous system.
Several other syndromes are also thought to be related to dysautonomia, like fibromyalgia, irritable bowel syndrome, and chronic fatigue syndrome.
It isn’t clear why the syndrome or any of the other types of dysautonomia develop, but there seems to be a familial predisposition.
Sometimes the first episode of POTS manifests after a health event like:
Pregnancy
Acute infectious illness, for example, a severe case of influenza.
An episode of trauma or concussion.
Major surgery
Diagnosis
A diagnostic evaluation will include a medical history, a physical examination, and diagnostic tests.
The healthcare provider will take blood pressure and pulse at least twice. Once while lying down and once while standing.
Blood pressure measurements and pulse rate lying down, sitting, and standing are orthostatic vitals.
Typically, standing up increases the heart rate by 10 beats per minute or less.
With POTS, heart rate increases by 30 beats per minute while blood pressure remains unchanged. (Dysautonomia International. 2019)
The heart rate stays elevated for over a few seconds upon standing/usually 10 minutes or more.
Symptoms happen frequently.
Lasts more than a few days.
Positional pulse changes are not the only diagnostic consideration for postural orthostatic tachycardia syndrome, as individuals can experience this change with other conditions.
During this test, blood pressure and pulse are measured several times when lying on a table and when the table is moved to an upright position.
Differential Diagnosis
There are various causes of dysautonomia, syncope, and orthostatic hypotension.
Throughout the evaluation, the healthcare provider may look at other conditions, like dehydration, deconditioning from prolonged bed rest, and diabetic neuropathy.
Medications like diuretics or blood pressure medication can cause similar effects.
Treatment
Several approaches are used in managing POTS, and individuals may require a multidisciplinary approach. The healthcare provider will advise regularly checking blood pressure and pulse at home to discuss the results when going in for medical checkups.
Fluids and Diet
Drinking non-caffeinated fluids can keep the body hydrated.
A healthcare provider can calculate the right amount of fluids that are needed each day.
Overnight dehydration is common, so it is especially important to drink fluids first thing in the morning, preferably before getting out of bed and standing.
Exercise and physical therapy can help the body learn to adjust to an upright position.
Because it can be challenging to exercise when dealing with POTS, a targeted exercise program under supervision may be required.
An exercise program may begin with swimming or using rowing machines, which do not require upright posture. (Dysautonomia International. 2019)
After a month or two, walking, running, or cycling may be added.
Studies have shown that individuals with POTS, on average, have smaller cardiac chambers than individuals who don’t have the condition.
Regular aerobic exercise has been shown to increase cardiac chamber size, slow heart rate, and improve symptoms. (Qi Fu, Benjamin D. Levine. 2018)
Individuals must continue an exercise program for the long term to keep symptoms from returning.
Medication
Prescription medications to manage POTS include midodrine, beta-blockers, pyridostigmine – Mestinon, and fludrocortisone. (Dysautonomia International. 2019)
Ivabradine, used for the heart condition of sinus tachycardia, has also been used effectively in some individuals.
Conservative Interventions
Other ways to help prevent symptoms include:
Sleeping in the head-up position by elevating the head of the bed off the ground 4 to 6 inches utilizing an adjustable bed, blocks of wood, or risers.
This increases the blood volume in circulation.
Performing countermeasure maneuvers like squatting, squeezing a ball, or crossing the legs. (Qi Fu, Benjamin D. Levine. 2018)
Wearing compression stockings to prevent too much blood from flowing into the legs when standing can help avoid orthostatic hypotension. (Dysautonomia International. 2019)
Conquering Congestive Heart Failure
References
National Institutes of Health. National Center for Advancing Translational Sciences. Genetic and Rare Diseases Information Center (GARD). (2023). Postural orthostatic tachycardia syndrome.
Sheldon, R. S., Grubb, B. P., 2nd, Olshansky, B., Shen, W. K., Calkins, H., Brignole, M., Raj, S. R., Krahn, A. D., Morillo, C. A., Stewart, J. M., Sutton, R., Sandroni, P., Friday, K. J., Hachul, D. T., Cohen, M. I., Lau, D. H., Mayuga, K. A., Moak, J. P., Sandhu, R. K., & Kanjwal, K. (2015). 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart rhythm, 12(6), e41–e63. https://doi.org/10.1016/j.hrthm.2015.03.029
Individuals in post-surgery recovery or dealing with illness or an injury can experience weakened muscles and endurance that can cause temporary loss of sleeping mobility and not being able to move around normally because of weakness, decreased range of motion, or pain. Can they benefit from physical therapy to help get back to normal functional mobility?
Sleeping Mobility
For individuals who are hospitalized or homebound from injury, illness, or surgical recovery, a physical therapist will assess various areas of functional mobility. These include transfers – from sitting to standing positions, walking, and sleeping mobility. Sleeping mobility is the ability to perform specific motions while in bed. A therapist can assess sleeping or bed mobility and recommend strategies and exercises to improve movements. (O’Sullivan, S. B., Schmitz, T. J. 2016) A therapist may have the individual use specific devices, like an over-the-bed trapeze or a sliding board, to help move around.
All of these movements require strength in different muscle groups. By checking out individual motions in sleeping mobility, a therapist can work out specific muscle groups that may be weak and require targeted exercises and stretches to restore mobility to normal. (O’Sullivan, S. B., Schmitz, T. J. 2016) Individuals visiting a therapist in an outpatient clinic or rehabilitation area may have the individual work on sleeping mobility on a treatment table. The same motions on the treatment table can be done in the bed.
Importance
The body is meant to move.
For individuals who cannot move comfortably on their bed, the body may suffer disuse atrophy or the wasting away of muscular strength, which can lead to increased difficulties. Not being able to move can also lead to pressure ulcers, especially for individuals who are severely deconditioned and/or remain in one position for a long period. Skin health may start to break down, leading to painful wounds that require specialized care. Being able to move around in bed can help prevent pressure ulcers. (Surajit Bhattacharya, R. K. Mishra. 2015)
Improvement
A physical therapist can prescribe specific exercises to strengthen muscle groups and improve sleeping mobility. The muscles include:
Shoulder and rotator cuff muscles.
Triceps and biceps in the arms.
Gluteus muscles of the hips.
Hamstrings
Quadriceps
Calf muscles
The shoulders, arms, hips, and legs work together when moving the body around the bed.
Various Exercises
To improve bed movement, physical therapy exercises can include:
Physical therapists are trained to assess these motions and functions and prescribe treatments to improve body movement. (O’Sullivan, S. B., Schmitz, T. J. 2016) Maintaining appropriate physical fitness can help the body stay active and mobile. Performing mobility exercises prescribed by a physical therapist can keep the right muscle groups working properly, and working with a physical therapist can ensure the exercises are correct for the condition and are performed properly.
Bhattacharya, S., & Mishra, R. K. (2015). Pressure ulcers: Current understanding and newer modalities of treatment. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India, 48(1), 4–16. https://doi.org/10.4103/0970-0358.155260
For individuals having difficulty moving or functioning normally due to injury, surgery, or illness, can a chiropractic and physical therapy team help expedite recovery?
Friction Massage
Individuals may develop scar tissue or tissue adhesions that limit normal motion after injury or surgery. A pain management team may use various treatments and modalities and may incorporate friction massage as part of a rehabilitation treatment plan. Friction massage, also known as transverse friction or cross friction massage, is a technique used to help improve scar tissue and adhesion mobility to move better and decrease the negative effects. The therapist uses their fingers to massage the scar in a direction that is at right angles to the scar line. It is a specialized technique that breaks up tissue adhesions that are limiting normal movement in the skin and underlying tissues. (Haris Begovic, et al., 2016)
Scar Tissue and Adhesions
For individuals who require surgery due to an injury or an orthopedic condition, their doctor will cut into the skin, tendons, and muscle tissue during the operation. Once sutured and healing has begun, scar tissue forms. Healthy tissue is made up of collagen that is comprised of cells that are arranged in a regular pattern. Healthy collagen is strong and can resist forces when tissues are pulled and stretched. (Paula Chaves, et al., 2017)
During the healing process after an injury, the collagen cells are laid down in a haphazard pattern and form scar tissue. The random accumulation of cells becomes tight and does not react well to tension and stretching forces. (Qing Chun, et al., 2016) The body can form scar tissue after a soft tissue injury, like a muscle or tendon strain. (Qing Chun, et al., 2016)
If a muscle or tendon gets strained the body will generate new collagen during the healing. The new collagen is laid down in a random fashion, and scar tissue or tissue adhesions can form that can limit the normal range of motion. Healthy tissue stretches and glides as the body moves. Scar tissue is rigid. At the site of the scar tissue, there can be some movement, but it is tight, less pliable, and can be painful. If scar tissue or adhesions are limiting motion, cross-friction massage can improve tissue gliding and sliding. This process is referred to as remodeling.
Massage Objectives
The objectives and goals of friction massage to adhesions or scar tissue may include:
Stimulation of nerve fibers to decrease and relieve pain.
The entire area of scar tissue or adhesion should be treated.
If the scar tissue is in a muscle, it should be relaxed.
If the scar tissue is in a tendon sheath, that tendon should be slightly stretched during the procedure.
The therapist places two or three fingers over the scar or adhesion and moves their fingers perpendicular to the scar to smooth the collagen fibers down.
The fingers and underlying tissues move together.
The massage should feel deep and uncomfortable but not painful.
There may be some pain, but should remain within the individual’s tolerance.
If the massage is too painful, less pressure may be used.
After several minutes the therapist will assess the tissue mobility.
Specific stretches may be done to elongate the scar tissue or adhesions.
At-home exercises and stretches may be prescribed to maintain flexibility.
Contraindications
There are situations where friction massage should not be used and can include: (Paula Chaves, et al., 2017)
Around an active open wound.
If there is a bacterial infection.
Areas with decreased sensation.
If calcification is present in the muscle or tendon tissue.
The therapist will explain the procedure and inform of the goals and risks associated with it.
Adhesive capsulitis in the shoulder/frozen shoulder.
Joint contracture.
Ligament tears.
Scar tissue buildup after surgery or trauma.
Friction massage is a popular technique used in physical therapy, but some research suggests it is not any more effective than other rehabilitation techniques. One study found that static stretches and exercises were more effective than massage in improving tissue length and strength in uninjured soccer players. Other studies have supported this, but individuals may find that the massage helps improve injured tissues’ movement as well. (Mohammed Ali Fakhro, et al. 2020)
The main goal of any treatment in physical therapy is to help the individual regain movement and flexibility. Friction massage, combined with targeted stretches and exercises, can help individuals expedite recovery and get back to normal.
Chiropractic Care After Accidents and Injuries
References
Begovic, H., Zhou, G. Q., Schuster, S., & Zheng, Y. P. (2016). The neuromotor effects of transverse friction massage. Manual therapy, 26, 70–76. https://doi.org/10.1016/j.math.2016.07.007
Chaves, P., Simões, D., Paço, M., Pinho, F., Duarte, J. A., & Ribeiro, F. (2017). Cyriax’s deep friction massage application parameters: Evidence from a cross-sectional study with physiotherapists. Musculoskeletal science & practice, 32, 92–97. https://doi.org/10.1016/j.msksp.2017.09.005
Chun, Q., ZhiYong, W., Fei, S., & XiQiao, W. (2016). Dynamic biological changes in fibroblasts during hypertrophic scar formation and regression. International wound journal, 13(2), 257–262. https://doi.org/10.1111/iwj.12283
Fakhro, M. A., Chahine, H., Srour, H., & Hijazi, K. (2020). Effect of deep transverse friction massage vs stretching on football players’ performance. World journal of orthopedics, 11(1), 47–56. https://doi.org/10.5312/wjo.v11.i1.47
Individuals feeling tingling or pins and needles sensations that overtake the arms or legs could be experiencing paresthesia, which occurs when a nerve has been compressed or damaged. Can knowing the symptoms and causes help in diagnosis and treatment?
Paresthesia Body Sensations
The numbness or tingling feeling when an arm, leg, or foot has fallen asleep is not so much about blood circulation but nerve function.
Paresthesia is an abnormal sensation felt in the body due to the compression or irritation of nerves.
It can be a mechanical cause like a compressed/pinched nerve.
Or it may be due to a medical condition, injury, or illness.
The symptoms typically last for 30 minutes or less.
Shaking the affected limb often relieves the sensations.
Paresthesia usually affects only one arm or leg at a time.
However, both arms and legs can be affected, depending on the cause.
Consult a healthcare provider if the symptoms last for more than 30 minutes. Treatment may be required if paresthesia body sensations are brought on by a serious underlying cause.
Causes
Sitting with incorrect and unhealthy postures can compress a nerve and generate symptoms. However, some causes are more concerning and can include:
If the symptoms don’t go away after 30 minutes or keep returning for unknown reasons, call a healthcare provider to find out what is causing the abnormal sensations. A worsening case should be monitored by a healthcare provider.
Peripheral neuropathy caused by diabetes usually begins with a feeling of paresthesia in the foot/feet and can worsen and lead to other complications.
A healthcare provider will work with the individual to understand the symptoms and perform the appropriate diagnostic tests to determine the cause. A healthcare provider will choose the tests based on a physical examination. Common diagnostic procedures include: (Merck Manual Professional Version. 2022)
Magnetic resonance imaging – MRI of the spine, brain, or extremities.
X-ray to rule out bone abnormalities, like a fracture.
Blood tests.
Electromyography – EMG studies.
Nerve conduction velocity – NCV test.
If paresthesia is accompanied by back or neck pain, a healthcare provider may suspect a compressed/pinched spinal nerve.
If the individual has a history of diabetes that is poorly controlled, they may suspect peripheral neuropathy.
Treatment
Treatment for paresthesia depends on the diagnosis. A healthcare provider can help determine the best course of action for the specific condition.
Nervous System
If symptoms are triggered by a central nervous condition like MS, individuals will work closely with their healthcare provider to get the appropriate treatment.
If paresthesia is caused by compression of a spinal nerve, like sciatica, individuals may be referred to a chiropractor and physical therapy team to release the nerve and pressure. (Julie M. Fritz, et al., 2021)
A physical therapist may prescribe spinal exercises to relieve compression of the nerve and restore normal sensations and motion.
Strengthening exercises to restore flexibility and mobility may be prescribed if weakness presents along with paresthesia body sensations.
Herniated Disc
If a herniated disc is causing the abnormal sensations, and there has been no improvement with conservative measures, a healthcare provider may suggest surgery to relieve pressure on the nerve/s. (American Association of Neurological Surgeons. 2023)
In surgical procedures like a laminectomy or discectomy, the objective is to restore nerve function.
Post-surgery, individuals may be recommended to a physical therapist to help regain mobility.
National Institute of Neurological Disorders and Stroke. (2023) Paresthesia.
American Association of Neurological Surgeons. (2023) Herniated disc.
National Institute of Diabetes and Digestive and Kidney Diseases. (2018) Peripheral neuropathy.
Merck Manual Professional Version. (2022) Numbness.
Razazian, N., Yavari, Z., Farnia, V., Azizi, A., Kordavani, L., Bahmani, D. S., Holsboer-Trachsler, E., & Brand, S. (2016). Exercising Impacts on Fatigue, Depression, and Paresthesia in Female Patients with Multiple Sclerosis. Medicine and science in sports and exercise, 48(5), 796–803. https://doi.org/10.1249/MSS.0000000000000834
Fritz, J. M., Lane, E., McFadden, M., Brennan, G., Magel, J. S., Thackeray, A., Minick, K., Meier, W., & Greene, T. (2021). Physical Therapy Referral From Primary Care for Acute Back Pain With Sciatica : A Randomized Controlled Trial. Annals of internal medicine, 174(1), 8–17. https://doi.org/10.7326/M20-4187
Are treatments more successful when patients know key terms that describe their back pain and associated conditions?
Nerve Pain Types
When individuals need to better understand their spine diagnosis, being able to distinguish between key terms can make a significant difference in understanding the development of a personalized treatment plan. Terms that describe back pain and various associated conditions can include:
Sciatica
Radiating and Referred pain
Radiculopathy
Radiculitis
Neuropathy
Neuritis
Causes of Back Pain
Back pain symptoms are most commonly caused by the continued practice of unhealthy/poor posture and overcompensated and weakened muscles. Even for individuals that exercise regularly, the movement choices that are made throughout the day can disrupt the way the muscles, tendons, ligaments, and fascia function to maintain proper body alignment.
Injuries to, and conditions of, the structures of the spinal column like the bones, discs, and nerves, are generally more serious than posture problems and soft tissue-related pain.
Depending on the diagnosis, structural problems can cause symptoms related to nerve compression, irritation, and/or inflammation. (Michigan Medicine, 2022)
Spine and Nervous System
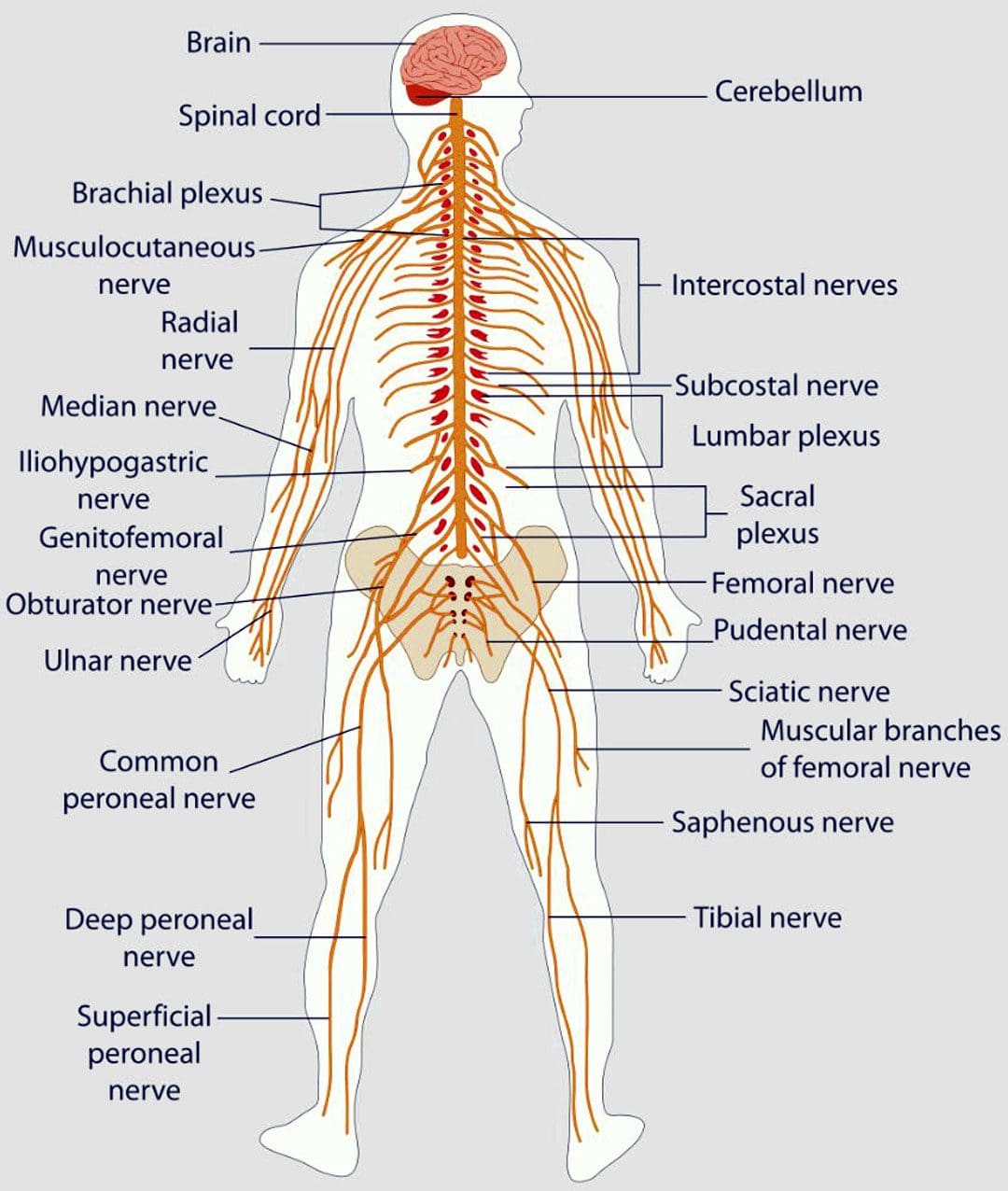
The peripheral nerves extend out to the extremities with sensation and movement capabilities.
Nerve roots exit the spinal canal which is part of the peripheral nervous system.
The branching of nerves from the spinal cord and exit out of the foramina occurs at every level of the spine.
Terms
There are different medical terms when getting a spine diagnosis or going through the treatment process.
Radiculopathy
Radiculopathy is an umbrella term, describing any disease process that affects a spinal nerve root and is something that’s happening to the body.
When a healthcare provider informs you that your pain is due to radiculopathy, a number of more specific diagnoses, clinical signs, and symptoms may be included as part of the description.
Common causes of radiculopathy include herniated disc/s and spinal stenosis.
Less common causes can include a synovial cyst or tumor that presses on the nerve root. (Johns Hopkins Medicine, 2023)
Radiculopathy can occur in the neck, low back, or in the thoracic area.
Often, radiculopathy is brought on by some form of compression of the nerve root.
For example, extruded material from a herniated disc can land on a nerve root, causing pressure to build.
This can cause symptoms associated with radiculopathy, including numbness, weakness, pain, or electrical sensations. (Johns Hopkins Medicine, 2023)
Even though there’s a spinal nerve root on either side of the spinal column, injury, trauma, or issues stemming from degeneration affect the nerves in an asymmetric fashion. Degenerative changes, known as normal wear and tear, typically occur in this fashion. Using the previous herniated disc example, the material that leaks from the disc structure tends to travel in one direction. When this is the case, the symptoms tend to be experienced on the side where the nerve root makes contact with the disc material, but not the other side. (American Association of Neurological Surgeons, 2023)
Radiculitis
Radiculitis is a form of radiculopathy but it is about inflammation and not compression. (Johns Hopkins Medicine, 2023)
Radicu– refers to the spinal nerve root.
The suffix – itis refers to inflammation.
The word refers to a spinal nerve root that is inflamed and/or irritated rather than compressed.
In disc herniations, it is the gel substance that contains various chemicals that is inflammatory.
When the gel substance makes contact with nerve roots, an inflammatory response is triggered. (Rothman SM, Winkelstein BA 2007)
Radiating or Referred Pain
Radiating pain follows the path of one of the peripheral nerves that transmit sensory information like heat, cold, pins and needles, and pain.
Referred pain is experienced in a different area of the body that is away from the pain source which tends to be an organ. (Murray GM., 2009)
It can be brought on by myofascial trigger points or visceral activity.
An example of referred pain is symptoms in the jaw or arm when an individual is having a heart attack. (Murray GM., 2009)
Radicular
The terms radicular pain and radiculopathy tend to get confused.
Radicular pain is a symptom of radiculopathy.
Radicular pain radiates from the spinal nerve root to either part or all the way down the limb/extremity.
However, radicular pain does not represent the complete symptoms of radiculopathy.
Radiculopathy symptoms also include numbness, weakness, or electrical sensations like pins and needles, burning, or shock that travels down the extremity. (Johns Hopkins Medicine, 2023)
Neuropathy
Neuropathy is another umbrella term that refers to any dysfunction or disease that affects the nerves.
It’s usually classified according to the cause, like diabetic neuropathy, or the location.
Neuropathy can occur anywhere in the body – including the peripheral nerves, the autonomic nerves/organ nerves, or nerves that are located inside the skull and innervate the eyes, ears, nose, etc.
Peripheral nerves are the long, thin strands that supply sensation, feeling, and movement impulses to all areas of the body located outside the central nervous system.
Piriformis syndrome is where a tight buttock/piriformis muscle constricts the sciatic nerve, which runs underneath. (Cass SP. 2015)
Chiropractic
Chiropractic adjustments, non-surgical decompression, MET, and various massage therapies can relieve symptoms, release stuck or trapped nerves and restore function. Through the treatments, the chiropractor and therapists will explain what is happening and why they are using a specific technique. Knowing a little about how the neuromusculoskeletal system operates can help the healthcare provider and the patient in developing and adjusting effective treatment strategies.
Sciatica During Pregnancy
References
Michigan Medicine. Upper and Middle Back Pain.
American Academy of Neurological Surgeons. Anatomy of the Spine and Peripheral Nervous System.
Johns Hopkins Medicine. Health Conditions. Radiculopathy.
American Association of Neurological Surgeons. Herniated Disc.
American Academy of Orthopaedic Surgeons. OrthoInfo. Cervical Radiculopathy (Pinched Nerve).
Rothman, S. M., & Winkelstein, B. A. (2007). Chemical and mechanical nerve root insults induce differential behavioral sensitivity and glial activation that are enhanced in combination. Brain Research, 1181, 30–43. https://doi.org/10.1016/j.brainres.2007.08.064
Murray G. M. (2009). Guest Editorial: referred pain. Journal of applied oral science: Revista FOB, 17(6), i. https://doi.org/10.1590/s1678-77572009000600001
American Academy of Orthopaedic Surgeons. OrthoInfo. Carpal Tunnel Syndrome.
Bostelmann, R., Zella, S., Steiger, H. J., & Petridis, A. K. (2016). Could Spinal Canal Compression be a Cause of Polyneuropathy? Clinics and practice, 6(1), 816. https://doi.org/10.4081/cp.2016.816
Cleveland Clinic. Mononeuropathy.
American Association of Neurological Surgeons. Glossary of Neurosurgical Terminology.
National Institutes of Health. U.S. National Library of Medicine. Medline Plus. Peripheral Nerve Disorders.
Cleveland Clinic. Spinal Stenosis.
Cass S. P. (2015). Piriformis syndrome: a cause of non-discogenic sciatica. Current sports medicine reports 14(1), 41–44. https://doi.org/10.1249/JSR.0000000000000110
Can chiropractic treatment protocols diagnose what’s causing head pressure in individuals, and provide effective treatment?
Head Pressure
Head pressure can have various causes and symptoms that affect different areas depending on whether the cause is a headache, allergies, injury, illness, or disease. The location of the pressure or pain can help a doctor of chiropractic determine the cause.
The underlying factor is usually not life-threatening, but the pressure that has built can be the result of serious conditions like a head injury or brain tumor.
Chiropractic care, which includes a combination of spinal manipulation, active and passive exercises, and massage, is often used for headache management and prevention. (Moore Craig, et al., 2018)
Chiropractic therapy is often sought out for tension and cervicogenic headaches, migraines, and each responds differently to the treatment.
The Head
The head is made up of a complex system of lobes, sinuses/channels, blood vessels, nerves, and ventricles. (Thau L, et al., 2022)
The pressure of these systems is regulated and any disruption to this balance can be noticeable.
Diagnosis can be difficult to figure out what is causing discomfort or head pressure.
Pain, pressure, irritability, and nausea are all symptoms that can occur with headaches. (Rizzoli P, Mullally W. 2017)
Head pressure can also occur only at times when standing up, bending down to pick up an object, or otherwise changing posture in some way that blood pressure is affected.
Chiropractic Treatment
The Injury Medical team will develop a personalized treatment plan to help relieve pressure symptoms through a multidisciplinary approach that can include. (Moore Craig, et al., 2018)
Moore, C., Leaver, A., Sibbritt, D., & Adams, J. (2018). The management of common recurrent headaches by chiropractors: a descriptive analysis of a nationally representative survey. BMC neurology, 18(1), 171. https://doi.org/10.1186/s12883-018-1173-6
Schizodimos, T., Soulountsi, V., Iasonidou, C., & Kapravelos, N. (2020). An overview of the management of intracranial hypertension in the intensive care unit. Journal of Anesthesia, 34(5), 741–757. https://doi.org/10.1007/s00540-020-02795-7
Wall M. (2017). Update on Idiopathic Intracranial Hypertension. Neurologic Clinics, 35(1), 45–57. https://doi.org/10.1016/j.ncl.2016.08.004
Factors that cause poor, unhealthy posture can be caused by the day-to-day effects of gravity on the body, personal, work, or sports injuries, illness, genetics, or a combination of these factors is also common. This leads to neck and back pain that leads to various musculoskeletal health issues. Achieving consistent healthy posture requires technique and practice. Chiropractic treatment with massage and/or physical therapy can restore muscles to optimal mobility and function.
Factors That Cause Unhealthy Posture
Factors that cause posture problems, like back pain, are often caused by issues with the strength and flexibility ratio between the body’s muscle groups that hold the body upright.
Muscle Guarding
After sustaining an injury, muscles can spasm to protect the injured and the surrounding area.
Muscle spasms can help keep injuries stable and protect them from worsening, but they can also limit movements and cause pain symptoms.
Prolonged muscle spasms can lead to weakened/vulnerable muscles, creating an imbalance between the muscles guarding against the injury and those still working normally.
This can cause the body posture to shift to compensate.
Muscle Tension
Muscle weakness or tension can develop when holding a prolonged position day after day or when doing daily tasks/chores in a way that places added stress on the body.
When certain muscle groups are weak or tense, posture will be affected.
Aches and pains begin to develop from the awkward positioning and the other muscles that must work overtime.
Unhealthy Habits
Compensation is when the body can still achieve its movement goal but with compromised and unhealthy alignment.
As the body compensates and accommodates muscle spasms, weakness, tension, and/or imbalance begin to present.
When this happens, the body may be forced to use alternate and less efficient muscle contraction and flexion patterns.
Technology
Using technology or working with several combined devices can slowly shift the body from correct alignment.
Incessant texting can cause text neck to develop, a condition in which the neck is held in too much flexion, or forward bending, for a prolonged time.
Discomfort, trigger points, and pain symptoms will develop, leading to further posture problems.
Stress and Mental Health
Individuals who experience stress regularly and easily are factors that cause posture problems.
Stress can contribute to shallow breathing or overly-contracted muscles, causing the body to shift out of alignment.
Adjusting posture can help counter the effects of stress.
Shoes
Footwear affects posture.
Heels extend the body’s weight forward, which can cause hip and spinal misalignment.
Individuals can wear down the outside or inside of their shoes faster because of things like:
Imbalanced kinetic forces will be translated up the ankle, knee, hip, and lower back.
This can lead to pain and discomfort in any of these joints.
Genetics
Sometimes, factors that cause unhealthy posture are hereditary.
For example, Scheuermann’s disease – a condition in which adolescent boys develop pronounced kyphosis in their thoracic spines.
It is recommended that the individual work with their primary/specialist healthcare provider in conjunction with a chiropractic specialist team for treatment and management.
Chiropractic treatment can help individuals achieve and maintain proper posture through various massage therapies to release tightness and relax the muscles, decompression to realign the spine, adjustments to realign the body, and postural training through exercises and stretches to develop healthy postural habits.
Quick Patient Intake
References
In, Tae-Sung et al., “Spinal and Pelvic Alignment of Sitting Posture Associated with Smartphone Use in Adolescents with Low Back Pain.” International Journal of Environmental Research and Public Health vol. 18,16 8369. 7 Aug. 2021, doi:10.3390/ijerph18168369
Korakakis, Vasileios, et al. “Physiotherapist perceptions of optimal sitting and standing posture.” Musculoskeletal Science & Practice vol. 39 (2019): 24-31. doi:10.1016/j.msksp.2018.11.004
Mansfield JT, Bennett M. Scheuermann Disease. [Updated 2022 Aug 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499966/
Mingels, Sarah, et al. “Is There Support for the Paradigm ‘Spinal Posture as a Trigger for Episodic Headache’? A Comprehensive Review.” Current pain and headache reports vol. 23,3 17. 4 Mar. 2019, doi:10.1007/s11916-019-0756-2
Mork, Paul Jarle, and Rolf H Westgaard. “Back posture and low back muscle activity in female computer workers: a field study.” Clinical biomechanics (Bristol, Avon) vol. 24,2 (2009): 169-75. doi:10.1016/j.clinbiomech.2008.11.001
Pope, Malcolm H et al. “Spine ergonomics.” Annual review of Biomedical Engineering vol. 4 (2002): 49-68. doi:10.1146/annurev.bioeng.4.092101.122107
Shaghayegh Fard, B et al. “Evaluation of forward head posture in sitting and standing positions.” The European Spine Journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society vol. 25,11 (2016): 3577-3582. doi:10.1007/s00586-015-4254-x
Tinitali, Sarah, et al. “Sitting Posture During Occupational Driving Causes Low Back Pain; Evidence-Based Position or Dogma? A Systematic Review.” Human Factors vol. 63,1 (2021): 111-123. doi:10.1177/0018720819871730
Wernli, Kevin, et al. “Movement, posture and low back pain. How do they relate? A replicated single-case design in 12 people with persistent, disabling low back pain.” European Journal of Pain (London, England) vol. 24,9 (2020): 1831-1849. doi:10.1002/ejp.1631
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine