Head and neck injuries related to phone use are on the rise. Since the first iPhone was released, according to a study in JAMA Otolaryngology-Head & Neck Surgery.
Doctors are warning cell phone users to be especially careful when:
Walking around and texting
It is a distraction and one of the leading causes of head and neck injuries.
2,501 reported cases of phone-related head and neck injuries that lead to emergency room visits between January 1998 and December 2017 found in a nationwide database. Injuries in teens and young adults aged 13 to 29 years old were about 40%, in women (55%) and men (45%).
Common Phone Injuries
Common injuries include:
Cuts
Bruises
Abrasions
Internal injuries usually happen around the eyes and nose
Possible trauma to the brain
Over 41% of these injuries happened at home and were minor with little or no treatment needed. Around 50% of injuries were a result of distracted driving and 30% from distracted walking.
Any type of phone distraction in and out of the home puts you and others at risk for:
Falls
Slips
Trips
All of which can lead to injuries and other possible consequences (e.g. a busted phone).
More individuals are getting injured because of phone use while moving around and not paying attention to what’s around them.
Children
Children under the age of 13 were at higher risk to suffer a mechanical injury like parents accidentally dropping the phone on their child or children hitting themselves in the face. For example, ninety cases of injuries occurred while playing Pokemon Go.
Spending as little as two to four hours a day hunched over a smartphone is enough to make a serious impact on the body over time. And though two to four hours may not seem like a long time, it isn�t hard to arrive at two hours by adding several 15-minute or half-hour segments together.
For teenagers, specifically, two to four hours on a smartphone has changed as of now teenagers spend around seven to eight hours on their phones. Spending twice as much time on afternoons or the space between classes or lunch. Think about the impact of 1500 plus hours of bad posture throughout the year. There is no surprise that teenagers are at risk.
The lasting impact of text neck and distracted phone use on today�s young people will be costly. Therefore, the public needs to be educated about the risks of distracted phone use and reducing this distracted behavior.
*Neck* Pain Chiropractic Care El Paso, Texas
NCBI Resources
If you begin noticing pain, spasms, or irritation around the neck, shoulders, or back make an appointment with a professional chiropractor. Explain when the pain occurred, the severity, and the activity that started it. A simple adjustment may be all that is needed to get re-aligned and gain relief from pain caused by overuse. A chiropractor can also help decrease the chances of the injury worsening over time.
SKULL FX: COMMON IN THE SETTINGS OF HEAD INJURIES. SKULL FX OFTEN POINT TO OTHER COMPLICATING FACTORS: INTRA-CRANIALHEMORRHAGING, CLOSED TRAUMATIC BRAIN INJURY AND OTHER SERIOUS COMPLICATIONS
SKULL X-RAYS ARE VIRTUALLY OBSOLETE IN EVALUATING HEAD INJURY. CT SCANNING W/O CONTRAST IS THE MOST IMPORTANT INITIAL STEP IN EVALUATION OF ACUTE HEAD TRAUMA. MRI HASA POOR ABILITY TO REVEAL SKULL FRACTURES, AND NOT TYPICALLY USED FOR AN INITIAL DX OF ACUTE HEAD TRAUMA.
SKULL FX ARE IDENTIFIED AS FXS OF SKULL VAULT, SKULL BASE AND FACIAL SKELETON EACH ASSOCIATED WITH SPECIFIC FEATURES AND HELP TO PREDICT COMPLICATIONS.
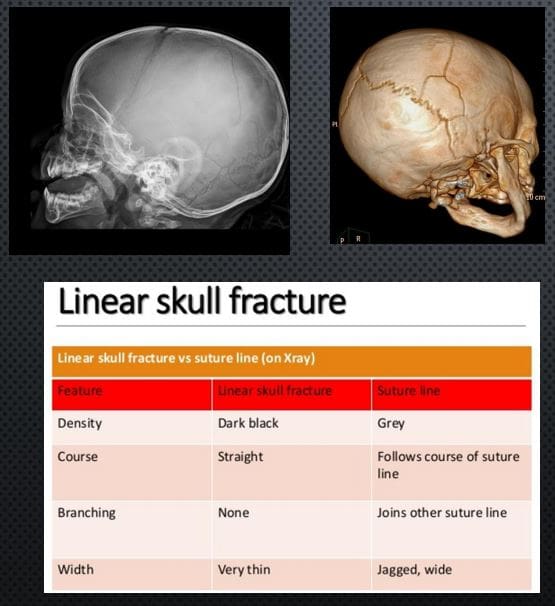
LINEAR SKULL FX: SKULL VAULT. M/C FX. CT SCANNING IS THE KEY TO EVALUATE ARTERIALEXTRADURAL HEMORRHAGING
X-RAY DDX: SUTURES VS. LINEAR SKULL FX. FX IS THINNER, �BLACKER� I.E. MORE LUCENT, CROSSESSUTURES,�AND VASCULAR GROOVES, LACKSSERRATIONS
RX: IF NO INTRACRANIAL BLEEDS THAT NO TREATMENT. NEUROSURGICAL CARE IF BLEEDSDETECTED BY CT SCANNING
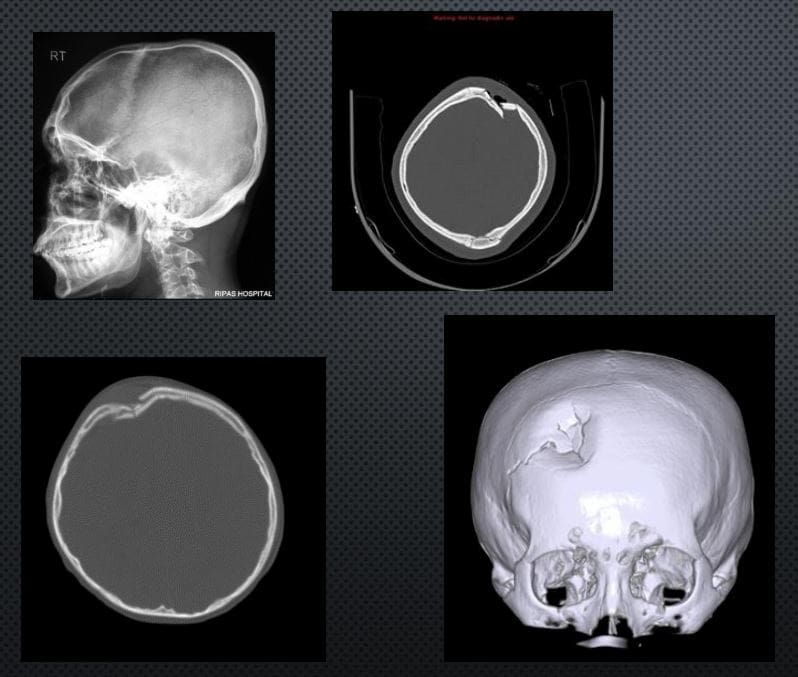
DEPRESSED SKULL FX: 75% IN THE VAULT. CAN BE DEADLY. CONSIDERED AN OPEN FX. MOST CASES NEED NEUROSURGICALEXPLORATION ESPECIALLY IFFRAGMENTS DEPRESSED >1-CM.COMPLICATIONS: VASCULAR INJURY/HEMATOMAS, PNEUMOCEPHALUS, MENINGITIS, TBI, CSF LEAK, BRAIN HERNIATION ETC.
IMAGING: CT SCANNING W/O CONTRAST
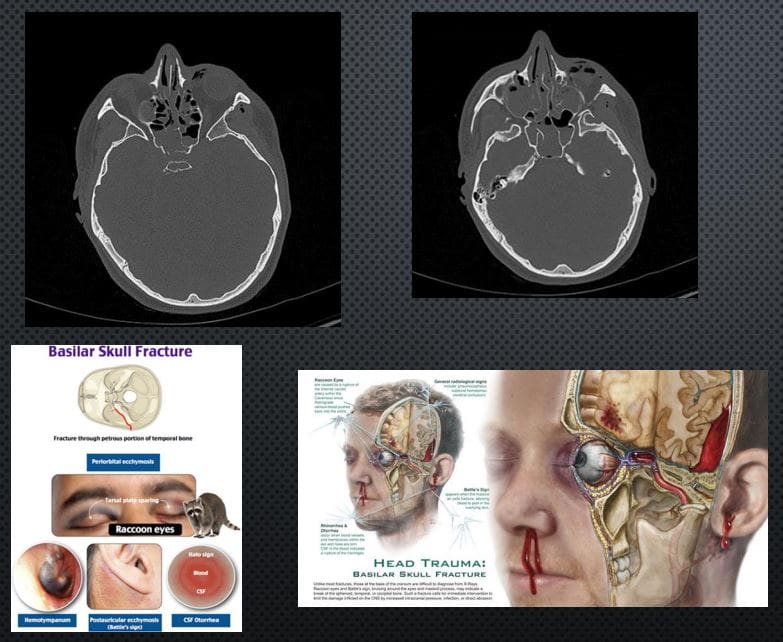
BASILAR SKULL FX: CAN BE DEADLY. OFTEN ALONG OTHER MAJOR HEAD TRAUMA OF THE VAULT AND FACIALSKELETON, OFTEN WITH TBI AND MAJORINTRACRANIAL HEMORRHAGING. OFTEN OCCUR AS �HEADBAND� EFFECT OF IMPACT AND MECHANICAL TENSION THROUGH THE OCCIPUT AND TEMPORAL BONES THROUGH SPHENOID AND OTHER BASE OF SKULL BONES. CLINICALLY: RACCOON EYES, BATTEL SIGN, CSFRHINO/OTORRHEA.
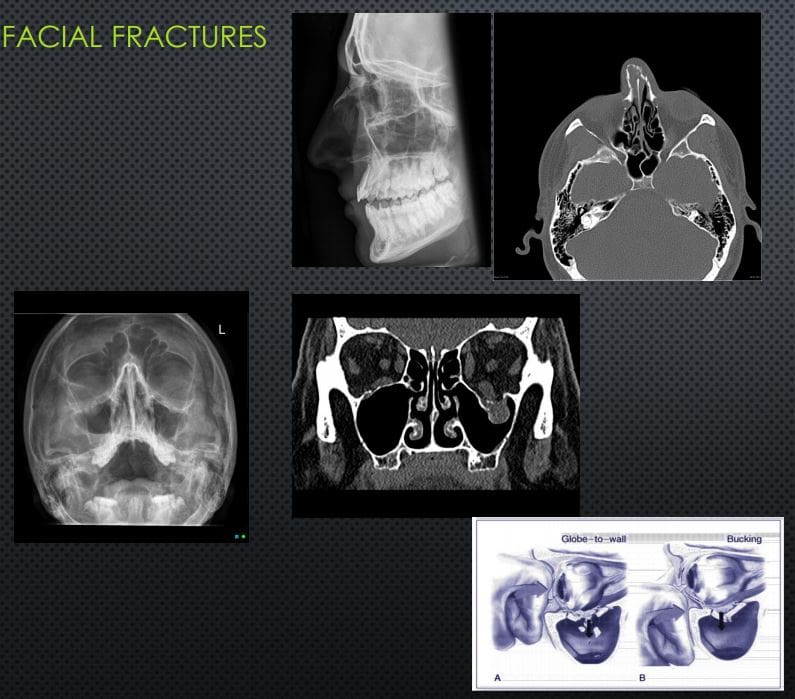
Facial Fractures
NASAL BONES FX: 45% OF ALLFACEFXM/C IMPACT IS LATERAL(FIST BLOW ETC.) IF UNDISPLACEDNO TREATMENT, IF DISPLACED MAY COMPLICATE AIR FLOW AND RESPIRATORY PASSAGE, MAY BE ASSOCIATED WITH OTHER FACIAL/SKULL INJURY. X-RAYS 80%SENSITIVE, FOLLOWED BY CT INCOMPLEX INJURIES.
ORBITAL BLOW OUT FX: COMMONORBITAL INJURY D/T IMPACT ON THE GLOBE AND/OR ORBITAL BONE. FX OF ORBITAL FLOOR INTOMAXILLARY SINUS VS. MEDIAL WALL INTO ETHMOID SINUS. COMPLICATIONS: ENTRAPPEDINFERIOR RECTUS M, PROLAPSEORBITAL FAT,�AND SOFT TISSUES, HEMORRHAGING AND OPTIC NERVE DAMAGE. RX: CONCERNS OF GLOBE INJURY ARE IMPORTANT, GENERALLY TREATEDCONSERVATIVELY IF NO COMPLICATIONS PRESENT
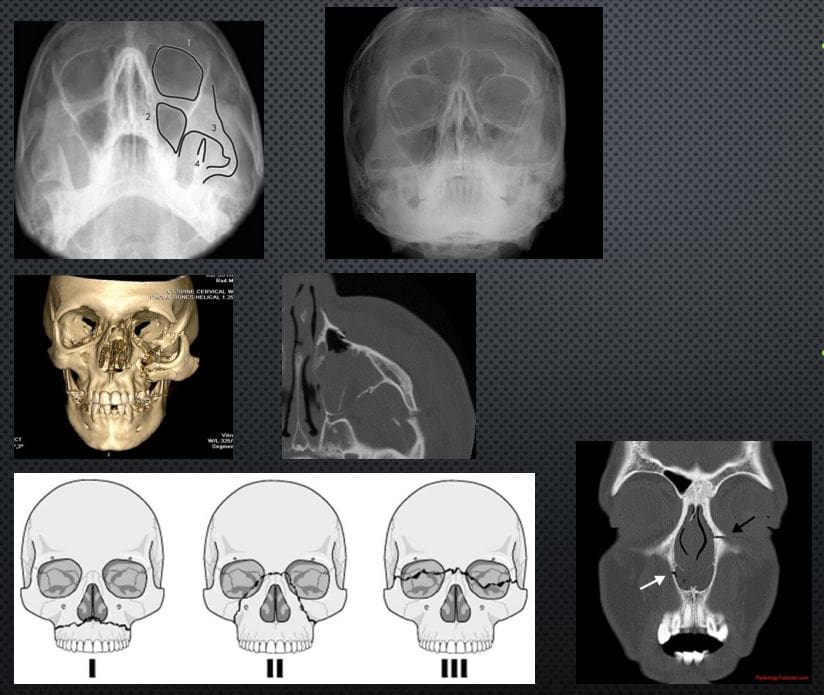
TRIPOD FX: 2ND M/C FACIAL FX#AFTER NASAL (40% OF MIDFACEFX) 3-POINT FX-ZYGOMATICARCH, ORBITAL PROCESS OF ZYGOMATIC BONE & SIDE OF MAXILLARY SINUS WALL, MAXILLARY PROCESS OF ZYGOMATIC BONE.COMPLICATED BY NERVE INJURY, TEMPORALIS M DAMAGE ETC. CT SCANNING IS MORE INFORMATIVE THAT X-RAYS (WATER�S VIEW).
LEFORT FX: SERIOUS FX ALWAYS INVOLVES PTERYGOID PLATES, POTENTIALLY SEPARATINGMIDFACE AND ALVEOLAR PROCESS WITH TEETH FROM THE SKULL. CONCERNS: AIRWAYS, HEMOSTASIS, NERVE INJURIES. CT SCANNING IS REQUIRED. POTENTIAL RISK OF BASILAR SKULL FX
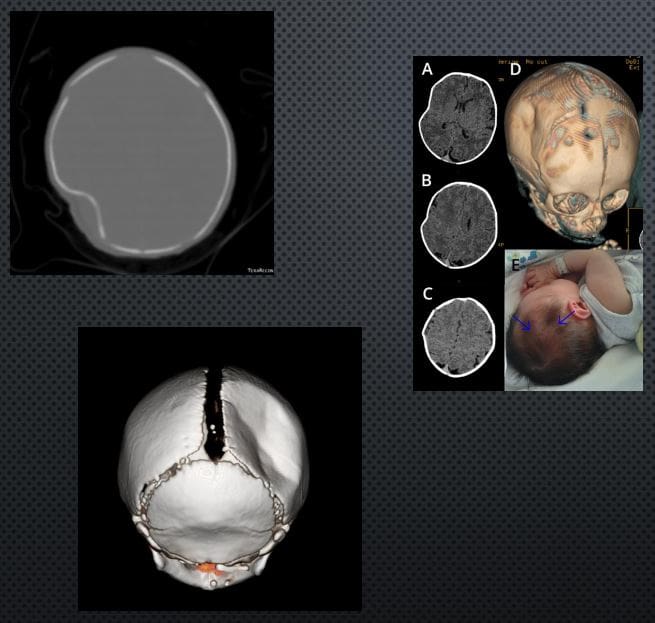
PING-PONG FX:�EXCLUSIVELY IN INFANTS. AN INCOMPLETE FX D/T FOCALDEPRESSION: FORCEPS DELIVERY, DIFFICULT LABOUR ETC. FOCALTRABECULAR MICROFRACTURIINGLEAVING DEPRESSION RESEMBLING APING-PONG. DX IS MAINLY CLINICALSEEN AS FOCAL DEFECT �DEPRESSION� IN THE SKULL. TYPICALLYNEUROLOGICALLY INTACT. CT MAY HELP IF BRAIN INJURY IS SUSPECTED. RX: OBSERVATIONAL VS. SURGICAL IN COMPLICATED INJURIES. SPONTANEOUSREMODELING HAS BEEN REPORTED
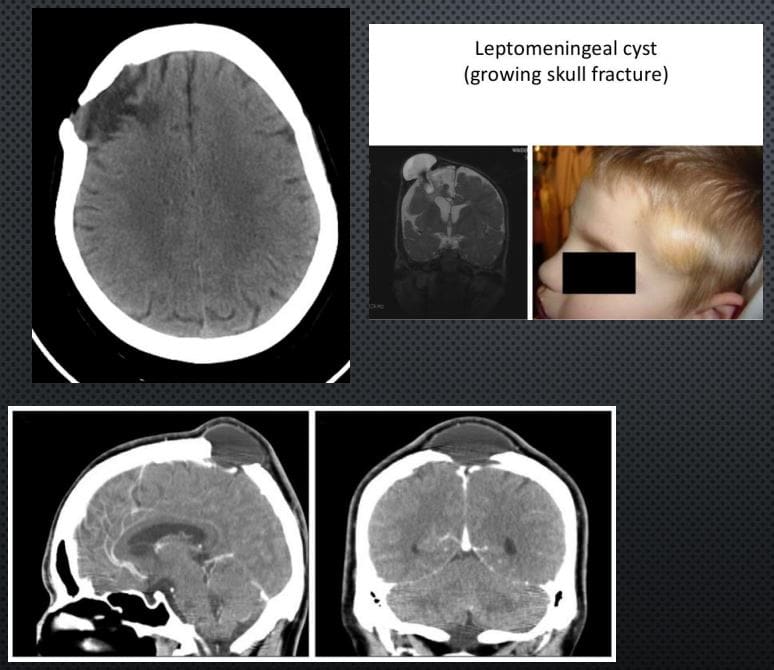
LEPTOMENINGEAL CYST (GROWING SKULL FX)- ARE AN ENLARGING SKULL FRACTURE THAT DEVELOPS ADJACENT TO POSTTRAUMATIC ENCEPHALOMALACIA
IT IS NOT A CYST, BUT AN EXTENSION OF THEENCEPHALOMALACIA THAT SEEN A FEW MONTHS POST-TRAUMA WITH PREVIOUS SKULL FX FOLLOWEDBY HERNIATION OF THE MENINGES AND ADJACENTBRAIN WITH PULSATIONS OF THE CSF. CT IS BEST ATDX THIS PATHOLOGY. INDICATES: GROWING FX AND ADJACENT ENCEPHALOMALACIA AS FOCALHYPOATTENUATING LESION.
DDX: INFILTRATING CELLS/METS/OTHER NEOPLASMSINTO SUTURES, EG, INFECTION ETC.
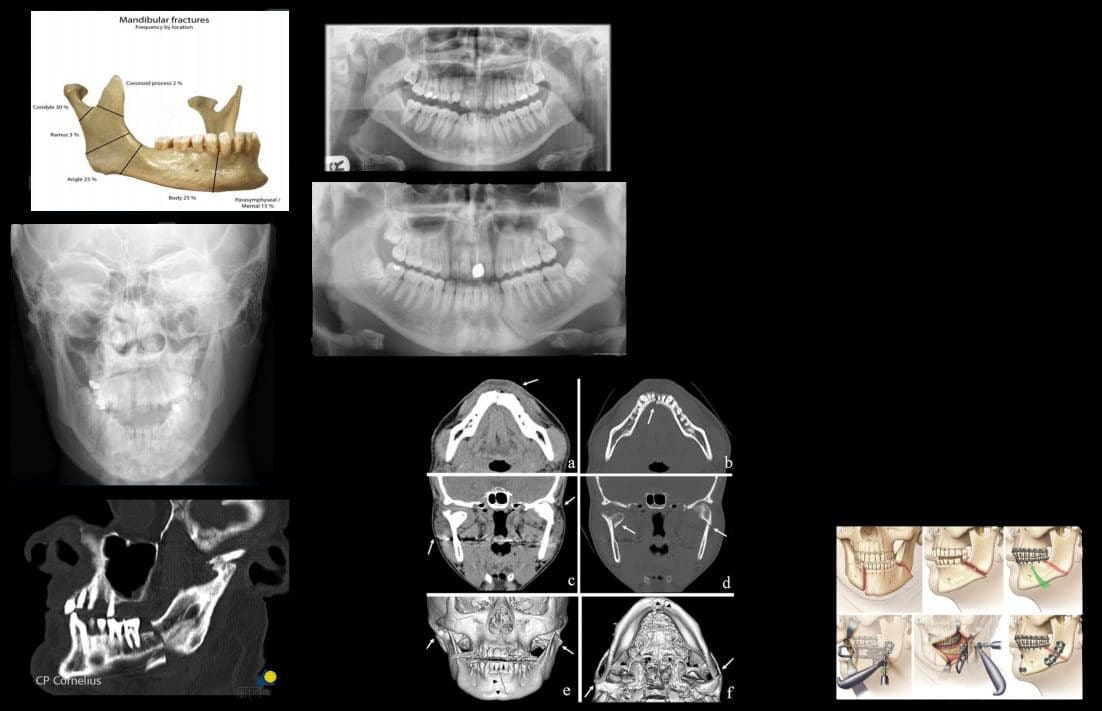
MANDIBULAR FXS: COMMON. POTENTIALLYCONSIDERED AN OPEN FX D/T INTRA-ORALEXTENSION. 40% FOCAL BREAK DESPITEMANDIBLE BEING A RING. DIRECT IMPACT(ASSAULT) M/C MECHANISM
PATHOLOGICAL FX D/T BONE NEOPLASMS, INFECTION ETC. IATROGENIC DURING ORAL SURGERY (TOOTH EXTRACTION)
IMAGING: MANDIBLE X-RAYS, PANOREX, CT SCANNING ESP. IN CASES OF ASSOCIATEDFACE/HEAD TRAUMA
COMPLICATIONS: AIRWAY OBSTRUCTION, HEMOSTASIS IS A MAJOR CONSIDERATION, DAMAGE TO MANDIBULAR N, OSTEOMYELITIS/CELLULITIS AND POTENTIAL SPREAD THROUGH FLOOR OF THE MOUTH (LUDWIGANGINA) AND NECK FASCIAL SOFT TISSUES INTOMEDIASTINUM. CANNOT BE NEGLECTED D/T HIGH MORTALITY RATES.
RX: CONSERVATIVE VS. OPERATIVE
Acute Intracranial Hemorrhage
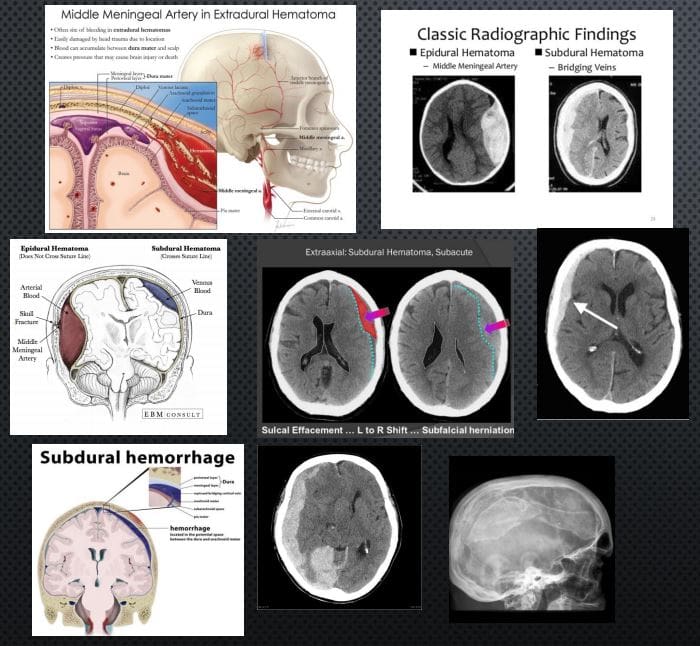
EPI AKA EXTRADURAL: (EDH) TRAUMATIC RAPTURE OF MENINGEAL ARTERIES (MMA CLASSIC) WITH RAPIDLY FORMING HEMATOMA BETWEEN THE INNER SKULL AND OUTER DURA. CT SCANNING IS THE KEY TO DX: PRESENTS AS �LENTIFORM� I.E. BICONVEX COLLECTION OF ACUTE (HYPERDENSE) BLOOD THAT DOES NOT CROSSSUTURES AND HELPS WITH DDX OF A SUBDURAL HEMATOMA. CLINICALLY: HA, LUCID EPISODE INITIALLY AND DETERIORATING IN A FEW HOURS.COMPLICATIONS: BRAIN HERNIATION, CN PALSY. O/A GOOD PROGNOSIS IF QUICKLY EVACUATED.
SUBDURAL HEMATOMA (SDH): RAPTURE OF BRIDGINGVEINS BETWEEN INNER DURA AND THE ARACHNOID.SLOW BUT PROGRESSIVE BLEED. MAY PARTICULARLYAFFECT THE VERY YOUNG AND ELDERLY AND IN ALL AGES (MVA, FALLS ETC.) MAY DEVELOP IN �SHAKEN BABY SYNDROME�. DX MAY BE DELAYED AND WORSEN THE PROGNOSIS WITH HIGH FATALITIES. IN ELDERLY HEAD TRAUMA MAY BE MINOR OR NOT RECALLED. EARLYIMAGING WITH CT IS CRUCIAL. PRESENTS AS CRESCENTSHAPEDCOLLECTION THAT CAN CROSS SUTURES BUT STOPPED AT DURAL REFLECTIONS. DIFFERENTATTENUATION ON CT D/T DIFFERENT STAGES OF BLOODDECOMPOSITION: ACUTE, SUBACUTE,�AND CHRONIC.MAY FORM A CHRONIC COLLECTION-CYSTICHYGROMA. CLINICALLY: VARIABLE PRESENTATION, 45-60% PRESENT WITH SEVERELY DEPRESSED CNS STATUS, PUPILLARY INEQUALITY. OFTEN WITH INITIAL BRAIN CONTUSION, THEN A LUCID EPISODE BEFORE SEVERELYDETERIORATING. IN 30% CASES OF FATAL BRAIN INJURY PATIENTS HAD SDH. RX: URGENT NEUROSURGICAL.
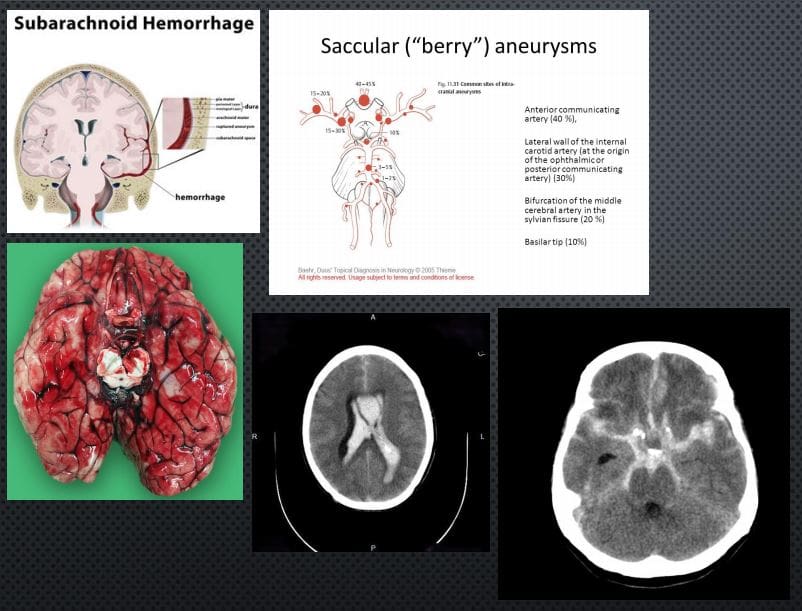
SUBARACHNOID HEMORRHAGE (SAH): BLOOD IN THE SUB-ARACHNOID SPACE AS THE RESULT OF TRAUMATIC OR NON-TRAUMATIC ETIOLOGY: BERRY ANEURYSMS AROUND CIRCLE OF WILLIS.SAH 3% OF STROKES, 5% OF FETAL STROKES.CLINICALLY: PRESENTS AS A �THUNDERCLAP HEADACHE� DESCRIBED AS A �WORST HA INLIFE�. PT COLLAPSES MAY OR MAY NOT REGAIN CONSCIOUSNESS. PATHOGY: DIFFUSE BLOOD INSA SPACE 1)SUPRASELLAR CISTERN WITH DIFFUSE PERIPHERAL EXTENSION, 2)�PERIMESENCEPHALIC, 3) BASAL CISTERNS. BLOOD LEAKED INTO SA SPACE UNDERARTERIAL PRESSURE INDUCES GLOBAL INCREASE IN INTRACRANIAL PRESSURE, ACUTE GLOBAL ISCHEMIA WORSENED BY VASOSPASM AND OTHER CHANGES.
DX: IMAGING: URGENT CT SCANNING W/O CONTRAST, CT ANGIOGRAPHY MAY HELP TO RULE OUT 99% OF SAH. LUMBAR PUNCTUREMAY HELP IN DELAYED PRESENTATION. AFTER INITIAL DX: MR ANGIOGRAPHY HELPS TO FIND THE CAUSE AND OTHER IMPORTANT FEATURES
IMAGING FEATURES: ACUTE BLOOD IS HYPERDENSE ON CT. FOUND IN DIFFERENTCYSTERNS: PERIMESENCEPHALIC, SUPRASELLA, BASAL, VENTRICLES,
RX: INTRAVENOUS ANTIHYPERTENSIVE MEDS, OSMOTIC AGENTS (MANNITOL) TO DECREASEICP. NEUROSURGICAL CLIPPING AND OTHER APPROACHES.
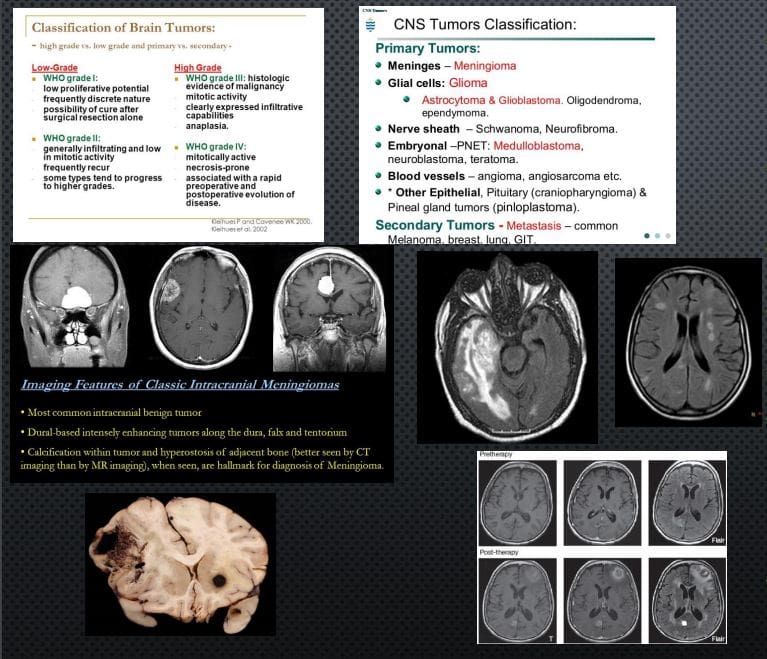
CNS Neoplasms: Benign vs. Malignant
BRAIN TUMORS REPRESENT 2% OF ALL CANCERS. ONE THIRD ARE MALIGNANT, OF WHICH METASTATIC BRAIN LESIONS ARE THE MOST COMMON
CLINICALLY PRESENT WITH LOCAL CNS ABNORMALITIES, INCREASED ICP, INTRACEREBRAL BLEEDING ETC. FAMILIALSYNDROMES: VON-HIPPEL-LANDAU, TUBEROUS SCLEROSIS, TURCOT SYNDROME, NF1 & NF2 INCREASE THE RISK. IN CHILDREN: M/C ASTROCYTOMAS, EPENDYMOMAS, PNETNEOPLASMS (E.G. MEDULLOBLASTOMA) ETC. DX: BASED ON WHO CLASSIFICATION.
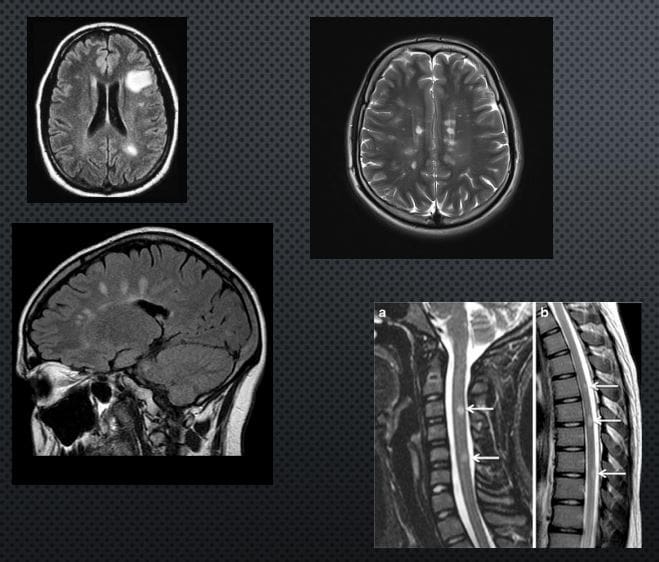
IMAGING IS CRUCIAL: INITIAL SYMPTOMS MAY PRESENT AS SEIZURE, ICP SIGNS HA. EVALUATED BY CT AND MRI WITH IV GADOLINIUM.
IMAGING DETERMINES: INTRA-AXIAL VS. EXTRA-AXIALNEOPLASMS. METS FROM PRIMARY BRAIN NEOPLASMS MAYO CCUR VIA CSF AND LOCAL VESSELS INVASION
NOTE AXIAL CT SLICE OF MENINGIOMA WITH AVIDCONTRAST ENHANCEMENT.
AXIAL MRI ON FLAIR PULSE SEQUENCE REVEALED EXTENSIVE NEOPLASM AND MARKED CYTOTOXIC EDEMA OF THE BRAIN PARENCHYMA CHARACTERISTIC OF GRADE IV GLIOMA (GBM) WITH VERY POOR PROGNOSIS. ABOVE FAR RIGHT IMAGE: AXIAL MRI FLAIR: BRAIN METASTASIS FROM BREAST CANCER. MELANOMA IS COMMONLY METASTASIZESTO THE BRAIN (SEE PATH SPECIMEN) MRI CAN BE DIAGNOSTIC D/T HIGH SIGNAL ON T1 AND CONTRAST ENHANCEMENT.
RX: NEUROSURGICAL, RADIATION, CHEMOTHERAPY,�IMMUNOTHERAPY TECHNIQUES ARE EMERGING
Concussions are traumatic brain injuries that affect brain function. Effects from these injuries are often temporary but can include headaches, problems with concentration, memory, balance and coordination. Concussions are usually caused by a blow to the head or violent shaking of the head and upper body. Some concussions cause loss of consciousness, but most do not. And it is possible to have a concussion and not realize it. Concussions are common in contact sports, such as football. However, most people gain a full recovery after a concussion.
Can also happen due to excessive shaking of the head or acceleration/deceleration
Mild injuries (mTBI/concussions) are the most common type of brain injury
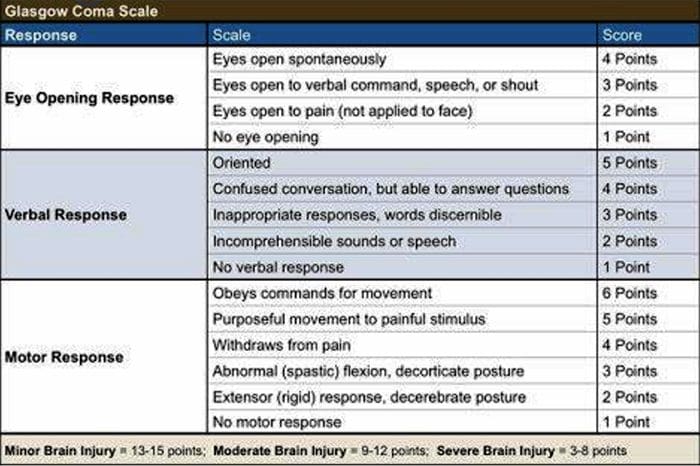
Glasgow Coma Scale
Common Causes Of Concussion
Motor vehicle collisions
Falls
Sports injuries
Assault
Accidental or intentional discharge of weapons
Impact with objects
Prevention
Prevention of concussive injuries can be paramount
Encourage Patients To Wear Helmets
Competitive sports, especially boxing, hokey, football and baseball
Horseback riding
Riding bicycles, motorcycles, ATVs, etc.
High elevation activates such as rock climbing, zip lining
Skiing, snowboarding
Encourage Patients To Wear Seatbelts
Discuss the importance of wearing seatbelts at all times in vehicles with all of your patients
Also encourage use of appropriate booster or car seats for children to ensure adequate fit and function of seat belts.
Driving Safely
Patients should never drive while under the influence of drugs, including certain medications or alcohol
Never text and drive
Make Spaces Safer For Children
Install baby gates and window latches in the home
May in areas with shock-absorbing material, such as hardwood mulch or sand
Supervise children carefully, especially when they�re near water
Prevent Falls
Clearing tripping hazards such as loose rugs, uneven flooring or walkway clutter
Using nonslip mats in the bathtub and on shower floors, and installing grab bars next to the toilet, tub and shower
Ensure appropriate footwear
Installing handrails on both sides of stairways
Improving lighting throughout the home
Balance training exercises
Balance Training
Single leg balance
Bosu ball training
Core strengthening
Brain balancing exercises
Concussion Verbiage
Concussion vs. mTBI (mild traumatic brain injury)
mTBI is the term being used more commonly in medical settings, but concussion is a more largely recognized term in the community by sports coaches, etc.
The two terms describe the same basic thing, mTBI is a better term to use in your charting
Evaluating Concussion
Remember that there does not always have to be loss of consciousness for there to be a concussion
Post-Concussion Syndrome can occur without LOC as well
Symptoms of concussion may not be immediate and could take days to develop
Monitor for 48 post head injury watching for red flags
Blurred eyesight or other vision problems, such as dilated or uneven pupils
Confusion
Dizziness
Ringing in the ears
Nausea or vomiting
Slurred speech
Delayed response to questions
Memory loss
Fatigue
Trouble concentrating
Continued or persistent memory loss
Irritability and other personality changes
Sensitivity to light and noise
Sleep problems
Mood swings, stress, anxiety or depression
Disorders of taste and smell
Mental/Behavioral Changes
Verbal outbursts
Physical outbursts
Poor judgment
Impulsive behavior
Negativity
Intolerance
Apathy
Egocentricity
Rigidity and inflexibility
Risky behavior
Lack of empathy
Lack of motivation or initiative
Depression or anxiety
Symptoms In Children
Concussions can present differently in children
Excessive crying
Loss of appetite
Loss of interest in favorite toys or activities
Sleep issues
Vomiting
Irritability
Unsteadiness while standing
Amnesia
Memory loss and failure to form new memories
Retrograde Amnesia
Inability to remember things that happened before the injury
Due to failure in recall
Anterograde Amnesia
Inability to remember things that happened after the injury
Due to failure to formulate new memories
Even short memory losses can be predictive of outcome
Amnesia may be up to 4-10 times more predictive of symptoms and cognitive deficits following concussion than is LOC (less than 1 minute)
Return To Play Progression
Baseline: No Symptoms
As the baseline step of the Return to Play Progression, the athlete needs to have completed physical and cognitive rest and not be experiencing concussion symptoms for a minimum of 48 hours. Keep in mind, the younger the athlete, the more conservative the treatment.
Step 1: Light Aerobic Activity
The Goal: Only to increase an athlete�s heart rate.
The Time: 5 to 10 minutes.
The Activities: Exercise bike, walking, or light jogging.
Absolutely no weight lifting, jumping or hard running.
Step 2: Moderate activity
The Goal: Limited body and head movement.
The Time: Reduced from typical routine.
The Activities: Moderate jogging, brief running, moderate-intensity stationary biking, and moderate-intensity weightlifting
Step 3: Heavy, non-contact activity
The Goal: More intense but non-contact
The Time: Close to typical routine
The Activities: Running, high-intensity stationary biking, the player�s regular weightlifting routine, and non- contact sport-specific drills. This stage may add some cognitive component to practice in addition to the aerobic and movement components introduced in Steps 1 and 2.
Step 4: Practice & full contact
The Goal: Reintegrate in full contact practice.
Step 5: Competition
The Goal: Return to competition.
Microglial Priming
After head trauma microglial cells are primed and can become over active
To combat this, you must mediate the inflammation cascade
Prevent repeated head trauma
Due to priming of the foam cells, response to follow-up trauma may be far more severe and damaging
What Is Post-Concussion Syndrome (PCS)?
Symptoms following head trauma or mild traumatic brain injury, that can last weeks, months or years after injury
Symptoms persist longer than expected after initial concussion
More common in women and persons of advanced age who suffer head trauma
Severity of PCS often does not correlate to severity of head injury
PCS Symptoms
Headaches
Dizziness
Fatigue
Irritability
Anxiety
Insomnia
Loss of concentration and memory
Ringing in the ears
Blurry vision
Noise and light sensitivity
Rarely, decreases in taste and smell
Concussion Associated Risk Factors
Early symptoms of headache after injury
Mental changes such as amnesia or fogginess
Fatigue
Prior history of headaches
Evaluation Of PCS
PCS is a diagnosis of exclusion
If patient presents with symptoms after head injury, and other possible causes have been ruled out => PCS
Use appropriate testing and imaging studies to rule out other causes of symptoms
Headaches In PCS
Often �tension� type headache
Treat as you would for tension headache
Reduce stress
Improve stress coping skills
MSK treatment of the cervical and thoracic regions
Constitutional hydrotherapy
Adrenal supportive/adaptogenic herbs
Can be migraine, especially in people who had pre-existing migraine conditions prior to injury
Reduce inflammatory load
Consider management with supplements and or medications
Reduce light and sound exposure if there is sensitivity
Dizziness In PCS
After head trauma, always assess for BPPV, as this is the most common type of vertigo after trauma
Dix-Hallpike maneuver to diagnose
Epley�s maneuver for treatment
Light & Sound Sensitivity
Hypersensitivity to light and sound is common in PCS and typically exacerbates other symptoms such as headache and anxiety
Management of excess mesencephalon stimulation is crucial in such cases
Sunglasses
Other light blocking glasses
Earplugs
Cotton in ears
Treatment Of PCS
Manage each symptom individually as you otherwise would
Manage CNS inflammation
Curcumin
Boswelia
Fish oil/Omega-3s � (***after r/o bleed)
Cognitive behavioral therapy
Mindfulness & relaxation training
Acupuncture
Brain balancing physical therapy exercises
Refer for psychological evaluation/treatment
Refer to mTBI specialist
mTBI Specialists
mTBI is difficult to treat and is an entire specialty both in the allopathic and complementary medicine
Primary objective is to recognize and refer for appropriate care
Pursue training in mTBI or plan to refer to TBI specialists
Sources
�A Head for the Future.� DVBIC, 4 Apr. 2017, dvbic.dcoe.mil/aheadforthefuture.
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
�Heads Up to Health Care Providers.� Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 16 Feb. 2015, www.cdc.gov/headsup/providers/.
�Post-Concussion Syndrome.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 28 July 2017, www.mayoclinic.org/diseases-conditions/post- concussion-syndrome/symptoms-causes/syc-20353352.
Expectant Mothers: Pregnancy is an exciting, precious time in a woman’s life, full of new experiences. Unfortunately, the baby’s development brings about bodily changes that often wreak havoc on the back and joints, and end up causing pain. These issues also frequently cause issues during delivery, and increase the time it takes for the body to recover post-pregnancy.
Expectant moms benefit from chiropractic care in a number of ways. Here are five key ways chiropractic care helps alleviate the toll pregnancy takes on a woman’s body.
#1: Expectant Mothers: Chiropractic Keeps The Spine In Alignment.
Pregnancy adds significant additional weight to a woman’s body in a short amount of time. This change bears on the spine, frequently pulling it out of alignment.
When this happens, the pain can be quite severe. Chiropractic care during pregnancy works to keep the spine in alignment and all supporting tendons working optimally, to be better prepared and able to adequately support the extra weight.
#2: Chiropractic Reduces Need For Pain Relievers.
Most times, individuals experiencing moderate pain pop a couple of over the counter pain relievers and think nothing of it. However, pregnant women strive to avoid medications when possible.
Chiropractic adjustments decrease the underlying issues that cause pain, so the patient relies less on medications. Experiencing less pain as well as eliminating the need for pain killers is a win-win situation for expectant mothers.
#3: Chiropractic Strengthens And Repairs Joints.
Pregnancy really beats up an expectant mothers joints. Chiropractic care for expectant mothers is a productive way to minimize the effect the large, protruding abdomen has on her hips, legs, and ankles.
Treating the body as a whole, chiropractic treatment works to strengthen the body and promotes healing of injured or strained areas.
#4: Chiropractic Helps Achieve Pelvic Alignment.
An aligned pelvis is critical to the birthing process, and increases the chances of being able to give birth naturally. According to the American Pregnancy Association,
“When the pelvis is misaligned it may reduce the amount of room available for the developing baby. This restriction is called intrauterine constraint. A misaligned pelvis may also make it difficult for the baby to get into the best possible position for delivery. This can affect the mother�s ability to have a natural, non-invasive birth.”
An experienced chiropractor can effectively align the pelvis before delivery, so the mother is able to deliver with little incident.
#5: Chiropractic Increases The Body’s Ability To Bounce Back.
Let’s face it, every pregnant woman thinks “will I ever fit in the clingy red dress again?” The healthier and stronger a woman’s body is before and during pregnancy, the easier it is to get back into shape once the baby is born. Eating right and safely exercising are effective ways to accomplish this.
Chiropractic care is also a valuable component to fitness. Expectant mothers who choose chiropractic enjoy better posture, less pain, and increased mobility, especially late in the third trimester.
This allows them to maintain exercise routines and be active longer than those suffering from back pain and achy joints. After the delivery, it’s easier to get back into a fitness routine, and into that red dress, if the new mother’s joints, back, and hips are aligned and functioning properly.
Chiropractic care can serve to reduce pain and increase the overall heath of expectant mothers, letting her relax and focus on the more pleasant aspects of pregnancy. Expecting women who commit to chiropractic care can look forward to a stronger body, the chances of a smoother delivery, and an easier recovery after the baby comes.
Pregnancy & Chiropractic Care
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine








 #3: Chiropractic Strengthens And Repairs Joints.
#3: Chiropractic Strengthens And Repairs Joints.




