“The clinical diagnosis shows a disc bulge in their neck and some arthritis, so their neck symptoms are not associated with the crash. Lots of folks have those and do not have pain although it could be a minimal herniation. It’s our diagnosis that it was there before the crash.” This statement from an adjuster is an argument that has been made for many years, allowing insurance companies to inappropriately reduce settlements to their clients based on the client’s inability to prove when or how the damage or injury occurred. To factually counter this sort of statement, an individual must use imaging and age dating to discuss causality. Without medical experts utilizing the current medical and academic research available, it will continue to be difficult for any argument to be made explaining effects of these injuries and their mechanism based on fact vs. rhetoric.
Imaging of the spine is critically important in most cases of injured clients. In cases, imaging is necessary for proper diagnosis and future management of injuries. Imaging needs to be performed as per the academic and modern criteria to ensure an accurate diagnosis. The most common injuries in car accidents are spinal related, and the simple imaging available includes x-rays, CAT scans and magnetic resonance imaging (MRI), allowing medical providers to make an accurate diagnosis, when medically indicated.
Every medical provider has a permit to see and treat automobile related injuries. However a “license” is not the same as “specialization.” By way of example, though psychiatrists may have a license to do heart surgery and are MDs, it would not be in the patient’s best interest. Nor would I go to a spine surgeon for psychological concerns although they are licensed to treat medical conditions. In spinal trauma, certain suppliers specialize in connective tissue injuries of the spine, allowing us to go one step farther in diagnosis, prognosis and management, including “age-dating” these generally found disc and ligament injuries.
Understanding Age-Dating of Injuries
To understand age-dating, one wants to have a basic medical understanding of anatomy and physiology, and what tissue is commonly injured and the probable “pain generator”. Since neck injuries are the most common injuries cervical joints will be our focus. Related to anatomy, every set of two vertebrae in the neck is connected with three joints; two facet joints and a single disc. These joints allow for normal movement of the spine (mobility). There are multiple ligaments that are responsible for stability and hold together these joints. The correct balance of mobility and stability is critical when looking at the part of patient’s injuries, meaning that too little or too much movement in spinal joints can lead to pain, secondary to damaged tissue. The tissue most commonly hurt in a car crash is nerve, ligament, disc, facet and muscle/tendon. Spinal cord and bone injuries also happen although less frequently. To determine causality, the supplier should comment on what tissue is injured, and also use imaging to help determine if this injury occurred (age-dating).
There are two fundamental problems that must be addressed. Fardon and Milette (2001) reported, “The phrase ‘herniated disc’ does not infer knowledge of cause, relation to trauma or activity, concordance with symptoms, or need for treatment” (p. E108). Simply having a disc herniation’s presence, without a physical exam or without symptom documentation that is appropriate, does not allow one to comment on the cause of the injury. In a rear impact collision by way of example, even if the diagnosis is confirmed, additional criteria will need to be fulfilled to answer the question of “Was there sufficient force generated into the vehicle and the occupant to induce the cervical/lumbar herniation?” Fardon, in a follow-up study (2014) reported that disc injury “in the absence of significant imaging evidence of associated violent injury, should be classified as degeneration rather than trauma.” (p. 2531). Thus, we must more objectively define the subjective connotations of “violent injury” and address the issue of “degeneration as opposed to trauma”. Although this statement can frequently be misleading, it gives the trauma trained expert doctor a basis in going forward understanding that every patient’s physiology is unique and not subject to rhetoric, but clinical findings.
Violent injury to the occupant can occur when there are sudden acceleration and deceleration forces (g’s) generated to the neck and head which overwhelm connective tissue or pull them past their physiological limit. To determine the acceleration force, ?V (delta V) is utilized. ?V is the change in speed of the occupant vehicle when it is hit from behind (i.e., going from a stopped position to seven mph in 0.5 seconds because of forces moved from the “bullet” vehicle to the “target” vehicle). Utilizing these data, research allows us to make specific comments related to violent injury. Since the cervical spine is subjected to shearing forces, and compression, tension we are oversimplifying. Along with g-forces and the elastic nature of the majority of rear impact crashes makes it almost impossible to discover an actual minimum threshold for injury even though the literature has given us many examples of low-speed crashes which are dependent not simply on speed, but the mass (weight) of the subject vehicles. Each individual’s susceptibility to injury is unique. While g-forces alone are insufficient to predict injury, Krafft et al. (2002) reported that in low-speed collisions there’s an injury threshold of 4.2 g’s for males and 3.6 g’s for females. Krafft’s analysis is unique in that she has access to insurance data inaccessible to researchers. Panjabi (2004) revealed that forces as low as 3.5g impacts would lead to damage to the front of the disc, and 6.5g and 8g impacts would lead to disc damage posteriorly where the neurological components are.
Diagnosis for Disc and Ligament Injuries
A spinal biomechanical expert can look for evidence that is conclusive by disc and pathology, according to two phenomena. First, it is recognized that the body is electric. We’re measuring activity to diagnose when an EMG is done. Second, there are bioelectrical fields in all tissues. This typical field is disrupted when an injury occurs, and in the case of joints calcium is drawn to the damaged tissue. Issacson and Bloebaum (2010) reported “The particular loading pattern of bone has been documented as a significant piezoelectric parameter since potential gaps in bone have been known to be due to charge displacement during the deformation period” (p. 1271). For the patient, we have the ability to tell just how much of this process has occurred before or after their crash, especially if we take into consideration the tissue damage and signs of bone/calcium deposition.
In addition, the body begins a healing process that includes regeneration and remodeling of the soft and hard tissue as reported by Issacson and Bloebaum (2010). Spinal vertebrae have a unique structure of bone which allows it to adapt to abnormal mobility and stability (injury) by changing shape, which can be found on radiographs or MRI. Moreover, shape will change according to patterns based on the pressure or load it undergoes post-injury. Issacson and Bloebaum stated that “Physical forces exerted on a bone change bone structure and is a well-established principle…” (p. 1271). This is a further understanding of a scientific principle called Wolff’s law established in the 1800’s. Because we know what “normal” is, when we see “abnormal” findings as a result of mechanical stress we could broach the topic of an acute injury versus a degenerative process being the cause of the abnormality and create specific medical predictions accordingly.
He and Xinghua (2006) studied the predictability of the bone remodeling process and were able to make predictions of pathological changes that will occur in bone, specifically the osteophyte (bone spur) on the edge of a bone structure. Significantly, they noted their findings “confirmed that osteophyte formation was an adaptive process in response to this change of mechanical environment”. They noted that factors are crucial to the morphology of bones, particularly bones such as the femur and vertebrae.
For readers familiar with current academic and medical accepted nomenclature for disc injury, recognized from the combined task forces of the North American Spine Society (NASS), the American Society of Spine Radiology (ASSR) and the American Society of Neuroradiology (ASNR), disc herniations must have a directional component. When this occurs, the additional and abnormal pressure at the level of the disc damage matched with the direction of the herniation will cause that section of the vertebrae.
Thus, if there’s a C5/6 right sided herniation (protrusion/extrusion) secondary to a cervical acceleration/deceleration injury, then only that side of the vertebrae will change shape, creating an osteophyte. Facet arthritis is additionally caused by this compounded loading on the facet joint. This process is very similar to the formation of a callous on your hand or foot. The callous is a recognized and expected tissue response to increased load/friction exposure. Similarly, an osteophyte is a known and anticipated bone response to a rise in load/friction exposure.
At a basic level, the body has an electrical and mechanical response to injury leading to additional stress that leads to calcium (bone) to flow in the region of injury to further support the joint. The joint then abnormally grows, developing a called hypertrophy, degeneration, disc osteophyte complex, or arthritis/arthropathy, common terms seen in the reports of doctor and radiology.
Everybody is subject to these morphological (structural) changes, always and predictably determined by mechanical imbalances in the spine. He and Xinghua (2006) concluded that, “…it will actually take about over half a year to discover the bone morphological changes…” (p. 101). This indicates that it takes approximately six months to get an osteophyte (bone spur) to be demonstrable post-mechanical breakdown or failure. This again provides a time frame to better understand whether pathology of the intervertebral disc has been present for a long period of time (pre-existing) or has been produced as the direct result of the specific traumatic event by deficiency of the existence of an osteophyte, meaning the disc pathology is less than six months old, dependent on location and management of the pathology.
Conclusion
In conclusion, that by definition, a disc is a ligament connecting a bone to a bone and it has the structural responsibility to the vertebrae above and below to maintain the spinal system in equilibrium. Damage to the disc because of a tear (herniation or annular fissure) or a bulge will create abnormal load-bearing forces in the injury site. These present differently based on [1] if traumatic failure on the side of the disc lesion, or [2] if age related, as a general complex. Since other research and human subject crash testing have defined the term “violent trauma” as not being dependent upon the amount of damage done to the vehicle but rather to the forces to which the neck and head are exposed, we can now accurately predict in a demonstrable way the timing of causality of this disc lesion. This depends upon the symptomatology of the the morphology of the structure and is a subject that can be predicated upon speculation or rhetoric.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References:
Fardon, D. F., & Milette, P. C. (2001). Nomenclature and classification of lumbar disc pathology: Recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology.�Spine, 26(5), E93�E113.
Fardon, D. F., Williams, A. L., Dohring, E. J., Murtagh, F. R., Rothman, S. L. G., & Sze, G. K. (2014). Lumbar Disc Nomenclature: Version 2.0:�Recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology.�Spine,�14(11), 2525-2545.
Krafft, M., Kullgren, A., Malm, S., and Ydenius, A. (2002). Influence of crash severity on various whiplash injury symptoms: A study based on real life rear end crashes with recorded crash pulses.� In�Proc. 19th�Int. Techn. Conf. on ESV, Paper�No. 05-0363, 1-7
Batterman, S.D., Batterman, S.C. (2002). Delta-V, Spinal Trauma, and the Myth of the Minimal Damage Accident.�Journal of Whiplash & Related Disorders, 1:1, 41-64.
Panjabi, M.M. et al. (2004). Injury Mechanisms of the Cervical Intervertebral Disc During Simulated Whiplash.�Spine 29 (11): 1217-25.
Issacson, B. M., & Bloebaum, R. D. (2010). Bone electricity: What have we learned in the past 160 years?�Journal of Biomedical Research, 95A(4), 1270-1279.
Studin, M., Peyster R., Owens W., Sundby P. (2016) Age dating disc injury: Herniations and bulges, Causally Relating Traumatic Discs.
Frost, H. M. (1994). Wolff’s Law and bone’s structural adaptations to mechanical usage: an overview for clinicians.�The Angle Orthodontist, 64(3), 175-188.
He, G., & Xinghua, Z. (2006). The numerical simulation of osteophyte formation on the edge of the vertebral body using quantitative bone remodeling theory.�Joint Bone Spine 73(1), 95-101.
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
In the prior writing we explored the criteria for vehicle integrity. In this writing we’ll expand on conservation of momentum. You’re encouraged to do so when you haven’t read the previous article.
Expanding on Conservation of Momentum
Remember we previously said, “The momentum moving into a collision could be accounted for at the outcome” when we discussed the concept of conservation of momentum. Here we will introduce the formula and walk through its parts; we have to comprehend this in order to explore each other influence.
The full formula:
Let�s walk through this, on the left side of the equation we have which is the weight of the first vehicle before the collision multiplied by which is the velocity (in feet per second) of the first vehicle before the collision. is the weight of the second vehicle before the collision times which is the velocity (in feet per second) of the second vehicle before the collision. On the right side of the equation we have which is the weight of the first vehicle after the collision multiplied by which is the velocity (in feet per second) of the first vehicle after the collision. is the weight of the second vehicle after the collision times which is the velocity (in feet per second) of the second vehicle after the collision.
Ok, I know this looks very intricate and the explanation is not jumping off the page so let’s write with a bit more ease of comprehension. Let us take the National Highway Transportation Safety Administration (NHTSA) standards for testing and place two of the identical mass vehicles in this. Let us use a 2012 Toyota Corolla, and we will say the other is blue and one is red because we need two of them.
Red Corolla * 5 mph + Blue Corolla * 0 mph = Red Corolla * 0 mph + Blue Corolla * 5 mph
The 2012 Toyota Corolla has a curb weight of 2,734 pounds, substituted in the formula it looks like this:
Now when we do the math to show the conservation of momentum we end up with the following:
20,094.9 + 0 = 0 + 20,094.9
20,094.9 = 20,094.9
Momentum conserved
Now we have proved the concept so we are going to apply it to a collision involving two different vehicles. We will substitute the 2012 red Toyota Corolla for a 2012 red Chevrolet Tahoe. The 2012 Chevrolet Tahoe weighs 5,448 lbs. Now the formula looks like this:
Red Tahoe * 5 mph + Blue Corolla * 0 mph = Red Tahoe * 0 mph + Blue Corolla * 9.96 mph
Now when we do the math to show the conservation of momentum we end up with the following:
40,042.8 + 0 = 0 + 40,042.8[1]
40,042.8 = 40,042.8
Momentum conserved
Three significant points can be observed in this protest.
First, when testing is done notice the change in rate at the Tahoe is 5 mph (5 to 0). This is less than the rates used by the Insurance Institute and we would expect the Tahoe to have minimal damage and no structural deformation.
The second point to note is the change in speed the Corolla experiences, 9.96 mph (0 to 9.96). This change in speed is four times the original.
Conclusion
Finally, neither vehicle exceeds the speed of 10 mph, which the automobile manufactures and insurance institute for highway safety often consider threshold for injury. This confirms that cars can easily deform and residents become injured in low speed crashes once you begin to check out the conservation of energy (momentum) and coefficient of forces moved to the target car.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .� References
Edmunds.com. (2012). 2012 Chevrolet Tahoe Specifications. Retrieved from Edmunds.com: www.edmunds.com
Edmunds.com. (2012). 2012 Toyota Corolla Sedan Specifications. Retrieved from Edmunds.com: www.edmunds.com
Brault J., Wheeler J., Gunter S., Brault E., (1998) Clinical Response of Human Subjects to Rear End Automobile Collisions. Archives of Physical Medicine and Rehabilitation, 72-80.
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
You may be familiar with osteoporosis, the so-called “brittle bone” disease, but there is another condition – sarcopenia – that can lead to disability as we age, a top expert says.
“Sarcopenia is an age-related condition that can make walking and daily functioning difficult. It can also set the stage for bone fractures but, unlike osteoporosis, few people are aware of it,” Dr. Neerav Padilya, Ph.D., tells Newsmax Health.
Sarcopenia is defined as condition resulting in age-related loss of muscle mass, strength, and function, the National Institutes of Health (NIH) says.
The condition was first described in 1997, and experts – including the NIH – say it is an independent risk factor for physical disability, unrelated to age or other health problems.
Our bones get larger and stronger until the age of 30, when muscle mass begins to diminish, and sarcopenia can begin to set in, says Padilya, vice president of research at Qurr, a New Jersey based company which makes a supplement that targets the condition.
“We rely upon our muscle mass for our mobility, as well as to maintain balance, so if you start to lose it due to sarcopenia, by time you’re in your late 60s or 70s, this will have a direct impact on your life,” adds Padilya, a researcher and patent-holding inventor.
“The condition also causes a lack of hand grip strength, so if this becomes weak, imagine trying to open a jar of pickles,” he adds.
In addition, a loss of muscle mass may increase the risk of diabetes, he says.
Research studies note that increased muscle mass can help the body handle glucose, reducing the risk of the disease, Padilya notes.
But the biggest danger that sarcopenia poses, says Padilya, is that it predisposes people to falling, and suffering a potentially life-threatening fracture.
“About 50 percent of the people over the age of 65 that die have suffered a fracture, so it is a very serious problem,” he adds.
Since muscle mass begins to diminish in your 30s, it’s never too early – or too late – to take steps to prevent sarcopenia, says Padilya.
Here are his recommendations:
Make sure you are eating enough protein. Eat foods with protein uniformly at meals throughout the day, not only at dinner. Consume 60 grams of protein daily, or 20 grams at each meal.
Get up and move. Even a small amount of activity on a daily basis really helps you reduce body fat and maintain muscle.
Introduce weight lifting and resistance training into your exercise program.
Make sure you’re getting enough vitamin D. Take a multi-vitamin with vitamin D in it, and also make sure you are getting calcium from milk or eggs. Bone health and muscle health are closely connected.
UK research has revealed that many middle-aged office workers are as sedentary as elderly pensioners.
Carried out by the University of Edinburgh’s Physical Activity for Health Research Centre, the team gathered data on 14,367 people in Scotland taken from the 2012-14 Scottish Health Survey, to look at how age and sex affected weekday and weekend sedentary time.
Defined as time spent in any waking activity done while sitting or reclined, sedentary time includes working, eating, reading, watching TV, or spending time on a computer.
Many recent studies have looked at the effects of sedentary time on health, with some experts warning that more than seven hours of inactivity a day can increase the risk of cardiovascular disease, type 2 diabetes, some cancers, and an early death, even if people are physically active at other times of the day.
The results of the new research found that men aged 45 to 54 spend on average 7.8 hours per weekday sitting down, compared with 7.4 hours for the over-75s.
Time spent sitting at work is the main reason for their sedentary time.
The team also found that only the youngest group of men — 16 to 24-year-olds — are significantly less sedentary than the over-75s on weekdays.
Most of the time spent sedentary in this age group is spent in front of a TV or screen.
At the weekend, those aged 25 to 54 were the least sedentary, sitting for between 5.2 and 5.7 hours a day, and in contrast the over 75s were the most sedentary, at 7.3 to 7.4 hours a day.
In addition, the researchers also found that men spend less time in front of a screen as they get older, with women peaking in middle-age.
The results now replace previous findings that older adults are the most sedentary age group in the UK and highlights the potential health risks of excessive sitting at work.
“Large parts of the population are dangerously sedentary, something we have underestimated. We need to tackle high levels of sedentary time in early and middle age, when patterns may develop. Our findings suggest that changing habits in the workplace could be an appropriate place to start, given how much time we spend sitting there every day,” commented one of the study’s authors Tessa Strain.
The findings were published in the Journal of Sports Sciences.
UTEP softball head coach Tobin Echo-Hawk announced the addition of pitcher Kira McKechnie on Wednesday. McKechnie played her first two years at Fresno State and will have two years of eligibility with the Miners.
McKechnie will join fellow transfer pitcher Julia Wright, and UTEP sophomore hurlers Devyn Cretz and Allie Johnson for the 2018 season.
�We are excited to have Kira on our roster for the upcoming season,� Echo-Hawk said. �It is always nice to add some depth to your pitching staff.�
McKechnie, a native of Sacramento, Calif., made a relief appearance in the circle during the 2017 campaign against San Diego and recorded a strikeout. In 2016, McKechnie made a pair of appearances in the circle, throwing 1.1 innings, while allowing two hits and no runs.
McKechnie attended Christian Brothers High School and was a dual-sport athlete. She was a four-year letterwinner in both softball and basketball. McKechnie was voted softball team captain in 2015 and capped her senior year with multiple accolades, which includes Sacramento Bee�s 2015 All-Metro first team, Cal-Hi first team All-State, CAL All-Optimist All-Star team, MaxPreps first team All-State and Cal-Hi D3 Athlete of Honor.
She was named Female Athlete of the Year by Character Combine, Bee Preps Show and MaxPreps Christian Brothers, while earning the Credit Union Athlete of the Week in 2015.
During her senior season, McKechnie hit .462 with 40 RBI, 11 doubles, a triple and eight home runs. She added 18 runs and was walked nine times. In the circle, McKechnie (12-7) fashioned a 1.95 ERA and recorded 195 Ks 140 innings (23 starts/25 appearances).
McKechnie has competed for the California Breeze (2005-09), Capital City Comets (2009-12), Nor Cal Patriots (2012-14) and Central Cal Dirt Dogs (2014-15). She also attended the 2012 OnDeck Elite Futures Camp and 2013 Colorado Sparkler All-Star/All-American game.
There are many factors that play a role in the dynamics of collisions. These include vehicle design and type, speeds, angles of approach, kinetic & potential energy, momentum, acceleration factor, friction… the list is quite long. There are a few constants in which we are curious. These constants are the building blocks of the planet and they make the world of collisions quantifiable and predictable.
Within this two-part series we will explore the factors which have the most influence in low speed collisions and how these factors are associated with injury. Note: nothing about these writings is inclusive, there is too much material to explore in depth. The objective of these writings is to present the concepts.
Conservation of Momentum & Auto Accidents
In this writing the subject of exploration is conservation of momentum and how it relates to low speed collisions and bodily injury of the occupant. Conservation of momentum is built on Sir Isaac Newton’s third law. Newton’s third law says “For every action there’s an equal and opposite reaction”.
In the interest of exploring conservation of momentum in a simple format, we aren’t likely to investigate and explain the history and physics of momentum; for this conversation, we’ll concentrate on the relationship to crash dynamics. It is momentum to speed collisions’ relationship that helps enlighten and is the causal factor of the injuries people who have held tight to the argument that is deceptive that no damage = no injuries.
While there is a formula and derivation, neither is needed just yet. For now, we’ll simply use the concept as follows: The momentum going into a collision can be accounted for in the outcome or the energy going in to the accident, must be accounted for at the end of the incident and that and what was exposed to and/or absorbed that energy.
Let’s apply some perspective to this notion with the following example.
Let us say we are standing at around a pool table and we are going to try the winning shot of the eight ball into a corner pocket. Following the cue ball is struck, we have and another. After the cue ball strikes the ball, then it stops moving and the eight ball begins moving. In this scenario the cue ball before the collision’s momentum is the same as the momentum of the eight ball after the collision[1]. The eight ball rolls to the corner pocket.
The transfer is extremely efficient due in part to the fact that neither pool balls can deform. Some of the energy would be used to perform this and less if either pool ball could deform. The National Highway Transportation Highway Safety Administration (NHTSA) mandates minimum performance standards for passenger vehicle bumpers. Vehicle bumpers are tested with 2.5 mph (3.7 fps)[2] impact equipment that has the same mass as the test vehicle. The test vehicle is struck with its brakes disengaged and the transmission in neutral. There’s no offset between the automobile and the barrier.
Performance Standards for Vehicle Safety
The NHTSA outlines acceptable damage to your vehicle’s various systems after the tests. Successful completion of these tests mandate operation of systems that are particular. The factory adjustment of the vehicle’s braking, steering, and suspension must be unaltered. In other terms, in order for a vehicle to pass these tests it canhave no change in its structure. If changes did occur the system that is braking, steering, and suspension would be out of factory adjustment.
The NHTSA isn’t alone in low rate bumper testing. The Insurance Institute for Highway Safety (IIHS) also conducts low rate bumper tests. The IIHS’s test rates are conducted at 6 mph (8.8 fps)[3] and the goal is to determine which vehicles have the least damage and therefore cost the least to repair. The vehicle ratings are proportional to the estimated cost of repair. The more costly the repair, the lower the rating.
While the vehicles used in the IIHS testing all show signs of contact with the barrier, none of the vehicles suffer harm which deforms the structure of the vehicle. Don’t have any change in its structure affecting the system, steering, and suspension, just as with the NHTSA the vehicles tested by the IIHS.
The lack of change in the structure (deformation) drives a test vehicle to accept the momentum transfer in the testing equipment. Further, the test vehicle is free to move after being destroyed. This testing scenario is like that of the cue ball and eight ball.
If a vehicle doesn’t deform during a low speed collision, then it will experience a change in speed (or velocity) very quickly; Consequently, the occupant(s) also experience this exact same change in speed. The key factor in these examples is that the mass of testing equipment and their vehicles involved, but what happens when the masses change?
Conclusion
When the mass of one vehicle changes the momentum also changes, the more mass the more momentum the vehicle can bring to the event and the greater the injury potential to the occupant. There are many complicating factors that now must be considered regarding injuries beyond the Laws of Momentum when determining trauma like the height, weight, muscle mass, occupant position, kind of seat belt used, etc.. However, the first step is to decide if there was enough energy as an initiating factor in low speed crashes to cause those injuries and to overcome no crash = no injury misconceptions and have a health expert in low speed injuries confirm relationship.
In the next installment, part II, we’ll discuss this in detail and it will necessary for the later subject of occupant injuries.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
REFERENCES:
Insurance Institute for Highway Safety. (2010, September). Bumper Test Protocol. Retrieved from Insurance Institute for Highway Safety: www.iihs.org
National Highway Transportation Safety Administration. (2011, October 1). 49 CFR 581 – BUMPER STANDARD. Retrieved from U.S. Government Publishing Office: www.gpo.gov
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
In the first part of this 2-part series, chiropractor, Dr. Alexander Jimenez looked at the likely signs and symptoms of disc Herniation, in addition to the selection standards for micro-discectomy surgery in athletes. In this report he discusses the lengthy rehab period following a micro-discectomy procedure, and provides a plethora of strength based exercises.
Surgeries to ease disc herniation, with or without nerve root compromise, comprise traditional open discectomy, micro-discectomy, percutaneous laser discectomy, percutaneous discectomy and micro- endoscopic discectomy (MED). Other surgical conditions are employed in The literature like herniotomy that’s interchangeable with fragmentectomy or sequestrectomy. The saying ‘herniotomy’ is defined as removal of the herniated disc fragment just, and the ‘standard discectomy’ as elimination of the herniated disc along with its degenerative nucleus in the intervertebral disc space.
When surgery is required, minimizing tissue disruption and strict adherence to an aggressive rehabilitation regimen may expedite an athlete’s return to perform(1), that explains why micro discectomy is a favored surgical procedure for athletes. Micro discectomy procedures entails Removing a small part of the vertebral bone over a nerve, or removing the fragmented disc stuff from under the compressed nerve root.
The surgeon can then enter the spine by removing the ligamentum flavum that insures the nerve roots. The nerve roots can be visualized with functioning eyeglasses or with an operating microscope. The surgeon will then move the nerve to your side and to subsequently remove the disc material from beneath the nerve root.
It’s also sometimes required to eliminate A small portion of the related facet joint to permit access into the nerve root, and additionally to relieve pressure on the nerve root resulting in the facet joint. This procedure is minimally invasive since the joints, muscles and ligaments are left intact, and the process doesn’t interfere with the mechanical construction of the spinal column.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques.�From the El Paso, TX. Spine Center.
Surgical Outcomes
In general, athletes with lumbar disc Herniation have a favorable prognosis with traditional therapy; more than 90 percent of athletes using a disc herniation improve with non-operative treatment. Many demonstrate a response to conservative treatment with increased pain and sciatica within 6 weeks of the initial onset(2). This implies that the requirement to function immediately could be considered hasty.
However, in case of failed Conservative therapy, or together with the pressure of a significant upcoming competition, surgery might be needed in some instances. Even though it involves surgical therapy, micro-discectomy has been reported to have a high success rate — over 90 percent in some studies(3,4). Patients generally have hardly any pain, are able to return to preinjury activity levels, and therefore are subjectively happy with their results.
The achievement rate of micro-discectomy is The following studies have been summarised to underline the success rate of micro-discectomy procedures:
1. In a survey on 342 professional athletes Diagnosed with lumbar disc herniation in sports like hockey, football, basketball and baseball, it was discovered that powerful return to perform occurred 82% of this time, and 81 percent of surgically treated athletes returned for an additional average of 3.3 years(5).
2. From a limb paresis which might be associated with a disc herniation following surgical treatment. If the preoperative paresis was mild then they could anticipate an 84% likelihood of full recovery. Patients with more severe paresis have less chance of recovery (55%)(6).
3. Wang et al (1999) in a study on 14 athletes demanding discectomy processes found that in single degree disc procedures, the return to game was 90%. However when the procedure involved 2 levels enjoyed considerably less favorable results(7).
4. In a study of 137 National Football League players with lumbar disc herniation, surgical treatment of lumbar disc herniation led to a significantly more career and greater return to play rate than those treated non-operatively(8).
5. Schroeder et al (2013) reported 85% RTP rates in 87 hockey players, with no substantial difference in outcomes or rates between the surgical and nonsurgical cohorts(9).
6. A study by Watkins et al (2003) coping with professional and Olympic athletes revealed the acceptable outcomes of micro-discectomy concerning return to play, since elite athletes in general were highly encouraged to return to perform(10). Also, athletes who had single-level micro- discectomy were more likely to come back to their original heights of sports activities than were people who’d two-level micro- discectomies.
7. A study by Anakwenze et al (2010) investigating open discectomy at National Basketball Association participants demonstrated that 75% of patients returned to perform again compared with 88 percent in control subjects who did not undergo the operation(11).
8. A recent review found that conservative therapy, or micro-discectomy, in athletes using lumbar disc herniation seemed to be satisfactory concerning returning the injured athletes into their initial levels of sports activities(12).
These studies conclude that though a Analysis of lumbar disc herniation has career-ending potential, most gamers have the ability to return to play and generate excellent performance-based outcomes, even if surgery is required.
What is also apparent from research Studies is the level of this disc herniation can also determine prognosis after surgery. Athletes shower a greater difference in progress between surgical and non-operative treatment for upper amount herniations (L2-L3 and L3-L4) compared to herniations at the L4-L5 and L5-S1 levels. Patients using the upper level herniations needed less progress with non-operative treatment and marginally better operative outcomes than those with lower degree herniations(13).
There are several possible explanations A range of studies have revealed that low spinal canal cross-sectional area is associated with an increased likelihood of symptomatic disc herniation, and increased intensity of herniation symptoms. The spinal cross-sectional region is the smallest (thus contains a larger possibility of nerve compromise) at the most upper posterior section and the cross-sectional region increases further down to the lower lumbar spine(14).
The location of the disc herniation�(foraminal, posterolateral or central) may also contribute to differences.�In this study, upper lumbar herniations were more likely to happen in the much lateral and foraminal positions than were people in the lower two intervertebral degrees(13).
Post-Surgical Rehab
After micro-discectomy surgery, the Small incision and restricted soft tissue injury makes it possible for the patient to be ambulatory reasonably fast, and they’re usually encouraged to start rehabilitation sooner or later during the 2-6 weeks after surgery.
In a review on the efficacy of busy Rehabilitation in patients following lumbar spine discectomy, it may be reasoned that individuals can safely take part in high or low-intensity supervised or home-based exercises initiated at 4 to 6 weeks following first-time lumbar discectomy(15).
Herbert et al (2010) discovered that with Effective post-surgical rehabilitation plans, there was a key accent on lumbar stabilisation exercises(16). Second, positive trials tended to initiate rehabilitation earlier in the postoperative interval compared to negative trials (about 4 vs 7 weeks).
Outcome Measures
The most widely used result Measure following back injury and/or disc surgery is the Oswestry Disability Questionnaire(17). This questionnaire is reported to have good levels of test-retest reliability, responsiveness, and also a minimum clinically important difference estimated as 6 percent(18) Furthermore, treatment success has been defined as a 50 percent decrease in the Modified Oswestry Disability Questionnaire score(19).
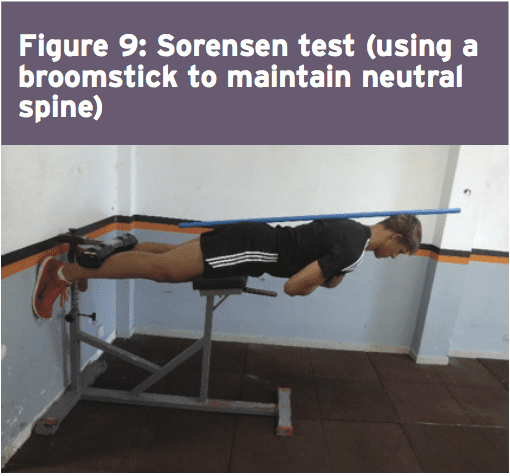
Concerning physical performance measures following back disc or pain operation, a commonly used clinical examination is that the Beiring-Sorensen Back Extension examination (see Figure 1)(20). This test is performed in a prone/horizontal body position with the spine and lower extremity joints at neutral position, arms crossed at the chest, lower extremities and pelvis supported with the top back unsupported against gravity.
Rehabilitation Program
Presented below is a five-stage rehabilitation program. The stages involved in rehabilitation are:
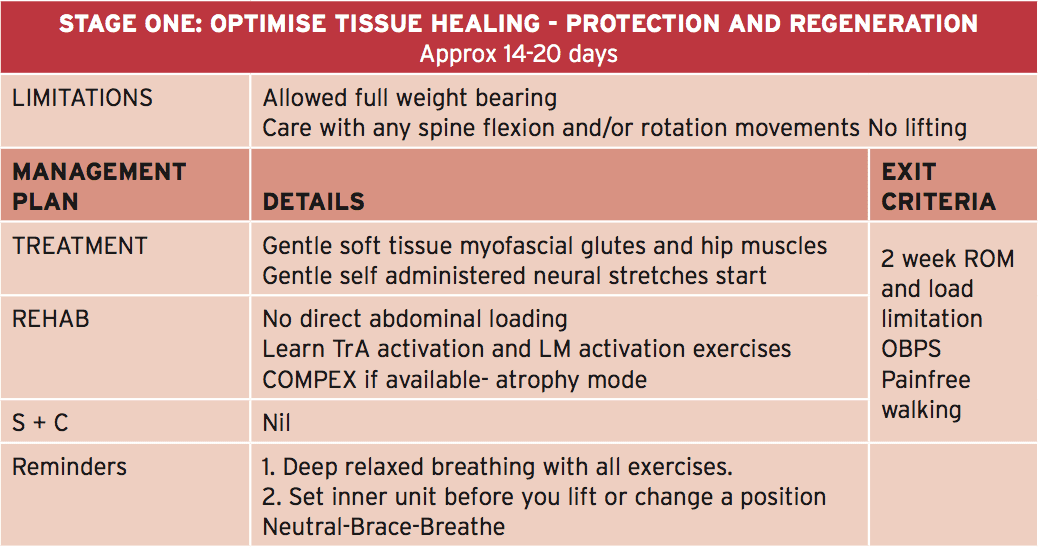
1. Optimize tissue healing — protection and regeneration
2. Early loading and foundation
3. Progressive loading
4. Load buildup
5. Maximum load
This program has been designed to get a field hockey player with had a L5/S1 lumbar spine discectomy. Even though the progressions from one point to the next are driven by the exit standards related to that stage, it might be anticipated that the athlete could progress in post-surgery to ‘fit to compete’ in about 12-13 weeks.
In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.
The athlete can begin with the physiotherapist with the objective to manage any gluteal and lumbar muscle trigger points and start�nerve mobilization techniques that show how to engage the TrA and LM muscles (see Figures 2a and 2b).�If the physiotherapist has access to your muscle stimulator (Compex), then this can be utilized in atrophy manner on the lumbar spine multifidus and erector spinae. The key criteria to exit this early phase are curable walking as well as also an Oswestry Disability Score of 41-60%.
Early Loading & Foundation
The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.
The athlete can also be encouraged to start hydrotherapy in the form of walking in water (waist high) along with swimming fitnesscenter. In addition, he/she must start a string of low degree muscle activation drills in this stage (see Figure 3) that can be performed every day. This exercise teaches the athlete to hip flex (fashionable hinge) whilst maintaining a neutral spine. The neutral spine is maintained by using a light broomstick aligned with the back with the touch points being the occiput, the 6th thoracic vertebrae (T6) and the posterior sacrum.
Progressive Loading
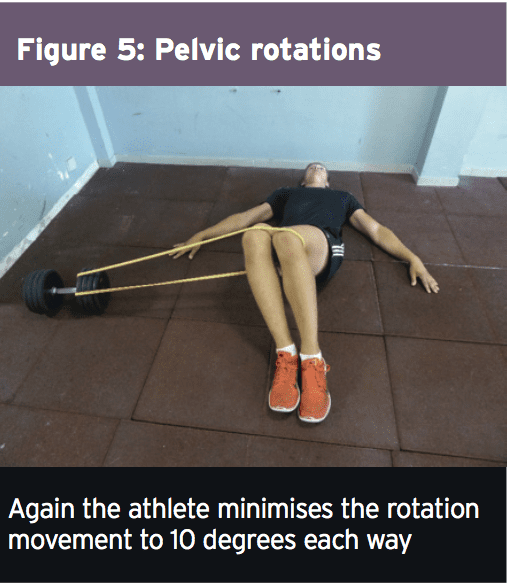
In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�Two exercises here are the �standing twisties� and the �crook lying pelvic rotation� exercise (Figures 4 and 5).�These movements are the introductory spinning based movements. The primary progression about fitness drills is the athlete can begin pool running drills.
Load Accumulation
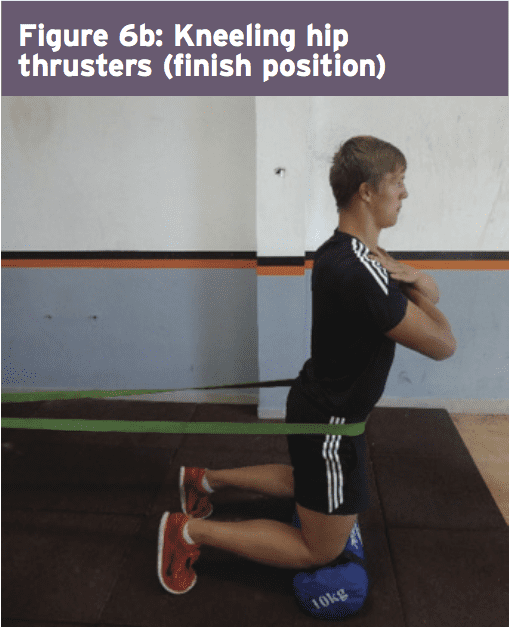
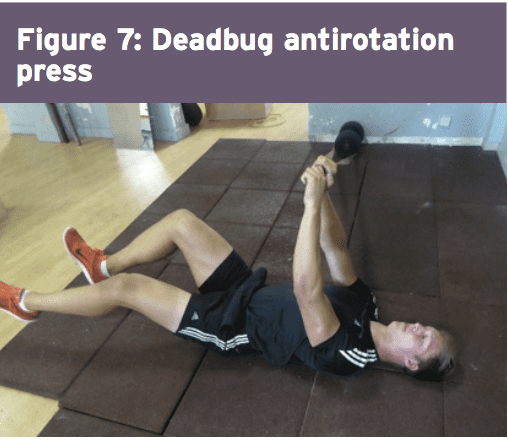
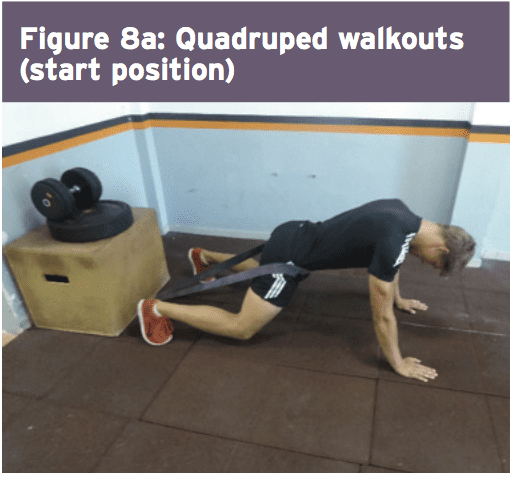
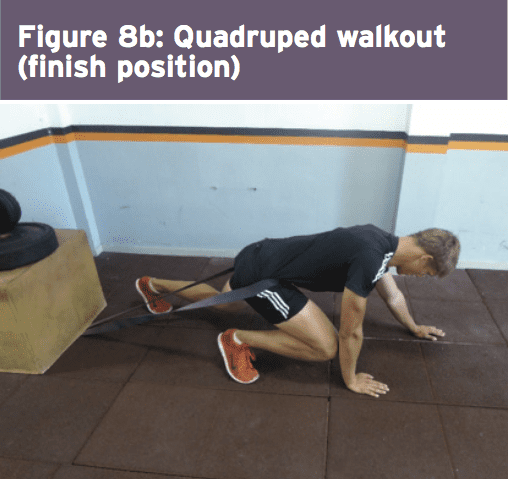
This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).
The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.
Maximum Load
In this final stage, the athlete spreads all core and strength exercises to maximum loads, and they work with the fitness trainer on coming to squat and functional fitness center lift movements. Skill progression can also be advanced alongside sprint and agility drills. The last exit standards prior to advancing to endless strength and training work is they have to keep the ‘Sorensen test’ for 180 seconds and their self documented Oswestry scale ought to be someplace between 0-20%.
Concussion, also known as mild traumatic brain injury (MTBI), has been a poorly understood condition known to the majority of healthcare providers as difficult to objectify and manage.
Historically, there has been no testing available to conclude an accurate diagnosis. In the absence of objective imaging findings of bleeding in the brain, a diagnosis of “mild traumatic brain injury” has been affixed to the condition, whereas if there’s evidence of traumatic bleeding then the diagnosis “traumatic brain injury” is applied.
Although Hartvigsen, Boyle, Cassidy and Carroll (2014) reported that 600 out of 100,000 Americans are affected every year by concussion, Jeter et al, (2012) reported that close to 40 percent of people experiencing a mild brain injury do not report it to their doctor, making accurate statistics very tricky to conclude. Despite potential under reporting in the people, we realize concussion is an issue that has consequences that are important from the perspective of a clinical result and we cannot afford to ignore this condition.
Mechanism of Injury: Mild Traumatic Brain Injury
Mild traumatic brain injury or concussion results from transfer of mechanical energy from the outside environment to the brain due to traumatic events where there’s a sudden acceleration and then a sudden deceleration of the mind and brain, such as in a Coup/Contrecoup injury during a whiplash scenario. As the brain is freely moving to a degree because it’s only surrounded by cerebral spinal fluid, it continues moving in the original direction and as the head “whips” rapidly in the opposite direction, the brain bounces off parts of the inner skull, which in turn rebounds shortly after the head changes direction. This is one easily defined mechanism of MTBI that doesn’t cause gross bleeding, yet leaves the brain injured through direct compression or overstretching (axonal shearing) of central nervous system components.
Although this has been examined extensively in the military, it’s been recently investigated in professional sports, where after several lawsuits and lives at risk, there are now definitive “concussion protocols” in place. Part of the protocols as reported from the British Journal of Sports Medicine (2016) is the Sports Concussion Assessment Tool 2 or SCAT2 that’s been adopted by numerous professional sports leagues. However, the majority of concussion victims are not active participants in the military or a professional sports team and many find their way into chiropractic practices as a consequence of sports injuries, car accidents, slip and falls and every other sort of head trauma etiology. Even though the mechanisms might vary, the induced end results are the same.
For generalized patient intake protocols, according to both Medicare and academia standards, a questionnaire outlining a summary of body systems is mandated, and part of those questions center on brain function. As reported by Jeter et al behavioral and cognitive symptoms, signs and symptoms are reported on standard patient intake questionnaires and require consideration of a diagnosis of concussion.
Prominent symptoms of concussion include: balance issues, vomiting, nausea, headache, drowsiness, dizziness, fatigue, vision, light or noise sensitivity and sleep disturbances. Cognitive symptoms include deficits in attention, concentration, memory, mental processing speed, and working memory or decision making. Behavioral symptoms include anxiety, depression, irritability, depression and aggression. The researchers went on to report that approximately 25 percent of the cases can have these symptoms persist.
Diagnosis and Treatment for MTBI
As a profession, chiropractic is a important part of the rehabilitation for the concussion population as the post-traumatic patient typically presents to the average chiropractic practice. As chiropractors (along with all healthcare providers), even if you mix the history with the above symptoms inclusive of neurological, behavioral and cognitive traits, you then have the direction or “triage road map” of the way to conclusively differentially diagnose your individual, including what tests to consider conducting in order to do so. The first line of testing is to consider imaging to rule out bleeding and ensure the patient does not require an immediate consultation. Treating blindly can place your patient in risk that is possible.
Imaging of the brain requires either MRI or CAT scans, MRI being the more sensitive, and in the absence of bleeding, the diagnosis is limited to MTBI or concussion (used interchangeably). More recently, diffusion tensor imaging (DTI) has been a tool available to picture mTBI victims that uses tissue water diffusion speeds to determine bleeding at a very small level giving demonstrable evidence to brain injury. As reported by Soares, Marques, Alves, and Sousa, (2013), DTI has several issues to overcome to certify accuracy including, but not limited to, tissue type, integrity, barriers and quantitative diffusion rates that are required to infer molecular diffusion prices. DTI is a model based upon assumption with a outlook as a tool.
Historically, MTBI was exclusively diagnosed by an omission of advanced imaging findings and the presence and persistence of the neurology, cognitive and behavioral signs and symptoms. Today, brain-derived neurotrophic factors (BDNF) offer responses about carpal brain pathology that is both conclusive and reproducible. Based on Korley et al. (2015), brain-derived neurotrophic factors is a secreted autocrine (compound hormone or messenger in blood) which promotes the development, maintenance, survival, differentiation and regeneration of neurons. BDNF also is important for synaptic plasticity (strengthening of synapses over time) and memory processing. Germane to MTBI and concussion, BDNF has been implicated in decreasing brain injury, with elevations and restoring traumatic brain injury.
Korley went on to report that BDNF levels were the highest in the normal group with lower values in mTBI and even lower in traumatic brain injury (TBI) subjects. In addition BDNF values were associated with incomplete recovery of patients that were MTBI compared to moderate or severe TBI patients. Because of this, it has been ascertained that BDNF has for identifying associated sequelae at 6 23, a prognostic value.
Korley stated that BDNF is the most abundantly secreted brain neurotrophin and as a secreted protein and can be readily measured using well-established immune-assay methods, identifying it as a non-necrosis brain injury biomarker. This distinguishes BDNF from other biomarkers which are components of neurons and myelin based proteins among other structures. In order for structural fibers to be found in high abundance in circulation, adequate cellular necrosis and damage to the blood barrier membrane must be observed, however BDNF does not require cellular damage or necrosis to be observed in circulation enabling DDNF to be more plentiful in flow than structural proteins.
Following a traumatic brain event, BDNF supports synaptic reorganization and recovery during the brain circuitry “reconnection” phase. Therefore, a better prognosis is indicated by lowered values. In patients with a co-morbidity of BDNF of anxiety, depressive disorders and schizophrenia BDNF values on the day of injury predispose this population to incomplete recovery as a risk element. Korley et al.. Concluded that serum BDNF discriminates between MTBI and TBI cases. Also, diminished BDNF values are associated with recovery in identifying and useful symptoms 6-months post-trauma.
Conclusion
Simply put, a blood test could assist providers in concluding the existence and/or severity of traumatic brain injury or mild traumatic brain injury. An early diagnosis is afforded by the results so you can devise a treatment plan inclusive of changing activities of everyday living to prevent additional damage and optimize the repair procedure with minimizing further chemical, physical or emotional stressors.
Based upon interviews with leading neurologists and neurosurgeons who understand and have first-hand expertise of both receiving chiropractic care and handling and treating MTBI patients, it is strongly recommended that until the signs and symptoms of the neurologic, cognitive and behavioral abate that high-velocity rotational cervical adjustments be avoided to enable the brain to “repair and rewire” the connections without additional possibilities of and Coup/ Contrecoup energy to the mind. This is a recommendation which we agree while recognizing that chiropractic care should not be avoided adapted to allow the brain to heal.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References:
1. Hartvigsen, J., Boyle, E., Cassidy, J. D., & Carroll, L. J. (2014). Mild traumatic brain injury after motor vehicle collision: What are the symptoms and who treats them? A population-based 1-year inception cohort study. Archives of Physical Medicine and Rehabilitation, 95(Suppl. 3), S286-S294.
2. Jeter, C. B., Hergenroeder, G. W., Hylin, M. J., Redell, J. B., Moore, A. N., & Dash, P. K. (2013). Biomarkers for the diagnosis and prognosis of mild traumatic brain injury/concussion. Journal of Neurotrauma, 30(8), 657-670.
3. British Journal of Sports Medicine. (2016). Sport concussion assessment tool 2. Retrieved from http://bjsm.bmj.com/content/43/Suppl_1/i85.full.pdf
4. Soares, J. M., Marques, P., Alves, V., & Sousa, N. (2013). A hitchhiker�s guide to diffusion tensor imaging. Frontiers in Neuroscience, 7(31), 1-14.
5. Korley, F. K., Diaz-Arrastia, R., Wu, A. H. B., Yue, J. K., Manley, G. T., Sair, H. I., Van Eyk, J., Everett, A. D., Okonkwo, D. O., Valadka, A. B., Gordon, W. A., Maas, A. I., Mukherjee, P., Yuh, E. L., Lingsma, H. F., Puccio, A. M., & Schnyer, D. M., (2015). Circulating brain-derived neurotrophic factor has diagnostic and prognostic value in traumatic brain injury. Journal of Neurotrauma, 32, 1-11.
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
Obesity is not only an epidemic for the human race. One third of dogs and cats also suffer from it, according to a new American study. A lack of exercise, overfeeding and genetics are all contributory factors.
According to this American study published recently by Banfield Pet Hospital, the number of overweight and obese cats rose by 169% in the US over the past 10 years. For dogs, the increase was 158%. And the numbers are still trending upwards.
The survey analyzed data gathered on 2,521,832 dogs and 505,389 cats based on visits and checks made at veterinary clinics across the country. Almost 30% of the dogs and 33% of the cats seen during these visits were overweight or obese.
The main causes are a lack of exercise and too much food. A genetic predisposition can also be a factor, as some breeds of dogs and cats are more likely to become obese. Pets that have been sterilized also have an increased risk of gaining weight, as hormonal changes can boost their appetite and make them less inclined to play and take a walk.
Obesity has consequences for animal health. It raises the risk of type 2 diabetes, arthritis and heart disease.
Banfield Pet Hospital says that up to the age of 4 months, a kitten should be fed 4 times a day, and then 3 times daily when it is aged between 4 and 6 months. After that, feeding should be no more than twice a day. For dogs, it varies according to the animal’s size, age, physical condition and how active it is.
The study warns against the common attitude of giving treats to a dog or filling its bowl out of love or guilt for leaving it home alone. Portion size is also a problem, as it is often too generous.
Banfield Pet Hospital advises that the ideal weight for a dog or cat is when you can feel the animal’s ribs without being able to see them. If the animal is 10% above its correct weight, its ribs are no longer visible and cannot be felt, and if it is 20% above, no waist can be seen. Anywhere above the 20% mark is considered to be obese.
Only sport and a diet should be used to lower a pet’s weight.
Obesity also affects other types of pets. A British study in 2014 undertaken by the Pet Food Manufacturing Association revealed that 28% of pet rodents were obese and 15% of indoor birds.
And awareness can be an issue. In France, a 2010 survey by BVA/Gamm Vert revealed that only 13% of pet owners thought that their dog had a weight problem.
Emmanuel Korir, Michael Saruni and Mickael Hanany qualified to the IAAF (International Association of Athletics Federation) World Championships over the weekend.
Running in Nairobi, Kenya, Korir qualified to the 800m final with a time of 1:45.50 in the first heat, Saruni followed with a time of 1:46.10 in the second. In the men�s final, Korir (1:43.86) notched the crown and Saruni took third with a personal best of 1:44.61.
The All-Americans garnered a spot on the Kenya national team which heads to London, England to compete at the World Championships on August 5-8.
Also making his way to London will be former UTEP track and field star Mickael Hanany (France). Hanany took gold at the 2017 Euro Superleague with a leap over 2.26m (7-5) in the high jump. The seven time All-American will compete in his fourth IAAF World Championship.
The Nigerian trails will take place on July 7-8.
For more information on UTEP track and field, follow the Miners on Twitter (@UTEPTrack) and on Instagram (uteptrack).
Check Also
New UTEP Tennis Head Coach Ivan Fernandez announced his first two signees on Friday. Erandi �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine







 In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.
In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.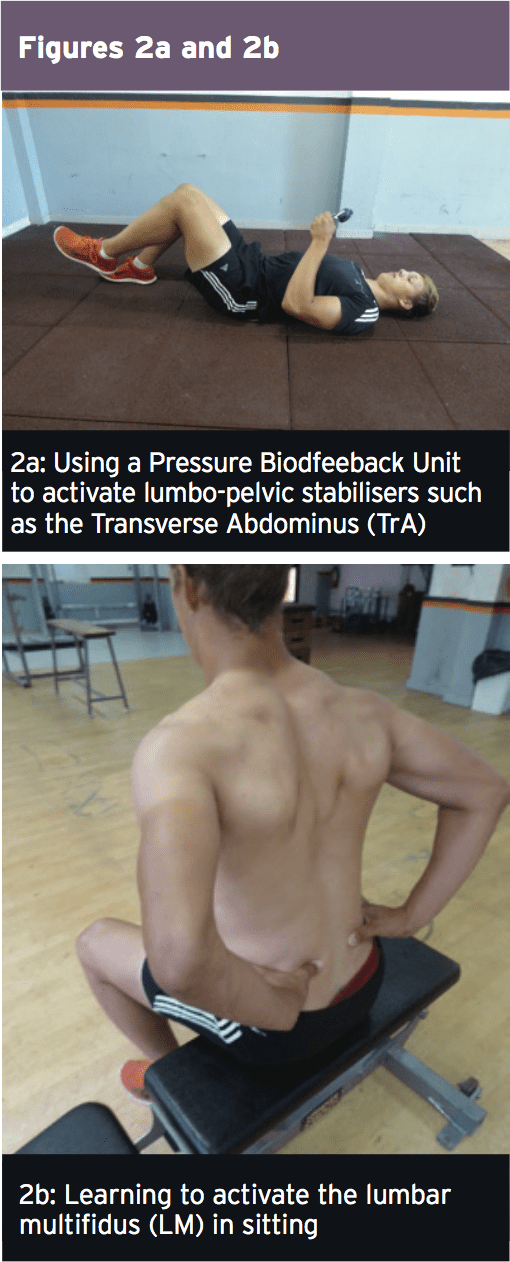 Early Loading & Foundation
Early Loading & Foundation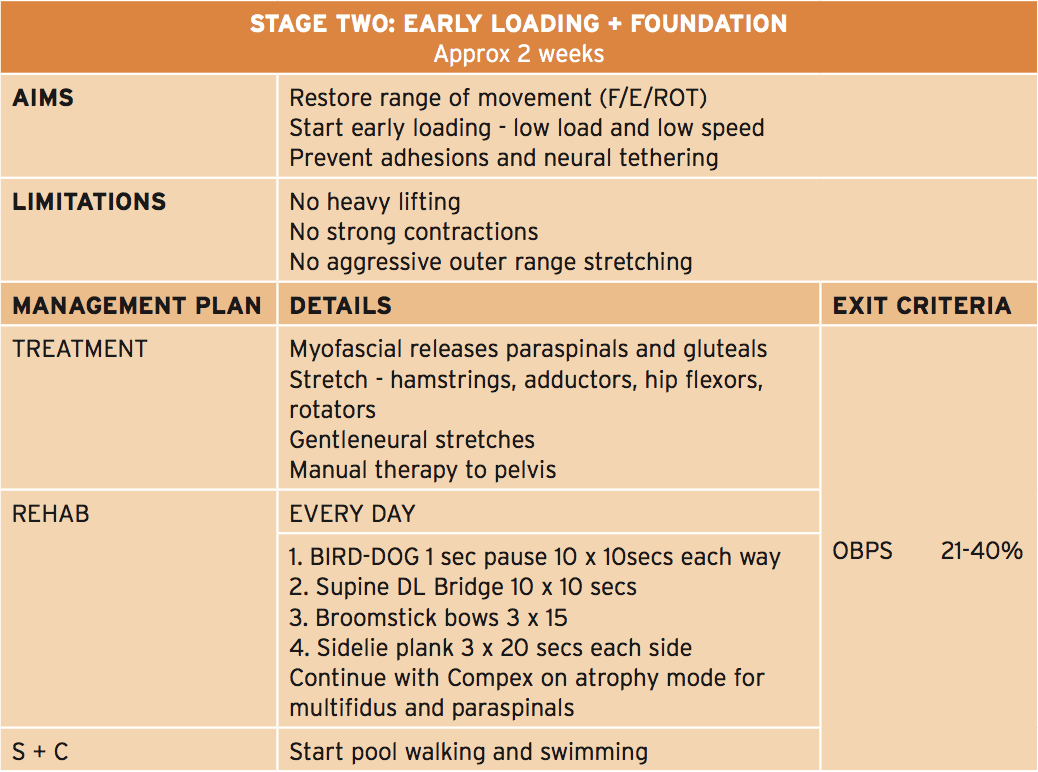 The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.
The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.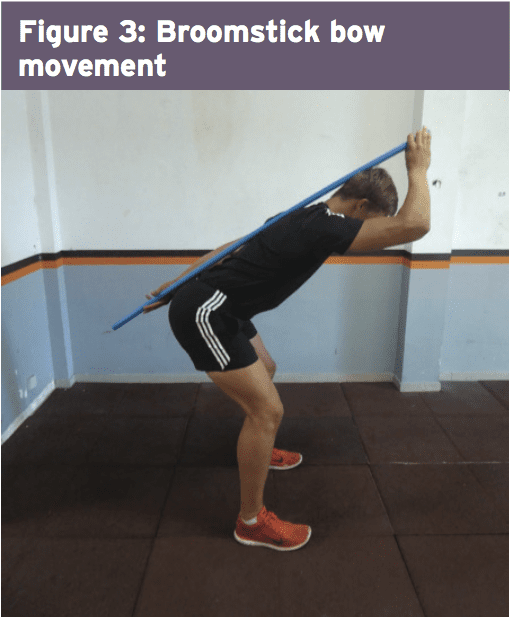 Progressive Loading
Progressive Loading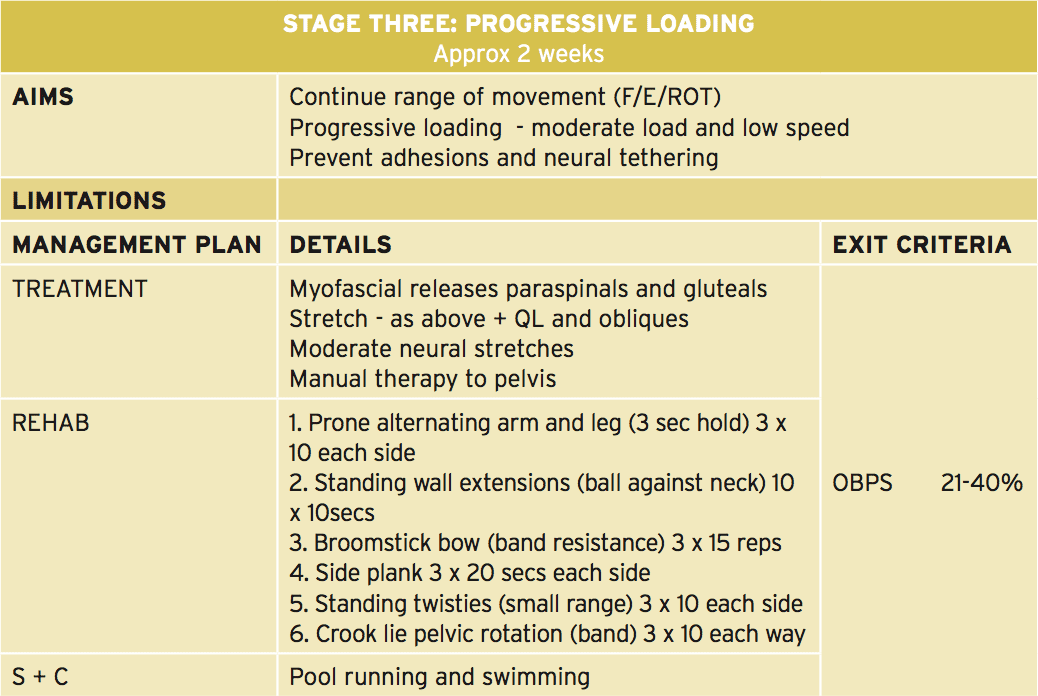 In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�
In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�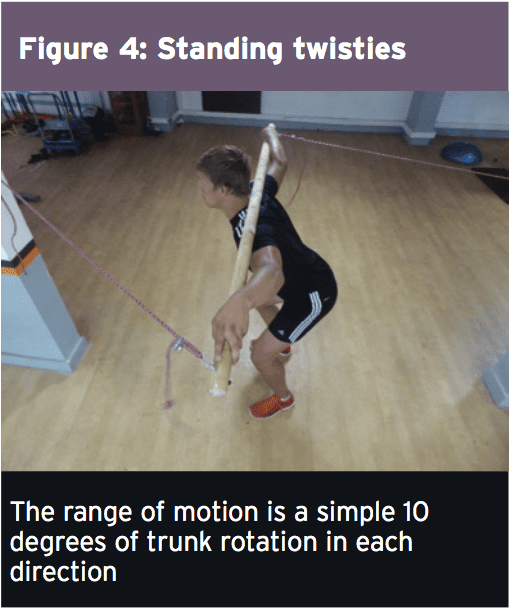
 Load Accumulation
Load Accumulation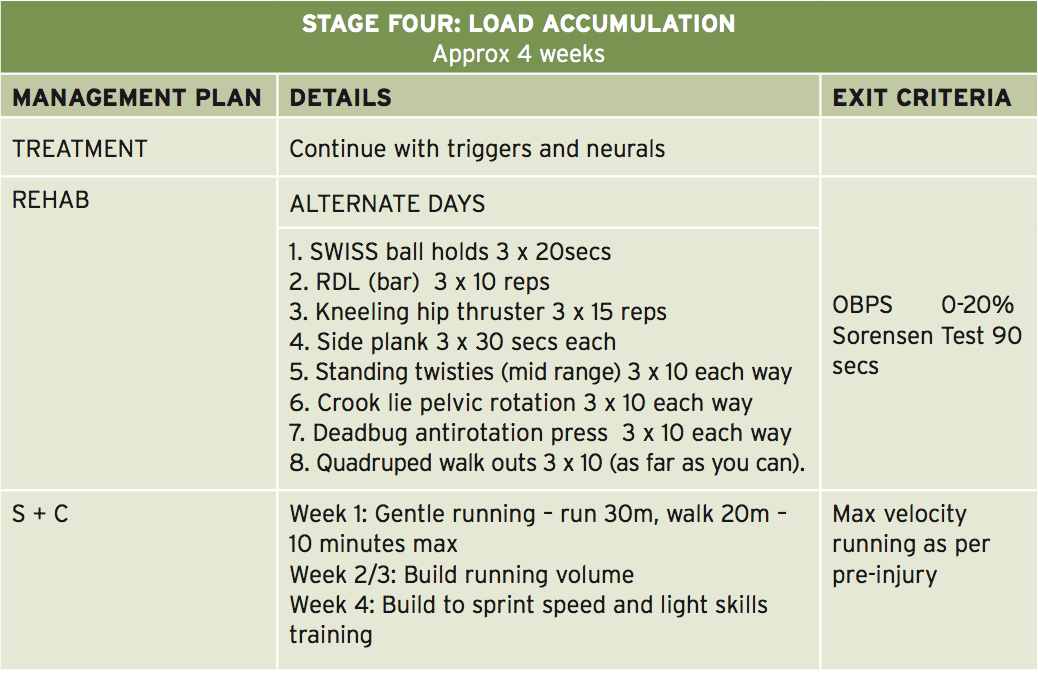 This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).
This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).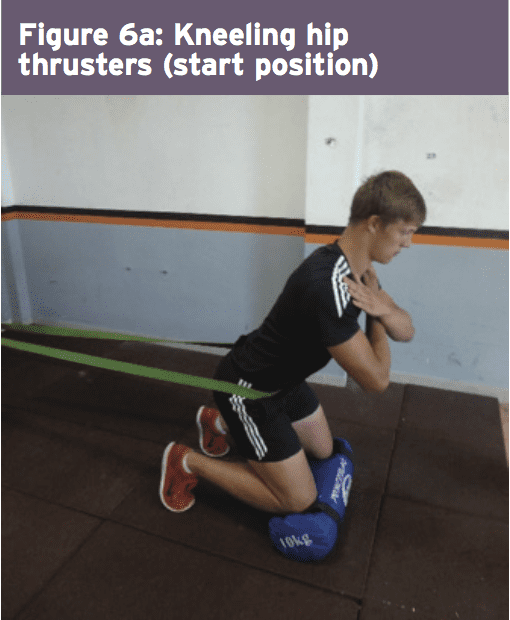
 The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.
The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.