When it comes to the body, the hands and fingers correlate with each other by giving the host the grip strength to carry and hold items. The items can range from the smallest to the largest, depending on the item’s weight that a person can physically hold. When the weight becomes overbearingly heavy that a person can not lift or hold, it can lead to unwanted symptoms that overlap with other chronic conditions. To that point, when the hand muscles begin to lose their grip strength, it can lead to the development of trigger points in the affected muscles connected to the hand muscles and tendons. Today’s article looks at a chronic condition associated with trigger points known as trigger fingers, what the symptoms are, and how to treat trigger fingers in the hands. We refer patients to certified providers specializing in hand and wrist pain therapies to aid many people suffering from trigger fingers affecting their hands. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
What Is Trigger Fingers?
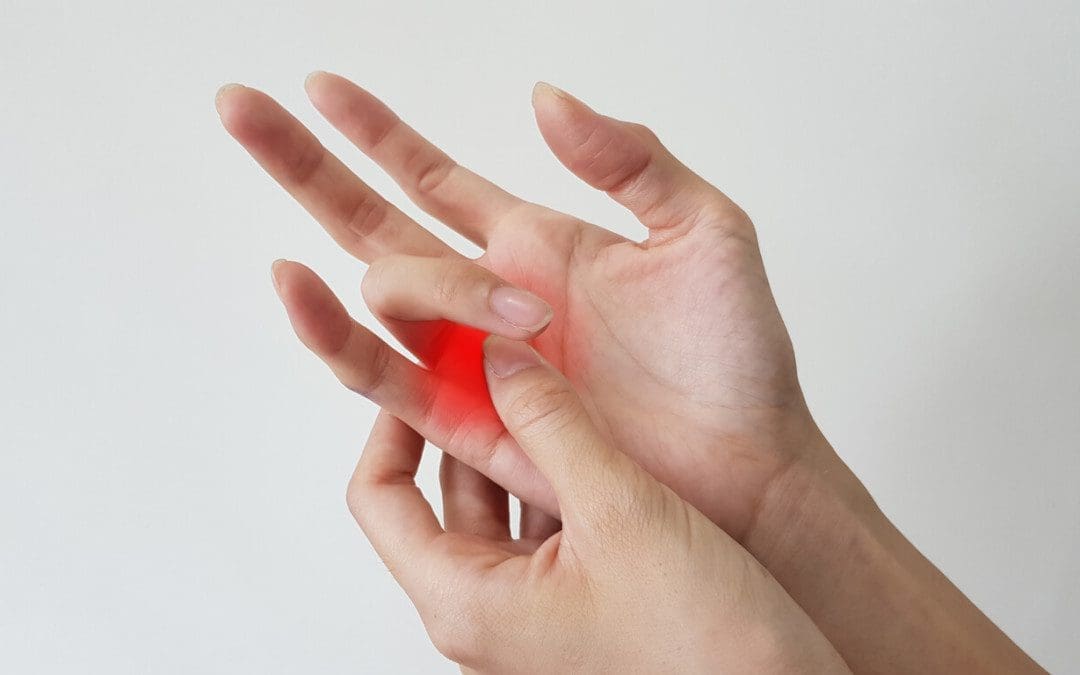
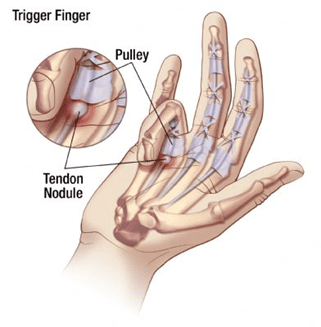
Have you encountered stiffness in your fingers? Do you feel pain radiating from your forearms to the palm of your hands? Does it seem difficult to carry or hold items for an extended period? Many people who have dealt with these symptoms believe it is something arthritic or just normal signs of age; however, it could correlate with triggering fingers affecting the hands. Trigger fingers or stenosing tenosynovitis happens when the flexor sheaths in the wrist become overused due to repetitive motions that cause the flexor tendon muscles in the forearm to be inflamed and development issues in the finger joints. This can be very problematic for many individuals who work with their hands as it can cause significant functional impairment to the hands and the fingers. Trigger fingers also commonly affect the individual’s dominant hand and involve the most common digit, the thumb.
The Symptoms
When many individuals are dealing with trigger fingers in their hands, they often complain about their fingers locking up in flexion or extension. When this happens, it can become problematic, as trigger fingers can affect the mobility of the fingers. Some of the symptoms that trigger fingers cause in the digits include:
Stiffness in the fingers
Popping or clicking sensations
Bumps at the base of the finger joint
Finger catching in a bent position and pops straight
Finger locking
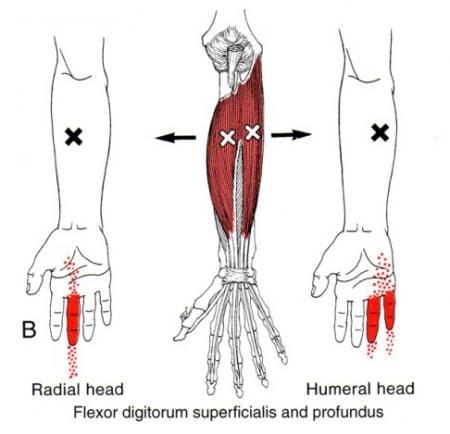
What is the correlation between diabetes and trigger fingers? Studies reveal that trigger fingers are a multifactorial chronic condition that can occur in anyone, especially those with diabetes. Trigger fingers are diagnosed by palpating a thickened tendon. Other issues cause trigger fingers to form due to active trigger points affecting the flexor muscles in the forearms. According to Dr. Travell, M.D.’s book, “Myofascial Pain and Dysfunction: The Trigger Point Manual,” individuals with active trigger points along their forearm muscles tend to experience difficulty in utilizing mobility strength with their hands. To that point, many individuals may not be able to cup and supinate their hands, extend or flex their fingers, or be able to grip items they are reaching.
An Overview Of Trigger Fingers- Video
Are you dealing with joint stiffness along your fingers? What about feeling pain from flexing or extending their fingers? Or do you feel pain and tenderness in your forearm muscles? Many individuals with these symptoms could be dealing with the pain associated with trigger fingers. Trigger fingers occur when the finger digits suffer from microtrauma by repetitive use or compression forces that invokes pain and inflammation along the tendons of the fingers. The video above overviews trigger fingers, their symptoms, and how to diagnose and treat trigger fingers in the hands. Many associated factors can lead to the development of trigger fingers, and one related factor is diabetes overlapping trigger points along the forearms. Studies reveal that trigger fingers are a complication affecting the upper extremities in diabetic individuals. Individuals with trigger fingers associated with diabetes can also cause overlapping risk profiles for cardiovascular diseases. This relationship is known as somato-visceral pain, where the damaged muscle affects the corresponding organ. In this case, the tendons for the fingers cause referred pain to the heart, thus potentially involving the cardiovascular system. Luckily there are various ways to treat trigger fingers and prevent pain from occurring in the hands in the future.
How To Treat Trigger Fingers
Since trigger fingers are a common source of pain and disability in the hands, many individuals seek pain specialists to manage and relieve pain associated with trigger fingers. Studies reveal that various methods are used to reduce the pain along the affected finger digits and bring back mobility to the finger joints. Doing gentle finger stretches, not gripping items so tightly, or applying heat to loosen up the locked joints, can help manage trigger fingers while preventing the pain-like symptoms from coming back. Incorporating these treatments can help bring mobility strength back to the hands and prevent the fingers from locking up. However, treatment alone can not be the only solution; after the individuals get treatment for trigger fingers, they have to do their part to prevent future issues from reoccurring again in their fingers.
Conclusion
The hands and fingers have a casual relationship, providing mobility and grip strength for the host to hold and carry items. However, when traumatic factors or normal activities begin to overuse the joints and muscles in their hands, it can lead to trigger fingers. Trigger fingers can cause the finger joints to lock up and invoke pain-like symptoms in the hands. This can make many individuals lose their mobility function in their hands and can make them miserable. Luckily, various treatments can help manage trigger fingers and help bring mobility back to the individual’s hands.
References
Akhtar, Sohail, et al. “Management and Referral for Trigger Finger/Thumb.” BMJ (Clinical Research Ed.), BMJ Publishing Group Ltd., 2 July 2005, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC558536/.
Jeanmonod, Rebecca, et al. “Trigger Finger – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 20 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK459310/.
Makkouk, Al Hasan, et al. “Trigger Finger: Etiology, Evaluation, and Treatment.” Current Reviews in Musculoskeletal Medicine, Humana Press Inc, June 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2684207/.
Mineoka, Yusuke, et al. “Trigger Finger Is Associated with Risk of Incident Cardiovascular Disease in Individuals with Type 2 Diabetes: A Retrospective Cohort Study.” BMJ Open Diabetes Research & Care, BMJ Publishing Group, Apr. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8039242/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
The hands are the main show when it comes to the body. They can be expressive when a person is talking, they can carry items from place to place, and when it comes to sports, they have excellent grip strength. The various muscles, tendons, nerve roots, and ligaments surround the joints to provide functionality and mobility to each finger digit. The hands also have a great relationship with the wrist and forearms because the muscles in the forearms travel down to the hands to provide mobility, flexion, and extension to the fingers. However, when the muscles become overused from repetitive motions, it can lead to the development of pain overlapping other conditions that can affect the wrist and hands. To that point, trigger points can develop over time to invoke pain in the affected muscles and cause referred pain to affect the hands. Today’s article looks at one of the muscles known as the palmaris longus, how trigger points affect the hand muscles, and various techniques to manage trigger points along the palmaris longus muscle. We refer patients to certified providers specializing in hand and wrist pain therapies to provide aid to individuals suffering from trigger point pain associated with the palmaris longus muscles located on the hand. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
What Is The Palmaris Longus Muscle?
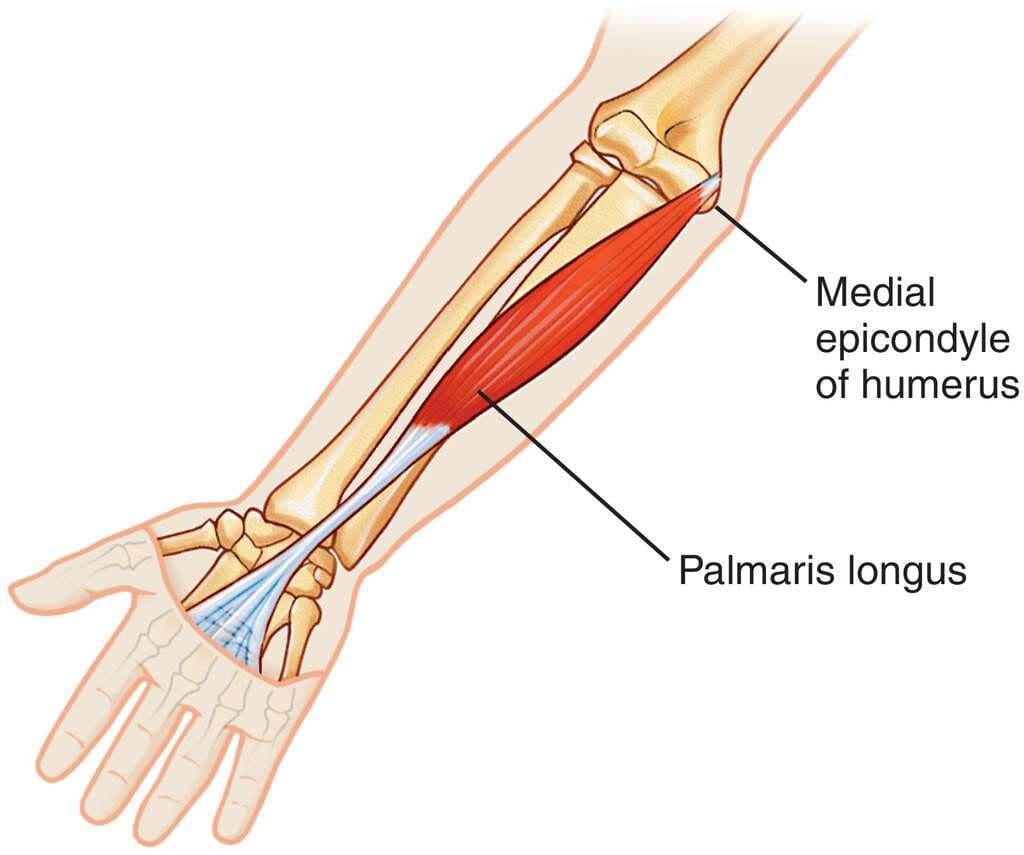
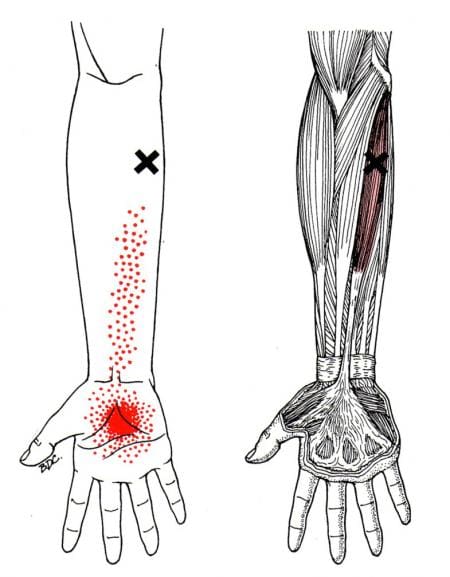
Have you been dealing with numbness in the palm of your hands? Have you been experiencing issues holding items for an extended period? Or do your wrist and forearm ache constantly? If you have been experiencing these overlapping issues, it could be the development of trigger points along the palmaris longus muscle. The palmaris longus is a small muscle located on the front of the forearms and extends down from the wrist to meet with the rest of the muscles and tendons of the hands. The palmaris longus also connects to the roof of the carpal tunnel bones, where the median nerves and digital flexors tendons reside and provide movement. According to Dr. Janet G. Travell, M.D.’s book, “Myofascial Pain and Dysfunction: The Trigger Point Manual,” the palmaris longus muscle function is to flex the hands at the wrist while being able to tense the palmar fascia. Studies reveal that the palmaris longus muscle flexes the wrist weakly as an accessory muscle and abducts the thumb for mobility. This muscle is also prone to injuries as it can develop pain-like symptoms along the wrist and the palm of the hands.
How Trigger Points Affect The Hand Muscles?
When the palmaris longus muscle succumbs to injuries, it can develop chronic issues that can cause pain in the wrist and hands. One of the chronic issues that can affect the hand muscles and the rest of the forearms is trigger points. Trigger points can lead to the development of referred pain along the forearms, wrists, and hands. To that point, trigger points can mimic overlapping chronic conditions along the affected muscle area. So when trigger points begin to affect the palmaris longus muscle, the pain-like symptoms can mimic carpal tunnel syndrome. Now studies reveal that the palmaris longus muscle is connected to the median nerve and the pathophysiology of carpal tunnel syndrome is more likely to interplay between anatomic and systemic factors. This causes the median nerve root to become compressed, thus causing pressure and pain to the hands. To that point, trigger points in the palmaris longus muscle may be activated by direct trauma. Some examples that can cause the development of trigger points are:
Gripping tools too tightly
Leaning on a cane
Holding a tennis racket at the end of the handle
Falling and landing on the hands
Many of these actions can result from overusing and causing issues in the palmaris longus muscle, leading to unwanted pain and muscle injury symptoms.
Trigger Points On The Palmaris Longus-Video
Are you experiencing any numbing sensations in the palm of your hands? What about feeling the symptoms of carpal tunnel syndrome along your wrist? Or have you experienced aches and pain along your forearms? Some of these symptoms correlate with the development of trigger points along the palmaris longus muscle. The palmaris is a small muscle in front of the forearms and travels down to the wrist to connect with the rest of the muscle tendons of the hands. When traumatic events begin to affect and injure the palmaris longus, it can develop trigger points and cause pain to radiate down to the wrists and hands. The video above explains where the palmaris longus muscle is located and how trigger points activate pain-like symptoms that mimic chronic conditions like carpal tunnel syndrome. Studies reveal that when the median nerve (which is connected with the palmaris longus muscle) is being entrapped, causing trigger points to mimic carpal tunnel syndrome symptoms. Alas, all is not lost, as there are various techniques that many people can utilize to relieve pain from the palmaris longus muscle and manage trigger points from developing further.
Various Techniques For Managing Trigger Points On The Hand Muscles
When it comes to managing trigger points on the hand muscles and palmaris longus muscle, many people will incorporate various remedies to reduce the pain-induced inflammation on the affected muscle and manage trigger points from causing more issues in the affected muscles. Treatments like massaging the forearm to the hands can help release trigger points from the palmaris longus muscle. Granted, there will be involuntary twitching, but the results prevent future trigger points from forming the muscle. Another technique is placing a heating pad on the forearm to relax the tense muscles and reduce pain. And finally, gentle stretches and reducing a tight grip can prevent hyperirritability on the palmaris longus muscle and strengthen the muscles that are connected with the palmaris longus muscle.
Conclusion
Regarding the body, the hands have a very important function as they provide grip strength and have a great relationship to the wrist and forearms. The palmaris longus muscle is a small band in front of the forearms and connects to the various muscles and tendons of the wrists and hands. When traumatic injuries affect the palmaris longus muscle, it can develop trigger points correlating with carpal tunnel symptoms. When trigger points affect the palmaris longus muscle, it can cause symptoms of pain and numbness in the wrist and hands, causing a person to lose their grip strength. Thankfully, various techniques to manage and treat trigger points can reduce the pain quality on the forearms and wrist while bringing the grip strength back to the hands.
References
Boltuch, Andrew D, et al. “The Palmaris Longus and Its Association with Carpal Tunnel Syndrome.” Journal of Wrist Surgery, Thieme Medical Publishers, Inc., Dec. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7708024/.
Cooper, David W, and Bracken Burns. “Anatomy, Shoulder and Upper Limb, Hand Palmaris Tendon.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 3 Sept. 2021, https://www.ncbi.nlm.nih.gov/books/NBK519516/.
Ioannis, Dimitriou, et al. “Palmaris Longus Muscle’s Prevalence in Different Nations and Interesting Anatomical Variations: Review of the Literature.” Journal of Clinical Medicine Research, Elmer Press, Nov. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4596262/.
Meder, Marek A, et al. “Reliability of the Infraspinatus Test in Carpal Tunnel Syndrome: A Clinical Study.” Journal of Clinical and Diagnostic Research : JCDR, JCDR Research and Publications (P) Limited, May 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5483796/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
The elbows and the forearms have a casual relationship with each other as they provide flexion and retraction of the arms in the body. Each different muscle group in the body has the job of making the body functional. The arms help the body to carry items while the shoulders provide stability to the head and neck. The head and neck work together to allow rotation and movement. Finally, the legs and hips stabilize the body’s upper half and move from place to place. Traumatic events or injuries that affect the arms can lead to pain along the muscles in the forearms. This can lead to the muscles becoming inflamed and developing myofascial pain syndrome or trigger points along the affected muscles. One of the muscles in the forearms that can be affected by myofascial pain syndrome is the supinator muscles. Today’s article looks at the supinator muscles, how myofascial pain affects the supinator muscles, and how to manage myofascial pain syndrome along the supinator muscles. We refer patients to certified providers who specialize in elbow pain treatments to aid individuals suffering from myofascial pain syndrome associated with the supinator muscles near the elbow and forearm. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
What Is The Supinator Muscle?
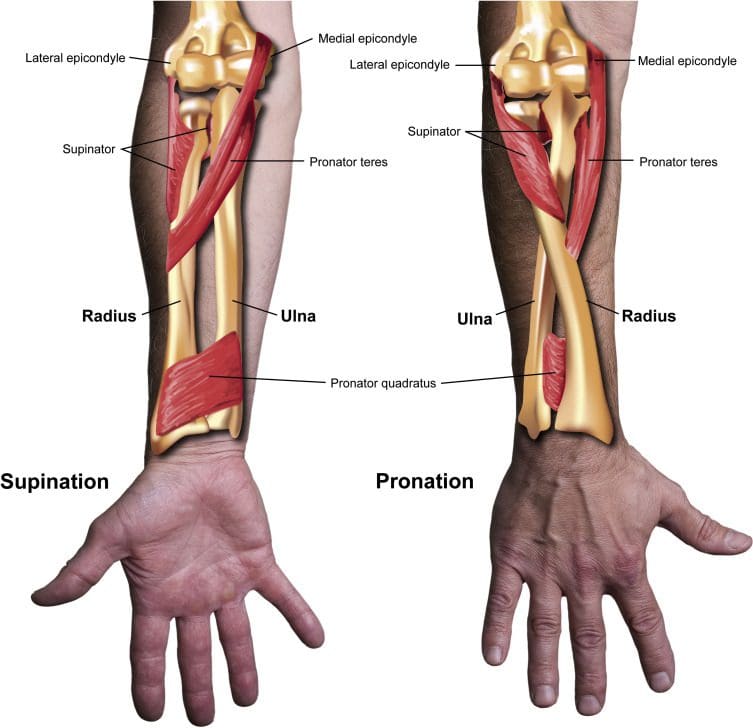
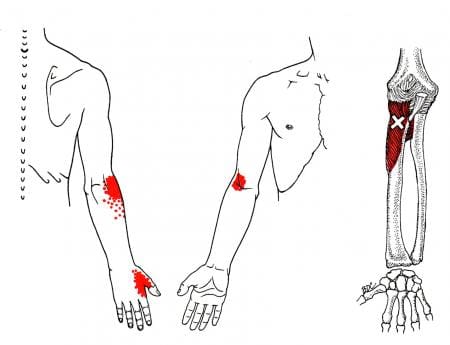
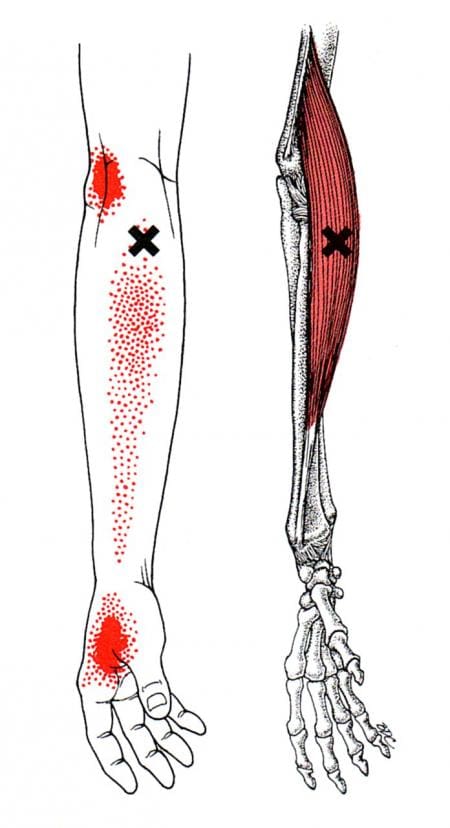
Are you experiencing any pain along your forearm or elbow? What about feeling stiffness along your thumb? Do you feel any tenderness or soreness in your forearm muscle? People who have been experiencing these symptoms might be dealing with myofascial pain syndrome that is affecting their supinator muscles. According to Dr. Travell, M.D.’s book, “Myofascial Pain and Dysfunction: The Trigger Point Manual,” the supinator muscle is a flat spiral muscle under the elbow joint and is located in the posterior compartment of the forearm. The supinator muscle function is to supinate or turn the forearm when the elbow is in a position of flexion or extension. The supinator muscle also works together with the bicep brachii muscles. Studies reveal that the biceps function provides stability and assists with internal rotation with the elbow joint by interacting with the supinator muscle. Both of these muscles provide supination and flexion strength to the elbow. However, the supinator muscle can also be affected by injuries in the elbows and forearms, causing referred pain along the forearms and parts of the hand, primarily the thumb.
Myofascial Pain Affecting The Supinator Muscle
When the supinator muscle is suffering from pain, various issues can cause the pain to occur near the elbow and forearm. Multiple factors can include:
Carrying a large, heavy bag.
Playing tennis.
Extreme movements cause the elbow to be hyperextended and lead to myofascial pain syndrome or trigger points along the supinator muscles.
Now tennis elbow is often associated with trigger points as it affects the lateral head of the triceps and the extensor muscles next to the supinator muscles. Studies reveal that tennis elbow usually occurs on the dominant arm and is regarded as an overuse injury that involves repetitive extension against resistance. To that point, the repetitive motions can lead to the development of trigger points along the supinator muscles.
Many people with active trigger points in the supinator muscles often complain about twinges of pain located in the front or back of the elbow, along with muscle tenderness in the supinator muscle. Myofascial pain syndrome can also mimic other chronic pain conditions in the arm that causes referred pain symptoms associated with the muscle. Myofascial pain syndrome causes the affected muscle to be hyperirritable and causes the surrounding nerves that are intertwined with the muscles to be compressed. This causes various symptoms in the forearms, like tingling sensations, numbness, and a decrease in grip strength. All is not lost as multiple ways to manage myofascial pain syndrome along the supinator muscles.
How To Release Supinator Trigger Points- Video
Are you experiencing twinges of pain near your elbow? What about radiating pain along your thumb? Do you feel tenderness or muscle weakness on your forearms or your elbow? Many of these symptoms are due to the development of myofascial pain syndrome or trigger points that are affecting the supinator muscles. Trigger points can mimic other chronic pain conditions that can cause referred pain to the rest of the body. The video above explains where trigger points are located in the supinator muscle and how to release the trigger points from that muscle. Various techniques can help manage myofascial pain syndrome that is affecting the supinator muscles and can help alleviate the pain-like symptoms that are along the muscle fibers.
Managing Myofascial Pain Syndrome Along The Supinator Muscles
When managing myofascial pain syndrome along the supinator muscles, many individuals can incorporate these techniques as part of their daily activities. Many individuals can go to a pain specialist that targets myofascial pain syndrome through palpations and massages. Studies reveal that incorporating a diagnosis of where the palpations have occurred and massaging the affected muscle can release the trigger points from the muscle and reduce pain. Another technique many people can utilize to manage myofascial pain syndrome is not overextending the elbow to cause trigger points to form. This is extremely important for tennis players to prevent tennis elbows from forming and reduce the chances of trigger points forming along the supinator muscles. And lastly, doing isotonic exercises can help strengthen and condition the supinator muscles to prevent injuries. These techniques allow the individual to be pain-free and continue with their daily lives.
Conclusion
The supinator muscles are located underneath the elbow, allowing forearm rotation when the elbow is flexed or extended. When the supinator muscle is affected by injuries or repetitive motions, it can develop trigger points or myofascial pain syndrome. This causes referred pain along the elbow to parts of the hand, primarily the thumb. Trigger points can even overlap and cause symptoms of “tennis elbow” to cause pain along the muscle and joints. Luckily, various techniques can prevent trigger points from developing further and reduce the pain in the elbows and forearms. To that point, the individual can continue doing their daily activities.
References
Bron, Carel, et al. “Interrater Reliability of Palpation of Myofascial Trigger Points in Three Shoulder Muscles.” The Journal of Manual & Manipulative Therapy, Journal of Manual & Manipulative Therapy, Inc., 2007, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2565638/.
Cutts, S, et al. “Tennis Elbow: A Clinical Review Article.” Journal of Orthopaedics, Elsevier, 10 Aug. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6926298/.
Güleçyüz, Mehmet F, et al. “Reference Values of Flexion and Supination in the Elbow Joint of a Cohort without Shoulder Pathologies.” BioMed Research International, Hindawi, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5674724/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Vol. 1, Williams & Wilkins, 1999.
The fingers are in a close relationship with the hands and the body. Each finger digit is controlled by various muscles encompassing the wrist and forearms. The fingers allow the host to be expressive and point and manipulate objects while protecting the joints in each digit. When chronic conditions or injuries begin to affect each finger digit, it can lead to referred pain along the hand muscles, the wrists, and the forearms, causing the development of trigger points to overlap the affected muscles in the fingers. Today’s article looks at how the finger extensor muscles work, how trigger points affect the finger extensor muscles, and how to manage pain associated with trigger points along the fingers. We refer patients to certified providers who specialize in hand pain treatments to aid individuals suffering from trigger points related to pain affecting the finger extensor muscles along the hands. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
How Do The Finger Extensor Muscles Work?
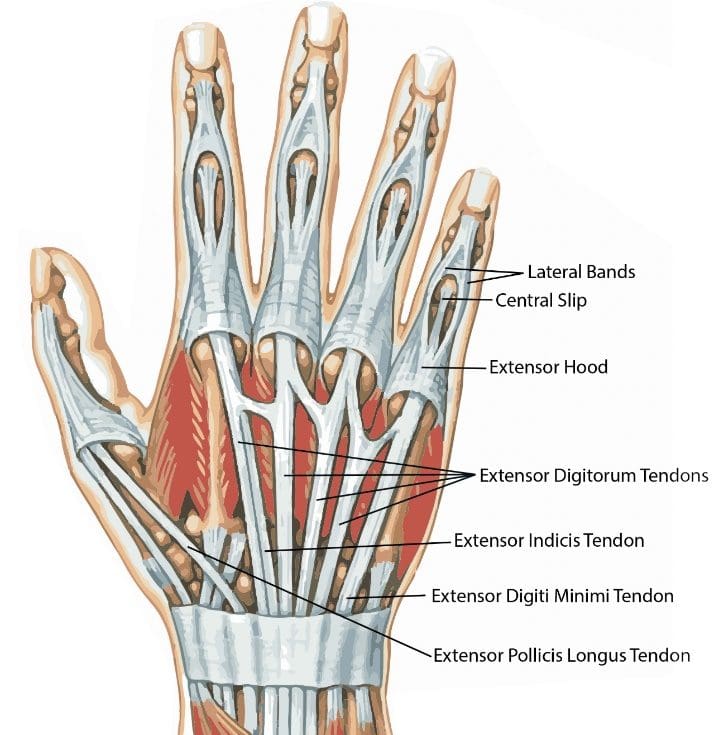
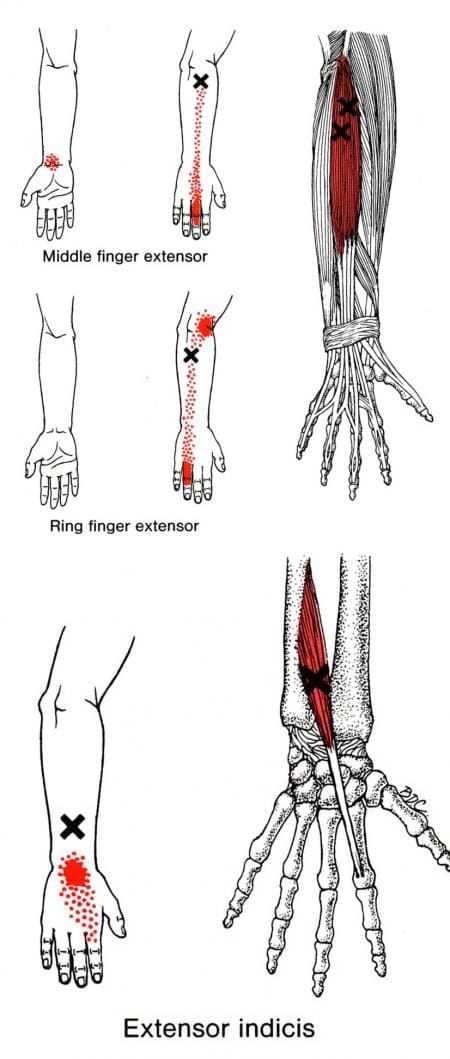
Are you experiencing pain in your fingers? Does it seem difficult to hold onto items even for a short period? Or are you experiencing muscle pain from your thumb to your wrist? Numerous individuals experiencing pain in their fingers and hands risk developing trigger points or myofascial pain syndrome in their fingers and hands. The hand muscles have many intricated muscles and insert themselves as the origin points for the bones, ligaments, and fascia of the hands. The finger extensor muscles begin at the forearms as the point of origin and stretch past the wrist to each finger digit which includes:
Thumb
Index finger
Middle finger
Ring finger
Pinky finger
The three main fingers that provide motion for the hands are the index, ring, and middle finger, which allow the muscles to be held in flexion and extension while giving extra support for hand actions for gripping items. Studies reveal that even though the structural and functional complexities of the human fingers have been recognized, each finger recognized an effective function of precise coordination of multiple muscles. To that point, this results in constrained finger motion by exerted forces from the joint capsules, ligaments, and joint articular surfaces. However, the tendons and the extensor muscles of the fingers suffer from injuries and conditions that can affect the functionality of each finger’s grip strength.
How Trigger Points Affect The Finger Extensor Muscles?
When the hands, wrists, and forearms are injured from traumatic forces or through ordinary factors like pulling a muscle or feeling unexplainable pain in the forearms, it can lead to referred pain along the affected muscles. This then leads to the development of trigger points along the affected muscles affecting mobility function with the fingers. According to Dr. Travell, M.D., when patients complain about pain in their hands, they often identify it with arthritis on the fingers when it is caused by trigger points affecting the extensor muscles in the fingers. Studies reveal that trigger points along the finger extensor muscles could refer to mechanical impingement of the tendon being narrowed through repetitive movements. When this happens, it can lead to inflammation and resistance of the tendon, causing the finger digit to lock up in a flex pose. Sometimes trigger points can even inhibit muscular contraction without pain, causing symptoms of grip weakness on the fingers. When trigger points affect the extensor muscles of the fingers and hands, it can make many individuals feel frustrated that they cannot hold onto items while doing their daily activities.
Trigger Points On The Extensor Digitorum-Video
Are you noticing that your grip strength has weakened? Do you feel pain starting from your forearm and ending at your fingertips? Or do your fingers lock up from time to time? Many of these symptoms affecting the fingers could develop signs of trigger points affecting the finger extensor muscles, causing hand pain. Trigger points usually form when the muscle from each section of the body has been through trauma, injuries, or overuse. To that point, the affected muscle has small knots along the muscle fibers, thus causing referred pain in the affected area. The video above explains where the extensor muscles are located in the forearm and how they branch out to each finger digit. When trigger points affect the muscle fibers of the extensor muscles, it can lead to hyperirritability of the muscle fibers and invoke referred pain in the surrounding tendons. Studies reveal that factors that pertain to overusing the fingers may be due to work-related musculoskeletal disorders, which lead to the association with intracellular compartmentation during non-invasive activities. This shows that latent trigger points may potentially occur on the affected muscle with or without pain.
Managing Pain Associated With Trigger Points On The Fingers
When it comes to managing trigger points along the extensor fingers, there are various techniques that many people can use to relieve pain in their hands, strengthen their grip strength, and prevent future trigger points from forming along the forearms. When many people go to their primary physicians and complain about losing their grip strength or feeling symptoms of inflammation associated with arthritis, their doctors begin to do a full examination. They communicate with them about what they have been doing with their hands. Once the doctors have a full diagnosis, they will begin to advise their patients on various techniques to relieve pain in their hands and strengthen their fingers. Some of the ways to manage trigger points along the fingers include:
Hand stretches to relieve stress on the finger joints
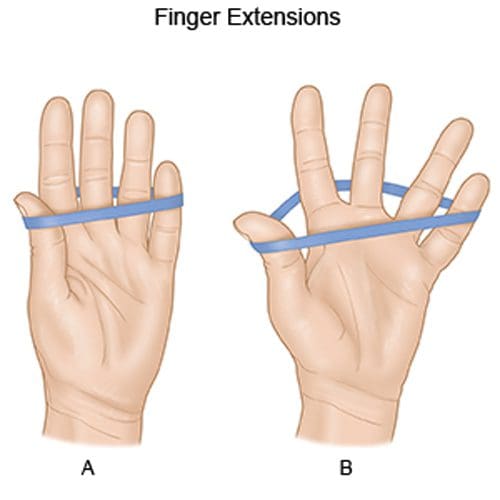
Finger extension extends with a rubber band
Avoid gripping items tightly
Sleep with fingers in a flex position
Use an ice pack to reduce inflammation in the forearm muscles
Incorporating these various techniques can reduce pain-like symptoms along the forearms, wrists, and hands and help manage trigger points from causing more issues on the hands. These techniques allow the finger extensor muscles to regain their strength and enable the individual to restore grip strength.
Conclusion
The fingers provide a close working relationship with the hands and body. The fingers allow motions expressively with the host and provide flexion and extension to each digit through extensor muscles that are located in the forearms. When injuries or hyperextension issues affect the extensor muscle, it can develop trigger points that can affect grip strength on the hands and cause pain along the finger digits and wrist. This can cause misery to the individual. Fortunately, various techniques reduce the pain in the hands and increase grip strength on the fingers while managing trigger points associated with the extensor muscles. When individuals begin to utilize stretches for their hands and wrists, it allows them to have finger mobility back to their hands and reduces the effects of pain along their forearms.
References
Ali, Stephen R, and Hussein Mohamedbahi. “Acute Trigger Finger Presenting as an Extensor Lag.” Eplasty, Open Science Company, LLC, 5 Jan. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5765627/.
Hu, Dan, et al. “Biomechanical Analysis of the Human Finger Extensor Mechanism during Isometric Pressing.” PloS One, Public Library of Science, 14 Apr. 2014, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3986208/.
Moreno-Torres, Angel, et al. “Work-Related Pain in Extrinsic Finger Extensor Musculature of Instrumentalists Is Associated with Intracellular Ph Compartmentation during Exercise.” PloS One, Public Library of Science, 9 Feb. 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2817730/.
Okwumabua, Ebubechi, et al. “Anatomy, Shoulder and Upper Limb, Hand Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 31 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK537229/.
The forearms have a casual relationship with the hands and the wrist as they are below the elbow and have very important motor functions. The hands and wrists help many individuals hold onto items, while the forearms provide support by carrying items without pain. The various muscles surrounding the forearms, hands, and wrist joints help provide mobility and flexibility to the arms. Injuries like muscle sprain, strains, or stiffness in the forearms, hands, or wrist can be due to trigger points along the brachioradialis muscles affecting the hands and wrist. Today’s article looks at the brachioradialis muscle functions on the hands and wrist, how trigger points affect the hands and wrist, and how to manage trigger points associated with the hands and wrist. We refer patients to certified providers who specialize in arm pain treatments to aid individuals suffering from trigger points associated with the brachioradialis muscles along the wrist and hands of the body. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
The Brachioradialis Function On The Hands & Wrist
Have you been experiencing stiffness in your wrist or forearms? Do you have trouble gripping items in your hands? Or do you experience radiating pain from your forearms to your wrist? Many people experiencing these pain-like symptoms are associated with trigger points along the brachioradialis muscle that affect the forearms, hands, and wrist. The brachioradialis is a superficial muscle that is located in the lateral forearm. The brachioradialis muscle works with different muscles attached to the upper arms to provide flexion to the elbow joints while working with various muscle tendons along the wrist and hands. Research studies reveal that the brachioradialis muscle works with the central nervous system by sending signals to the forearm and provides reflexes to the wrist and fingers by lightly tapping the muscle tendon of the brachioradialis. This light tapping motion sends the signal back to the brain and shows which muscle is activated. However, injuries along the brachioradialis muscle can invoke referred pain to the wrist and hands.
Trigger Points Affecting The Hands & Wrist
As stated in many research studies, trigger points or myofascial pain syndrome is a chronic musculoskeletal disorder that causes hard, discrete, tiny nodules along the taut muscle fiber bands of the affected muscle, causing pain. When the brachioradialis muscle has succumbed to pain-like symptoms from common factors or injuries, it can lead to the development of referred pain associated with trigger points affecting the hands and wrist of the body. So how would trigger points affect the hands and wrist? Well, trigger points can mimic other chronic conditions and cause pain to the affected muscles. So when trigger points affect the brachioradialis muscle, it also affects the hands and wrists.
Studies reveal that when trigger points affect the hands and the wrist, it can lead to symptoms of pain, stiffness, burning, or tingling sensations in the hands and wrist. To that point, a person can experience these pain symptoms even if they are not injured. Trigger points can form when the individual has made repetitive motions to the muscle that causes it to be overused and cause strain on the muscle, thus leading to trigger points associated with joint and muscle pain. Other studies reveal that non-specific shoulder pain associated with trigger points can increase pain intensity to the brachioradialis and affect hand grip strength. This can make many individuals unable to hold onto the items they carry.
Wrist & Hand Trigger Points- Video
Are you having trouble making a fist in your hands? Do you experience a burning sensation on your forearm down to your wrist? What about feeling pain radiating down from your elbows to your hands? Many people experiencing these pain symptoms might risk developing trigger points along the brachioradialis muscle affecting the hands and wrist. The video above explains what happens when trigger points affect the wrist and hand extensors muscles that work together with the brachioradialis muscles. Trigger points along the brachioradialis can cause referred pain to the forearms and lead to chronic symptoms that affect the functionality of the wrist and hands. This can lead to a decrease in grip strength and cause hand mobility issues for many people. At last, all is not lost, as various treatments are available to manage trigger points associated with the hands and wrist.
Managing Trigger Points Associated With The Hands and Wrist
Various treatments can help many individuals dealing with trigger points associated with the hands and wrist. Many people would go to pain specialists like chiropractors, massage therapists, or physiotherapists to manage trigger points affecting the brachioradialis muscles along the hands and wrist. These pain specialists will incorporate various techniques to reduce the pain and address the trigger points along the affected muscle. Studies reveal that acupuncture on the hands and wrist can reduce pain intensity caused by trigger points and bring back mobility function to the hands and wrist. This can regain the grip strength of the individual and improve hand and wrist functionality without pain. Other studies also reveal that trigger point therapy can also be utilized to reduce pain-like symptoms affecting the hands and wrist. Combined with gentle massages can prevent trigger points from forming in the future and reduce pain symptoms affecting grip mobility on the hands.
Conclusion
The forearms have a casual relationship with the hands and wrist as the brachioradialis muscles help provide mobility functions. The hands and wrist help grip items a person carries, while the forearms offer support. When injuries or ordinary factors are causing pain-like symptoms on the forearm, it can lead to the development of trigger points affecting the mobility function of the hands and wrist. To that point, it can lead to a burning sensation or decreased grip strength on the hands. This can affect a person as they won’t be able to hold onto items and are dealing with a numbing sensation along the wrist and hands. Luckily there are pain specialists available that can utilize various techniques to help manage trigger points along the affected muscle and help bring back grip function and mobility to the hands and wrist. People who incorporate these treatments as part of their daily life schedule can begin to get their sense of belonging back without pain in their wrists and hands.
References
Calvo Lobo, Cesar, et al. “Comparison of Hand Grip Strength and Upper Limb Pressure Pain Threshold between Older Adults with or without Non-Specific Shoulder Pain.” PeerJ, PeerJ Inc., 9 Feb. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5345821/.
Cao, Talia, and Prasanna Tadi. “Brachioradialis Reflex.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 26 Mar. 2022, https://www.ncbi.nlm.nih.gov/books/NBK554537/.
Hong, C Z. “Specific Sequential Myofascial Trigger Point Therapy in the Treatment of a Patient with Myofascial Pain Syndrome Associated with Reflex Sympathetic Dystrophy.” Australasian Chiropractic & Osteopathy : Journal of the Chiropractic & Osteopathic College of Australasia, BioMed Central, Mar. 2000, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2050812/.
Lung, Brandon E, et al. “Anatomy, Shoulder and Upper Limb, Forearm Brachioradialis Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 31 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK526110/.
Oh, Sein, et al. “Causes of Hand Tingling in Visual Display Terminal Workers.” Annals of Rehabilitation Medicine, Korean Academy of Rehabilitation Medicine, Apr. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3660483/.
Trinh, Kien, et al. “The Effect of Acupuncture on Hand and Wrist Pain Intensity, Functional Status, and Quality of Life in Adults: A Systematic Review.” Medical Acupuncture, U.S. National Library of Medicine, 1 Feb. 2022, https://pubmed.ncbi.nlm.nih.gov/35251436/.
One of the many muscles that help stabilize the shoulders and provide movement when the arms are in motion. The tricep muscles are one of the most underrated muscles that many people don’t seem to take care of when working out. The other muscles in the upper arms and shoulders are more likely to be worked on when it comes to being physically active. The deltoids, biceps, and brachialis muscles are some of the muscles that get much more attention when working on shoulder mobility. Still, the triceps provide the functionality to the shoulders as well. When the shoulders or the upper arms are injured and develop pain-like symptoms in the muscle groups, it can develop trigger points along the affected muscle. Today’s article looks at the tricep muscles, how trigger points affect them, and ways to manage trigger points along the tricep muscles. We refer patients to certified providers who specialize in arm pain treatments to aid individuals suffering from trigger points associated with the tricep muscles along the upper arms and elbows. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
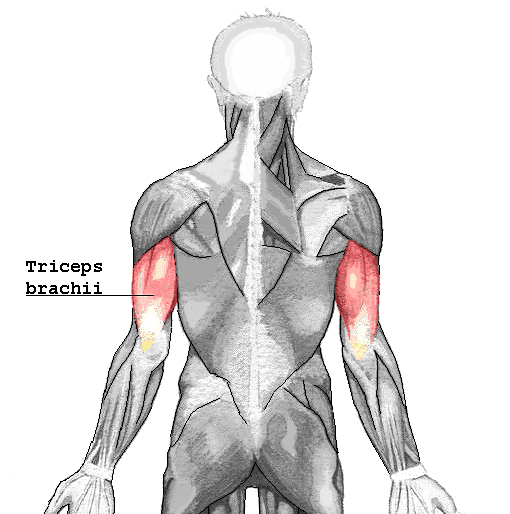
What Do The Tricep Muscles Do?
Do you experience pain underneath your forearm? How about feeling a dull ache on your elbows? Or do you feel a numbing sensation on your ring and pinky fingers? Individuals experiencing these symptoms in their arms could potentially develop trigger points along their tricep muscles. The tricep muscles are located under the upper arm and are a large, thick horseshoe-shaped muscle at the end of the arm. As stated earlier, the tricep muscles are one of the most underrated muscles in the arm that no one tends to work on during a workout, so they can be easily overlooked. However, the tricep muscles help in providing stability to the shoulders and help strengthen the arms. One of the main functions the triceps offer is that they allow the extension of the elbow joints. Studies reveal that the three head tendons that make up the triceps can influence elbow extension torque. The three heads of the triceps have different patterns of force when it comes to various activities during different shoulder evaluations. To that point, multiple combinations of the shoulder and elbows at different angles can affect the tricep’s shoulder extensions. Since many individuals don’t work on their triceps often, it can potentially develop issues that can make this underrated muscle weak.
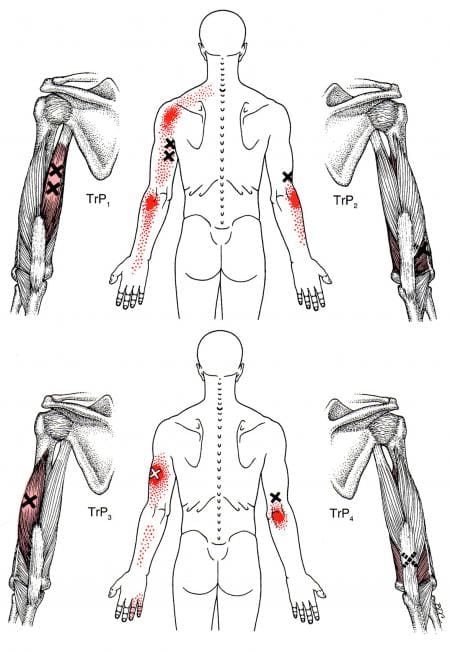
How Trigger Points Affect The Tricep Muscles?
When the triceps don’t get worked on during a workout, it can lead to muscle weakness when doing pushups or when someone suffers from an injury with direct trauma in the elbows. When the tricep muscles become affected, it can lead to chronic conditions that are associated with myofascial pain or trigger points. Trigger points in the triceps can be formed when there are restrictions in extending the elbow joints. Studies reveal that when the triceps become overloaded from overusing the forearms from normal activities, it could potentially lead to tricep tendon rupture. To that point, which leads to the development of trigger points to invoke pain in the triceps and elbow joint. According to Dr. Janet Travell, M.D., trigger points associated with the tricep muscles could potentially involve referred pain in the vicinity of the elbow joints. What this refers to is that trigger points can mimic other chronic conditions so in this case, referred pain caused by trigger points associated with the tricep muscles can be mistakenly attributed to arthritis on the elbow joints. All is not lost, as there are ways to manage trigger points affecting the tricep muscles.
Treating Trigger Points On The Triceps- Video
Have you been experiencing pain in your shoulders, elbows, and hands? Do you have limited mobility when extending your elbows? Or do you notice that your triceps are weaker than normal? If you have been dealing with any of these symptoms, it could be due to trigger points associated with the tricep muscles that are causing referred pain to the upper arms and elbows. The triceps in the upper arms is one of the most underrated muscles people tend to overlook. When individuals begin to succumb to injuries that affect their triceps, it can lead to the development of trigger points along the muscle fibers in the tricep muscles. Trigger points can occur in the tricep muscles due to overusing the forearm muscles, causing stress in the elbow joint and the muscle itself. When the trigger points become active, it can lead to limited mobility to the elbow joint, causing the individual thinks they are developing arthritis when it is the trigger points causing the referred pain. There are ways that many people can manage trigger points associated with the elbows along the triceps to relieve the pain from the muscle. The video above shows where the active trigger points are located and how to release them through palpations and massage. Treating the trigger points along the tricep muscles allows many individuals to regain mobility in their elbows and upper arms.
Managing Trigger Points Along The Triceps
As stated earlier, the triceps are the underrated muscle that people tend to forget. When the tricep muscles succumb to trigger points, it can lead to referred pain along the elbow joints, causing pain-like symptoms affecting the elbow’s mobility function. When this happens to the upper arms, there are various ways to strengthen the tricep muscles and manage trigger points from developing in the future. Incorporating exercises targeting the tricep muscles can help improve mobility to the elbows and shoulders. If a person is playing sports like tennis, they can opt for a lighter racket and have a more lightweight grip on the handle. Suppose a person is in pain from their triceps. In that case, however, studies reveal that upper limb rehabilitation can help reduce the pain along the triceps and improve the mobility range caused by pain associated with trigger points. People can continue their daily activities without pain when they utilize these various ways to enhance their triceps’ functionality.
Conclusion
As the most underrated muscle that people tend to forget to work out, the tricep muscle can be overlooked. This large, thick horseshoe-shaped muscle has a job that provides stability to the shoulders and allows an extension to the elbow joints. When individuals don’t work on their tricep muscles, it can lead to muscle weakness and pain-like symptoms that lead to the development of trigger points. Trigger points associated with the tricep muscles can cause referred pain to the elbow joint, making many individuals believe they have arthritis. However, many individuals can regain mobility to their elbows by incorporating exercises targeting the triceps and utilizing treatments to manage trigger points along the muscle fibers. They can do daily activities that require the triceps without pain.
References
Landin, Dennis, et al. “Functions of the Triceps Brachii in Humans: A Review.” Journal of Clinical Medicine Research, Elmer Press, Apr. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5827912/.
Lennon, Olive, et al. “Effect of the Triceps Brachii Facilitation Technique on Scapulohumeral Muscle Activation during Reach and Point in a Healthy Population.” Physiotherapy Canada. Physiotherapie Canada, University of Toronto Press, 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6855346/.
Mangano, Tony, et al. “Chronic Tendonopathy as a Unique Cause of Non Traumatic Triceps Tendon Rupture in a (Risk Factors Free) Bodybuilder: A Case Report.” Journal of Orthopaedic Case Reports, Indian Orthopaedic Research Group, 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4719357/.
Tiwana, Manpreet S, et al. “Anatomy, Shoulder and Upper Limb, Triceps Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 6 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK536996/.
When it comes to the human body in motion, the arms can carry, lift, and move items from one place to another without pain. The arms have different muscles that work together to protect the arm and shoulder joints while providing mobility and movement. One of the muscles that help the arms carry items is the brachialis muscles, which work together with the bicep and tricep muscles. As part of the forearm, it can succumb to various injuries affecting the muscle, tendons, and ligaments. When this happens, referred pain can affect the arm and develop trigger points to overlap chronic conditions that can potentially cause more pain. Today’s article looks at the brachialis muscle’s function, how trigger points affect the muscle, and various ways to manage brachialis trigger points. We refer patients to certified providers who specialize in arm pain treatments to aid individuals suffering from trigger points associated with the brachialis muscles along the upper arms. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
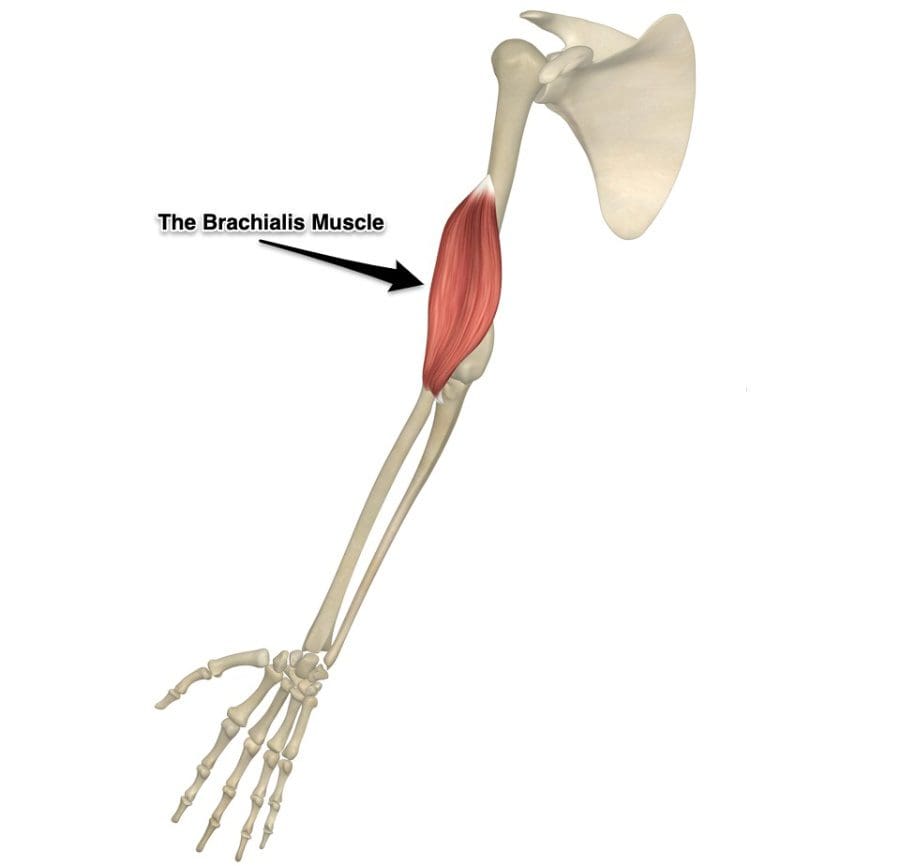
What Is The Brachialis Muscle Function?
Have you been experiencing muscle strain in your forearms? What about stiffness in your wrist? Or do your arm muscles begin to spasm out of nowhere? Many people who have experienced these pain symptoms might be caused by trigger points associated with the brachialis muscle. The brachialis is an important muscle that flexes the forearm at the elbow. This muscle works with the biceps as it can carry heavy items, like the deltoid, and is the opposite of the tricep muscles. However, it can become overused and succumb to injuries that can invoke pain in the arm muscles, thus leading to the development of trigger points along the brachialis muscle.
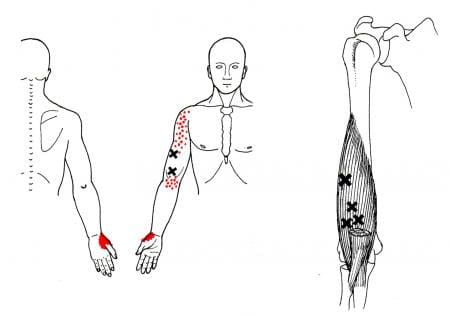
How Does Trigger Points Affect The Brachialis Muscle?
When the brachialis muscle becomes injured, many people will experience pain when flexing their elbows inward or outward. According to Dr. Travell, M.D., these pain symptoms may be due to referred pain and tenderness from brachialis trigger points or radial nerve entrapment. During heaving lifting, the forearm flexion stress overload activates trigger points along the brachialis. Studies reveal that excessive sudden physical stress or repetitive activities may result from a muscle sprain or tear in the brachialis muscle. To that point, these symptoms associated with trigger points can cause overlapping risk profiles that can mask the condition. Some of the conditions that can overlap and activate trigger points include:
Carrying heavy groceries
Holding power tools
Tennis elbow
Playing a string instrument
Studies also reveal that active trigger points along the affected muscle can increase weight coefficients and alter motor control without co-contraction patterns. This is due to trigger points becoming tricky to diagnose and mimic other conditions affecting the arms’ muscle group. Many people with pain-like symptoms associated with trigger points often complain about numbness or deep pain in their arms and hands. To that point, trigger points can also be involved with nerve entrapment in the brachialis muscles.
The Brachialis Trigger Points Release-Video
Have you been experiencing stiffness in your hands and arms? What about muscle spasms near your elbow? Or does constant pain affect your forearm muscles when you bend your arm? Many of these symptoms are associated with trigger points affecting the brachialis muscle that is causing pain in the forearms. Trigger points or myofascial pain syndrome can affect a person’s well-being by impairing their mobility in the affected areas, causing pain, and even reducing their overall sense of life. Trigger points affecting the brachialis muscles can mimic chronic conditions like nerve entrapment that can affect the motor function of the forearm. Luckily, trigger points are treatable, and there are ways to reduce the pain-like symptoms from the affected brachialis muscles. The video above shows how to treat trigger points along the forearm. Incorporating non-invasive treatments to reduce future trigger points to form can reduce the pain symptoms and release the trapped nerves that are causing motor function problems in the arms.
Ways To Manage Brachialis Trigger Points
As stated earlier, trigger points are tricky to diagnose since they can mimic other chronic conditions along the affected muscles. When the affected muscle succumbs to injuries and is not treated, it can develop tiny knots along the taut muscle band fibers known as trigger points over time. To that point, it can cause referred pain-like symptoms along the muscle group. Luckily, treatments can help reduce pain-like symptoms and prevent trigger points from forming along the muscle fibers. Studies reveal that trigger point injections are one of the various treatments that can help reduce pain in the brachialis muscle. With gentle stretching and physical therapy, allow mobility back to the arm. One way to manage brachialis trigger points that many people can use is to place a pillow at the angle of the elbow to prevent the arms from tightening or use a hot pack to relax the forearm muscles to relieve muscle strain and aches. Another way is not to overuse their forearms when playing an instrument or carrying items on their forearms. This can prevent trigger points from forming in the future and reduce pain-like symptoms from affecting the forearms.
Conclusion
The brachialis is the main muscle that is important to the forearms. This large muscle works with the bicep and tricep muscles to help the host carry heavy objects while bending at the elbows. However, like all the muscles in the body, the brachialis muscles can succumb to injuries and develop trigger points along the brachialis muscle fiber bands. Trigger points along the brachialis muscle are associated with pain-like symptoms that can mimic conditions like tennis elbow or nerve entrapment in the forearms. Fortunately, various treatments are utilized by doctors to help many patients dealing with trigger points along the brachialis muscle and can help reduce pain in the forearms. This allows mobility back to the arms and prevents future trigger points from forming.
References
Geri, Tommaso, et al. “Myofascial Trigger Points Alter the Modular Control during the Execution of a Reaching Task: A Pilot Study.” Scientific Reports, Nature Publishing Group UK, 5 Nov. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6831581/.
Plantz, Mark A, and Bruno Bordoni. “Anatomy, Shoulder and Upper Limb, Brachialis Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 22 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK551630/.
Sharma, Pankaj, et al. “Isolated Traumatic Brachialis Muscle Tear: A Case Report and Review of Literature.” Bulletin of Emergency and Trauma, Shiraz University of Medical Sciences, Oct. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5694606/.
Suh, Mi Ri, et al. “Ultrasound-Guided Myofascial Trigger Point Injection into Brachialis Muscle for Rotator Cuff Disease Patients with Upper Arm Pain: A Pilot Study.” Annals of Rehabilitation Medicine, Korean Academy of Rehabilitation Medicine, Oct. 2014, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4221396/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine