Emmanuel Korir, Michael Saruni and Mickael Hanany qualified to the IAAF (International Association of Athletics Federation) World Championships over the weekend.
Running in Nairobi, Kenya, Korir qualified to the 800m final with a time of 1:45.50 in the first heat, Saruni followed with a time of 1:46.10 in the second. In the men�s final, Korir (1:43.86) notched the crown and Saruni took third with a personal best of 1:44.61.
The All-Americans garnered a spot on the Kenya national team which heads to London, England to compete at the World Championships on August 5-8.
Also making his way to London will be former UTEP track and field star Mickael Hanany (France). Hanany took gold at the 2017 Euro Superleague with a leap over 2.26m (7-5) in the high jump. The seven time All-American will compete in his fourth IAAF World Championship.
The Nigerian trails will take place on July 7-8.
For more information on UTEP track and field, follow the Miners on Twitter (@UTEPTrack) and on Instagram (uteptrack).
Check Also
New UTEP Tennis Head Coach Ivan Fernandez announced his first two signees on Friday. Erandi �
Not only do tires play a vital role in the performance of your car or truck, but a lot of information can be garnered about what happened before, during, and after a crash. Tire marks will be explored by us and, generally, what those marks tell us.
First let us discuss where the marks come from. Skid marks are created by the extreme thermal relationship of a tire against the roadway surface during extreme stresses put on the tire, a simpler way to say this is, a tire will “mark” when it nears, or exceeds, the limits of its relationship with the roadway. These marks occur because the oils in the roadway and/or the tire(s) are brought to the surface and “melted or burnt” into the roadway. If a tire is heated enough since the surface of the tire will have changed, it’ll be obvious, it is going to have a spot and obvious abrasions.
Kinds of Skid Marks.
There are three specific kinds of marks we will talk about, these are the most typical four wheeled car and light duty truck marks. (Other vehicles, such as motorcycles, have different specific marks).
Light to Dark or Dark to Light
All marks can be placed into two categories when referencing the management of the vehicle which made them. Light to dark marks (in the direction the vehicle was traveling) support a vehicle making the marks through some kind of deceleration (extra points if you wanted to read “negative acceleration”). Dark to light marks (again, in the direction the vehicle was traveling) support a vehicle making the marks through some form of acceleration, usually excessive wheel spin.
Darker from the Middle, Darker on the Outsides, or Uniform
Marks that are darker in the center indicate a tire that’s overinflated, conversely marks that are darker on the outside edges indicate a tire which is underinflated. Indicate a tire.
ABS Versus Regular Marks
ABS (Anti-lock Brake System) marks are lighter than conventional marks and have more tire tread definition in them, Non-ABS marks rarely have tread definition inside them. ABS marks are also shorter when compared to non ABS marks from a vehicle traveling in precisely the speed.
What else can skid marks tell us?
As you have already found skid marks may tell us about the tires inflation, ABS or non-ABS braking, and direction of travel. Marks can also tell us something when and in which the decision to brake occurred. This is the most under-utilized and under explored aspect even more so in speed crashes. Some basic calculations can be made, using a variety of aspects of the skid marks, to determine where the driver made the decision.
Why is this so important? Consider the following illustration.
This drawing is a timeless teaching example used to demonstrate the value of skid marks. Consider this situation, the blue car says he had the green light and was hit at the intersection. The car says so that that he braked hard he also had the light and saw the car. There isn’t any other evidence or witnesses.
Now the student would be asked to calculate the position of the cars once the decision to brake was created using the beginning of the skid marks, ultimately this would place the vehicles in the place labeled 1.
Now the apparent problem with the red car’s situation now that we have used the skid marks to ascertain where he determined to brake, a construction blocks his view of the blue car (position 1 for both vehicles). This begs the question as to why did he decide then to brake? The answer, the light was red for the red car and the driver was braking for traffic lighting, not the blue car making the red car culpable in this situation as the physical evidence affirms the “at fault” party.
Another valuable piece of advice is that rubber is biodegradable and there are naturally occurring nitrogen based bacteria that “eat” rubber. These bacteria are competitive and will eat rubber in most environments, therefore if you’re trying to determine causality and the “at fault” party, it is in your best interest to take pictures of the roadway whenever possible. Skid marks are gone in a brief amount of time.
Skid marks are a valuable item of evidence and a great tool for determining many facets in a collision; it is extremely important none of them are overlooked or underestimated.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
There are several reasons engineering and accident reconstruction reports are problematic. Let’s address the biggest and first issue, cost. Many attorneys won’t realize the real value of cases if they deal with doctors who do not know how to document the patient’s injuries correctly, leading to issues related to poor documentation management.
This is a massive benefit to the insurance company who have banked on the sloppiness and ignorance of the entire medical-legal community. However, there is a growing number of doctors and attorneys who do know.
In this sense, the insurance carrier knows they’ll pay, a vast majority of this time, a minimum amount for a collision even if the case needs to have a much greater value due to the nature of the injuries. The insurance companies know this for a number of reasons, but the biggest reason is cost, not for them but you.
Accident Reports and Insurance Companies
For the sake of discussion let’s say the average case settles for $15,000. If the collision specialist costs $2,000 to $5,000 (along with the doctors and the other experts), this is an expense which cannot or chooses not to be absorbed by solo attorney’s, smaller and even bigger legal firms. This is known by the insurance company and use it whenever it presents itself.
Why can a “deep pocketed” insurance company afford to pay a specialist on a smaller case? There are few reasons but the two are the insurance companies can absorb the expense of the consultants AND a smaller instances will perform the work, as good faith towards the client, pro bono, in some cases.
Obviously, if the attorney cannot make any money they will not take the situation and paying for a collision professional is a substantial factor in this decision, especially if the defense already has you. This greatly reduces the attorney’s costs per case while making you more valuable as a resource AND affords the attorney the chance to take on cases.
Identifying Inaccuracies
The cost concerns cause a second problem, identifying inaccuracies. I have yet to meet an crash engineering defense pro who will explain the shortfall of a case because it is going to expose their inaccuracies and will not bode well for them regarding referrals. MANY low speed collisions have gaps which must be filled in with information that is vetted and carefully selected. Using generalized data (that is the standard in the industry to work with) is quite dangerous as it makes the difference for results reliability too wide. The results will have margin for error and that margin of error is the difference between being or prevailing on the side and all accepted as accurate, but is not.
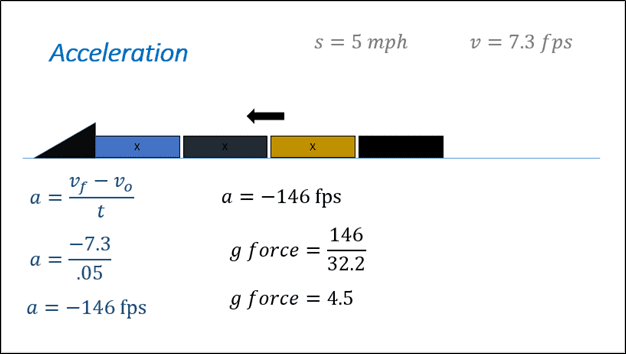
In this section we discuss why time is a critical element. In the picture above, we illustrate a train, which collides with a barrier at 100 miles per hour and crushes. The related math demonstrates how increasing the time decreases acceleration (see circled numbers). There is not any room for doubt regarding injury as its speed and acceleration is beyond accepted thresholds. What if the speeds change so they are very close to those injury thresholds?
Consider the second example, here the speed of the train represents final approach to a stop hurdle in which the engineer is a little careless and bumps the cease hurdle. What’s important to notice about this visual is the moment. If we double the time (from .05 to .1) the last g force is halved (resulting in 2.267 g’s). What if there were studies that we could cite which say the time necessary to stop for a train is .075 seconds? The first time value of .05 would be too brief, the second value of .1 would be too big, and both do not fit the cited studies.
In this case the period variable changes a tiny amount but the resulting change in the g forces may no longer be sufficient to substantiate a claim for injury. This is the reason the justification for any values is so significant. If you don’t understand they were selected and why the variables are there, they you do not know if they’re accurate or not. A deviation is often the arbiter in determining if there were sufficient transference of forces needed for 27, in a case for failure or success.
Conclusion
Cost and inaccuracies are a couple of the problems commonly faced by attorneys regarding collision reconstruction. For doctors, there’s now a recognized course to offer you the training to be an collision engineer/reconstructionist and for the attorney, when there is a defense engineer, you should have someone dissecting the math to ensure accuracy because usually the “guestimates” used will work against you in settlement or litigation.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
Chiropractor, Dr. Alex Jimenez looks at lumbar spine disc herniation. What are the Likely signs and symptoms associated with disc herniation, and what would be the selection criteria for micro-discectomy operation in athletes? Complaint in the young college age athlete and professional athlete, and it’s been estimated that over 30% of athletes complain of back pain at least once in the profession(1).
Lumbar spinal disc herniation is one kind Of lumbar injury that can’t just cause painful low back pain, but can also compress nerve roots and create radicular referral of pain into the lower leg with related sensation changes and muscle contraction. This injury will not only influence the short-term opponent ability of the athlete, but might also reoccur and eventually become persistent possibly causing a career ending injury.
Managing disc herniation from the athlete Usually begins with conservative therapy and if this fails, surgical solutions are considered. But often elite athletes will request a quicker resolution to their symptoms to minimize time away from competitors. Therefore, providing the criteria for lumbar spine surgery are suggested, the conservative period will often be compressed, and surgery will be sought earlier. The favored surgical process for the athlete with a disc herniation is that the lumbar disc micro-discectomy.
Anatomy & Biomechanics
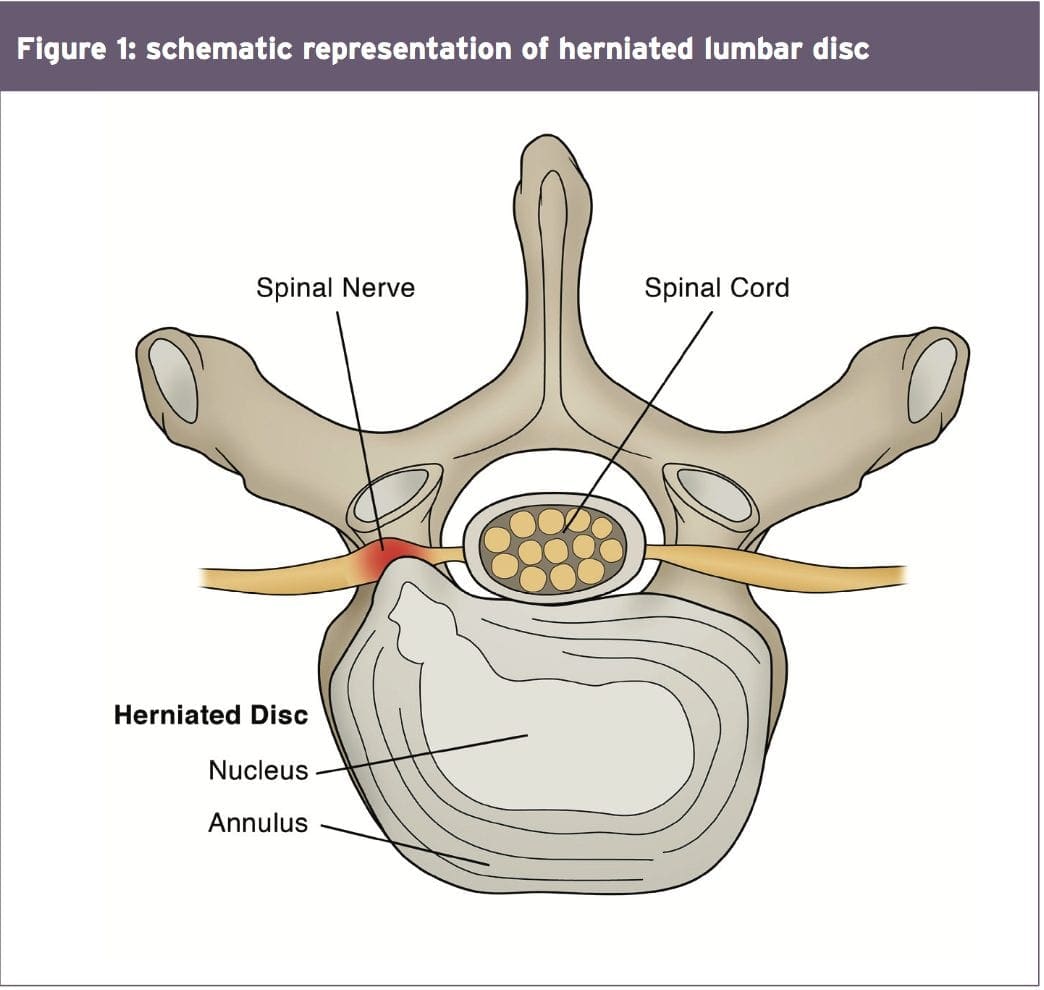
A significant biomechanical role in the spine, allowing for motion between the spinal segments while spreading compressive, shear, and torsional forces(2). These discs include a thick outer ring of fibrous cartilage termed the annulus fibrosis (akin to the onion rings enclosing the center of the onion), which encompasses a more gelatinous core called the nucleus pulposus, which is included within the cartilage end plates inferiorly and superiorly.
The intervertebral disc consists of Cells and substances such as collagen, proteoglycans, and thin fibrochondrocytic tissues, which enable transmission and absorption of forces arising from body weight and muscle activity. To do so, the disc depends mainly on the structural condition of the nucleus pulposus, annulus fibrosis and the vertebra lend plate. If the disc is normal and is functioning optimally, then forces are spread across the disc evenly(3).
But disc degeneration (mobile Degradation, lack of hydration( disc failure) may decrease the capacity of the disc to withstand extrinsic forces, as forces are no longer distributed and spread evenly. Tears and fissures from the annulus can lead, and with adequate external forces, the disc material may herniate. Alternatively, a sizable biomechanical force set on a healthy, ordinary disc may cause extrusion of disc material as a result of crushing failure of this annular fibers — illustrations include a hefty compression type mechanism because of a fall on the tailbone, or strong muscle contraction such as heavy weight lifting(4).
Herniations represent protrusions of Disc material beyond the confines of this annular lining and in the spinal canal (see Figure 1)(5). If the protrusion does not invade the canal or undermine nerve roots then back pain may be the only symptom.
Endoscopic Discectomy 3D Simulation
The pain associated with lumbar Radiculopathy happens due to a mix of nerve root ischemia (due to compression) and inflammation (because of neurochemical inflammatory mediators released from the disc). Throughout a herniation, the nucleus pulposus puts pressure on weakened regions of the annulus, and proceeds through the diminished websites in the annulus in which it ultimately forms a herniation(6 ft). It follows from this that some kind of disc degeneration may exist prior to the disc may really herniated(7).
In contrast to other respiratory Tissues, discs have a inclination to degenerate earlier in life, with some studies demonstrating adolescents presenting signs of degeneration between the ages of 11 to 16(8). With increasing age, there’s further degeneration of the intervertebral discs.
While the disc might be in danger of harm in All fundamental planes of motion, it’s particularly susceptible during repetitive flexion, or hyper-flexion, combined with lateral bending or rotation(10). Traumatic events such as excessive axial compression may also damage the inner structure of the disc. This can occur as a result of a fall or powerful muscular forces developed during tasks such as heavy lifting.
Athletes are generally exposed to high loading conditions. Examples of this include:
1. World-class power lifters, in which the calculated compressive loads on the backbone are involving 18800 Newtons (N) and also 36400N acting in the L3-4 motion segment(11).
2. Elite level football linesmen who have Been proven to present time-related hypertrophy of this disc and changes in vertebrae endplate in response to this repetitive high loading and axial pressure(12).
3. Long distance runners have been Shown to undergo significant strain into the intervertebral disc, indicated by a reduction in disc height(13).
Herniations could be classified depending on Ultimately, herniations are also identified based on level, with most herniations happening at the L4/5 and L5/S1 intervertebral disc level; these can then in turn affect the L5 and S1 nerve roots resulting in clinical sciatica(15). Upper level herniations are less common, and when they do occur with radiculopathy, they will affect the femoral nerve. Finally, the prevalence of disc injury rises increasingly caudally, with the best numbers at the L5/S1 degrees(16).
Herniation In Athletes
The offending movements implicated in The 20-35 age group are the most common group to herniate a disc, most likely because of the fluid nature of the nucleus pulposis and due to behavior(18). This age group are more likely to participate in sports which need high lots of flexion and spinning or are reckless with their positions and positions during loading.
The sports most at risk of disc herniation are:
Hockey
Wrestling
Soccer
Swimming
Basketball
Golf
Tennis
Weightlifting
Rowing
Throwing events
These are the sports that involve either significant Furthermore, those who take part in more and more severe training regimes seem to be at higher risk of spinal pathologies, as do people involved in sports.
Signs & Symptoms Indicating Discectomy
The efficacy of management programs for lumbar spine disc herniation — in terms of the decision to operate or treat conservatively — will be discussed in greater depth in part 2 of this series. However, the decision to operate within an athlete is generally driven by the motivation and approaching goals the athlete has put themselves. They may in fact favor a comparatively simple micro-discectomy instead of waiting for symptoms to abate through an extended period of rehabilitation.
This conservative period of Management may involve medicine therapy, epidural injections, relative back and back muscle recovery, acupuncture, osteo/chiropractic interventions. On the other hand, the normal presenting symptoms and signs that suggest a substantial disc herniation that will require surgical intervention in the athlete comprise:
Low back pain with pain radiating down one or both legs
Positive straight leg raise test
Radicular pain and neurological signs consistent with the nerve root level affected
Mild weakness of distal muscles such as extensor hallucis longus, peroneals, tibialis anterior and soleus. These would fit with the myotome relevant for the disc level
MRI confirming a disc herniation
Possible bladder and bowel symptoms
Failed conservative rehabilitation
Time span in which to enable conservative rehabilitation to be effective. In the overall population, medical practitioners will most likely prescribe a minimal 6-week traditional period of treatment with an overview at 6 weeks as to whether to expand the rehabilitation a further 6 weeks or to seek a specialist opinion. The expert may then attempt more medically orientated interventions such as epidural injections.
The athlete nevertheless will have these They might be more inclined to experience an epidural very early in the conservative period to assess the effectiveness of this procedure. If no signs of progress are evident in a couple of weeks then they may choose to get an immediate lumbar spine micro- discectomy.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques. From the El Paso, TX. Spine Center.
Imaging
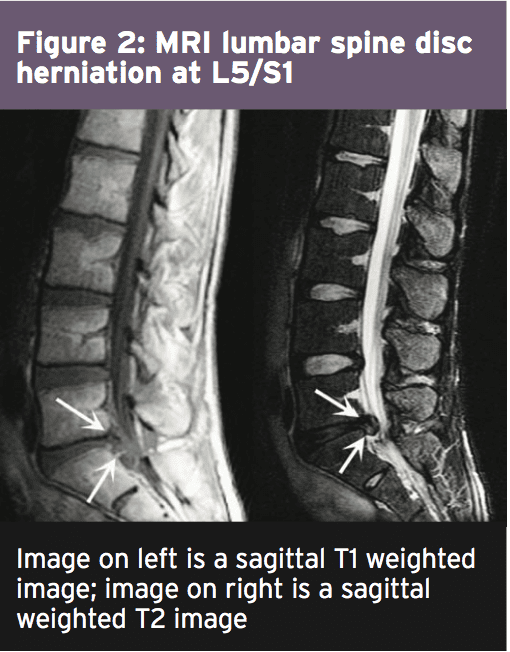
MRI remains the favored system of Identifying lumbar spine disc herniation, since it’s also very sensitive to detecting nerve root impingements(23). However, abnormal MRI scans can occur in otherwise asymptomatic patients(25); hence, clinical correlation is always essential before any surgical thought. What’s more, patients can present with clinical signs and symptoms which suggest the diagnosis of acute herniated disc, and yet lack evidence of sufficient pathology on MRI to warrant operation.
Therefore it has been proposed that a Volumetric analysis of a herniated disc on MRI may be potentially beneficial in checking the suitability for operation. Several writers have previously mentioned the possible value of volumetric evaluation of herniated disc on MRI as part of their selection criteria for lumbar surgery(26).
In a survey conducted in Michigan State University, it was found that the size and positioning of the herniated disc determined that the likelihood for operation with what researchers called ‘types 2-B’ and ‘types 2-AB’ being the most likely candidates for surgery(27).
The MRI protocol to your lumbar spine consists of (see Figure 2)
1.Sagittal plane echo T1- weighted sequence
2. Sagittal fast spin echo proton density sequence
3. Sagittal fast spin echo inversion recovery sequence
4.Axial spin echo T1- weighted sequence
Summary
Disc herniations are not a common Complaint in athletes, but they do happen in sports which involve high loads or repetitive flexion and rotation movements. Sufferers of a disc herniation will normally feel focused low-back pain, maybe with referral in the lower limb with associated neurological symptoms if the nerve root was compressed.
Managing a disc herniation within an General population as frequently the risk of a Protracted failed rehabilitation period is Bypassed for the protected and low risk Micro-discectomy procedure. In the Discuss the exact surgical alternatives involved Observing a lumbar spine micro-discectomy.
References
1. Sports Med. 1996;21(4):313�20
2. Radiology. Oct 2007;245(1):62-77
3. Arthritis Research & Therapy. 2003;5(3):120-30
4. The Journal of Bone and Joint Surgery. American volume. Feb 2004;86-A(2):382 � 96
5. Radiology. Oct 2007;245(1):43-61
6. Spine. Sep 15 1996;21(18):2149-55
7. Spine. May-Jun 1982;7(3):184-91
8. Spine. Dec 1 2002;27(23):2631-44
9. Lancet 1986;2:1366�7
10. Disease-A-Month:DM. Dec 2004;50(12):636-69
11. Spine. Mar 1987;12(2):146-9
12. The American Journal of Sports Medicine. Sep 2004;32(6):1434-9
13. The Journal of International Medical Research. 2011;39(2):569-79
14. Spine. 2001;26:E93-113
15. Spine. 1990;15:679-82
16. British Journal of Sports Medicine. Jun 2003;37(3):263-6
17. Prim Care. 2005;32(1):201�29
18. McGill, S.M. Low back disorders: Evidence based prevention and rehabilitation, Human Kinetics Publishers, Champaign, IL, U.S.A., 2002. Second Edition, 2007
19. Spine. Apr 1991;16(4):437-43
20. Skeletal radiology. Jul 2006;35(7):503-9
21. British Journal of Sports Medicine. Nov 2007;41(11):836-41
22. The American Journal of Sports Medicine. Jun 2009;37(6):1208-13
23. Spine. Mar 15 1995;20(6):699-709
24. Phys Sportsmed. 2005;33(4):21�7
25. J Bone Joint Surg Am 1990 . 2:403�408
26. J Orthop Surg (Hong Kong) 2001. 9:1�7
27. Eur Spine J (2010) 19:1087�1093
The more alcohol people drink, the faster their cells appear to age. Researchers from Japan’s Kobe University Graduate School of Medicine found that alcoholic patients had shortened telomeres which placed them at greater risk for age-related illnesses.
Telomeres are the pieces of DNA that act as protective caps on the ends of chromosomes. Chromosomes, which protect our genes, get shorter every time a cell divides. Once a chromosome gets too short, it dies. Many studies have shown that shortened chromosomes are associated with the diseases of aging, especially cardiovascular disease, dementia, and diabetes.
“Telomeres, the protein caps on the ends of human chromosomes, are markers of aging and overall health,” said Naruhisa Yamaki, M.D. But aging isn’t the only cause of shortened telomeres.
“Our study showed that alcoholic patients have a shortened telomere length, which means that heavy drinking causes biological aging at a cellular level,” he said.
Yamaki and his co-authors recruited 255 study participants from alcoholism treatment services at Kurihama National Hospital in Yokosuka, Japan: 134 alcoholic patients and 121 age-matched controls or non-alcoholics, ranging in age from 41 to 85 years old. DNA samples, as well as drinking histories and habits, were collected from all participants.
“We also found an association between telomere shortening and thiamine deficiency (TD),” said Yamaki. Thiamine is a B vitamin.
“TD is known to cause neuron impairments such as Wernicke-Korsakoff Syndrome. Although how exactly TD can cause neural impairments is unclear, it is well known that oxidation stress causes telomere shortening and, thus, it is possible that oxidation stress may also cause neuron death.”
According to a study from King’s College London, one in five seniors drinks too much, which could have devastating effects on baby boomers. “As the baby boomer generation become seniors, they represent an ever increasing population of older people drinking at levels that pose a risk to their health,” said lead author Dr. Tony Rao.
“This study shows the need for greater awareness of the potential for alcohol related harm in older people.”
Good Night’s: Feeling stressed at work can lead to us reaching for unhealthy snacks and extra portions, but a new study has found that getting enough sleep could help buffer the negative effect of stress on eating habits.
Carried out by a team of researchers from Michigan State University, the University of Illinois, the University of Florida, and Auburn University in the US, along with Sun Yat-sen University in China, the study is one of the first to look at how psychological experiences at work can affect eating behaviors.
The team looked at two studies of 235 total workers in China who experienced regular stress in their jobs.
One study included IT employees who had a high workload and felt there was never enough time in the workday, while the second included call-center workers who experienced stress from dealing with rude and demanding customers.
The researchers found that in both studies employees who had a stressful workday also had a tendency to take these negative feelings home with them, and to the dinner table, leading to them eating more than usual and make unhealthier food choices.
However, the study also showed that sleep could be a way to buffer this effect of stress on unhealthy eating, with the team finding that employees who got a good night’s sleep the night before tended to eat better the next day after a stressful day at work.
Yihao Liu, co-author and assistant professor at the University of Illinois gave two possible explanations for the findings.
“First,�eating is sometimes used as an activity to relieve and regulate one’s negative mood, because individuals instinctually avoid aversive�feelings�and approach desire feelings,” he said.
“Second, unhealthy eating can also be a consequence of diminished self-control. When feeling stressed out by work, individuals usually experience inadequacy�in exerting effective control over their cognitions and behaviors to be aligned�with personal goals and social norms.”
Chu-Hsiang “Daisy” Chang, MSU associate professor of psychology and study co-author, also commented that the findings that sleep has a protective effect against unhealthy food habits shows how the three health behaviours of sleep, stress, and eating are related.
“A good night’s sleep can make workers replenished and feel vigorous again, which may make them better able to deal with stress at work the next day and less vulnerable�to unhealthy eating,” she explained.
The team now believe that companies should take into consideration the importance of sleep and healthy behaviors and think about providing sleep-awareness training and flexible scheduling for employees, as well as rethinking�food-related job perks, which have become very common.
“Food-related�perks may only serve as temporary mood-altering remedies�for stressed employees,” Chang said, “and failure to address the sources of the�work�stress�may have potential long-term detrimental effects on�employee�health.”
The findings were published in the�Journal of Applied Psychology.
There is an assortment of questions which centered around police reports and accident scenes. We’ll address reports exist, how conclusions are made, and what exactly you should take from the role of the police officer and a report as an investigator. This topic can be broken down into lots of classes; here we will concentrate on collision analysis and general reporting.
Why do police take general reports? The brutal answer is because nobody will recall the facts in just two days, much less two decades and they’ll argue it but it’s also because a third party who should be an impartial fact evaluator is needed by society. “Should” is emphasized, but we need to describe what an impartial evaluator of reality is at the context of the writing. We are currently assuming the officer / deputy has training that is sufficient to ascertain what evidence plays into the circumstance. Imagine if you went into a call for attack involving wife and a husband. Upon arrival you are told that the husband is using drugs and sexually assaulting a young child by the wife. When you question the husband he denies the claim and also has the wife’s prescription bottle in his hand — the medicine’s listed side effect is “hallucinations”. This is relevant evidence that the law enforcement officer should weigh in her or his choice.
We are also likely to assume that the officer / deputy doesn’t have any bias or stereotype towards the parties involved OR they perform however recognize it and adjust accordingly. Imagine if the officer went through a tough divorce and from above is female. Does her life have an impact on thinking the husband? What exactly does should she do about it, if it does?
Police Reports After Auto Accidents
Authorities write collision reports for the nation (in which they operate) departments of transportation. The report is designed to collect information regarding roadway design, operator error, alcohol and /or drug use, etc.. One of the concerns that are final is for the report to record for the parties, while significant.
With utilizing report templates, expertise, training, and bias may significantly impact collision reports. Why?
There are many reasons police have errors in their accounts, but by far, the main reason is lack of coaching. To be able to make a police officer, candidates attend an academy that averages some are more. Collision investigation for recruit training is less than a day’s worth of training. In this time the educator should cover everything from scene safety to general hazards to traffic patterns. In reality, unless the student after graduation and into his or her livelihood chooses to attend further training there will be refreshers no updates, upgrades, or continuations to the academy foundation.
Specialty training is imperative to understand the concepts as well as the physics behind a motor vehicle collision and these aren’t part of this basic academy curriculum. Therefore, when determining specifics of the injury it’s critical to determine the extent of training of the police officer.
To address the last point, what you ought to take away from a collision report, we will go over a true case brought to me by one of you.
A while back I was contacted by a physician, his family member had been involved in a collision where she had been rear ended by a truck in heavy traffic; double. The officer their vehicle was launched with the truck behind it in a lane of travel was told by the family member. The vehicle struck on the vehicle while in traffic. The truck driver told the investigating officer he didn’t understand where the vehicle he broke was, but he was coming onto the road through an “on ramp” and thought the vehicle tried to pass him at the shoulder and cut in front of him that is why he broke it.
The investigating officer admitted there were not any marks at the roadway to establish where the event happened but he didn’t write the report in favor of this truck driver. When I inquired about his foundation he told me and his reasoning:
“I wrote that the report in favor of the truck driver based on the damage to the vehicles although I had no formal training on harm interpretation and event correlation and couldn’t establish through signs, in which the vehicles were in the lanes of travel.” In this case the municipality who uses him would be the main problem while the gut reaction would be to blame the officer. This agency has failed to train the officer and also supply guidelines to function inside to him.
All that can be taken away from the crash itself would be the vehicle rear ended the vehicle and it likely occurred as the vehicle driver described in which the vehicle driver admitted not knowing where the vehicle was supposed to begin with.
Conclusion
So what do you remove a police crash report? Those facts that can be verified soundly proof, or by witness reasoned by them both. The police are fact gatherers, not “causality arbiters” and must be utilized as such. The caveat is that there are police specialists who have advanced training in accident reconstruction, crash dynamics and accident investigation. My training makes me to be adept in all those disciplines, but the average police officer is not and shouldn’t be considered as a person.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 . �
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
A good read to understanding alteration of motion segment integrity (AOMSI) is the article �Biomechanical Analysis of clinical instability in the cervical spine� White, et al., Clin Ortho Relat Res, 1975;(109):85-96.
AOMSI is a biomechanical analysis. It�s all about numbers that have clinical meaning and significance. Threshold values have been determined that quantify without a doubt the patient has serious injury. It is a test of structural integrity of the ligaments interconnecting the motion segments. In this case, structural integrity has to do with the material properties of ligament tissue. Those properties include strength and flexibility. When a material is both strong and flexible, it�s called a semi-rigid material. Strength is related to the composition of the material. Strength might be thought of as load carrying capacity before failure.
Mechanism of Injury: Ligaments
Ligament tissue has previously been bench tested to describe its physical characteristics of stress/strain. That is, given so much load (stress) how much elongation will occur (strain). During normal physiologic loads the ligament remains intact and recoils to its original length when the load is removed. If the load becomes too large the materials (ligaments) begin to yield. They go past their elastic limit. When this happens the (strained) ligament fibers will not return to their original shape. The ligament loses its restraining capacity to hold the joint in normal stabilization and hypermobility occurs.
The ligaments, if sufficiently strained or avulsed results in AOMSI. The following paragraphs illustrates that if AOMSI is found there must be gross destruction or yielding of multiple ligaments. We need to build a BIG motion segment with Velcro ligaments. When you tear them off, they make a really nice ripping noise. That drives home the point.
In the White et al work, they found that the motion segment stayed intact i.e., less than 11 degrees� rotation (angualr mtion) and less than 3.5 mm translation, until they transected over 50% of the ligaments from an anterior or posterior approach. And when they transected from either approach the loss of stability was not linear but suddenly catastrophic. And they meant that suddenly the two vertebra totally separated in rotation or translation.
Suddenly Separated: pulled apart, head off of body, all neural components compromised, paralysis. Keeping that in mind, what are the injuries of someone just under the threshold? Severe to very severe. They stand the possibility of a serious event with much less force.
Prevalence of Ligament Injury: AOMSI
If AOMSI is detected, think about more than 50% of ligaments transected. That will start to explain the seriousness of the finding. In a patient/child that demonstrates hypermobility everywhere, then you take a statistical average of all segments, and look at the aberrant statistical finding if it exists. There are clues to injury everywhere when you understand what the numbers mean in reference to stability and function.
To diagnose ligament laxity, it is imperative that imaging be performed and a basic flexion-extension x-ray is all that is required. In today�s medical economy, advanced imaging of MRI or CT Scan, although accurate becomes an unnecessary expenditure and an x-ray renders very accurate demonstrative images to conclude a definitive diagnosis. In determining if there is an impairment, it is necessary to follow the AMA Guides to the Evaluation of Permanent Impairment as the 4th, 5th and 6th editions all render an impairment for AOMSI as sequella to ligament laxity, which is damage to the ligament from trauma.
This document is intended to serve as a simple explanation as to the severity of ligament damage and how to demonstrably diagnose the injury. It is also critical to remember that ligament do �wound repair.� In normal physiology, ligaments grow during puberty from cells within the ligaments called fibroblasts. They produce both collagen (white) and elastin (yellow) tissue, which gives the ligaments both tensile and elastic strength. Upon puberty the cells stop producing tissue and remains dormant. Upon injury, the fibroblast reactivates, but can only produce collage leaving the joint wound repaired in an aberrant juxtaposition (place) with poor movement abilities due to the lack of the requisite elastin. In turn, according to Hauser et. Al (2013) this leads to permanent loss of function of the ligament and arthritis of the joint. This is not a speculative statement; it is based upon Wolff�s that dates back to the late 1800�s and has been a guiding principle in healthcare for more than a century.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References:
White, et al., Clin Ortho Relat Res, 1975;(109):85-96
Hauser, Dolan,Phillips, Newlin, Moore Woldin, B.A.(2013) Ligament injury and healing: A review of current clinical diagnostics and therapeutics.The Open Rehabilitation Journal, 6,1-20.
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
When the aberrant sequela to victims in car crashes has been investigated, providers often overlook and concurrently underestimate the tissue pathology and resultant biomechanical failures of spinal ligamentous damages commonly known as �strain � sprain.� In addition, the courts have been �blinded� by rhetoric in allowing this pathology to be deemed transient. There is an ever growing body of scientific literature that verifies strain – sprain as permanent pathology, which is the standard being taught in today�s medical and chiropractic academia.
In addition, strain � sprain as sequela to whiplash, renders a 25% whole person impairment based upon the American Medical Association�s Guide to the Evaluation of Permanent Impairment fifth and sixth editions.
Whiplash Associated Disorder Sequela Injuries
Juamard, Welch and Winkelstein (2011) reported:
��Rear end accelerations have been used to study the response of a variety of soft tissues in the cervical spine, including the facet capsular ligament. For simulations of whiplash exposures, the strains in the capsular ligament were found to be two � five times greater than those sustained during physiological motions of the cervical spine. In a similar but separate study, the facet joints of the cervical spine�s that were previously exposed to a whiplash injury ridden exercise under low � level tension and found to undergo elongations nearly 3 times greater than on exposed ligaments for the same tensile loads. Those capsular ligaments were also found to exhibit greater laxity after the purported injury. Since increased laxity may be linked to a reduction in the joints ability to stabilize the motion segment during sagittal motion, this finding suggests that whiplash exposure may alter the structure of the individual�s tissues of the facet, such as the capsular ligament, and/or the mechanotransduction processes that could maintain and repair the ligamentous structure. Accordingly, such an injury exposure could initiate a variety of signaling cascades that prevent a full recovery of the mechanical properties of the tissues of the facet joint.� (Pg 15)
Simply put, if we focus on the last sentence above, this �prevents a full recovery of the mechanical properties of the tissues of the facet joint,� which is referencing the ligaments of the spine that make up the tissues of the facet joint. In lay terms; it means that once injured, a joint is permanently damaged and it is demonstrable on x-rays with an extension and flexion view that does not have to show a full dislocation. Therein lies the core of the issue. Most radiologists are not trained in the latest literature on biomechanical tissue failures and therefore underreport the pathology.
Last month I attended a presentation by Michael Modic MD, Neuroradiology, a nationally renowned educator in neuroradiology who focuses on spondylolisthesis (vertebral segmental abnormal movements) and I asked a simple question �why don�t radiologist report more on abnormal positioning due to biomechanical failure as a result of ligament pathology� and his answer was �because their training focuses more on disease pathology.� Although I agree that is critical, so are biomechanical failures that lead to chronic degeneration, which is epidemic in our society. Simply look at the posture of our elderly for verification and much of that started with a simple �fender bender� years ago where the strain-sprain was either undiagnosed or deemed transient and not treated.
Ligament Pathology Diagnosis and Prognosis
The above scenario is why the American Medical Association values ligament pathology at 25% whole body impairment. There is also a growing body of doctors who are trained and credentialed in Spinal Biomechanical Engineering that understand how to create a diagnosis and prognosis, along with treatment plans around ligament pathology and fully understand the long-term effects of damaged facet joint tissues. These doctors are currently educating, based upon the current scientific literature their respective radiology communities to be able to diagnose and document the full extent of the injuries sustained.
We must also recognize that there is a significant amount of evidence in the scientific literature that verifies ligamentous damage as permanent and refutes the rhetorical claim of �transient.� In the end, it must be the facts of human physiology verified by science that sets the standards of healthcare and not deceptive rhetoric at any level.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References:
Cocchiarella L., Anderson G., (2001) Guides to the Evaluation of Permanent Impairment, 5th Edition, Chicago IL, AMA Press
Juamard N., Welch W., Winkelstein B. (July 2011) Spinal Facet Joint Biomechanics and Mechanotransduction in Normal, Injury and Degenerative Conditions, Journal of Biomechanical Engineering, 133, 1-31
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
Gray hair could be an early warning sign of heart disease. Hiccups that won’t go away may foreshadow cancer. Sometimes your body sends seemingly unrelated signals that something is wrong.
Since the key to treating most health problems is to catch them early, it can pay off big time to spot the tip-offs. And the first thing to check out is your skin.
“Skin is the only organ of the body that you wear on the outside,” says dermatologist Dr. Robert Brodell. “Since it’s connected to internal organs through blood vessels, nerves and other things, it can be like a window to see what’s going on inside.”
Here are 10 symptoms and what they may really mean:
Rash on shins: Formally called necrobiosis lipoidica diabeticorum (NLD), a raised red-brown patch with yellow blotches could mean that you have diabetes or are poised to get it. “Sometimes we see this in patients and know they are diabetic before they know it themselves,” says Brodell, chairman of the dermatology department at the University of Mississippi Medical Center. “In some cases, their blood sugar is normal, but over the next six months to two years, they develop diabetes.”
Splinter hemorrhages: They look like thin red splinters running lengthwise under fingernails and could be caused by endocarditis, a bacterial infection of the heart valves. “You wouldn’t think that someone looking at fingernails could detect what could be a significant heart problem,” Brodell tells Newsmax Health.
Rash on eyelids: This violet-hued rash is a symptom of dermatomyositis, an inflammatory muscle disease that is associated with various forms of cancer, most commonly ovarian. Other symptoms include raised scaly bumps on knuckles and ragged cuticles that separate from the nail.
Skin discoloration: The most common is jaundice, a yellowing of the skin that is a classic symptom of hepatitis and other liver conditions. Less known is a darkening of the skin in creases and old scars that may indicate an adrenal gland problem, such as Addison’s disease.
Tender nodules on shins: A condition called erythema nodosum is marked by red swollen bumps on the front of the legs. Brodell says that while they are sometimes a reaction to medications or oral contraceptives, they could also be a warning of the inflammatory pulmonary disease sarcoidosis.
Persistent hiccups: For most of us, this spasm of the diaphragm is an annoying but harmless problem. But when hiccups last two days or more, they could be an early warning sign of deadly esophageal cancer.
Shoplifting: If your elderly mom or dad starts getting sticky fingers, it could be a sign of a certain type of dementia. A study published in the Journal of the American Medical Association’s Neurology details how people with frontotemporal dementia lose their sense of societal conventions and may take items in shops without paying for them.
Color blindness: The inability to distinguish between different hues is a sign of Parkinson’s disease. Other odd symptoms of the neurological disorder are writing smaller and swimming in circles.
Earlobe wrinkle: A diagonal crease in one or both earlobes has long been linked to heart disease. Also called “Frank’s sign” after Dr. Sanders T. Frank, the physician who first made the association, this odd symptom has been supported in several studies, though no one has yet to figure out why.
Gray hair: A touch of gray is another early warning sign of cardiovascular problems, regardless of age and other factors, according to a recent study by Egyptian researchers. Heart disease in general can generate several seemingly unrelated symptoms, including bleeding gums, swollen feet, frequent urination at night, uncontrollable head bobbing, yellow spots on eyelids…and the list goes on.
“The reason that heart disease has so many varied symptoms may be because there are many types of heart disease that will present in different ways,” explains Dr. Richard Greenberg, a cardiologist at Temple University Hospital in Philadelphia, Pa. “Another reason is that the circulatory system is connected to every cell in the body, so it follows that symptoms of heart disease could show up anywhere.”
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine