Constipation is a leading cause of low back pain in America and can cause a chain reaction in the rest of the body. When the digestional tract swells, it generates added stress on the back and surrounding nerves. Prolonged constipation and pressure can cause sciatica symptoms. Constipation sciatica can be relieved through chiropractic treatment, therapeutic massage, non-surgical spinal decompression, and functional medicine to alleviate symptoms and restore optimal body function.
Constipation Sciatica
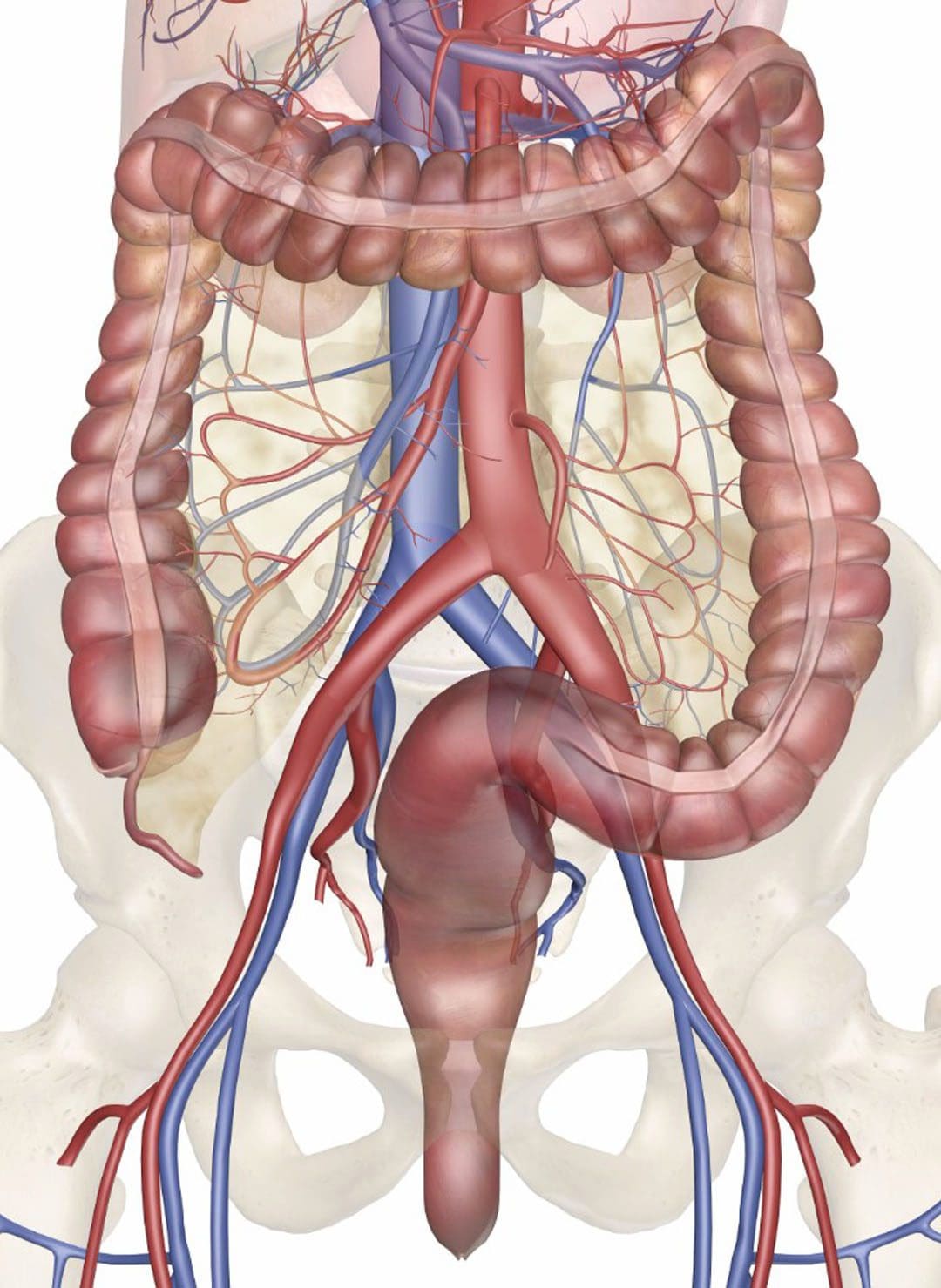
Sciatica is irritation, compression, and inflammation of the sciatic nerve, which supplies the thighs, lower legs, and feet. It is usually caused by a pinched/compressed of one or more spinal nerve roots between the vertebrae of the lower back. The buildup of stool in the intestines can cause a dull aching sensation in the low back that can radiate to surrounding areas. Common causes of constipation include:
Bowel movements vary for everyone, and not having a movement daily does not mean constipation is occurring. Some individuals have only three movements a week, while others have multiple movements daily. A recommended indicator of constipation is if there has been a sudden decrease in typical bowel movements. The digestive tract occupies a significant region of the lower torso. Back pain symptoms can present after the rectum becomes obstructed or stools have solidified in the colon. Once constipation has developed, the blockage presses against the nerves and muscles of the back. This causes a range of discomfort signaling by the brain, which worsens as the backup grows. Symptoms of general constipation include:
Feeling full despite not eating anything.
Bloating.
Swelling.
Abdominal cramping.
Infrequent bowel movements.
Discomfort or aching when trying to pass a stool.
Hard and/or lumpy stool.
Constipation is considered chronic when two or more of the following symptoms occur for at least three months:
Further decreased bowel movements.
Straining to defecate.
Stools do not loosen without the use of laxatives.
Passage of hard pebble/pellet stools.
Consistent abdominal pain that is relieved by even slight movement.
Feeling as if the bowels are not fully emptied or a blockage in the rectum.
Feeling the need to assist the release by pressing on the abdomen.
Chiropractic Treatment
Chiropractic treatment can realign the spine, release compressed nerves, increase the frequency of bowel movements, and through the massage and relaxation of the muscles, help to soften stools. Intestinal muscles push the stool to the anus, where it leaves/evacuates the body. Special nerve cells in the intestine, known as ganglion cells,innervate the muscles to push. These nerves connect to the celiac ganglion, which connects to the spinal cord through nerve roots that exit the spine in the lower thoracic and upper lumbar region. The celiac ganglion innervates the liver, stomach, gallbladder, spleen, kidneys, small intestine, and the ascending and transverse colon. Treatment for constipation and back pain depends on the cause of the symptoms. For example, if the constipation is caused by dehydration, a chiropractor will instruct the patient on water intake as part of the personalized treatment plan.
Diagnosis to Recovery
References
Fernandes, Walkyria Vilas Boas, et al. “The effect of a six-week osteopathic visceral manipulation in patients with non-specific chronic low back pain and functional constipation: study protocol for a randomized controlled trial.” Trials vol. 19,1 151. 2 Mar. 2018, doi:10.1186/s13063-018-2532-8
Panarese, Alba, et al. “Chronic functional constipation is strongly linked to vitamin D deficiency.” World journal of gastroenterology vol. 25,14 (2019): 1729-1740. doi:10.3748/wjg.v25.i14.1729
Rédly, Monika. “The effects of chiropractic care on a patient with chronic constipation.” The Journal of the Canadian Chiropractic Association vol. 45,3 (2001): 185–191.
Trager, Robert James, et al. “Association between radicular low back pain and constipation: a retrospective cohort study using a real-world national database.” Pain reports vol. 6,3 e954. 26 Aug. 2021, doi:10.1097/PR9.0000000000000954
The buttock and the lower back have a casual relationship to the body, as the lower back has various muscles and nerves surrounding the spinal column. In contrast, the buttock region has multiple muscles and the sciatic nerve to keep the body upright. The sciatic nerve travels from the lumbar region of the spine across the gluteus muscles and down to the legs. The gluteus muscles include the Maximus, medius, and minimus, and they work with the sciatic nerve regarding good posture. When normal or traumatic factors begin to affect the body, like sciatica or poor posture, it can lead to developing trigger points associated with the gluteus minimus affecting the sciatic nerve. Today’s article examines the gluteus minimus, how trigger points mimic sciatic pain on the gluteus minimus, and various treatments to relieve sciatic nerve pain. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like sciatic pain treatments related to trigger points, to aid individuals dealing with pain symptoms along the gluteus medius muscles associated with sciatica. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Gluteus Minimus?
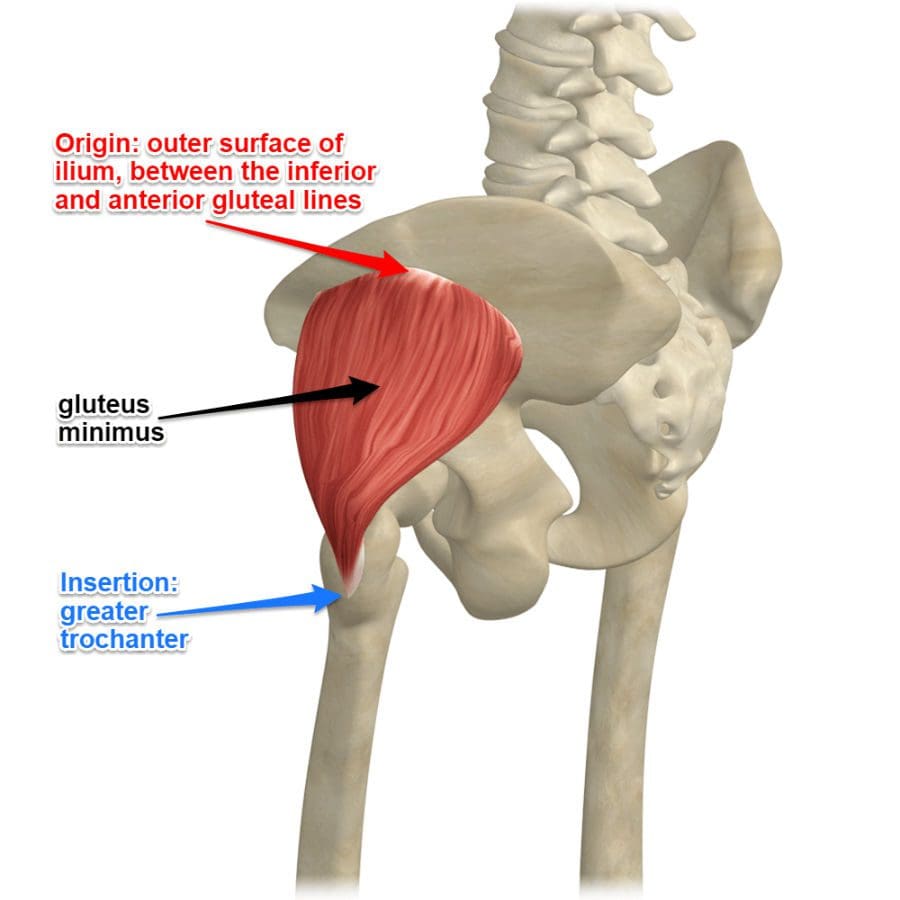
Have you been experiencing radiating pain traveling down to your leg? Do you have difficulty walking or sitting down? Do you feel tenderness or referred pain near your buttock region? Some of the issues correlate with trigger points affecting the gluteus minimus, causing pain in the sciatic nerve. As the smallest muscle in the gluteal region of the buttock, the gluteus minimus shares similar characteristics to the gluteus medius while being located beneath the medius muscle. One of the primary functions of the gluteus minimus is that it predominantly acts as a hip stabilizer and abductor. The nerves from the gluteal muscles include the sciatic nerve, which is on top of the gluteus muscles and the other nerves help supply the muscles to function in the posterior region of the body. Studies reveal that the structural integrity of the gluteus minimus muscles is the key to the lateral hip muscle, which contributes to pelvic stability and lower extremity function. However, when issues affect the gluteal muscles’ posterior region could trigger point pain mimicking sciatica.
How Trigger Points Mimic Sciatic Pain On The Gluteus Minimus?
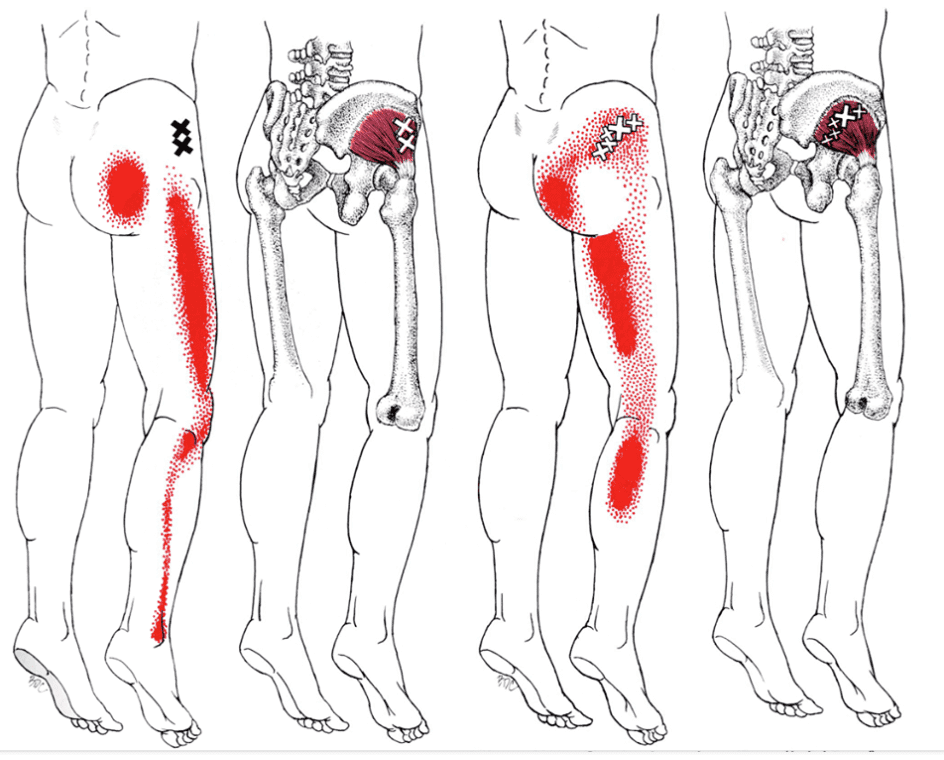
When the lower body extremities begin to suffer from multiple issues that cause the individual to have mobility dysfunction, various factors could correlate to the dysfunction. When the gluteus minimus muscles have been overused or been through a traumatic experience, they can develop trigger points along the muscle fibers and even cause nerve entrapment along the sciatic nerve. Trigger points along the gluteus minimus can mimic sciatic nerve pain down to the back or even the side of the legs that causes excruciating and deep pain in the posterior region. Studies reveal that pain in the buttock region is a deep gluteal syndrome caused by non-discogenic pain that causes sciatic nerve entrapment.
The book, “Myofascial Pain and Dysfunction,” written by Dr. Janet G. Travell, M.D., states that many patients with active trigger points located in their gluteus minimus would complain about hip pain that could cause them to limp-walk when they are going to places. The pain caused by the active trigger points can make it difficult to stand up from a seated position due to the painful movements. The associated pain that the trigger points are causing to the gluteus minimus can be constant and excruciating; even small stretches can not alleviate the pain. The book also mentioned that trigger points could cause referred pain to the gluteus minimus that can cause various somato-visceral issues to the hips, legs, and knees if the pain worsens.
Sciatic Type Pain: Gluteus Minimus Trigger Points- Video
Are you dealing with pain in your hips, low back, and legs? Do you find it difficult to walk or stand up constantly? Or are you experiencing sciatic nerve pain that is radiating down your leg? All these pain-like symptoms are associated with trigger points along the gluteus minimus affecting the sciatic nerve. The gluteus minimus is the smallest of the gluteal muscles with the same function as the gluteus medius and predominately acts as the hip’s stabilizer and abductor. When the gluteus minimus muscles have been overused from traumatic events or normal factors, they can develop trigger points in the muscle fibers, entrap the sciatic nerve and irritate the nerve causing sciatica. The video above explain where the gluteus minimus is located and pinpoints where the trigger points are in the muscle fibers. Trigger points along the gluteus minimus can mimic sciatica by causing referred pain to travel down the leg. This can cause the individual to be unable to walk or even stand up due to the excruciating pain that they are in. Luckily, trigger points are treatable even though they are tricky to diagnose.
Various Treatments To Release Sciatic Nerve Pain
Even though trigger points along the gluteus minimus are tricky to diagnose, they are treatable through various treatments to alleviate the pain that the person is experiencing and can reduce sciatic nerve pain from causing more issues in the legs. Studies reveal that the effectiveness of active soft tissue release and trigger point block treatments combined can release entrapped nerves from the gluteus minimus and reduce low back and sciatic pain from the lower extremities. Now the treatments alone can only do so much to the individual, as many doctors tell their patients to take corrective actions or techniques to reduce the chances of trigger points from forming again on the gluteus minimus. Techniques like glute stretches, ischemic compressions, or using a foam roller can break the myofascial triggers from the gluteus minimus muscles and reduce the pain in the glutes and legs. This will help bring mobility back to the lower extremities.
Conclusion
As the smallest muscle in the body’s gluteal region, the gluteus minimus is the lower body’s predominant hip stabilizer and abductor. The gluteus minimus contributes to pelvic stability and lower extremity functionality that can be overused and can develop trigger points associated with sciatica. Trigger points along the gluteus minimus can cause referred pain to the legs and lower back while mimicking sciatic nerve pain. Thankfully various treatments and techniques can help reduce the chances of trigger points forming along the gluteus minimus and release nerve entrapment from the aggravated muscles pressing on the sciatic nerve, bringing back lower extremity mobility to the body.
References
Greco, Anthony J, and Renato C Vilella. “Anatomy, Bony Pelvis and Lower Limb, Gluteus Minimus Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 29 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK556144/.
Kameda, Masahiro, and Hideyuki Tanimae. “Effectiveness of Active Soft Tissue Release and Trigger Point Block for the Diagnosis and Treatment of Low Back and Leg Pain of Predominantly Gluteus Medius Origin: A Report of 115 Cases.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6382483/.
Martin, Hal David, et al. “Deep Gluteal Syndrome.” Journal of Hip Preservation Surgery, Oxford University Press, July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4718497/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Whiler, Lisa, et al. “Gluteus Medius and Minimus Muscle Structure, Strength, and Function in Healthy Adults: Brief Report.” Physiotherapy Canada. Physiotherapie Canada, University of Toronto Press, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5963550/.
Many individuals deal with sciatic nerve discomfort and pain that radiates from the lower back down through the glutes, legs, and feet. It can affect anyone and be challenging to deal with because it can be sudden and unpredictable. A professional hands-on therapeutic massage can play a vital role in alleviating back and sciatic pain but is not always available. This is when a quality massage chair can provide pain relief and relaxation at home.
Sciatica
Not everyone who has sciatica will have the same symptoms. But common symptoms include:
Tingling, numbing sensations in the lower back and down the leg.
Electrical sensations running down the leg.
Lower back pain that spreads into the buttocks, thighs, calves, and feet.
Pain may be described as mild, dull, achy, and sharp.
Sneezing or coughing can increase the pain.
Weakness in the leg.
Massage Chair
A massage chair can assist with sciatic pain by soothing tense muscles and relieving the pressure on the surrounding tissues. When the back muscles are tense, they contract and compress down on the nerves, including the sciatic nerve. Massaging the tight muscles minimizes the pressure on the sciatic nerve and helps alleviate pain. Research has shown the main reasons why massage is beneficial:
Improves Circulation
Massaging the muscles increases blood flow.
Increasing blood circulation facilitates the absorption of nutrients into the muscles and tissues.
Choosing one will be based on specific needs and budget. Some tips to help figure out which is the most beneficial massage chair include:
Consult A Doctor
A doctor, spine specialist, or chiropractor can recommend the best type of massage chair for the individual’s specific injury, condition, and/or disorder.
A doctor will inform the individual if a massage chair is a safe option for their sciatica pain if they have health conditions like high blood pressure or neuropathy.
Chair Objectives
Figure out what the chair will help with short and long-term before shopping.
For example, if the goal is to relieve sciatica and lower back tension, an L-Track massage chair can go further down the spine to the glutes and hamstrings.
Injury Medical DOC Spinal Decompression Table
References
Cygańska, Anna, et al.” Impact of Exercises and Chair Massage on Musculoskeletal Pain of Young Musicians” International journal of environmental research and public health vol. 17,14 5128. 16 Jul. 2020, doi:10.3390/ijerph17145128
de Souza, Talita Pavarini Borges et al.”“The effectiveness of Chair Massage on Stress and Pain in Oncology” International journal of therapeutic massage & bodywork vol. 14,3 27-38. 2 Sep. 2021, doi:10.3822/ijtmb.v14i3.619
Hand, Mary et al.” “Massage Chair Sessions: Favorable Effects on Ambulatory Cancer Center Nurse” Perceived Level of Stress, Blood Pressure, and Heart Rate” Clinical journal of oncology nursing vol. 23,4 (2019): 375-381. doi:10.1188/19.CJON.375-381
Kim, Seung-Kook, et al.” “Clinical outcomes and cost-effectiveness of massage chair therapy versus basic physiotherapy in lower back pain patients: A randomized controlled trial.” Medicine vol. 99,12 (2020): e19514. doi:10.1097/MD.0000000000019514
Kumar, Saravana, et al. “The effectiveness of massage therapy for the treatment of nonspecific low back pain: a systematic review of systematic reviews.” International journal of general medicine vol. 6 733-41. 4 Sep. 2013, doi:10.2147/IJGM.S50243
The sciatic nerve is the longest in the body and is the central nerve in the leg. A critical nerve that comes off the spine runs through the pelvis, into the buttocks, down the back of each thigh, and finally into the feet. It is a mixed nerve meaning it is made up of both motor/movement) and sensory/sensation fibers. The nerves merge with the spinal nerve roots before they enter the spinal cord, where the sensory information travels to and from the brain. If the nerve is inflamed, compressed, twisted, damaged, or injured, this can negatively affect the muscles’ function, leading to chronic pain conditions. Injury Medical Function Restoration Chiropractors will do precisely that for the sciatic nerve and the rest of the body.
Nerve Roots and Branches
Different nerve roots make up the sciatic nerve, with two starting in the lower back and three at the bottom of the spine or sacrum. At the knees, the nerve splits into two branches:
The peroneal nerve runs from the knee’s outer part to the foot’s outer part and splits into two main branches below the knee.
The tibial nerve goes down the back of the calf, extending to the heel and sole.
There are smaller branches at the:
Hips
Inner thighs
Calves
Feet
Sciatic Nerve Function
The sciatic nerve’s purpose serves motor functions by assisting the muscles in the legs and feet to move, walk, run, and stand. And for the sensory function of feeling sensations in the legs and feet includes pain, numbness, burning, and electrical sensations.
Motor Functions
The nerve provides motor functions that power movement to the muscles that move the thighs, legs, and feet. Essential motor functions:
Motor function signs of sciatic nerve problems include difficulty or inability to walk, bend the leg, and/or stand on tiptoe or the heel.
Sensory Functions
The nerve provides sensation to the different areas; when the nerve is injured, the corresponding area may feel unique/abnormal sensations with differing degrees of numbness, pins-and-needles, and pain. Commonly affected areas include:
Front, back, and outside the thigh.
Front, back, and outside the lower leg.
The top and outer side of the foot.
Bottom of the foot.
Between the toes.
Like motor function disruption, sensory impairment is determined by where the problems are occurring.
Function Restoration Chiropractor
Affected, reduced, and inhibited motor and sensory functions can lead to muscle weakness, chronic pain, and permanent nerve damage. Function restoration chiropractor and physical therapeutic massage can help manage nerve compression and irritation. Spinal manipulations restore misaligned vertebral discs taking the pressure off the nerve relieving the pain, and regaining nerve signal flow and mobility. Chiropractic will induce deep muscle relaxation to stop muscle spasms, release tension, soothe the nerve, release endorphins, and restore sciatic nerve function.
Spinal Decompression
References
Bouche, P. “Compression and entrapment neuropathies.” Handbook of clinical neurology vol. 115 (2013): 311-66. doi:10.1016/B978-0-444-52902-2.00019-9
Cook, Chad E et al. “Risk factors for first-time incidence sciatica: a systematic review.” Physiotherapy research international: the journal for researchers and clinicians in physical therapy vol. 19,2 (2014): 65-78. doi:10.1002/pri.1572
Giuffre BA, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2021 Jul 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482431/
In the lower half region of the body, a large nerve connects to the lumbar region of the spine that travels down to the legs. This is the sciatic nerve, and its primary function is to provide mobility to the legs. The legs use the sciatic nerve to move, feel, and stabilize the body as it is in motion. When the lumbar region of the spine begins to natural wear and tear from injuries or ordinary factors like lifting heavy objects can cause the spinal discs in the spine to herniate and press on the sciatic nerve. When this happens, the sciatic nerve sends out pain signals that travel down the legs and back to the brain, causing symptoms like sciatica to develop. Luckily some therapies can help prevent sciatica from developing further and provide relief to many suffering individuals. Today’s article focuses on the factors that cause sciatica and how treatments like decompression therapy can help prevent sciatica-like factors from progressing further for many individuals. Referring patients to qualified and skilled providers who specialize in spinal decompression therapy. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is essential for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Sciatica?
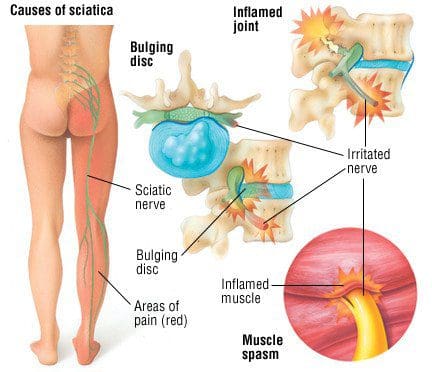
Do you feel pain running down your legs? Does it hurt when you are walking, even for a short distance? How about muscle stiffness that is occurring in your lower back and legs? All these symptoms are signs that you are experiencing sciatica. Research studies have defined sciatica as a throbbing, sharp pain that affects one side of the body and travels down each leg. Whenever a person is suffering from sciatica, the pain symptoms usually vary, depending on how severe it affects the legs. Sciatica usually forms when the spine suffers from a herniated disc, or the piriformis muscle starts to compress on the sciatic nerve, causing it to become irritated. Additional information shows that various conditions that can structurally impact or even compress the sciatic nerve can result in sciatica symptoms that can hinder a person’s ability to walk. Injuries to the spine are not the only factors that can cause sciatica to occur, as ordinary factors can also be an issue.
Factors That Cause Sciatica
Now many factors can cause sciatica to develop. Some of these factors can be ordinary everyday habits that many have adopted that don’t realize are causing sciatica pain. Research studies have shown that many individuals that are suffering from low back pain from strenuous working conditions like sitting down in a desk job for long periods can cause an increased risk of developing sciatica. Sitting for an extended period can cause a person to create poor posture, which leads to low back pain and thus developing sciatica. Another factor that can lead to sciatica is lifting heavy objects. Additional research studies have shown that when workers handle carrying or lifting heavy objects can affect their lower back. The heavyweight of the object causes stress and tension on the lower muscles causing the individual to ache in pain. These painful symptoms can cause the lower muscles to compress and aggravate the sciatic nerve. Luckily some treatments can help prevent these factors from irritating the sciatic nerve and prevent sciatica from progressing.
Things To Avoid With Sciatica-Video
Are you feeling muscle strain from lifting or carrying heavy objects? Does your lower back ache after an extended period of sitting down? Do you feel aggravating pain in the back of your legs? You could be suffering from sciatica, and decompression therapy might be able to help. The video above explains the ten things to avoid when dealing with sciatica. Decompression therapy allows the individual experiencing sciatica to feel relief in their lower back. It uses gentle traction on the spine to enable the aggravated sciatic nerve to relax while also loosening up the stiff muscles that are causing immobility to the lower back. Incorporating decompression therapy as a wellness treatment is beneficial. This link will explainhow decompression offers optimal comfort for many people who suffer from sciatica while also returning them to their health and wellness journey.
How Decompression Can Alleviate Sciatica Factors
Many treatments are available to help with sciatica symptoms and low back pain symptoms that can relieve the suffering individual. Research studies have shown that decompression treatments for sciatica can be delivered to many individuals by reducing the pain that the piriformis muscle has trapped. When the piriformis muscle is gently moved away from the sciatic nerve, the pain signals will lessen from sending information to the brain. Other research studies have shown that decompression treatments for trapped sciatic nerves will provide pain reduction to the leg muscles and relieve the buttock muscles from suffering from muscle spasms. Many individuals that suffer from sciatica will also feel relief from the negative pressure that decompression treatment has provided.
Conclusion
Overall, sciatica can be caused by factors that can be ordinary, like sitting for an extended period, lifting, or carrying heavy objects. Other factors can be simple as a herniated disc or piriformis syndrome. Decompression treatments allow the individual to feel instant relief from sciatica by gently stretching the spine to alleviate the pressure off of the sciatic nerve. Once the sciatic nerve starts to feel better after being aggravated, the lower half of the body will begin to relax, and the individual will become pain-free.
References
Davis, David, et al. “Sciatica – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 6 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK507908/.
Euro, Ulla, et al. “Work-Related Risk Factors for Sciatica Leading to Hospitalization.” Scientific Reports, Nature Publishing Group UK, 25 Apr. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6484005/.
Hogan, Elizabeth, et al. “A Minimally Invasive Surgical Approach for the Treatment of Piriformis Syndrome: A Case Series.” Chinese Neurosurgical Journal, BioMed Central, 30 Mar. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7398220/.
Lis, Angela Maria, et al. “Association between Sitting and Occupational LBP.” European Spine Journal : Official Publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, Springer-Verlag, Feb. 2007, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2200681/.
Park, Myung-Sik, et al. “Clinical Results of Endoscopic Sciatic Nerve Decompression for Deep Gluteal Syndrome: Mean 2-Year Follow-Up.” BMC Musculoskeletal Disorders, BioMed Central, 20 May 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4875686/.
Staff, Mayo Clinic. “Sciatica.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 1 Aug. 2020, https://www.mayoclinic.org/diseases-conditions/sciatica/symptoms-causes/syc-20377435.
The lower half of the body helps provide stability to the upper half of the body. The hips, legs, and feet have sensory and motor functions from the nerves part of the peripheral nervous system. These nerves are connected to the lumbar region of the spine that makes the hips rotate, the feet sense where it is going, and the legs move around freely. One of the nerves connected to the lumbar regions of the spine is the sciatic nerve. The sciatic nerve extends from the spinal cord’s lower lumbar region through the buttock muscle region and travels down to the legs. When unwanted symptoms start to affect the lower half of the body, it can cause the sciatic nerves to become trapped in the buttock muscle region and irritated, causing sciatica to develop. Today’s article will focus on the deep gluteal syndrome, how it affects the sciatic nerve, and how decompression treatments can help relieve trapped sciatic nerves. Referring patients to qualified and skilled providers who specialize in spinal decompression therapy. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is essential for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Deep Gluteal Syndrome?
Do you feel pain in your hips and buttock regions? How about stinging, burning pain that is causing leg pain? Do your buttock muscles gradually begin to feel numbness or spasms throughout the day? If you have been dealing with these symptoms, it could be deep gluteal syndrome. Research studies have defined deep gluteal syndrome as a presence of pain located in the buttock region that causes the surrounding muscles to press on the nerve roots and cause unwanted pain. When a person suffers from an accident like falling and landing on their butt, the muscles feel the effects of that fall and start to compress the sciatic nerve that is traveling down the leg and causes pain to the body’s lower extremities. Other studies have shown that deep gluteal syndrome factors can cause this condition to develop over time due to increased muscle tension that aggravates the sciatic nerve. Other causes of the deep gluteal syndrome can include prolonged sitting. The butt muscles start to pinch the sciatic nerves constantly, the muscles from the buttock start to feel tender to the touch, and abnormalities in the piriformis muscles can lead to the development of sciatica.
How Does It Affect The Sciatic Nerve & Symptoms?
Since deep gluteal syndrome causes muscle tension in the buttock region, it can aggravate the sciatic nerve and causes sciatica-like symptoms in the legs. Research studies have mentioned that deep gluteal syndrome can cause a painful presence in the buttock muscles while trapping the sciatic nerve within the gluteal space, causing the sciatic nerve to become irritated. Since the sciatic nerve is located in the spinal cord and goes all the way to the legs, sciatica is presented whenever the lower half of the body is suffering from factors like herniated discs, piriformis syndrome, and even deep gluteal syndrome.
Some of the symptoms that deep gluteal syndrome causes to the lower regions of the body are sciatica. Since the sciatic nerve is located in the lower back and runs across the butt and down to the legs, it can cause leg pain since the nerves are either trapped by the buttock muscles or irritated due to a compressed disc in the spine. Other symptoms that are caused by deep gluteal syndrome involve:
Muscle tenderness
Tingling sensations traveling down the legs
Pain becomes worse during light to moderate exercises
Muscle aches on the hips, lower back, and buttock
Spinal Decompression With The DRX9000- Video
Do you feel less mobility in your hips? How about the excruciating pain that travels down to your legs? Does it hurt when you walk or sit down for long periods? This could result from deep gluteal syndrome associated with sciatica, and decompression therapy might be the relief you are looking for. The video above explains how the DRX9000 helps relieve herniated discs from aggravating the sciatic nerve. The DRX9000 is part of a wellness treatment known as decompression therapy that incorporates gentle traction on the spinal discs by increasing their height between the spinal joints and promoting a healing factor for those suffering from low back pain issues. Decompression therapy can be in surgical and non-surgical treatments depending on the severity of pain that the spine is in. Incorporating spinal decompression as part of your wellness treatment is beneficial. This link will explainhow decompression offers optimal comfort for many people who suffer from sciatica and deep gluteal syndrome while also getting them back to their health and wellness journey.
How Decompression Can Help Relieve Deep Gluteal Syndrome
With sciatica-like symptoms associated with deep gluteal syndrome affecting the buttock and the legs, many people have turned to find some relief to ease the tense muscles that aggravate the sciatic nerve. Research studies have shown that endoscopic decompression surgery allows the individual to be supine while physicians gently move the piriformis muscle away from the sciatic nerve and relieve the pain. Other decompression treatments can also help lower the sciatic nerve’s inflammation, causing the legs to be under and reducing muscle spasms occurring, as research has found.
Conclusion
Overall, having pain in the lower half of the body is never a good thing. The lower half of the body allows stability for the upper half as the motor functions provide the legs to move around. When an injury starts to affect the lower half, it can cause sciatica-like symptoms associated with the deep gluteal syndrome. These conditions can cause motor dysfunction in the legs and cause a person to become unstable. Treatments like decompression therapy allow the buttock muscles to ease off the sciatic nerve and provide relief to the legs. As part of a person’s wellness journey, decompression treatments will enable the return of leg mobility to the individual without feeling pain around the lower regions of the body.
References
Ham, Dong Hun, et al. “Effectiveness of Endoscopic Sciatic Nerve Decompression for the Treatment of Deep Gluteal Syndrome.” Hip & Pelvis, Korean Hip Society, Mar. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5861023/.
Hopayian, Kevork, and James Heathcote. “Deep Gluteal Syndrome: An Overlooked Cause of Sciatica.” The British Journal of General Practice : the Journal of the Royal College of General Practitioners, Royal College of General Practitioners, 26 Sept. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6774708/.
Martin, Hal David, et al. “Deep Gluteal Syndrome.” Journal of Hip Preservation Surgery, Oxford University Press, July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4718497.
Son, Byung-Chul, et al. “Decompression of the Sciatic Nerve Entrapment Caused by Post-Inflammatory Scarring.” Journal of Korean Neurosurgical Society, The Korean Neurosurgical Society, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4345190/.
Inside the body are countless nerves that intertwine with each other and are all spread out. These nerves are functioned to give motor and sensory function to the body that allows a person to feel, sense, touch, and move. As part of the peripheral system in the body, these nerves are connected to the spinal cord and spine as they branch out in the spinal columns and send signals to and forth to the brain. When the body suffers from an accident or an injury, the nerves send the pain signals to the brain allowing the immune system to go to the affected area and start healing the injury. Sometimes the body suffers from natural wear and tear and that causes pain to the nerves, making the body lose the sensory and motor functions that the nerves provide. This causes radiculopathy in the body and there are treatments that allow relief to reduce the effects of radiculopathy. Today’s article post will discuss the sciatic nerve and radiculopathy, its symptoms, and how decompression therapy can help individuals that are suffering from sciatic radiculopathy. Referring patients to qualified and skilled providers who specialize in spinal decompression therapy. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is essential for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
The Sciatic Nerve & Radiculopathy
Have you been experiencing pain traveling down to the lower extremities of your body? Does the pain feel hot to the touch? Is the pain a sharp, stabbing pain or a burning, searing pain in the sciatic nerve? If you have encountered these symptoms, these symptoms might be due to radiculopathy along the sciatic nerve. The sciatic nerve is part of the peripheral nervous system; its primary sensory and motor functions ensure that the legs move and stand in the body. When the body goes through natural aging, wear and tear, accidents and injuries, it can cause radicular pain along the spine while compressing the nerve roots, including the sciatic nerve. Research studies have shown that radicular pain along the sciatic nerve root can cause deficits in the lower extremities’ motor and sensory function. This radicular pain can cause many problems and conditions when not treated right away.
Research studies have defined radiculopathy as one of the reasons that many people have been suffering from low back pain. Radicular pain is located along the spine in the cervical, thoracic, and lumbar areas. When these areas are affected, it can severely damage the underlying nerve roots, thus causing the lower extremities to lose all sensory and motor functions. Additional information has found that sciatica is a type of radiculopathy that pinch the sciatic nerve causing sharp, radiating pain that travels from the lower back down to the legs. Depending on how severe the radicular pain is, it can affect the sciatic nerve over time and develop into sciatica.
The Symptoms
When the sciatic nerve is pinched and irritated, it can send radiating pain down the legs and transmit signals to the brain. These pain signals can disrupt the brain signals and cause the immune system to constantly send inflammatory cytokines to the affected areas along the legs, lower back, and buttocks regions. Some of the common symptoms that occur when a person is dealing with sciatic radicular pain or sciatica will experience:
Feeling muscle weakness alongside the lower back, legs, and feet? Does the pain range from mild to a burning sensation after physical activity? How about feeling discomfort or relief after shifting positions while relaxing? If you have experienced these symptoms, you might be experiencing sciatic radiculopathy, and non-surgical decompression treatment is the answer you are seeking. Suppose you want to learn more about decompression treatments and how they can benefit you in providing relief from sciatic radiculopathy? The video above introduces the Chatanooga traction machine that allows the person suffering from sciatic radiculopathy to feel relief. This traction machine is part of non-surgical decompression therapy. It enables the spine to be gently pulled slowly to allow the compressed spinal discs to release their hold on the irritated sciatic nerve. After the pressure has been removed from the pinched sciatic nerve, the affected leg, low back, and buttock muscles will begin to relax, and the pain signals to the brain will start to diminish. Incorporating spinal decompression as part of your wellness treatment is beneficial. This link will explainhow decompression offers optimal comfort for many people who suffer from sciatica or other sciatic radicular pain.
How Decompression Therapy Can Help With Sciatic Radiculopathy
When radiating pain is shooting down to the leg and feet, many individuals try to find relief for sciatic radiculopathy. Some people will incorporate heat and ice compressed pads to be placed in the affected areas. At the same time, others use electromagnetic pulses along their legs to relax the muscles trapping the sciatic nerve roots. One of the treatments that many people have incorporated into their wellness treatments is decompression therapy. Research studies have learned that when the gluteal muscles entrap the sciatic nerve, it can become irritated or pinched, causing radiating pain down the legs. Decompression can help release the trapped sciatic nerve from the gluteal muscles and reduce the pain. Another reason that decompression therapy can help with sciatic radiculopathy is because it can help dampen the effects that the inflammatory cytokines have caused along the lower region of the body. Additional research studies have found that decompression surgery has provided less soft tissue and muscle damage, reduced pain symptoms along the legs, decreased the risk of re-herniation occurring, and faster recovery. Many individuals will experience less leg pain and low back pain from occurring when they add decompression into their wellness treatment.
Conclusion
The sciatic nerve can succumb to radicular pain like herniated discs or gluteal muscles trap the sciatic nerve making it irritated or aggravated. When this happens, the sciatic nerve causes motor and sensory dysfunction in the legs and radiating, throbbing pain to the side. Treatments like decompression therapy can help alleviate sciatic radiculopathy by releasing the compressed disc or muscle off the sciatic nerve and dampening the painful effects it causes. Decompression therapy is a beautiful addition to any wellness treatment for individuals trying to regain their health and wellness.
References
Aljawadi, Ahmed, et al. “Sciatica Presentations and Predictors of Poor Outcomes Following Surgical Decompression of Herniated Lumbar Discs: A Review Article.” Cureus, Cureus, 21 Nov. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7681772/.
Dydyk, Alexander M, et al. “Radicular Back Pain.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 2 Nov. 2021, https://www.ncbi.nlm.nih.gov/books/NBK546593/.
Feinberg, Joseph, and Shikha Sethi. “Sciatic Neuropathy: Case Report and Discussion of the Literature on Postoperative Sciatic Neuropathy and Sciatic Nerve Tumors.” HSS Journal : the Musculoskeletal Journal of Hospital for Special Surgery, Springer-Verlag, Sept. 2006, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2488172/.
Medical Professionals, Cleveland Clinic. “Radiculopathy: Symptoms, Causes & Treatment.” Cleveland Clinic, 16 Mar. 2022, https://my.clevelandclinic.org/health/diseases/22564-radiculopathy.
Park, Myung-Sik, et al. “Clinical Results of Endoscopic Sciatic Nerve Decompression for Deep Gluteal Syndrome: Mean 2-Year Follow-Up.” BMC Musculoskeletal Disorders, BioMed Central, 20 May 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4875686/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine