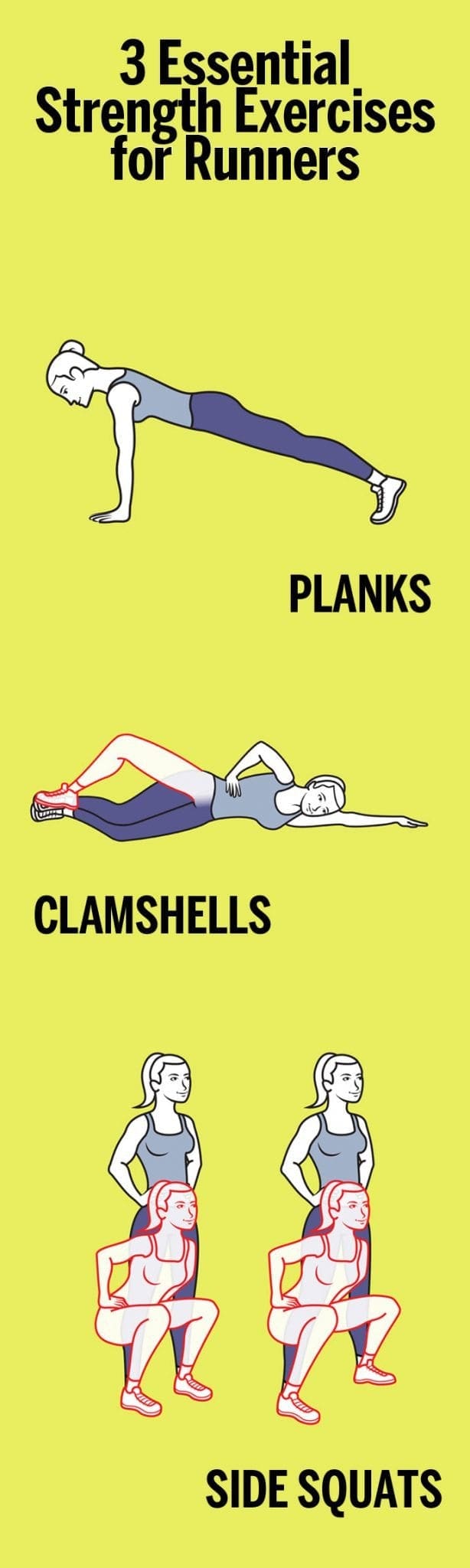
Trying to be a better runner? It’s not just about logging miles (although that certainly helps). The key to running strong and long also has a lot to do with shoring up your muscles, activating your core and back in addition to your lower body,�and keeping your movements fluid. To help do that, start incorporating these full-body strengthening�moves from Nike+ Run Club coach Julia Lucas to your routine three days a week, before or after a run. You’ll start noticing a difference in your strength in no time.
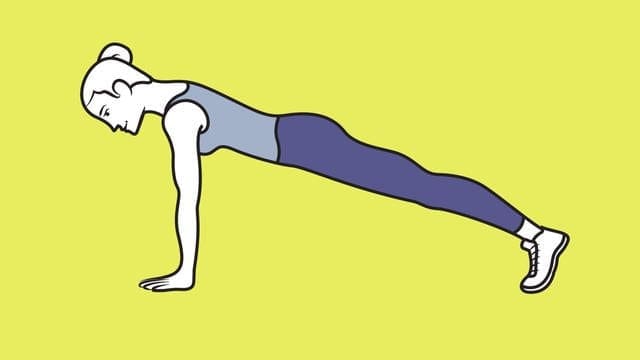
1. Planks
�
Planks have long been considered one of the best exercises for your core. In addition to your abs, this move engages your back, quads, and hamstrings, making it a great full-body exercise for runners. To do it, get into the �up� part of a push-up, with palms�on the floor directly under shoulders and legs extended behind you, forming a straight�line from head to heels. Hold for 10 to 30 seconds, keeping abs tight. Do�2 or 3 sets.
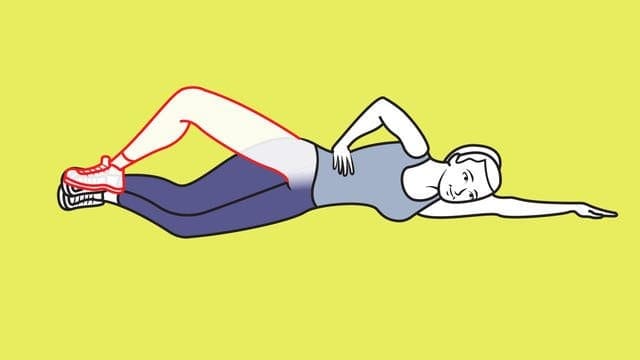
Clamshells work your hips and glutes, parts of the body that runners regularly need to activate. To do them, start out by lying�on your side with legs stacked and knees bent at 45 degrees. Rest head on arm; place top hand on hip. With inside edges of feet touching, lift top knee as high as you can without shifting hips or pelvis. Pause; lower knee. Do 2 or 3 sets of 10 reps per side.
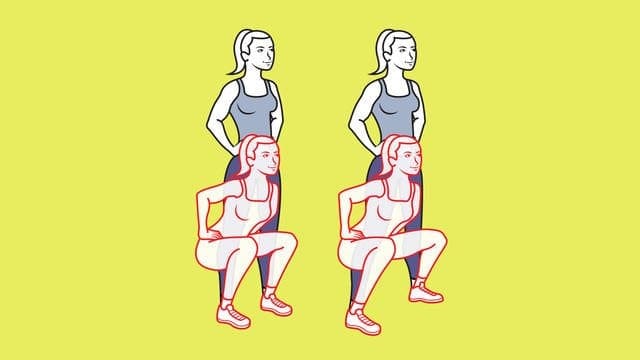
3. Side squats
Side squats are a great way to strengthen your outer highs, hips, and glutes. To do, stand with feet hip-width apart, hands on hips; squat. Stand; move left foot a step out. Squat again; step left foot in as you rise. Continue, alternating sides. Do 2 or 3 sets of 10 to 12 reps per side.
Men and women of a certain age realize quickly that their muscles diminish faster than they used to, and that muscles do not respond to exercise the way they used to. A new study shows that it’s all in the mitochondria — the part of the cell responsible for energy and vitality — and there is an exercise plan that can benefit the older crowd, even surpassing — surprisingly — benefits for the younger crowd.
Among various regimens of exercise, researchers found that interval training for a group older than 64 altered the working mechanisms in an amazing 400 genes — compared to only 274 for a group 30 or younger. The vitality in the older crowd’s cells responded more robustly than the younger crowd — adding another layer to the need for older folks to hit the gym.
Here’s how the experiment was conducted: 72 healthy but sedentary men and women were divided into two groups — 30 or younger, or older than 64 by researchers at the Mayo Clinic in Rochester, Minn. Their vitals were measured, including blood-sugar levels, gene activity, and mitochondrial health in their muscle cells. Then the volunteers were randomly assigned to 1 of 3 exercise regimens.
Some did vigorous weight training several times a week; some did brief interval training three times a week on stationary bicycles (pedaling hard for four minutes, resting for three minutes, then repeating for three times); some rode stationary bikes at a moderate pace for 30 minutes a few times a week and lifted weights lightly on other days. For control purposes, a fourth group did not exercise.
After 12 weeks, vitals were again checked for all involved. All exercise groups experienced improvements in fitness and blood sugar regulation.
Strength and endurance were affected differently, but predictively: The gains in muscle mass and strength were greater for those who exercised only with weights, while interval training had the strongest influence on endurance.
But biopsied muscle cell activity proved to be surprisingly different. Among the 30 and younger who went through interval training, the activity levels had changed in 274 genes, compared with 170 genes for those who exercised more moderately and 74 for the weightlifters. In the older crowd, almost 400 genes were working differently — more activley — for interval training, compared with 33 for the weightlifters and only 19 for the moderate exercisers.
Those who did the interval workouts showed increases in the number and health of their mitochondria. The takeaway: Interval training seems to be the best way to achieve vital cell health for muscle mass —particularly for those who are age 64 and older. Better muscle mass means a healthier, stronger body.
The decline in the cellular health of muscles associated with aging seemed corrected with interval exercise, especially if intense, Dr. Sreekumaran Nair, a professor of medicine and an endocrinologist at the Mayo Clinic and the study’s senior author, told The New York Times. Moreover, as his results show, older people’s cells responded in some ways more intensely than the cells of the younger group — suggesting, he says, it is never too late to benefit from exercise. Nair and his research team’s results were published in the journal Cell Metabolism.
New research has found more evidence to suggest a positive link between exercise and depression, this time finding that children who exercise could benefit from a reduce risk of developing depression in the future.
Carried out by a team from The Hospital for Sick Children (SickKids) and University of Calgary researchers at the Alberta Children’s Hospital, the study is the first meta-analysis to examine the potential protective effect of childhood physical activity on depression later in life.
According to the Canadian Mental Health Association 3.2 million children in Canada between the ages of 12 and 19 are at risk for developing depression.
A number of exercise intervention programs for children have been launched in recent years to support treatment for mental health issues, however current research shows large discrepancies on the effectiveness of exercise. Although some studies show strong support for physical activity’s effect on reducing depression, other studies show no relationship at all.
To look further into the validity of exercise interventions based on the existing evidence the team conducted a meta-analysis of 40 studies involving a total of 90,000 participants between the ages of eight and 19 years old. Study participants were healthy and had not been diagnosed with depression.
The team found a statistically significant association between increased physical activity and a lower risk of future depressive symptoms; however, the link was not as strong as they expected.
Explaining the results principal investigator, Dr. Daphne Korczak, said, “This suggests that physical activity is one factor, but that there are other factors that are important in determining a child’s risk for developing depression,” adding that factors such as having a family history of depression, particularly in a parent, or struggling at school academically or socially can all play a role.
Korczak added that further research looking at children with depression or examining the frequency, type or intensity of exercise would be useful in developing a better understanding of how physical activity affects the brain and the body to impact someone’s mood.
The Canadian Psychological Association recommends children and adolescents get 60 minutes of physical activity a day, but statistics published by the Canadian Society for Exercise Physiology suggest that only 15 percent of children (5 to 11 years) and five percent of adolescents (12 to 17 years) meet this recommended amount.
The study can be found online published in the journal Pediatrics.
Historically athletes were barefoot in the sporting arena and it is only a relatively recent phenomenon for shoes to be worn in competition. In Roman times wrestlers competed barefoot, whilst runners wore little more than thin leather sandals to compete over long distances.
More recently several athletes have achieved significant success competing barefoot: Abebe Bikila from Ethiopia won the Rome Olympic marathon in 1960, and Zola Budd became the world record holder over 5000 meters. Since the 1970�s athletic shoe manufacture has boomed and with it so too has the incidence of running-related lower limb injuries. This prompted the question of whether these new designs were to blame for the injuries or simply reflected the growing interest in distance running as a sport. That notwithstanding, the interest around barefoot running to reduce such injuries has grown exponentially. This account aims to appraise some of the literature on this contentious subject.
Gait Cycle & Running Biomechanics
The normal gait cycle consists of both stance and swing phases. The stance phase occupies 60% and swing 40% of the time taken to complete one cycle of consecutive heel striking by the same foot. The stance phase itself is divided into contact, midstance and propulsive phases. It begins and ends with both feet in contact with the ground known as the �double support phase�. The swing phase is divided into follow-through, forward swing and foot descent phases. The phases of running are very similar except for the fact that there is a flight phase when neither foot is in contact with the ground between stance phases. Evidently, with slower jogging the stance phase is longer than the flight phase, however, during sprinting this relationship reverses and the stance phase becomes the shorter of the two phases.
There are several key biomechanical considerations that must be borne in mind before a comparison can be made between barefoot and shod running. During running there is an increase in rotation at the pelvis, hip, and knee which must be absorbed by increasing the muscle forces acting over these joints. Moreover, as running speed increases the point of foot impact changes from predominantly heelstriking to that of forefoot weight-bearing when sprinting. The normal angle of gait is approximately 100 abducted from the line of progression. As speed increases this angle decreases approaching zero as the foot strike nears the line of progression. Runners who have developed stride patterns that incorporate low levels of impact force and rapid pronation are at a reduced risk for over-use running injuries such as stress fractures, plantar fasciitis, and ligamentous sprains. It is important to note that many shod runners never develop injuries, however, the available data indicates that 19-79% will develop an injury over their years spent running.
Biomechanical Abnormalities and Injury
Excessive Pronation � Pronation of the foot occurs at the sub-talar joint and when it occurs in excess is associated with many running-related injuries. Examples include, first metatarsophalangeal joint abnormalities, medial arch and plantar fascia strain, Achilles and tibialisposterior tendinopathy, patellofemoral joint dysfunction, and stress fractures. One study illustrated that shod running decreased torsion and increased pronation significantly, the paper concluded that the reduction in torsion produced by stiff soled shoes may well be a factor in running injuries caused by excessive pronation.
Excessive Supination
This movement also occurs at the subtalar joint and may compensate for a weakness of the antagonist pronating musculature (e.g. peroneal) or as a result of spasm or tightness of the supinating musculature (e.g. tibialis posterior, and the gastrocnemius- soleus complex). The supinated foot is less mobile and provides inferior shock-absorption which may well predispose to the development of stress fractures of the tibia, fibula, calcaneus and metatarsals. Lateral instability of the foot and ankle may be associated with excessive supination resulting in an increase incidence of ligamentous sprains of the foot and ankle. Such a lateral stress on the lower limb could result in tightening of the ileo-tibial band with associated bursitis of the femoral epicondyle.
Abnormal Pelvic Mechanics
During normal running the pelvis assumes a rotated position with anterior-posterior and lateral tilt. Weakness in the muscles needed for stabilisation of this position will result in excessive movement in any one of the three planes. A less efficient transfer of force will subsequently occur. The most common pelvic abnormalities are excessive anterior tilt, excessive lateral tilt and asymetrical pelvic movement. The complex inter-play of musculature to compensate for each of these abnormalities may well result in muscle tightness, strains and tendinopathy. Adaptation and biomechanics of running barefoot A leading study on the subject of barefoot running was conducted by Lieberman et al. who compared foot striking patterns and collision forces in habitually barefoot with shod runners. They found that habitually barefoot endurance runners often land on the fore-foot (fore-foot strike) before bringing down the heel. Less frequently they may also land with a flat foot (mid-foot strike), or even less often, on the heel (rear-foot strike). In contrast, shod runners mostly rear-foot strike which is facilitated by the elevated and cushioned heel of the modern running shoe.
The same study conducted kinematic and kinetic analyses on the two populations and discovered that even on hard surfaces, barefoot runners who fore-foot strike generate smaller collision forces than shod rear-foot strikers. This is brought about by the manner in which the barefoot runner�s foot is more plantarflexed at landing with a greater degree of ankle compliance at impact. These features combine to decrease the effective mass of the body that collides with the ground and so potentially reducing injury through repeated heavy loading. In addition, the stride length of barefoot runners is shorter and the strides have a greater vertical leg compliance which acts to lower the body�s centre of mass relative to the force of impact. Again, these features work to reduce jarring and result in a smoother running motion experienced by the individual.
Footwear and Injury
It has been surmised that modern footwear produces a lower level of perceived foot impact than that actually experienced and thus increases injury risk. There is good evidence to show that the more cushioning runners believe to be under the foot, the harder they strike. Furthermore, modern shoe designs are far more forgiving on poor running technique and since the athlete suffers less pain bad habits become re-inforced. In contrast, barefoot runners have been found to have a reduction in impact peak with reduced mechanical stress and enhanced ankle extensor function. In one particular study peak load in the hip and knee joints of participants with osteoarthritis was decreased significantly in barefoot walkers. These findings appear to point to the supposition that shoes may increase loads in poor physiological patterns and thus perpetuate injury.
Bipedalism has been around for millions of years and it is only relatively very recently that humans have been shod. The running technique of early distance running bipeds almost certainly differed enormously from the style that is seen today with modern foot-wear. The pre-historic �hunter-gatherer� would be more likely to have had a fore-foot or mid-foot-strike gait which studies have shown to be protective from many of the running injuries seen today.
Modern running shoes allow a greater degree of �laziness� in running style and in so doing ingrain bad habits which ultimately predispose to injury. Information on how barefoot running can be integrated into one�s training and how to overcome the obvious hazards of penetrating and friction injuries are growing at a great rate through internet forums and sites. There are already products available such as the Vibram FiveFingers� which are gaining in
popularity as the option of running barefoot or �nearly barefoot� grows. Furthermore, interest in the subject has been helped enormously by popular literature such as the bestselling book �Born to Run� by Christopher McDougall which follows the Tarahumara Indians of Northern Mexico who run ultra-marathons in simple leather strapped sandals.
In short, the evidence indicates two clear points. Firstly, from observations of populations who run barefoot or are habitually barefoot there appears to be lower injury rates versus the shod population. Secondly, the wearing of modern running shoes promotes a heavy impacting heelstrike gait which predisposes to injury. For the subject to gain wide-spread acceptance there will need to be an increase in the number of well designed prospective and randomised controlled trials on the subject.
References:
1. Clinical Sports Medicine by Peter Brukner and Karim Khan. Third Edition, Chapter 3; pp.45-55
2. Hreljac A. Impact and overuse injuries in runners.
Med Sci Sports Exerc 2004; 36:845-9 3. van Gent RN, Siem D, van Middelkoop M, van Os AG, Bierma-Zeinstra SM, Koes BW. Incidence and
determinants of lower extremity running injuries in long distance runners: a systematic review. Br J Sports Med 2007; 41(8):469-80
4. Buschbacher R, Prahlow N, Dave SJ (eds). Sports Medicine and Rehabilitation: A Sports Specific
Approac, 2nd ed. Baltimore (MD): Lippincott Williams and Wilkins; 2008, p. 200-1
5. Stacoff A, Kaelin X, Stuessi, Segesser B. The torsion of the foot in running. Int J Biomech 1989; 5:375-89
6. Lieberman DE, Venkadesan M, Werbel WA, Daoud AI, D-Andrea S, Davis IS, Mang-Eni RO, Pitsiladis Y. Foot strike patterns and collision forces in the
habitually barefoot versus shod runners. Nature 2010; 463:531-535 7. Jungers WL. Barefoot running strikes back. Nature
2010; 463:433-434 8. Robbins S, Waked E. Hazard of deceptive advertising of athletic footwear. Br J Sports Med
1997; 31(4):299-303. 9. Divert C, Mornieux G, BaurH, et al. Mechanical comparison of barefoot and shod running. Int J
Sports Med 2005; 26:593-8 10. Shakoor N, Block JA. Walking barefoot decreases loading on the lower extremity joints in knee
osteoarthritis. Arthritis Rheum 2006; 54:2923-7 11. Christopher McDougall. Born to run: the hidden
tribe, the ultra-runners and the greatest race the world has never seen. Profile books, published 2009.
12. Robbins SE, Hanna AM. Running-related injury prevention through barefoot adaptations. Med Sci Sports Exerc 1987.;19:148-56
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: What is Chiropractic?
Chiropractic care is an well-known, alternative treatment option utilized to prevent, diagnose and treat a variety of injuries and conditions associated with the spine, primarily subluxations or spinal misalignments. Chiropractic focuses on restoring and maintaining the overall health and wellness of the musculoskeletal and nervous systems. Through the use of spinal adjustments and manual manipulations, a chiropractor, or doctor of chiropractic, can carefully re-align the spine, improving a patient�s strength, mobility and flexibility.
Plantar fasciitis is a common affliction affecting many athletes, in particular runners. Adam Smith has written a great piece in the September issue of Sports Injury Bulletin outlining the relevant anatomy, how the injury occurs, how to differentiate from other similar pathologies, such as neural irritation in the tarsal tunnel, and finally how to manage it.
Speaking from experience as a former sufferer of plantar fasciitis, it can be a frustratingly recalcitrant condition and I have heard of some extreme measures to manage it. Read on for a story on the drastic measures an AFL player took to overcome the problem, and to understand more about the condition.
Many years ago an elite level AFL player had suffered a 2 year history of plantar fasciitis with no relief from any form of treatment. In the end the sports doctor at the club involved injected the plantar fascia origin with a corticosteroid injection the day before a game.
The hope was that as the plantar fascia weakened due to the steroid injection, the player would rupture it, go through the standard week rehab protocol, and then be pain free for ever more.
And yes, the player did rupture the plantar fascia during during the game and was consequently placed in a boot for about 10 days. He soon was walking, then running, and was playing again within four weeks with no more problems. The podiatrist made an orthotic to control the dropped arch and all the problems went away.
What has happened to that player now is anyone’s guess. He may now suffer from long term issues due to a poorly controlled arch that have caused other issues such as achilles tendon, knee pain and/or hip pain.
So do we really need the plantar fascia and why is it such a problem when it is injured?
Being bipedal (walking on two leg) animals, the plantar fascia gives the natural plantar arch support in weight bearing positions. It is a passive structure that acts like a high tension wire to keep the arch bones supinated as we push off.
Without a plantar fascia in place, we would need a better active system to create the arch support, such as the intrinsic plantar arch muscles, and also the extrinsic long arch support muscles such as the tibialis posterior, flexor hallucis longus (FHL) and the flexor digitorum longus (FDL). These muscles would need extra work to improve their arch control abilities. Alternatively, we could use a passive support mechanism in the form of an orthotic to control the arch position.
The majority of plantar fascia problems stem from a build up of tensile and compressive forces that degenerate the plantar fascia origin against the heel bone. The combination of tensile (stretch) force due to overpronation and the added compressive force as the plantar fascia is pushed against the heel bone leads to a pathological state whereby the plantar fascia degenerates and creates dysfunction and pain.
Therefore like other degenerative tendon issues (such as Achilles tendons) once the patient starts to feel pain often the injury has been building for months to years. Which explains why it then becomes so problematic to deal with.
Proper management takes time to not only correct the muscle imbalances that cause it � such as tight calves, poor hip control, poor pronation control � but due to its degenerative nature it requires a huge amount of time to even slightly change the existing pathology.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: What is Chiropractic?
Chiropractic care is an well-known, alternative treatment option utilized to prevent, diagnose and treat a variety of injuries and conditions associated with the spine, primarily subluxations or spinal misalignments. Chiropractic focuses on restoring and maintaining the overall health and wellness of the musculoskeletal and nervous systems. Through the use of spinal adjustments and manual manipulations, a chiropractor, or doctor of chiropractic, can carefully re-align the spine, improving a patient�s strength, mobility and flexibility.
Stress fractures to the ribs occur in rowers, golfer, canoeists, lacrosse players and baseball pitchers. They are more common in sports involving an element of trunk rotation with scapula movement across the rib cage.
A stress fracture is described as an overload to the bone caused by repetitive loading due to a particular movement. Any load on the bone will create a stress in the bone. However, given enough recovery time the bone heals and ends up stronger. This is known as Wolfe�s law. But, if the bone load is too high or too frequent, then the bone does not repair quickly enough, a stress response occurs and a fracture follows.
In rowing, the repetitive loading is created by a number of factors. Muscles such as the serratus anterior and abdominals that directly attach to the ribs can lead to loading on the ribcage due to contraction. Bad rowing technique, perhaps caused by poor hip flexibility, which then requires an excessive compensatory thoracic rotation, may then lead to rib breakdown.
Other causes include equipment issues such as the oar type (lighter carbon oars increase rib loading), bigger boats with more drag and position in the boat (bow rowers have less incidence due to lower stroke rate and force). Rib cross section and density also influence the chance of stress fractures, and women have a higher chance due to greater likelihood of bone density issues. Finally, training variables such as volume, intensity, type of loading and off water training can also be factors in stress fracture development.
The signs and symptoms are usually straight forward. These include generalised rib pain with a focused spot of tenderness, pain rolling onto the ribs whilst sleeping and pain with deep breathing. They can be confirmed with bone scan (black spot) and/or MRI (white spot).
Unfortunately for the rower, the immediate management of the injury involves rest. Usually 4-6 weeks away from rowing will be enough to allow some bone healing and this is followed by a progressive increase in rowing load over another 4 weeks before the athlete is back to full training.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: Chiropractic and Athletic Performance
Chiropractic care is a popular, alternative treatment option which focuses on the diagnosis, treatment and prevention of injuries and/or conditions associated to the musculoskeletal and nervous system, primarily the spine. Many athletes, and civilians alike, seek chiropractic care to restore their natural health and wellness, however, chiropractic has been demonstrated to benefit athletes by increasing their athletic performance.
The talk in soccer circles this week is the imminent return to action of Theo Walcott, the Arsenal and England star who damaged his knee back at the start of 2014. After 286 days of rehab, Walcott made a return to Arsenal’s Under 21 team last week. This has left journalists salivating at finding out when he will be returning to the main team.
For a young professional sports person, nine months is a long time out of the game. For Walcott, missing out on this Summer’s soccer World Cup in Brazil was perhaps more than just rubbing salt into the wound.
In issue 139 of Sports Injury Bulletin, I present a case study of a similar problem in a rugby player of identical age. This big lump of a kid ruptured his lateral meniscus in the knee — a bit different to Walcott’s ACL injury. However, this player also missed a big chunk of the season (17 weeks) and I had to live with his personal frustrations, and the yo-yo of daily emotions.
The piece shows the knee anatomy, details the types, clinical features and management of meniscus tears, and the required post-surgical rehabilitation.
On a recent Rehab Trainer course, one of the participants asked me what she should do about the small lateral meniscal tear in her knee. This is a bit like answering “how long is a piece of string?”, as it depends on so many things.
But to wrap it up in a nutshell, the surgeon will use a set of criteria to determine if a meniscal tear needs repairing, removing, or to be left well alone.
Criteria for Surgery
1. Age
The younger the patient, the more comfortable surgeons are about operating. Often the small degeneration tears in older patients are just a precursor to a knee that is about to become arthritic. With older patients, many surgeons will try for rehab first.
2. Function
This depends on what the knee has to do. If the patient does nothing but collect stamps all day and the knee does not bother them, then clearly the surgeon will want to leave it alone. But if the patient is an athlete with a repetitive catching and locking knee due to a meniscal tear, they will be more comfortable about operating.
3. Type of tear
Issue 139 of Sports Injury Bulletin details the types of tears we see in meniscus. In short, tears such as bucket handle tears do not do well without surgery, while small longitudinal tears can do well without surgery.
4. Location of tear
The outer portion of the meniscus has a nice, rich blood supply (hence, called the “red-red zone”). These areas can do well if left alone. Inner third zone tears (the “white zone”) with no blood supply don’t heal, so they need repairing or removing.
So, if the patient is lucky and fits the criteria for conservative management, or let’s say they simply don’t want surgery, then what options do we have to prevent the injury from getting worse?
Suggestions to Avoid Further Meniscus Injuries
Avoid positions that catch the meniscus. For example, full squatting may catch the posterior horn of the meniscus and flare it up, so the patient has to learn to avoid these positions if possible.
Keep the quadriceps working. If the quads remain strong and active then the shearing effect of the tibia moving across the femur is reduced. This will limit the stress to the meniscus.
Watch for swelling. Regular assessments for a knee effusion (called a “fluctuation test”) may need to be done a few times a week to make sure the knee stays dry. The knee’s biggest enemy is an effusion as it shuts off the quads straight away.
Intervene if the knee has an effusion. Donut felt compression, regular icing, NSAIDS if indicated, needle aspiration if indicated. Avoiding an effusion at all costs is pretty important for any knee injury.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Preventing Sports Injuries
Many athletes largely depend on chiropractic care to enhance their physical performance. New research studies have determined that aside from maintaining overall health and wellness, chiropractic can also help prevent sports injuries. Chiropractic is an alternative treatment option utilized by athletes to improve their strength, mobility and flexibility. Spinal adjustments and manual manipulations performed by a chiropractor can also help correct spinal issues, speeding up an athlete’s recovery process to help them return-to-play as soon as possible.
Perhaps you bent the wrong way while lifting something heavy. Or you�re dealing with a degenerative condition like arthritis. Whatever the cause, once you have low back pain, it can be hard to shake. About one in four Americans say they�ve had a recent bout of low back pain. And almost everyone can expect to experience back pain at some point in their lives.
Sometimes, it�s clearly serious: You were injured, or you feel numbness, weakness, or tingling in the legs. Call the doctor, of course. But for routine and mild low back pain, here are a few simple tips to try at home.
Chill It
Ice is best in the first 24 to 48 hours after an injury because it reduces inflammation, says E. Anne Reicherter, PhD, PT, DPT, associate professor of Physical Therapy at the University of Maryland School of Medicine. �Even though the warmth feels good because it helps cover up the pain and it does help relax the muscles, the heat actually inflames the inflammatory processes,� she says. After 48 hours, you can switch to heat if you prefer. Whether you use heat or ice � take it off after about 20 minutes to give your skin a rest. If pain persists, talk with a doctor.
Keep Moving
�Our spines are like the rest of our body � they�re meant to move,� says Reicherter. Keep doing your daily activities. Make the beds, go to work, walk the dog. Once you�re feeling better, regular aerobic exercises like swimming, bicycling, and walking can keep you � and your back � more mobile. Just don�t overdo it. There�s no need to run a marathon when your back is sore.
Stay Strong
Once your low back pain has receded, you can help avert future episodes of back pain by working the muscles that support your lower back, including the back extensor muscles. �They help you maintain the proper posture and alignment of your spine,� Reicherter says. Having strong hip, pelvic, and abdominal muscles also gives you more back support. Avoid abdominal crunches, because they can actually put more strain on your back.
Stretch
Don�t sit slumped in your desk chair all day. Get up every 20 minutes or so and stretch the other way. �Because most of us spend a lot of time bending forward in our jobs, it�s important to stand up and stretch backward throughout the day,� Reicherter says. Don�t forget to also stretch your legs. Some people find relief from their back pain by doing a regular stretching routine, like yoga.
Think Ergonomically
Design your workspace so you don�t have to hunch forward to see your computer monitor or reach way out for your mouse. Use a desk chair that supports your lower back and allows you to keep your feet planted firmly on the floor.
Watch Your Posture
Slumping makes it harder for your back to support your weight. Be especially careful of your posture when lifting heavy objects. Never bend over from the waist. Instead, bend and straighten from the knees.
Wear Low Heels
Exchange your four-inch pumps for flats or low heels (less than 1 inch). High heels may create a more unstable posture, and increase pressure on your lower spine.
These could be signs that you have a nerve problem or another underlying medical condition that needs to be treated.
Call Today!
Are Functional Orthotics Part of Your Wellness Protocol?
Most Chiropractors advertise pain relief without drugs and care for injuries. Recently, some doctors and practices have begun labeling and promoting themselves as Wellness Centers. A wellness practice is focused on both maintaining a pre-existing level of musculoskeletal balance and postural health and preventing conditions that might alter this state of health. The challenge is, how can healthy patients be protected from problems that might arise in the future? The answer is simple: custom-made orthotics. Custom orthotics may be traditionally seen as a preventative measure, but so are most treatments of old. They are the perfect, foundational support your patients will never want to go without.
Wellness is a great concept�one of those �win-win� situations for doctor and patient. Orthotics are the perfect way to implement this concept and help establish a �preventative� approach, in addition to the traditional reactive ones, if need be. Let�s take at a look at the foundation of the body, and see just how useful they can be.
Look To The Feet
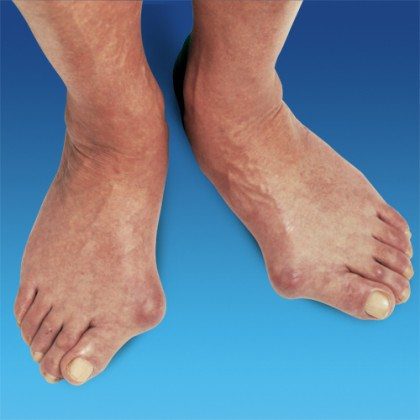
The feet are the foundation of the body. By age 40, nearly everyone has a foot condition of�some sort, many of which eventually contributing to health concerns farther up the Kinetic Chain (Figure 1). Therefore, it�s in the best interest of healthy patients to be offered a wellness program which stresses preventative care for normal, healthy feet, in order to prevent foot problems from occurring later in life.
�Pictured above, patient with severe bunions, or Hallux Valgus.
Figure 1. While 99% of all feet are normal at birth, 8% develop troubles by the first year of age, 41% at age 5, and 80% by age 20 (Fig. 1).�By age 40, nearly everyone has a foot condition of some sort.
How Can Orthotics Help?
Patients who participate in Chiropractic wellness programs can benefit from custom-made orthotics nearly as much as patients who seek Chiropractic care for musculoskeletal injuries and conditions. Foot Levelers� custom orthotics have been shown to effectively support the pedal foundation for both categories of patients, and can prevent problems well into the future with static and dynamic support.
Static support.Static support. A 1999 study using radiographic measurements found that custom-made, flexible orthotics can significantly improve the alignment of the arches when standing.2 In the wellness-practice concept of orthotic use, custom-made, flexible orthotics can be used to maintain a properly functioning arch alignment.
Dynamic support. During gait, the foot undergoes substantial changes and must permit a smooth transfer of the body�s center of mass over the leg in order to conserve energy and keep the work expenditure to a minimum.3 This requires a flexible, yet supportive orthotic that accommodates varying weights and forces and allows proper movement and function of the foot, while supporting all three arches�in order to prevent eventual arch collapse.
Postural benefits. Since the entire body structure is balanced on one foot at a time when walking and running, improving foot alignment can help maintain knee, hip, pelvic and even spinal postural alignment,4 and prevent joint degeneration (of the hip, knee, or spinal joints). A pelvic or spinal tilt or recurrent subluxations will often respond rapidly to orthotic support of the arches in the feet.
Orthotics For Everyone
Custom-made, flexible orthotics have long been recognized as a valid adjunct to Chiropractic care for many musculoskeletal conditions. In the wellness model of Chiropractic care, Foot Levelers� custom-made, flexible orthotics (Fig. 2) can be utilized as a preventative modality for the preservation of optimal arch support and the postponement or prevention of joint imbalances in later years. Therefore, orthotics are appropriate for virtually all Chiropractic patients.
The truth: How much water you should drink each day really, truly depends on the person, Robert A. Huggins, PhD, of the University of Connecticut explained to Health. �Fluid needs are dynamic and need to be individualized from person to person. Factors such as sex, environmental conditions, level of heat acclimatization, exercise or work intensity, age, and even diet need to be considered.�
What this means is that simply listening to your thirst is the best way to gauge when to drink. Another way to monitor hydration is to look at your pee before you flush. You want it to look like lemonade; if it’s darker than that, you should down a glass.
Drinking Water and Exercise
To gauge how much water you specifically should take in during exercise, Huggins recommends doing a small experiment on yourself.
First, before you work out weigh yourself wearing with little to no clothing. �If you can, [make sure you’re hydrated beforehand] and avoid drinking while you exercise to make the math easy,” Huggins says. But if you get thirsty, don’t ignore it: drink some and make sure to measure the amount.
After you’re done exercising, weigh yourself again. Then, take your first weight and subtract the second weight, and you�ll end up with how much fluid you lost. Convert this to kilograms (if you search it, Google will return the number for you or try a metric converter), then drink that amount in liters. (If you drank some water during exercise, subtract the amount of water you drank from your final total.)
This is your “sweat rate,” Huggins says. It’s the amount of water you should drink during or after your next workout to replace what you’ve lost. (You can also use an online calculator for sweat rate; just plug in your numbers.)
Complicated much? We agree. Huggins estimates that most people lose between one to two liters of sweat for each hour of moderate intensity exercise. But ultimately thirst should still be your guide.
Why It’s Essential to Drink the Right Amount
You already know that dehydration can be dangerous, but over-hydrating may actually be just as bad.
In fact, a new consensus report in the British Journal of Sports Medicine found that many athletes are at risk of exercise-associated hyponatremia, which is an electrolyte imbalance that can be caused by drinking too much liquid. This can lead to nausea and vomiting, headaches, fatigue, and in serious cases, coma and even death.
While it was previously thought to only be a concern for long-distance athletes competing in events like marathons and Ironmans, the paper (which was funded by CrossFit, Inc.) concluded that many athletes are actually dangerously over-drinking during events as short as 10K races and even bikram yoga classes, Tamara Hew-Butler, PhD, lead author of the paper, explained to Health.
Because “it is impossible to recommend a generalized range especially during exercise when conditions are dynamic and changing, there is not one size that fits all!” she adds.
So the best method to keep you in that sweet spot between over- and under-hydrated is, as with many things, to listen to your body.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: Whole Body Wellness
Chiropractic care is well-known as a safe and effective alternative treatment option utilized to improve as well as maintain whole body health and wellness. Common chiropractic treatment methods and techniques, such as spinal adjustments and manual manipulations, can be used to treat a variety of injuries and/or conditions, including neck pain and back pain. Regular chiropractic care along with a balanced nutrition and physical exercise is a natural approach to ensure the body’s overall health and wellness, restoring the individual’s original well-being.
Wondering exactly how much protein you should be consuming each day? The Recommended Dietary Allowance (RDA), which is the minimum amount you need to be healthy, is 0.8 grams per kilogram (0.36 grams per pound) of body weight per day�46 grams for an average woman. That equals as little as 10% of daily calories. If you’re not super active, that’s likely adequate, and you’ll hit the target effortlessly if you follow a typical Western diet.
To get your personal protein “RDA,” multiple the number 0.36 by your weight in pounds. (For a sedentary 150-pound woman, that would be 54 grams.) Double it if you’re very active or aiming for “optimal protein,” which can help you maintain muscle as you age and support weight loss.
American women already eat about 68 grams a day, according to the latest data from the National Health and Nutrition Examination Survey. “There’s no reason to go out of your way to get protein,” says Dariush Mozaffarian, MD, dean of the Tufts Friedman School of Nutrition Science & Policy. “Just eat a variety of fish, nuts, beans, seeds, and dairy, including yogurt.” However, increasing your protein well above the RDA may make sense if…
That means getting at least 35 to 40 minutes of moderate exercise four or five days a week, including resistance training two or more times a week. Consider eating 1.2 to 2 grams of dietary protein per kilogram (or about 0.5 to 0.9 grams per pound) of body weight each day, says Nancy Rodriguez, PhD, professor of nutritional sciences at the University of Connecticut. That amount is best for rebuilding muscle tissue, especially if you do a lot of high-intensity workouts, research suggests.
Protein takes longer to digest than carbs, helping you feel full, and also pushes your body to secrete the gut hormone peptide YY, which reduces hunger. “When you bring protein to about 30% of your daily calories, you’ll naturally eat less,” says Lauren Slayton, RD, founder of Foodtrainers, a nutrition practice in New York City, and author of The Little Book of Thin. “Protein decreases appetite and also, in my experience, helps you manage cravings.”
While studies are mixed about whether consuming more protein leads to weight loss, research is pretty clear that protein can help you retain more of your lean muscle as you lose fat. One 2011 study suggests amping up protein to as much as 1.8 to 2 grams per kilogram (roughly 0.8 to 0.9 grams per pound) of body weight per day to stave off muscle loss when restricting calories. Cut back on refined carbs to balance out the extra calories from adding protein.
Eating more protein as you get older may help you maintain muscle and ward off osteoporosis, “so you can stay stronger and more functional,” says Rodriguez. In a 2015 study, adults over the age of 50 who roughly doubled the RDA (eating 1.5 grams of protein per kilogram, or 0.68 grams per pound, of body weight) were better able to rebuild and retain muscle after only four days, compared with control groups eating the RDA.
Doubling the RDA gives you “optimal protein,” a concept that Rodriguez and more than 40 nutrition scientists advanced at a recent Protein Summit, the findings from which were published in 2015 in The American Journal of Clinical Nutrition. Optimal protein works out to be about 15% to 25% of your daily calories, still below the level recommended by many popular high-protein diets. Over a day, that could look like 20-30 grams per meal and 12 to 15 grams per snack, for a total of 90 to 105 grams daily.
Be sure to consult your healthcare provider on the proper nutrition and diet according to your specific needs.
For more information, please feel free to ask Dr. Jimenez or contact us at 915 850-0900 .
Additional Topics: What is Chiropractic?
Chiropractic care is an well-known, alternative treatment option utilized to prevent, diagnose and treat a variety of injuries and conditions associated with the spine, primarily subluxations or spinal misalignments. Chiropractic focuses on restoring and maintaining the overall health and wellness of the musculoskeletal and nervous systems. Through the use of spinal adjustments and manual manipulations, a chiropractor, or doctor of chiropractic, can carefully re-align the spine, improving a patient�s strength, mobility and flexibility.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




















 Static support.Static support. A 1999 study using radiographic measurements found that custom-made, flexible orthotics can significantly improve the alignment of the arches when standing.2 In the wellness-practice concept of orthotic use, custom-made, flexible orthotics can be used to maintain a properly functioning arch alignment.
Static support.Static support. A 1999 study using radiographic measurements found that custom-made, flexible orthotics can significantly improve the alignment of the arches when standing.2 In the wellness-practice concept of orthotic use, custom-made, flexible orthotics can be used to maintain a properly functioning arch alignment.

 Shoes for Kids
Shoes for Kids









