The body’s lower extremities have a very important role as it helps support the upper body’s weight and provide stability to the lower body. The lower half of the body consists of the lower abdominals, hips, pelvic, and buttock regions, which have various muscles surrounding the lumbar and pelvic areas of the spine. These muscles help protect the lower vital organs and work with the central nervous system to utilize the sensory-motor function of the legs and feet. When normal factors like prolonged sitting or standing begin to affect the lower body, it can cause referred pain to travel down to the legs and push the lower extremities to develop symptoms associated with trigger points on the lower torso. Today’s article looks at the lower torso, how trigger points affect the lower torso, and therapeutic ways to manage trigger points in the lower torso. We refer patients to certified providers who incorporate various techniques in more inadequate body pain treatments related to trigger points to aid people suffering from pain-like symptoms along the lower torso muscles along the body’s lower extremities. We encourage and appreciate patients by referring them to our associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Lower Torso?
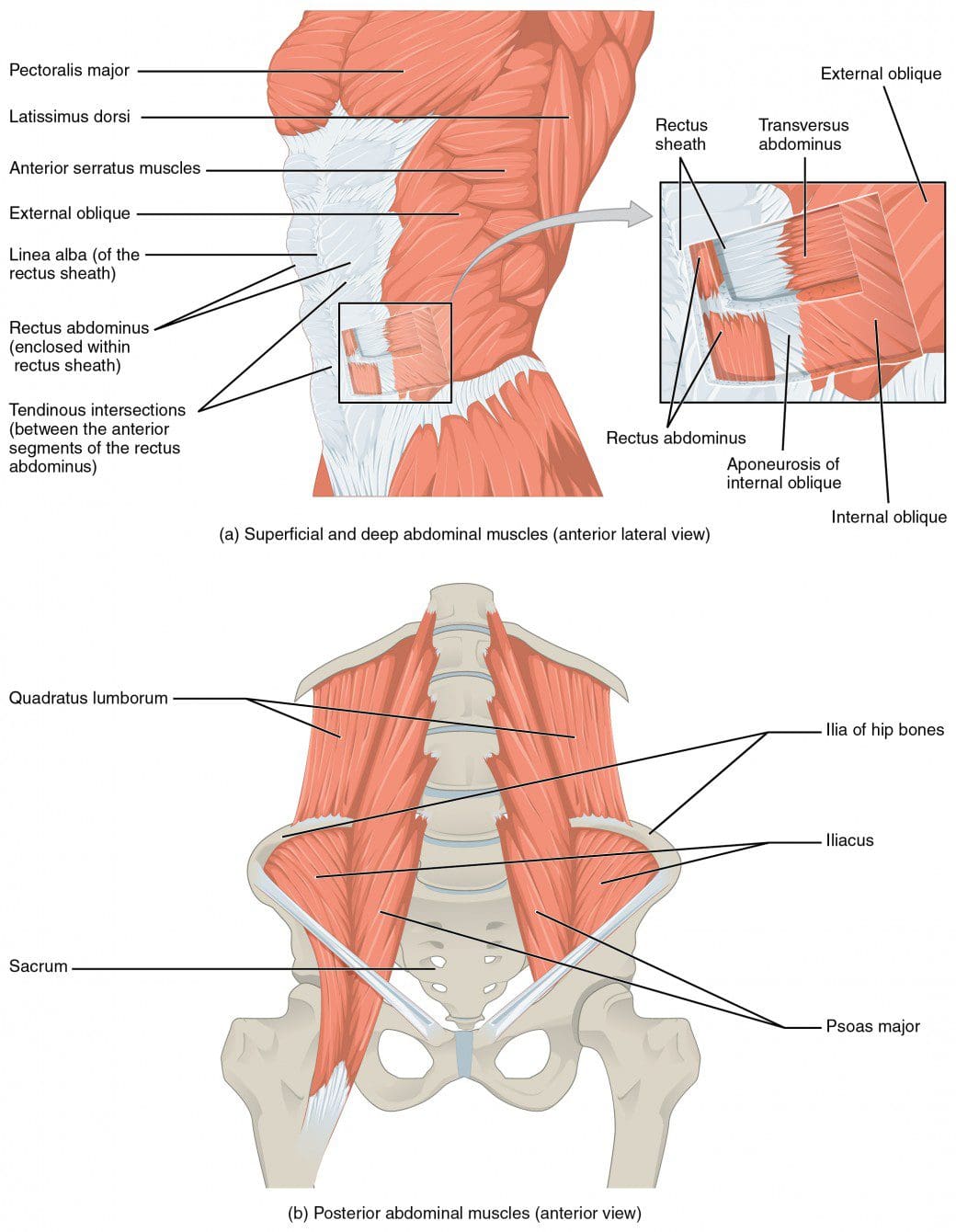
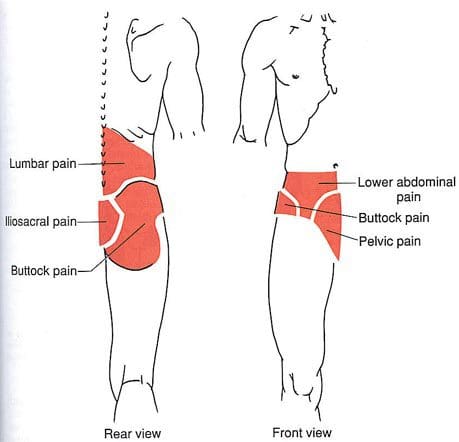
Have you been feeling stiffness around your hips lately? Have you noticed that you are leaning forward constantly, causing strain on your lower back? Or have you been experiencing pain in one location in your lower half? When dealing with these issues in the lower half of the body, it could correlate with somato-visceral symptoms associated with trigger points in the lower torso. The lower torso of the human body, or the lower abdominals, is defined as the anterior region of the trunk between the thoracic diaphragm and serves as the cavity to house the digestive, urinary, endocrine, and parts of the reproductive system. The lower torso has various muscles and nerves that surround the lower back, the hips, the pelvis, and the buttock region of the body that stabilizes the legs when in motion and supports the upper body. The muscles in the lower torso also surround the lumbar and pelvic areas of the spine to protect the joints and vertebrae from becoming dysfunctional. When issues begin to rise and affect the lower torso, it can lead to overlapping problems affecting the body’s lower extremities.
How Do Trigger Points Affect The Lower Torso?
Some of the issues affecting the lower torso that most people don’t realize are that prolonged sitting or standing can cause problems to the legs, hips, pelvis, and feet. This causes the blood supply to pool into the legs and feet, thus causing swelling and muscle weakness in the lower torso muscles. Another issue is when the lower torso has been through a traumatic event that can cause the affected muscles to develop tiny nodules known as trigger points to cause problems in the lower back, hips, pelvis, and buttock region of the body. Studies reveal that trigger points are often characterized by pain causing a limited range of motion in the joints while causing muscular contracture and mimicking other chronic conditions affecting the muscles. When trigger points affect the muscles in the lower torso, “Myofascial Pain and Dysfunction,” written by Dr. Janet Travell, M.D., pain associated with movement can cause tingling or electric sensations down to the lower extremities causing somato-visceral referred pain to the lower torso. Since the nerve roots from the spinal cord branch out to the various muscles and become irritated, causing referred pain to different areas of the lower extremities.
Trigger Point Therapy For The Abs- Video
Have you been dealing with hip mobility issues? What about experiencing low back pain after being in a hunch position for an extended period? Or have you been experiencing problems in your pelvic region? Many of these issues are correlated with trigger points associated with the lower torso. Trigger points or myofascial pain syndrome are caused when the affected muscles have been overused or been through a traumatic event that causes referred pain to different body locations. The video explains where trigger points are located in the lower torso, especially in the abdomen and how to release them through palpations and massage. These techniques can help reduce the pain symptoms that affect the lower torso and manage myofascial pain from developing in the future.
Therapeutic Ways To Manage Trigger Points In The Lower Torso
Pain specialists like chiropractors and massage therapists will use various techniques to reduce the pain and alleviate the trigger points from the affected muscles. Many often go to a pain specialist who deals with trigger points through recommendations by their primary doctor. They will go through an examination process and explain to the pain specialist where the pain is located. Afterward, they will devise a treatment plan with the patient’s primary doctor, allowing them to follow a routine to prevent the pain from returning. Various techniques like stretching the abdominals, exercising, and resting can manage trigger points from returning to the affected muscles and even help bring muscle strength back to the body.
Conclusion
The lower torso consists of the hips, lower back, pelvis, and buttock region while protecting the body’s vital organs. The lower torso helps stabilize, the lower body extremities and supports the upper body’s weight. When normal issues like prolonged sitting or standing start to cause muscle strain to the lower torso region, it can develop trigger points to cause various problems to that region and cause mobility issues in the lower abdominal area. When the pain becomes unbearable, many individuals go to a pain specialist to help manage the trigger points from affecting the lower torso region and bring back mobility function to the lower extremities.
References
Akamatsu, Flavia Emi, et al. “Anatomical Basis of the Myofascial Trigger Points of the Gluteus Maximus Muscle.” BioMed Research International, Hindawi, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5733974/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Wade, Christian I, and Matthew J Streitz. “Anatomy, Abdomen and Pelvis, Abdomen – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK553104/.
When it comes to the torso is surrounded by various muscles that help protect the vital organs known as the gut system and help with stabilizing the spinal column in the body. The abdominal muscles are essential to maintaining good posture and core support for many individuals. When normal activities or chronic issues begin to affect the body, the abdominal muscles can also be affected and can cause referred pain all around the torso area. When the abdominal muscles are dealing with referred pain, it can develop into trigger points that mask other chronic conditions affecting the torso and the thoracolumbar region. Today’s article looks at the abdominal muscles and their function, how trigger points are affecting the abdomen, and how various treatments help manage trigger points associated with abdominal pain. We refer patients to certified providers who provide different techniques in abdominal pain therapies related to trigger points to aid many suffering from pain-like symptoms along the abdominal muscles along the torso. We encourage patients by referring them to our associated medical providers based on their examination when it is appropriate. We designate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
The Abdominal Muscles & Their Function
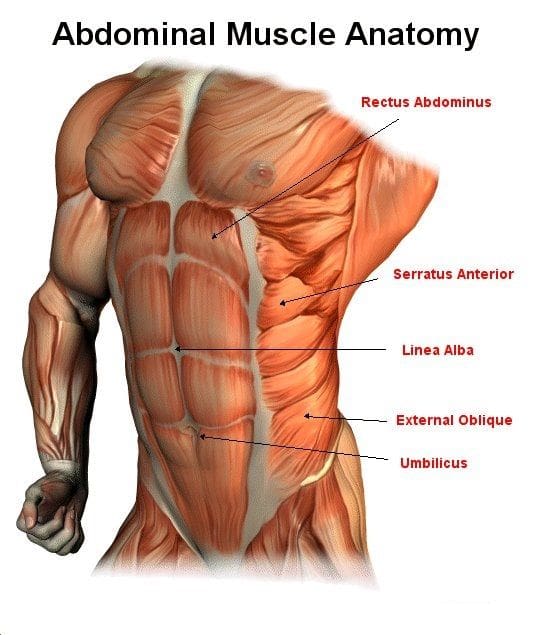
Do you have trouble moving around? Have you been dealing with muscle spasms along your abdomen? Does it hurt when you are sneezing, laughing, or coughing constantly? All these actions affecting your abdominal muscles might correlate with trigger points along the muscles and disrupt the torso area. The abdomen in the body has various muscles, a complex organ with many functions that contribute to a person’s quality of life. The abdominal muscles have many important parts, from supporting the trunk, allowing movement like twisting and turning, and holding the organs in the gut system in place through internal abdominal pressure regulation. The abdominal muscles have five main muscles that work together with the back muscles to keep body stability. They are:
Pyramidalis
Rectus Abdominus
External Obliques
Internal Obliques
Transversus Abdominis
Studies reveal that the abdominal muscles can help increase the stability of the lumbar region of the body from the vertebral columns by tending the thoracolumbar fascia and raising the intra-abdominal pressure. This allows the abdominal muscle to bend and flex in different positions without feeling pain. However, overusing the abdominal muscles can lead to unnecessary issues that can affect not only the torso but the surrounding muscles around the torso.
How Trigger Points Are Affecting The Abdomen
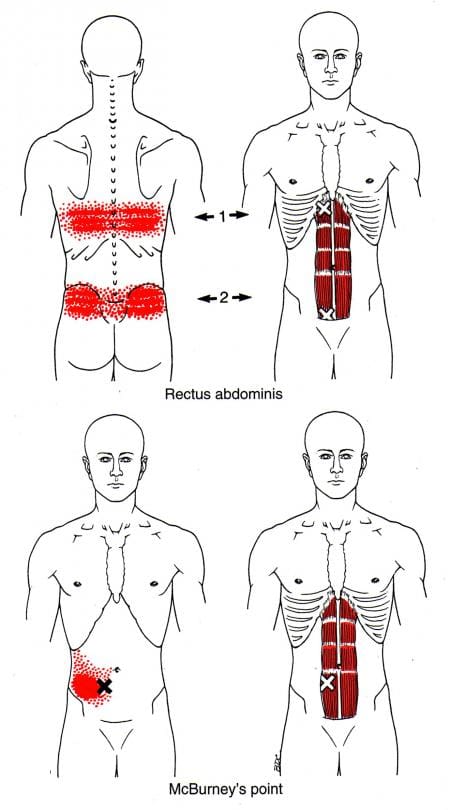
The book “Myofascial Pain and Dysfunction,” by Dr. Janet Travell, M.D., mentioned that abdominal symptoms are common and can cause diagnostic confusion for many people. Since the abdominal muscles can provide stability to the body’s trunk when a person overuses the abdominal muscles through various activities like quick and violent twisting of the mid-section, lifting heavy objects with the core instead of the legs, overdoing exercise regimes, or having a persistent cough, these various activities could potentially lead to the development of trigger points in the abdominal muscles causing pain in the abdomen and causing referred pain to the lower back. Studies reveal that trigger points along the abdominal muscles are developed through aggravating factors like prolonged sitting or standing can cause the abdominal muscles to become extremely tender and hyperirritable along the taut muscle bands. When trigger points affect the abdominal muscles, they can produce referred abdominal pain and visceral disorders (somato-visceral effects) that work closely together to mimic visceral diseases. This pertains to many individuals thinking something is wrong in their gut system, but their abdominal muscles are causing issues in their bodies.
Releasing Trigger Points In The Abdominal Muscles-Video
Have you been experiencing abdominal issues around your torso? Does it hurt when you laugh, cough, or sneeze? Do you feel muscle stiffness or tenderness along your abdominals? If you have been dealing with these symptoms throughout your life, you could be experiencing abdominal pain associated with trigger points in your torso. Abdominal pain is common for many individuals and can vary from gut issues or muscle issues that various factors can cause in the torso. Abdominal issues can even cause confusion to doctors when they are diagnosing the issues that are affecting their patients. When various actions cause pain to the abdominals, it can develop referred pain associated with trigger points. Trigger points develop when the muscle has been overused, creating tiny nodules in the taut band. Trigger points can be tricky to pinpoint but are treatable. The video above shows where the trigger points are located in the abdominal muscles and how to release them from the affected abdominal muscles to provide relief and reduce the mimic effects of visceral-somatic pain.
Managing Trigger Points Associated With Abdominal Pain Through Various Treatments
When abdominal pain affects the muscles, the symptoms can develop trigger points. When this happens, it can lead to confusion and often misdiagnosed. All is not lost; there are ways to manage trigger points associated with abdominal pain through various treatments. Studies reveal that various therapies like dry needling combined with palpations can reduce trigger points from causing more referred pain issues in the abdomen. Other ways to prevent trigger points from developing in the future are through exercises that can help strengthen the abdominal muscles. Exercises like abdominal breathing, pelvic tilts, sit-ups, and even laughter can help strengthen weak abdominal muscles and positively affect the body.
Conclusion
The torso has various muscles, known as abdominal muscles, that help protect the vital organs in the gut system, help stabilize the spinal column, and maintain good posture for many individuals. Various factors affecting the abdominal muscles can lead to a confusing diagnosis, as it could be an internal or external issue. When the abdominal muscles are affected by being overused through various activities, it can develop into trigger points in the muscles, causing visceral referred pain to the torso and cause muscle weakness. Luckily multiple treatments can help reduce the effects of trigger points associated with abdominal pain and can help strengthen the core of the body. This allows the individual to feel better and consider what not to do to their abdominals.
References
Balyan, Rohit, et al. “Abdominal Wall Myofascial Pain: Still an Unrecognized Clinical Entity.” The Korean Journal of Pain, The Korean Pain Society, Oct. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5665744/.
Rajkannan, Pandurangan, and Rajagopalan Vijayaraghavan. “Dry Needling in Chronic Abdominal Wall Pain of Uncertain Origin.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, Jan. 2019, https://pubmed.ncbi.nlm.nih.gov/30691770/.
Seeras, Kevin, et al. “Anatomy, Abdomen and Pelvis, Anterolateral Abdominal Wall.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK525975/.
Tesh, K M, et al. “The Abdominal Muscles and Vertebral Stability.” Spine, U.S. National Library of Medicine, June 1987, https://pubmed.ncbi.nlm.nih.gov/2957802/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
Many individuals don’t realize that the various muscles in their back help provide functionality to the body. The back muscles help move, bend, rotate, and help the individual stand up straight when they are out and about. The back muscles also help protect the cervical, thoracic, and lumbar sections of the spine and work together with the head, neck, shoulders, arms, and legs to provide mobility. When the body begins to wear down with age naturally, it can lead to back issues that can limit a person’s mobility, or normal activities can cause the back muscles to be overused and develop trigger points to invoke back pain or lumbago. Today’s article looks at the thoracolumbar paraspinal muscles in the back, how the lumbago is associated with trigger points, and treatments to relieve the lumbago in the thoracolumbar muscles. We refer patients to certified providers who provide different techniques in thoracic lumbar back pain therapies associated with trigger points to aid many suffering from pain-like symptoms along the thoracolumbar paraspinal muscles along the back, causing lumbago. We encourage patients by referring them to our associated medical providers based on their examination when it is appropriate. We designate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
The Thoracolumbar Paraspinal Muscles In The Back
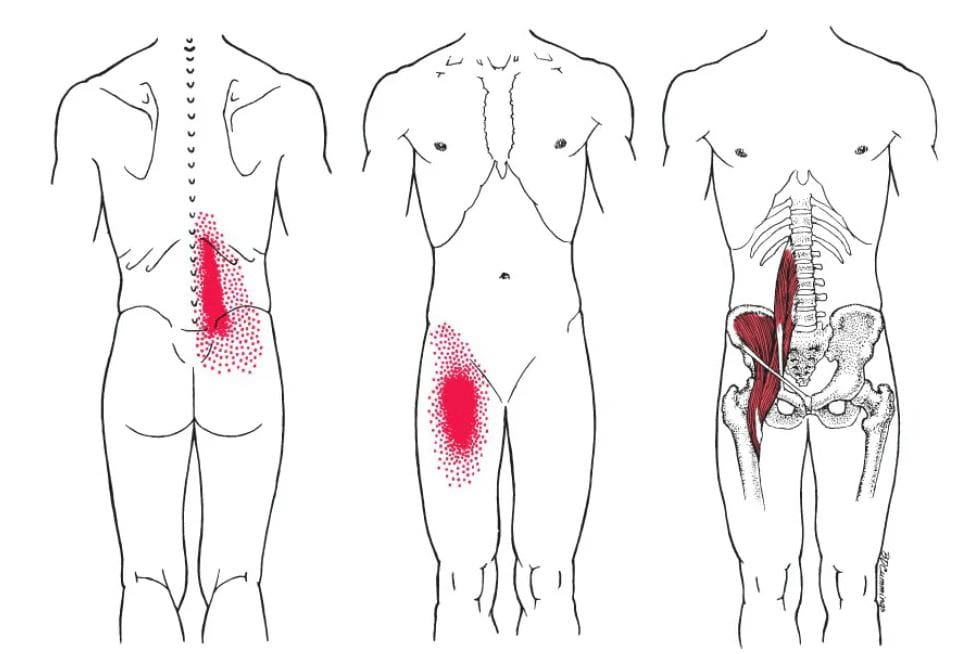
Have you been finding it difficult to walk even for a short period? Do you feel aches and soreness when getting out of bed? Are you constantly in pain when bending over to pick up items from the ground? These various actions that you are doing incorporate the thoracolumbar paraspinal muscle in the back, and when issues affect these muscles, it can lead to lumbago associated with trigger points. The thoracolumbar paraspinal in the back is a group of muscles closely surrounded by the thoracolumbar spine, where the thoracic region ends, and the lumbar region begins. The thoracolumbar paraspinal muscles in the back have a casual relationship with the body as it requires contribution from the systems requiring movement. Studies reveal that the thoracolumbar paraspinal muscles are modulated through communication with the three sub-systems, which include:
The passive system: vertebrae, discs, and ligaments
The active system: muscles and tendons
The control system: central nervous system and nerves
Each system provides muscular activities when a person is bending down to pick up an object or doing simple movements. However, when the muscles become overused, it can lead to various issues affecting the back and surrounding muscles.
Lumbago Associated With Trigger Points
Studies reveal that paraspinal muscle integrity plays a very critical role when it comes to the maintenance of spinal alignment in the back. When the thoracolumbar paraspinal muscles become overused from normal activities, it can affect the back by causing back pain symptoms or lumbago associated with trigger points. In Dr. Travell, M.D.’s book “Myofascial Pain and Dysfunction,” trigger points may be activated due to sudden movements or sustained muscular contraction over time that leads to the development of lumbago. Atrophy issues in the paraspinal muscles can contribute to lumbago associated with trigger points that cause deep referred pain in the thoracolumbar regions of the back. Active trigger points in the deep muscle group of the thoracolumbar paraspinal can impair movement between the vertebrae during flexion or side bending.
An Overview Of Lumbago- Video
Lumbago or back pain is one of the most common issues that many individuals, from acute to chronic, depending on how severe the pain is inflicted on the back. Have you been feeling pain in your mid-lower back? Do you feel an electric shock when you run down your leg in a weird position? Or have you felt tenderness in the middle of your back? Experiencing these symptoms could indicate that the thoracolumbar paraspinal muscles are affected by trigger points associated with lumbago. The video explains what lumbago is, the symptoms, and various treatment options to relieve the pain and manage trigger points that are causing the thoracolumbar muscles issues in the back. Many individuals who suffer from lumbago don’t often realize that various factors can affect the surrounding muscles in the thoracolumbar region and mask other previous conditions from which they could suffer. Regarding managing lumbago associated with trigger points, various treatment options can help reduce the pain affecting the thoracolumbar paraspinal muscles while managing trigger points for progressing further in the back.
Treatments To Relieve Lumbago In The Thoracolumbar Muscles
Since lumbago or back pain is a common issue for many people, various treatments can reduce the pain-like symptoms in the thoracolumbar muscles and manage the associated trigger points. Some of the simplest treatments that many individuals can use are to correct how they are standing. Many individuals often lean on one side of their bodies which causes the thoracolumbar paraspinal muscles on the opposite sides to be overloaded. This causes spinal subluxation or misalignment to the thoracolumbar region. Another treatment that many people can incorporate into their daily lives is by going to a chiropractor for a spinal adjustment for the thoracolumbar spine. Studies reveal that chiropractic care combined with physical therapy can relieve the thoracolumbar back while reducing the pain symptoms associated with trigger points by loosening the stiff muscles and causing relief to the back.
Conclusion
The back has various muscles known as the thoracolumbar paraspinal muscles that allow movement and mobility to the body. The back muscles help protect the cervical, thoracic, and lumbar sections of the spine while working with the rest of the body’s components to keep the body stable. When natural aging or actions affect the back muscles, it can lead to various pain issues that can activate trigger points causing lumbago or back pain. Fortunately, some treatments can help alleviate back pain in the thoracolumbar paraspinal muscles while managing trigger points to bring back mobility to the back.
References
Bell, Daniel J. “Paraspinal Muscles: Radiology Reference Article.” Radiopaedia Blog RSS, Radiopaedia.org, 10 July 2021, https://radiopaedia.org/articles/paraspinal-muscles?lang=us.
du Rose, Alister, and Alan Breen. “Relationships between Paraspinal Muscle Activity and Lumbar Inter-Vertebral Range of Motion.” Healthcare (Basel, Switzerland), MDPI, 5 Jan. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4934538/.
He, Kevin, et al. “The Implications of Paraspinal Muscle Atrophy in Low Back Pain, Thoracolumbar Pathology, and Clinical Outcomes after Spine Surgery: A Review of the Literature.” Global Spine Journal, SAGE Publications, Aug. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7359686/.
Khodakarami, Nima. “Treatment of Patients with Low Back Pain: A Comparison of Physical Therapy and Chiropractic Manipulation.” Healthcare (Basel, Switzerland), MDPI, 24 Feb. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7151187/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
As the “backbone” of the body, the thoracic region of the back has various muscles that help support the ribcage and protect the heart and lungs from injuries. The thoracic spine’s main function is providing respiration and maintaining good posture. However, various habits can cause issues to the muscles in the thoracic spine, which leads to upper back pain and the development of trigger points. One of the thoracic muscles affected by trigger points is the serratus posterior inferior muscle. Today’s article looks at the serratus posterior inferior muscle, how trigger points affect the thoracic region of the back, and how to manage thoracic back pain associated with trigger points. We refer patients to certified providers who provide different techniques in thoracic back pain therapies associated with trigger points to aid many suffering from pain-like symptoms along the serratus posterior inferior muscle along the back. We encourage patients by referring them to our associated medical providers based on their examination when it is appropriate. We designate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
What Is The Serratus Posterior Inferior Muscle?
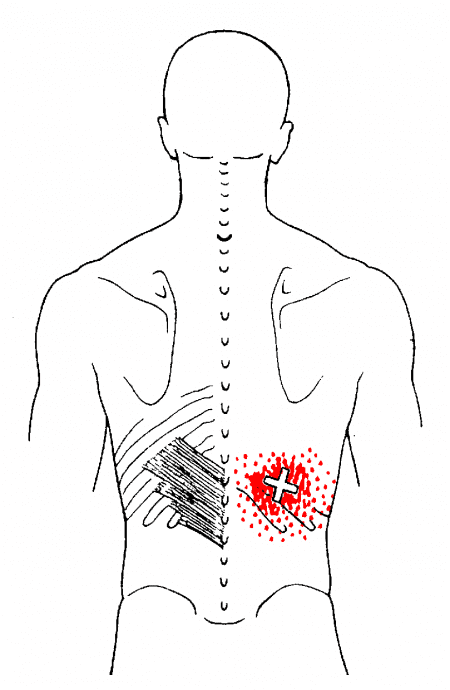
Have you felt aches and pain when bending down to pick something up? What about feeling tenderness near your lower back? Or have you experienced muscle stiffness when stretching? Many of these symptoms are associated with back pain that correlates to overusing the thoracic muscles, which includes the serratus inferior posterior muscles. The serratus posterior muscles (superior and inferior) are accessory breathing muscles as part of the extrinsic muscles. The serratus posterior inferior helps with the chest cavity’s expiration, while the superior help with inspiration. Some of the functionalities that the serratus posterior inferior provides are that in a bilateral action, the inferior works with the superior muscles to reduce the extension of the thoracic vertebrae.
In contrast, the unilateral action for the serratus posterior inferior muscle helps rotate the spine to the opposite sides. Studies reveal that based on the attachment of the serratus, the posterior inferior and superior are generally considered insignificant muscles. Since the serratus posterior muscles help aid respiration to the thoracic region, it can be succumbed to trigger points or myofascial pain syndrome that can affect the thoracic part of the back.
How Trigger Points Affect The Thoracic Region?
When the serratus posterior muscles in the thoracic region are affected by myofascial pain syndrome or trigger points, it correlates to the various activities the person has been doing that cause muscle strain along the serratus inferior posterior muscle. The book, “Myofascial Pain & Dysfunction” explains that when individuals feel a nagging ache in the lower thoracic region of the back, it correlates to residual backache associated with trigger points. Studies reveal that trigger points or myofascial pain syndrome are musculoskeletal pain disorder that affects one or multiple muscles in the body. Since back pain is common, trigger points can cause hyperirritability in the muscle’s taut band due to various factors that can cause strain on the affected muscle. When it comes to the serratus posterior inferior muscle developing active trigger points, it’s due to overload strain from combined movements like lifting, turning, and reaching for items that can also affect the surrounding muscles in the thoracic region of the back.
Trigger Point Of The Week: Serratus Posterior Inferior- Video
Have you been dealing with pain in your upper back in the thoracic region? Do you experience tenderness or soreness near your ribcage? Or have you felt a twinge of pain when turning your torso? Most of these symptoms are common signs that the thoracic region is affected by trigger points along the serratus posterior inferior muscle. The video explains where the serratus posterior inferior is located while pinpointing where the trigger points are located in the thoracic region of the back. Trigger points associated with thoracic back pain mimic other chronic conditions that can cause muscle tension and strain on the upper back. Studies reveal that latent and active trigger points affecting the upper thoracic area muscles can make many individuals feel more pain than they can tolerate. This can affect how a person functions and can make them feel inadequate. However, it is possible to incorporate a variety of treatments to reduce the pain and manage trigger points from progressing further in the thoracic region of the back.
Managing Thoracic Back Pain Associated With Trigger Points
Various treatments are available to reduce the pain affecting the thoracic region of the back and even manage trigger points associated with the serratus posterior inferior muscle. Many individuals often go to a chiropractor to relieve their back pain. Chiropractors utilize their hands and various techniques to manipulate the spine and can even pinpoint where the trigger points affect the multiple muscles in the thoracic region. Chiropractors even work with other pain specialists to devise a treatment procedure to reduce the symptoms while managing thoracic back pain associated with trigger points. Studies reveal that by when pain specialists like chiropractors begin identifying proper treatment strategies for managing thoracic back pain associated with trigger points, it might be able to reduce pain and improve function for many people dealing with thoracic back pain.
Conclusion
The thoracic region of the back has various muscles that help support the ribcage and protect vital organs, which include the heart and the lungs. One of the muscles in the thoracic region is the serratus posterior inferior muscle, an accessory breathing muscle that helps with the chest cavity expiration and helps reduce the extension of the thoracic vertebrae. When the inferior muscle becomes overused by various movements, it can develop trigger points along the inferior muscle, causing thoracic back pain. Trigger points along the serratus inferior posterior muscles can mimic other chronic conditions that can cause symptoms of muscle tension and strain on the upper back. Luckily, various treatments have been available to reduce pain symptoms and manage thoracic back pain associated with trigger points. These treatments can bring back mobility to the thoracic region of the back without the individual being in pain.
References
Chen, Chee Kean, and Abd Jalil Nizar. “Myofascial Pain Syndrome in Chronic Back Pain Patients.” The Korean Journal of Pain, The Korean Pain Society, June 2011, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3111556/.
Dor, Adi, et al. “Proximal Myofascial Pain in Patients with Distal Complex Regional Pain Syndrome of the Upper Limb.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, July 2019, https://pubmed.ncbi.nlm.nih.gov/31563368/.
Mitchell, Brittney, et al. “Anatomy, Back, Extrinsic Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 Aug. 2022, https://www.ncbi.nlm.nih.gov/books/NBK537216/.
Ortega-Santiago, Ricardo, et al. “Widespread Pressure Pain Sensitivity and Referred Pain from Trigger Points in Patients with Upper Thoracic Spine Pain.” Pain Medicine (Malden, Mass.), U.S. National Library of Medicine, 1 July 2019, https://pubmed.ncbi.nlm.nih.gov/30821833/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
Vilensky , J A, et al. “Serratus Posterior Muscles: Anatomy, Clinical Relevance, and Function.” Clinical Anatomy (New York, N.Y.), U.S. National Library of Medicine, July 2001, https://pubmed.ncbi.nlm.nih.gov/11424195/.
The upper body works because it provides stability for the body and motor-sensory functions to the arms, neck, shoulders, and chest. The muscles surrounding each body section have different roles and outputs that have specific jobs for body functionality. For the chest body area, the various muscles are there to support the shoulders and arms while protecting the chest cavity and the internal organs inside. Some of the different chest muscles even support the internal organs and the rest of the muscles. One of those muscles is known as the serratus anterior muscle. Today’s article looks at this muscle, how trigger points affect the serratus anterior muscle, and various actions to manage trigger points along the serratus anterior. We refer patients to certified providers who provide different techniques in pain therapies associated with trigger points to aid many suffering from pain-like symptoms along the serratus anterior muscle along the ribcage. We encourage patients by referring them to our associated medical providers based on their examination when it is appropriate. We designate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
What Is The Serratus Anterior?
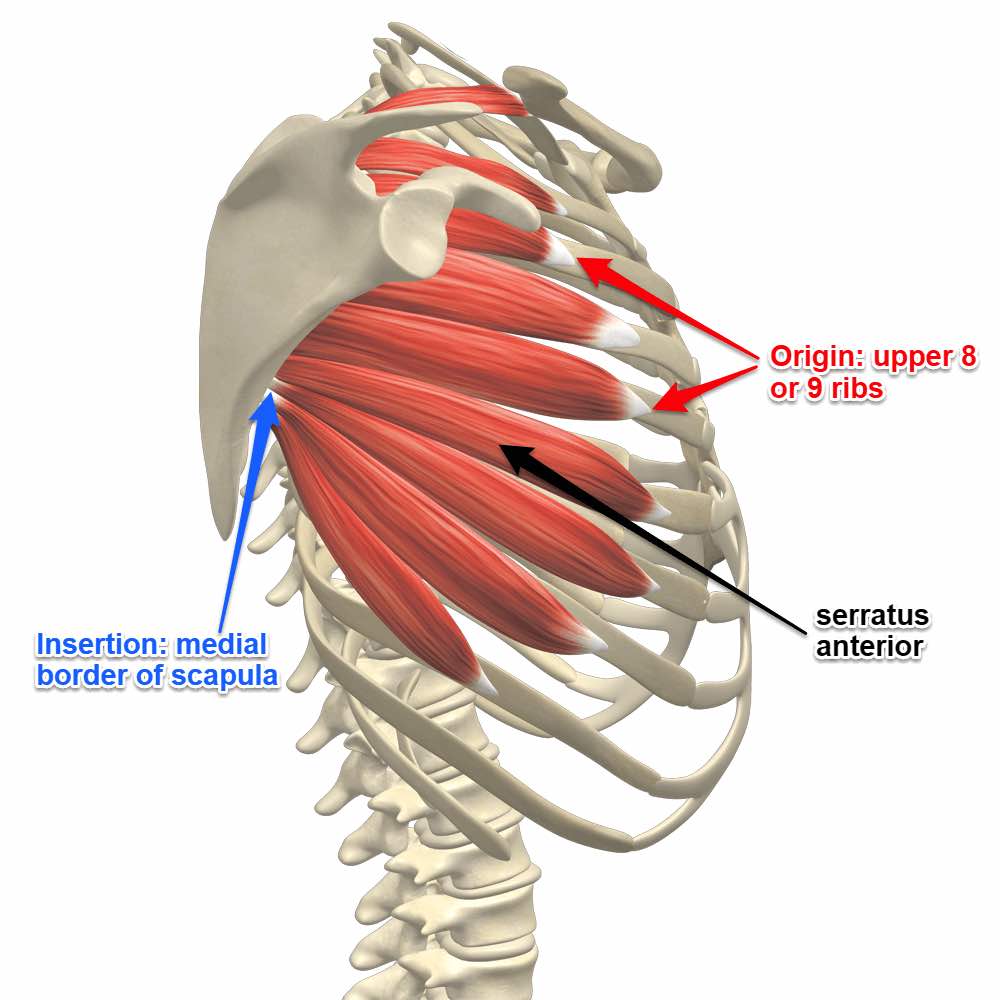
Have you been experiencing pain in your sides? Do you notice that your shoulders feel stiff when rotating backward? Or are you experiencing any cardiovascular disorders that are causing you pain? Pain can come in many forms and affect a person differently, as most of these symptoms are associated with trigger points affecting the serratus anterior muscle along the side of the ribs. The serratus anterior muscles work in the body because this muscle is located deep within the scapula (shoulder blades) and the pectoral muscles. Some of the functions that the serratus anterior provides are that it helps pull the shoulder blades forward around the thorax by allowing anteversion and protraction of the arms.
A great example is when a boxer is throwing a punch. This motor action is done with the long thoracic nerve. The long thoracic nerve originated from the C-5 and C-6 regions of the cervical spine and is the motor nerve for the serratus anterior muscle to allow an anterolateral motion for the shoulder blades that allows arm elevation. Another function of the serratus anterior is that it helps lift the ribs and provide assistance with respiration. The serratus anterior muscle also helps protect the side of the ribcage.
Trigger Points Affecting The Anterior Serratus Muscle
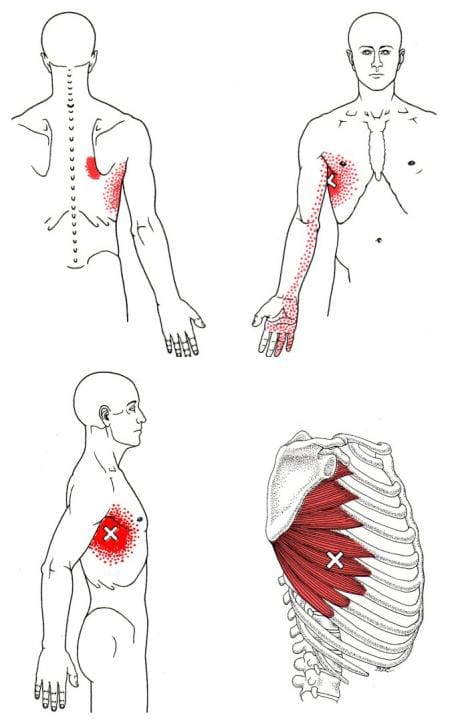
The serratus anterior muscle and the long thoracic nerve work hand-in-hand to provide motor function to the arms but can succumb to various injuries that can cause the development of trigger points or myofascial pain syndrome in the anterior serratus muscle. According to Dr. Travell, M.D.’s book, “Myofascial Pain & Dysfunction,” trigger points may be activated when the serratus anterior muscle has been overused and strained from excessive exercises like prolonged running, pushups, or heavy weight lifting or even extreme coughing from respiratory diseases. Other studies reveal that trigger points affecting the serratus anterior muscle can cause radiating pain along the anterior chest wall that can mimic radiculopathy and often be confused with chronic mechanical neck pain, instability in the glenohumeral, and even shoulder impingement syndrome. Trigger points are often difficult to diagnose due to the referred pain in the affected muscle. The various factors that contribute to the development of trigger points can be simple, like an overused muscle or even a slightly poor posture stance that can cause an imbalance in the body.
Trigger Point Release On The Serratus Anterior- Video
Have you been dealing with pain in the side of your ribs? What about experiencing stiffness or pain when throwing a punch? Do you feel any aches or soreness when adjusting your posture? These symptoms you are experiencing could contribute to the development of trigger points affecting the serratus anterior muscle. The serratus anterior covers the side of the ribcage and lies deep within the scapula and pectoral muscle. This muscle allows the motor function to the arms as it pulls the scapula forward around the thorax when someone throws a punch. However, when the muscle is overused, it can develop trigger points along the serratus anterior muscle and mimic chronic issues in the chest cavity. This causes referred pain to travel from the side of the ribs down to the hand, causing pain-like symptoms to the ring and pinky fingers. Fortunately, various treatments help manage trigger points in the serratus anterior muscle. The video above shows where the trigger points are located in the serratus anterior and how to release the trigger points from the affected muscle to relieve the pain and manage trigger points from returning to the muscle.
Various Actions To Manage Trigger Points Along The Serratus Anterior
When the serratus anterior is affected by trigger points, many people will often feel pain along their sides and complain about their chest hurting for an unknown reason. When this happens, they would be referred to a pain specialist like a chiropractor or a massage therapist to manage trigger points associated with the serratus anterior through various techniques. Studies reveal that techniques like intramuscular neural distribution of the serratus anterior muscle can help reduce the effects of trigger points in the affected muscle to reduce pain-like symptoms. Other methods like thoracic spinal manipulation, dry-needling, acupuncture, or stretching the muscle group can help loosen the stiff muscles and lower trigger points from forming. However, other actions that many people should consider are modifying or avoiding strenuous activities that can reactivate the serratus anterior muscle trigger points. Even when the person is sleeping, putting a pillow under to support the arm can prevent the scapula from falling forward.
Conclusion
The serratus anterior muscle is located at the side of the ribs and is deep within the scapula (the shoulder blades) and the poster muscles. The serratus anterior muscle works with the long thoracic nerve by providing motor function to the arms by allowing anterolateral motion. This allows the individual to throw a punch in a boxing match while lifting the ribs and assisting with respiration. When the serratus anterior muscle succumbs to injuries or has been overused, it can develop into trigger points and cause various issues affecting the body’s chest cavity. Trigger points are treatable through multiple therapies that can manage trigger points while reducing the pain effects rendered in the serratus anterior muscles. These therapies return mobility and motor function to the arms and the serratus anterior muscles.
References
Bautista, Alexander, et al. “Serratus Anterior Muscle Pain Syndrome: A Diagnostic Conundrum.” OUP Academic, Oxford University Press, 11 Feb. 2017, https://academic.oup.com/painmedicine/article/18/8/1600/2990174?login=false.
Long, Kirsten, and Forshing Lui. “Anatomy, Thorax, Long Thoracic Nerve.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 31 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK535396/.
The body’s ability to heal itself is quite remarkable. When injury or illness presents, the body’s systems activate to deal with the problem and restore itself to health. The spine’s bones protect the communication pathways of the spinal cord and nerve roots. If the nervous system suffers injury or is damaged in some way, causing impairment, it can cause malfunctioning of the tissues and organs throughout the body. Chiropractic care combined with functional medicine can restore and enhance the body’s self-healing abilities to optimal levels.
The Body’s Ability To Heal Itself
A healthy body regenerates, fights infection, heals wounds, and repairs damage. The body is in a constant state of removing damage and producing new, healthy tissues.
Cells can heal themselves when they become unhealthy and replicate to replace injured or damaged cells.
The body produces new cells to heal the damage if a bone gets fractured or broken.
When the skin gets cut, the blood clots, stopping the bleeding, white blood cells remove the injured and dead cells, and new healthy cells repair the damaged tissue.
The immune system deals with viruses, bacteria, and toxins.
Natural destroyer cells recognize when the body’s cells have been invaded by a virus and destroy the infected cell.
Inflammation
Inflammation is the body’s reaction to an injury or infection, activating the immune system to restore the injured or infected area to health.
A fever is the body’s raising its temperature to levels that will kill viruses and bacteria.
The elevation in temperature also triggers certain cellular mechanisms which help the body fight the infection.
Stem Cells
The body heals and regenerates itself through stem cells.
Once the body is formed, embryonic stem cells disappear, and adult stem cells take over.
The adult stem cells divide, producing an identical stem cell and a healthy, mature cell of a specific type.
Each type of adult stem cell only can become certain types of tissue.
For example, Mesenchymal Stem Cells can regenerate bone, fat, muscle, and cartilage cells.
Neural Stem Cells help regenerate nerve tissue in the brain and spinal cord.
Epithelial Stem Cells regenerate skin.
Adult stem cells can reproduce for a long time but eventually stop reproducing as efficiently.
Nervous System
The nervous system assists the whole body in maintaining communication, using electrical and chemical impulses to send and receive messages. The system reacts to changes inside and outside the body. Infections, injuries, disorders, and conditions can cause imbalances causing communication problems that can lead to health issues. Common problems of the nervous system include:
Sciatica – Pressure on a nerve/s caused by a slipped, bulging, or herniated disc in the spine or arthritis of the spine and, sometimes, other factors.
Parkinson’s disease – The death of neurons in a part of the brain called the midbrain. Symptoms include shaking and mobility problems.
Epilepsy – Abnormal electrical activity in the brain causing seizures.
Meningitis – Inflammation of the membrane covering the brain.
Multiple sclerosis – The myelin sheaths protecting the nerves of the central nervous system become damaged and deteriorates.
Chiropractic Care
Subluxations are misaligned or damaged joints that are not functioning correctly. These joints can place pressure on a nerve, which interferes with the normal nervous system function. Chiropractic care can realign, restore and maintain neuromusculoskeletal system health to reactivate the body’s natural healing abilities.
Cerebral Palsy Chiropractic Treatment
References
Haavik, Heidi, et al. “Effects of 12 Weeks of Chiropractic Care on Central Integration of Dual Somatosensory Input in Chronic Pain Patients: A Preliminary Study.” Journal of manipulative and physiological therapeutics vol. 40,3 (2017): 127-138. doi:10.1016/j.jmpt.2016.10.002
Lee, Courtney, et al. “Mind-body therapies for the self-management of chronic pain symptoms.” Pain medicine (Malden, Mass.) vol. 15 Suppl 1 (2014): S21-39. doi:10.1111/pme.12383
Maltese PE, Michelini S, Baronio M, Bertelli M. Molecular foundations of chiropractic therapy. Acta Biomed. 2019 Sep 30;90(10-S):93-102. doi: 10.23750/abm.v90i10-S.8768. PMID: 31577263; PMCID: PMC7233649.
McSwan, Joyce, et al. “Self-Healing: A Concept for Musculoskeletal Body Pain Management – Scientific Evidence and Mode of Action.” Journal of pain research vol. 14 2943-2958. 21 Sep. 2021, doi:10.2147/JPR.S321037
Navid, Muhammad Samran et al. “The effects of chiropractic spinal manipulation on central processing of tonic pain – a pilot study using standardized low-resolution brain electromagnetic tomography (sLORETA).” Scientific reports vol. 9,1 6925. 6 May. 2019, doi:10.1038/s41598-019-42984-3
The upper back is part of the thoracic region of the spine, surrounded by various muscles that protect the thoracic joints and help assist with respiratory functionality for the lungs. The upper back muscles consist of the rhomboids and the trapezoid muscles that provide functionality to the scapula or shoulder blades. Other superficial muscles offer assistance to the thoracic spine. The serratus posterior muscle is one of the superficial muscles that helps the thoracic spine and, like all superficial muscles, can succumb to injuries that can lead to the development of overlapping referred pain symptoms known as trigger points. Today’s article focuses on the serratus posterior muscle function in the back, how trigger points are causing upper back pain, and various techniques to manage trigger points in the upper back. We refer patients to certified providers who are diverse in upper back pain therapies to aid many people suffering from myofascial pain syndrome or trigger points associated with the serratus posterior muscle along the upper back. We advised patients by referring them to our associated medical providers based on their examination when appropriate. We indicate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
The Serratus Posterior Muscle Function In The Back
Have you been dealing with constant upper back pain? Do you feel soreness at the base of your neck? Or are you having difficulty breathing? Most of the symptoms cause pain in the serratus posterior muscles that can lead to the development of myofascial pain syndrome or trigger points along the upper back. The serratus posterior has various roles in the upper back as it is not only part of the extrinsic muscles but also part of the accessory breathing muscle. The serratus posterior muscle helps with inspiration, which causes the chest cavity to expand as it is a superficial muscle attached to the ribs and is less commonly known. Studies show that the serratus posterior muscle is deep within the rhomboid muscles and is superficial. Even though this muscle is superficial when it has been overused through various activities, that can cause hypertrophy in the accessory respiratory muscles. Additional studies reveal that the serratus posterior superior muscle is considered clinically insignificant but has been impaired by myofascial pain syndrome or trigger points that can lead to upper back pain.
Trigger Points Causing Upper Back Pain
As stated earlier, the upper back is part of the thoracic region of the spine, and when various factors begin to affect the body, the back muscles tend to be involved. Studies reveal numerous sources of spinal pain in the thoracic spine. One is a myofascial pain syndrome affecting the serratus posterior muscles causing referred upper back pain. Myofascial pain syndrome or trigger points can be activated when the serratus posterior muscle is overloaded from thoracic respiratory issues like coughing due to pneumonia, asthma, or chronic emphysema. When respiratory problems affect the muscles in the thoracic region of the back, it leads to the development of trigger points, leading to overlapping issues like referred pain, motor dysfunction, and autonomic phenomena. According to Dr. Travell, M.D., in the upper back, trigger points can make the serratus posterior muscle cause overlapping risk profiles along the shoulder blades and have referred pain travel to the hands. This can make many individuals suffer from serious pain-like symptoms, causing them to be miserable.
Releasing Trigger Points Related Tension In The Upper Back-Video
Have you been dealing with respiratory issues causing you to be hunched over constantly? Do you feel soreness or tenderness at the base of your neck? Or are you suffering from upper back pain? These symptoms are associated with trigger points that are affecting the serratus posterior muscles causing upper back pain. Trigger points, or myofascial pain syndrome, is a musculoskeletal disorder that causes tenderness along the affected muscle that causes referred pain to the surrounding muscles in the body. Trigger points associated with the serratus posterior muscles can cause referred pain in the upper back and mimic various chronic conditions. Trigger point pain is difficult to diagnose but can be manageable with treatment. The video above gives examples of how to treat trigger points to relieve tension in the upper back.
Various Techniques To Manage Trigger Points In The Upper Back
When it comes to upper back pain, many individuals will go to pain specialists like massage therapists or chiropractors to relieve any issues affecting the upper back. These pain specialists utilize various techniques like stretching, spinal manipulation, massages, and ischemic compression to alleviate pain and manage trigger points from forming further in the affected muscle. Pain specialists like massage therapists or chiropractors are excellent for locating pain-like symptoms associated with trigger points. Even though treatment can help manage symptoms associated with trigger points, many people can still incorporate these techniques, like deep breathing or correcting their posture, to prevent the upper back muscles from becoming strained and causing more issues than before.
Conclusion
The serratus posterior muscles have various roles in the upper back region of the body. These superficial muscles are extrinsic and accessory breathing muscles that help expand the chest cavity. When multiple issues affect the upper back muscles, like strenuous activities or respiratory problems, it can develop trigger points along the serratus posterior muscles and invoke pain-like symptoms to travel down to the hand, causing mobility issues. Thankfully, various techniques that pain specialists like chiropractors and massage therapists use can help manage trigger points from escalating and can bring upper back mobility to the body once again.
References
Altafulla, Juan J, et al. “An Unusual Back Muscle Identified Bilaterally: Case Report.” Cureus, Cureus, 15 June 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6093753/.
Briggs, Andrew M, et al. “Thoracic Spine Pain in the General Population: Prevalence, Incidence and Associated Factors in Children, Adolescents and Adults. A Systematic Review.” BMC Musculoskeletal Disorders, BioMed Central, 29 June 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2720379/.
Mitchell, Brittney, et al. “Anatomy, Back, Extrinsic Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 4 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK537216/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
Vilensky, J A, et al. “Serratus Posterior Muscles: Anatomy, Clinical Relevance, and Function.” Clinical Anatomy (New York, N.Y.), U.S. National Library of Medicine, July 2001, https://pubmed.ncbi.nlm.nih.gov/11424195/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine